
Abstract
Background:
Between 25% and 50% of patients suffering from treatment-resistant schizophrenia fail to achieve a clinical response with clozapine. The rapid identification and treatment of this subgroup of patients represents a challenge for healthcare practice.
Aims:
To evaluate the relationship between metabolic alterations and the clinical response to clozapine.
Methods:
A multicenter, observational, case–control study was performed. Patients diagnosed with schizophrenia treated with clozapine were eligible (minimum dose 400 mg/d for at least 8 weeks and/or clozapine plasma levels ⩾ 350 µg/mL). According to the Positive and Negative Syndrome Scale (PANSS) total score, patients were classified as clozapine-responsive (CR) (<80 points) or clozapine non-responsive (CNR) (⩾80 points). Groups were compared based on demographic and treatment-related characteristics, together with body mass index (BMI), waist circumference, insulin, leptin, and C-reactive protein plasma levels. Plasma levels of clozapine and its main metabolite, nor-clozapine, were measured in all the participants. In addition, the potential relationship between PANSS scores and leptin or insulin plasma levels was assessed.
Results:
A total of 46 patients were included: 25 CR and 21 CNR. BMI and waist circumference, fasting insulin and leptin plasma levels were lower in the CNR group, while C-reactive protein was not different. Moreover, significant negative correlations were observed between PANSS positive and general psychopathology subscores, on one hand, and insulin and leptin plasma levels, on the other hand, as well as between PANSS negative subscores and leptin plasma levels.
Conclusions:
Our results suggest that the lack of metabolic effect induced by clozapine is associated with the lack of clinical response.
Introduction
Schizophrenia is a chronic and disabling mental illness that impairs functionality and decreases life expectancy. Around the world, there are 21 million people who have schizophrenia, and 2 million are diagnosed annually, which results in a prevalence of around 0.3%. However, despite these prevalence values, the disease is associated with high levels of disability since it has an early onset, chronic course and compromises the functioning of those suffering from it (Charlson et al., 2018; GBD 2016 Disease and Injury Incidence and Prevalence Collaborators, 2017; Whiteford et al., 2013).
Antipsychotics and psychosocial support are the cornerstones of treatment for patients with schizophrenia, but despite this, many patients do not achieve remission. Samara et al. reported that about 20% of patients failed to show any symptomatic reduction, and 43% had a decrease of ⩽25% of the symptoms measured with the Positive and Negative Syndrome Scale (PANSS) and the Brief Psychiatric Rating Scale (Samara et al., 2019). Patients who do not present clinical improvement after two trials with different types of antipsychotics, administered for at least 8 weeks at recommended doses, are considered to have treatment-resistant schizophrenia (Keepers et al., 2021; National Institute for Health and Care Excellence (NICE), 2014).
A recently published systematic review of clinical practice guidelines for acute and maintenance management of schizophrenia shows that clozapine is the unanimously recommended treatment for patients having treatment-resistant schizophrenia (Correll et al., 2022). Clozapine is superior to other second-generation antipsychotics in reducing general and cognitive symptoms, improving general clinical impression based on Clinical Global Impression Scale scores, and preventing hospitalization and treatment discontinuation for any cause (Kane et al., 1988; Masuda et al., 2019; McEvoy et al., 2006).
However, clozapine is not efficacious for all treatment-resistant patients. One of the most cited works in this field, published by Kane et al. (1988), reported only a 30% positive response rate to clozapine in treatment-resistant patients. This initial observation was replicated in other studies showing a range of positive responses ranging from 25% to 55% (Agid et al., 2011; Dan et al., 2017; Köhler-Forsberg et al., 2017; Semiz et al., 2007). Altogether it seems that many treatment-resistant patients are also non-responsive to clozapine (CNR).
Considering the prevalence of schizophrenia, and the burden associated with this disease, those patients with CNR require further study.
In the search for parameters that identify the group of non-responders to antipsychotics in general or to clozapine in particular, several authors have proposed that changes in metabolic parameters are associated with good clinical response to antipsychotics. Such associations have been observed in several studies with different antipsychotics (Hermes et al., 2011; Luckhoff et al., 2019; Sharma et al., 2014). However, results concerning clozapine are conflicting. While some authors reported that clinical improvement was associated with an increase in body mass index (BMI) or weight gain (Bai et al., 2006; Meltzer et al., 2003), others failed to replicate such an association (Umbricht et al., 1994).
