
Abstract
Background:
Clozapine is the primary antipsychotic (APD) for treatment-resistant schizophrenia (TRS). However, only 40% of patients with TRS respond to clozapine, constituting a subgroup of clozapine-resistant patients. Recently, the neuropeptide orexin-A was shown to be involved in the pathophysiology of schizophrenia. This study evaluated the association of orexin-A levels with the clozapine response in patients with TRS.
Methods:
We recruited 199 patients with schizophrenia, including 37 APD-free and 162 clozapine-treated patients. Clozapine-treated patients were divided into clozapine-responsive (n = 100) and clozapine-resistant (n = 62) groups based on whether they had achieved psychotic remission defined by the 18-item Brief Psychiatric Rating Scale (BPRS-18). We compared blood orexin-A levels among the three groups and performed regression analysis to determine the association of orexin-A level with treatment response in clozapine-treated patients. We also explored the correlation between orexin-A levels and cognitive function, assessed using the CogState Schizophrenia Battery.
Results:
Clozapine-responsive patients had higher orexin-A levels than clozapine-resistant and APD-free patients. Orexin-A level was the only factor significantly associated with treatment response after adjustment. Orexin-A levels were negatively correlated with BPRS-18 full scale and positive, negative, and general symptoms subscale scores. We also observed a positive correlation between orexin-A levels and verbal memory, visual learning and memory, and working memory function.
Conclusions:
This cross-sectional study showed that higher levels of orexin-A are associated with treatment response to clozapine in patients with TRS. Future prospective studies examining changes in orexin-A level following clozapine treatment and the potential benefit of augmenting orexin-A signaling are warranted.
Introduction
Schizophrenia is a severe mental disorder that ranks as the eighth leading cause of disability-adjusted life years among individuals aged 15–44 years glo (Rossler et al., 2005). Antipsychotic drugs (APD) are the mainstay of treatment; however, approximately 30–50% of patients exhibit resistance to APD treatment (Haddad and Correll, 2018), constituting a subset known as treatment-resistant schizophrenia (TRS). Kane et al. (1988) first defined TRS as the absence of at least a 20% reduction in symptom severity after two distinct treatment courses with adequate doses of APD, each lasting a minimum of 4 weeks. While positive symptoms are often the hallmark of TRS, the enduring symptoms might also encompass negative and cognitive aspects (Howes et al., 2017). Clozapine is the only licensed APD for TRS (Kane et al., 1988). Unfortunately, only 40% of TRS patients exhibit sufficient response to clozapine treatment, categorizing them as clozapine-resistant or ultra-resistant (Siskind et al., 2017). Clozapine-resistant patients are probably the most disabled of all patients with schizophrenia (Chiu et al., 2020) and are characterized by a protracted course, poorer quality of life, and greater social and socioeconomic burden than clozapine-responsive patients (Buckley et al., 2001). These individuals also are more prone to distinct pathological processes and cognitive impairment (Rajkumar et al., 2011), yet they face a dearth of effective medications. However, the underlying biological mechanisms that differentiate clozapine-resistant and clozapine-responsive patients remain predominantly unexplored (Samanaite et al., 2018). Once elucidated, these mechanisms could offer valuable insights into exploring innovative treatment strategies targeting clozapine resistance.
Evidence has shown that TRS is associated with a multitude of neurobiological perturbations encompassing not only changes in dopaminergic (DA) (e.g., supersensitivity) and glutamate signaling but also alterations in the signaling pathways of neuropeptides, which are often co-localized and interact with monoaminergic neurotransmitters to work as paracrine or neuroendocrine to contribute to the symptoms of schizophrenia and modulate the response to APDs (Rodríguez et al., 2020). Orexins (also known as hypocretins) sit at the nexus of neuropeptides that are implicated in the pathophysiology of schizophrenia. They are secreted by orexin neurons in the lateral hypothalamus (Sakurai et al., 1998), which are also regulated by serotoninergic, DA, adrenergic, and glutamatergic inputs (Linehan et al., 2019; Yamanaka et al., 2006) with functions involving arousal, energy homeostasis, mood regulation (Strawn et al., 2010), and cognitive function (Deutch and Bubser, 2007). In humans, the blood levels of orexin-A are linearly correlated with levels in the cerebrospinal fluid (correlation coefficient = 0.78) (Strawn et al., 2010) and have been recognized as a potential marker to reflect central orexin activity in patients with neuropsychiatric illnesses (Lee et al., 2020; Steward et al., 2019). One recent investigation reported that in first-episode APD-naive patients with schizophrenia, the orexin-A levels are lower relative to healthy controls both centrally and peripherally (Lu et al., 2021). In contrast, under chronic APD treatment, either clozapine or other APDs, patients with schizophrenia have increased orexin-A levels compared with healthy controls (Chen et al., 2019) and even APD-free patients (Chen et al., 2022). Chien et al. (2015) reported that patients with higher orexin-A levels exhibit fewer negative and disorganized symptoms. Nevertheless, it remains unclear whether response to clozapine in patients with TRS is associated with orexin-A levels.
Emerging evidence suggests an association between higher glutamatergic transmission and the clozapine response (Goldstein et al., 2015). Given that orexin-A robustly enhances glutamatergic system activity in the brain (Aracri et al., 2015; Calva et al., 2018), we hypothesized that a higher orexin-A level might correlate with a better response to clozapine. This study aimed to compare orexin-A levels between clozapine-responsive and clozapine-resistant patients, evaluating their association with treatment response. Additionally, considering that APD treatment has been linked to an upregulation of orexin-A levels (Chen et al., 2022), we further utilized an overlapping sample of APD-free patients from our previous study (Chen et al., 2022) as a comparison group. Moreover, we investigated the correlation of orexin-A levels with the psychopathology and cognitive function of in clozapine-treated patients.
