
Abstract
Objective:
Utilizing two-sample Mendelian randomization (TSMR) analysis, this study aims to explore the potential bidirectional causal relationship between common nonsteroidal anti-inflammatory drugs (paracetamol, ibuprofen, aspirin) and major depression (MD) from a genetic standpoint.
Methods:
We employed summarized data from a Genome-Wide Association Study (GWAS) of European populations. The inverse variance weighted (IVW) method was used for TSMR analysis; outcomes were evaluated based on p-value, OR (Odds Ratio), and 95% confidence interval (95% CI).
Results:
From a genetic perspective, the study found that the use of paracetamol and ibuprofen increased the risk of MD (IVW (MRE): OR = 2.314, 95% CI: 1.609–3.327; p = 6.07E-06) and (IVW (MRE): OR = 2.308, 95% CI: 1.780–3.653; p = 0.002), respectively. No significant causal relationship was found between aspirin and MD (p > 0.05). Reverse TSMR analysis found that MD increased the genetic predisposition to use paracetamol, ibuprofen, and aspirin (IVW (MRE): OR = 1.042, 95% CI: 1.030–1.054, p = 3.07E-12), (IVW (FE): OR = 1.015, 95% CI: 1.007–1.023, p = 1.13E-04), (IVW (MRE): OR = 1.019, 95% CI: 1.009–1.030, p = 4.22E-04), respectively. Other analytical methods and sensitivity analyses further supported the robustness and reliability of these findings.
Conclusion:
This study provides preliminary genetic evidence through bidirectional TSMR analysis that MD increases the genetic predisposition to use paracetamol, ibuprofen, and aspirin, aiding clinicians in devising preventive strategies against the misuse of non-steroidal anti-inflammatory drugs. Moreover, we found that the use of paracetamol and ibuprofen increases the risk of MD, whereas aspirin did not. This suggests a crucial clinical implication: clinicians treating MD patients could opt for the relatively safer aspirin over paracetamol and ibuprofen.
Introduction
According to data from the World Health Organization, depression affects approximately 350 million people globally, becoming a major cause of both mental and physical disability, as well as a significant component of the global burden of disease (WHO, 2021). Major depression (MD) is a severe mental health issue that significantly negatively affects the quality of life, social capabilities, and physical health of patients. It is widely considered one of the most common and troubling mental health issues globally and is a focus in the field of public health (Monroe and Harkness, 2022). Research by Liu et al. (2020) shows that over the past 30 years, the number of people affected by MD worldwide has increased by almost 50%, currently affecting over 264 million people.
Currently, the main clinical treatment for MD is antidepressant medication. However, even after a full course of antidepressant treatment, approximately one-third or more patients fail to respond effectively, and the therapeutic effects of the medication may take an extended period to manifest (Du et al., 2023; Khan et al., 2017; Li, 2021). In addition, patients undergoing antidepressant therapy often experience adverse reactions such as gastrointestinal discomfort and decreased libido, which affects their compliance with the treatment (Marwaha et al., 2023). Therefore, there is an urgent need for new drug treatment strategies to prevent or alleviate MD.
Despair and affective temperament are considered predictors of MD, with patients who have higher levels of despair reporting moderate to severe depression more frequently (87.1% vs 38.9%; p < 0.001; Pompili et al., 2012). Some hypotheses suggest that inflammation is one of the risk factors for depression (Jeon and Kim, 2017). Elevated levels of inflammatory cytokines, including interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and C-reactive protein (CRP), are observed in the bodies of MD patients (Bahrini et al., 2016; Kappelmann et al., 2021; Wang et al., 2019). In addition, the study found that neutrophils, platelets, mean platelet volume, the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and monocyte-to-lymphocyte ratio may not only be important predictors of MD but also predictors of hypomania (Fusar-Poli et al.,2021). Regulating these cytokine levels may help improve depressive symptoms. Some research has found that non-steroidal anti-inflammatory drugs (NSAIDs) may exhibit antidepressant effects by reducing inflammatory cytokine levels. Observational studies indicate that NSAIDs can effectively treat and improve symptoms of depression, cognitive function, and physical discomfort in patients (Bai et al., 2020; Fourrier et al., 2018; Köhler et al., 2014; Liu and Fu, 2020). However, other studies do not support the efficacy of NSAIDs in treating depression, arguing that they are irrelevant to MD (Eyre et al., 2015; Molero et al., 2019). The reason for these contradictory conclusions may be that traditional observational epidemiological methods, although useful for exploring the potential relationship between NSAIDs and MD, are inherently susceptible to potential confounding factors and reverse causality, making causal inference difficult.
Mendelian randomization (MR) is a statistical method that uses single nucleotide polymorphisms (SNPs) as instrumental variables (IVs) to overcome the biases caused by confounding and reverse causality in traditional observational epidemiological methods (Davey Smith et al., 2020; Smith et al., 2003). Leveraging the large amount of data from Genome-Wide Association Study (GWAS) databases, MR is widely applied to infer causal relationships between exposure and outcome variables.
Currently, both domestic and international understanding of the causal relationship between NSAIDs and MD is limited. No studies using MR methods have been conducted to explore the causal relationship between commonly used NSAIDs and MD. Therefore, this study uses two-sample Mendelian randomization (TSMR) based on GWAS databases to explore the bidirectional causal relationship between common NSAIDs (paracetamol, ibuprofen, aspirin) and MD. Through this research, we aim to better understand the therapeutic effects of NSAIDs and provide clinical references for the treatment of MD.
