
Abstract
Background:
Several studies have reported that a switch to the dopamine partial agonist (DPA) aripiprazole (ARP), especially when the switch is abrupt, is likely to fail and sometimes worsen psychosis in schizophrenia patients already under high-dose antipsychotic treatment. Such a switching failure is speculated to be related to be the dopamine supersensitivity state. The risks of switching to the DPA brexpiprazole (BREX) have not been reported.
Aims and Methods:
We retrospectively analyzed the cases of 106 patients with schizophrenia to identify any factors related to the success or failure of switching to BREX.
Results:
The comparison between the patients with dopamine supersensitivity psychosis (n = 44) and those without (n = 62) revealed no significant difference in the switching failure judged at the sixth week. A comparison of the patients with successful switching (n = 80) and those who failed (n = 26) revealed that patients with treatment-resistant schizophrenia (TRS) were significantly more likely to fail. A logistic regression analysis also revealed that patients with past failure of switching to ARP are likely to succeed in switching to BREX. The 2-year follow-up of the patients with successful switching to BREX suggested that the patients who were treated with BREX, even temporarily, experienced some improvement in their Global Assessment of Functioning and Clinical Global Impression-Severity scores.
Conclusions:
Overall, the results indicate that patients with schizophrenia can be switched more safely to BREX compared to ARP. However, the failure of switching to BREX could be higher in patients with TRS, and thus, starting BREX treatment in refractory patients warrants careful monitoring.
Introduction
Schizophrenia is a chronic mental disorder affecting approximately 1% of the global population (Häfner and an der Heiden, 1997). Individuals with schizophrenia suffer most commonly from hallucinations or delusions, but patients with this disorder can exhibit multiple psychiatric symptoms such as negative symptoms, cognitive impairment, and emotional disturbance. Positive symptoms of schizophrenia are generally controlled by antipsychotics, which remain the main treatment for schizophrenia. However, the majority of successfully treated patients with schizophrenia (i.e., those whose symptoms remit with medication) eventually experience relapse (Bowtell et al., 2018; Haddad et al., 2014). The prevention of relapse in patients with schizophrenia is critical in clinical practice; it is imperative to encourage patients to continue taking their medication over the long term while appropriately controlling the adverse effects of long-term medication use such as extrapyramidal symptoms, metabolic syndrome, and hyperprolactinemia (Taylor et al., 2005).
The development of dopamine supersensitivity (DS) is an additional serious problem in the long-term treatment of schizophrenia. DS is induced by high-dose and/or long-term treatment with one or more antipsychotics (Chouinard and Jones, 1978; Chouinard, 1991), and it has been presumed that an upregulation of dopamine D2 receptors (DRD2) is the underlying mechanism of DS (Iyo et al., 2013). Clinically, DS is observed as an episode of dopamine supersensitivity psychosis (DSP), which is characterized by (i) rebound psychosis, that is, a relapse episode immediately following the tapering-off, discontinuation, or switching of antipsychotic(s), and (ii) tolerance to antipsychotics’ effects, that is, no alteration of a worsening episode despite an increase in the antipsychotic dose (Kirkpatrick et al., 1992; Moncrieff, 2006). Tardive dyskinesia (TD) is considered a symptom of DSP, since the supersensitivity of DRD2 underlies TD (Chouinard and Chouinard, 2008; Iyo et al., 2013).
The results of investigations using animal models suggest that (i) DRD2 pathology alone cannot fully explain the mechanism of schizophrenia’s nonresponse to antipsychotic(s) and (ii) the presynaptic neurons could also be involved in the process of failure of antipsychotic treatment, that is, a lower dopamine state in the synaptic clefts that are derived from the alterations of dopamine release via dopamine autoreceptors and alterations of dopamine reuptake via dopamine transporters (Amato et al., 2018, 2020). Furthermore, the basic research reported that failure of antipsychotic treatment could involve (iii) other multiple mechanisms such as functional loss of post-DRD2 (but not supersensitivity), altered synaptic plasticity on DRD2-medium spiny neurons (MSN) at the terminals of glutamatergic neurons, and reduction of the glutamine transporter GLT-1 on astrocytes, all of which converge to the DRD2-MSN excitability (Kruyer et al., 2021; Tibrewal et al., 2023).
Once DS has developed in a patient with schizophrenia, he/she is more vulnerable to relapse and more likely to require a higher dose of one or more antipsychotic medications to control psychosis, thus meeting the criteria of treatment-resistant schizophrenia (TRS). It was suggested that approximately 50% of patients with TRS have symptoms of DSP (Chouinard and Chouinard, 2008; Suzuki et al., 2015), and it is thus important to address DS and DSP in order to stabilize individuals with schizophrenia over the long term.
Brexpiprazole (BREX) is categorized as a dopamine partial agonist (DPA) along with aripiprazole (ARP) and cariprazine. BREX acts as a partial agonist at DRD2 and 5-HT1A receptors and as an antagonist at 5-HT2A receptors and noradrenaline α1B/2C receptors (Maeda et al., 2014; Otsuka Pharmaceutical Co., Ltd, 2015; Stahl, 2016). In several randomized controlled trials (RCTs), BREX was shown to be more effective than a placebo for patients under an acute psychotic state (Correll et al., 2015; Kane et al., 2015). Other open-label trials showed that the efficacy of BREX was maintained for up to 52 weeks in patients with schizophrenia in a state of clinical stability (Forbes et al., 2018; Ishigooka et al., 2018). BREX was also shown to be effective for preventing relapses in multiple randomized and placebo-controlled trials (Fleischhacker et al., 2017).
Compared to the effects of a DRD2 full antagonist, DPAs such as BREX offer a lower potential for adverse effects related to the blockade of DRD2, such as extrapyramidal symptoms, hyperprolactinemia, and TD (Frankel and Schwartz, 2017). In rat models, DS was observed to be unlikely as a result of treatment with DPAs (including BREX) (Amada et al., 2019; Tadokoro et al., 2012). The findings obtained by Tadokoro et al. (2012) suggested that treatment with ARP could reverse DS states that had developed due to a chronic administration of haloperidol, although this phenomenon was not confirmed in humans. These features could be an advantage in the long-term medication of schizophrenia (Kanahara et al., 2020; Kimura et al., 2021).
However, in patients who have already developed DS, switching to a DPA may induce rebound psychosis and worsen psychotic symptoms, and DPAs may, therefore, be inappropriate for patients with DSP due to the high risk of failure when switching to these agents (Chouinard et al., 2017; Kanahara et al., 2021). Several research groups have reported that in patients treated with high-dose and/or long-term antipsychotics, switching to ARP was significantly more likely to result in failure (Lin et al., 2009; Takaesu et al., 2016; Takase et al., 2015; Takeuchi and Remington, 2013; Takeuchi et al., 2009), but this was not confirmed in a meta-analysis (Takeuchi et al., 2018). Other studies indicated that an abrupt switch to ARP could also be related to switching failure, although significant differences were not observed in some studies with small sample sizes (Casey et al., 2003; Obayashi et al., 2020; Pae et al., 2009).
