
Abstract
Background:
Clinical use of psychedelics has gained considerable attention, with promising benefits across a range of mental disorders. Current pharmacological and psychotherapeutic treatments for body dysmorphic disorder (BDD) and eating disorders (EDs) have limited efficacy. As such, other treatment options such as psychedelic-assisted therapies are being explored in these clinical groups.
Aims:
This systematic review evaluates evidence related to the therapeutic potential of psychedelics in individuals diagnosed with BDD and EDs.
Methods:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, we conducted a systematic review of all study designs published to the end of February 2022 that identified changes in ED/BDD symptom severity from psychedelics using validated measures to assess symptom changes.
Results:
Our search detected a total of 372 studies, of which five met inclusion criteria (two exploratory studies, two case reports, and one prospective study). These were included in the data evaluation. Effects of psychedelics on BDD and various ED symptoms were identified mostly through thematic analyses and self-reports.
Conclusions:
Our findings highlight that more research is needed to determine the safety and efficacy of psychedelics in BDD and EDs and we suggest avenues for future exploration.
Keywords
Introduction
There are several psychiatric disorders characterized by excessive concern with physical appearance, to the extent of distress and functional impairment. One such disorder is body dysmorphic disorder (BDD), an obsessive-compulsive related disorder (OCRD) identified by misperceptions of appearance features being defective, flawed, and unattractive, and intrusive preoccupations concerning their physical appearance. Behavioral symptoms of BDD include avoiding or constantly checking mirrors, skin picking, and excessive hair plucking (Pavan et al., 2008). Another group of disorders in which concerns regarding appearance are a major feature are eating disorders (EDs), notably anorexia nervosa (AN). EDs are characterized by severe disturbances in eating behavior, body image, and body weight. They are associated with high rates of morbidity, mortality, and hospitalization, as well as significantly impaired quality of life. There is overlap between BDD and AN such that around 25–39% of people with AN have concerns about aspects of their physical appearance not specific to shape and weight (Grant et al., 2002; Rabe-Jablonska Jolanta and Sobow Tomasz, 2000). Evidence from neuroimaging and neurophysiology studies have found similar abnormalities in visuospatial processing and structural connectivity in both populations which may contribute to distorted body image across these disorders (Phillipou et al., 2019). In addition, BDD and AN patient populations demonstrate commonalities in sociodemographic characteristics, level of body dissatisfaction and preoccupation, and altered experience of emotion (Phillipou et al., 2019). People with BDD and EDs also frequently suffer from comorbid psychological symptoms and disorders such as substance use disorders, obsessive-compulsive disorder (OCD), self-harm, and suicidality (Anderson et al., 2002; Phillipou et al., 2019; Pisetsky et al., 2013). Treatment modalities for EDs depend on the type and severity, but generally include both therapeutic programs such as family-based therapy for adolescents and cognitive behavioral therapy (CBT) and pharmacological interventions such as serotonin reuptake inhibitors (SERTs) and drugs for psychosis (Harding et al., 2021). Unfortunately, relapse rates remain high and treatment response remains low (Berkman et al., 2007; Khalsa et al., 2017). BDD treatment usually incorporates CBT, often in addition to SERTs and drugs for psychosis (Singh and Veale, 2019). As with EDs, people with BDD often have suboptimal responses to these treatments, and many have residual disabling symptoms. Not surprisingly, there has been a call for new treatments for these vulnerable populations (Schmidt and Campbell, 2013). Recent studies have explored the potential of brain stimulation therapies such as deep brain stimulation (Lipsman et al., 2013, 2017; Murray et al., 2022) and repetitive transcranial magnetic stimulation (McClelland et al., 2016; Murray et al., 2022; Van den Eynde et al., 2013), and a synthetic tetrahydrocannabinol known as dronabinol (Andries et al., 2014). Although there have been several advances in the field, there is still much room for improvement in treatment outcomes and dropout rates (Berkman et al., 2007; Linardon and Wade, 2018).
After several decades, the use of classic psychedelic compounds in psychiatry is garnering renewed research interest. Classic psychedelics are traditionally defined as hallucinogenic drugs that impact the serotonergic system in the human body. Generally, psilocybin, lysergic acid diethylamide (LSD), and ayahuasca, among others, are included in this category. These drugs were first investigated as therapeutic agents for psychiatric illnesses in the late 1940s (Nichols and Walter, 2021). However, political concerns over public consumption and an emerging “counter culture” resulted in a halt in psychedelic research until more recently (Nichols and Walter, 2021). In particular, a resurgence in research involving patients with end-of-life anxiety and depression has demonstrated supportive evidence that psilocybin combined with psychotherapy is both safe and efficacious in reducing psychological symptoms (Agin-Liebes et al., 2020; Carhart-Harris et al., 2021; Davis et al., 2021; Griffiths et al., 2016; Grob et al., 2011). Mechanistically, classic psychedelics activate serotonin receptors, specifically 5-HT2A, located in cortical and subcortical structures in the brain (Vollenweider and Preller, 2020). This is postulated to help disrupt habitual thought patterns and promote cognitive flexibility which may be of therapeutic potential in the treatment of disorders in which people become “stuck” in an internal cycle of obsessive concern, including EDs as well as OCD (Moreno et al., 2006), to which BDD is related (Foldi et al., 2020).
In light of the overlap in symptoms and some convergence in neurobiological underpinnings between BDD and EDs, as well as the pressing need for better treatments in these disorders, the present systematic review collects and critically evaluates published evidence related to the therapeutic impact psychedelics have on patients diagnosed with EDs and BDD.