Methods
Setting
This cross-sectional study was conducted at Taipei City Psychiatric Center, Taipei City Hospital, from July 2011 to July 2019 after approval was obtained from the Research Ethics Committee (IRB Nos. TCHIRB-1000407 & TCHIRB-1020812).
Study participants
As an extension of our previous work, which involved 141 clozapine-treated and 36 APD-free patients who had been assessed by the18-item Brief Psychiatric Rating Scale (BPRS-18) for psychopathology, this study further recruited one APD-free patient and 21 patients treated by clozapine, comprising a total of 199 patients. Recruitment took place from either the outpatient department or inpatient wards. The inclusion criteria were as follows: (1) age 20–65 years; (2) a diagnosis of schizophrenia based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision criteria, confirmed by two senior psychiatrists. The APD-free group consisted of patients who had never taken APDs or had not taken them in the preceding 24 weeks. The clozapine-treated group comprised patients with TRS who had continuously used clozapine for at least 24 weeks before enrollment. TRS was defined as the presence of persistent moderate positive psychotic symptoms (Clinical Global Impression–Schizophrenia positive score ⩾4) after at least two trials of APDs with a chlorpromazine equivalent dose ⩾600 mg/day for ⩾6 weeks (Chan et al., 2020). Patients were excluded if they (1) had any other comorbid psychiatric diagnosis confirmed using the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998), including mood disorders, substance use disorders other than nicotine use disorder, neurodevelopmental disorders, or major neurocognitive disorders; or (2) had any other medical conditions such as seizures, brain tumors, or a history of severe traumatic injuries. Written informed consent was obtained from each participant. Demographic and clinical information, including age, sex, years of education, diagnoses, age of schizophrenia onset, illness duration, smoking status, and the dosage and duration of clozapine treatment, were collected from clinical interviews and medical records.
Assessment of psychopathology and definition of treatment response to clozapine
BPRS-18 was rated by a trained research assistant with a major in psychology. This scale is further divided into positive, negative, and general symptoms subscales (Kane et al., 1988). Treatment response was determined by the achievement of psychotic remission according to criteria from Andreasen et al. (2005), who defined remission as the presence of mild symptom intensity (i.e., 3 points or less) of representative items on the BPRS, namely grandiosity, suspiciousness, unusual thought content, hallucinatory behavior, conceptual disorganization, mannerism or posturing, and blunted affect. Clozapine-treated patients were categorized into the clozapine-responsive and clozapine-resistant groups based on their achievement of psychotic remission under clozapine treatment, following the definition from Veerman et al. (2016). The phenotypes of clozapine-response or clozapine-resistance were not defined until the BPRS assessment for all patients was completed. Both participants and the rater were kept unaware of the study hypothesis or whether the patients were categorized into clozapine-response or clozapine-resistant groups.
Cognitive function assessment
Cognitive function was evaluated in a subset of recruited clozapine-treated patients (N = 55) using the CogState Schizophrenia Battery (Cogstate Inc., New Haven, CT, USA). This computer-based battery cognitive assessment is composed of a series of standard neuropsychological tests for 11 cognition domains: psychomotor speed (detection task, DET), attention and vigilance (identification task, IDN), verbal learning (international shopping list task, ISLT), visual learning and memory (one card learning task, OCL), paired associate learning (continuous paired associate learning task, CPAL), verbal memory (ISLT: delayed recall, ISRL), visual memory (Groton maze learning task (GML): delayed recall, GMR), working memory (one-back task, ONB; and 2-back task, TWOB), executive function (GML), and social-emotional recognition (social-emotional cognition task, SEC). For DET and IDN, reaction times for correct responses were assessed and logarithmically transformed for normality, with higher scores indicating poorer performance. For ISLT and ISRL, the total number of correct responses was assessed, and higher scores indicated better performance. For CPAL, GML, and GMR, the total number of errors was assessed, with higher scores indicating poorer performance. OCL, ONB, TWOB, and SEC accuracy was assessed and arcsine-transformed for normality, with higher scores indicating better performance. This battery was previously validated in patients with schizophrenia (Pietrzak et al., 2009). Participants were required to complete the battery as quickly and accurately as possible within approximately 40 min.
Measurement of plasma orexin-A level
Venous blood samples were collected between 8:00 and 9:00 am after an overnight fast. Plasma was separated by centrifugation and was immediately frozen and stored at −80°C until analysis. Plasma orexin-A levels were analyzed using an extraction-free enzyme immunosorbent assay (Cat. No. EKE-003-30; Phoenix Pharmaceuticals, Belmont, CA, USA). The intra-assay coefficient of variation was <5%, and the kit had no cross-reactivity with any other substance, including orexin-B, Agouti-related protein, neuropeptide, alpha-melanocyte-stimulating hormone, and leptin. The minimum detectable amount of orexin-A was 0.17 ng/mL (provided by the manufacturer).
Metabolic parameters
As metabolic syndrome (MS) has been associated with orexin-A levels in patients with schizophrenia (Chen et al., 2019), we also assessed the MS factors for each patient so that we could assess the impact on orexin-A levels. MS was determined based on modified criteria from the 2005 National Cholesterol Education Program-Adult Treatment Panel III (Grundy et al., 2005).
Statistical analyses
Descriptive statistics were used to present the demographic, clinical, and metabolic characteristics of the participants. Logarithmic transformation was applied to data that did not meet the assumption of normality. Student’s t-test or analysis of variance was used to compare the continuous variables among different groups. Chi-squared tests were used to compare the categorical variables. In order to test the association between orexin-A levels and clozapine treatment response, multivariate logistic regression was used to assess the association between plasma orexin-A levels (the major exposure of interest) and treatment outcomes in clozapine-treated patients with adjustment for potential confounders including age (Hunt et al., 2015), sex, years of education, age of schizophrenia onset, dosage and duration of clozapine treatment (Chan et al., 2020), smoking history (Rajkumar et al., 2011), and the presence of MS or body mass index (BMI) (Bai et al., 2006). Furthermore, partial correlation was used to examine the correlations between orexin-A and the cognition parameters in clozapine-treated patients with adjustment for possible confounders, including age, sex, years of education, and clozapine dosage. Missing values were replaced by the median of other available values for continuous variables, resulting in conservative estimations. All p values in the statistical tests were two-sided, and p < 0.05 was considered statistically significant. All analyses were conducted using Stata version 15 (StataCorp LLC, College Station, TX, USA).