Overall, these findings suggest that in patients with schizophrenia who have already developed DS due to high-dose antipsychotic treatment, the partial agonism of treatment with ARP, when introduced for a short period in particular, could stimulate the supersensitive DRD2 and worsen psychotic symptoms. This high risk of switching failure to a DPA (such as ARP) is a serious problem, since patients with established DS have an even greater need for treatment by a DPA.
Here, we investigated whether BREX can be introduced to patients with DS more safely than ARP. We hypothesized that BREX allows safer switching even in patients with DS since BREX has slightly lower dopamine endogenous activity compared to that of ARP (Maeda et al., 2014).
To this end, we conducted a retrospective analysis of patients with schizophrenia who underwent a switch from antipsychotics to BREX, and we examined the possible relationship between DSP and the failure of switching to BREX. We investigated the following two points: (i) to what degree the success or failure of switching to BREX was affected by DS, and (ii) whether the symptoms of patients who were successfully switched to BREX and continued BREX thereafter improved.
Subjects and methods
Subjects and study design
The study design was a retrospective analysis of the cases of patients who had been diagnosed as having schizophrenia or schizoaffective disorder according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and were being treated at a ward or outpatient clinic of one of six participating hospitals during the period from January 2018 (when BREX was launched in Japan) to March 2022.
We first screened a prescription database for patients who were prescribed BREX during this period. The research physician at each of the hospitals then selected patients who underwent a switch to BREX from any other antipsychotic(s). We extracted the clinical information described below from each patient’s medical records and examined the factors that affected the switch to BREX.
The exclusion criteria were patients (1) not taking antipsychotic(s) before the introduction of BREX; (2) in their first episode of psychosis; (3) with a history of drug abuse; (4) with a history of serious head trauma; (5) with serious physical disease; (6) with a comorbidity of intelligence disability (DSM-5); (7) pregnant; or (8) with insufficient information in their medical records.
The study protocol was approved by the Ethics Committee of Chiba University Graduate School of Medicine and each of the other research hospitals. Regarding the procedure of informed consent, notification of the study was added to each institution’s homepage or notice board, and patients and their family members were allowed to opt out of the study.
Measurements
Using the patients’ medical records, we extracted age and sex as the demographic indexes, diagnosis, age at disease onset, treatment period, number of hospitalizations, total period of hospitalization, presence/absence of TRS, and presence/absence of DSP as the disease-related factors, the success or failure of switching to BREX, the antipsychotic(s) used before the switch, the Global Assessment of Functioning (GAF) score, the Clinical Global Impression-Severity (CGI-S) score, the success or failure of switching to ARP (if any), and the speed of the switching process as the switching-related factors.
For the patients with a successful switch to BREX, we extracted information about the subsequent periods of continuous BREX treatment following the switch to BREX, the GAF score, the CGI-S score, and the Clinical Global Impression of Change (CGI-C) value at the time of the study analyses. For the patients with a failed switch to BREX, the reason(s) for the failure of switching were identified.
These procedures were conducted by one, two, or three investigators at each facility. Consultations were held with a patient’s attending physician if necessary. Several measures that require a more detailed explanation are described below.
Dopamine supersensitivity psychosis
We evaluated the presence of DSP episode(s) during the patients’ treatment history prior to the BREX introduction. The DSP criteria used in this study were based on the original version by Chouinard (1991), slightly modified by our team as follows: (a) the presence of or a history of TD; (b) withdrawal psychosis, that is, an acute relapse or exacerbation of psychosis after a dose reduction or discontinuation of antipsychotic(s) within 6 weeks for oral medication or 3 months for long-acting intramuscular injection; and (c) the development of tolerance to an antipsychotic effect, that is, an exacerbation of psychosis occurring independently of a dose reduction or discontinuation of antipsychotic therapy that could not be successfully controlled by a 20% increased titration of the drug.
Based on the available information from the medical records, if at least one of the three items listed above was met, the patient was classified as DSP(+); others were classified as DSP(−).
Treatment-resistant schizophrenia
In this study, the diagnosis of TRS was based on the nonresponder criteria of the Clozaril Patient Monitoring Service: that is, patients for whom two different chemical classes of antipsychotic (at least one atypical antipsychotic) with a sufficient dosage (>chlorpromazine-equivalent (CP-eq.) dose of 600 mg/day) for >4 weeks did not sufficiently relieve their positive symptoms and whose mean GAF score did not exceed 41 points were diagnosed as having TRS. We did not consider the patients who met the intolerance criteria as having TRS.
Switching to BREX
We defined patients who continued BREX for 6 weeks after BREX commencement as a switching success, and we defined patients who discontinued BREX for any reason during the 6 weeks following BREX commencement as a switching failure.
Regarding the method of switching to BREX, we defined two patterns: (1) abrupt switching, that is, the discontinuation of all previous antipsychotic(s) when BREX was introduced; and (2) gradual switching, that is, a gradual decrease or continuation and then a tapering-off of the previous antipsychotic(s) after BREX was introduced.
The 2-year follow-up of treatment with BREX
In order to examine the long-term efficacy of BREX for DSP patients, we examined treatment course following the successful switch to BREX up to 2 years and evaluated GAF, CGI-S, and CGI-C at the 2-year time point or the discontinuation of BREX for available patients. Then, these measures were compared between the patients who continued BREX for 2 years and the patients who discontinued BREX at any point. Additionally, these comparisons were conducted for all the patients with successful switching to BREX.
Statistical analysis
We used two approaches to examine our main purpose. In the first approach, we divided the entire patient series into two pairs of subgroups and compared them: the DSP group versus the non-DSP group, and the patients whose switch to BREX was successful versus the patients whose switch failed. As the second approach, we conducted a logistic regression analysis to identify any other factors (other than DSP factors) that are related to the success/failure of switching to BREX.
We used Student’s t-test to analyze differences between pairs of groups, and we conducted an analysis of variance among three groups for continuous variables. We applied the χ2 test or Fisher’s exact test for categorical variables.
In a logistic regression analysis, we used the success or failure of switching to BREX as the objective variable, and we used sex, age, age at onset, number of hospitalizations, presence of TRS, presence of DSP, success or failure of switching to ARP, the antipsychotic dose before switching to BREX, and the speed of BREX switching as the explanatory variables. We examined the remaining indicators as the final step, using the stepwise method (the likelihood reduction method).
In an analysis comparing the treatment effects of BREX between the patents who continued and those who discontinued BREX, we performed a mixed-model analysis with Group (patients who continued BREX and patients who discontinued BREX) and Time (baseline and 24-month) as fixed effects and the GAF and CGI-S as dependent variables.
The statistical threshold level was set at α = 0.05. We used SPSS ver. 22.0 (IBM, Armonk, NY, USA) for the statistical analyses.
Results
A total of 106 people were included in the study. Their average age was 49.7 years; there were 54 males (~51%) and 52 females (~49%); 95 patients had schizophrenia and the other 11 patients had schizoaffective disorder (Table 1).
