
Abstract
Background:
Interoceptive processes may underlie maladaptive patterns of alcohol use. Bodily sensations experienced during alcohol intoxication could therefore reveal distinct mechanistic components relevant for addiction theory and research. Here, we apply novel tools to examine how intoxication impacts somatic awareness using bodily maps and a cardiac interoception task.
Methods:
In a double-blind, within-subjects, placebo-controlled study, social drinkers (n = 37, 17 female) were administered 0.4 g/kg of alcohol. We measured changes in self-reported bodily sensations during the ascending and descending limbs of the blood-alcohol curves using the emBODY tool. Additionally, we recorded biphasic measures of subjective alcohol effects (sedation and stimulation), changes in heart rate, and assessed psychophysical measures of cardiac beliefs using the heart rate discrimination task.
Results:
Acute alcohol administration altered bodily sensations, reflected by strong sensations in the chest, limbs, and head, with lesser effects in the placebo condition. Linear-mixed models examined correlates of bodily sensations across conditions. Extent of bodily sensations correlated with heart rate changes and breath alcohol content. In the ascending limb, bodily sensations negatively correlated with subjective stimulation and positively with sedation. Finally, extent of bodily sensations correlated with the metacognitive sensitivity of cardiac beliefs, suggesting a cross-dimensional integration between sensations and interoceptive awareness.
Discussion:
These findings highlight the value of bodily mapping in psychopharmacology, as interoceptive components of alcohol intoxication may provide a somatic basis for addiction. We interpret our results through low-sensitivity models, suggesting individuals with reduced bodily sensations during intoxication may face elevated risk for alcohol use disorder, a hypothesis that will be examined in future research.
Keywords
Introduction
Research on interoception, the processing of internal physiological states (Desmedt et al., 2023; Suksasilp and Garfinkel, 2022), provides theoretical and technical tools to study the way our body responds to external stimulations and how the brain processes these responses. This multifaceted process can offer new dimensions to the study of mental disorders (Khalsa et al., 2018), and indeed has already been shown to be relevant for understanding addictive behaviors (Naqvi et al., 2007; Naqvi and Bechara, 2010; Verdejo-Garcia et al., 2012). However, the majority of conceptual and experimental neuroscience findings regarding addiction have focused on the direct impact of substances on cerebral processes, without considering the many concordant changes in the body. Modulation of bodily sensations following acute or chronic substance consumption remains a neglected domain by influential theoretical models of addictive disorders.
Previous lesion, neural, and animal studies (Lovelock et al., 2021; Paulus and Stewart, 2014; Verdejo-Garcia et al., 2012), show how dysregulated interoceptive processes underlie the development or persistence of addiction. Yet, the physiological changes generated by acute consumption, and their impact on interoceptive processes, is largely unknown in pharmacological contexts. Indeed, pharmacological agents provoke a cascade of physiological responses and bodily adaptations, and these changes can in turn be perceived and processed through interoceptive pathways (Leganes-Fonteneau et al., 2019). Individual variation in the magnitude and awareness of these acute bodily changes following consumption may yield new insights in addiction research. For example, acute hedonic bodily sensations after drug consumption might foster positive reinforcement and hence, the maintenance of addiction through interoceptive mechanisms, beyond the well-documented brain modifications involved in such reinforcement (e.g., in the reward system). Here, we bridge this gap by using recently developed tools to quantify the topology and calibration of bodily sensation, using bodily maps to measure the topography of phenomenological bodily sensations linked to acute alcohol effects.
Beyond its well-established cognitive effects (e.g., disinhibition, Rose and Duka, 2007), the administration of alcohol induces immediate alterations in bodily states such as changes in cardiovascular functioning, increasing (Bau et al., 2011; Conrod et al., 2001; Ireland et al., 1984; Ray et al., 2006) or decreasing (Vatsalya et al., 2014) heart rate during the ascending limb of the blood–alcohol curve as a correlate of subjective measures of intoxication. Other metabolic functions, such as thermal regulation (Yoda et al., 2005), gastric emptying (Bujanda, 2000), and glucose metabolism (Lanng et al., 2019) are also impacted by alcohol administration. These alcohol-induced physiological changes are relevant in modulating reward-related behaviors (Leganes-Fonteneau et al., 2021a), serving as risk markers for alcohol use disorder (Conrod et al., 1997; Leganes-Fonteneau et al., 2020a).
Concomitant with those changes, alcohol triggers distinct bodily sensations of warmth and glow and peripheral effects such as euphoric bodily rushes (McCollam et al., 1980). These bodily sensations could influence the development of subjective alcohol effects, operationally defined as the self-reported internal experiences resulting from alcohol consumption (Martin et al., 1993; Rueger and King, 2013). Specifically, subjective sedation refers to feelings of decreased alertness and slowed functioning, measured here by self-reported ratings of feeling “sedated,” “sluggish,” or having “slow thoughts,” whereas subjective stimulation refers to heightened feelings of energy and arousal, measured here by ratings of feeling “energized,” “excited,” or “up” (Holdstock and Wit, 1998; Martin et al., 1993; Rueger and King, 2013). These sensations, which fluctuate across the ascending and descending phases of the blood–alcohol curve, can serve as key discriminative cues that influence an individual’s affective responses and potentially guide subsequent drinking behavior (Duka et al., 1998).
Despite this initial interest for the effects of alcohol on bodily sensations, novel techniques, and conceptualizations emanating from interoceptive research have not been fully integrated in psychopharmacological research. Research on interoception often focuses on cardiac detection tasks, measuring participants’ ability to detect their own heartbeat. Alcohol can acutely impact different indices of cardiac interoception, and these interoceptive changes may participate in the experience of intoxication, as they correlate with subjective feelings of inebriation (i.e., light-headedness, mood, Duka et al., 1999; Leganes-Fonteneau, 2024a; Leganes-Fonteneau et al., 2019, 2021b) feeding via learning mechanisms (Bevins and Besheer, 2014) into long-term alcohol expectancies that can influence future drinking attitudes and behaviors (Leganes-Fonteneau, 2024a; Leganes-Fonteneau et al., 2021b).
However, the initial attempts to study acute effects of alcohol on interoception present fundamental limitations inherent to cardiac detection tasks. These measures, particularly the heart-beat discrimination task, have exhibited significant methodological limitations, primarily due to their lack of reliability and validity (Desmedt et al., 2018). Additionally, measuring cardiac detection abilities overlook the broader impact of alcohol on bodily substrates, represented by a wider array of interoceptive processes (e.g., gastric feelings, warm sensations, peripheral activation). Although changes in the ability to detect cardiac signals might serve as a proxy for sensitivity to the bodily states influenced by alcohol, they do not comprehensively capture the phenomenological aspects of bodily sensations experienced during intoxication. Phenomenological perspectives of acute alcohol effects on bodily sensations could thus provide fine-tuned theoretical and experimental approaches for the study of interoception.