Materials and methods
Study design
This study employs a TSMR analysis to assess the bidirectional causal relationship between commonly used NSAIDs (paracetamol, ibuprofen, aspirin) and MD. Using publicly available GWAS summary databases, three commonly used NSAIDs—paracetamol, ibuprofen, and aspirin—are selected as exposure variables, with MD as the outcome variable. In addition, a reverse TSMR analysis is conducted with MD as the exposure variable and paracetamol, ibuprofen, and aspirin as outcome variables.
For MR analysis, three key assumptions must be satisfied (Sekula et al., 2016): relevance assumption: SNPs serving as instrumental variables (IVs) should be strongly associated with the exposure variable. Independence assumption: IVs should not be related to any potential confounding variables. Exclusion assumption: IVs should affect the outcome variable solely through the exposure variable.
Data sources
The genetic data for both the exposure and outcome variables in this study are sourced from the GWAS database (https://gwas.mrcieu.ac.uk). The genetic data for paracetamol, ibuprofen, and aspirin are obtained from European populations within the UKBiobank. Specifically, the data for paracetamol consist of 462,933 samples, including 85,782 cases and 377,151 controls. The data for ibuprofen consist of 462,933 samples, including 57,738 cases and 405,195 controls. The data for aspirin consist of 457,547 samples, including 64,534 cases and 393,013 controls.
The data for MD are sourced from Howard et al. (2019), comprising 500,199 samples from European populations, including 170,756 cases and 329,443 controls. The diagnosis of MD is primarily based on self-reported depressive symptoms coupled with related impairments, as well as MD identified from hospital records (Howard et al., 2018). In addition, some data are derived from structured clinical interviews and other content based on broader criteria (Wray et al., 2018), Table 1.
Basic information of sample data.

Selection of instrumental variables
We have selected SNPs that are closely related to the exposure variables (paracetamol, ibuprofen, aspirin, and MD) and meet the following criteria as instrumental variables (IVs): For MD-related SNPs, we select those with genome-wide significance (p < 5E-08). However, since there are few SNPs related to paracetamol, ibuprofen, and aspirin with genome-wide significance (p < 5E-08), we select SNPs with genome-wide significance at a relaxed threshold (p < 5E-06). Eliminate SNPs with linkage disequilibrium (r2 < 0.001, clumping distance = 10,000 KB). Exclude SNPs associated with confounding variables. All SNPs must be screened through F-statistics to avoid weak instrumental variable bias, with an F-value greater than 10 serving as a stability indicator. The formula for F is F = [(N − K − 1)/K] * [R2/(1 − R2)], where N is the sample size of the exposure variable, K is the number of IVs, and R2 is the proportion of exposure variance explained by the IVs (Bowden et al., 2016).
Statistical analysis
The study primarily employs the inverse variance weighted (IVW) method for analysis, which yields robust results when horizontal pleiotropy is not present. Weighted median, weighted mode, and MR Egger are also used as supplementary methods to check for robustness. Horizontal pleiotropy is detected through the ME Egger intercept. If p > 0.05, the data show no horizontal pleiotropy, making the results obtained through IVW robust. Heterogeneity among IVs is analyzed through Cochran’s Q-test. If heterogeneity is not significant (p > 0.05), a fixed-effects IVW method is used. If heterogeneity is significant (p < 0.05), a multiplicative random-effects IVW method is applied to minimize bias due to heterogeneity (Wang et al., 2023). Furthermore, to ensure the reliability of the overall effect, a “leave-one-out” sensitivity analysis is conducted. One SNP is excluded at a time, and the MR analysis effect of the remaining SNPs is calculated to assess the stability of the TSMR analysis results. To interpret the results more intuitively, this study uses the odds ratio (OR) and the 95% confidence interval (95% CI) as effect indicators. A p-value less than 0.05 is considered statistically significant. All analyses are conducted using R (version 4.0.3) and the R package “TwoSampleMR” (version 0.5.5) (Gibran et al., 2018).
Results
Results of IV selection
According to the criteria, we have separately screened 74, 34, and 55 SNPs that are closely related to the exposure factors, paracetamol, ibuprofen, and aspirin, respectively, to serve as IVs affecting the outcome factor MD. In addition, 50 SNPs were selected that are closely related to the exposure factor MD to serve as IVs. Among these, 47 affect the outcome factors, paracetamol and aspirin, and 44 affect the outcome factor, ibuprofen (Figure 1). Simultaneous F-statistic results show that the F-values for SNPs related to paracetamol (20.905–90.389), ibuprofen (20.883–61.840), and aspirin (29.882–120.913) are all greater than 10. Likewise, the F-values for SNPs related to MD (30.250–78.449) are all greater than 10. This suggests that there is no weak IV bias, making the study data reliable.