Materials and methods
Search strategy
This systemic review was conducted in accordance with the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). A search to identify relevant studies was conducted for the following databases: PsycInfo, PubMed, Embase, Web of Science, Google Scholar, Cochrane Library, and CINAHL. Gray literature was searched using WorldCat and Google Scholar. The following keywords were searched and adapted to each database to find appropriate articles: “Psychedelic*” OR “Hallucinogen*” OR “LSD” OR “Lysergic Acid Diethylamide” OR “Psilocybin” OR “Psiloci*” OR “Mescaline” OR “Trimethoxyphenethylamine” OR “Mezcalin” OR “Peyote” OR “DMT” OR “N,N-Dimethyltryptamine” OR “Ayahuasca” OR “Psychedelic Serotonin Agonist*” AND “Body Image” OR “Body Image Disorder*” OR “Anorexia Nervosa” OR “AN” OR “Bulimia” OR “Bulimia Nervosa” OR “BN” OR “Binge-Eating Disorder” OR “BED” OR “Avoidant/Restrictive Food Intake Disorder” OR “ARFID” OR “Eating Disorder Not Otherwise Specified” OR “EDNOS” OR “Atypical Eating Disorder” OR “Body Dysmorphic Disorder” OR “Body Dysmorphia” OR “BDD” OR “Muscle Dysmorphia” OR “dysmorphophobia” OR “Other Specified Feeding and Eating Disorder” OR “OSFED” OR “Unspecified Feeding or Eating Disorder” OR “UFED”. All studies written in English, published through to the end of February 2022 were considered. The search was limited to classic psychedelic drugs that function largely through the activation of the serotonin 5-HT2A receptor. Due to differing modes of action, trials investigating the use of 3,4-methylenedioxymethamphetamine (MDMA) were not included in the search.
Inclusion and exclusion criteria
All study designs (e.g., case reports, observational studies, randomized controlled trials) reporting on the use of psychedelic drugs in patients with EDs and/or BDD were included in the study. Following the Population, Intervention, Comparison, Outcomes (PICO) framework, criteria for selecting the studies were as follows: Population (P): patients with a diagnosis of an ED and/or BDD as defined by the International Classification of Diseases 10th Revision or the Diagnostic and Statistical Manual of Mental Disorders (DSM); Intervention (I): Serotonergic psychedelic use including, but not limited to, psilocybin, mescaline, LSD, ayahuasca, and/or dimethyltryptamine; Comparison (C): Low dose of psychedelic drugs, placebo, active placebo, or a test group acting as their own control. Studies that did not include control groups or comparators (e.g. case reports) were included; and Outcomes (O): Descriptive (e.g. case studies, dissertations) changes in ED/body image disorder symptom severity, and/or any validated measures to assess symptom changes.
The exclusion criteria were as follows: (1) articles not published in English and (2) studies conducted in animals only. Citation lists of retrieved articles and reviews were searched. In addition, registered clinical trials were searched on the World Health Organization International Clinical Trials Registry Platform, ClinicalTrials.Gov, and the Australia and New Zealand Clinical Trial Registry.
Data extraction
All studies generated from the search were uploaded into the online software Covidence (Veritas Health Innovation, Melbourne, Australia) and duplicate studies were automatically removed. Title and abstract screening as well as full-text review was conducted by two independent reviewers (NL and JR). Conflicts at the title/abstract screening stage and the full-text review stage were resolved by a third independent reviewer (DC). Due to the limited number of articles, data were extracted by one reviewer (NL) and reviewed with the study team. The variables extracted included the following: (1) study objectives, (2) study design, (3) sample characteristics, (4) ED diagnosis investigated, (5) psychedelic assessed, (6) assessment measures, and (7) results.
Results
A flow chart of the selection process is reported in Figure 1. Our search yielded a total of 372 studies. Of these studies, 92 duplicates were removed and 26 articles were full-text reviewed. No additional studies were found by reviewing the citation lists of retrieved studies. After reviewing full texts, 21 articles were excluded for specified reasons, namely wrong publication type, wrong study outcomes, and unsuitable study population. A total of five articles met eligibility criteria (Table 1). Only one case report was of a patient with BDD.