Bodily mapping techniques, such as the emBODY tool (Nummenmaa et al., 2014), offer a computerized method in which participants mark the location and intensity of their bodily sensations on an illustrated human figure, denoting areas of perceived activation and deactivation. This technique has been instrumental in unveiling the phenomenology of bodily sensations across different feeling states, uncovering distinctive patterns of activation linked to emotions (Nummenmaa et al., 2014), and other subjective experiences (e.g., stress, relaxation; Nummenmaa et al., 2018). Such a tool has also been used to explore the physiological sensations related to drunkenness, but only through retrospective measures (Nummenmaa et al., 2018), failing to document the actual bodily sensations felt during the ascending and descending limbs of an intoxication episode in a placebo-controlled manner. This method shows great potential for advancing the phenomenological description of bodily sensations related to other facets of alcohol use and misuse, including intoxication, hangover (Prat et al., 2008), negative affect, and craving (Billaux et al., In press, Under review). Moreover, bodily sensations may, in a similar fashion to cardiac measures of interoception, correlate with concurrent subjective feelings of intoxication, highlighting their validity as an interoceptive measure of alcohol effects.
This report describes a nonregistered exploratory examination of the subjective bodily sensations experienced following a within-subjects placebo-controlled alcohol administration procedure (0.4 g/kg). As part of a larger registered report (Leganes-Fonteneau, 2024b), participants completed a computerized version of emBODY to indicate their bodily sensations following beverage administration throughout ascending and descending limbs, together with a well-validated questionnaire of subjective alcohol effects, the Brief Biphasic Alcohol Effects Scale (B-BAES, Rueger and King, 2013). Before and right after beverage administration, a measure of heart rate was extracted. At baseline and at the end of each session, participants also undertook an instance of the heart-rate discrimination task (HRD; Legrand et al., 2022), measuring changes in the sensitivity, precision, and metacognitive calibration of cardiac interoception.
Our primary objective was to delineate the phenomenological experience of intoxication by visually mapping the topography of bodily sensations associated with acute alcohol consumption. Additionally, we provided concurrent validity to the use of bodily maps in the context of alcohol administration by examining their correlation with subjective feelings of intoxication and changes in cardiac interoception. We posited that bodily sensations of intoxication would differ from those experienced following placebo administration, as shown through confusion matrices (Hypothesis 1). We expected that objective and physiological markers of intoxication (breath alcohol content (BrAC) and heart rate) will correlate with the extent of bodily sensations (Hypothesis 2). Furthermore, we postulated that there will be a correlation between the extent of bodily sensations and subjective alcohol effects across ascending and descending limbs. This builds upon previous studies on alcohol administration and cardiac interoception to focus on the principal dimensions of the B-BAES: sedation and stimulation (Hypothesis 3). Finally, we explored the interplay between phenomenological and performance-based measures of interoception, expecting that changes in cardiac interoception will map onto alcohol effects on bodily sensations (Hypothesis 4), independently of changes in control exteroceptive performance.
Methods
Beverage administration
In this double-blind, placebo-controlled experiment the alcohol beverage consisted of a 0.4 g/kg dose of alcohol (190-proof Everclear), mixed with sugar-free tonic water (Schweppes) and five drops of angostura bitters to make up a 200 ml solution. In the placebo session, participants received 200 ml of tonic water mixed with five drops of angostura. The 200 ml solution was divided in five 40 ml-glasses presented on a tray. Alcohol was sprinkled over the tray to provide olfactory cues and participants were instructed to drink one glass at a time every 2 min at their own pace. Additional details regarding beverage administration are presented in (Leganes-Fonteneau et al., 2021c), and participants were told they would be administered different doses of alcohol on both sessions. BrAC was measured using an Alco-Pro FST breathalyzer at three time points following beverage administration: 10 min postadministration (t1, ascending limb; mean BrAC = 62.77, SD = 28.65), 30 min postadministration (t2; mean BrAC = 59.13, SD = 14.53), and approximately 75 min postadministration (t3, descending limb; mean BrAC = 51.30, SD = 13.20).
Questionnaires
Initial surveys included a demographic questionnaire, with alcohol use assessed through the Alcohol Use Disorder Identification Test (AUDIT) (Saunders et al., 1993) and the Alcohol Use Questionnaire (AUQ; Mehrabian and Russell, 1978), adjusted for the college demographic in the U.S. (Leganes-Fonteneau et al., 2021a). Alcohol use scores are reported solely for descriptive purposes.
This report focuses on a state survey of alcohol effects, the B-BAES (Rueger and King, 2013), which evaluates feelings of stimulation and sedation. This survey was administered at two different time points (t1 and t3) following alcohol administration to gauge subjective alcohol effects across ascending and descending limbs.
Bodily maps
We utilized an adapted computerized version of the emBODY tool. Participants were given instructions prior to starting the experiment. At various time points during each session (baseline, t1, t2, t3, as outlined in the procedure), they were prompted to indicate areas in their bodies where they experienced sensations of activation (e.g., high arousal) and deactivation (e.g., numbness) in the present moment. This was accomplished by drawing with a mouse cursor across two body outlines (Figure 1(b)). The tool’s design incorporates a feature where a longer presses over a body area indicate higher intensity ratings, with the interface providing feedback by increasing the number of lit pixels on the screen.