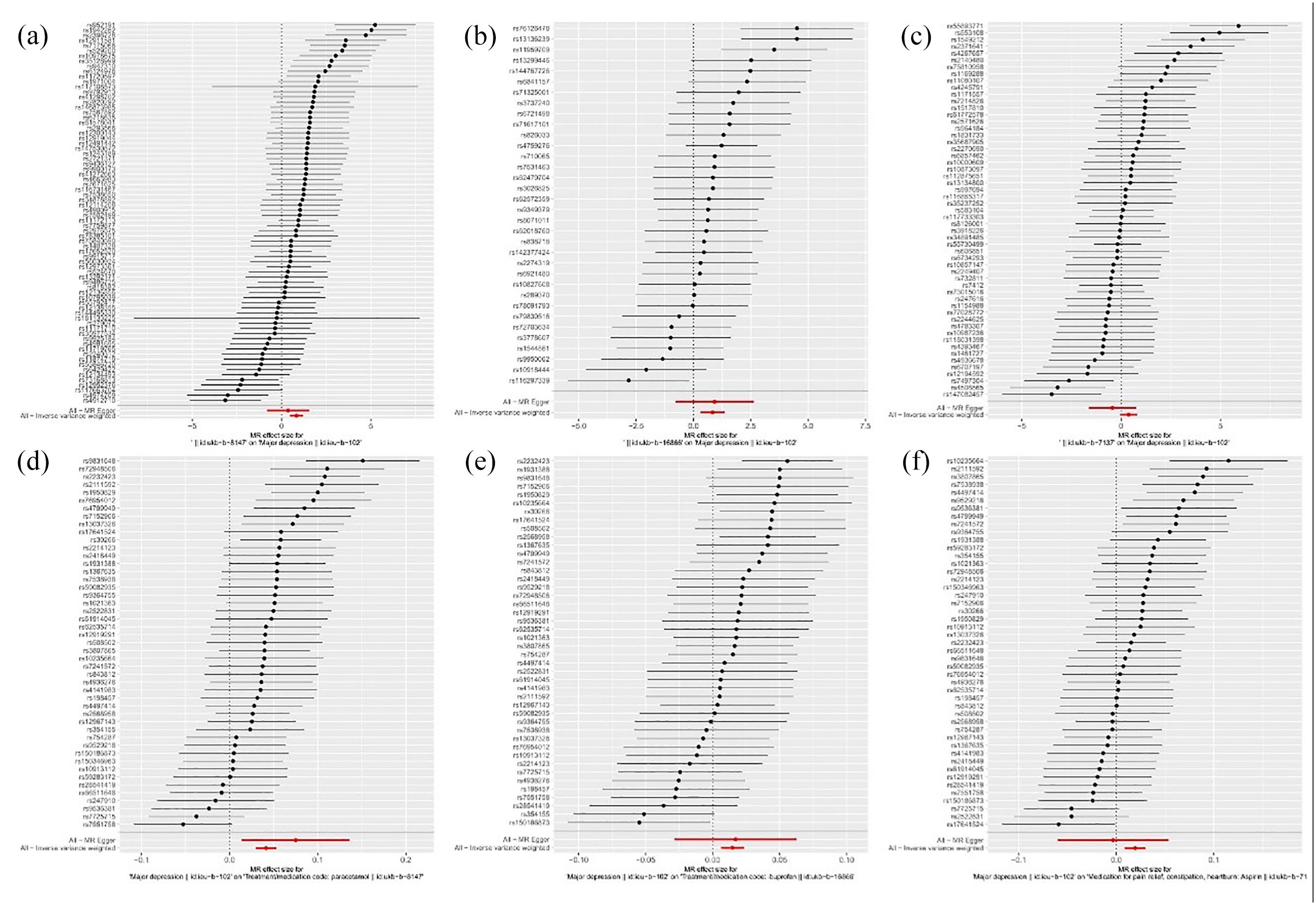
Forest plot of TSMR analysis. (a) Paracetamol and MD. (b) Ibuprofen and MD. (c) Aspirin and MD. (d) MD and paracetamol. (e) MD and ibuprofen. (f) MD and aspirin.
Results of heterogeneity and pleiotropy tests
The ME Egger intercept test shows no presence of pleiotropy (p > 0.05), indicating that the results obtained by the IVW method are robust and reliable. Thus, this study primarily employs the IVW method for analysis. Cochran’s Q heterogeneity test suggests that, apart from the analysis of MD and ibuprofen which showed no heterogeneity (p > 0.05), the rest showed significant heterogeneity (p < 0.05). Therefore, the TSMR analysis for MD and ibuprofen employs the IVW (FE) method, while others use the IVW (MRE) method for TSMR analysis (see Table 2).
Heterogeneity and pleiotropy tests.