From a physiological point of view, abdominal obesity is a source of leptin. Therefore, in clozapine-treated patients, an increase in waist circumference or BMI is expected to be associated with changes in leptin plasma levels. Similarly, one might think that plasma insulin levels will correlate with a good response to clozapine. Since both hormones exert not only their well-known metabolic effects but also participate in brain remodeling and cognitive and emotional regulation (Paz-Filho et al., 2008, 2010; Shi et al., 2014), changes in their levels could be part of the explanation of the psychopathological response to the drug. Leptin and insulin have been investigated in antipsychotic-treated patients with conflicting results (Melkersson and Hulting, 2001; Nurjono et al., 2014; Roffeei et al., 2014; Sentissi et al., 2008). Kivircik et al. (2003) examined both parameters in patients treated with clozapine, but the participants in their study were all responders to the drug. To the best of our knowledge, information about the relationship between leptin or insulin levels and CNR patients has never been reported.
The main goal of the present study was to evaluate the relationship between metabolic alterations and the clinical response to clozapine. We hypothesize that clinical improvement in positive and negative symptoms and general psychopathology are associated with increased BMI, abdominal adipose tissue increments, and two biochemical parameters related to these changes: insulin and leptin plasma levels. For this purpose, we performed a case–control study comparing patients responsive to clozapine (CR) with CNR. The potential relationships between PANSS total scores as well as scores in the three PANSS subscales on one side and the plasmatic concentrations of insulin and leptin on the other were also evaluated in the complete sample as a whole.
Methods
Study design
A multicenter, observational case–control study was conducted between January 2017 and December 2018 in two facilities: the Hospital Neuropsiquiátrico Braulio A. Moyano and the Hospital Interdisciplinario Psicoasistencial José Tiburcio Borda, both in the City of Buenos Aires, Argentina. These hospitals assist low-income patients with and without health insurance and are located in the metropolitan area of Buenos Aires, which has a population of 12.8 million. The study protocol was approved by the Institutional Review Boards of the participating hospitals (Approval # IEC 1070/16). Written informed consent was obtained from all participants.
Participants
A convenience sample of outpatients and in-patients receiving the diagnosis of schizophrenia and treated with clozapine (minimum dose 400 mg/d and/or clozapine plasma concentration measured by HPLC-MS/MS ⩾ 350 µg/mL) for at least 8 weeks were eligible for the present study.
Patients were included if (a) were native Spanish speakers, (b) were ⩾18 years old, and (c) were diagnosed with schizophrenia by MINI interview (Sheehan et al., 1998). Subjects were excluded if they were (a) unable to participate in clinical assessments or complete symptom ratings because of illness, medication, sensory or speech impairment, or lack of language fluency, or (b) did not consent to participate in the study.
Patients were classified on the basis of their clinical status at the time of recruiting, being considered CNR, those with a total PANSS score ⩾80 points (cases), and CR those with a total PANSS score <80 points (controls) (Campana et al., 2021; Leucht et al., 2009, 2014).
Sociodemographic characteristics, substance use, and PANSS
The clinical severity of schizophrenia was measured with the PANSS (Kay et al., 1987), and the score was used to categorize the patients.
The following variables were collected to assess the comparability between groups: sex, age, employment status and education, consumption of psychoactive substances, alcohol and/or tobacco (number of cigarettes per day) in the last 2 weeks.
Clinical and therapeutic variables
Clinical variables used to compare the groups were number of previous hospitalizations, the time elapsed since the beginning of the symptoms, comorbid conditions and the concomitant medications.
The following data concerning antipsychotic treatment were also obtained to compare the groups: months of untreated psychosis, number of antipsychotics received before clozapine prescription, months from the beginning of the illness until the start of clozapine treatment and the clozapine daily dose (mg/day).
Blood samples were obtained to quantify insulin and leptin plasma levels, C-reactive protein (see below), and the concentration (steady state through) of clozapine and nor-clozapine. These determinations were carried out in the Clinical Pharmacokinetics Unit of the Parasitology and Chagas Service, Buenos Aires Children’s Hospital Ricardo Gutierrez, Buenos Aires, Argentina. Briefly, a quantitative HPLC-MS/MS method was developed for clozapine (generously provided by Rowan Laboratories) and nor-clozapine (commercially obtained from LGC Standards).