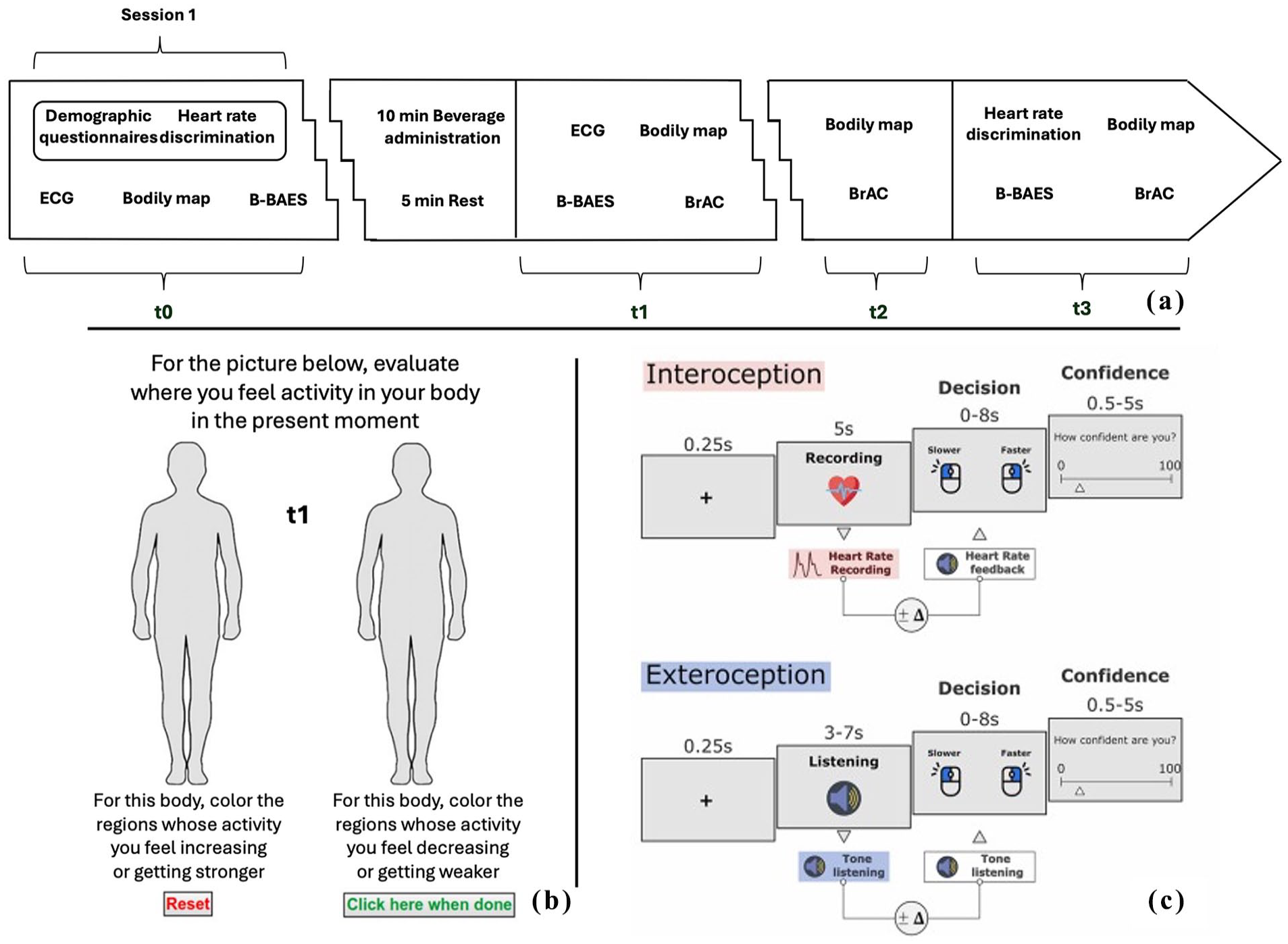
(a) Experimental procedure. Only during session 1, participants undertook an initial assessment including demographic questionnaires and the heartrate discrimination task at baseline. All other experimental components are equivalent for sessions 1 and 2. (b) Depiction of the emBODY tool response window, adapted from (Nummenmaa et al., 2014). (c) Task description for the heart rate discrimination task, as adapted from (Legrand et al., 2022).
HRD task
Full methodological details concerning the HRD paradigm are available in (Jeganathan et al., 2024; Legrand et al., 2022), (Figure 1(c)). We adhered to the established procedure, which incorporates both interoceptive and exteroceptive control conditions within a mixed-trials format. In brief, a Nonin fingertip pulse oximeter is used to record participant heartrate throughout the task. During the interoceptive condition, participants focus on their heartbeat for a 5 s listening interval, followed immediately by the presentation of a feedback tone, consisting of beats that may be faster or slower than the participant’s actual heartbeat measured during that period. Participants must determine whether the tones were faster or slower than their heartbeat and indicate their confidence in this decision. An exteroceptive condition is included to control for noninteroceptive factors (e.g., working memory or temporal estimation biases). Here, instead of comparing their heart rate to a feedback tone, participants listen to two tone sequences in quick succession, a “reference” sequence and a second sequence that is slightly faster or slower, according to a staircase procedure. This approach pinpoints each participant’s threshold, or point of subjective equality, where they are equally likely to judge the second sequence as “faster” or “slower” than the reference. From this task, we extract measures of metacognitive bias (average confidence), and metacognitive sensitivity or insight (relationship between confidence and accuracy computed as area under the ROC curve) Equivalent measures are obtained for the exteroceptive condition, enabling a direct comparison of interoceptive and exteroceptive processing. Here, we compute difference scores between the postbeverage HRD task and the baseline administration in session 1 to index alcohol and placebo effects on interoceptive and exteroceptive processing (Leganes-Fonteneau, 2024a).
Procedure
Participant recruitment (n = 37), compensation details, and general procedures are outlined in the original registered report (Leganes-Fonteneau, 2024b), with ethical clearance provided by the Rutgers University IRB. Eligibility required participants to be 21 or older, have consumed over 3 alcohol units per week in the past 3 months, and have no history of learning disabilities, psychiatric disorders, substance use disorder treatment, current AUD (AUDIT < 20), or regular drug use. Pregnant women and those with a BMI 20% above or below normal were excluded. Across the two experimental sessions, participants underwent a double-blind, placebo-controlled, alcohol administration protocol (0.4 g/kg), with session order counterbalanced by gender.
In the first session, participants filled out demographic and alcohol consumption questionnaires (AUDIT, AUQ) and underwent the HRD measure of cardiac interoception at baseline. At t0 participants were instructed to drink water to familiarize themselves with the bodily mapping tool by providing a reference interoceptive sensation (swallowing water, data not analyzed). This was followed by baseline state assessments using B-BAES.
Next, participants undertook an emotional visual search task as part of a larger registered report, not discussed here (Leganes-Fonteneau et al., 2020b). Cardiovascular measurements were obtained during a 5 min low-demand vanilla task (Jennings et al., 2007), using a 3-lead electrocardiography (ECG) configuration (Powerlab, AD Instruments Ltd.). This was followed by a 10-min beverage administration procedure and a 5-min rest period. During the ascending phase of intoxication, at t1, another cardiovascular measure was obtained, providing a measure of heart rate difference score (postbeverage minus prebeverage). Following ECG measurement, participants completed a bodily map, state surveys, and BrAC readings. Following a 15-min repeat of the emotional visual search task (data not presented), participants performed a second bodily map and had BrAC measurements at t2. The session ended with a postbeverage HRD task and a final bodily map, state surveys, and BrAC readings at t3, during the descending phase. The second session mirrored the structure of the first, but without the preliminary questionnaires or baseline HRD and emotional visual search tasks (Figure 1(a)). Participants read and signed an informed consent before the start of the experiment and were compensated USD 10/h for their time with gift vouchers at the end of the second session.
Data analysis and results
Demographic data
Thirty-seven participants (17 female), completed the experiment, but due to data loss at different time points (one with invalid physiological data, one who did not complete both sessions, and three with invalid HRD data), degrees of freedom vary across analyses (Table 1). Two participants reported being daily nicotine users.
Descriptives for demographic information, alcohol use, and subjective number of drinks in each condition.