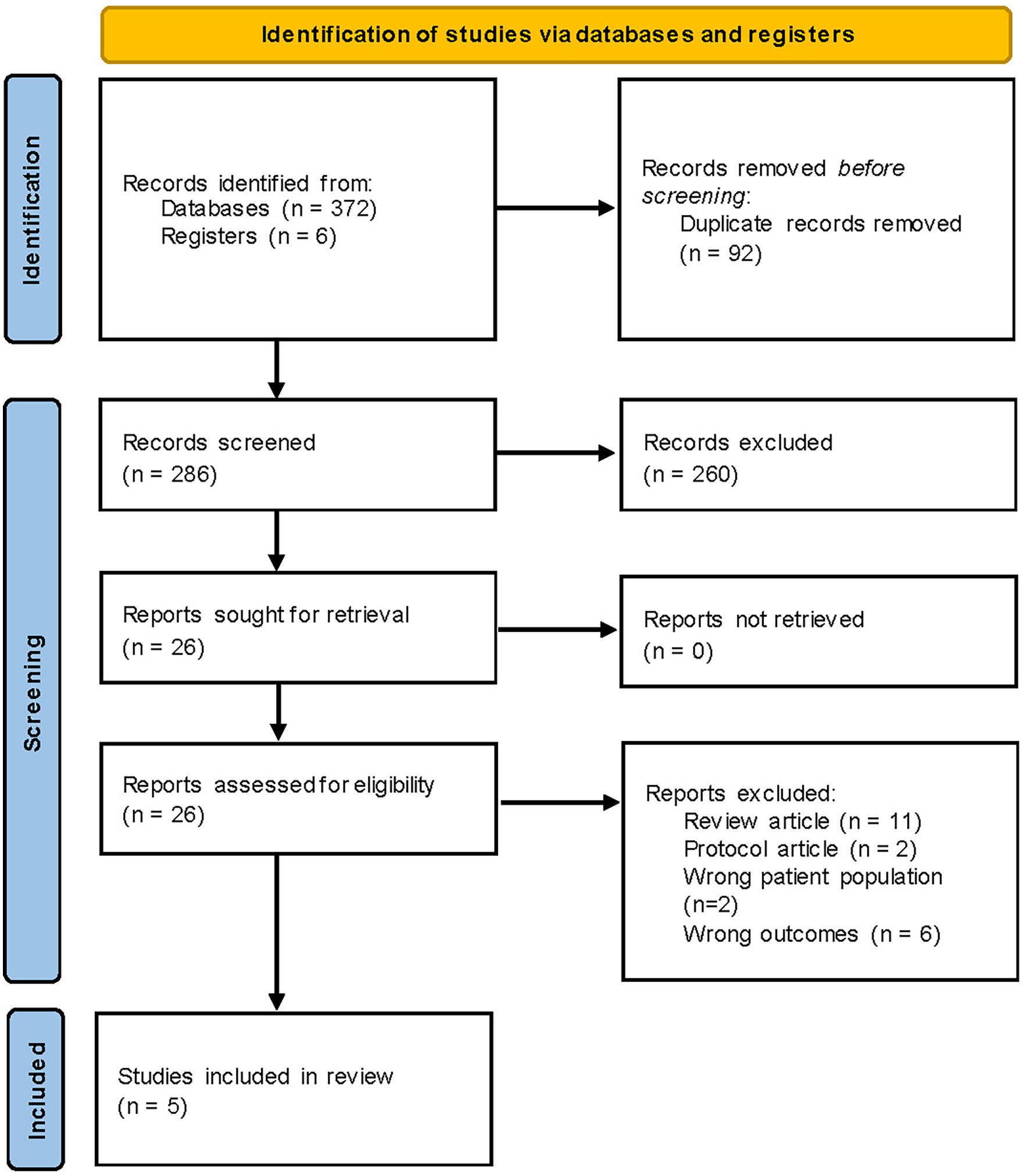
PRISMA diagram.
Summary of studies.
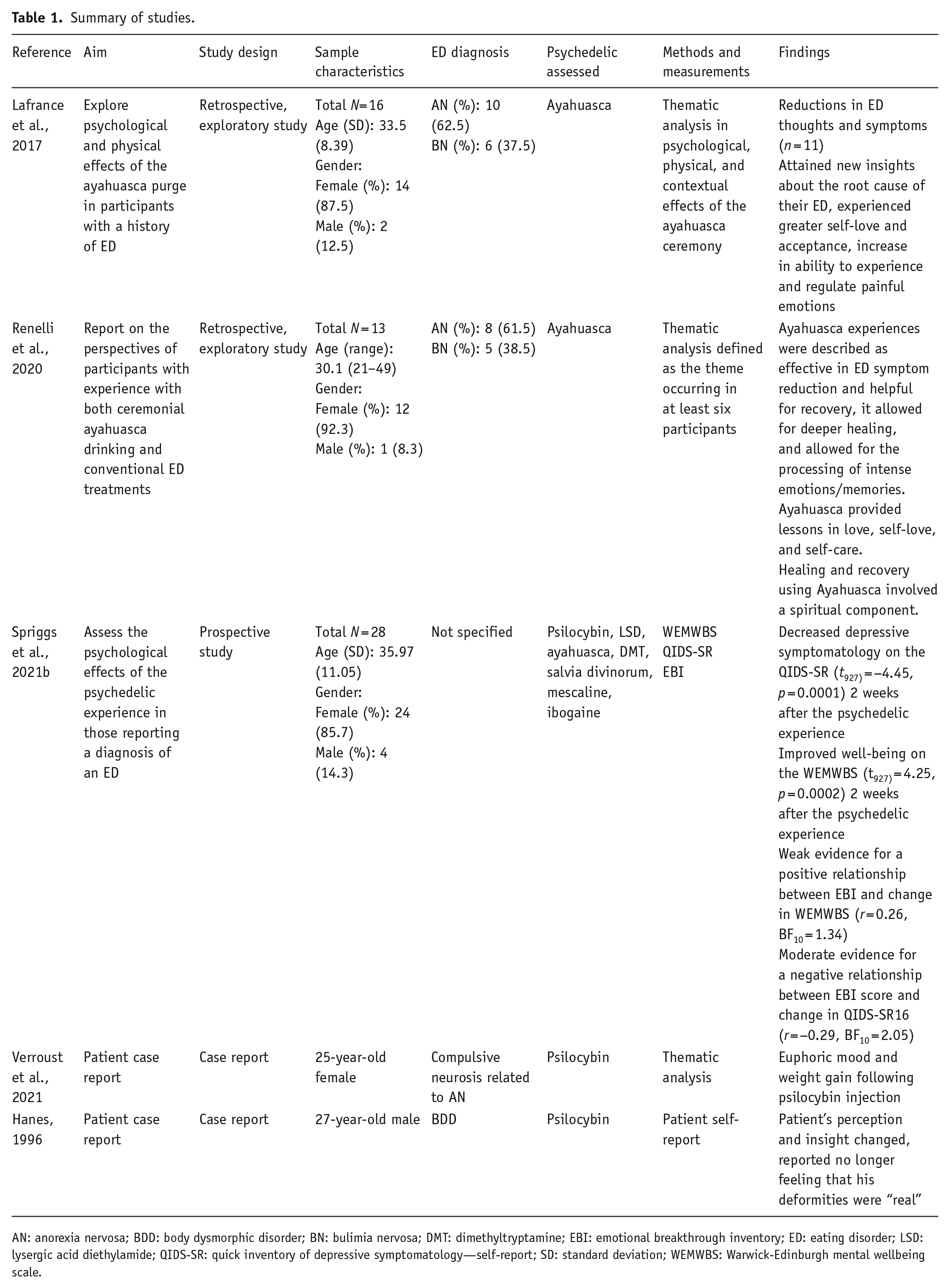
AN: anorexia nervosa; BDD: body dysmorphic disorder; BN: bulimia nervosa; DMT: dimethyltryptamine; EBI: emotional breakthrough inventory; ED: eating disorder; LSD: lysergic acid diethylamide; QIDS-SR: quick inventory of depressive symptomatology—self-report; SD: standard deviation; WEMWBS: Warwick-Edinburgh mental wellbeing scale.
