
Abstract
Background:
A new cell-based serum anticholinergic activity (cSAA) assay that measures anticholinergic activity specifically at muscarinic M1 receptors and eliminates many of the drawbacks of the existing assay was developed by our team.
Aims:
We aimed to study the relationship between changes in working memory and executive function with changes in cSAA using the new assay in cognitively healthy older adults.
Methods:
Cognitively healthy participants aged 50 years and above, received a single dose of 0.4 mg of intravenous scopolamine. Cognition and cSAA levels were measured before and 30 min after receiving scopolamine. Cognition was measured using the Cambridge Neuropsychological Test Automated Battery.
Results:
Ten participants were recruited, and nine (mean age = 69.8, SD = 9.5, range 59–86 years) completed the study. Following scopolamine, participants experienced an increase in cSAA (cSAA pre = 0.90 ± 0.97 vs cSAA post = 12.0 ± 3.70 pmol/L; t-test (df = (8) = −9.5, p < 0.001). In addition, there was an association between change in cSAA and changes in working memory (Spearman’s ρ = 0.68, p = 0.042) and executive function (Spearman’s ρ = 0.72, p = 0.027).
Conclusions:
In our sample of cognitively healthy older adults, the new cSAA assay was able to quantify the scopolamine induced increase in anticholinergic load which correlated significantly with the observed decline in working memory and executive function.
Introduction
Use of medications with anticholinergic properties has been associated with deleterious effects on cognition. Increase in mild cognitive impairment (MCI) diagnosis among older patients on anticholinergic medications at a 1-year follow-up and decline in global cognitive function among those on these medications at a 4-year follow-up have been reported (Ancelin et al., 2006; Carriere et al., 2009) Further, chronic anticholinergic burden predicts longitudinal cognitive decline and eventual diagnosis of MCI (Ancelin et al., 2006). This is especially a concern in older adults who take numerous medications with anticholinergic properties (Chew et al., 2008; Green et al., 2019) and are more susceptible to the adverse effects due to a combination of factors including lower cognitive reserve, more permeable blood–brain barrier, and fewer cholinergic receptors (Cai et al., 2013; Cardwell et al., 2015; Gerretsen and Pollock, 2011). Some of the common medications with anticholinergic properties taken by older adults include bladder antimuscarinics such as tolterodine, solifenacin, fesoterodine, and darifenacin; antihistaminics such as diphenhydramine, dimenhydrinate, and promethazine; and antidepressants such as paroxetine, nortrypyiline, and amitryptiline; cardiovascular medications including digoxin; and diuretics such as furesemide and Parkinsonian medications including trihexyphenidyl and tropatepine.
The validity of the existing serum anticholinergic activity (SAA) assay, introduced in the early 1980s (Tune and Coyle, 1980, 1981) as a measure of anticholinergic burden, is a subject of continuous debate because of its limitations.(Carnahan et al., 2002; Cox et al., 2009; Salahudeen, Chyou et al., 2016). Anticholinergic medications but also plasma proteins and endogenous anticholinergic hormones, such as cortisol, may all contribute to measurable SAA (Carnahan et al., 2002; Cox et al., 2009; Kersten and Wyller, 2014). The assay measures serum displacement of radioactive [3H]Quinuclidinyl benzilate binding to an in vitro suspension of rat brain homogenates. There is inherent variability associated with the preparation of these homogenates. Most published studies use cross-sectional rather than longitudinal designs and show significant interindividual variability in SAA, with no clear cutoff that predicts the presence of delirium or chronic neurocognitive dysfunction (Carnahan et al., 2002; Cox et al., 2009). Further, the assay does not discriminate between various subtypes of muscarinic receptors, which may limit the applicability of this methodology in research on cognition. Only two of the five known muscarinic receptor subtypes (M1 and M2) have been shown to be involved in cognitive functions (Anagnostaras et al., 2003). M1 receptors are the most abundant muscarinic receptor type in the brain and have been most implicated in cognitive functions (Abrams et al., 2006; Anagnostaras et al., 2003).