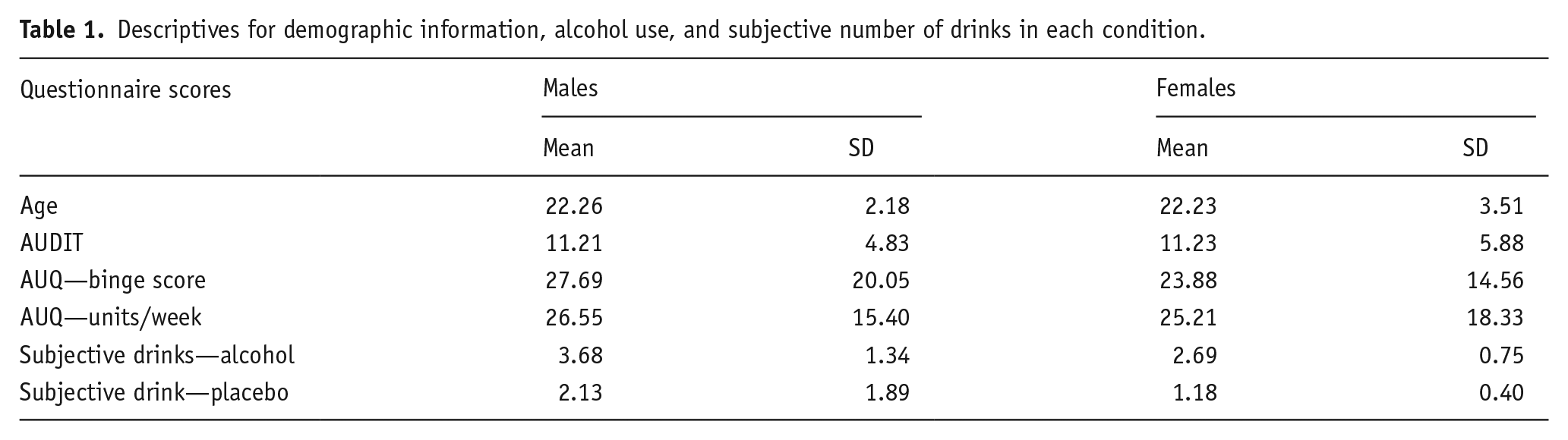
Exploratory analyses reveal a significant effect of sex on subjective number of drinks consumed in the alcohol condition, t(29) = 2.6772, p = 0.012. This variable was included in final exploratory analyses.
Topography of alcohol-induced bodily sensations
Following the analytical procedure described in (Nummenmaa et al., 2014), bodily maps were created for each data point (Figure 2). For each participant, data were first cleaned to include only the pixels located within the figure, and a data matrix was generated by subtracting deactivation maps from activation maps. In order to construct a visual representation of bodily maps, t-tests were conducted on each pixel by incorporating data from all subjects, color-mapping pixels at a significance threshold of p < 0.05, with nonsignificant t-values represented in black (Figure 2, top). Additional exploratory bodily maps display separately activation and deactivation sensations (Figure 2, middle, bottom), although these maps were not corrected for multiple comparisons due to lack of statistical power.
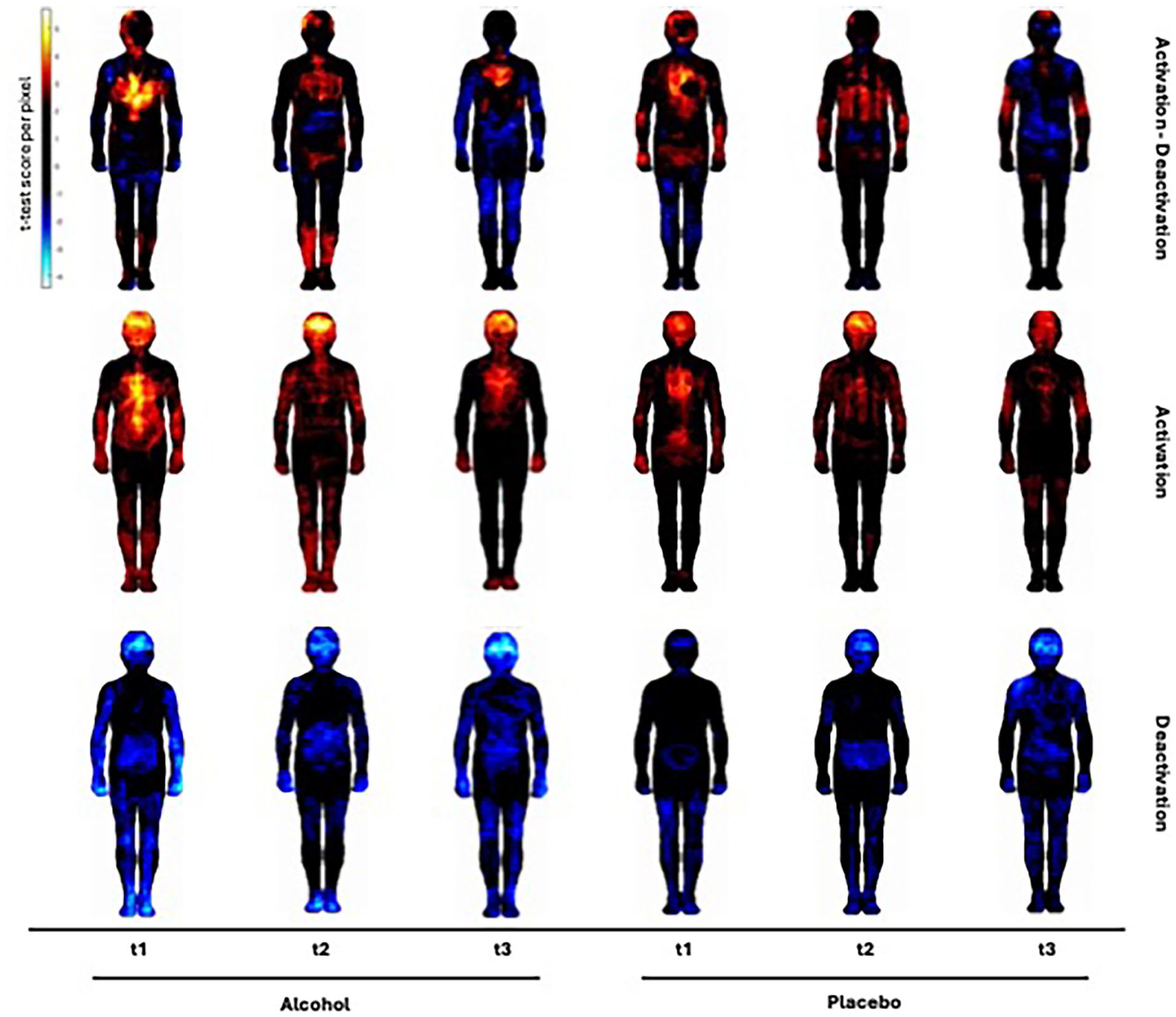
Heatmaps presenting the topography of bodily sensations experienced following beverage administration at the three time points. Each colored pixel represents a significant “activation” or “deactivation,” thresholded at a p < 0.05 level. Colormap depicts the t-value at each pixel. Activation minus deactivation maps highlight different bodily sensations across the blood-alcohol curve, with participants reporting strong activation in the chest during the ascending limb that decrease through time. In the placebo condition, we find analogous sensations, particularly in the ascending limb, whereas the extent of bodily sensations diminishes through time. Activation and deactivation maps show a more nuanced view of the sensations experienced and how beyond strong feelings in the chest, alcohol also generates sensations in the limbs.
Specific bodily patterns arise following beverage administration (Figure 2), with intense sensations experienced in the chest and head at t1 following both alcohol and placebo, although the activation pattern is more specific and intense in the alcohol condition. At t2, we observe stronger peripheral effects of activation (i.e., lower legs) that do not appear following placebo. Finally, at t3 we observe a clear pattern of activation in the upper chest together with generalized feelings of deactivation in the limbs, all of which are not present in the placebo condition.
