
Abstract
Background:
Clozapine has anti-suicidal properties and significant effects on sleep. Sleep disturbances are associated with suicide risk. Daytime somnolence and sedation are commonly reported adverse effects of clozapine treatment.
Aims:
Systematic review and meta-analysis of somnolence in randomized controlled trials (RCTs) of patients with schizophrenia treated with clozapine.
Methods:
We systematically searched PubMed, PsycINFO, and Web of Science databases. We included RCTs, in English, with data on somnolence in patients with schizophrenia treated with clozapine versus other antipsychotics. Data were pooled using a random effects model.
Results:
Twenty-two RCTs (2991 patients: 1404 on clozapine and 1587 on other antipsychotics) met inclusion criteria. Patients treated with clozapine had a significantly increased odds of somnolence compared to other antipsychotics (36.3% vs 21.9%, OR = 2.06, 95% CI: 1.65–2.57, p < 0.01). Clozapine was also associated with significantly increased odds of somnolence compared to olanzapine and risperidone. In meta-regression analyses, clozapine dose, age, sex, race, and publication year were unrelated to the association.
Conclusions:
Clozapine is associated with significantly more somnolence, compared to other antipsychotics. A greater mechanistic understanding of associations between sleep changes and suicide risk in patients treated with clozapine is needed.
Introduction
Clozapine is protective against suicide in patients with schizophrenia compared to other antipsychotics, and it is the only antipsychotic with the Food and Drug Administration (FDA)-recognized indication for reducing the risk of suicide in patients with schizophrenia (Meltzer et al., 2003; Pompili et al., 2016). The mechanism of this association is unknown, but clozapine’s effect on sleep parameters has been suggested as a possible contributing factor to this relationship. There is meta-analytic evidence that insomnia is an indicator of suicide risk in schizophrenia (McCall and Miller, 2023) and that clozapine is associated with less insomnia compared to other antipsychotics (Miller et al., 2023). Using data from the U.S. FDA Adverse Event Reporting System, compared to clozapine, other second-generation antipsychotics were associated with a significantly increased reported odds ratio (rOR) of both insomnia and suicidal ideation and behavior as a suspected psychiatric adverse drug reaction, and these rORs were positively correlated (Miller and McCall, 2022). Furthermore, a secondary analysis of data from the Clinical Antipsychotic Trials of Intervention Effectiveness schizophrenia trial found that improved terminal insomnia was associated with the resolution of suicidal ideation after clozapine treatment (Vayalapalli et al., 2024).