Results
Participants’ characteristics
Among 162 clozapine-treated patients with TRS, 62 (38.3%) of them met the criteria for clozapine-resistant schizophrenia. Table 1 presents the demographic and clinical characteristics of the APD-free, clozapine-responsive, and clozapine-resistant groups. APD-free patients exhibited a later onset of disease, a shorter duration of illness, longer educational years, and a lower rate of MS compared to the other two groups. Clozapine-responsive patients had lower scores on the BPRS total, positive, and general symptoms subscales compared to either APD-free or clozapine-resistant patients, and they also had lower scores on the negative symptoms subscale compared to clozapine-resistant patients. No significant differences were noted in age, sex distribution, smoking status, or BMI among the three groups.
Demographics and clinical characteristics among drug-free, clozapine-responsive and clozapine-resistant patients with schizophrenia (N = 199).
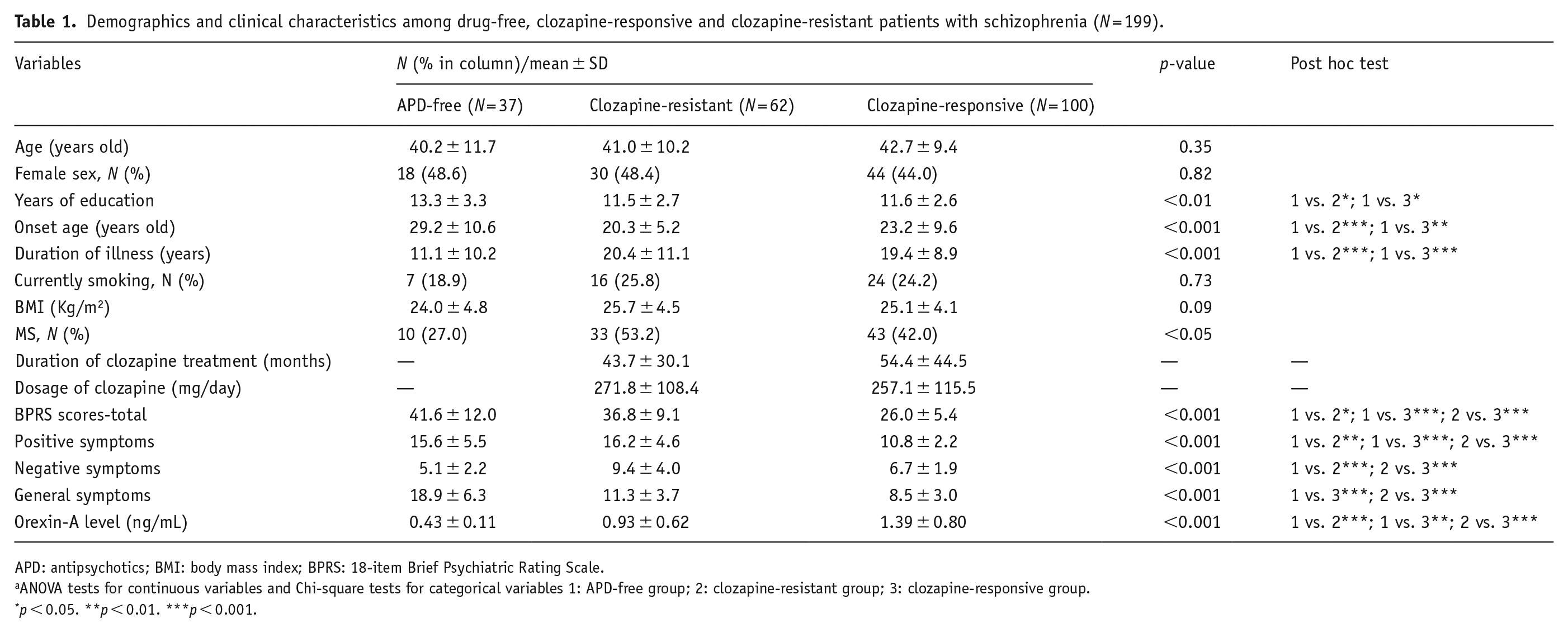
APD: antipsychotics; BMI: body mass index; BPRS: 18-item Brief Psychiatric Rating Scale.
ANOVA tests for continuous variables and Chi-square tests for categorical variables 1: APD-free group; 2: clozapine-resistant group; 3: clozapine-responsive group.
p < 0.05. **p < 0.01. ***p < 0.001.
Figure 1 illustrates the orexin-A levels and BPRS scores of three groups. We observed an ascending pattern in orexin-A levels: APD-free patients showed the lowest levels (0.43 ± 0.11 ng/mL), followed by clozapine-resistant patients (0.93 ± 0.62 ng/mL), and then clozapine-responsive patients (1.39 ± 0.80 ng/mL) (F(2,196) = 30.5, with post-hoc comparisons using the Games-Howell test showing significance for each pair of comparisons, all p < 0.001). In contrast, BPRS scores displayed an inverse trend: the APD-free group had the highest scores (41.6 ± 12.0), followed by the clozapine-resistant group (36.8 ± 9.1), and then the clozapine-responsive group (20.0 ± 5.4) (F(2,195) = 62.4, with post-hoc comparisons using the Games-Howell test showing significance for each pair of comparisons, namely APD-free versus clozapine-resistant, p < 0.05; drug-free versus clozapine-responsive, p < 0.001; clozapine-resistant versus clozapine-responsive, p < 0.001).