Expert consensus derived rating scales such as the Anticholinergic Burden Scale and the Anticholinergic Drug Scale are an alternative method for assessing anticholinergic burden. However, these are also associated with a lack of uniformity and variability of outcomes (Salahudeen et al., 2015). The Drug Burden Index, a method used to quantify burden due to anticholinergic and sedative medications, is not selective for measuring anticholinergic burden alone (Hilmer et al., 2009). A nonlinear model to predict anticholinergic burden among hospitalized older patients using population level data was developed by Salahudeen et al. (2015).
To address these limitations, our team developed a new cell-based serum anticholinergic activity (cSAA) assay. This is a high-throughput protocol using 96-well microplates and involves radioligand binding to cultured cells that stably express M1 receptors (Nobrega et al., 2017). This is in contrast to the use of rat brain tissue in the existing assay, which potentially expressed various types of muscarinic receptors (Tune and Coyle, 1980). Possible confounds caused by endogenous proteins in serum are addressed by using a perchloric acid pretreatment. The differences between the original assay and the modified cell-based assay are summarized in Table 1.
Differences between original SAA and the cultured cSAA.
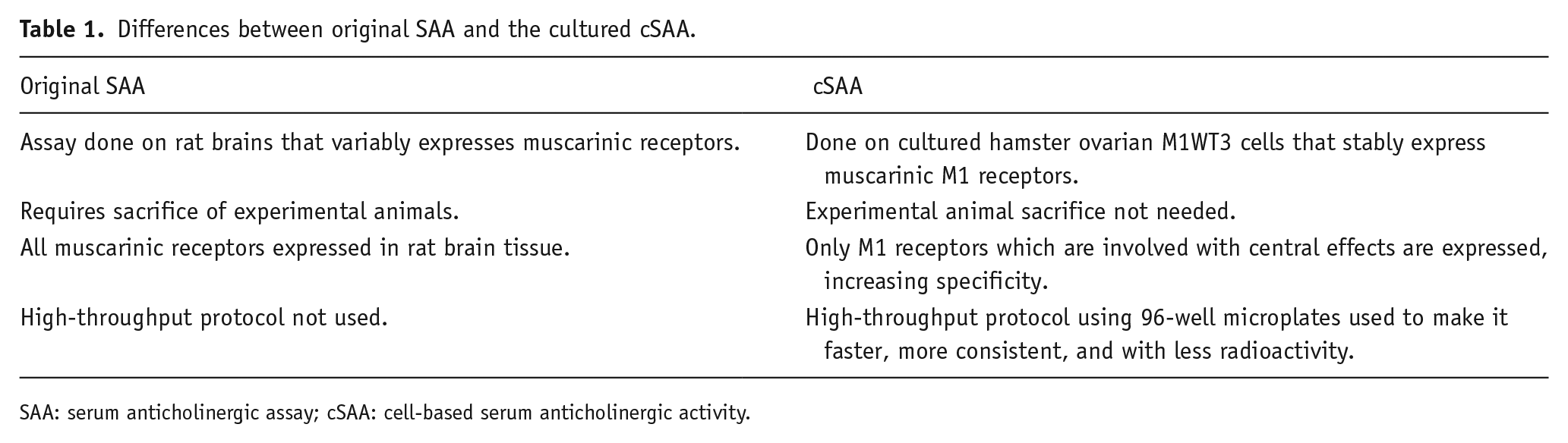
SAA: serum anticholinergic assay; cSAA: cell-based serum anticholinergic activity.
However, this assay has not been validated longitudinally in vivo in human volunteers. Thus, we aimed to conduct an exploratory study to test the validity of this novel and enhanced method of measuring anticholinergic burden using blood samples obtained from cognitively healthy human participants before and after receiving a single dose of scopolamine, a well-tolerated medication associated with increased anticholinergic load (Molchan et al., 1992). Secondly, we aimed to test the relationship between the new cSAA measure and cognitive performance. We hypothesized that cSAA values would be significantly increased after a single dose of scopolamine. Previous research has demonstrated that the cholinergic system plays an important role in working memory and complex attentional processes and cue detection essential for executive function (Hasselmo and Sarter, 2011; Rajji et al., 2015). Further, the muscarinic system is known to support working memory through multiple mechanisms including cue detection and control of attention (Demeter and Sarter, 2013) Based on this, we hypothesized that cognitive performance, especially working memory, would decline after receiving single-dose scopolamine, and this decrease, that is, an increase in working memory errors would be positively correlated with the change in cSAA values.