Exploratory analyses allow observing distinct activation and deactivation patterns that are otherwise obscured by the main subtractive analysis. Both activation and deactivation patterns on the head are observed through alcohol administration, probably reflecting individual differences in the extent to which participants perceived sensations in the head as activation or deactivation. Sensations in the chest remain largely linked to feelings of activation, whereas gastric sensations are related to feelings of deactivation toward the descending limb.
Similarity matrix
Spearman’s correlations quantifying the similarity between discrete bodily maps across different conditions analysis were performed between all levels.
The correlation matrix (Figure 3) revealed that the highest similarity was observed between alcohol at t2 and t3 (r = 0.43). Moderate similarities were found between alcohol at t1 and t2 (r = 0.36), alcohol at t1 and t3 (r = 0.34), and placebo at t1 and t2 (r = 0.28). Other condition pairs showed lower correlations, indicating distinct body sensation maps, notably there was a 0 correlation between activation patterns at t3 in the alcohol and placebo condition.
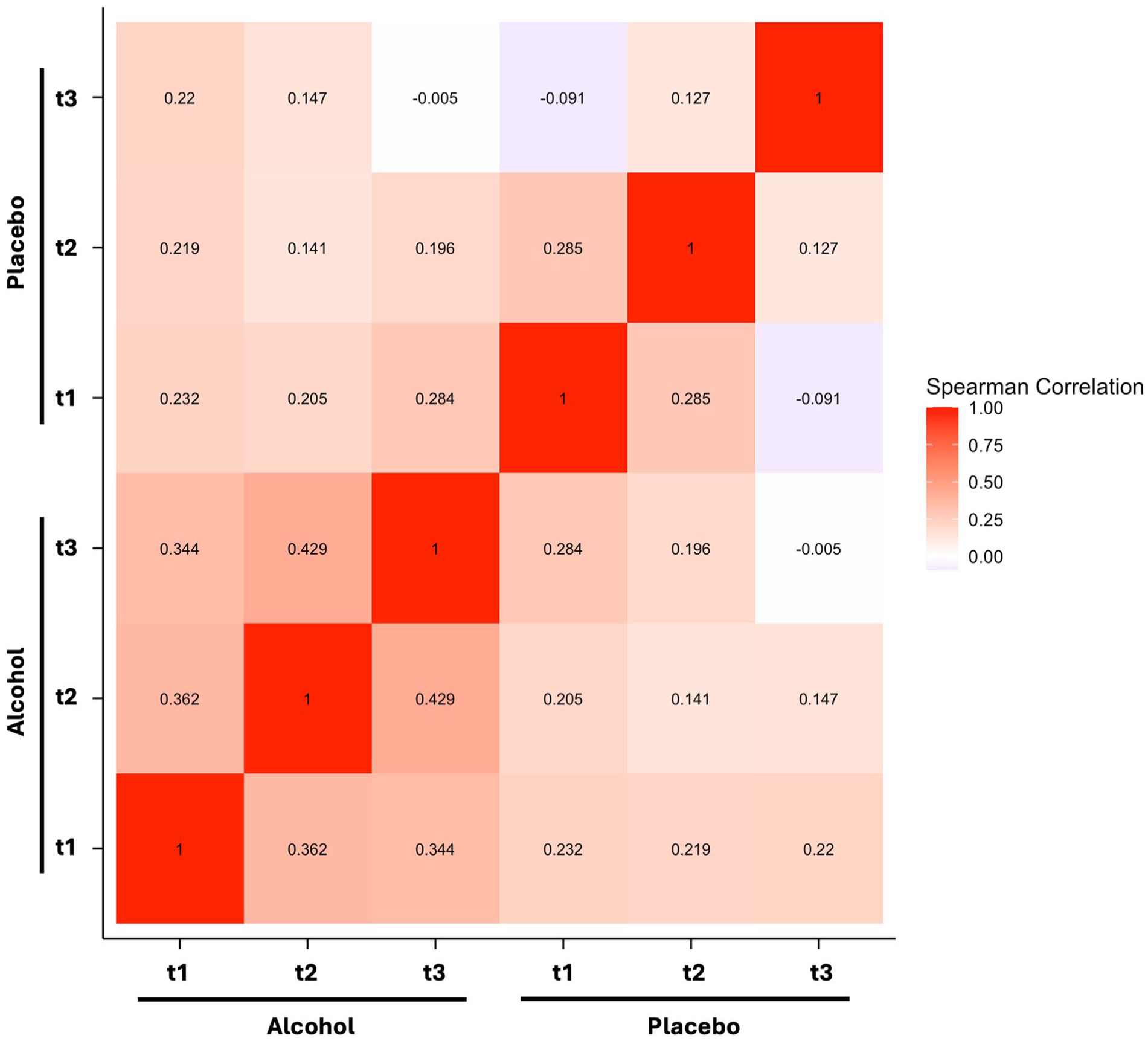
Spearman’s correlation matrix presenting the interaction between bodily sensations following beverage administration at each time point. The strongest correlations are observed within the alcohol condition, whereas there is no observed correlation between sensations experienced following placebo and alcohol at t3.
Interaction analyses
We calculated the extent of bodily sensations at each time point as the proportion of nonzero pixels in the bodily map derived from subtracting deactivation maps from activation maps. For any given pixel, a value of 0 could occur only if the pixel was not selected in either map or if the patterns of activation and deactivation perfectly mirrored each other. Linear mixed models (LMMs) were used to examine whether the condition (alcohol vs placebo) modulates the relationship between the extent of bodily sensations and various variables across different time points (Table 2). For simplicity, both significant interactions and main effects were followed up with Pearson’s correlations computed separately for each condition (Figure 4). However, it is important to note that only significant interactions provide evidence of a differential effect of condition on the correlation between bodily sensations and the variables of interest. For BrAC, Pearson’s correlations alone sufficed as these measures are relevant only in the alcohol condition.
Results of linear mixed models examining the interaction of extent of bodily sensations and various dependent variables, including beverage induced changes in heart rate, sedation, stimulation, and meta-cognitive interoception across condition (alcohol vs placebo). Time points are denoted as t1 (10 min postadministration; ascending limb), and t3 (approximately 75 min postadministration; descending limb).