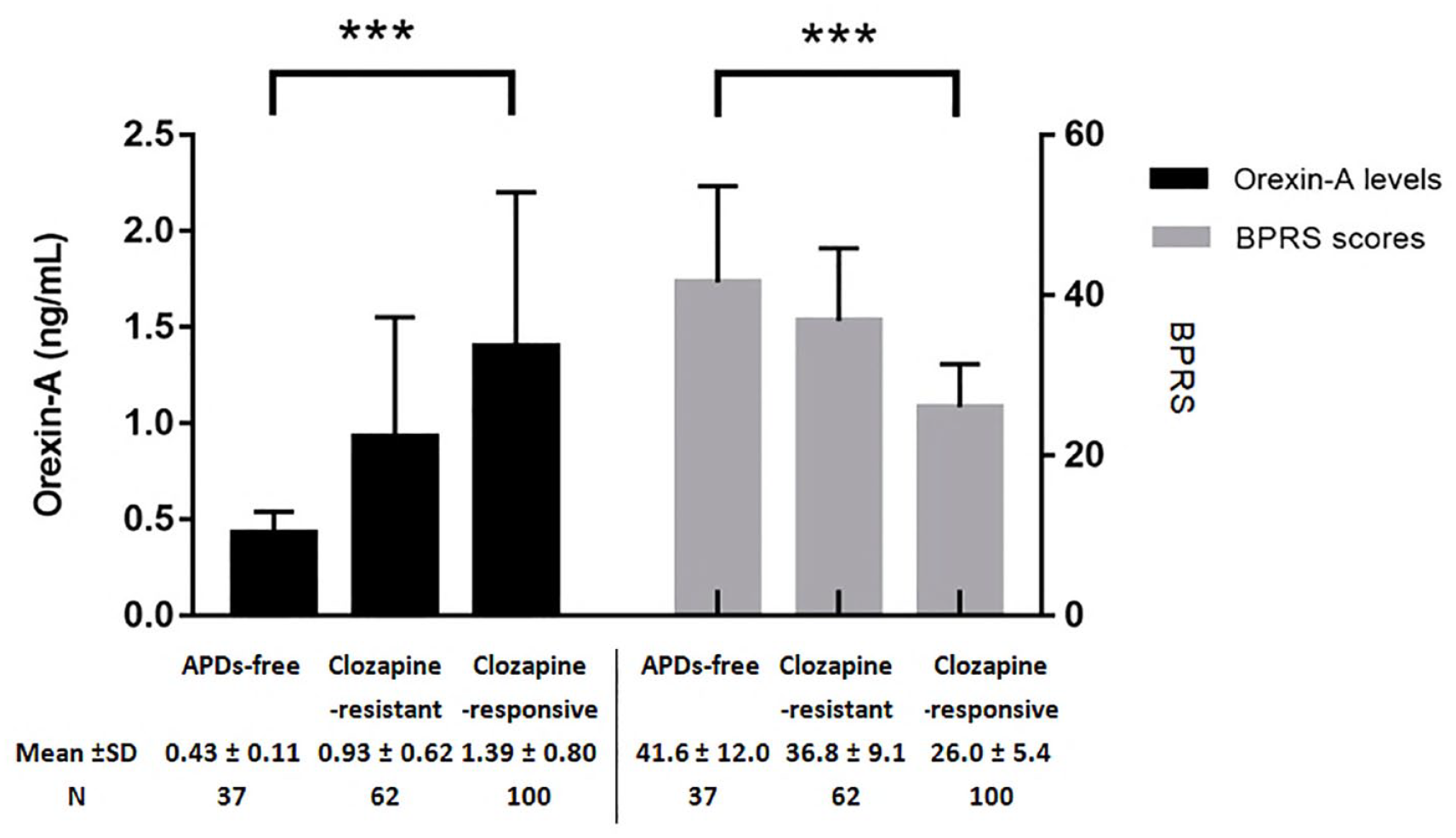
The comparison of plasma orexin-A levels and psychotic symptoms severity among APD-free, clozapine-resistant and clozapine-responsive patients with schizophrenia.
Association of orexin-A level with the clozapine response
Table 2 displays the association between treatment outcomes (response vs. resistance) and clinical characteristics, as determined using multivariate logistic regression adjusting for potential factors. Orexin-A level was the only variable significantly associated with clozapine treatment response, with higher levels showing an association with treatment response.
Association of demographics and clinical factors with treatment outcomes (response vs. resistance) in clozapine-treated patients (N = 162).
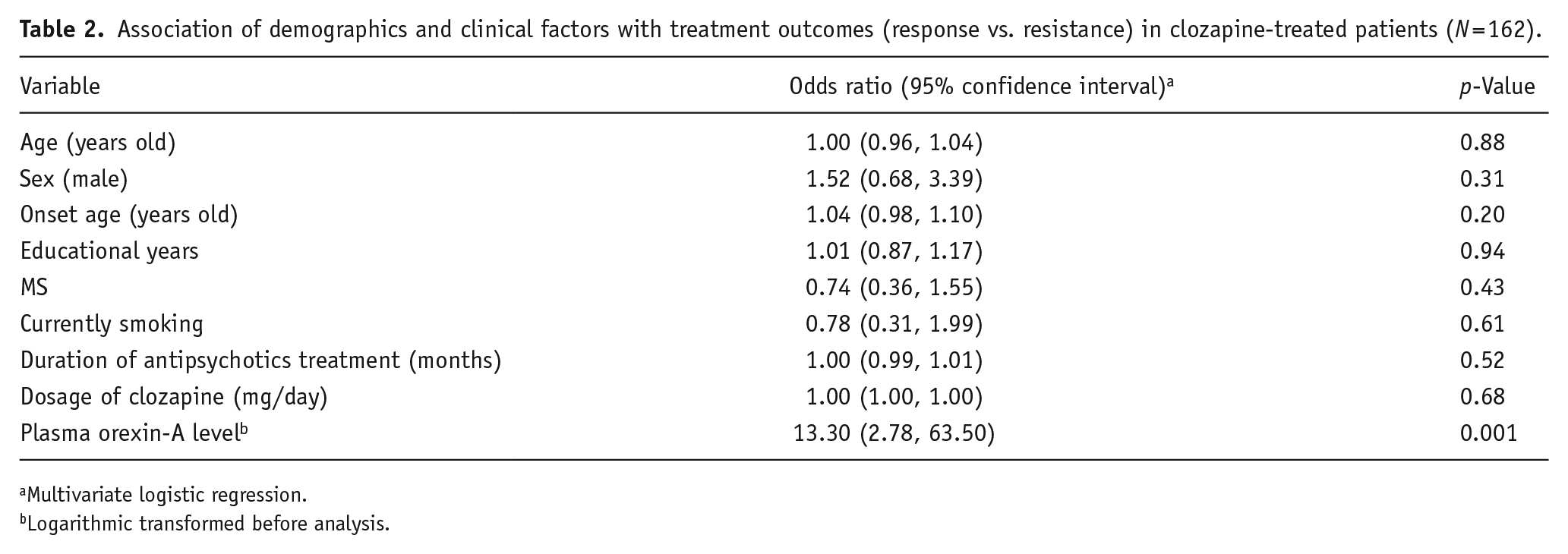
Multivariate logistic regression.
