
Abstract
The authors offer a model for curriculum for education and training in substance-assisted psychotherapy (SAP), that is, psychedelic, psycholytic, and entactogen/MDMA (3,4-methylenedioxymethamphetamine)-assisted psychotherapy, addressing both the detailed contents of training and the question of experiential training. All authors of this model have an abiding interest and extensive experience in both the theory and practical aspects of SAP and questions relating to training. The model curriculum has been written through an international consensus building process and represents a consensus statement about the topic. The model includes an enumeration of theoretical themes and topics, which we suggest for inclusion in an SAP curriculum. The practical part of the curriculum includes experiential training with the following components: (1) apprenticeship observation: learning from observing experienced therapists, (2) ongoing clinical supervision: conducting treatment under direct supervision of experienced SAP therapists, and (3) a proposal for the inclusion of self-experiences for the trainees. Other parts address the use of peer supervision and conventional supervision. The authors are aware of the abiding need for respect of intercultural differences. We are conscious that the proposed model is one largely adapted to western industrialized countries with established graduate level education and training procedures for psychotherapists. However, the model curriculum includes teachings about the use of related substances and treatment techniques in indigenous cultures and traditions. This curriculum model may be valuable to psychedelic researchers, those endeavoring to train therapists for research studies, and those preparing for the clinical work to follow, once SAP is conducted outside of research settings.
Keywords
Introduction and overview
In the past 25 years, a rapid increase in the scientific study of the therapeutic potential of some psychedelic and entactogenic drugs has been seen. Results suggest that substance-assisted psychotherapy (SAP) with compounds such as psilocybin, lysergic acid diethylamide (LSD) or 3,4-methylenedioxymethamphetamine (MDMA) may be effective in the treatment of several psychiatric disorders.
Recently, the U.S. Food and Drug Administration has designated breakthrough therapy status two times for psychedelic treatments: (a) psilocybin for major and treatment-resistant depression, and (b) MDMA-assisted therapy (MDMA-AT) for the treatment of severe posttraumatic stress disorder (PTSD). If the current Phase 2 and Phase 3 trials are successful and marketing approval is granted, there will be a need for professional education and training in SAP. Standards and procedures for certification are beginning to be introduced in this rapidly developing field.
The following model for the training of psychotherapists in the use of SAP has been produced by a group of therapists and researchers, who represent extensive practical clinical experience with SAP, using psilocybin, LSD, N,N-dimethyltryptamine (DMT), and MDMA. The model curriculum drew on both older and more contemporary scientific literature, but mainly on professional experience conducting psychedelic/psycholytic/entactogen-assisted therapy. It has been written as a consensus article to contribute to a process of establishing guidelines for such trainings.
We delineate the three major approaches to SAP:
Psycholytic therapy typically uses lower doses of psilocybin-like psychedelics and the sessions occur with greater frequency. This approach is usually embedded in long-term psychotherapy, typically within a psychodynamic framework. The focus is on biographical, psychodynamic, and interpersonal aspects of the experiences. Goal of the treatment is alteration of defenses, revision of life narratives, the development of psychological flexibility, and healing of trauma and other developmental problems (cf. e.g., Passie et al., 2022).
Psychedelic therapy typically involves a smaller number of sessions (usually 1 or 2) and a higher dose of psilocybin-like psychedelics. There are typically a few preparatory and integration sessions, which focus on preparing the patient for the experience and are not an evocative of personal narratives and psychological conflict and/or character pathology. The approach is centered around the induction of a mysticoform peak experience of ego dissolution and connectedness, often interpreted in a transpersonal psychology framework (cf. e.g., Savage and Wolf, 1967).
Entactogen-assisted psychotherapy is currently most widely seen in the treatment of trauma, specifically PTSD and Complex PTSD. This approach usually involves three to five sessions, using a moderate dose of an entactogen (e.g., MDMA). These medicine-facilitated sessions are always embedded in the course of a short-term trauma-informed psychotherapy (cf. e.g., Mithoefer et al., 2015).
As researchers may develop new psychoactive substances as well as new procedures to facilitate psychotherapy by these agents, we use the encompassing term SAP.
This is a model curriculum for a comprehensive training of professional psychotherapists interested in learning to practice SAP. It is not a curriculum for practitioners who are not licensed as psychotherapists and are not conducting psychotherapy, for example, it is not for “sitters,” “monitors,” “facilitators,” “guides,” or other paraprofessional psychedelic-assisted practitioners who may assist licensed psychotherapists during sessions but do not provide psychotherapy. In most recent studies, only licensed psychotherapists were used even though the process is not designated as psychotherapy. Our curriculum is primarily offered as a guideline for the training of SAP psychotherapists to conduct SAP. When implemented to its full extent, the curriculum can be used to prepare certified, licensed, advanced practitioners working with a variety of substances and indications.
Training curricula for SAP: Past and present
Past: In spite of a certain distribution of psycholytic therapy in Europe during the 1960s (cf. Passie, 2024), no formal training curriculum has been established and come forward into the present day. A government-approved rudimentary curriculum was developed for use with LSD in Czechoslovakia. The following criteria were set there as defining a curriculum for SAP: an active medical license, training in psychiatry and psychotherapy, five controlled self-experiences, and 30 supervised therapeutic LSD sessions with five different patients (Hausner and Doležal, 1971; Hausner et al.,1967. In 1989, prominent psycholytic therapist Prof. Hanscarl Leuner (Göttingen University, Germany) provided a draft for a certified training program in psycholytic therapy (Leuner, 1989). From 1988 to 1993, five psychiatrists of the Swiss Physicians Society for Psycholytic Therapy (SÄPT) were granted a permit for the use of LSD and MDMA in psychotherapy. In this context, psychiatrist Samuel Widmer MD assembled a practical outline that defined training in SAP (Widmer, 2013).