Anthropometric and metabolic parameters
BMI (kg/m2) was calculated using weight (kg) and height (m). Also, waist circumference was measured between the lowest rib and the iliac crest with the subjects standing.
After clinical evaluation, overnight fasting blood was collected to measure insulin (µIU/mL) and leptin (ng/mL) plasma levels. Fasting insulin plasma concentration was measured using standardized laboratory methods. Plasma leptin was quantified using a commercially available ELISA kit (Human ELISA Leptin SimpleStep ABCAM®).
Inflammatory parameter
Additionally, ultrasensitive C-reactive protein was measured by immunoturbidimetric method.
Statistical analysis
Categorical measures were reported as frequency or percentage and were compared by Fisher’s exact test. Continuous variables were reported as mean with 95% confidence interval (CI) and compared by Wilcoxon rank-sum test (Mann-Whitney U-statistic) for non-normally distributed continuous data. Since an overall potential relationship between PANSS scores and plasmatic concentrations of insulin and leptin would strengthen our observations and give support to our hypothesis, the Spearman’s rank correlation coefficient was applied to the values of the whole sample (CR and CNR). Benjamini-Hochberg’s false discovery rate was used to correct for multiple comparisons, and all p-values presented are adjusted. Statistical significance was set in p < 0.05.
Graph-Pad Prism 5.0 software was employed for statistical analysis.
Results
Sociodemographic characteristics
A total of 46 patients with schizophrenia were enrolled. Table 1 shows the comparison between patients with CR and CNR. The PANSS total scores and those obtained with the positive, negative, and psychopathology subscales were higher in CNR participants, thus confirming their correct allocation. No patients reported the consumption of illicit drugs or alcohol in the 2 weeks before the interview.
Sociodemographic characteristics, substance use, and PANSS.
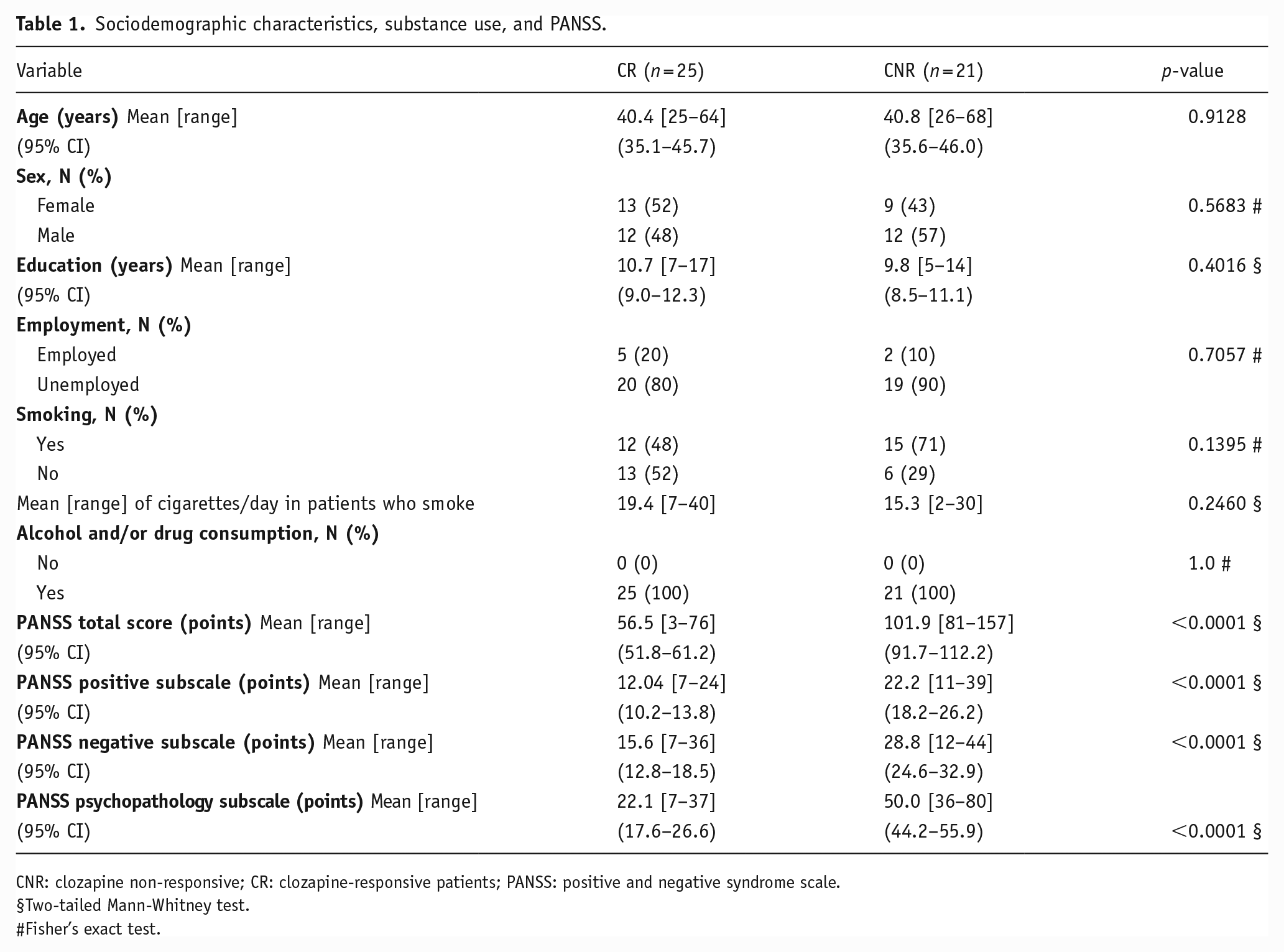
CNR: clozapine non-responsive; CR: clozapine-responsive patients; PANSS: positive and negative syndrome scale.
Two-tailed Mann-Whitney test.
Fisher’s exact test.
Clinical and therapeutic variables
There were no differences in the time from the beginning of the symptoms, the number of previous hospitalizations, or the number of antipsychotics trials previous to clozapine initiation between CNR and CR patients (Table 2). The mean duration of untreated psychosis was longer in CNR than in CR (35.4 months (95% CI: 18.9–51.9) vs. 14.0 months (95% CI: 6.3–21.7), p < 0.05). When comparing the mean time elapsed since the beginning of the illness and the prescription of clozapine we observed more extended periods of disease without clozapine in CNR than in CR (197.6 months (95% CI: 59.9–243.3) vs. 123.4 months (95% CI: 83.1–163.8), p < 0.01).