The DSP and non-DSP groups’ characteristics.
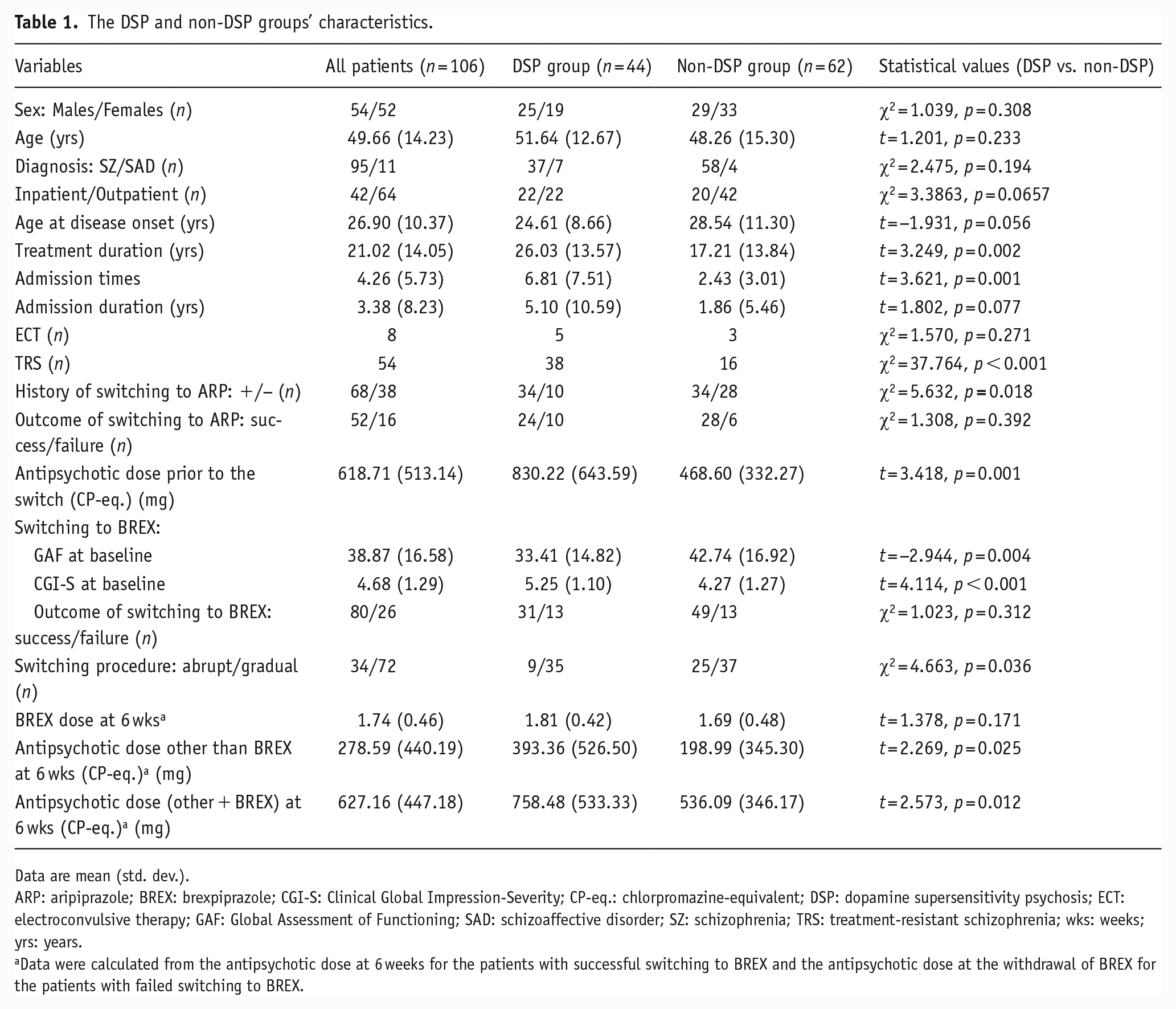
Data are mean (std. dev.).
ARP: aripiprazole; BREX: brexpiprazole; CGI-S: Clinical Global Impression-Severity; CP-eq.: chlorpromazine-equivalent; DSP: dopamine supersensitivity psychosis; ECT: electroconvulsive therapy; GAF: Global Assessment of Functioning; SAD: schizoaffective disorder; SZ: schizophrenia; TRS: treatment-resistant schizophrenia; wks: weeks; yrs: years.
Data were calculated from the antipsychotic dose at 6 weeks for the patients with successful switching to BREX and the antipsychotic dose at the withdrawal of BREX for the patients with failed switching to BREX.
Comparison of the DSP and non-DSP groups
As shown in Table 1, 44 patients (41.5%) were categorized in the DSP group, and 62 (58.5%) were categorized in the non-DSP group. There was no significant difference between the DSP and non-DSP groups in terms of age or sex. The DSP group had a significantly greater ratio of inpatients/outpatients, significantly longer treatment durations, and a significantly higher number of hospitalizations. The age at disease onset tended to be earlier and the duration of hospitalization tended to be longer, in the DSP group relative to the non-DSP group. The ratio of patients with TRS was significantly higher in the DSP group than in the non-DSP group. Although a history of switching to ARP was significantly more common in the DSP group, there was no significant difference in the switching failure rate between the DSP and non-DSP groups. Compared to the non-DSP group, the DSP patients were taking significantly higher doses of antipsychotics and had lower GAF scores and higher CGI-S scores just before switching to BREX.
Concerning the outcomes of the switch to BREX, there was no significant difference in the rate of switching failure between the DSP (13 of 44 patients; 29.5%) and non-DSP groups (13 of 62 patients; 21.0%) (Table 1). The most frequent reason for switching failure in the DSP group was self-discontinuation of BREX (n = 5), and the second most frequent reason was worsening psychosis (4 of the 44 patients; 9.1%). The most frequent reason for switching failure in the non-DSP group was worsening psychosis (10 of the 62 patients; 16.1%). The ratio of patients who underwent an abrupt switch was greater in the non-DSP group.
At the sixth week following BREX commencement, although the BREX dose did not differ significantly between the two groups, the dosage of other agents and the total dose of all antipsychotics including BREX were significantly higher in the DSP group than in the non-DSP group (Table 1). Regarding the switching to BREX monotherapy, 14 of the 44 patients in the DSP group were switched to monotherapy with BREX (successful switching, n = 12; switching failure, n = 2), and the other 30 patients were partially switched to BREX. Thirty-five of the 62 patients in the non-DSP group were switched to BREX monotherapy (successful switching, n = 30; switching failure, n = 5), and the other 27 patients were partially switched to BREX.
Nineteen patients did not undergo a dose reduction of prior antipsychotic(s) at all following the start of BREX administration up to the sixth week, implying that their adjustments were a simple “add-on” of BREX and not a switch to BREX: six patients in the DSP group (switching failure, n = 2) and 13 patients in the non-DSP group (switching failure, n = 3). The cases of these 19 patients were removed, and the above analysis was performed for the remaining patients (DSP group: n = 38, non-DSP group: n = 49). The results of the analysis were completely the same with and without the inclusion of the “add-on” patients.