Logarithmic transformed before analysis.
Correlation of orexin-A levels with BPRS total and subscale scores
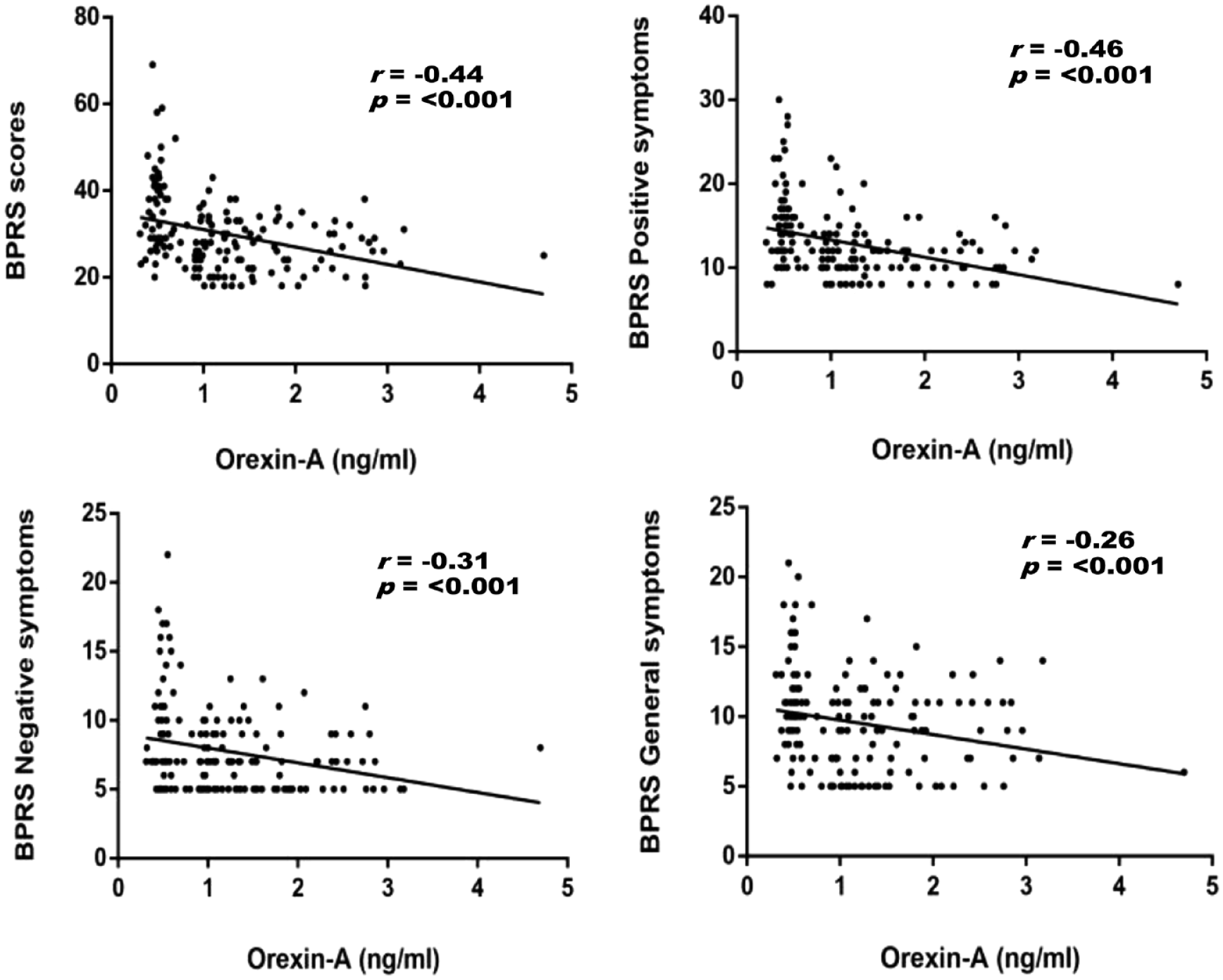
Figure 2 displays scatterplots illustrating the negative correlation between orexin-A levels and BPRS scores. Orexin-A levels were negatively correlated with BPRS total (r = −0.44, p < 0.001), positive symptom (r = −0.46, p < 0.001), negative symptom (r = −0.31, p < 0.001), and general symptom (r = −0.26, p < 0.001) subscale scores. Furthermore, in Table 3, orexin-A levels were negatively correlated with BPRS total scores and positive, negative, and general symptoms subscales (all p < 0.001) after adjusting for all confounding variables by linear regression. This suggests that lower orexin-A levels were independently associated with a poorer psychopathological profile in clozapine-treated patients. Additionally, we observed that the onset age of the disease was negatively associated with the total and general symptoms subscale scores of BPRS (p < 0.01).