Comparison of participant’s clinical and therapeutic variables according to the response to clozapine.
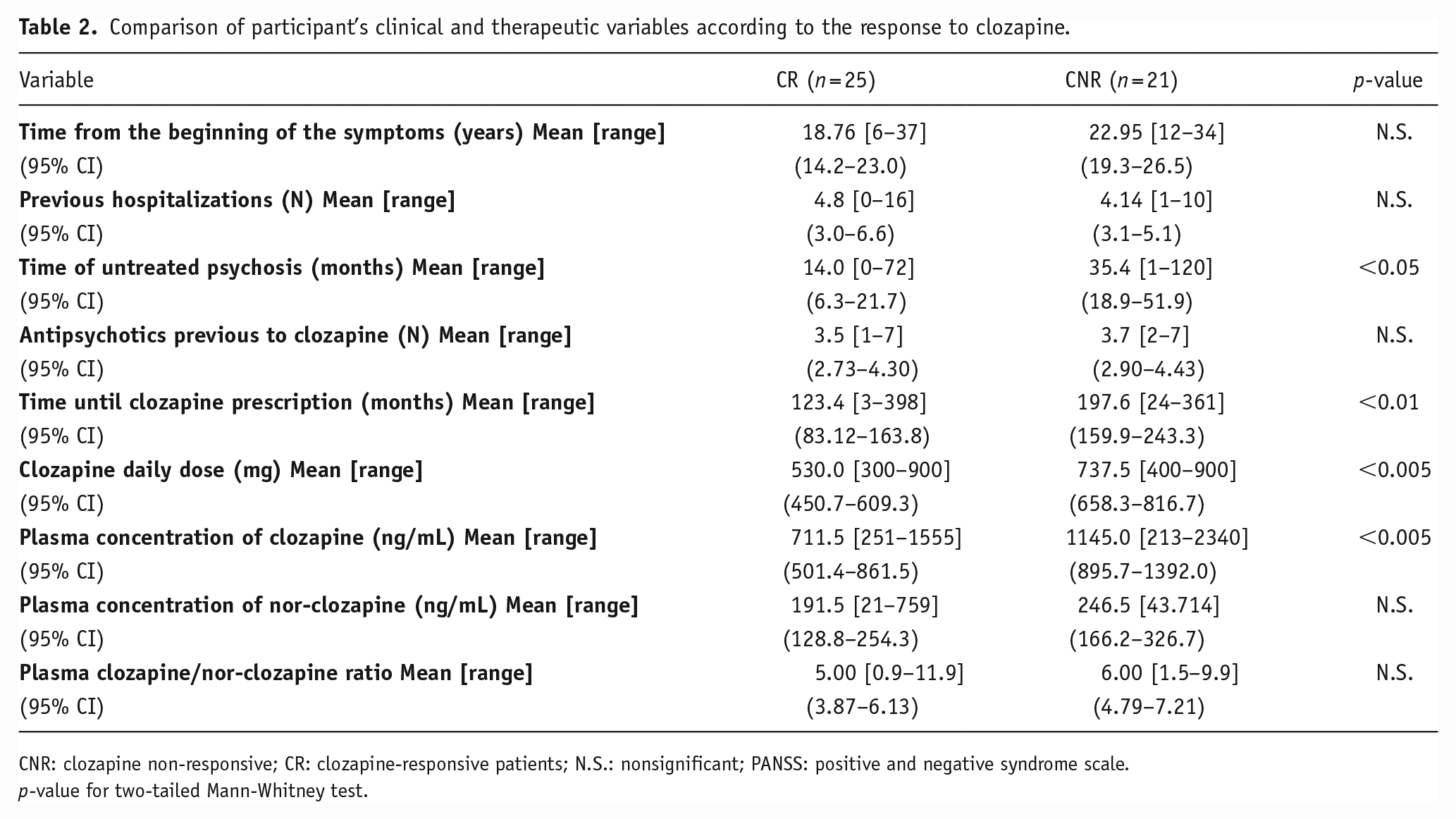
CNR: clozapine non-responsive; CR: clozapine-responsive patients; N.S.: nonsignificant; PANSS: positive and negative syndrome scale.
p-value for two-tailed Mann-Whitney test.
Mean doses of clozapine were higher in CNR than in CR (737.5 mg/day (95% CI: 658.3–816.7) vs. 530.0 mg/day (95% CI: 450.7–609.3), respectively, p < 0.005), which seems to reflect the intention of optimizing the treatment to achieve a clinical response. Accordingly, the mean plasma concentration of the drug was also higher in CNR when compared with CR patients (1145.0 ng/mL (95% CI: 895.7–1392.0) vs. 711.5 ng/mL (95% CI: 501.4–861.5), p < 0.005). The active metabolites of clozapine, nor-clozapine, and the ratio of clozapine/nor-clozapine were not different between groups. The clinical comorbidities and concomitant medications are shown in Supplemental Table 1.
Anthropometric and metabolic parameters
Table 3 compares the anthropometric and metabolic parameters between CR and CNR. Mean BMI was higher in CR than in CNR participants (31.9 kg/m2 (95% CI: 29.5–34.3) vs. 24.2 kg/m2 (95% CI: 22.6–25.7), respectively, p < 0.001). Similarly, waist circumference was also higher in the CR group than that in the CNR group, both in females and males (see Table 3).
Comparison of participant’s anthropometric and metabolic.
