
Abstract
Alcohol use disorder (AUD) is a prevalent condition associated with high degree of comorbidity and mortality. Among the few approved pharmacotherapies for AUD, two involve opioid receptor antagonism. Naltrexone and nalmefene are thought to act via opioid receptor blockage to reduce neural response to alcohol and drug-associated cues and consumption, but there have been limited efforts to characterize these effects in humans. In these studies, we sought to test the magnitude of opioid antagonism effects on neural response to monetary rewards in two groups: light drinkers (for the naltrexone study) and heavy drinkers (for the nalmefene study). We conducted double-blind, randomized, crossover pilot studies of reward activation in the brain following acute administration of opioid antagonist and placebo in 11 light and 9 heavy alcohol users. We used a monetary incentive delay task during functional MRI. We found a main effect of cue type on BOLD activation in the nucleus accumbens, demonstrating a neural reward response. The effect of opioid antagonism, relative to placebo, was small and nonsignificant for reward activation in the accumbens for both light and heavy alcohol users. Based on the results of two pilot studies, opioid antagonist medications do not appear to decrease neural activation to monetary rewards in the nucleus accumbens relative to placebo.
Keywords
Introduction
Naltrexone and nalmefene are among the few drugs approved to treat alcohol use disorder (AUD); (Winslow et al., 2016), and they are effective at reducing alcohol use (Anton et al., 2006; Mann et al., 2013; Oslin et al., 2015). Both drugs are competitive antagonists at opioid receptors, with affinity primarily for mu and kappa subtypes (Raynor et al., 1994). Alcohol use causes the release of endogenous opioids (Mitchell et al., 2012; Tanda and Di Chiara, 1998), and these drugs are believed to reduce the reinforcing effects of alcohol by blocking opioid receptor activation (Heilig et al., 2011). Previous studies have examined whether opioid-receptor antagonism affects general reward responding in the nucleus accumbens, the brain region most closely associated with reward. A single dose study of naltrexone found no effect on activation (Nestor et al., 2017) during a monetary incentive delay (MID) task, but used a small reward value (<$1). Another study showed that nalmefene reduced accumbens response during the MID task (Quelch et al., 2017), but used a similarly small reward value. To clarify opioid receptor antagonism effects in the nucleus accumbens, we conducted two randomized, double-blind, placebo-controlled crossover studies (one with naltrexone, the other with nalmefene) using a MID task with a high ($5) reward, which has been shown to induce robust activation (Knutson et al., 2001). We hypothesized that naltrexone and nalmefene administration would reduce levels of reward-related activation in the nucleus accumbens in both light and heavy drinkers since we expect the basic neural circuitry to be similar, and since both drugs have shown strong occupancy for opioid receptors (Raynor et al., 1994).
Material and methods
Participants
For the naltrexone study (NCT04854551), we recruited healthy adults at the University of Colorado Anschutz Medical Campus. Exclusion criteria included an AUD Identification Test (Saunders et al., 1993) score >10 and being a nondrinker. For the nalmefene study, we recruited adults with current heavy alcohol use patterns for a study at the National Institutes of Health Clinical Center in Bethesda, Maryland (NCT02639273). Participants must have averaged at least one binge day (>4/5 drinks in a 2-h period for women/men) per week for the 90 days prior to the study. Study protocols were approved by institutional review boards at the individual institutions. Participants completed an informed consent process prior to enrolling.
Study design and procedures
Both studies used a counterbalanced crossover design, where each participant completed an MRI scan following a placebo and an active medication dose. In the University of Colorado study, 5 days of medication were used for each condition (naltrexone and placebo), with naltrexone dosing at 25 mg/day for days 1–2, and 50 mg/day for days 3–5. For the National Institutes of Health study, participants were given nalmefene (18 mg) or placebo as a single dose approximately 1 h prior to each MRI scan. For both studies, the second scan was scheduled at least 7 days after the first scan to allow washout.
Measures
Participants completed the MID task (Knutson et al., 2001). The task presents participants with three cues, a triangle, a circle, and a square, representing the chance to avoid losing $5, gain $5, or gain $0, respectively. After the cue was shown, a target rectangle appeared and participants tried to press a button while it was present to succeed on the trial. In the nalmefene study, there were two conditions (safe and threat) for the task, indicated by a colored border. The border indicated potential to hear an aversive noise (i.e., a scream) and see a fearful face, but previous work has shown that the threat condition does not modulate reward response in the accumbens (Penner et al., 2022), so we averaged across the safe and threat conditions. In both studies, the number of trials of lose $5, gain $0, and gain $5 were balanced, with at least 18 of each trial type. Participants’ success rates varied, but average rates were between 55% and 60% correct for each trial type, indicating engagement with the task. Participants could win up to $110 but typical earnings were $40 per run.