Present: More recently, training manuals have been written for the treatment of cancer related existential distress using psilocybin-assisted psychedelic therapy, for example, one by Jeffrey Guss et al. (2020) and one by the Psychedelic Research Group at Johns Hopkins University (2008). These are specific and limited to this subpopulation of patients. Another example is the training for MDMA-assisted psychotherapy therapy provided by the Multidisciplinary Association for Psychedelic Studies (MAPS) for use in its randomized clinical trials of MDMA-assisted therapy for PTSD. The MAPS training includes a rudimentary theoretical part and mainly learning from videotaped therapeutic sessions. A controlled self-experience for therapists with MDMA-assisted therapy has been offered as an option for some therapist trainees in the MAPS research (Lykos Therapeutics, 2024). A broader scope is realized in the Certificate Program in Psychedelic Therapies and Research at the California Institute for Integral Studies (CIIS) (CIIS, undated). It lacks the practical component, and it offers only a survey of important issues in substance-assisted therapy; it is not a comprehensive training program, but rather an introduction to the field. A quite comprehensive training program, including six controlled self-experiences and carefully supervised clinical experiences, has been recently offered by the SÄPT in Switzerland (SÄPT, 2018).
Other more streamlined teaching/training programs have been established to suit specific research study needs. Most of them are intended to instruct therapists in clinical studies in a short time span. Usually, these programs provide a few days of theoretical learning and role-playing and practical training specific to the research study therapy manual. Usually, they do not include any self-experiences. These programs will not prepare therapists to deliver SAP outside of the research environment.
The International Society for Substance-Assisted Psychotherapy (ISSP)
In 2019, an effort was undertaken to establish an international organization to provide educational, administrative, and professional support for psychotherapists practicing SAP. In 2020, the ISSP was established as a non-profit expert association under European law with a tax-exempt status. Its primary missions are: (1) to develop consensual positions on topics of significance for SAP and (2) to contribute to the development of training and treatment standards (ISSP, 2019). Consequently, the Board and Advisory Boards of the ISSP consist of an international array of experts in the field of SAP. The ISSP has published a position paper on ethical principles and practices for the use of psychoactive substances in psychotherapy (ISSP, 2020). The drafting of the present model involved most members of the board and the advisory board of the ISSP.
History and development of the current model
The initial version of the present model was written by T. Passie, Anja Loizaga-Velder, and Jeffrey Guss in April 2021. The draft was then repeatedly extended and revised around 50 times over a period of 2 years by its 22 authors.
For the preparation of the proposal, the following materials were reviewed and partially incorporated:
Concept of a training curriculum as published by the SÄPT (2018). Three authors of the present proposal (J. Styk, P. Oehen, T. Passie) participated in the development of that training curriculum, up to its most recent format.
Guidelines for Training in Psycholytic Therapy by Leuner (1989, unpublished). Two authors had years-long training in psycholytic therapy under the guidance of Hanscarl Leuner (M. Schlichting, T. Passie).
Communiques of the European Medical Society for Psycholytic Therapy (1964–1974), (cf. Passie, 2024).
Developing Guidelines and Competencies for the Training of Psychedelic Therapists by Janis Phelps (2017) and Phelps and Henry (2022).
The Manual for MDMA-Assisted Psychotherapy in the Treatment of PTSD (MAP/MAT) by the Multidisciplinary Association for Psychedelic Studies (Mithoefer et al., 2015).
How to make use of the model
The model curriculum offered below offers a comprehensive framework for training licensed psychotherapists in the safe and efficacious use of SAP in community-based (non-research) settings. It is based on both clinical and empirical knowledge in SAP gained by most of the authors. It is written to allow adaptation for different countries, cultures, and settings. The authors are conscious that the proposed model is one for developed health systems in industrialized countries with a stable healthcare system, including availability of psychotherapy for the population as well as professional and state-certified psychotherapy trainings. However, the “theoretical component” of the draft is independent from the practical component and each can be used separately. Furthermore, regulations and requirements in some jurisdictions and for some specific SAP protocols may require additional items not covered here, such as training on the specifics of “scope of practice” issues where SAP will be practiced under a newly defined type of license to practice.
Our model is not intended to regulate the conduct of training in SAP. We offer it as an outline for developing training programs, comprising educational modules specifically devoted to SAP. The practical component of this training model will create considerable challenges in some countries at present. However, we are hopeful that there may be rapid growth in such training environments where SAP will be conducted, and in which SAP therapists can learn. The goal will be to offer affordable and excellent treatment, conducted by therapists-in-training under direct supervision of an experienced therapist. This curriculum is not designed for quick, inexpensive training; we are knowingly offering an ideal training curriculum. Ideally, opportunities for self-experience will be included for therapists-in-training as part of the overall training process.
We are aware that the model curriculum reflects the values, privilege, and professional cultural practices most readily available in Western industrialized countries. The use of psychoactive substances in other therapeutic contexts, especially in indigenous cultures, may have profound therapeutic effects, but is based on different traditions, methods, and cosmologies, which influences treatment as well as training procedures. Traditional indigenous approaches for using psychedelic drugs need to be studied with respect, and, wherever possible, to work with collaborative learning methods. However, these methods differ significantly from culture to culture and even from tribe to tribe (cf. Hofmann et al., 2001). The authors of the present paper realize that we are working, teaching, training, and conducting research within a Western cultural tradition and have neither particular competency in indigenous practices nor any claim to deep understanding of the cultures in which they are embedded. Therefore, our model cannot reflect this broad array of models and practices, and our curriculum is limited to the application of psychotherapy within western industrialized countries with established academic education in psychiatry, psychology, and psychotherapy.