Methods
This was an open-label prospective study design, conducted at the Centre for Addiction and Mental Health (CAMH), Toronto. Ten cognitively intact healthy participants were recruited, through referrals by word of mouth, referrals from clinicians in the community, from within CAMH through use of the existing database, posting on CAMH research registry, and advertisements. Voluntary written informed consents were obtained prior to study procedures.
Participants
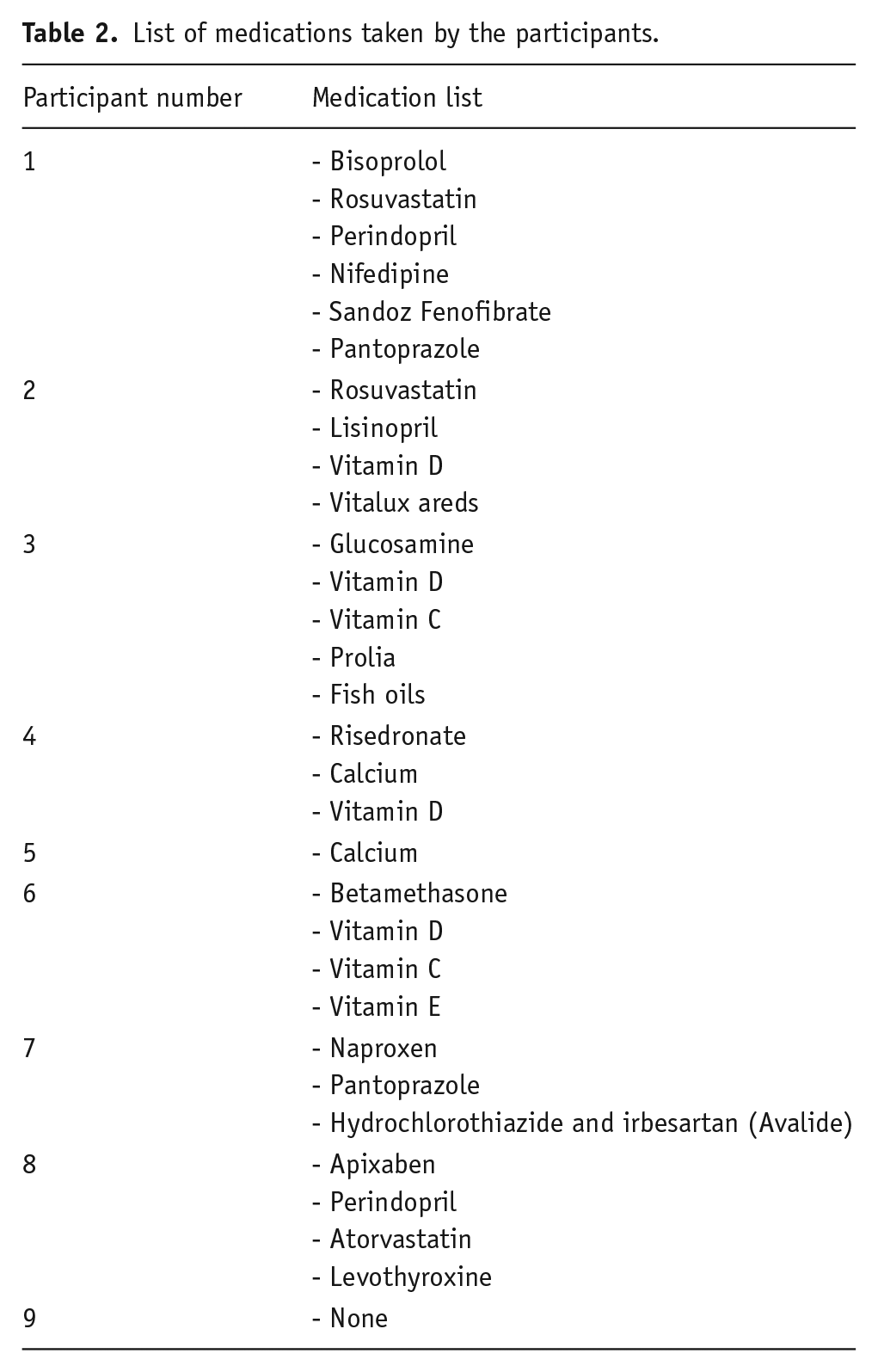
Both males and females aged 50 years or above were considered for the study. They needed to have an available study partner who had regular contact with the participant for confirmation of cognitive status and the ability to read and communicate in English. Participants who met DSM IV criteria for any diagnosis, had significant neurological or unstable medical conditions that would preclude safe use of scopolamine, were currently using medications with anticholinergic activity, or were hypersensitive to scopolamine or belladonna alkaloids were excluded from the study. A list of medications taken by the participants at the time of the study is provided (Table 2). Participants who had risk factors for developing angle closure glaucoma were required to undergo an eye exam prior to participation.