Of the five articles, two conducted a thematic qualitative analysis (Lafrance et al., 2017; Renelli et al., 2020); two articles were case reports (Hanes, 1996; Verroust et al., 2021); and one study was a prospective survey (Spriggs et al., 2021b). Four of the reviewed articles described a reduction in ED or BDD symptoms following ingestion of ayahuasca or psilocybin (Hanes, 1996; Lafrance et al., 2017; Renelli et al., 2020; Verroust et al., 2021). The fifth study did not directly assess post-ingestion ED symptoms but noted that well-being improved while depressive symptoms decreased (Spriggs et al., 2021b); similar results were seen in the study conducted by Lafrance et al., (2017). Two exploratory studies conducted by the same group investigated ayahuasca as a treatment for EDs (Lafrance et al., 2017; Renelli et al., 2020). Both studies were retrospective qualitative interviews of individuals who were diagnosed with an ED and had participated in at least one ayahuasca ceremony. It is important to note that the ceremonies were not necessarily focused on ED healing and reasons for participation were not assessed; thus, individuals may have partaken in the ceremony for reasons other than ED treatment. The sample characteristics of both studies were predominantly female, with an AN or bulimia nervosa (BN) diagnosis. Thematic analyses conducted by the authors outlined how participants felt they were better able to identify root causes of their ED and experienced a shift in self-perception that was centered around more self-love and self-forgiveness (Lafrance et al., 2017; Renelli et al., 2020). In the case report by Hanes (1996), the individual with BDD reported having three experiences under the acute influence of psilocybin in which his appearance in the mirror no longer looked deformed to him, suggesting perceptual changes. In addition, following these experiences, he was no longer convinced that his perceived bodily deformations were “real” and decided to pursue treatment with fluoxetine. The second case report is an English translation dated 1959, from a French presentation given at the Societe Medico-psychologique describing a patient who was injected twice with psilocybin for treatment of a “compulsive neurosis” (Verroust et al., 2021). It is unclear whether the individual had a binge ED or AN, and there is little information to determine the extent of the effects psilocybin had on the individual’s symptoms. The authors state that the patient was euphoric and increased weight rapidly following the second dose of psilocybin (Verroust et al., 2021); however, these results were not sustained at the 1-year follow-up (Verroust et al., 2021).
Discussion
This study investigated the published literature on the impact of classic psychedelics on clinical symptoms in participants with BDD and those with EDs. Few available studies were found and included in this review; however, the early and preliminary data appear to be promising. It should be noted that two articles were found incidentally outside of the conducted literature search and were not located in the reference lists of the full texts reviewed. 1 No other articles were found. The data for both articles came from archives of patients that applied for compensation for psychological and physical harm related to LSD treatment in the 1960s (Larsen, 2017, 2016). Two individuals diagnosed with AN demonstrated acute improvement following LSD administration, however the authors note that the case material upon which these data are based is incomplete (Larsen, 2017). In the follow-up article, it is stated that one patient, a 17-year-old female, underwent LSD treatment for AN (Larsen, 2016). Her symptoms improved over the years, although it is unclear whether this was due to the LSD or other factors, and she suffered from mood swings and permanent flashbacks as a result of the treatment (Larsen, 2016).
Neurobiological mechanisms of action of psychedelics
As clinical trials proceed in various psychiatric disorders, theoretical mechanisms of action of psychedelic drugs are emerging. A growing body of research in humans and animal models suggests two potential ways that psychedelics may help individuals with BDD and EDs. The first theory points toward alleviating symptoms related to dysfunctional serotonergic signaling and cognitive inflexibility. The second theory focuses on how psychedelics can induce an ideal condition for psychotherapeutic processes.
Serotonergic pathways have been implicated in the pathogenesis of several psychiatric disorders including major depressive disorder (MDD), OCD, BDD, and AN (Foldi et al., 2020). Brain imaging studies note patterns of 5-HT alterations in patients with EDs. Using single photon emission computed tomography, researchers found that compared with healthy volunteers, individuals with AN displayed significantly lower 5-HT2A binding in parts of the frontal, parietal, and occipital cortices (Audenaert et al., 2003). This reduced binding also seems to persist beyond body weight recovery. Similar studies using positron emission tomography demonstrated a significant reduction in various areas of the brain in individuals with recovered BN and/or AN (Bailer et al., 2004; Frank et al., 2002; Kaye et al., 2001). Compared to healthy controls, individuals with recovered and current AN and BN have demonstrated increased 5-HT1A binding in the frontal cortex, temporal/amygdala, cingulate cortex, and parietal cortex (Bailer et al., 2004, 2005; Galusca et al., 2008; Tiihonen et al., 2004). These disturbances in 5-HT signaling are manifested behaviorally in part through a phenotype known as cognitive inflexibility.