A model curriculum for the training in SAP
Target groups, prerequisites, procedures
Target groups
The training is primarily designed for:
Medical doctors specialized in psychiatry and psychotherapy
Licensed psychotherapists or psychotherapists in training (PhD, PsyD, LCSW)
Medical doctors in training to become licensed psychiatrists/psychotherapists
Medical doctors in other specialties with advanced psychotherapeutic training
Researchers and research assistants working in scientific trials with SAP
Licensed clinical professional counselors (LCPC)
Psychiatric nurse practitioners
Licensed marriage and family therapists (MFTs)
A prerequisite for training and qualification in SAP is completion of accredited training in a recognized method of psychotherapy. Therefore, training in SAP can currently only be offered as continuing education or for work in jurisdictions that allow licensing specifically for the provision of SAP.
An intake interview conducted in advance of matriculation to assess motivation and level of maturity, including assessment of suitability for further training in SAP. If self-experiences are part of training, the candidates should be screened for potential contraindications (e.g., psychiatric or somatic disorders).
Responsibilities of the organizers and trainers
The organizers of the training, in some cases authorized by the appropriate federal or state level institutions, are responsible for the training curriculum. They are to decide on the admission procedures, the matriculation process, and the training itself, and are required to assess that required learning has occurred in a timely fashion. The institution offering the training also sees that ethical and clinical competencies are achieved and, finally, is responsible for issuing the certificates of completion.
Lecturers of the training
Ideally, the training directors will possess appropriate expertise to function as instructors, along with the chosen internal and external instructors. The instructors should have proper and recognized psychotherapeutic training apart from psychedelic therapy, per se. The practicum training should only be carried out using supervising therapists who are fully trained in the method with a minimum of 400 h of experience in conducting SAP with actual patients/clients.
Structure and sequence of the training
Ideally, the training will take place in fixed, stable cohorts and is likely to require 2–3 years to complete. The training should have both theoretical components and a practical component (supervised clinical work with actual patients/clients. After an introductory phase in which the basic didactic (theory and practical aspects of treatment) content is taught, practical training (supervised work with patients) can begin. Further theoretical education then will take place in parallel with the practical training. Practical training should start with direct observation of SAP (by advanced clinicians) by observing (and being observed by) an experienced therapist, supervision by therapists experienced in SAP. More advanced students may work also in peer supervision groups.
Our foundational recommendation is that practical training should take place in actual clinical conditions (e.g., hospital or day clinic) and ideally performed by multidisciplinary therapeutic teams.
Overview of the contents of the training
Below, we offer an overview of the content and topics which we recommend be included in any comprehensive SAP training program for psychotherapists who intend to become fully independent advanced certified practitioners and are prepared to work with a variety of substances and indications and types of patients. Not all modules may be necessary for therapists who are working in more limited ways, for instance in research settings, under supervision, under state licenses for only one substance, and/or with only one or a few substance/indication combination(s):
1. Attendance at didactic lectures combining theoretical topics with practical aspects
This includes the clinical applications of theoretical knowledge by watching videos of sessions and discussing the therapy and the attendees’ reactions to observing this potentially intense material, with time for discussion with instructors and peers.
2. Practical training with the following components: a. Observation of individual sessions that are led by an experienced SAP therapist. b. Self-experiences (the trainee receiving SAP, him/herself in a therapeutic setting (highly recommended but not mandatory). c. Conducting Individual substance-assisted treatment sessions, with patients, performed under on-site clinical supervision by an experienced therapist and teacher.
If group therapy training is offered: d. Participation in SAP group sessions as an observer and assistant therapist. e. Participation in SAP group sessions as a co-lead-therapist.