List of medications taken by the participants.
The study took place over two visits. During the first visit, written informed consent was obtained, and eligibility criteria were assessed. During the second visit, the eligible participants underwent cognitive testing and provided blood samples prior to and after a 0.4-mg dose of intravenous (IV) scopolamine. The study flow is represented in Figure 1.
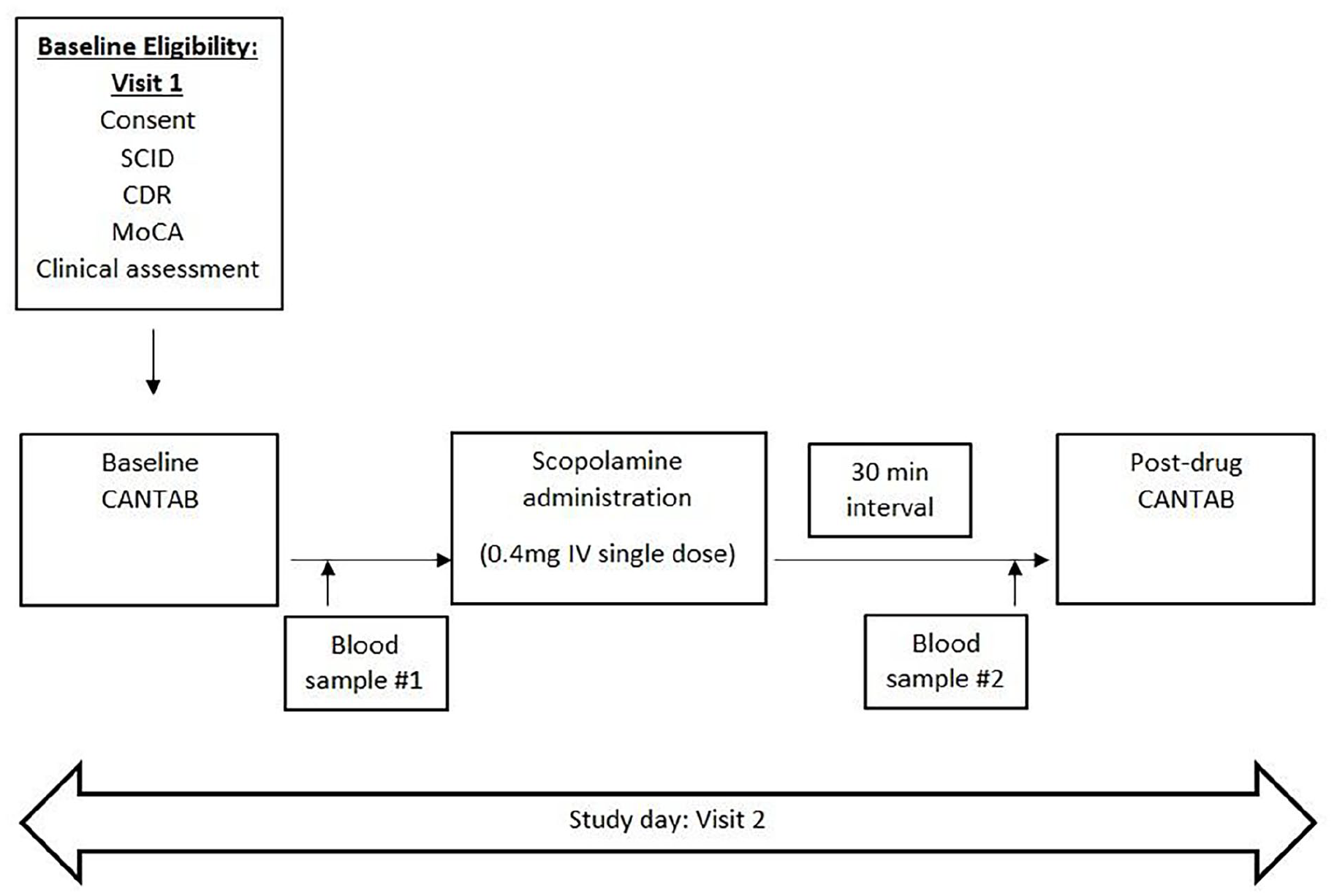
Study flow.