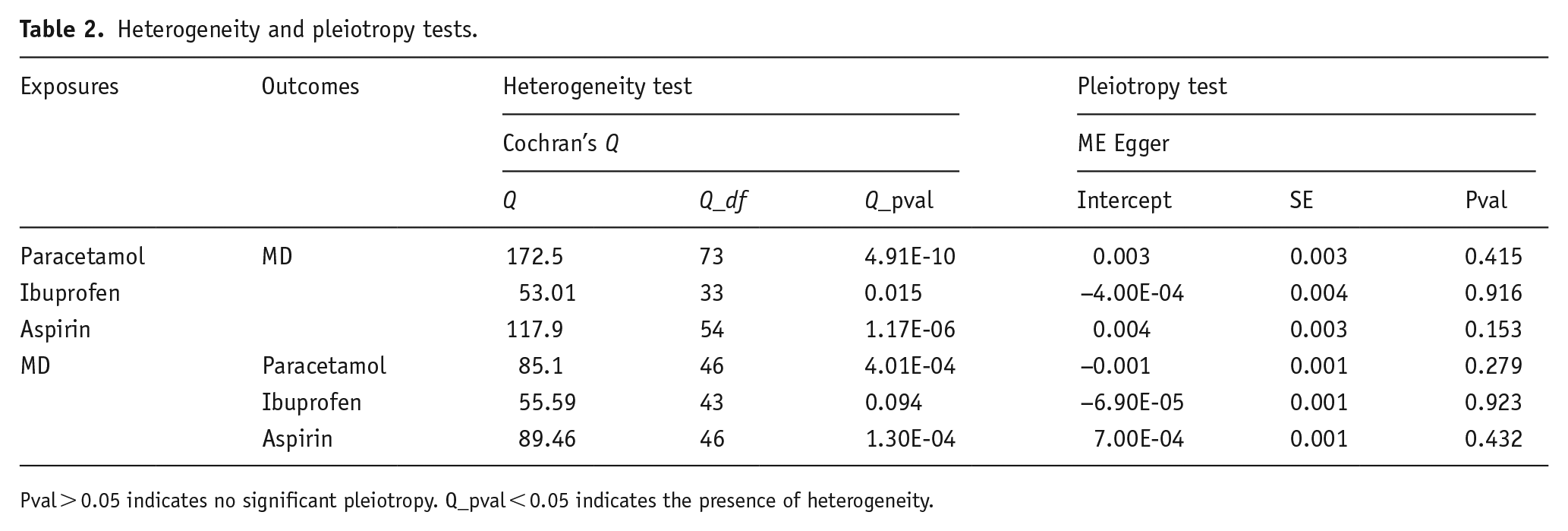
Pval > 0.05 indicates no significant pleiotropy. Q_pval < 0.05 indicates the presence of heterogeneity.
Causal relationship between paracetamol, ibuprofen, aspirin, and MD
The IVW (MRE) results show a significant positive correlation between paracetamol and MD. Genetically, the use of paracetamol increases the risk of MD (OR = 2.314, 95% CI: 1.609–3.327; p = 6.07E-06 < 0.05). The weighted median and weighted mode methods (p < 0.05) also indicate a significant positive correlation between the two, and all four TSMR analysis methods point in the same positive direction, further validating their positive relationship (Figures 2 and 3(a)).
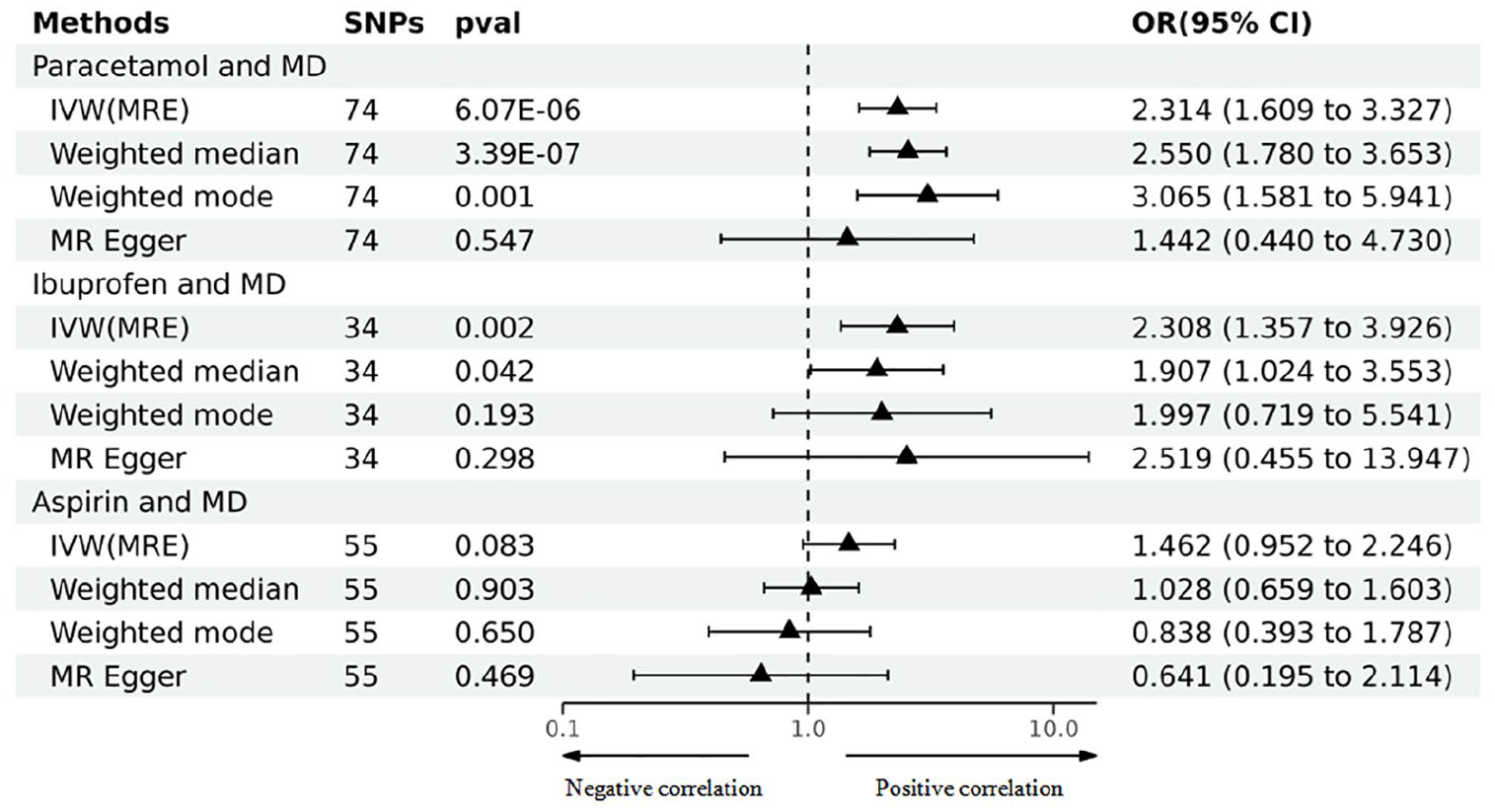
TSMR analysis results for paracetamol, ibuprofen, aspirin, and MD.