3. Participation in a peer group with exchange of experiences (e.g., peer supervision).
4. Participation in supervision sessions provided by experienced therapists.
5. Study of relevant literature and other learning materials.
6. Colloquium for preparing a final thesis (optional).
Theoretical component
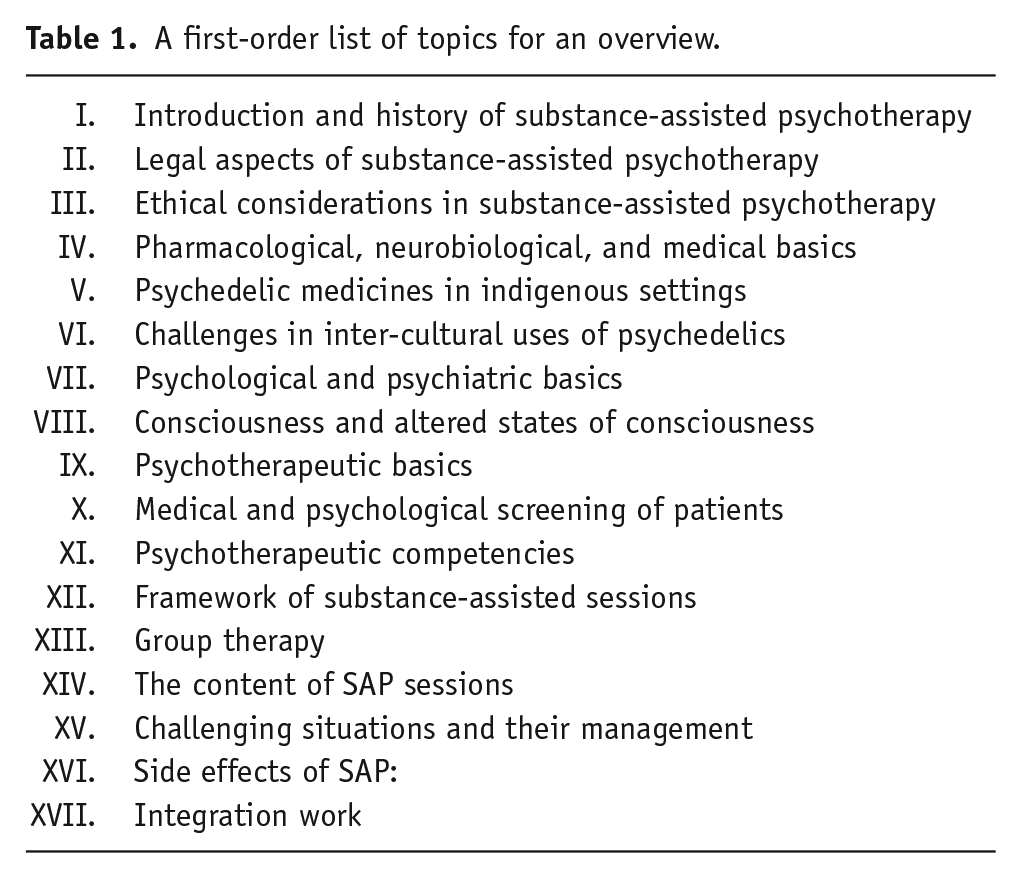
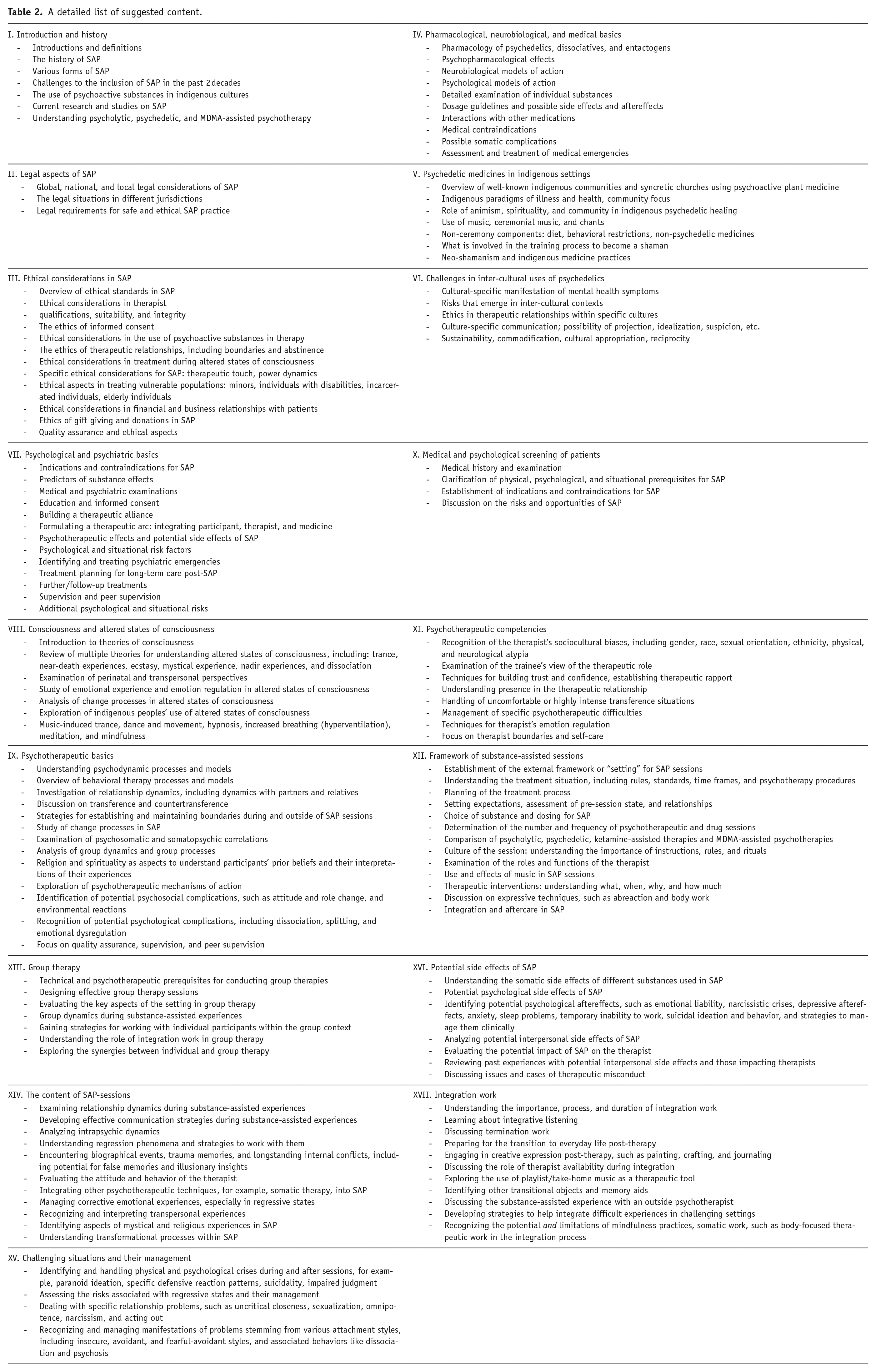
The contents of the theoretical component should be divided into thematic blocks. Each thematic block includes lectures, seminars, and an exchange of experiences with the trainers and other instructors to convey the contents. Table 2 provides a list of topics which should be included in the theoretical part of the curriculum.