However, daytime somnolence and sedation are also commonly reported adverse effects of clozapine treatment (Flanagan et al., 2020; Iqbal et al., 2020). Prolonged sleep duration as an adverse drug reaction has been associated with lower satisfaction in patients taking clozapine (van der Horst et al., 2025). Whether clozapine is associated with more somnolence compared to other antipsychotics has not been extensively explored. We performed a meta-analysis of randomized controlled trials (RCTs), hypothesizing that compared to other antipsychotics, there is an increased odds of somnolence in patients with schizophrenia treated with clozapine.
Methods
Study selection
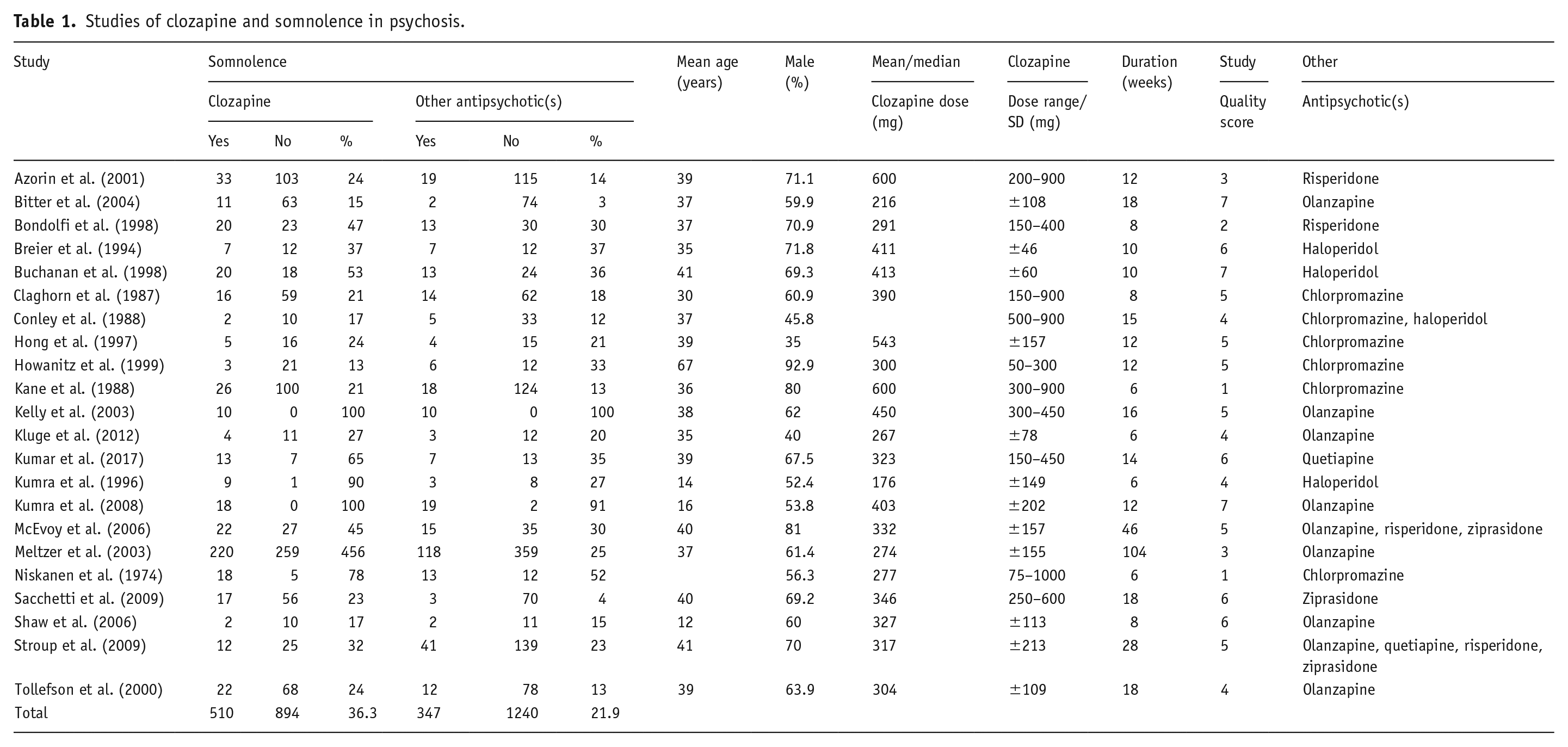
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Page et al., 2021). Studies reporting on somnolence in RCTs of patients with schizophrenia treated with clozapine were systematically searched using PubMed (National Center for Biotechnology Information, U.S. National Library of Medicine, Bethesda, MD, USA), PsycINFO (via Ovid, American Psychological Association, Washington, DC, USA), and Web of Science (Clarivate, London, UK) from inception through August 2024. The primary search strategy was “clozapine AND (schizophrenia OR psychosis),” limiting to title/abstract searches and RCTs where possible. The inclusion criteria were as follows: (1) RCTs of clozapine versus at least one other antipsychotic in adult patients with schizophrenia and/or schizoaffective disorder; (2) data on somnolence, sedation, sleepiness, or drowsiness were available (typically reported as adverse events, herein referred to collectively as “somnolence”); (3) published studies; and (4) studies in English. The exclusion criteria were as follows: (1) studies without a non-clozapine antipsychotic group; (2) studies that did not present data on somnolence, sedation, sleepiness, or drowsiness; and (3) significant overlap in study population. Independent searches were performed by two authors (MRH and BJM), 791 titles and abstracts were screened, and 22 studies were identified for inclusion and summarized in Table 1. The reference lists of these studies were also reviewed. A flow chart summarizing the study selection process is presented in Figure 1. Each of the included studies was assigned a “Quality score” after assessment for the presence of certain factors (one point for each): whether the study considered potential effects of age, sex, race, socioeconomic status, weight or BMI, smoking, substance use, baseline psychopathology ratings, by either (1) matching subjects in the clozapine and non-clozapine groups or (2) controlling for these variables after analysis. Studies with a defined clozapine titration schedule received one additional point toward the quality score.
Studies of clozapine and somnolence in psychosis.