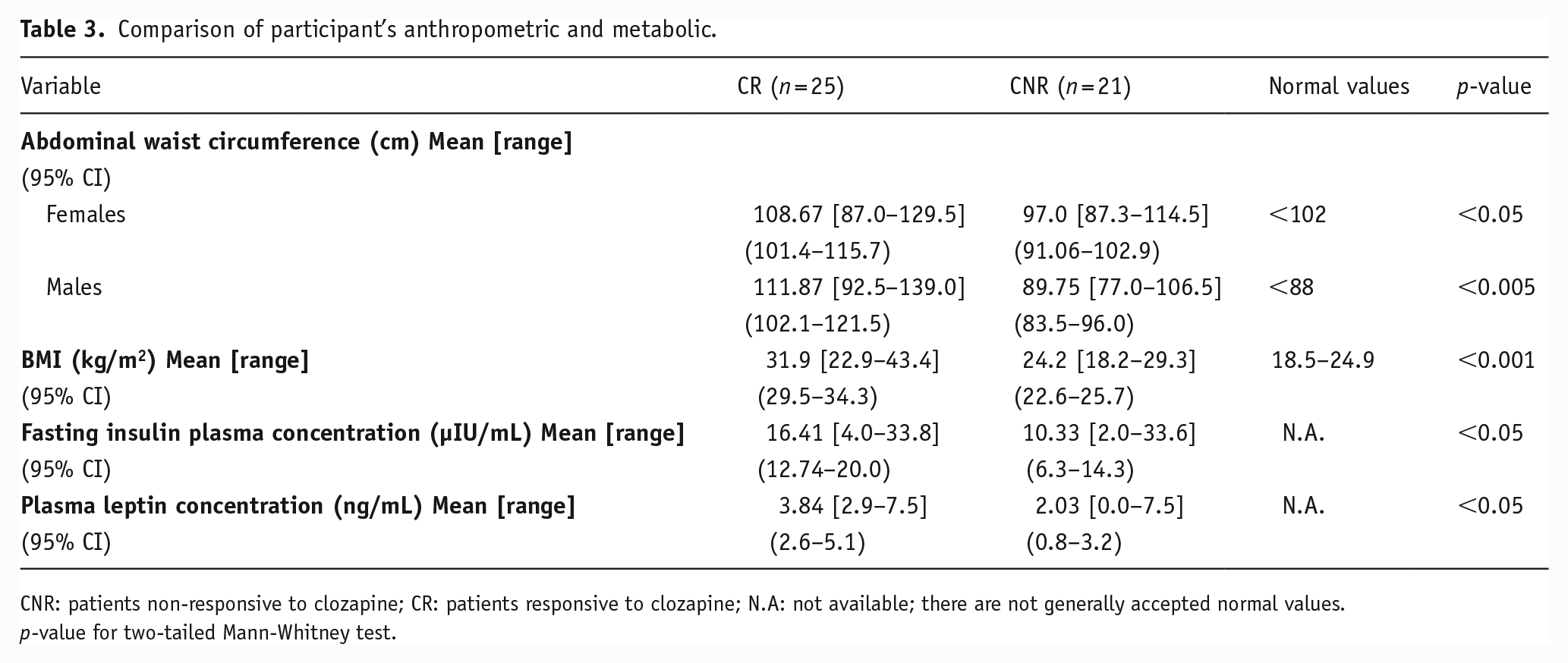
CNR: patients non-responsive to clozapine; CR: patients responsive to clozapine; N.A: not available; there are not generally accepted normal values.
p-value for two-tailed Mann-Whitney test.
We also measured plasma concentrations of two metabolism-related hormones: fasting insulin and leptin. Both were higher in CR than in CNR (16.4 µIU/mL (95% CI: 12.74–20.0) vs. 10.3 µIU/mL (95% CI: 6.3–14.3) for insulin and 3.8 ng/mL (95% CI: 2.6–5.1) vs. 2.0 ng/mL (95% CI: 0.8–3.2) for leptin, p < 0.05 for both parameters).
The PANSS total scores are moderately and negatively correlated with leptin plasma concentrations (r = −0.53 (p < 0.005)) and insulin plasma concentrations (r = −0.50 (p < 0.005)). When analyzing the PANSS subscales, a moderate and negative correlation was also observed for the PANSS positive subscale (r =−0.665 (p < 0.001); and r = −0.5039 (p < 0.005), for leptin and insulin plasma levels, respectively) and for the PANSS general psychopathology subscale (r = −0.6185 (p < 0.001) and r = −0.4599 (p < 0.01), for leptin and insulin plasma levels, respectively). When analyzing the correlation with the PANSS negative subscores, a low and negative correlation was observed for leptin plasma concentrations (r = −0.3622 (p < 0.05)), and no significant correlation was observed for insulin plasma levels (r = −0.2497 (p = 0.13)).