Broadly, cognitive flexibility is the ability to move between multiple tasks, operations, or mental sets (Miyake et al., 2000). Impairments in cognitive flexibility can play a role in the persistence of unhealthy and rigid cognitive and behavioral patterns. In AN, this can contribute to the development and maintenance of symptoms including pathological fixation of weight control, calorie-counting, and extensive exercise routines (Rößner et al., 2017). Research in MDD patients has shown the potential of serotonin agonists like psilocybin to enhance cognitive and neural flexibility (Davis et al., 2021; Doss et al., 2021). Doss et al. (2021) reported that after a week of psilocybin-assisted therapy, cognitive flexibility improved and functional connectivity between the posterior and anterior cingulate cortex (ACC) increased. More studies are needed to translate these results to EDs; however, the reported reductions in ED thoughts and symptoms (Lafrance et al., 2017; Renelli et al., 2020) and changes in self-image (Hanes, 1996) associated with psychedelics may be explained by enhanced cognitive flexibility.
EDs, BDD, and OCD share several phenomenological and biological similarities, including cognitive inflexibility and possible serotonergic involvement. In fact, clinical similarities between BDD and OCD including obsessive and recurrent thoughts, repetitive/compulsive behaviors, illness course, and symptom severity prompted the re-classification of BDD from a somatoform disorder to an OCRD in DSM-5 (Malcolm et al., 2018). Several case reports (Leonard and Rapoport, 1987; Lugo-Radillo A Md and Cortes-Lopez, 2021; Moreno and Delgado, 1997; Wilcox, 2014) and one clinical trial (Moreno and Delgado, 1997; Moreno et al., 2006) have noted reductions in intrusive thoughts and compulsions following consumption of psychedelics. These reports in the literature may help to better understand potential similar therapeutic targets of psychedelics in EDs and BDD. To date, we are aware of only one study that has examined the effects of psilocybin in OCD in a controlled manner (Moreno et al., 2006). Using low to high doses of psilocybin, these researchers demonstrated that psilocybin was associated with an acute reduction in OCD symptoms, but the long-term effects were not documented and there were no significant dose or time-by-dose interactions. It remains to be explored how far these data can be extrapolated to the potential for psychedelics to reduce intrusive thoughts and repetitive behaviors in BDD and EDs.
While the role of serotonin in the pathogenesis of BDD is uncertain, both AN and OCD have been associated with a polymorphism in the 5-HT2A promotor (Ricca et al., 2002; Sorbi et al., 1998; Walitza et al., 2002). Whether cognitive inflexibility is directly moderated by this gene is unknown; however, given both conditions share these phenomenological and genetic features may suggest a possible association. Moreover, the potential for serotonergic hallucinogens to increase cognitive flexibility aligns with the hypothesis that psychedelics may help interrupt rigid thought patterns and behaviors seen in OCD and AN.
Preclinical research also sheds some light on psilocybin’s therapeutic potential in EDs. Two studies have reported that psilocybin reduced marble-burying behavior—an animal model of OCD—in mice (Matsushima et al., 2009; Odland et al., 2021). However, the effect was not sustained, and linkages from animals to humans in term of reducing repetitive and compulsive behaviors characteristic of EDs and BDD cannot necessarily be drawn.
It has been posited that psychedelics create a “desirable” brain state that can leave the individual more amenable to psychotherapy. Because individuals with EDs and BDD are often mentally bound up with their symptoms and are afraid of challenging their associated behaviors (Thompson-Brenner, 2016), interventions that aid in deconstructing these mindsets are critical. In this regard, a system of brain regions known collectively as the default mode network (DMN) is of particular interest (Steward et al., 2018). The DMN includes the ventromedial prefrontal cortex, perigenual ACC, and the posterior cingulate cortex (Foldi et al., 2020). It is deactivated during most tasks, and its activity is found to be associated with mental processes including considerations of past and future (Scharner and Stengel, 2021), self-referential cognition (Sheline et al., 2009), and moral judgments (Foldi et al., 2020; Spreng et al., 2009). Altered activity and connectivity of the DMN are linked to several mental disorders including MDD (Zhang et al., 2016) and OCD (Koch et al., 2018; Stern et al., 2012). A review of neural network alterations in EDs implicated DMN abnormalities but whether activity is increased or decreased remains inconclusive (Steward et al., 2018). One study examining the functional connectivity of the dorsal ACC (dACC) in a sample of AN and BN patients found stronger synchronous activity between the dACC and retrosplenial cortex and heightened synchronous activity between the dACC and orbitofrontal cortex, respectively. Both groups also exhibited greater synchronous activity between the dACC and precuneus, which correlated with symptom severity (Lee et al., 2014). One study in BDD found greater activation of the DMN than in controls during task-negative periods (Feusner et al., 2011). Psychedelics are hypothesized to downregulate the DMN (Carhart-Harris et al., 2012; Palhano-Fontes et al., 2015), leaving the brain to form new neural connections, be more globally integrated (Daws et al., 2022) and find alternate ways to relay information. In the right set and setting (e.g., coupled with psychotherapy), this may aid individuals with EDs or BDD in “resetting” rigid thought patterns that perpetuate their symptoms.