The IVW (MRE) results display a significant positive correlation between ibuprofen and MD. From a genetic perspective, the use of ibuprofen increases the risk of MD (OR = 2.308, 95% CI: 1.780–3.653; p = 0.002 < 0.05). The weighted median method (p < 0.05) also reveals a significant positive relationship between the two, and all four TSMR analysis methods consistently indicate a positive direction, further substantiating their positive relationship (Figures 2 and 3(b)).
However, the results from IVW (MRE) and the other three methods all show that the causal relationship between Aspirin and MD is not significant (p > 0.05) (Figures 2 and 3(c)).
Causal relationship between MD and paracetamol, ibuprofen, aspirin
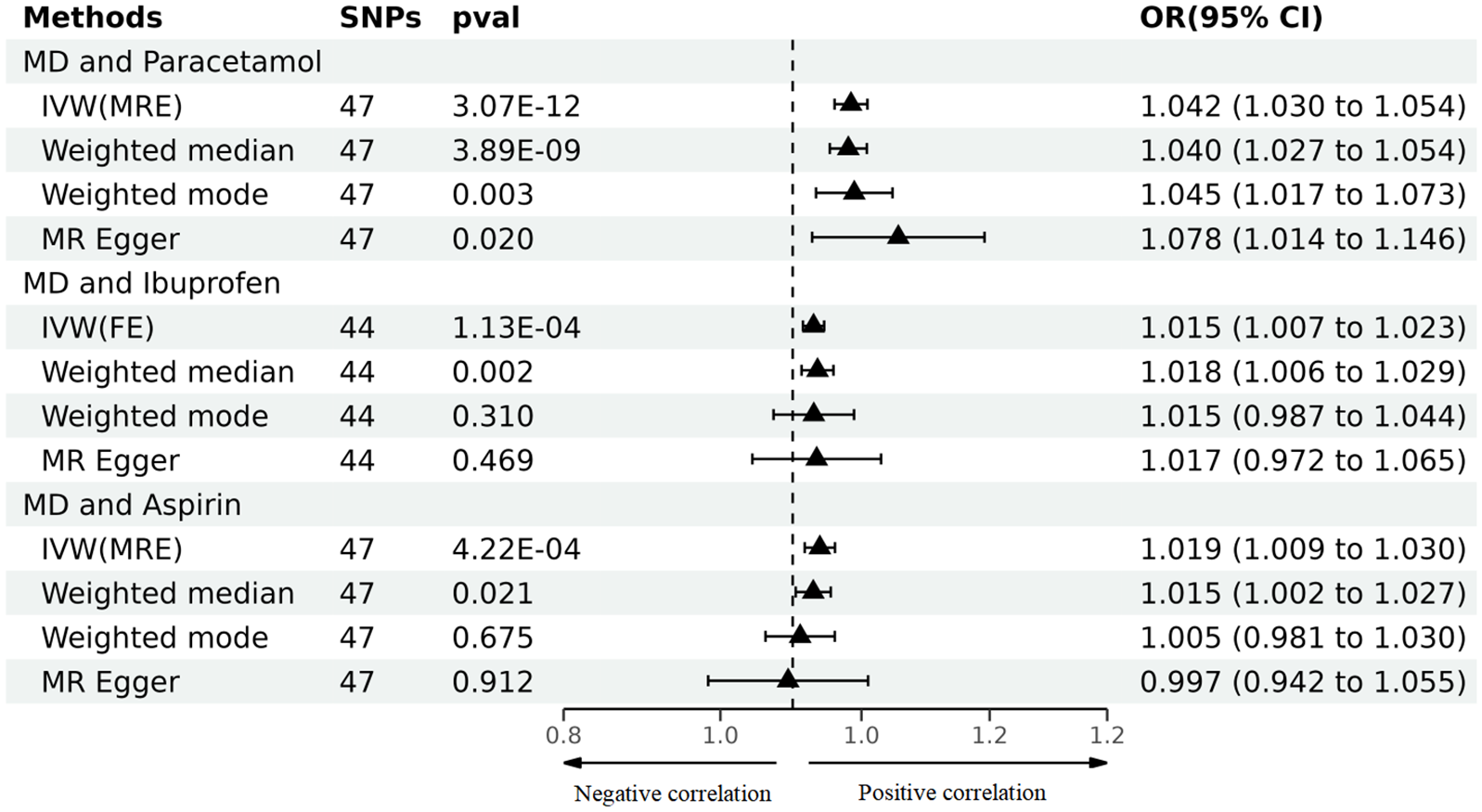
We conducted a reverse TSMR analysis. The IVW (MRE) results show a significant positive correlation between MD and paracetamol. MD increases the genetic predisposition risk of using paracetamol (OR = 1.042, 95% CI: 1.030–1.054, p = 3.07E-12 < 0.05). In addition, the weighted median, weighted mode, and MR Egger methods (p < 0.05) all indicate a significant positive relationship between the two, further substantiating their positive correlation (Figures 3(d) and 4).