A first-order list of topics for an overview.
A detailed list of suggested content.
Practical component: Varieties of experience with SAP
In addition to the theoretical training, it can be of considerable value for the training candidates to become familiar with SAP through direct experience under the guidance of an experienced therapist in a clinical setting.
One part of the training experience may be carried out through controlled self-experience of the substance-induced states in a therapeutically-oriented clinical context with an experienced SAP therapist. While this is not a rigid requirement, it is based on our experience and the historical consensus (cf. Oram, 2018; Passie, 2024) at least recommended.
A concurrent part is the practical learning of SAP by observing an experienced SAP therapist guiding both SAP drug and non-drug preparation and integration sessions. Subsequent steps are SAP treatment provided by the candidate under direct supervision of an experienced SAP therapist and then to provide SAP sessions alone, being supervised by an experienced SAP therapist and participating in peer supervision groups with colleagues.
Observation of individual sessions by an experienced SAP therapist
Ideally, a trainee has the opportunity to observe a variety of SAP sessions as guided by a psychotherapist highly experienced in SAP. The trainee could function as an assistant therapist to the patient, with the trainer being the main therapist. In these sessions, the trainees have the opportunity to experience and learn therapeutic interventions during actual SAP sessions, using the instructor as a model. In doing so, they can develop their therapeutic skills through observation and discussion of the process after the patient has left the session.
Controlled self-experience
From a learning perspective, there are several reasons direct experience may be of great value and perhaps indispensable for SAP students. Carefully constructed self-experience makes possible the direct experience of the altered experience, which provides a foundation for empathy, attunement, and imagination. Difficult experiences and situations that may feel overwhelming can strengthen the therapist’s sensitivity, empathy, and understanding of such states, as well as the opportunity to learn that staying with difficult experiences rather than moving away from them can be an opportunity for deep healing rather than an undesirable effect of the substance. The student therapist in dire straits may learn from the senior clinician offering the teaching. Self-experience in a group familiarizes the training candidates with a somewhat different way of working, since group dynamics have a profound effect on psychedelic experience. A therapeutic experience of SAP for the therapist may be very effective form of learning.
It is possible that an SAP trainee may prefer not to pursue a self-experience (or has contraindications to do so), and this choice should be explored respectfully and accepted after sincere discussion. In such cases, controlled self-experiences with other altered states of consciousness induced by non-drug practices such as holotropic breathwork could be considered. However, because of substantial differences to psychedelic-induced altered states of consciousness (ASCs) (e.g., experiential characteristics, duration, and controllability), it cannot be taken as equivalent. Refusing to engage in direct experience may indicate exploration to determine possible personal/psychological issues that may underlie the refusal.
There are also risks introduced by therapists self-experiences: (1) overgeneralizing from one’s own experience leading to the assumption that patients will have or should have similar experiences; (2) narcissistic response, for example, “now I have deep wisdom and power to heal”; and (3) discouragement of an otherwise promising therapist due to a difficult experience.
Training in practical implementation
The initial practical training should take place in individual treatment of patients, as this allows the trainers to observe the training candidates more closely, and trainee-specific details can be better elicited, communicated, and reflected upon. In addition, individual biographical backgrounds, resources, and dispositions of trainees and their role in shaping the experience as SAP practitioners can be more clearly identified and addressed. First, SAP treatment is provided by the candidate under direct supervision of an experienced SAP therapist, and then, the trainee conducts SAP sessions alone, being receiving supervision by an experienced SAP therapist. Peer supervision groups with colleagues may be another valuable part of training.
In historical trainings in psycholytic therapy, trainees had the opportunity to watch experienced therapists while they give SAP sessions. A similar practice is realized in the MAPS training system, in which trainees watch a series of videotaped therapy sessions as a central part of the training process. This observational approach can broaden and deepen understanding of the therapeutic situation, the processes taking place, and possible interventions. Observational learning can also help to learn to recognize and handle critical situations. It gives the student ample opportunity to ask questions and share responses to the treatment that is being shown. The patient’s confidentiality has to be protected according to established standards.
Supervised assistance
If not done per audio/video recording, the practical training may begin with observation of fully trained co-therapists conducting SAP. In doing so, trainees have the opportunity to experience and learn therapeutic interventions during actual SAP sessions, using the instructor as a model. They can also develop therapeutic skills through observation and discussion of the process after the patient has left the session.
Individual sessions under direct supervision
Following these co-therapy sessions, candidates next are invited to conduct session under direct supervision, that is, the supervisor is present in the background or as a co-therapist during drug-assisted sessions. We suggest a minimum of five consecutive individual sessions with the student taking being the active therapist in the drug-facilitated session. The subsequent debriefing allows for analysis and reflection of the student’s work.
Supervision during practice
In the next phase, the training candidate conducts SAP sessions on their own and is supervised at regular intervals by the trainers/clinical supervisors and by peer-supervision setting. Supervision by a clinical supervisor in this phase serves to safeguard the therapy, to work through difficulties that arise, and to foster therapeutic competence and the development of the unique identity as an SAP practitioner.