Another proposed neurobiological mechanism of psychedelics that could impact body image in those with BDD and EDs involves the role of 5-HT agonism on the visual system. Psilocybin, LSD, and ayahuasca have agonistic effects on 5-HT2A receptors, which are highly expressed in the visual cortex (as well as 5-HT1A receptors, which are also expressed in the visual cortex) (Dyck and Cynader, 1993; Gerstl et al., 2008; Moreau et al., 2010; Watakabe et al., 2009). 5-HT2A agonism results in hyperexcitability of the visual cortex, which can result in visual experiences when there are no external visual stimuli (visual hallucinations) or alter the perception of external visual stimuli (illusions) (Kometer et al., 2013). Although not uniformly reported across the studies of psychedelics in EDs reviewed here, in the case report in BDD (Hanes, 1996), it is possible that the individual may have experienced changes in visual perception while looking in the mirror under the acute influence of psilocybin as he noted that his appearance “changed” and no longer looked deformed following use. However, this explanation not directly stated by the author and other possible mechanisms for psychological change are possible, including enduring changes in self-image and self-acceptance. Also, the patient was later treated with a selective serotonin reuptake inhibitor, which presumably conferred symptomatic response. Overall, the effects of psychedelics on perceptual distortions of appearance in those with BDD and in some with EDs require further investigation.
A further mechanism of psychedelics in those with EDs may involve changes in predictive coding of self-body experiences (Ho et al., 2020). Under this model, one’s experience of the bodily self involves an integration and contrast of top-down attentional processes (“reflective self”) and bottom-up low-level perceptual inputs (“pre-reflective self”). In those with EDs with body image disturbances, top-down prior information, such as beliefs one may hold about their appearance, are over-prioritized and rigid, which may combine with deficits in bottom-up perceptual multisensory integration (Riva and Gaudio, 2018; Riva, 2012) necessary for real-time egocentric updating. The possible effect of psychedelics could be reducing the focus on top-down prior beliefs via enhancing cognitive flexibility. This would allow a more balance contribution from bottom-up sensory information during predictive error contributions, resulting in an updated and more reality-based experience of body size/shape and a subsequent recalibration of appearance beliefs.
Psychological mechanisms of action of psychedelics
As stated, BDD and EDs are characterized by rigid thought patterns leading to deeply ingrained schemas that are maladaptive and resistant to change (Keegan et al., 2021) and cognitive inflexibility is also common in patients diagnosed with OCD which has shown improvement following psychedelic use. Classic psychedelics may be able to disrupt rigid thought patterns biochemically, through 5-HT binding, and psychologically through spiritual and mystical experiences and/or the confrontation of challenging emotions (Murphy-Beiner and Soar, 2020; Roseman et al., 2019; Zeifman et al., 2020). It is believed that these experiences are what lead to personal insight and enhanced cognitive flexibility. More specifically, it has been suggested that more frequent psychedelic use results in higher emotion regulation which predicts less disordered eating (Lafrance et al., 2021). Aligned with this concept are descriptions from ayahuasca users stating that they were unable to avoid difficult experiences once the psychedelic was taken (Lafrance et al., 2017; Renelli et al., 2020). After the acute effects of the psychedelic wore off, participants reported feeling better able to experience and regulate emotions, particularly those associated with painful experiences related to their body image (Lafrance et al., 2017; Renelli et al., 2020). These results are similar to psychedelic studies in depression (Watts et al., 2017) and life-threatening cancer (Griffiths et al., 2016) and are also described in the AN case report translated by Verroust et al. (2021), reviewed above. It is possible that psychedelics may work by relaxing limiting beliefs and, in parallel, promote emotional release and insight (Nutt et al., 2020). Similar to depressive populations (Stuhrmann et al., 2011), the identification and processing of emotional faces has been shown to be impaired in patients with BDD and with AN (Buhlmann et al., 2004, 2006; Feusner et al., 2010; Pollatos et al., 2008; Rangaprakash et al., 2018; Stuhrmann et al., 2011). Interestingly, the processing of emotional facial expressions has demonstrated improvement after taking psilocybin which also showed a correlation to a reduction in depressive symptoms (Stroud et al., 2018). These results offer support for the hypothesis that emotion regulation and interpretation may be a key component in understanding the mechanism by which psychedelics could help to treat EDs and BDD.
Psychedelic experiences may also help patients reform their perception of both their bodies and their illness. Early descriptive texts from psychedelic users include how “. . . many changes can be observed in body ego feeling. The unity of the body ego cannot be maintained; the parts of the body seem dislocated. . . the symmetry of the body is lost and it assumes enormous plasticity. . .” (Savage, 1955). These shifts in body perception appear to be a common theme among users and it is speculated that alterations occur in line with the allocation of attention to certain body parts (Masters and Houston, 2000; Savage, 1955). The experience of changing body image in patients with EDs and BDD may be an important mechanism of action for treatment if it can lead to long-lasting changes toward a more positive self-identity and/or improved insight. In line with this concept are the results from three of the articles reviewed here, where participants reported shifts in body image and respect for their body following ingestion of psychedelics (Hanes, 1996; Lafrance et al., 2017; Renelli et al., 2020) and improvement in insight (Hanes, 1996). In addition, studies in smoking cessation (Noorani et al., 2018) and treatment-resistant depression (Watts et al., 2017) have all described a similar shift toward more positive self-identity following psychedelic use.