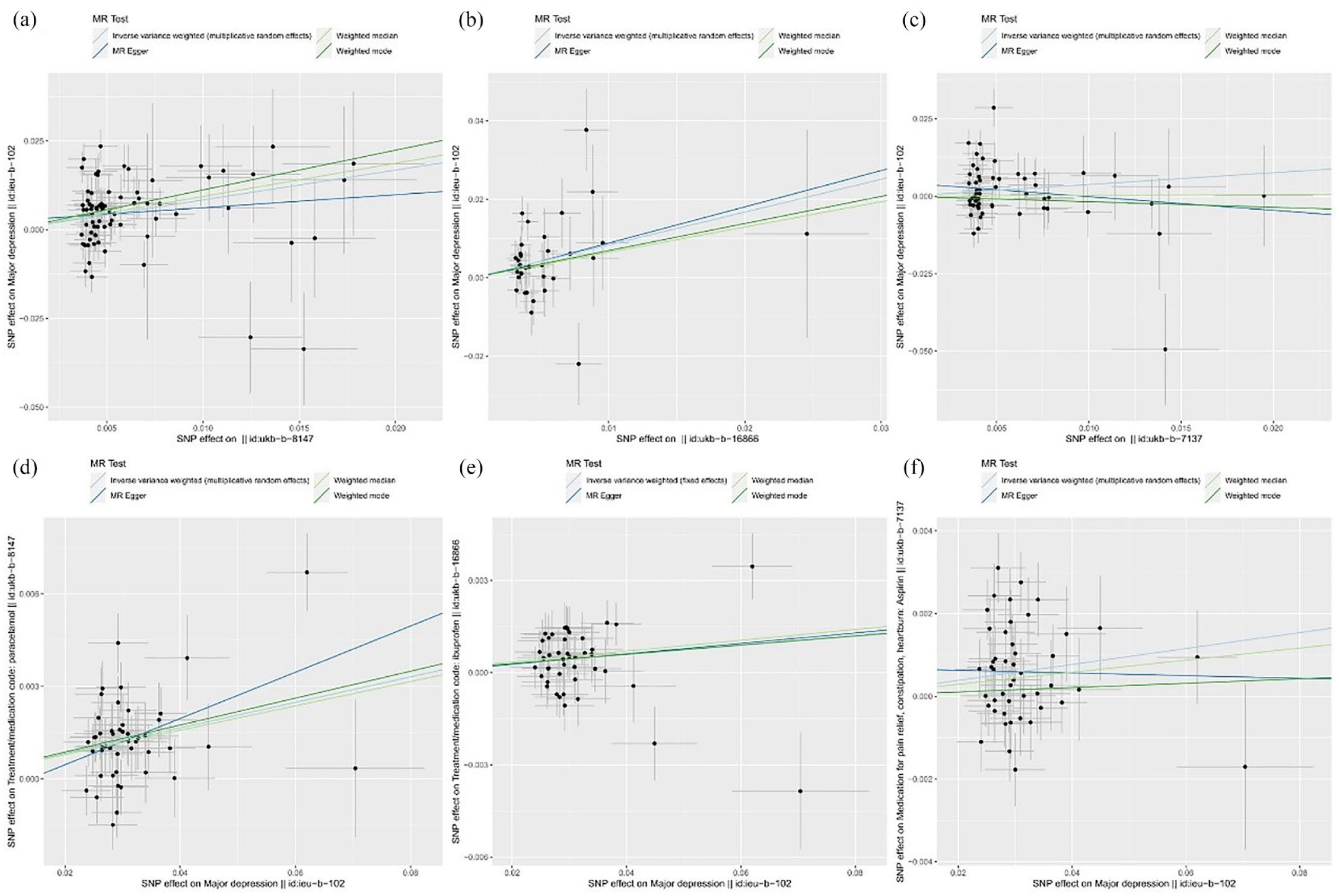
Scatter plots of the TSMR analysis. (a) Paracetamol and MD. (b) Ibuprofen and MD. (c) Aspirin and MD. (d) MD and paracetamol. (e) MD and ibuprofen. (f) MD and aspirin. The slope of the line indicates the causal relationship. Each color represents a different MR method. An upward tilt of the slope indicates a positive correlation, while a downward tilt indicates a negative correlation.
TSMR analysis results for MD and paracetamol, ibuprofen, and aspirin.
The IVW (FE) results show a significant positive correlation between MD and ibuprofen. MD increases the genetic predisposition risk of using ibuprofen (OR = 1.015, 95% CI: 1.007–1.023, p = 1.13E-04 < 0.05). The weighted median method (p < 0.05) also reveals a significant positive relationship between the two, and all four TSMR analysis methods point in the same positive direction, further validating their positive relationship (Figures 3(e) and 4).