MRI collection and analysis
Both studies were collected on a Siemens Skyra 3T magnet with a 20-channel head coil. We collected a T1-weighted scan for anatomical reference and a T2-weighted sequence for the functional task run. Data were preprocessed with Analysis of Functional NeuroImaging (AFNI) software (Cox, 1996) using standard procedures (afni_proc.py). We used the Harvard-Oxford atlas (Goldstein et al., 2007) to generate the nucleus accumbens masks and 3dROIstats to extract activation (beta-weights). We conducted linear mixed effects models in R software version 4.2.1 with main effects of cue-type (gain $5, gain $0), medication (active, placebo), and their interaction. The dependent variable was nucleus accumbens activation, averaging across the left and right side. We report effect sizes as Cohen’s d for all primary contrasts since this may be more meaningful than p-values in these small studies.
Results
Participants in the naltrexone study were 11 young adults (8 females, mean age = 24.2 years, SD = 4.6) who were nonhazardous drinkers (mean AUDIT score = 5.6, SD = 2.8). Participants in the nalmefene study were nine young adults (five females, mean age = 31.7 years, SD = 6.1) who were hazardous drinkers (mean AUDIT score = 15.6, SD = 8.2).
Naltrexone imaging results
Imaging analysis revealed a main effect of cue-type (F1,30 = 17.1, p < 0.001) but no effect of medication (F1,30 = 0.54, p = 0.469) or cue-by-medication interaction (F1,30 = 0.45, p = 0.505, see Figure 1). Participants showed greater activation for the gain $5 (d = 1.20) cues relative to the gain $0 cue. However, they showed equivalent activation during naltrexone and placebo for the gain $5 cue (d = 0.08).
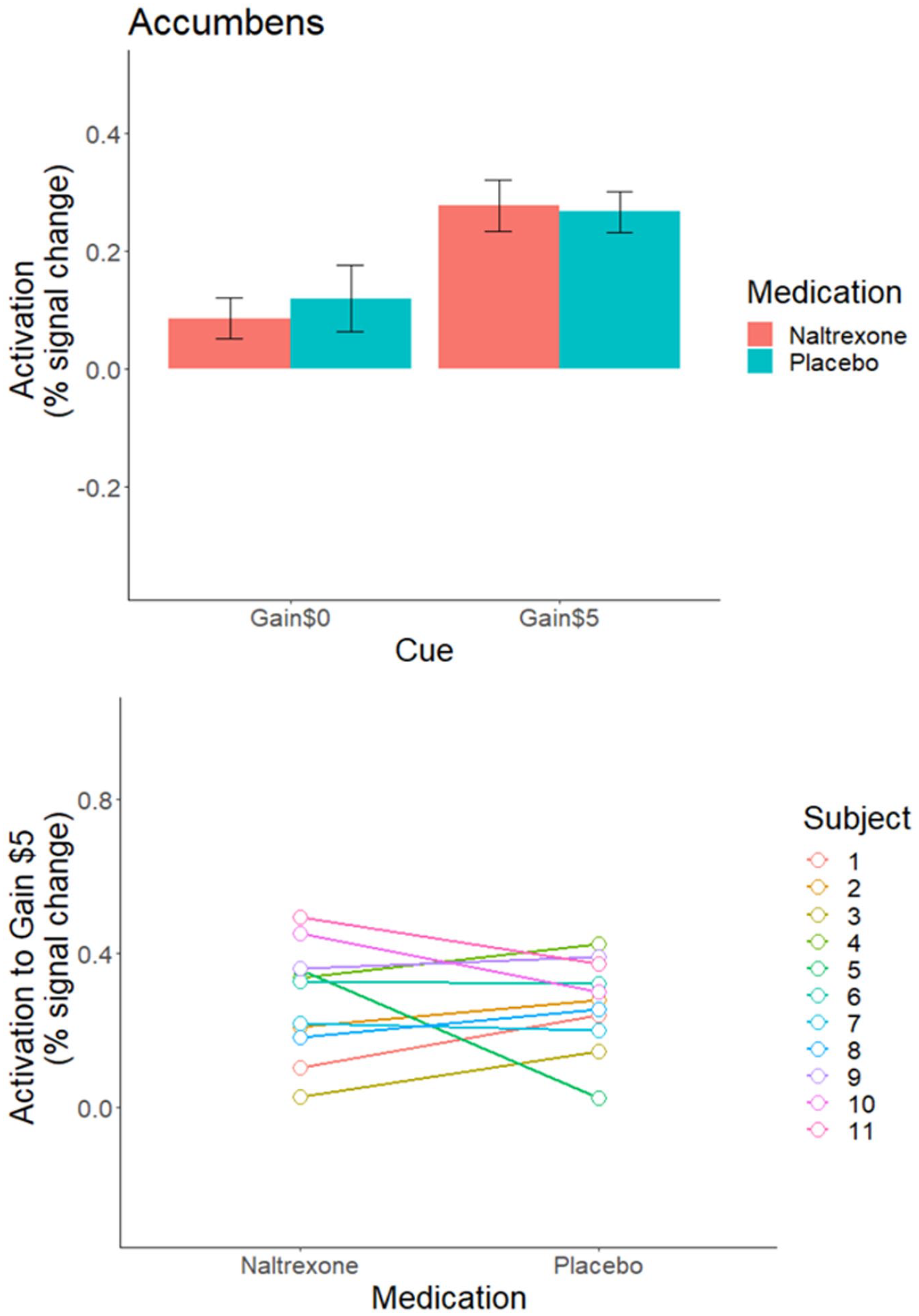
The top panels depict the mean activation to each cue type for participants on the following: the 5-day naltrexone (NTX) or 5-day placebo (PLC) regimens. The error bars represent standard error of the mean. Activation was extracted from a nucleus accumbens mask. There was a main effect of cue (p < 0.001), but there was no main effect of medication and no cue-by-medication interaction (all p > 0.05). The bottom panels depict the values from individual participants, and each participants values are connected by a line to show the change between the naltrexone and placebo conditions.