Correlations between orexin-A levels and BPRS scores in clozapine-treated patient.
Explainable factors for psychotic symptom severity in patients with schizophrenia treated by clozapine using linear regression (N = 162).
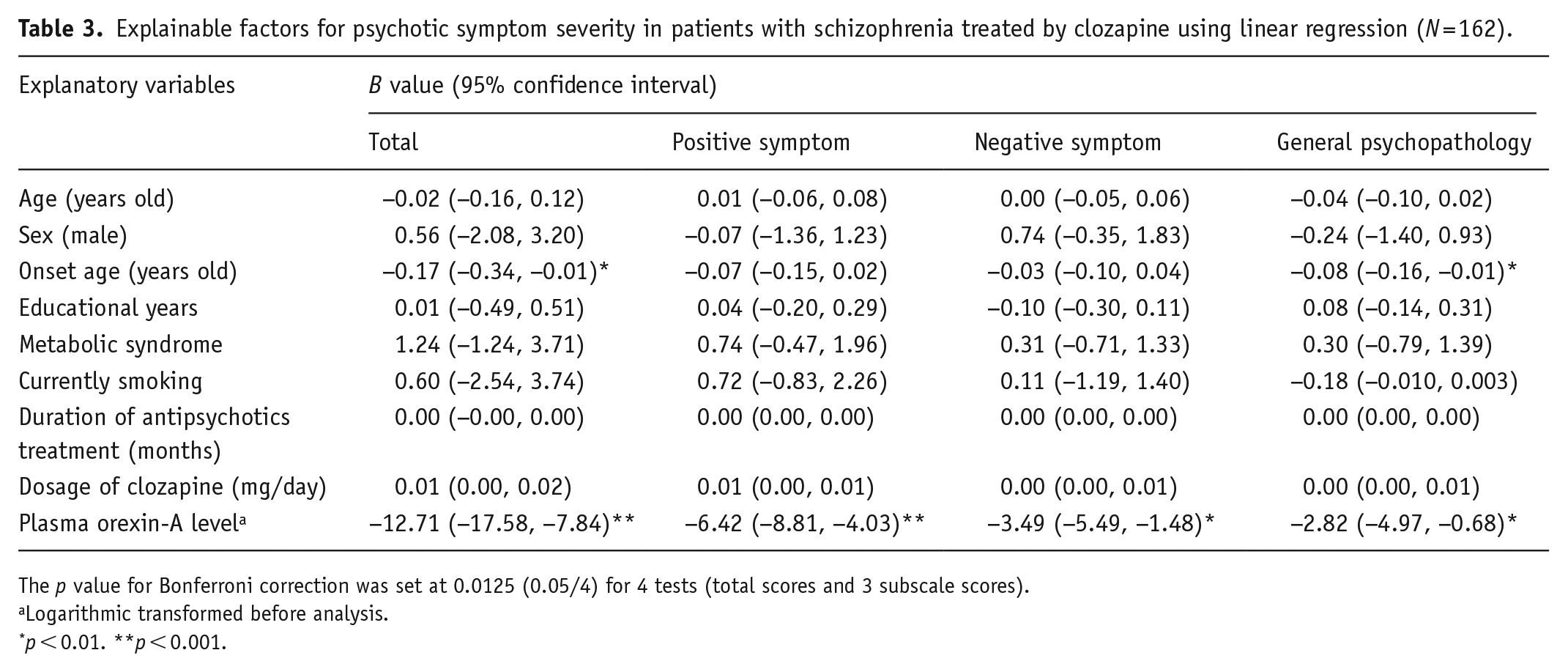
The p value for Bonferroni correction was set at 0.0125 (0.05/4) for 4 tests (total scores and 3 subscale scores).
Logarithmic transformed before analysis.
p < 0.01. **p < 0.001.
Correlation of orexin-A levels with cognitive function
Cognitive function was assessed in a subset of patients who completed the test (n = 55), with 22 (40.0%) belonging to the clozapine-responsive group. The clozapine-resistant group exhibited higher psychotic symptom severity, lower orexin-A levels, and poorer cognitive performance in verbal memory (ISRL, 18.7 ± 5.1 vs. 15.0 ± 5.8; t = –2.4, p < 0.05) and social-emotional recognition (SECT, 1.06 ± 0.29 vs. 0.86 ± 0.28; p < 0.05) (Supplemental Table 1).
Table 4 illustrates the correlation of orexin-A levels with cognitive function. We found a positive correlation of orexin-A levels with verbal memory (ISRL, r = 0.35, p < 0.05), visual learning and memory (OCL, r = 0.33, p < 0.05), and working memory (TWOB, r = 0.36, p < 0.01) after adjusting for age, sex, years of education, and clozapine dosage. No significant correlations were observed between orexin-A levels and performance in attention (IDN, r = −0.13, p = 0.37), psychomotor function (DET, r = −0.20, p = 0.16), paired associate learning (CPAL, r = −0.27, p = 0.06), verbal learning (ISL, r = 2.38, p = 0.08), visual memory (GMR, r = 0.12, p = 0.41), executive function (GML, r = −0.00, p = 0.98), working memory (ONB, r = 0.16, p = 0.28), or emotional recognition (SECT, r = 0.17, p = 0.22).
Correlations between orexin-A levels and cognitive function in clozapine-treated patients with schizophrenia (N = 55).