The IVW (MRE) results show a significant positive correlation between MD and aspirin. MD increases the genetic predisposition risk of using aspirin (OR = 1.019, 95% CI: 1.009–1.030, p = 4.22E-04 < 0.05). The weighted median method (p < 0.05) also indicates a significant positive relationship between the two, and all three TSMR analysis methods consistently indicate a positive direction, further substantiating their positive relationship (Figures 3(f) and 4).
Sensitivity analysis
Furthermore, we validated all our results. The ME Egger intercept test indicated no pleiotropy (p > 0.05), suggesting that the results of this study are robust and reliable (see Table 2). We also performed a “leave-one-out” sensitivity analysis on all results, testing them by iteratively excluding each SNP. The results showed that no single SNP has a major impact on the robustness of the findings, further confirming the reliability of our study outcomes (Figure 5).
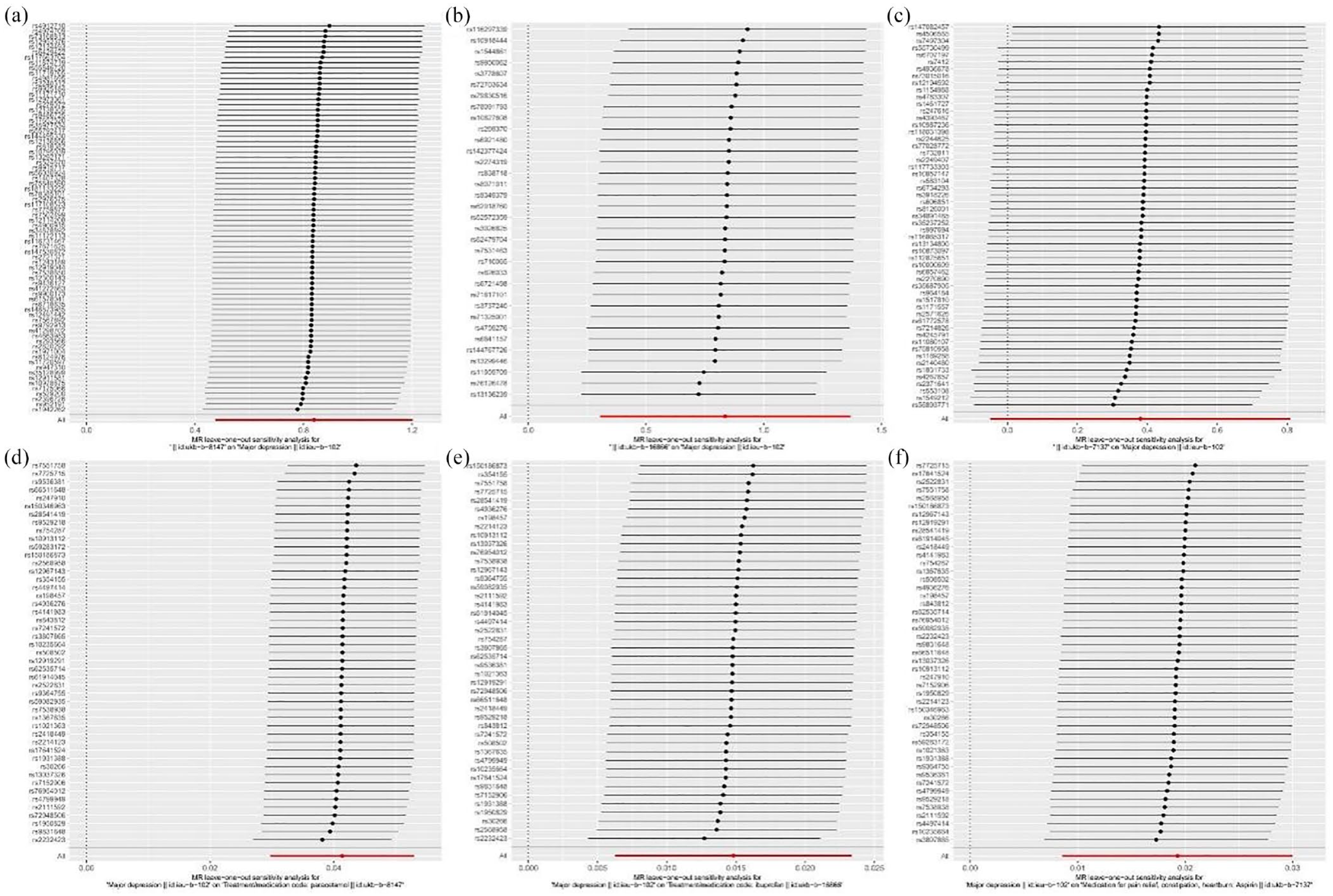
Leave-one-out plots of the TSMR analysis. (a) Paracetamol and MD. (b) Ibuprofen and MD. (c) Aspirin and MD. (d) MD and paracetamol. (e) MD and ibuprofen. (f) MD and aspirin.
Discussion
Through TSMR studies, we discovered a bidirectional positive correlation between the genetic inclination to use paracetamol, ibuprofen, and MD. We found that MD leads to an increased genetic tendency to use paracetamol, ibuprofen, and aspirin. Furthermore, the use of paracetamol and ibuprofen also heightens the risk of MD onset, but surprisingly, there is no direct association between aspirin and MD risk.
In addition, we employed the weighted median, weighted mode, and ME Egger methods to further validate, which, to some extent, all supported our findings. Moreover, we subjected our results to the ME Egger intercept test and “leave-one-out” sensitivity analysis. Neither showed significant pleiotropic bias or substantial influence from any single SNP, further emphasizing the robustness and reliability of our study’s results.