Assessments
Structured clinical interview for the DSM-IV (SCID-IV): The SCID-IV assesses current and lifetime psychiatric disorders. It was used to clarify psychiatric inclusion and exclusion criteria (First et al., 2002).
The Montreal Cognitive Assessment (MoCA) is a validated, brief cognitive screening tool for detecting MCI with high sensitivity and specificity (Nasreddine et al., 2005).
Clinical Dementia Rating Scale (CDR) quantifies the severity of dementia based on six domains of cognitive and functional ability: memory, orientation, judgment, and problem-solving, community affairs, homes and hobbies, and personal care (Hughes et al., 1982).
Cambridge Neuropsychological Test Automated Battery (CANTAB-AD): This is a standardized and validated battery, based on well-established neurocognitive experimental paradigms (www.cambridgecognition.com). It consists of 22 tasks that assess neurocognitive processes within a wide range of relatively independent cognitive domains, including visual memory, attention, working memory, and problem-solving. Each of the tasks is graded, allowing the assessment of patients with varying levels of impairment. The tasks are automated and therefore testing is given in a standardized manner with standardized feedback about accuracy and speed. The CANTAB has a normative database based on more than 2000 normal controls between 4 and 90 years of age. Estimates of test–retest reliability and of practice effects are available for many of the CANTAB tasks based on an elderly sample. The CANTAB has been used in a variety of clinical populations providing an opportunity to compare findings related to different disorders. Finally, the CANTAB tasks are independent of language and culture and can be used in populations for whom English is not a primary language (Strauss et al., 2006).
Biomarkers
Blood samples were collected before and 30 min after scopolamine administration for evaluating cSAA.
The modified assay includes the use of the following key components:
(i) M1WT3 cells which stably express M1 receptors. This is in contrast to rat brain tissue that possibly expresses several types of muscarinic receptors. This would help increase specificity and decrease variability and would also avoid sacrifice of experimental animals.
(ii) Ninety-six-well microplates to obtain high throughput, that would increase consistency, reduce time, and reduce the amount of radioactivity needed.
(iii) Neutralization of the confounding effects of endogenous proteins through perchloric acid pretreatment.
Study drug
Scopolamine hydrobromide is a naturally occurring alkaloid of the belladonna plant and is an antimuscarinic agent which antagonizes the action of acetylcholine at muscarinic receptors. The advantages of administering it using an IV route include rapid onset of action (5–10 min), known pharmacokinetics (plasma levels peak at 30 min), shorter half-life (approximately 1 h), and availability (oral form is not available in Canada) (Putcha et al., 1989; Renner et al., 2005). Scopolamine is commonly used as a standard drug for inducing cognitive deficits in healthy humans and animals for the purposes of research. It produces widespread cognitive deficits in a dose- and time-dependent manner (Klinkenberg and Blokland, 2010; Lenz et al., 2012; Snyder et al., 2005). Cognitive functions approach their maximum level of depression by 30–45 min after the dose (Petersen, 1977), which is reflected in the study design. Scopolamine at a 0.4-mg dose is associated with a significant decline in psychomotor function, visual learning, and executive function at 2 and 3 h after administration; however, the reduction of these symptoms is linear and by 9 h after dosing cognitive function conditions return to baseline levels (Ebert et al., 1998; Fredrickson et al., 2008).
The most frequently reported adverse effects of scopolamine are dry mouth and drowsiness, occurring in 29% and 17% of patients, respectively (Jovaisas and Farnham, 2014). Other less frequent side effects include ocular effects such as blurred vision, mydriasis, cycloplegia, and acute angle-closure glaucoma in predisposed patients; dermatologic effects such as rash and rarely, erythema (Jovaisas and Farnham, 2014). Central nervous system effects such as disorientation, confusion, hallucinations, and delirium are possible, with older adults being more susceptible. For the purposes of this research, the risk of acute glaucoma was excluded by obtaining participants’ medical history and conducting a brief clinical examination to check for the presence of ocular pain, vision loss, blurred vision, halos around light, eye redness, headache, visual field loss, inability to read newspaper headlines, history of glaucoma, history of increased intraocular pressure or eye surgery, and family history of glaucoma (Gupta and Chen, 2016; Prum et al., 2016).