Comparison of the patients whose switch to BREX was successful and the patients whose switch failed
We next divided the entire patient series into two groups based on the success or failure of switching to BREX in order to explore factors (other than DSP) affecting the success or failure of the switch. Eighty patients (75.5%) were judged as having a successful switch to BREX, and the other 26 patients (24.5%) were judged as having a switching failure (Table 2).
Comparison of the patients with success and the patients with failure of switching to BREX.
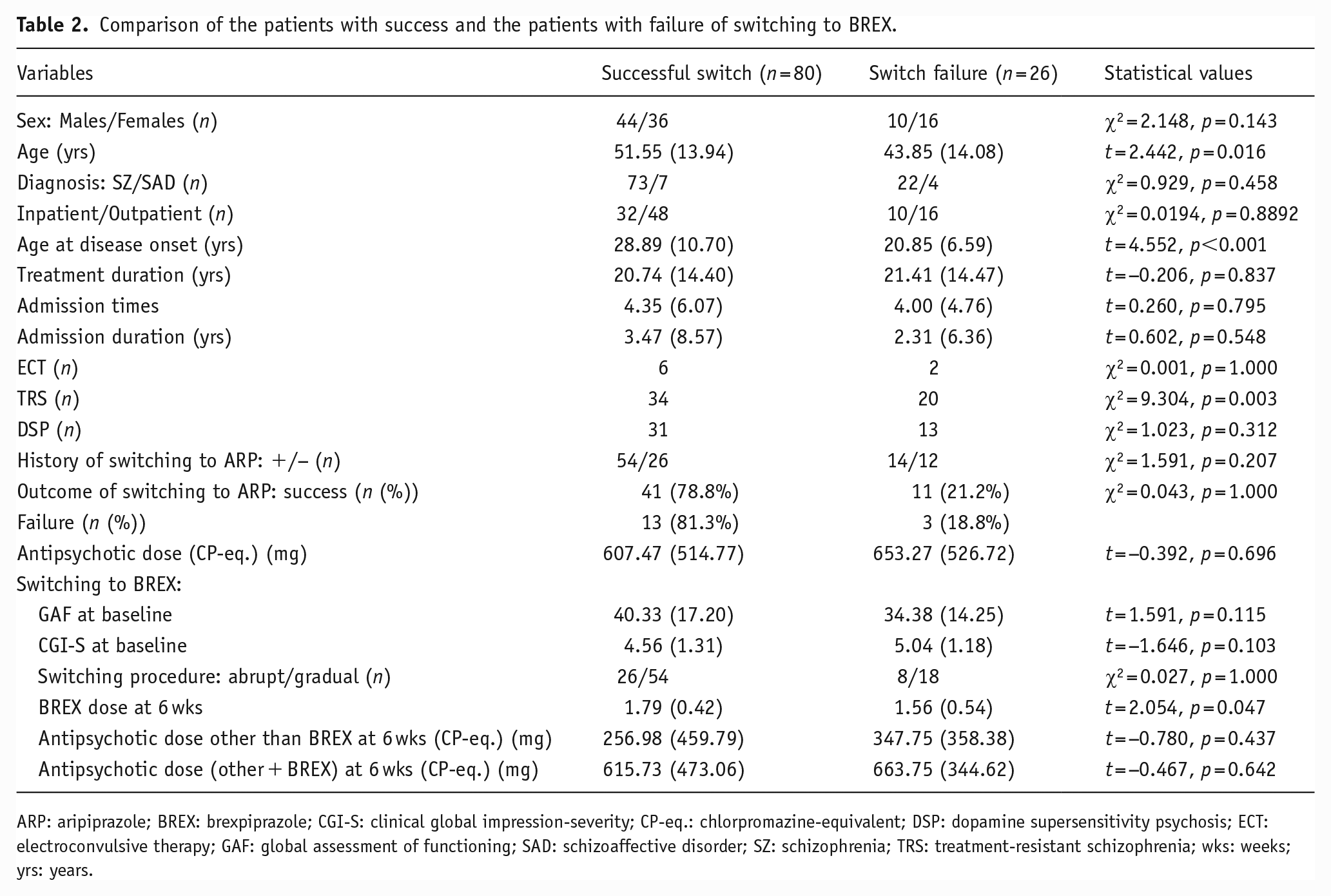
ARP: aripiprazole; BREX: brexpiprazole; CGI-S: clinical global impression-severity; CP-eq.: chlorpromazine-equivalent; DSP: dopamine supersensitivity psychosis; ECT: electroconvulsive therapy; GAF: global assessment of functioning; SAD: schizoaffective disorder; SZ: schizophrenia; TRS: treatment-resistant schizophrenia; wks: weeks; yrs: years.
There was no significant difference between the switching success and switching failure groups in terms of sex, but the patients’ age and the age at disease onset were significantly lower in the patients with switching failure compared to those with success. There were no significant between-group differences in the ratio of inpatients/outpatients, treatment duration, or the number or duration of hospitalizations. The ratio of patients with TRS was significantly higher in the patients with switching failure (20 of the 26 patients; 76.9%) versus the patients with success (34 of the 80 patients; 42.5%).
The history of switching to ARP and the success/failure of the switching to ARP did not differ significantly between the success and failure groups (Table 2). The ratio of DSP, the antipsychotics dose, the GAF and CGI-S scores just before the switch to BREX, and the BREX switching procedure also did not differ significantly between the patients with success and those with failure switching to BREX.
At the sixth week following BREX commencement, the BREX dose of the success group was significantly higher than that of the failure group, although there were no significant differences in the dosage of other antipsychotic agents or the total antipsychotic dose including BREX between the two groups. Regarding the switching to BREX monotherapy, among the 80 patients with successful switching, 42 patients were switched to monotherapy with BREX, whereas among the 26 patients who failed the switch, seven patients were switched to BREX monotherapy at the switching failure.
The additional analysis with the removal of the 19 patients with a simple BREX add-on revealed almost the same results. However, the CGI-S score prior to the initiation of BREX did differ, with higher scores in the patients with switching failure when add-on BREX patients were omitted.
The logistic regression analysis of the success/failure factors of the switching to BREX
We applied a logistic regression analysis to the success or failure of switching to BREX for the 87 patients whose treatment was switched to BREX (the 19 patients with a simple add-on of BREX were not included in this analysis).
Five factors (sex, age, age at disease onset, TRS, and a history of failure of switching to ARP) remained at the final step of the analysis (Table 3). The two factors of TRS and a history of failure of switching to ARP were significant: interestingly, the past success of switching to ARP was more closely related to the failure of switching to BREX, along with the presence of TRS (Table 3 and Figure 1).
Logistic regression analysis predicting success/failure of switching to BREX.