Inflammatory parameter
The C-reactive protein was not statistically different between groups.
Discussion
Schizophrenia patients with no response to clozapine represent a challenge for clinical practice. Therefore, tools are necessary to rapidly identify these patients and provide them with another therapeutic option. Unfortunately, few studies have focused on potential biomarkers that recognize these patients. To fill this gap, we carried out the present study in which we hypothesized that increased central obesity and BMI could differentiate between CR and CNR patients.
The relationship between antipsychotic-induced weight gain and symptomatic improvement in patients with schizophrenia presented conflicting results. Initial studies have reported that the increase in weight was unrelated to the clinical response (Umbricht et al., 1994). However, a systematic review that compiled all the published studies reported an overall positive association between antipsychotic-induced weight gain and clinical response in 22 (71%) of the 31 studies reviewed (Raben et al., 2018). Concerning specifically to clozapine treatment, recently published studies informed a positive association between weight gain or increments in BMI and the reduction of positive symptoms in patients with schizophrenia treated with clozapine (Bai et al., 2006; Meltzer et al., 2003; Sharma et al., 2014). So far, the information suggests that weight gain can be considered a predictor of symptom improvement in patients with schizophrenia. Based on this, we chose BMI and waist circumference as potential CNR markers in our study. Our results show that the antipsychotic response to clozapine is positively associated with larger central obesity and BMI in patients with CR schizophrenia. We observed that BMI in CR was almost 30% higher than that in CNR. Furthermore, the BMI of CR patients was within the range of obesity (29.5–34.3), while BMI of CNR patients was within the normal range (22.6–25.7) (Obesity Expert Panel, 2013). Additionally, larger waist circumference—in most cases above the recommended range (Obesity Expert Panel, 2013)—was observed in women and men of the CR group, which is interesting since some authors pointed out that factors associated with body weight changes were not the same for both sexes (Lau et al., 2016). This result has significant clinical relevance. By implementing two low-cost measures, such as determining BMI and waist circumference, the mental health professional could have a valuable parameter to potentially identify patients resistant to clozapine. It should be noted that under our experimental conditions, we cannot ensure that the metabolic alterations of the CR group preceded the prescription of clozapine. However, either due to previous metabolic conditions or the effect of clozapine treatment, BMI and waist circumference seem to discriminate between both groups.
In the present study, together with higher BMI and waist circumference, we observed that plasma leptin levels were higher in the CR patients than those in the CNR group. Since leptin is an adipocytokine released by white adipose tissue, such an association could be expected. Moreover, previous reports found that patients with schizophrenia who presented antipsychotic-induced weight gain and a good clinical response also showed increments in leptin levels (Venkatasubramanian et al., 2007). To our knowledge, this parameter has not been examined in association with the response to clozapine. Our results suggest that leptin could be a potential biomarker to identify CNR patients.
Moreover, we have correlated leptin levels with the score in the different subscales of the PANSS. Our results show a correlation of greater magnitude in the general psychopathology and positive symptoms subscale. This is in line with previous observations of Takayanagi et al., who reported that serum leptin levels are inversely correlated with the severity of positive symptoms among patients with schizophrenia treated with olanzapine (Takayanagi et al., 2013).
On the other hand, although normal population insulin plasma levels are not yet firmly established, their most accepted clinical usefulness is as a biomarker of insulin-resistance in the context of type-2 diabetes, one of the adverse consequences of antipsychotic treatment. However, some other associations between insulin and schizophrenia have been proposed. Based on the potential role of brain insulin-modulated pathways, changes in this hormone plasma levels could also be seen as a link between antipsychotic-induced metabolic changes and clinical efficacy (see reviews by Agarwal et al., 2020 and Sharma et al., 2014). In fact, some authors informed a positive relationship between clinical response to treatment (total, positive, and general psychopathology PANSS scores) and insulin plasma levels (Fan et al., 2006). In the present study, we observed that fasting insulin plasma levels were higher in CR patients than those in CNR. Moreover, similarly to what we found for leptin levels, higher insulin levels correlated with better scores in total, positive, and psychopathological PANSS scores. The only score in PANSS that did not correlate with insulin was the negative PANSS score. As far as we know, differences in insulin levels between CR and CNR have not been explored before, and we herein provide the first evidence supporting such a relationship. Additionally, it would be interesting to know whether these correlations are similar when CR and CNR groups are considered separately, but unfortunately the sample size did not allow us to make such evaluation, which would be performed in future studies.