The risks of scopolamine were explained in detail to participants, and close clinical monitoring was carried out to ensure the appropriateness and safety of their continued participation. The participants remained on site for observation for 3 h after scopolamine administration. Since drowsiness, disorientation, and confusion could occasionally occur with the use of scopolamine, patients were cautioned about the potential risk of engaging in activities that require mental alertness, such as driving a motor vehicle or operating dangerous machinery and were asked to be accompanied or driven to and from the appointment for any potential safety concerns.
Statistical analysis
We computed the baseline demographic and clinical characteristics of our sample. Student’s t-test was used to test for significant increase in cSAA after scopolamine injection, and Spearman’s correlations were used to assess correlation between changes in cSAA and changes in cognition. For all the tests, the statistical significance threshold was determined at the 0.05 level. The statistical software used was IBM SPSS Statistics version 24 (IBM Corp, Armonk, NY, USA).
Results
Baseline characteristics
Ten participants were recruited, and nine (mean age = 69.8, SD = 9.5, range 59–86 years) completed the study. One participant was withdrawn due to gastrointestinal distress following scopolamine administration. Two out of the nine were males (22.2%). The mean McCA score for all participants was 27.6 ± 2.5, and mean CDR score was 0.05 ± 0.16 (Table 1).
CSAA scores pre and post scopolamine
Following IV scopolamine administration, participants demonstrated an increase in cSAA levels, measured in pmol/L (cSAA pre = 0.90 ± 0.97 vs SAA post = 12.0 ± 3.70). Paired sample t-test was performed to calculate the mean difference between the two and was found significant (t-test (df = 8) = −9.5, p < 0.001) (Table 3).
Baseline characteristics of study sample, n = 9.
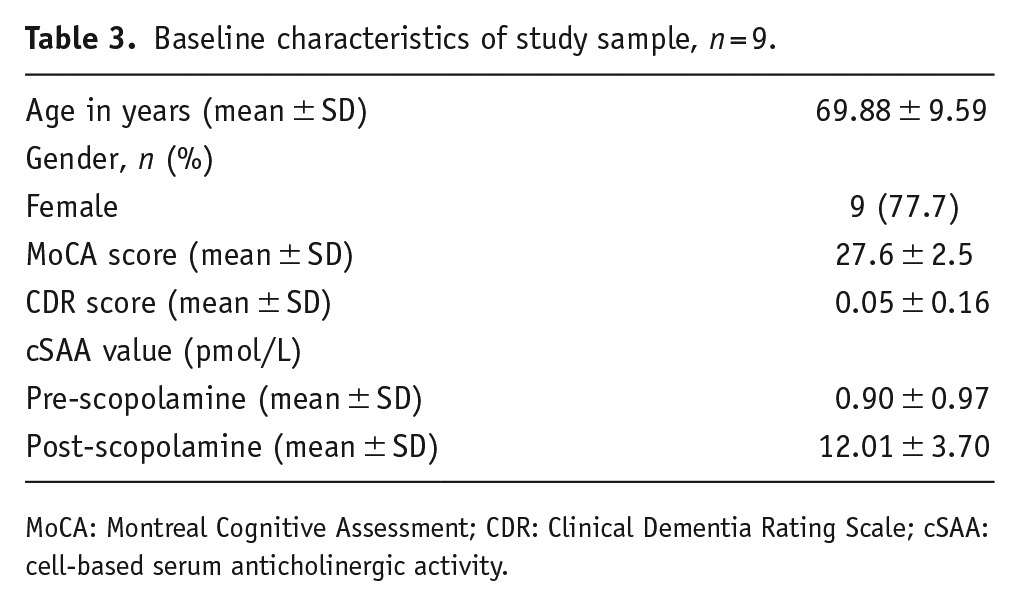
MoCA: Montreal Cognitive Assessment; CDR: Clinical Dementia Rating Scale; cSAA: cell-based serum anticholinergic activity.