Nalmefene imaging results
Imaging analysis revealed no significant main effects of cue (F1,24 = 2.67, p = 0.115), medication (F1,24 = 3.68, p = 0.067), or interactions (F1,24 = 2.87, p = 0.103, see Figure 2). Participants showed greater activation for the gain $5 (d = 1.13) cues relative to the gain $0 cue. However, they showed equivalent activation during nalmefene and placebo for the gain $5 cue (d = −0.19). The trend for an effect of medication seems to be driven by reduced activation to gain $0 under the placebo condition relative to nalmefene.
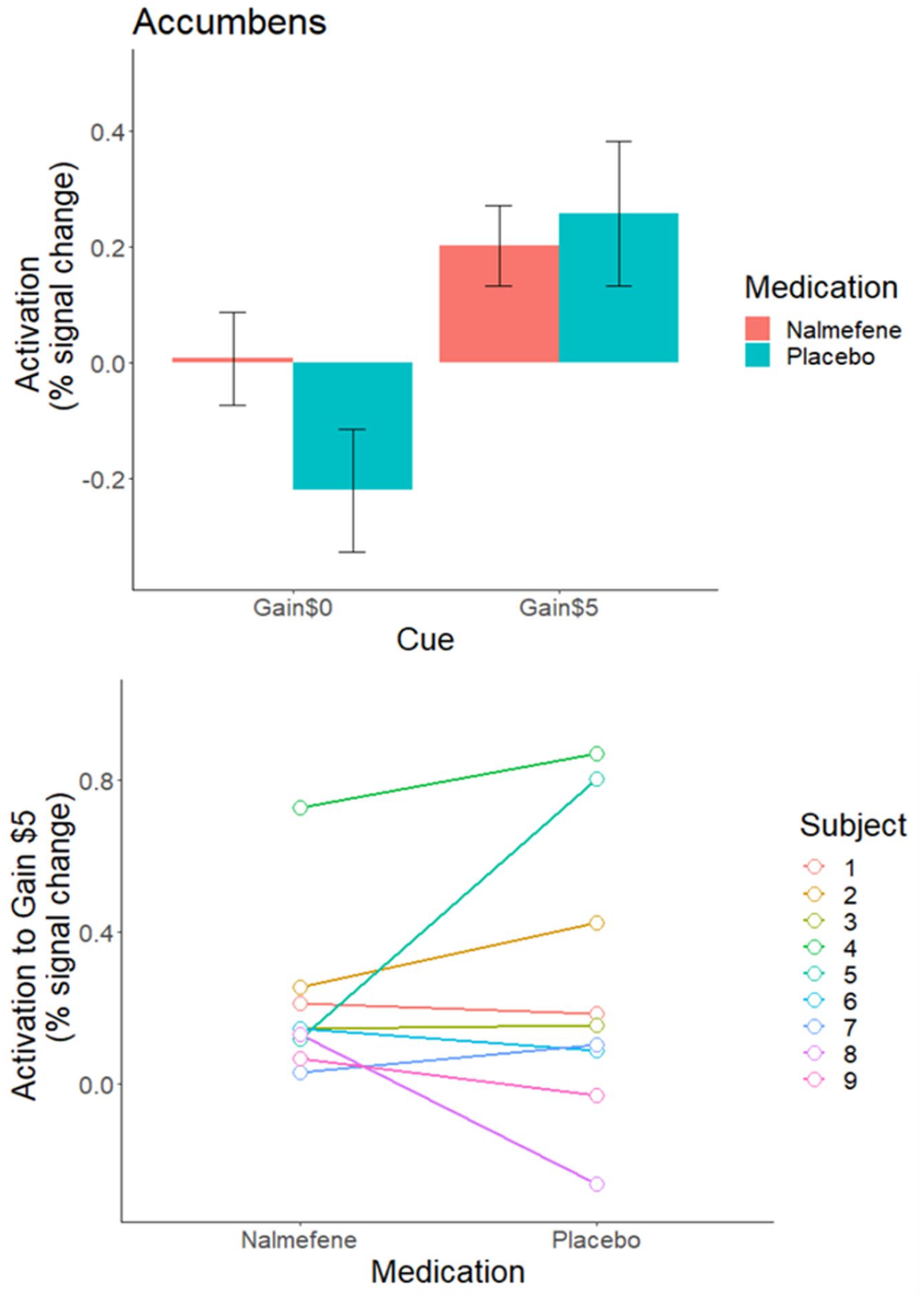
The top panels depict the mean activation to each cue type for participants on nalmefene or placebo days. The error bars represent standard error of the mean. Activation was extracted from a nucleus accumbens mask. The bottom panels depict the values from individual participants, and each participants’ values are connected by a line to show the change between the nalmefene and placebo conditions.
Discussion
We did not find evidence that opioid receptor antagonism reduced reward activation in the nucleus accumbens of light or heavy drinkers, corroborating the null results of naltrexone from the previous study (Nestor et al., 2017). Both studies had small sample sizes, which was a limitation of these analyses, although the effect sizes found in each study were small and in the case of naltrexone in the opposite of the hypothesized direction. Interestingly, in the nalmefene study there was some evidence of reduced activation to gain $0 cues under the placebo condition, which we suspect is noise, but this underscores the limitation of the small sample sizes in these studies.
In the nalmefene study, one individual participant (subject 5, Figure 2) had a robust change in nucleus accumbens signaling when taking nalmefene compared to placebo. Future studies should determine whether subsets of individuals with AUD may have greater change in reward signaling with opioid antagonists and whether this is related to treatment response. Some studies in adults with AUD have shown that naltrexone reduces striatal activation to alcohol cues (Myrick et al., 2008; Bach et al., 2020), and that degree of reduction in brain response may relate to likelihood of reduced heavy