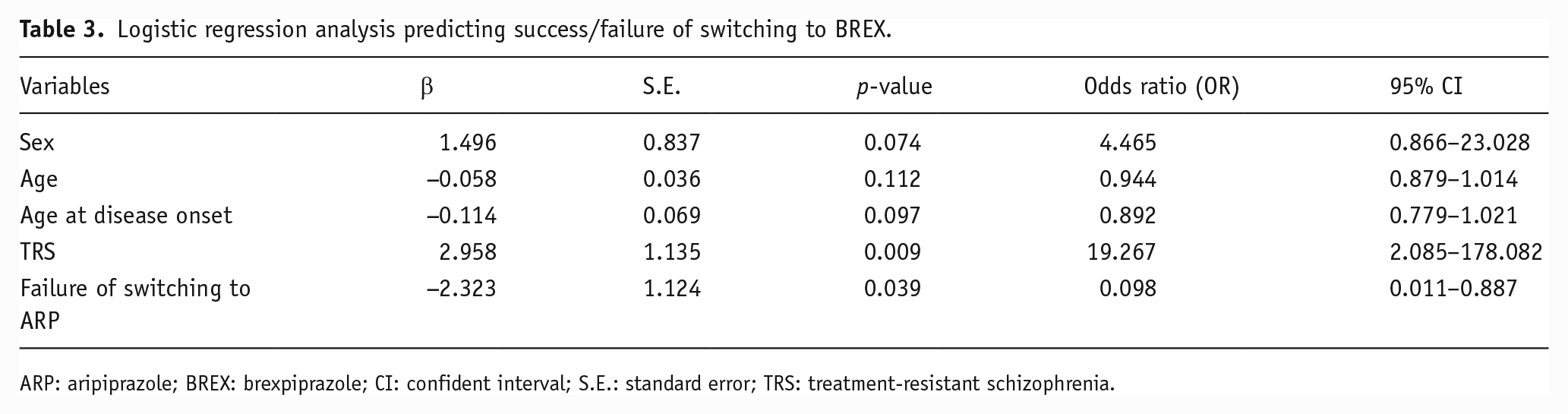
ARP: aripiprazole; BREX: brexpiprazole; CI: confident interval; S.E.: standard error; TRS: treatment-resistant schizophrenia.
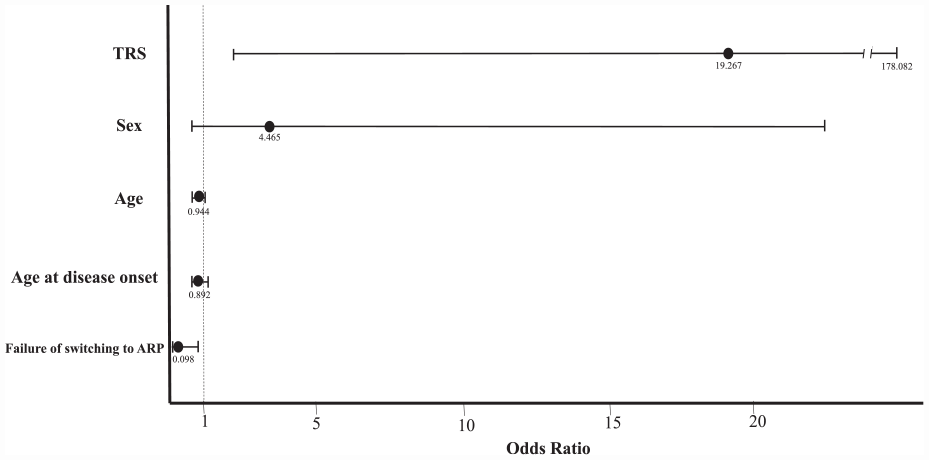
Odds ratio of failure of switching to BREX from the logistic regression analysis.
The additional logistic regression analysis concerning the success/failure of switching to BREX for the 38 patients in the DSP group identified two significant factors: age at disease onset (β = −0.453, p = 0.044, odds ratio (OR) = 0.636, 95% CI: 0.409–0.988) and history of failure of switching to ARP (β = −7.402, p = 0.016, OR 0.001, 95% CI: 0.000–0.258).
Effects of BREX treatment for patients with DSP
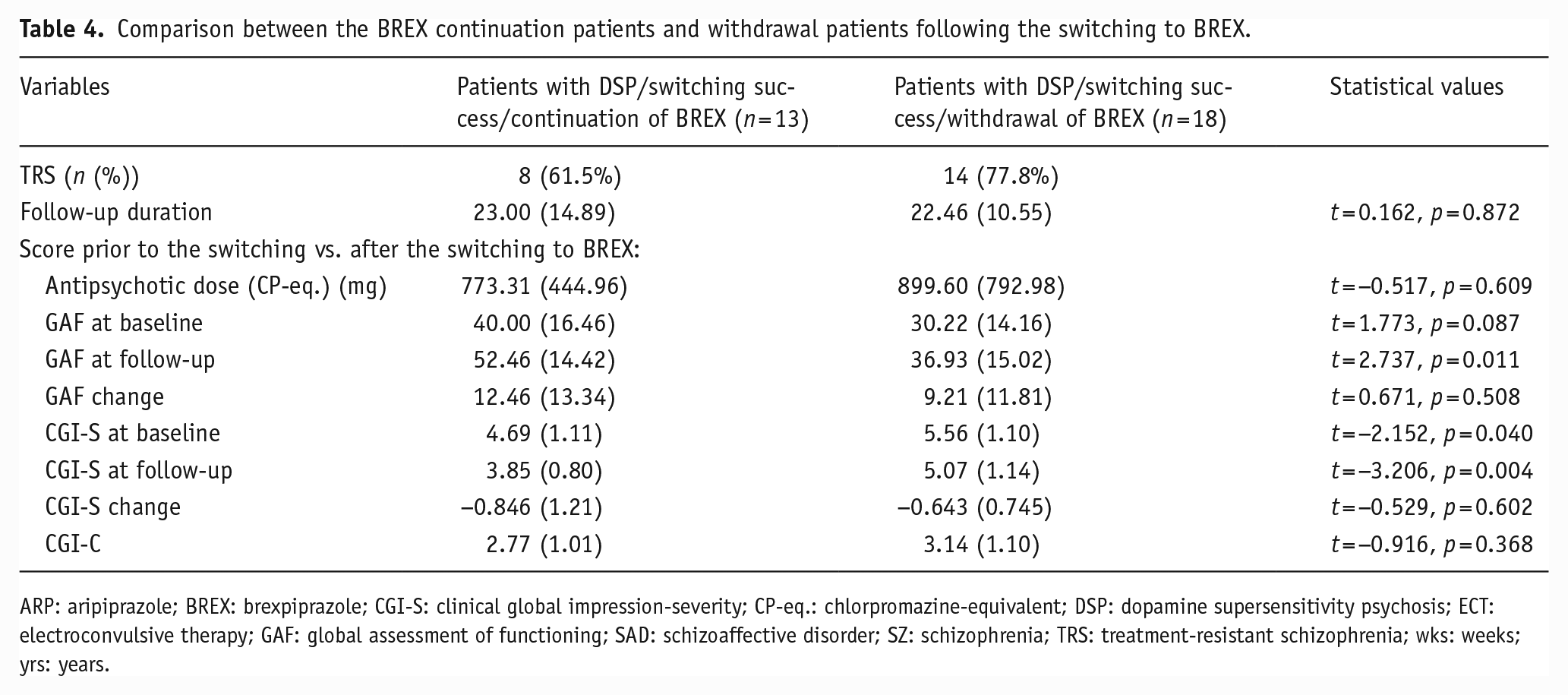
We examined the prognoses of the patients with DSP after the switch to BREX by comparing the patients who continued BREX treatment for approximately 24 months (n = 13) with those for whom BREX was discontinued at any point during the 24 months after the switch to BREX (n = 18).