CANTAB scores pre and post scopolamine
A change in multiple cognitive domains was noted post scopolamine. These included working memory which was close to significance (pre = 27.2 ± 15.4 vs post = 47.1 ± 30.0; t-test (df = 8) = −2.1, p = 0.061) and significant changes in episodic memory (pre = 3.1 ± 0.7 vs post = 1.8 ± 1.2; t-test (df = 8) = 2.4, p = 0.038), reaction time (pre = 378 ± 93.1 vs post = 485.6 ± 68.8; t-test (df = 8) = −3.4, p = 0.009), and sustained attention (pre = 0.9 ± 0.02 vs post = 0.84 ± 0.06; t-test (df = 8) = 4.0, p = 0.004) (Table 4).
Changes in cognitive functions pre and post scopolamine and correlation between differences in cognitive scores and difference in cSAA, n = 9.
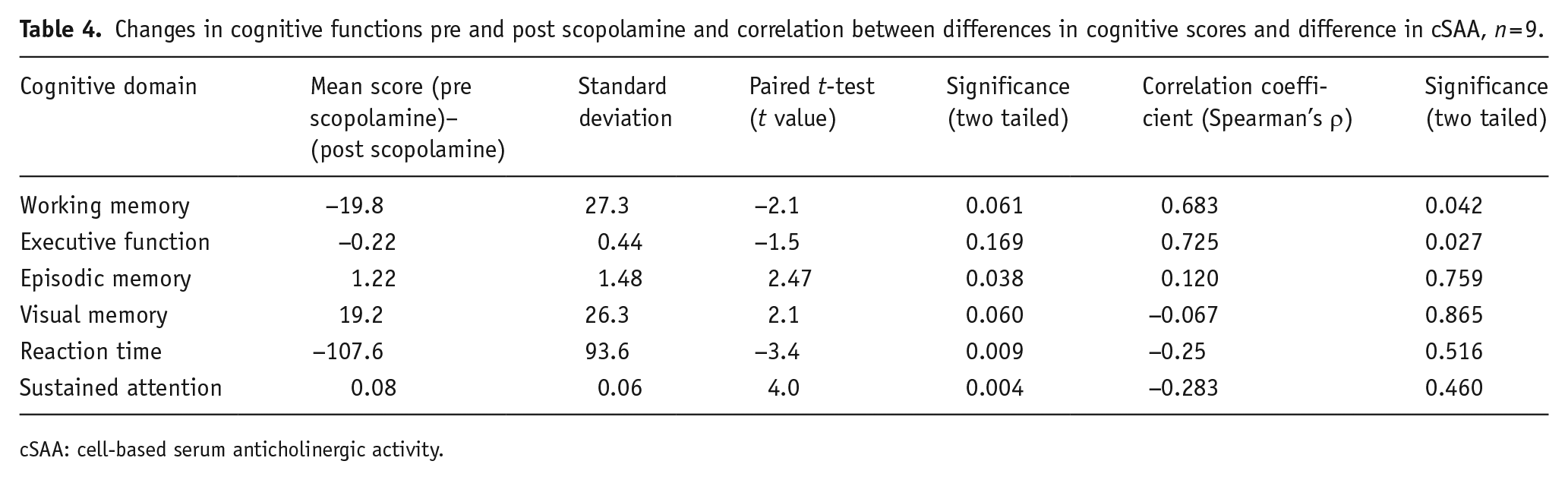
cSAA: cell-based serum anticholinergic activity.
Correlation between changes in CANTAB scores and cSAA pre and post scopolamine
As predicted, there was an association between change in cSAA with and change in working memory (Spearman’s ρ = 0.68, p = 0.042), as well as with change in executive function (Spearman’s ρ = 0.72, p = 0.027). We did not find significant association of changes in SAA scores with those of reaction time, visual memory, episodic memory, or sustained attention (Table 3)
Discussion
The current study applied the newer cSAA on a small sample of human volunteers over 50 years of age. We repeated the assay and cognitive testing before and after the administration of scopolamine and studied the association between changes in the assay with those of cognitive functions. The assay was able to quantify the changes in anticholinergic burden caused by scopolamine, with significant increase in values after the administration of the test drug. Further, the increase in the assay values correlated significantly with decline in working memory and executive function post scopolamine.