alcohol use when taking naltrexone (Schacht et al., 2017). However, other well-powered studies showed no effect of naltrexone on striatal response to alcohol cues (Lukas et al., 2013; Schacht et al., 2013). The study showing that nalmefene reduced reward response had participants complete the task while exposed to a moderate dose of alcohol (Quelch et al., 2017), raising the possibility that nalmefene’s effects may require the presence of alcohol. However, given the mixed evidence for naltrexone on alcohol cue reactivity, it remains possible that opioid receptor antagonism affects striatal response to neither monetary nor alcohol rewards. This is surprising given that mu-opioid receptors are abundant on dopaminergic neurons that originate in the ventral tegmental area and project to the nucleus accumbens, and that the addictive potential of opioid agonists like heroin is believed to be mediated by this neurobiological reward pathway (Fields and Margolis, 2015).
The strengths of the present studies include a within subject design, clinical dosing regimens (naltrexone at 50 mg/day and single doses of 18 mg nalmefene p.r.n), and high reward value. Our results indicate that opioid antagonism does not affect nucleus accumbens response to monetary rewards relative to placebo.
Footnotes
Acknowledgements
We thank the Research Pharmacy and the nurses and staff at the Clinical and Translational Research Center at the University of Colorado Anschutz Medical Campus. We thank the Brain Imaging Center and its staff. We appreciate the technical support of Benson Stevens, and clinical support of Nancy Diazgranados, MD, MS, Tonette Vinson, CRNP, and Yvonne Horneffer, CRNP. We thank the NIH Clinical Center Pharmacy, the MRI technicians, research assistants, and the nursing staff from the 5-SWS day hospital unit of the NIH Clinical Center. We thank Brian Knutson for advice on task implementation and interpretation of results.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by NIH/NCATS Colorado CTSA Grant Number UL1 TR002535, the NIAAA Division of Intramural Clinical and Biological Research (Z1A AA000466 PI: Ramchandani), and a career development award (K99AA024778, PI: Gowin). Its contents are the authors’ sole responsibility and do not necessarily represent official NIH views.