The results revealed that at the baseline (i.e., prior to the BREX switch), the patients who later continued BREX exhibited significantly lower CGI-S scores and a tendency of higher GAF scores compared to the patients with BREX discontinuation (Table 4).
Comparison between the BREX continuation patients and withdrawal patients following the switching to BREX.
ARP: aripiprazole; BREX: brexpiprazole; CGI-S: clinical global impression-severity; CP-eq.: chlorpromazine-equivalent; DSP: dopamine supersensitivity psychosis; ECT: electroconvulsive therapy; GAF: global assessment of functioning; SAD: schizoaffective disorder; SZ: schizophrenia; TRS: treatment-resistant schizophrenia; wks: weeks; yrs: years.
The results of our comparison of the data at the last time point following BREX initiation (average observational period: 24 months) revealed that the endpoint GAF scores were higher and the CGI-S scores were lower in the patients with BREX continuation compared to those with BREX discontinuation (Table 4). Each of these subgroups showed significant improvement from the baseline to the last time point in terms of GAF and CGI-S scores. However, the between-subgroup analyses showed no significant difference in the degree of improvement (i.e., GAF change, CGI-S change, and CGI-C); these negative results confirmed the results of a mixed-model analysis: GAF, Time effect, F = 18.899, p < 0.001; Group effect, F = 5.655, p = 0.024; Time × Group effect, F = 0.747, p = 0.395; CGI-S, Time effect, F = 13.802, p = 0.001; Group effect, F = 8.529, p = 0.007; and Time × Group effect, F = 0.519, p = 0.478. These results suggest that the two patient subgroups experienced similar improvements following the BREX introduction, even though BREX was discontinued in one subgroup. The results were the same when we removed four patients with BREX as an add-on from the analyses (patients with continuation of BREX, n = 1; patients with withdrawal of BREX, n = 3).
In addition, the analysis comparing outcomes following the switch to BREX in the 80 patients (regardless presence or absence of DSP) showed no significant difference for most of the measures. The exception was DSP: the patients who discontinued BREX included a higher ratio of DSP compared to the patients who continued BREX (Supplemental Table).
Discussion
We sought to identify factors that affect the success or failure of switching to BREX, which was judged at 6 weeks after the commencement of BREX, and our three main findings were as follows. (1) DSP and the speed of switching to BREX do not affect the success or failure of switching to BREX. (2) TRS and a history of successful switching to ARP independently affect the failure of switching to BREX. (3) The continuation of BREX (for 24 months) improves the symptoms of patients with DSP. Overall, these results indicate that compared to ARP, BREX can be introduced more safely as a switch from other antipsychotic agent(s). This study is the first to deal with switching to BREX head-on in the clinical course of patients with schizophrenia. However, these findings are premature since this study had both a retrospective design and a relatively small sample.
Comparison of the DSP and non-DSP groups
Several studies of ARP have shown that failure of switching to ARP is related to the worsening of psychosis in patients treated with high-dose and/or long-time antipsychotic medication(s) (Lin et al., 2009; Takaesu et al., 2016; Takase et al., 2015; Takeuchi et al., 2009; Takeuchi and Remington, 2013; ), and other studies revealed that such failure tends to be related to abrupt switching in particular (Casey et al., 2003; Obayashi et al., 2020; Pae et al., 2009) However, a meta-analysis by Takeuchi et al. (2018) did not support such risks of ARP treatment. Our present investigation of BREX did not confirm the results obtained in the above-cited studies regarding switching to ARP.
We observed that the present DSP group had significantly longer treatment durations, a higher number of hospitalizations, and a higher mean dose of antipsychotic(s) prior to the switch to BREX (Table 1). Lower GAF and higher CGI-S scores just before the switch were observed in the DSP group as well. These data suggest that the patients in the DSP group had been under treatment long enough to develop DS in the chronic course of their disease.
The failure rate of switching to BREX due to any reason was 29.5% (n = 13/44) in the DSP group and 24.5% (n = 26/106) in the entire series (i.e., the DSP and non-DSP groups). These failure rates were higher than the results of pivotal RCTs conducted by Fleischhacker et al. (2017) and Ishigooka et al. (2020): Fleischhacker’s trial reported a failure rate of ~7.0%, and Ishigooka’s trial reported a failure rate of 17.0% (=34/200). Notably, in the Fleischhacker et al. (2017) trial, the data showed that the rate of switching failure was 27.8%, derived from 14.4% (=58/404) of patients who failed a switch to BREX monotherapy in the first conversion and washout phase plus 13.4% (=54/404) of patients who withdrew from the trial in the single-blind stabilization phase up to the eighth week, but the results also indicated that the majority of these cases entailed either a withdrawal of consent by the patients themselves or early termination of the trial defined by the interim analysis. These RCTs required switching to BREX monotherapy and excluded patients with TRS, whereas our present study reflected predominantly partial switching to BREX and included many real-world patients with TRS, which was a factor that was likely related to the relatively high rate of the failure of switching to BREX in our study.
On the other hand, the rate of switching failure to BREX due to worsening of psychosis that we observed herein was different from the result of the switching failure to ARP. The failure rate based on the worsening of psychotic symptoms only was 6.8% (n = 3/44) in the DSP group and 12.3% (n = 13/106) in the entire patient series. Our previous study on switching to ARP (Takase et al, 2015) applying the same methodology as the present study obtained a much higher rate of switching failure than the present study: the failure rate of switching to ARP for any reason was 80% (n = 56/70), and that due to worsening psychosis was 22.9% (n = 16/70). These data indicate a clear trend of a lower rate of failure of switching to BREX compared to switching to ARP, but a firm conclusion regarding safer switching to BREX is difficult to make since many factors would differ in the same patients between switching to ARP and switching to BREX, such as the patient’s disease stage, clinical psychopathology, the switching method of ARP or BREX, concomitant medications, and more. Most importantly, the outcomes of our DSP and non-DSP patients did not differ in the failure rate of switch to ARP, which was inconsistent with our previous study (Takase et al., 2015; Table 1). These research aspects prevent a conclusion about comparisons of the switching failure between ARP and BREX, and the accumulation of such data in clinical practice is desired.