Ethical considerations and implications for future research
Given the significant burden on quality of life and disability, there is a clear need to develop novel and effective treatments for EDs and BDD. Classic psychedelics that activate the serotonergic system may serve as a promising option. The literature reviewed in this article is limited, but the results of published studies are encouraging. However, rigorous scientific methodology is required before any concrete conclusions can be made and this appears to be the direction that the field is moving in. Currently, there are five clinical trials registered across North America and Europe (Table 2). All of these trials are investigating the use of psilocybin, most for the treatment of AN, and one for BDD. It will be important to create safe, accessible, and transparent protocols for this research such as the one outlined by Spriggs et al. (2021a). Although considered an entactogen and not a classic psychedelic, MDMA has some similarities in its activation of the serotonergic system and psychological effects such as feelings of empathy and connection (Reiff et al., 2020). A recent study looked at exploratory data on ED psychopathology from a study that used MDMA-assisted therapy (MDMA-AT) for the treatment of post-traumatic stress disorder (PTSD) (Brewerton et al., 2022). Despite excluding participants who were underweight and who had current histories of an ED with active purging, 41 of the 82 participants with PTSD had scores in the clinical or high-risk range on the Eating Attitudes Test 26 (EAT-26) at baseline (Brewerton et al., 2022). In study completers, there was a significant reduction in total EAT-26 scores in the MDMA-AT group compared to placebo (F(2,79) = 4.68, p = 0.0335; Hedge’s g = 0.33) after controlling for scores at baseline (Brewerton et al., 2022). However, Reliable Change Index (RCI) values for placebo and MDMA groups for the total sample was not indicative of reliable change (RCI = −0.15 and −0.84, respectively) or determined to be to be clinically meaningful (Brewerton et al., 2022). Overall, this study demonstrates that there is ED and BDD treatment potential in serotonergic drugs such as MDMA and classic psychedelics. Moreover, it would be beneficial to assess the impact, if any, of psychedelic compounds on sets of symptoms in overlapping disorders. For example, investigating the impact of weight and shape concerns in patients with BDD, which are common, would help to accelerate the field and provide a more comprehensive picture of how psychedelics impact disordered body image in patients. It is also not uncommon for patients to be diagnosed with more than one ED, in addition to other comorbidities such as depression, anxiety, and substance use as was seen in the recent MDMA study involving participants with ED-PTSD (Brewerton et al., 2022). Thus, assessing the clinical effects of psychedelics across multiple domains should be a consideration factor in protocol development.
Registered clinical trials.
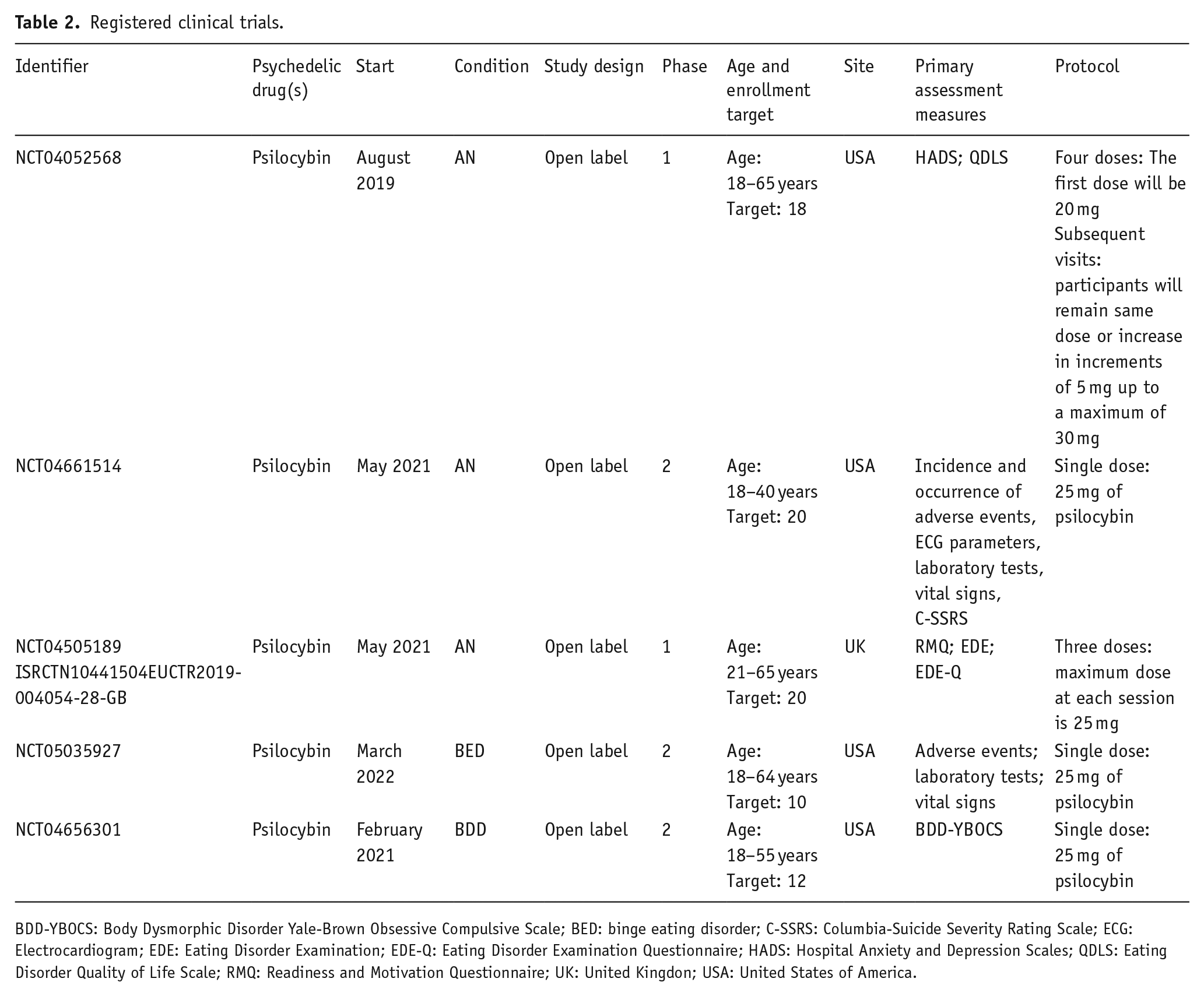
BDD-YBOCS: Body Dysmorphic Disorder Yale-Brown Obsessive Compulsive Scale; BED: binge eating disorder; C-SSRS: Columbia-Suicide Severity Rating Scale; ECG: Electrocardiogram; EDE: Eating Disorder Examination; EDE-Q: Eating Disorder Examination Questionnaire; HADS: Hospital Anxiety and Depression Scales; QDLS: Eating Disorder Quality of Life Scale; RMQ: Readiness and Motivation Questionnaire; UK: United Kingdon; USA: United States of America.