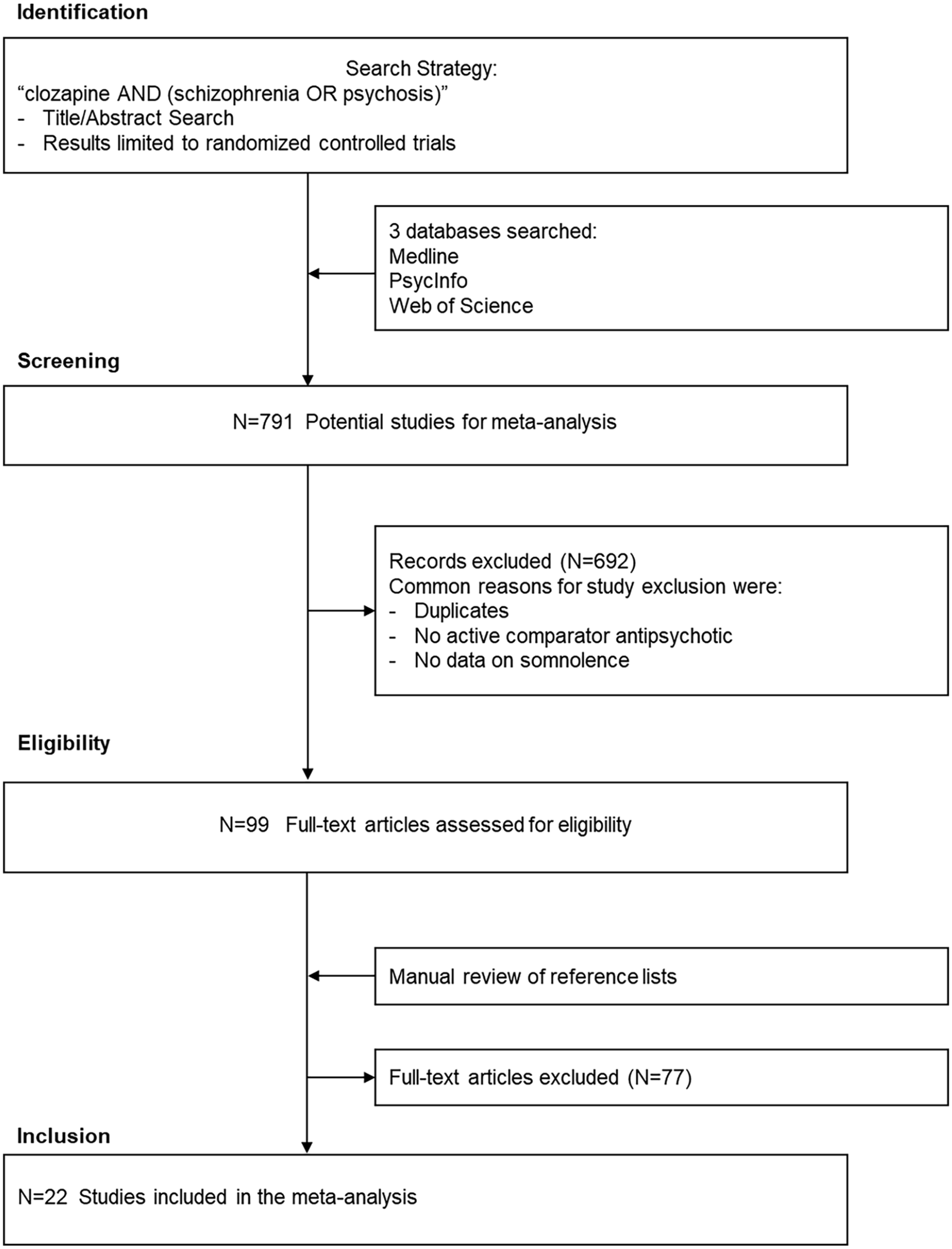
Flowchart of the study selection process.
Data extraction and meta-analysis
Data on sample size and the number of subjects with somnolence for patients treated with clozapine and other antipsychotics were extracted for each study. We also extracted descriptive data on age, mean clozapine dose, sex, race, and geographical site. One author (MRH) extracted the data, which was independently verified by another author (BJM). Effect size estimates (odds ratios (ORs) and 95% confidence intervals (95% CIs)) were aggregated utilizing the random effects method (DerSimonian and Laird, 1986). Random effects methods are considered to provide a more conservative estimate of the average weighted effect size (Field, 2001). In secondary analyses, we repeated the meta-analysis procedure for studies of clozapine versus individual antipsychotics considered separately. The meta-analysis procedure also calculates a τ2 value for between-study variance, and I2, the proportion of the variation in effect size attributable to between-study heterogeneity. We also performed meta-regression analyses to explore possible moderating effects of age, sex, race, mean clozapine dose, and year of publication on the association between clozapine and somnolence. Sterne’s funnel plot analysis and Egger’s test were used to examine for potential publication bias (Sterne and Egger, 2001). The statistical analyses were performed in Stata 17.0 (StataCorp LP, College Station, TX, USA; StataCorp, 2007). All statistical tests were two-sided, and p-values were considered statistically significant at the α = 0.05 level.