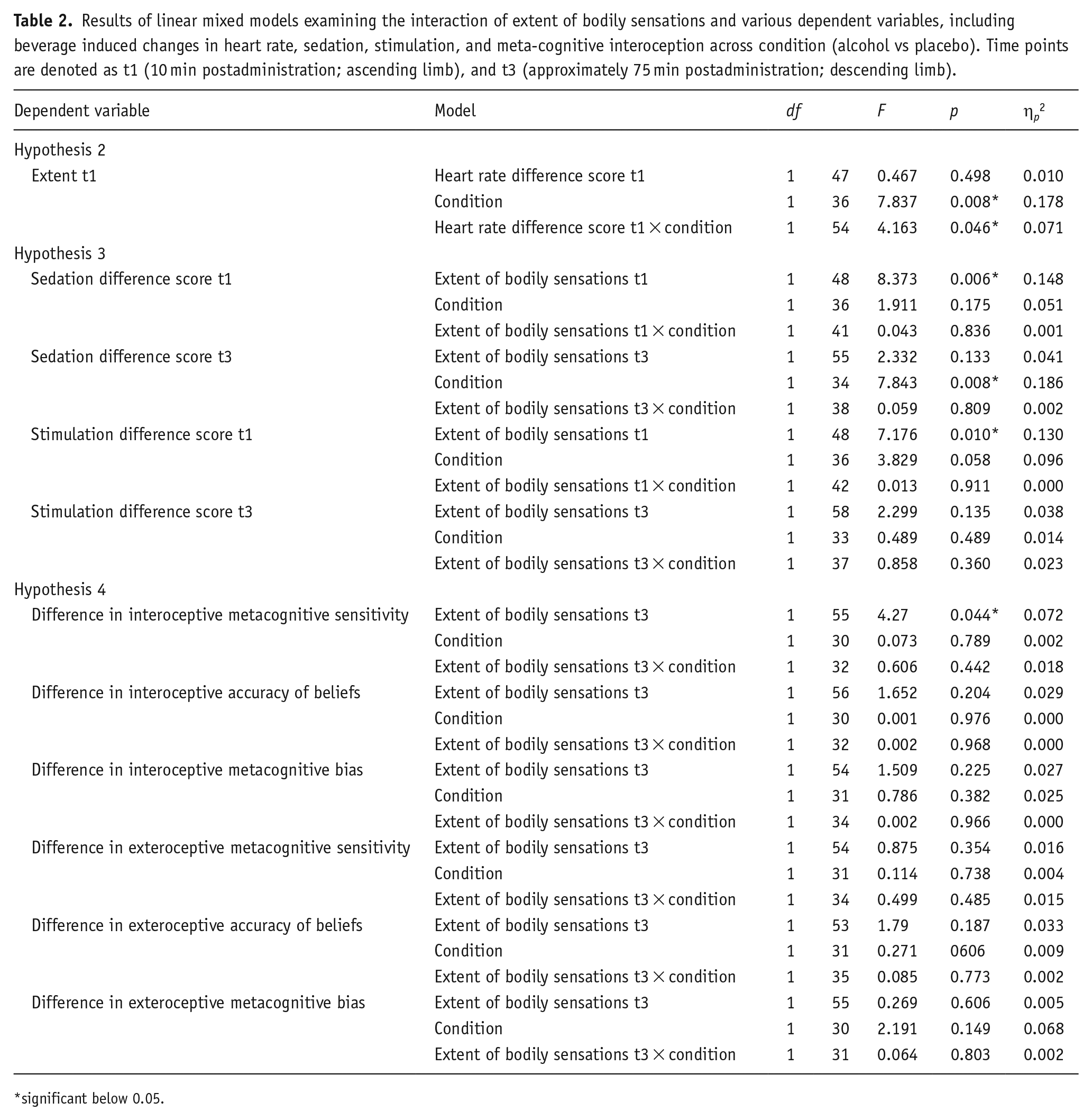
significant below 0.05.
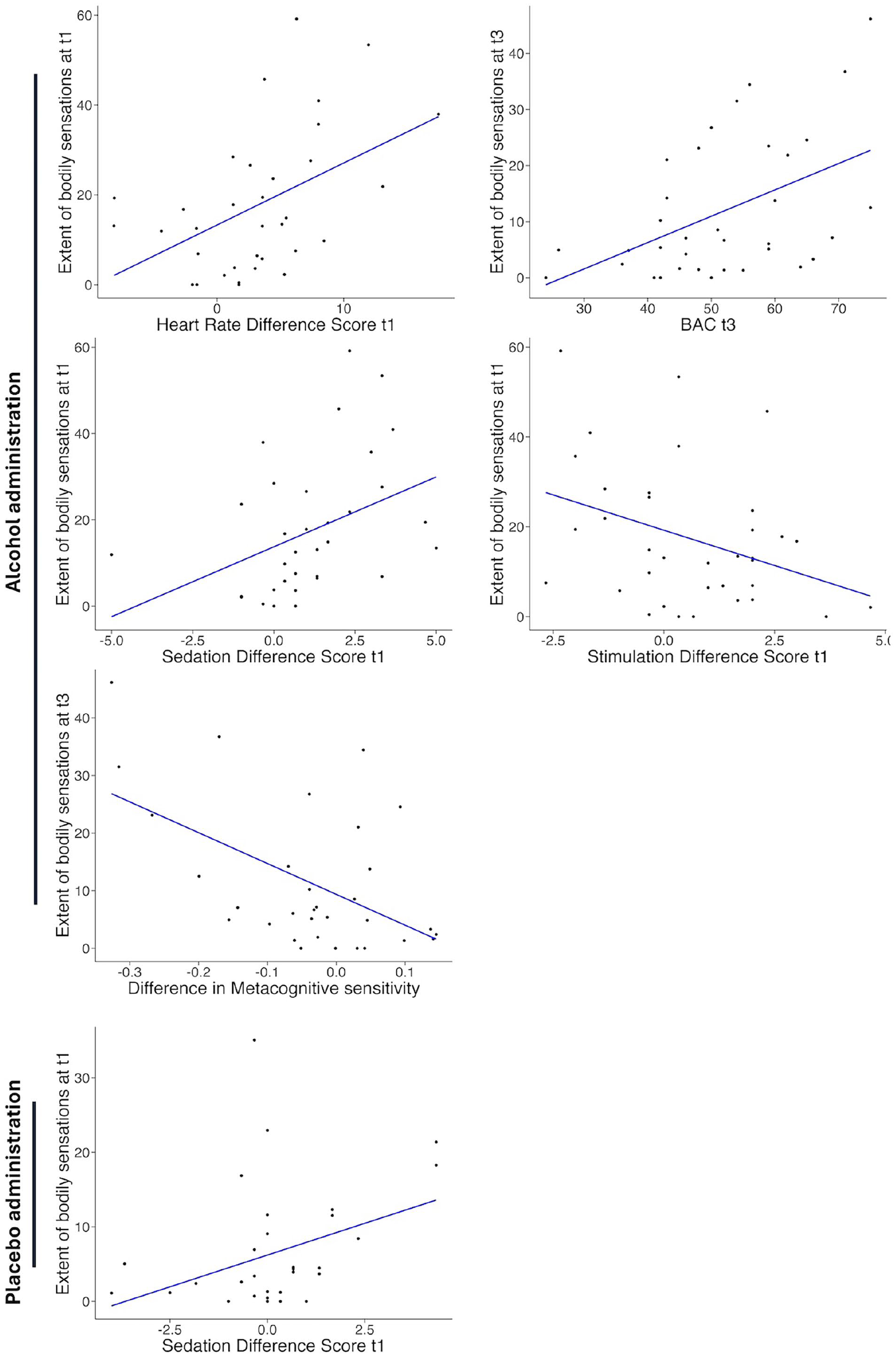
Scatterplots illustrating the interactions between the extent of bodily sensations at different time points and BrAC, as well as changes in sedation, stimulation, and meta-cognitive interoception following alcohol (top) and placebo administration (bottom). Time points are denoted as t1 (10 min post-administration; ascending limb), t2 (30 min post-administration), and t3 (approximately 75 min post-administration).