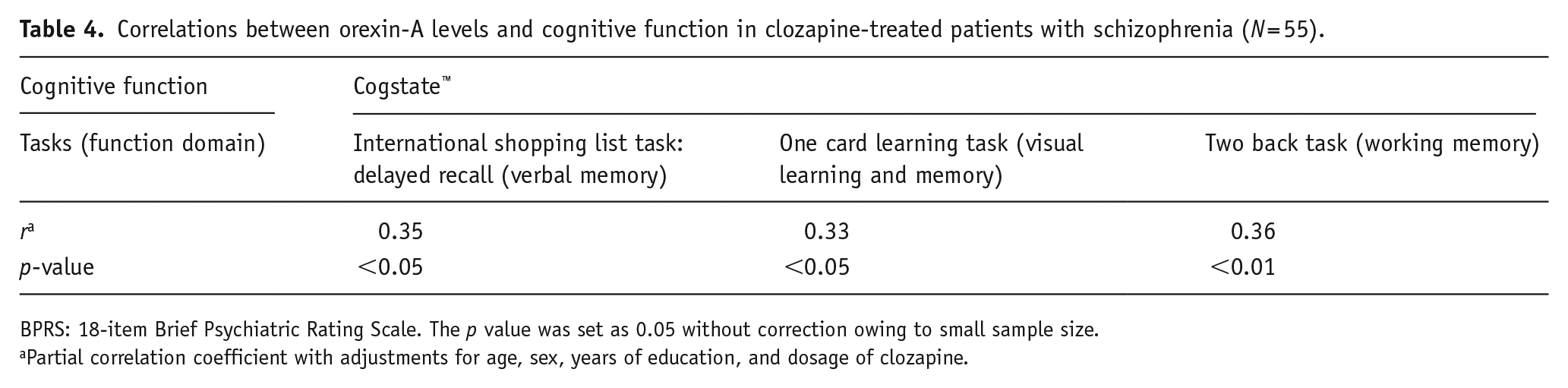
BPRS: 18-item Brief Psychiatric Rating Scale. The p value was set as 0.05 without correction owing to small sample size.
Partial correlation coefficient with adjustments for age, sex, years of education, and dosage of clozapine.
Discussion
As previously shown in a partially overlapping sample, we found patients under clozapine treatment had higher orexin-A levels than APD-free patients (Chen et al., 2022). To our knowledge, this study is the first to show the clozapine-responsive group had significantly higher orexin-A levels than clozapine-resistant group. In line with it, the regression model demonstrated that higher orexin-A levels were associated with clozapine response. In addition, the levels were negatively correlated with the BPRS total and all subscale scores but positively correlated with cognitive function in relation to verbal memory, visual learning and memory, and working memory. Collectively, these results suggest that orexin-A may play a role in the response of patients to clozapine treatment.
Previous reports have indicated that orexin signaling is involved in the effects of clozapine. For example, orexin neurons that project to the prefrontal cortex (PFC) are strongly activated by clozapine (Deutch and Bubser, 2007; Fadel et al., 2002). An in vitro study revealed that D1-like receptor agonists induce excitatory orexin neuron activity (Linehan et al., 2019). Because clozapine has high D1 agonistic affinity (Ahlenius, 1999), it is likely that this agent increases the activity of orexin neurons and thus regulates its expression. The effects of clozapine on the PFC may be blocked by orexin antagonists (Deutch and Bubser, 2007), providing further support that the clozapine response is, at least in part, mediated by the orexin system.
We found clozapine-treated patients with lower orexin-A levels had a higher severity of positive symptoms. Although the underlying mechanisms are not clear, this observation might be explained by the enhanced effect of orexin on parvalbumin-labeled (PV+) inhibitory fast-spiking GABAergic interneurons. The hypofunction of N-methyl-D-aspartate receptors (NMDARs) is considered to be a potential mechanism underlying TRS. Hypofunction of NMDARs on PV+ fast-spiking GABAergic interneurons in the cortex and hippocampus decreases GABAergic inhibition of downstream glutamatergic pyramidal neurons, which in turn leads to excessive glutamate release (Nakazawa et al., 2017) as well as downstream hyperdopaminergic activity (Grace and Gomes, 2019). Preclinical studies have shown that the effects of clozapine or electroconvulsive therapy on TRS are associated with restored upstream GABAergic inhibition (Kaster et al., 2015) and attenuated downstream glutamate release (Gillespie et al., 2017). In line with these findings, animals supplemented with orexin-A have shown activated PV+ fast-spiking GABAergic interneurons in the hippocampus (Selbach et al., 2004; Wu et al., 2002) and the PFC (Aracri et al., 2015; Usui et al., 2019). Taken together, these observations indicate a beneficial role of orexin-A in counteracting the dysfunction of GABAergic interneurons and downstream hyperglutaminergic activity. This may explain the negative correlation between orexin-A levels and the severity of positive symptoms in the current study.
Accumulating evidence suggests that the negative symptoms of schizophrenia are linked with hypodopaminergic function and glutamate deficiency with NMDAR function abnormality in the PFC as well as the nucleus accumbens and ventral tegmental area (VTA), which are implicated in reward and motivation (Correll and Schooler, 2020). Preclinical studies have reported that orexin-A infusion enhances DA efflux in the VTA (Vittoz et al., 2008) and PFC (Vittoz and Berridge, 2006), and influences arousal and affect regulation. In addition, orexin-A potentiates excitatory NMDAR action in DA neurons in the VTA (Borgland et al., 2006) and PFC (Aracri et al., 2015), and also increases glutamate efflux in the PFC (Calva et al., 2018). Furthermore, reduced orexin-A levels in the VTA and mPFC (Nocjar et al., 2012) or the blockade of orexin neuron signals to GABAergic neurons in the ventral pallidum (Ji et al., 2019) have been associated with anhedonia and social avoidance. These findings collectively support the observation in our study that patients with lower orexin levels have more significant negative symptoms.