The potential difference between ARP and BREX in the difficulty of switching may be related to the fact that BREX has less intrinsic activity for DRD2 compared to ARP (Maeda et al., 2014); BREX is less likely than ARP to cause stimulation of supersensitive DRD2. The longer half-life of BREX (90 h) might be beneficial in the switch to BREX from other agents. Moreover, in Japan, the approved maximum dose of BREX is 2 mg (unlike the 4 mg available in the majority of countries), and a substantial portion of the present patients underwent only partial switching with the addition of 2-mg BREX and a tapering-off of their previous polytherapy from a mean of 830 mg to a mean of 430-mg CP-eq. dose. All of these pharmacodynamics and pharmacokinetic characteristics of BREX would contribute to a lower rate of switching failure.
Our analysis of the switching speed also revealed that eight of the nine patients in the DSP group who underwent an abrupt switch had a successful BREX introduction (Table 1), which supports the concept of safer switching to BREX and is in contrast to the greater impact of the switching speed on the success or failure of switching to ARP. For patients with high-dose treatment such as patients with DSP, the gradual switch from one antipsychotic(s) to another while maintaining the total antipsychotic dosage at an early step of the switch (i.e., plateau switching) is a key method for success: maintenance of the same DRD2 occupancy rate by the previous agent(s) and new agent(s) during the switching process can help prevent the occurrence of rebound psychosis (Kanahara et al., 2020; Kimura et al., 2021).
Our finding regarding the speed of switching to BREX showed that a higher number of patients in the DSP group (under high-dose medication) underwent a gradual switch, whereas the majority of patients in the non-DSP group underwent an abrupt switch. It is possible that when the treating physicians attempted to switch antipsychotics for their patients under high-dose antipsychotic(s), they could not help but select a gradual switching procedure to BREX. These physicians’ considerations might have contributed to the higher rate of successful switching in the DSP group.
This result is consistent with a finding obtained in a post-hoc analysis of the pooled three pivotal RCTs of BREX, that is, that the speed of switching to BREX did not affect the success or failure of switching (Correll et al., 2019). That finding, showing a lesser risk even in abrupt switching, also suggests that BREX can be introduced safely.
Comparison of the patients with successful switching to BREX and those with switching failure
We compared the patients with successful switching to BREX and the patients with switching failure in order to identify the influences of other factors. The analysis yielded that the patients’ age, age at disease onset, and TRS significantly differed between these two patient groups; namely, younger age, younger age at disease onset, and the existence of TRS were significantly related to switching failure (Table 2). This result was partly confirmed by the logistic regression analysis, which showed that TRS was a significant predictor of failure of switching to BREX (Table 3 and Figure 1).
Regarding the reasons for switching failure, we note that there were few patients with TRS due to worsening psychosis or adverse events immediately after the introduction of BREX. We, thus, speculate that the switching failed because BREX was judged to be ineffective by their physicians, or the clinical benefit in treating TRS patients was not immediately apparent. It is possible that this result concerning the higher failure in TRS patients may be related to the TRS-specific pathology. In patients with TRS with multiple pathophysiologies other than that involving the dopamine system (Kane et al., 2019; Potkin et al., 2020), switching from high-dose antipsychotic(s) with sedating effects to BREX, a nonsedating agent, might have made it easier for the core symptom domain (i.e., hallucinations and delusions) to become more apparent (even without worsening psychosis or relapse). As a result, the treating physician might have been forced to make an early decision about the feasibility of the long-term control of refractory positive symptoms with BREX.
This result might raise an alternative but logically possible interpretation of the effects of the diagnosis of DSP and TRS on the success or failure of switching. That is, patients with both DSP and TRS may tend to fail a switch to BREX due to TRS mediated by DSP, although our present analyses indicate that DSP did not have an effect on the switching failure in the two-group comparison (Table 1), since 38 patients among the 54 TRS patients were included in the DSP group, implying that TRS and DSP overlapped in these patients (Table 1).
The logistic regression analysis in this study revealed that the success or failure of switching to ARP was another significant predictor of the success of switching to BREX (Table 3). This result was the same when the analysis included all of the patients and when patients with DSP were included. The negative value of β (−2.323) indicates that failure of switching to ARP was related to the success of switching to BREX, or vice versa that success of switching to ARP was related to the failure of switching to BREX, or both. Our analyses demonstrated that 13 of the 16 patients who failed a switch to ARP succeeded in BREX switching whereas only 11 of the 52 patients with successful switching to ARP failed BREX switching, suggesting that the results of the logistic regression analysis were strongly related to the higher success rate of switching to BREX in patients with a failure of switching to ARP.
Of course, the patients’ treating physicians may have been especially careful about methods of switching to BREX and provided closer observation in patients who had already failed the switch to ARP; this extra care may have contributed to the higher rate of successful switching to BREX.
Effects of BREX treatment for the patients with DSP
Regarding the patients in the DSP group with successful switching to BREX, when we examined the psychopathology after 24 months of BREX treatment, we observed similar degrees of improvement in both the continuation and withdrawal subgroups in terms of changes in the GAF and CGI-S scores (Table 4). Despite a high number of TRS patients at 60% (8 of 13 patients), the BREX continuation subgroup exhibited >12-point improvement on the GAF, yielding a breakout from the threshold of TRS (i.e., 40 points). The additional analysis of outcomes with BREX treatment for the 80 patients who were switched to BREX showed that the patients who withdrew BREX at any point included a higher ratio of DSP compared to the patients who continued BREX for 2 years (Supplemental Table), suggesting some difficulty in continuing BREX for patients with DSP.
We reported that long-term treatment with ARP resulted in the clinical stability of patients with DSP (Kanahara et al., 2020). This might be related to the downregulation of DRD2 by the DRD2 partial agonism of ARP (Tadokoro et al., 2012). It has also been reported that an atypical antipsychotic long-acting injectable can improve psychotic symptoms in DSP patients treated with CP doses of 600–900 mg (Kimura et al., 2014, 2016). In the present study, it is unclear whether BREX truly reduced the density of DRD2 in the DSP + BREX continuation subgroup. It is possible that 24 months of continuous treatment with BREX may have contributed to the improvement of DSP symptoms due to its DPA profile, which is less likely to induce the DS state. However, since these results are based on the data of >13 patients and are based on a retrospective evaluation of CGI-S and GAF scores, they could be a type II error, which requires careful interpretation.
It is intriguing that a similar level of improvement was observed in the BREX withdrawal subgroup (Table 4), but this result is difficult to interpret from the viewpoint of psychopharmacology. In this subgroup, the withdrawal of BREX was defined as occurring after successful switching was established (after 6 weeks from the start of switching). Upon evaluation, we observed that the withdrawal subgroup had been taking a higher total antipsychotic dose (approximately 800-mg CP dose) relative to the continuation subgroup, which is consistent with a study showing that patients treated with doses >800 mg failed to continue BREX after the switch (Yoshimura et al., 2020), although that study did not note whether patients were switching to BREX monotherapy or not. Since we did not investigate the reasons for the withdrawals, we do not know why the present withdrawal subgroup patients experienced some improvements of psychotic symptoms but withdrew from treatment with BREX.