Hypothesis 2 tested the relationship between physiological markers of intoxication, including changes in heart rate and BrAC, and the corresponding extent of bodily sensations. At t1, a LMM revealed a significant interaction between heart rate difference scores (post- minus pre-beverage) and condition, indicating that alcohol modulates the relationship between heart rate changes and bodily sensations differently from placebo. Follow-up Pearson correlations revealed a significant positive relationship between changes in heart rate and extent of bodily sensations in the alcohol condition, r(32) = 0.475, p = 0.005, but not in the placebo condition (p = 0.17). For BrAC, Pearson correlations showed a significant positive relationship at t3 (descending limb) between BrAC and bodily sensations, r(27) = 0.415, p = 0.025. No significant correlations were found at t1, p = 0.857.
Hypothesis 3 tested the relationship between B-BAES scores for sedation and stimulation, computed as difference scores from baseline to each time point, and the corresponding extent of bodily sensations. At t1, after removing an extreme outlier with negative changes in sedation but high bodily sensations in the placebo condition, a LMM showed a significant main effect of bodily sensations on sedation. Follow-up analyses showed significant positive relationships between bodily sensations and changes in sedation in both the alcohol, r(28) = 0.414, p = 0.023, and the placebo condition, r(28) = 0.373, p = 0.039. For stimulation, we found a significant main effect of bodily sensations. Follow-up analyses revealed a significant negative relationship between bodily sensations and changes in stimulation in the alcohol condition, r(28) = −0.428, p = 0.015, but not in the placebo condition, r(28) = −0.300, p = 0.096.
This result partially contradicts the expected effect of higher stimulation in the ascending limb. Despite these unexpected correlations, an exploratory t-test confirmed that stimulation scores were higher than sedation scores at t1, t(31) = 2.932, p = 0.006. At t3, we found no significant main effects or interactions between changes in bodily sensations and sedation or stimulation.
Hypothesis 4 explored the relationship between changes in cardiac interoceptive beliefs (postbeverage minus baseline) and bodily sensations at t3, immediately after each postbeverage HRD measure. Alcohol’s effects on exteroceptive performance were also examined as a control. LMMs focused on metacognitive sensitivity (correspondence between accuracy and confidence), accuracy of beliefs, and metacognitive bias (average confidence) as dependent variables. For interoceptive metacognitive sensitivity, we found a significant main effect of extent of bodily sensations, but no significant interaction between condition and extent bodily sensations. Despite the nonspecificity of these results, exploratory follow-up analyses revealed a significant negative relationship between bodily sensations and changes in metacognitive sensitivity in the alcohol condition, r(28) = −0.500, p = 0.005, but not in the placebo condition, p = 0.55. No other significant main effects or interactions were observed for interoceptive or exteroceptive performance variables.
Due to observed sex differences in the effects of alcohol on the subjective number of drinks consumed, we conducted an exploratory LMM examining the effect of extent of bodily sensations across conditions while accounting for sex and subjective number of drinks consumed. No significant interaction or main effect emerged, beyond a main effect of condition (p < 0.001). Furthermore, subjective number of drinks did not significantly predict any of the dependent variables (ps > 0.16), suggesting that extent of bodily sensations is a stronger predictor of subjective intoxication (e.g., sedation, stimulation) than the perceived number of drinks consumed.
Discussion
We explored acute alcohol effects on interoception from a phenomenological perspective. Using bodily maps, we obtained a topographical representation of bodily sensations during intoxication, revealing unique activation patterns across ascending and descending limbs. In the ascending limb, alcohol mostly triggers subjective activation in the chest, accompanied by sensations in the head and arms, and decreased sensations in the belly. Toward the descending limb, feelings of activation dissipate, leading to increased sensations of deactivation. These results contrast with previous research that assessed intoxication-related bodily sensations through retrospective self-reports (Nummenmaa et al., 2018). In that study, participants reported large activations in the head and limbs, but no activation patterns appeared in the torso area. However, because that study only used retrospective accounts of 100 feeling-states, it did not capture the acute sensations experienced during intoxication. These contrasting results might be due to a higher salience of some of those bodily sensations in the long term, or the inherent discrepancies between naturalistic alcohol administration, in which drinkers do not necessarily consciously reflect on broader bodily sensations, and a laboratory setting in which they were asked to observe those sensations without distraction.
We found a relationship between extent of bodily sensations and changes in heart rate at t1 and BrAC at t3 as physiological markers of intoxication. We propose that the intense and immediate effects of alcohol on heart rate and other components of the sympathetic nervous system are reflected in increased bodily sensations during the ascending limb, regardless of BrAC, whereas during the descending limb bodily sensations reflect individual differences in alcohol metabolic rates. This first phenomenological examination of the psychophysiological correlates of such bodily sensations exemplifies how physiological states are indeed integrated in the higher-order perception of bodily sensations. Bodily maps can thus offer a phenomenological counterpart to the physiological changes triggered by substances and other environmental demands.
Regarding how bodily sensations relate to subjective feelings of sedation and stimulation, our findings highlight that the extent of these sensations plays a notable role during the ascending limb of alcohol administration. As is common, alcohol initially produced stimulating effects before shifting to predominantly sedating effects throughout the descending limb (Hendler et al., 2013), and these changing subjective states have been found to be partly driven by physiological fluctuations such as heart rate (Brunelle et al., 2007; Vatsalya et al., 2014). In our view, the measures of sedation (e.g., feeling sedated, sluggish, or slow in thought) and stimulation (e.g., feeling energized, excited, or up) used here primarily capture the cognitive dimension of subjective alcohol’s effects. We propose that bodily sensations can provide a critical link between physiological changes and the subjective experiences of intoxication, integrating somatic and cognitive aspects into a unified alcohol effect profile.
Moreover, we interpret our results within the Differentiator Model (Newlin and Thomson, 1990), which posits that individuals who experience relatively heightened stimulation and reduced sedation in response to alcohol are at elevated risk for developing AUD. Importantly, our bodily mapping approach expands this model by suggesting that individuals who report fewer bodily sensations during intoxication exhibit enhanced stimulation and diminished sedation, thereby potentially increasing their risk for problematic drinking. Existing research emphasizes that those with low levels of responsiveness to alcohol’s effects (i.e., requiring more drinks before feeling intoxicated) are at higher risk for AUD (Morean and Corbin, 2010; Quinn and Fromme, 2011; Schuckit, 2022). Yet, such findings predominantly rely on self-reports focused on cognitive aspects of alcohol use. We argue that insensitivity to the bodily dimension of intoxication may be an essential endophenotypic risk factor for AUD, one that underlies and shapes higher-order cognitive evaluations of alcohol effects. Future studies should clarify these interrelationships, investigate the predictive role of bodily sensations in the development of AUD, and examine how these factors evolve with repeated drinking experiences (Kohen et al., 2024).