Ultra-resistant schizophrenia has been associated with chronic low-grade peripheral inflammation (Fond et al., 2019). In the present study, although we have detected 50% higher C-reactive protein levels in patients with CNR compared to CR, this difference is not statistically significant, probably due to the small sample size.
The patients in our sample were treated with clozapine doses above the recommended values (Campana et al., 2021; Subramanian et al., 2017). Therefore, differences in clinical response observed between both groups could not be attributed to insufficient drug levels. Moreover, the plasmatic concentration of the clozapine active metabolite, nor-clozapine, was similar in both groups, as was the ratio of clozapine/nor-clozapine. Clozapine is demethylated by the CYP1A2 and CYP3A4 isoforms of the CYP450 superfamily of enzymes, but according to in vivo studies, the latter is the major catalyst (Thorn et al., 2018). Since substrates potentially saturate CYP1A2, and clozapine concentrations are high in both groups of patients, we can speculate that the absence of differences in nor-clozapine plasma levels between CR and CNR participants could reflect the saturation of the CYP1A2 pathway.
Overall, our results show that patients with CNR, in comparison to those with CR, show lower BMI and waist circumference. In addition, they have lower levels of leptin and insulin. All these data show that in patients with treatment-resistant schizophrenia who receive clozapine, the lack of metabolic effect induced by the drug is associated with the lack of clinical response. This parallelism, even in the presence of therapeutic concentrations of clozapine and its metabolite, could reflect that resistance to clozapine is rather a systemic event and not just limited to the antipsychotic response. This way of thinking about clozapine resistance could lead to the search for different etiopathological factors that differentiate responders from non-responders.
Strength
A strength of this study is the classification of the CR and CNR groups. Having measured clozapine and its metabolite in the blood allows us to ensure the correct classification of the patients in CR and CNR since the non-responders are patients with therapeutic concentrations in the blood but who do not present a clinical response. Another study’s strength is that we use validated tools to measure clinical variables applied by trained psychiatrists. Additionally, although the sample is small, considering the rare condition of non-response to clozapine, we think it is sufficient to draw conclusions that allow us to proceed with more extensive studies.
Limitations
One of the study’s limitations is that we didn’t use a matched case–control design. Although the ideal scenario would have been to match at least by sex and age, the infrequent nature of the CNR made it impossible for us to get as many patients as needed to have a matched sample. Despite this, as seen in Table 1, the sample does not present significant differences in gender and age. Another limitation was that some variables related to weight gain were unable to be controlled, such as diet and physical activity. However, most of the participants in both CR and CNR were in-patients, and all followed the same diet plan during hospitalization with no free access to food. Physical activity was also comparable for all patients throughout the study period.
Supplemental Material
sj-docx-1-jop-10.1177_02698811231181565 – Supplemental material for Body mass index, waist circumference, insulin, and leptin plasma levels differentiate between clozapine-responsive and clozapine-resistant schizophrenia
Supplemental material, sj-docx-1-jop-10.1177_02698811231181565 for Body mass index, waist circumference, insulin, and leptin plasma levels differentiate between clozapine-responsive and clozapine-resistant schizophrenia by Guillermo Hönig, Federico M Daray, Demián Rodante, Lucas Drucaroff, María Laura Gutiérrez, Mariela Lenze, Facundo García Bournissen and Silvia Wikinski in Journal of Psychopharmacology
Footnotes
Acknowledgements
We thank all the individuals who participated in the study.
Authors’ Note
Demián Rodante is also affiliated to Facultad de Medicina, Instituto de Farmacología, Universidad de Buenos Aires, Buenos Aires, Argentina.
Federico M Daray and Lucas Drucaroff are also affiliated to Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), Argentina.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SW acknowledged the following funding sources: UBACYT # 20020170100017BA; CONICET # 11220130100266CO; and ANPCyT PICT-Start-Up 2018 #2902.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.