Studies have indicated that patients with TRS have greater deficits in verbal ability, verbal memory, learning, and visual memory than patients who respond adequately to first-line APDs (Gillespie et al., 2017). In our study, clozapine-resistant patients had even worse verbal memory and social emotional recognition than clozapine-responsive patients. Of note, we found orexin-A level was positively correlated with the most common cognitive deficits in patients with TRS, namely verbal, visual, and working memory. A preclinical study revealed that intranasal orexin-A administration increased c-fos, a marker of neuronal activation, in the PFC and the brainstem pedunculopontine nucleus, which are involved in cognition, arousal, and attention. Orexin-A supplementation also increased glutamate and acetylcholine efflux, which are beneficial for attention, learning, and memory in rats (Calva et al., 2018). In addition, orexin-A produces excitatory effects on hippocampal neurons through orexin receptor type 1 activity (Chen et al., 2017), enhances long-term potentiation (Wayner et al., 2004) and neurogenesis in the dentate gyrus (Zhao et al., 2014), and generates gamma band oscillations (Vassalli and Franken, 2017). Hippocampal projections to the PFC are critical for cognitive performance, especially memory, and the formation of gamma band oscillations is crucial for cognitive processes (Gonzalez-Burgos et al., 2015). Accordingly, research has shown that orexin deficiency may impair spatial memory, learning, and social memory, whereas orexin-A supplementation can restore these impairments (Yang et al., 2013; Mavanji et al., 2017). Some clinical observations have shown that orexin-A levels are positively correlated with favorable cognitive function in patients with anorexia nervosa (Steward et al., 2019), Alzheimer’s disease (Shimizu et al., 2020), and schizophrenia (Chien et al., 2015). Our result further suggests that orexin-A plays a role in the cognitive function of patients with TRS.
Limitations
This study had several limitations. First, because TRS is a distinct subtype of schizophrenia, caution should be exercised when generalizing the current findings to other patients with schizophrenia. Second, the mean dosage of clozapine in our clozapine-resistant schizophrenia was 271.8 ± 108.4 mg/day, less than the average dose 300–600 mg/day in Caucasians to reach the therapeutic range (350 ng/mL) (Wagner et al., 2020). A recent paper reported that Asian patients require only half of the clozapine dose prescribed for Caucasians (approximately 250 mg/day for female non-smokers to 550 mg/day for male smokers), with the dose needed for clinical response ranging between 150 mg/day for female non-smokers to 300 mg/day for male smokers because of a higher rate of genetic poor metabolism for clozapine (de Leon et al., 2020). However, we did not measure the plasma levels of clozapine and its metabolites, and clozapine treatment compliance was judged based on patient reports, which may not be reliable. To enhance the reliability, drug compliance was confirmed by closed family member. In addition, many confounding factors, such as genetic, demographic, and environmental factors (Sanguesa et al., 2022), which affect clozapine metabolism were not taken into consideration in the current study. Therefore, the possibility of poor drug compliance or individual differences in clozapine metabolism, which could affect treatment response, cannot be ruled out. Third, the sample size was relatively small, especially patients who received cognitive function tests. Fourth, our previous work suggested a relationship between MS and orexin-A levels. In the present study, we did not find differences in the rate of MS in both clozapine groups and any significant effect from metabolic status in the regression model. However, it should be noted that various physiological functions, such as sleep, energy homeostasis, and stress regulation (Strawn et al., 2010), which have been implicated in orexin-A expression, were not assessed. Fifth, the causal relationship between orexin-A levels and treatment response could not be established in the current cross-sectional study. Additionally, the definition of clozapine treatment response is based on the achievement of psychotic remission, using criteria from Andreasen et al. (2005), rather than the changes in BPRS. Furthermore, lacking data on orexin-A levels prior to clozapine treatment also precludes us from establishing whether higher orexin-A levels may exist in the clozapine-responsive group. Prospective studies are required to investigate whether orexin-A levels constitute a state or trait marker of clozapine response and to accurately identify treatment response. Finally, clozapine has many pharmacological actions, and its impact on orexin may be unrelated to its therapeutic effect.
In conclusion, our findings suggest that orexin-A may have a role in influencing the treatment response to clozapine. Specifically, clozapine-resistant patients had significantly lower orexin-A levels than clozapine-response patients. The orexin-A levels were negatively correlated with severity of psychopathology and positively correlated with cognitive performance in clozapine-treated patients. Our results also highlight the possibility that orexin-A may help determine the probability of treatment responses or resistance to clozapine. Researchers have recommended the early initiation of clozapine in the disease course of TRS to reduce the rate of treatment resistance to clozapine (Chan et al., 2020; Griffiths et al., 2021). More prospective studies are necessary to determine whether orexin-A is a trait or a state marker of clozapine treatment response in patients with TRS. Additionally, exploring the possibility of using orexin-A supplementation as a therapeutic avenue to enhance clozapine responses requires further investigation.
Supplemental Material
sj-docx-1-jop-10.1177_02698811231225610 – Supplemental material for Higher orexin-A levels are associated with treatment response to clozapine in patients with schizophrenia: A cross-sectional study
Supplemental material, sj-docx-1-jop-10.1177_02698811231225610 for Higher orexin-A levels are associated with treatment response to clozapine in patients with schizophrenia: A cross-sectional study by Po-Yu Chen, Chih-Chiang Chiu, Chin-Kuo Chang, Mong-Liang Lu, Cho-Yin Huang, Chun-Hsin Chen and Ming-Chyi Huang in Journal of Psychopharmacology
Footnotes
Acknowledgements
We thank the Taipei Institute of Pathology for their technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science and Technology, Taiwan (MOST 109-2314-B-532-005, 110-2314-B-532-004, 111-2314-B-532 -004 -MY3 [PYC]; 110-2314-B-532-005-MY3 [MCH]; 109-2314-B-038-084, 111-2314-B-038-062-MY2 [CHC]); Taipei City Government (TPECH 11101-62-031, 112-01-62-202 [PYC]; 11301-62-016 [MCH]); Taipei City Hospital, Taiwan (TPCH 111-57, 112-55 [PYC]; 112-52, 113-56 [MCH]); and Taipei Institute of Pathology (TIP-110-003 [PYC]), Taiwan. All funding resources had no further role in the study design; collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.