Our results corroborate and enhance observational studies. Literature from observational studies suggests that due to combined therapeutic effects and drug side effects, MD patients are more receptive to NSAIDs compared to other anti-inflammatory drugs (Uher et al., 2012). Notably, many patients rely on combined treatment due to the high comorbidity between depression and pain-inducing diseases (Manning and Jackson, 2013). Köhler et al. found in a study from 1997 to 2006 among SSRI-using depression patients (N = 123,351) that 8.3% concurrently used paracetamol, 7.5% used aspirin, and 5.1% used ibuprofen (Köhler et al., 2015). Research by Rosoff et al. (2021) found that MD increases the genetic propensity to take NSAIDs, supporting the well-known link between depression and physical pain. In addition, comorbid depression and pain can detrimentally affect physical, mental, and social functions when they surpass the existence of either depression or pain as individual conditions.
Furthermore, some studies found that the use of NSAIDs increases the risk of MD (Rosoff et al., 2021; Wium-Andersen et al., 2017). The use of NSAIDs may increase the risk of depression, with the cumulative days of NSAID use being the sixth largest predictor of depression in the elderly, and overall positively correlated with depressive events (Shaikh et al., 2023). Köhler et al. (2015) identified that concurrent use of NSAIDs raised the risk of depression (hazard ratio (95% CI): 1.31 (1.11–1.55)), while aspirin was unrelated (0.71 (0.50–1.01)). Molero et al. (2019) similarly found in non-aspirin NSAIDs a significant and mild increase in depression risk (risk ratio: 1.90 (1.15–3.17)), but no such link in aspirin (risk ratio: 0.74 (0.36–1.51)). An 8-year cohort study, including 137 aspirin-using participants (average age 65), found no significant protective effects of aspirin against depressive symptoms (Veronese et al., 2018). Another study of 1631 adults aged 35–66 found that aspirin lacked preventive efficacy against depression (Glaus et al., 2015).
These findings are consistent with our study. Our research complements and verifies the aforementioned literature, elucidating the specific NSAID drugs, paracetamol, and ibuprofen, whose use heightens MD risk. This bridges a gap in the global research on the causal relationship between paracetamol, ibuprofen, and MD. We speculate that this might be related to adverse neuropsychiatric symptoms caused by NSAIDs (paracetamol, ibuprofen) (Browning, 1996; Onder et al., 2004). Moreover, our findings from a genetic perspective validate the lack of a direct association between aspirin and MD, consistent with previous studies.
On one hand, we utilized the GWAS database with a large sample size and high measurement accuracy, enhancing the statistical power and lending greater credibility to our findings. Furthermore, we validated our results using multiple MR analytical methods and sensitivity analyses, bolstering the reliability of our conclusions. Compared to traditional observational studies, we employed genetic material SNPs to ascertain causal relationships, mitigating the effects of confounding variables. In addition, our bidirectional TSMR analysis negated the potential for reverse causality. To date, there has been no research either domestically or internationally exploring the causal relationships between commonly used NSAIDs (paracetamol, ibuprofen, aspirin) and MD. Our innovative application of bidirectional TSMR to investigate these relationships fills this research gap.
Our study does have certain limitations. While both our exposure and outcome variables were based on European populations, minimizing the potential for bias from population stratification and ensuring the plausibility of our TSMR assumptions, our results may not generalize to other populations, ethnicities, or regions without further validation. Moreover, despite our groundbreaking discovery of a bidirectional causal relationship between paracetamol, ibuprofen, aspirin, and MD, our analysis only accounts for the use or non-use of these NSAIDs. We cannot assess potential dose-dependent variations, and the precise mechanisms underlying their interactions remain unclear, warranting further in-depth research.
Conclusion
This study, utilizing bidirectional TSMR analysis, provides preliminary genetic evidence suggesting that MD increases the genetic propensity for the use of paracetamol, ibuprofen, and aspirin. This insight can aid clinicians in devising preventive strategies against the misuse of NSAIDs. Furthermore, we found that the use of paracetamol and ibuprofen can elevate the risk of MD, while no such risk was identified for aspirin. This signals a crucial clinical directive, suggesting that patients with MD opting for NSAIDs might consider the relatively safer aspirin, and exercise caution with paracetamol and ibuprofen.
Footnotes
Acknowledgements
Not applicable.
Author contributions
Zhiqiang Du and Haohao Zhu conceived the study; Ying Jiang, Yucai Qu, Qin Zhou, Haohao Zhu, and Zhiqiang Du collected the report; Zhenhe Zhou, Zhiqiang Du, and Haohao Zhu wrote the manuscript and edited the manuscript. All authors have approved to publication of the manuscript.
Availability of data and materials
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work is supported by the National Natural Science Foundation of China (No. 82104244), Wuxi Municipal Science and Technology Bureau (Nos. K20231039 and K20231049), Wuxi Municipal Health Commission (Nos. Q202101 and ZH202110), Top Talent Support Program for young and middle-aged people of Wuxi Health Committee (No. HB2023088), Wuxi Taihu Talent Project (No. WXTTP2021), Wuxi Medical Development Discipline Project (No. FZXK2021012), and Jiangsu Research Hospital Association for Precision Medication (No. JY202105).
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.