As an alternative to SAP sessions under direct supervision, training with small supervised groups, led by an advanced clinical supervisor, could be an alternative.
If possible and desired, training in substance-assisted group therapy could be added (usually at a later stage of the training).
In training for SAP in group settings, the training candidate should initially act as a co-therapist in the group sessions for a few times, followed by moving toward leading groups as a lead therapist. Participation in at least six substance-assisted group sessions as a co-therapist is recommended. SAP groups generally have 5–10 patients. Ideally, based upon our clinical experience, there will be a 4:1 ratio of patients to therapists (cf. Fontana, 1965, Oehen and Gasser, 2022). Co-therapists may be of diverse genders; determination of the best make-up of co-therapy teams should be made on a clinical basis of the group being treated.
Ideally, candidates will write an experience log and a self-reflection log after participating in substance-assisted individual or group sessions in each case.
Further learning settings
Self-study
The trainees have to study relevant literature on SAP and directly related topics (e.g., psychodynamics, psychology of religion, and spirituality) through independent reading. The study should be based on a list of recommended literature that will be provided to training candidates in advance. Self-study provides an opportunity for trainees to explore topics that are of interest to them such as specific historical aspects or clinical applications of SAP.
Peer group work/peer supervision
In the peer group sessions, the therapeutic experiences are being discussed with a focus on relevant theoretical and practical components of treatment. These peer sessions also serve the joint study of literature and the independent elaboration and discussion of questions arising from self-experience and theoretical work. Transference and countertransference matters will be privileged in these peer-led group supervision sessions (aka intervision). We suggest that peer groups should each have at least four participants in order to ensure an adequate diversity of perspectives and reflections.
Peer supervision groups are self-led and should be considered confidential to the members of the group. We suggest a minimum of three and a maximum of eight persons per group, which should take place at least once every 2 months.
Colloquium (case conference)
Parallel to the practical training, a colloquium for the training candidates will be offered. The central subject of the colloquium is the carefully constructed presentation of a clinical treatment case by the training candidates and discussion of all aspects of the case: selection, preparation, SAP sessions, integration, and any other clinically relevant issues.
Examinations
For the practical component, a review of the trainee’s competency is facilitated via direct supervision, peer supervision, and peer group work. For the theoretical learning content, oral or written examinations may be appropriate, if necessary throughout following the completion of didactic modules. At the time of writing, there is no recognized certification examination for advanced practitioners of SAP; however, individual programs can and do create their own comprehensive assessment of learning objectives, which are used as part of granting a certificate in SAP. Those who will seek licensure at the state professional level will likely be required to pass a nation-wide licensure exam.
Discussion
In the rapidly developing field of SAP, there is a pressing need for the development of comprehensive, professional, and ever evolving standards for training. The model for a training curriculum described in this article may be considered as a set of suggestions, assembled by an international group of researchers, therapists, and teachers with an interest in this field and in educating trainees for practice of SAP. The authors of the proposed model are aware of no models for comprehensive training programs to be studied from past efforts in this field. Most of what was done with respect to training or education of SAP therapists has an act of improvisation (cf. Hausner, 2009; Oram, 2018; Passie, 2024). Education in SAP remained alive until the 1980s in several clinics in Germany and the former Czechoslovakia, but without a comprehensive formal curriculum (cf. Hausner, 2009; Leuner, 1981).
In Switzerland, a training program, including self-experiences for the participating trainees, was conducted between 1988 and 1993 (Widmer, 2013) and has been restarted in the recent years (SÄPT, 2018, 2023). In the past, as well as in most RCT (Randomized Clinical Trial) therapy training today (e.g., SÄPT, 2018), it is a requirement that the trainee is a licensed mental health practitioner with specific training in psychotherapy. The training curriculum offered here is a more comprehensive training process, developing additional skills and knowledge for a licensed practitioner who already possesses fundamental knowledge about and experience in conducting psychotherapy.
Some recent trends in training for SAP
In recent years, RCTs have used different models for training study therapist in the skills needed to practice and to assess essential competencies:
Basic skills trainings for guides/facilitators to work with experimental subjects in research and experimental treatments.
Trainings for certified psychotherapists for the use of SAP with specific indications (e.g., the MAPS training for treatment of PTSD, EMBARK, etc.).
Comprehensive trainings for clinicians, sometimes including self-experiences and practical components (e.g., SÄPT Training, AWE Training, CIIS, Integrative Psychiatry Institute, etc.).
The latter category has recently witnessed a proliferation of novel educational programs and trainings. In some instances, these programs are affiliated with professional associations in psychology, psychiatry, or psychotherapy, or linked to universities. However, none of these programs confer a state-sanctioned license where training and experience are precisely delineated.
SAP today remains in the experimental phase and is the subject of ongoing scientific research. Consequently, there are only very few instances of these treatments being administered in a “real world” setting outside the confines of scientific studies (Haridy, 2023). There are hence very few “real-world contexts” available for educational and training purposes.
The question of self-experiences for therapists
Historically, there has been a strong consensus among therapists involved in clinical psychedelic or psycholytic work about the value of a few self-experience for the training in SAP. Expert organizations such as the European Society for Psycholytic Therapy (EPT) (1965–1974), the Czechoslovakian Administration for LSD Psychotherapy (1965–1978) and the recent Swiss SÄPT made direct experience with SAP a requirement in their trainings. In the U.S., the largest center for psychedelic therapy trials (the Maryland Psychiatric Research Center in Baltimore) conducted systematic self-experiences for staff and therapists between 1965 and 1975. (cf. Oram, 2018). MAPS has initiated a study to make self-experience available to their trainees for MDMA-assisted psychotherapy (Multidisciplinary Association for Psychedelic Studies, 2019).