The original serum anticholinergic assay developed by Tune and Coyle (1980) is based on the displacement of [3H]QNB binding in rat brain homogenates by human serum. There have been many doubts about the validity of this assay (Carnahan et al., 2002; Lampela et al., 2015; Salahudeen, Nishtala et al., 2016). Serum proteins might act as confounders in measuring the anticholinergic burden in the older assay (Cox et al., 2009). Further, it does not differentiate between different subtypes of muscarinic receptors. Only M1 and M2 receptors have been proven to be involved in cognitive functions (Anagnostaras et al., 2003). Specifically, the M1 receptor has been most clearly associated with cognitive functions and is dominantly present in the brain. (Levey et al., 1991) (Abrams et al., 2006; Xiong et al., 2019). This, along with the numerous limitations present in the use of anticholinergic rating scales (Salahudeen et al., 2015) provided the stimulus for the development of the newer serum anticholinergic assay. Our team has previously demonstrated the relationship between the cSAA with working memory in a sample of older adults with MCI or major depressive disorder or both (Chandramouleeshwaran et al., 2021), but this is the first report on longitudinal change in cSAA and cognition.
Scopolamine is often used as a research drug to induce reversible and time-dependent cognitive decline in human and animal models (Klinkenberg and Blokland, 2010) and produced cognitive changes in multiple domains including sustained attention, working memory, episodic memory, and reaction time (Broks et al., 1988; Petersen, 1977). When used in our study, it produced significant decline in these domains.
Previous findings indicate that anticholinergic burden selectively affects certain cognitive domains more than others; specifically, executive function and working memory appear to be domains that are exquisitely sensitive to anticholinergic effects (Carriere et al., 2009; Han et al., 2008; Uusvaara et al., 2013). This has also been shown by our team while studying the effects of clozapine on working memory in schizophrenia patients (Rajji et al., 2015) The changes in the cSAA significantly correlated with changes in working memory and executive function, post scopolamine, adding validity to the new assay. The changes in the assay post scopolamine did not show significant association in other domains such as visual memory, episodic memory, sustained attention, or reaction time.
We would like to acknowledge some limitations of this study. The sample size was small, as this was an exploratory study in which we used the newer assay on human volunteers for the first time and was therefore not designed as a randomized control trial. Further, the assay tests peripheral blood and would therefore may not reflect the direct impact of the scopolamine on the brain, though we did note a significant association with changes in the assay with changes in working memory and executive function. Despite our attempts to overcome the effect of plasma proteins and endogenous anticholinergic hormones, it is also possible that they may still affect the assay results (Nobrega et al., 2017). We also acknowledge the possibility of type 1 error in this exploratory study.
Despite these limitations, we were able to determine potentially useful findings that merit future research. We conducted a trial of a new laboratory assay, which is designed to overcome the limitations of the existing assay and tested it on a group of older adults. The assay was able to significantly pick up the changes in blood anticholinergic levels after introduction of a single dose of scopolamine and quantified this change. We further established a significant correlation between the changes in this new assay and those of working memory and executive function, before and after the use of scopolamine. These results support the validity of this new assay. Future studies with larger samples examining the predictive value of the new cSAA on cognition are required.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JNN, RR, and BGP are holders of United States Provisional Patent No. 16/490,680, Canadian Provisional Patent No. 3,054,093; and JNN, RR, and BGP are holders of United States Provisional Patent No.17/396,030 for a cell-based assay and kits for assessing serum anticholinergic activity. TKR has received research support from Brain Canada, Brain and Behavior Research Foundation, BrightFocus Foundation, Canada Foundation for Innovation, Canada Research Chair, Canadian Institutes of Health Research, Centre for Aging and Brain Health Innovation, National Institutes of Health, Ontario Ministry of Health and Long-Term Care, Ontario Ministry of Research and Innovation, and the Weston Brain Institute. TKR also received for an investigator-initiated study in-kind equipment support from Newronika and in-kind research online accounts from Scientific Brain Training Pro and participated in 2021 in one advisory board meeting for Biogen Canada Inc. TKR is also an inventor on the United States Provisional Patent No. 17/396,030 that describes cell-based assays and kits for assessing serum cholinergic receptor activity.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by CAMH Foundation.