Our present results suggest that introducing BREX to patients with DSP may improve certain aspects of their DS symptoms and stabilize the patients clinically. BREX could be an option for patients who are good candidates for switching to ARP due to metabolic syndrome caused by other atypical antipsychotic(s) but face the additional challenge of an established DS state.
Study limitations
Our findings might have been influenced by the following multiple drawbacks and, thus, should not be generalized to all patients with schizophrenia. This was a retrospective study conducted at multiple psychiatry hospitals and included a heterogeneous group of patients with wide variations in patient background, previous medications, concomitant medications with BREX, and more. The decisions about switching to BREX and decisions about the switching strategy were made by the patients’ physicians and, thus, were not standardized. The 6-week observation period following the commencement of BREX treatment might have been too short to accurately judge the success or failure of the switch to BREX, as episodes of worsened symptoms beyond 6 weeks could be missed. These may have had some impact on the results of the switches to BREX.
Further, the present study did not include a psychopathological evaluation (i.e., the Positive and Negative Syndrome Scale (PANSS)) or identify detailed adverse events, and we did not confirm the inter-rater reliability among the study facilities: these omissions could have led to lower reliability to some degree. Outpatients counted for approximately 60% of the entire patient series, which may be related to adherence. These drawbacks, based mainly on the study design and small sample size, preclude firm conclusions about our results. It is necessary to conduct studies with a prospective design and a standardized switching procedure.
In addition, about half of the patients (38 of 80) who were judged as achieving a successful switch to BREX were treated with polytherapy, that is, they were taking antipsychotic(s) other than BREX. The limited approved dose of BREX in Japan (2 mg) may be related to the partial switching to BREX. Two positron emission tomography (PET) studies measured the occupancy of DRD2 with BREX (Girgis et al., 2020; Wong et al., 2021). Using 11C-raclopride, Wong et al. (2021) investigated healthy subjects taking a single dose 2–4 mg of BREX demonstrated that the occupancy rate in the dose range used in clinical treatment (i.e., 2–4 mg) was 53%–74%. Using 11C-[+]-PHNO, Girgis et al. (2020) examined patients with schizophrenia who took BREX at 1 or 4 mg for 10 days; they reported that the occupancy rate of 1-mg BREX was 64% and that of 4-mg BREX was 80%. However, a simulation analysis of population-based pharmacodynamics of BREX by Otsuka Pharmaceuticals suggested that approximately 90% of subjects taking 2 mg under a steady-state situation could temporarily exceed an occupancy rate of 80% (Otsuka Pharmaceutical Co., Ltd, 2018). Our study of the failure of switching to ARP demonstrated that abrupt worsening of psychosis during the switching happened at the average ARP dose of 21 mg (Takase et al., 2015), for which the DRD2 occupancy rate is clearly over 80% according to several PET studies (Gründer et al., 2008; Kegeles et al., 2008; Mamo et al., 2007; Yokoi et al., 2002). No firm conclusion has been made regarding the precise occupancy data for BREX, especially in the clinical range 2–4 mg (Hart et al., 2022). If the BREX dose is switched to 4 mg, the failure rate may have been greater than that at 2 mg due to the stronger dopamine agonism signal provided by a higher occupancy rate.
Conclusions
The results of this study of 106 patients with schizophrenia or schizoaffective disorder suggest that compared to ARP, a switch to BREX may be safer and may provide sufficient efficacy for patients with DS. Patients with schizophrenia require long-term medication, but long-term treatment with antipsychotic medication poses serious problems such as drug-induced metabolic side effects and the development of DSP. The present findings suggest the safety and efficacy of switching to BREX for the treatment of schizophrenia and further confirm the utility of BREX as having a low risk of inducing supersensitivity psychosis due to its pharmacologic profile.
Supplemental Material
sj-doc-1-jop-10.1177_02698811231177268 – Supplemental material for Can brexpiprazole be switched safely in patients with schizophrenia and dopamine supersensitivity psychosis? A retrospective analysis in a real-world clinical practice
Supplemental material, sj-doc-1-jop-10.1177_02698811231177268 for Can brexpiprazole be switched safely in patients with schizophrenia and dopamine supersensitivity psychosis? A retrospective analysis in a real-world clinical practice by Fumiaki Yamasaki, Nobuhisa Kanahara, Yusuke Nakata, Shinji Koyoshi, Yuta Yanagisawa, Takeru Saito, Takahiro Oiwa, Masanobu Kogure, Tsuyoshi Sasaki, Taisuke Yoshida, Hiroshi Kimura and Masaomi Iyo in Journal of Psychopharmacology
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NK reports honoraria from Otsuka Pharmaceutical Co., Ltd., Sumitomo Pharma Co., Ltd., Janssen Pharmaceutical K.K., Meiji Seika Pharma Co., Ltd., Mitsubishi Tanabe Pharma Co., Ltd., Yoshitomi Pharmaceutical Industries, Ltd., and Eisai Co. Ltd. YN reports honoraria from Otsuka Pharmaceutical Co., Ltd., Sumitomo Pharma Co., Ltd., Meiji Seika Pharma Co., Ltd., and Takeda Pharmaceutical Co., Ltd. TsuS reports grant from Shionogi & Co., Ltd. and honoraria from Sumitomo Pharma Co., Ltd., Takeda Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Meiji Seika Pharma Co., Ltd., Nobelpharma Co., Ltd., Kyowa Kirin Co., Ltd., Towaseiyaku Co., Ltd., Eisai Co. Ltd., Janssen Pharmaceutical K.K., Yoshitomi Pharmaceutical Industries, Ltd., and Shionogi & Co., Ltd. HK reports honoraria from Otsuka Pharmaceutical Co., Ltd., Sumitomo Pharma Co., Ltd., Janssen Pharmaceutical K.K., and Meiji Seika Pharma Co., Ltd. MI received consultant fees from Eli Lilly Japan K.K., Sumitomo Pharma Co., Ltd., Pfizer Japan Inc., Abbott Japan Co., Ltd. and Janssen Pharmaceutical K.K., and reports honoraria from Janssen Pharmaceutical K.K., Eli Lilly Japan K.K., Otsuka Pharmaceutical Co., Ltd., Meiji Seika Pharma Co., Ltd., Astellas Pharma Inc., Sumitomo Pharma Co., Ltd., Ono Pharmaceutical Co., Ltd., GlaxoSmithKline K.K., Takeda Pharmaceutical Co., Ltd., Mochida Pharmaceutical Co., Ltd., Kyowa Kirin Co., Ltd., MSD K.K., Eisai Co. Ltd., Daiichi-Sankyo Co. Ltd., Novartis Pharma K.K., Teijin Ltd., Shionogi & Co., Ltd., Hisamitsu Pharmaceutical Co., Inc. and Asahi Kasei Corporation. FY, SK, YY, TakS TO, MK, TY has no conflict of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a Grant-in-Aid for Scientific Research (21K07476) from the Japan Society for the Promotion of Science (JSPS).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.