The consensus among seasoned therapists, both past and present, leans toward endorsing self-experience as beneficial and valuable. However, some have hesitated to make it a mandatory prerequisite, given the lack of empirical evidence indicating a difference in therapeutic outcomes between treatments conducted by practitioners with and without self-experience and the ethical implications of mandated psychedelic experience. Nielson and Guss (2018) gave a recent perspective about this discussion.
Anecdotal evidence by researchers and therapists, who provided self-experiences to their trainees (e.g., Grof, 1980; Hausner, 2009; Leuner, 1981; Lykos Therapeutics, 2024; Oram, 2018), suggest that self-experiences are safe when guided by an experienced therapist. Up to now, the potential beneficial effects of self-experiences have not been tested empirically in a scientific fashion. However, in 2023, the Swiss SÄP, in collaboration with the University of Basel, has initiated a study on the safety, effects, benefits, and potential adverse effects of self-experiences in trainees participating in their training program (Müller et al., 2022). A similar study in the Netherlands will investigate the safety and effects of MDMA self-experiences in trainees for MDMA-assisted psychotherapy (Krediet, 2023).
From a clinical training perspective, there are five reasons why direct experience may be valuable, and perhaps indispensable, for trainees:
Controlled self-experience allows individuals to become familiar with the specific drug-induced ASCs by assuming the patient role. Without first-hand experience of such ASCs, therapists may struggle to comprehend and connect with their patients’ experiences. This empathic limitation can hinder the understanding of the affective and cognitive aspects of inner experiences and potential therapeutic interventions. Self-experience also reveals that profound experiences may occur even when it may seem that little is happening. It has been argued that patients under the influence of psychedelics can become highly sensitive to the insecurities and anxieties of therapists, which are easier to recognize and handle if therapists are familiar with these extraordinary sensitivities.
Navigating challenging experiential passages and situations during self-experiences strengthens therapists’ sensitivity, empathy, and understanding, while also demonstrating clinical methods for managing difficult phases of the therapeutic process.
Accumulated clinical experience has demonstrated that the therapeutic relationship can be massively altered under the influence of psychedelics. Psychodynamic theories conceptualize this as “intensification of the transference and countertransference situation.” Patients experience their relationship to the therapist (“transference”) possibly in other ways and with more intensity than usual, for example, feelings of dependency. This can reach dramatic proportions with delusional thinking about the therapists or pseudohallucinatory alterations of the therapist’s appearance. Ongoing SAP therapists are usually not much aware of this potentially dramatic altering/magnifying effect on the therapeutic relationship. Self-experience provides personal experience with these complex and hard to understand alterations. They can also help to realize that the therapist’s relationship to the patient is also intensified (“counter-transference”), what bears the risk for deformed perception of the patient or acting out. A more intense “transference and countertransference situation” implies higher demands on the therapist’s to control the interpersonal situation. Therefore, it may be instructive to live through such an intensified relationship experience.
Controlled self-experience allows individuals to encounter and work on their own traits, inner schemas, fears, longings, and other personal aspects, often at a level of depth not easily matched by other therapeutic modalities. This exploration and self-reflection can help therapists become more aware of and work on personal issues, for example, to ensure that unconscious influences stemming from these personal aspects do not hinder progress and safety in their work with patients.
Self-experience in a group setting familiarizes trainees with the dynamics of working in groups, exposing them to the power of group dynamics and enhancing their ability to navigate group interactions.
Some may have questions about methods for assessing the quality or depth of such learning experience as there is a challenging question of “how many.” The EPT as well as the Swiss SÄPT recommend five or six self-experiences for trainees in their programs. Practice of others like MAPS/Lykos and COMPASS suggests that one learning experience may be enough.
It is possible that an SAP trainee may strongly prefer not to pursue a self-experience (or may have acute or chronic contraindications), and this choice should be explored respectfully and accepted after sincere discussion. If a rejection of controlled self-experience results from personal preferences or anxieties, it should be reflected if a person with such preferences/anxieties is the appropriate candidate to guide patients through severely altered states of consciousness induced by psychedelic drugs.
Despite the potential benefits of therapists self-experience, we are aware of the potential problem of introducing biases in studies led by researchers who have had self-experiences with these compounds.
The question of intercultural compatibility
There are many different cultural contexts for SAP, which makes the adaptability and applicability of curricula such as this a challenge. All training programs are by nature embedded in their own cultural milieu and, as such, will be influenced by the setting, the teachers and the students that come to them, especially the overall goals, ethics, and world view in which they operate. SAP is conceptualized and implemented in different ways in different cultural contexts. Our model curriculum is offered as a framework for programs to use to develop training that is suited to the location in which it exists, using our suggestions as a reference that is comprehensive in scope but not rigid in implementation. Some cultures will have very different norms and boundaries regarding touch (within ethical and consensual practices); some cultures have strong preferences for or against group work and so forth. Other examples concern the question of openness and shame with respect to the supervised self-experience. However, even in a given culture, there are sensitivities to be aware of and to address in therapist training, supervision, and in the actual therapy process—such as race-, sexuality-, gender-related topics and trauma. It is considered important that such sensitivities are being welcomed and incorporated in the training of therapists. In our discussions, we also came across the topic of what can be named “cultural arrogance,” which means that a lot of colleagues seem to imply that the “psychedelic renaissance” is an international phenomenon, but it is in fact rather limited to a small professional subsegment of just some industrialized western countries. Broader dissemination must be conducted in ways that are culturally appropriate, respectful, and aligned with community norms, laws, and standards of care.