Importantly, evidence from a community survey demonstrates that ED patients are generally in support of psychedelic research, but have concerns regarding possible side effects, fear of the drug effects, and stigma (Harding et al., 2021). In the development of research protocols, scientists should involve feedback from those with lived experience to ensure that these concerns are adequately addressed (Spriggs et al., 2021a). Factors such as set and setting have been deemed to be essential in psychedelic-assisted psychotherapy since the early 1960s. Participants in the ayahuasca study conducted by Lafrance et al. (2017) emphasized the importance of feeling safe, and appreciated when medical professionals were present. Although not specific to EDs and BDD, a crucial process in psychedelic treatment may be the confrontation of challenging emotions and experiences (Lafrance et al., 2017). Thorough patient preparation about encountering and working through difficult experiences should be a priority.
Finally, published clinical trials of psilocybin and other serotonergic psychedelics have reported that adverse events are transient, tolerable, and resolved when the acute effects have worn off (Galvão-Coelho et al., 2021). Common adverse effects include increased blood pressure, nausea, headaches, and in some cases (particularly with ayahuasca), vomiting (Johnson et al., 2008). As previously mentioned, the two articles reviewed by Larsen (2016); Larsen (2017) outlined that one of the patients experienced long-lasting adverse effects including flashbacks and mood swings (Larsen, 2016, 2017). Several other patients involved in these trials developed similar long-term side effects; however, the data on the 151 individuals came from records of participants who had reported physical or psychological harms as a result of treatment and therefore, are inherently biased (Larsen, 2016). It should be noted that early research studies frequently reported long-term psychological consequences including flashbacks and the development of hallucinogen-persisting perception disorder in patients (Horowitz, 1969; van Amsterdam et al., 2011). However, strict protocols regarding dosage, therapy, and inclusion criteria including age and diagnosis were not followed as is demonstrated by the 17-year-old participant that received LSD for treatment of AN (Larsen, 2016). Current data indicate that there is a risk of developing flashbacks (Müller et al., 2022) but no contemporary trials have reported any such cases. In addition, although LSD is one of the most potent psychedelics currently administered, it is believed to have a high safety ratio (Gable, 2004) and is not associated with major health impairments (Johansen and Krebs, 2015; Krebs and Johansen, 2013). Continued research should focus on how psychedelic-assisted therapy can be made as safe as possible and more importantly, transparency and thorough reporting of results and adverse events will help to provide a more comprehensive picture of safety.
Limitations and future directions
There are a number of limitations to the present review. First, our search was conducted in English and thus, articles published in different languages may have been missed. Second, there is very limited data to draw any concrete conclusions about the use of psychedelics to treat body image and ED symptoms. Included articles had small sample sizes and there were no randomized-controlled trials identified. Future studies should develop research protocols that can rigorously test the use of psychedelics to treat EDs and BDD, with larger sample sizes drawing samples that are representative of the treatment population. Such data will be important in determining the safety and efficacy of these drugs.
Conclusion
In this systematic review, we evaluated published evidence investigating the therapeutic use of psychedelics for patients diagnosed with BDD and EDs. Our search yielded only five eligible articles addressing this issue, with all findings showing psychedelic drugs to have had a positive effect on core symptoms. In addition, evidence from psychedelic trials in other psychiatric disorders, such as MDD and OCD, which have similarities in pathogenesis of the serotonergic system and cognitive rigidity, can be extrapolated to provide further support for exploring psychedelic-assisted therapy in BDD and EDs. Taken together, this preliminary evidence supports the concept that psychedelics may be an effective treatment option for these disorders. Given the number of currently registered clinical trials of psychedelics in patients with EDs, and one in those with BDD, emerging evidence will provide important data on their safety and efficacy for these debilitating mental disorders.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MIH receives research support from the Brain and Behavior Research Foundation, Canadian Institutes of Health Research, CAMH Foundation, the PSI Foundation, and the University of Toronto. He has provided consultancy to Mindset Pharma (for whom he holds stock options), PsychEd Therapeutics, and Wake Network. He has conducted contracted research for Compass Pathways Limited. Potential conflicts of interest for DC (past 36 months: November 2022): DC has received grant monies for research from Servier, Boehringer Ingelheim; Travel Support and Honoraria for Talks and Consultancy from Servier, Seqirus, Lundbeck. He is a founder of the Optimal Health Program (OHP), and holds 50% of the IP for OHP; and is part owner (5%) of Clarity Healthcare. DC is an Advisory Board Chair of a not-for-profit institute specializing in psychedelic medicines research. He does not knowingly have stocks or shares in any pharmaceutical company.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.