Under the placebo condition, participants displayed similar activation patterns during the ascending limb, particularly at t1, based on visual inspection of bodily maps and confusion matrices. However, these patterns were not associated with any changes in physiological markers (e.g., heart rate). As the limb progressed, the placebo-related sensations gradually diminished, suggesting that prior intoxication experiences shape early placebo responses before expectancies give way to actual BrAC effects around t3. Moreover, given that the strongest placebo effects emerged during the ascending limb, when symptoms such as tiredness or boredom are unlikely to have set in, and considering our explicit double-blind protocol (informing participants that they would receive different doses of alcohol on both sessions), the observed responses are more consistent with alcohol expectancies rather than generalized nonspecific sedative effects. While previous studies have examined placebo responses using sham irritants and laser stimulation (Beissner et al., 2015) using basic mapping methods, this marks the first application of the emBODY tool to examine placebo effects. Integrating advanced bodily mapping techniques thus provides a promising way to uncover the mechanisms of placebo and nocebo phenomena, potentially bridging knowledge gaps in pharmacological alcohol research and enhancing therapeutic potential of placebos (Enck et al., 2017).
We also observed that bodily sensations correlated with feelings of sedation at t1 and t3 in the placebo condition, suggesting that placebos can elicit somatic responses akin to intoxication. This effect may be understood through classical conditioning, in which bodily sensations of intoxication function as an unconditioned response, triggered by beverage administration over repeated exposures. Over time, cues like taste and smell become linked to these somatic experiences (Bevins and Besheer, 2014; Leganes-Fonteneau, 2024a). As a result, administering a placebo that mimics these cues can reinstate the familiar bodily sensations, triggering in turn subjective feelings of intoxication even in the absence of pharmacological effects. Viewed through a predictive processing lens (Clark, 2023; Seth, 2013, 2021), these findings highlight how placebo effects may arise from an alignment of embodied and subjective experiences, underscoring the powerful role of learned expectations in shaping intoxication responses.
Beyond its implications for psychopharmacology and addiction research, our findings enrich the framework of basic interoceptive research. Interoception encompasses various taxonomical levels, ranging from high-order perceptions of bodily signals and interoceptive beliefs to objective measures like cardiac detection tasks, down to low-order psychophysiological indices (Suksasilp and Garfinkel, 2022). However, these indices often fail to converge; for instance, cardiac measures of interoception do not reliably align with self-reported questionnaire data (Ainley and Tsakiris, 2013; Garfinkel et al., 2015; Slotta et al., 2021). In contrast, here we observed that the extent of bodily sensations at t3 was associated with shifts in interoceptive metacognitive sensitivity, while no effects were observed in exteroceptive performance. It thus seems that the stronger the impact of alcohol on subjective bodily experiences, the easier it is for subjects to metacognitively evaluate their own interoceptive abilities, implying a convergence between high-order interoceptive dimensions. The linkage between the extent of bodily sensations and alterations in metacognitive sensitivity for cardiac interoception effectively bridges disparate interoceptive dimensions, substantiating the validity of both bodily mapping techniques and the heartrate discrimination task in the assessment of high-order interoceptive processing, while nonsignificant results were obtained for accuracy of beliefs, metacognitive bias, or any exteroceptive control measure. Together with the psychophysiological correlates of bodily sensations, and the subjective feelings of intoxication, this brings forth evidence for a cross-dimensional integration of multiple interoceptive processes via bodily mapping.
Limitations
The present study is a secondary analysis of an existing dataset, and we lacked statistical power to compute fine-grained analyses and examinations of the different patterns of activation underlying subjective feelings of intoxication (i.e., sensations in the head might support feelings of sedation, whereas sensations in the chest could correlate with perceived stimulation). To address this and other limitations (e.g., lack of ECG measurement throughout the response curve, different dosages), a follow-up study is warranted. Alternatively, given the ease of implementation and the rapid administration of the emBODY tool, a collaborative effort across multiple laboratories to integrate this measure into experimental protocols could offer a more effective approach to understanding these dynamics.
In this protocol, participants completed a measure of cardiac interoception at baseline on the first session and at t3 on each session. This task may have generated an interoceptive priming, whereby participants are more likely to focus on their bodily sensations, particularly on the heart and in the descending limb, affecting their perceived bodily sensations. This interoceptive priming effect could be compounded to the repetition of bodily maps. However, since bodily sensations directly correlated with psychophysiological markers at both t1 (heart-rate) and t3 (BrAC), any interference by interoceptive priming might be residual. Additionally, only a single baseline measurement of the HRD was obtained (session 1), which limits the validity of computing difference scores (postbeverage minus baseline) for both sessions. However, our data reveal substantial interindividual variability in baseline metacognitive sensitivity (Leganes-Fonteneau, 2024a), reflecting individual’s differences in interoceptive capacity. These inherent differences may obscure the interpretation of raw postbeverage scores. Therefore, despite its limitations, the use of difference scores provides a more sensitive measure of beverage-related change by accounting for each participant’s initial sensitivity.
We also note several limitations regarding our alcohol administration protocol. First, sex differences in bodily sensations and subjective effects should be explored in future research, particularly when using a uniform dose across participants. However, our sample was likely underpowered to detect robust between-group differences in these sensations and their underlying physiological mechanisms. Moreover, participants completed the experiment at varying times of day, ranging from 11:00 AM to 3:00 PM, and may have used other substances (e.g., nicotine, caffeine), both of which could influence the results. Future studies should implement tighter controls or standardized procedures to account for these potential confounds.
Conclusion
We proposed an innovative approach to demonstrate that a large range of bodily sensations emerge at the phenomenological level during alcohol intoxication and can be efficiently measured using bodily maps. Such subjective bodily sensations are not only underpinned by robust psychophysiological mechanisms but also guided by previous experiences and expected effects of alcohol, as illustrated by the bodily maps related to placebo (Leganes-Fonteneau, Bates, et al., 2021a; Leganes-Fonteneau, 2024a). Increasing evidence suggests that interoceptive processes and bodily sensations can serve as valuable markers for individual differences in alcohol responsiveness, particularly as low sensitivity to alcohol effects has been linked to a heightened risk of AUD (Morean and Corbin, 2010; Quinn and Fromme, 2011; Schuckit, 2022). Further research is needed to elucidate the potential of bodily responses as predictors of future drinking behaviors, using bodily maps as a cross-dimensional integrator of multiple interoceptive processes.
Footnotes
Author contributions
ML-F: Conceptualization Data curation, Formal analysis, Funding acquisition Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft. OD: Formal analysis, Visualization, Writing – review and editing. MGA: Writing – review and editing. RWW: Writing – review and editing. PM: Writing – review and editing.
Data availability
Upon publication of the manuscript data will be made available on OSF together with additional measures obtained during the experiment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by New Jersey NJ Institute for Food, Nutrition and Health. Dr. Leganes-Fonteneau is funded by a Marie Curie-Sklodowska fellowship and the FNRS Charge de Recherche scheme. Dr. Desmedt is funded by the Swiss National Science Foundation (SNSF) and the Swiss Foundation for Alcohol Research (SSA).
Ethical considerations
Ethical clearance was provided by the Rutgers University Institutional Review Board.
Consent to participate
All participants provided written informed consent.
Consent for publication
Not applicable.