Future directions
During the last 10 years, there has been a substantial surge in research and interest surrounding the potential of psychedelics as a treatment for certain mental conditions, including substance use disorders. This shift has seen the movement of this topic from academic studies to profit-driven drug development endeavors, with the goal of applying these methods on a larger scale. Consequently, there has been a growing demand for comprehensive training programs in this field. A crucial component of training is the development of both training and treatment approaches that are both affordable and readily accessible, including insurance reimbursement.
Thus, therapist training in this area exists within a multicultural and multifaceted economic and sociocultural context, requiring training programs that are affordable, accessible, and well-defined. It is highly likely that, in the future, comprehensive training programs with state or federal licensure will become an integral component of the SAP field.
Again, we acknowledge that the present paper outlines a model that is most appropriate for training centers located well-established institutions (both academic and community based and in environments with well-developed healthcare systems. However, we hope that all therapists, researchers, and institutions with an interest in SAP will find value in our theoretical and practical considerations, using them as a foundation for the design and implementation of SAP training programs.
Footnotes
Acknowledgements
We would like to thank Michael Bogenschutz MD who made relevant suggestions to the manuscript. Thanks to Simon D Brandt PhD for his generous support.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TP was a consultant for Diamond Therapeutics (psilocybin microdosing). TP is involved with the Swiss Medical Association for Psycholytic Therapy (SÄPT) training program. TP has occasionally lectured at the California Institute of Integral Studies (CIIS), the AWE Psychedelic Therapy training program and the Integrative Psychiatry Institute Online Psychedelic-Assisted Therapy Training. AL-V has worked in the Certificate Program at the Center for Psychedelic Therapies and Research at the California Institute of Integral Studies (CIIS), the Foundations of psychedelic psychotherapy, Michener Institute, University of Toronto, the Psychedelic Practitioner Training Synthesis Institute, the AWE Psychedelic Therapy training. AD has been co-investigator on a psilocybin clinical trial at The Lundquist Institute that receives philanthropic funding from, Samberg Foundation, Cohen Foundation, Norris Foundation, and Anonymous donors. CSG has worked with the Heffter Research Institute and with MAPS. CSG has received funding from the Cohen Foundation, Norris Foundation, Samberg Foundation, Gordon Foundation. CSG has lectured in the Certificate Program at the Center for Psychedelic Therapies and Research at the California Institute of Integral Studies (CIIS), the UC Berkeley psychedelic therapy program and the Integrative Psychiatry Psychedelic Therapy Program in Colorado. GRG has worked for the Center for Psychedelic Therapies and Research (CPTR) training program at the California Institute of Integral Studies (CIIS). DE is a paid advisor for Aya Biosciences, Lophora Aps, Clerkenwell Health, and Mindstate Design Lab. PO declares no potential conflicts of interest. JS is involved with the Swiss Medical Association for Psycholytic Therapy (SÄPT) training program. MS declares no potential conflicts of interest. EV is principal investigator of a MAPS-sponsored open label MP18 trial using MDMA-AT for PTSD. EV is principal investigator of a trial testing psilocybin in the treatment of PTSD funded by a grant from Veterans Care Research. IWG has received support from MAPS for an MDMA-AT trial for PTSD. IWG is running an online introductory training in MDMA-AT through Psykologvirke clinic. TP owns shares in Psyon s.r.o. and in Společnost pro podporu neurovědního výzkumu s.r.o. TP is founder of the Psychedelic Research Foundation (PSYRES). TP acts as a consultant for GH Research and CB21-Pharma. TP was involved in research work by Compass Pathways, the Multidisciplinary Association for Psychedelic Studies (MAPS), Ketabon and GH-Research. MCM worked for MAPS Public Benefit Corp and has received consulting fees from Lycos Therapeutics. MCM is on the Scientific Advisory Board of Awakn Life Sciences. MCM conducted training and educational programs in MDMA-assisted Therapy. AM worked for MAPS Public Benefit Corp. (now Lykos Therapeutics). BA declares no potential conflicts of interest. EK declares no potential conflicts of interest. PG is president of the Swiss Medical Association for Psycholytic Therapy (SÄPT). PG was a paid consultant for COMPASS Pathways, MindMedicine Inc., and the Reconnect Foundation. EMN is co-Founder and Chief Visionary Officer at Fluence International Inc. EMN acts as advisor to Tactogen and Good Cap. EMN owns shares or options in Tactogen, Beckley Psytech, and Good Cap. IG is co-Founder and Chief Executive Officer of Fluence International Inc. IG owns stock options of Beckley Psytech and Journey Clinical. JP is director of the Center for Psychedelic Therapies and Research (CPTR) training program at the California Institute of Integral Studies (CIIS). JP is affiliated with the Heffter Research Institute (HRI) and the Holos Institute in San Francisco. JP has been paid for consultations for the Usona Institute and the University of Toronto. ABB acts as paid Chief Clinical Officer for Cybin Inc. ABB is a paid consultant for Adelia Therapeutics. He has filed patents on the use of psychedelic compounds for the treatment of psychiatric indications. ABB has received financial compensation for training and educational programs from Yale University, Chacruna Institute, the Integrative Psychiatry Institute, ATMA, Synthesis Institute, Karolinska Institute, Cybin, Adelia Therapeutics, and the Embody Lab. JG acts as Lead Trainer for the training of psychedelic therapists at Fluence International Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.