Results
We identified 22 trials, comprising 2991 patients with schizophrenia (including 1404 patients treated with clozapine and 1587 patients treated with other antipsychotics) for inclusion in the meta-analysis. Additional details regarding the clinical study populations, details of clozapine treatment, and assessment of somnolence are also presented in Table 1. Specific details on the assessment of somnolence were generally not provided, beyond being reported in the list of “adverse events.” Twenty of the 22 trials included patients with inadequate response or intolerance to previous antipsychotic trials. The other two trials were conducted in elderly patients with chronic schizophrenia (Howanitz et al., 1999) and in patients with schizophrenia at high risk for suicide (Meltzer et al., 2003).
The mean patient age was 35.5 years, and 63% of patients were male. The mean clozapine dose was 360 mg/day (range: 176–600). In all trials combined, there was a significantly increased odds of somnolence in patients treated with clozapine compared to other antipsychotics (36.3% vs 21.9%, OR = 2.06, 95% CI: 1.65–2.57, p < 0.01) and between-study heterogeneity was not significant (τ2 = 0.03, p = 0.27; I2 = 13.9%; Figure 2(a)). As shown in Figure 2(b), there was an increased odds of somnolence in patients treated with clozapine versus risperidone (32.8% vs 17.9%, OR = 2.14, 95% CI: 1.38–3.31) and olanzapine (40.9% vs 23.6%, OR = 2.46, 95% CI: 1.94–3.12). Clozapine was associated with increased prevalence of somnolence versus other antipsychotics (chlorpromazine, haloperidol, quetiapine, and ziprasidone), but the differences were not statistically significant.
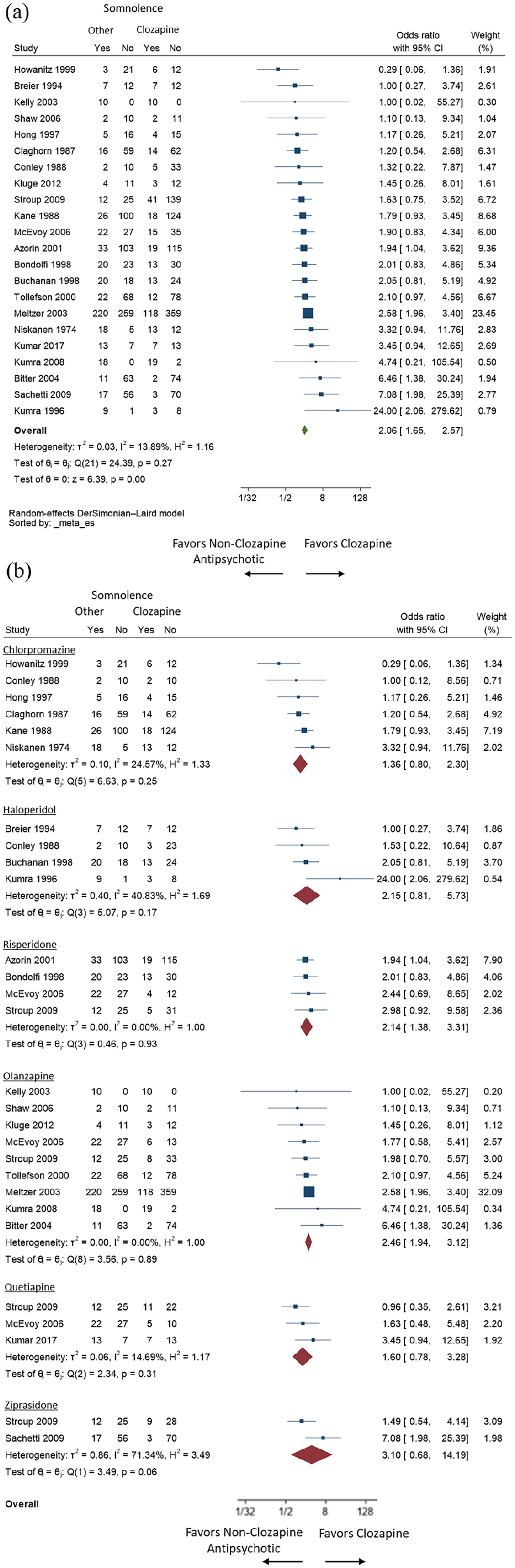
Meta-analysis of clozapine and somnolence. (a) All studies and (b) clozapine versus individual antipsychotics.
A funnel plot of all trials and Egger’s test (p = 0.88) did not suggest evidence of potential publication bias (Figure 3). In meta-regression analyses, mean clozapine dose, age, sex, race, and year of publication were all unrelated to the association between clozapine and somnolence (see Supplemental Material).
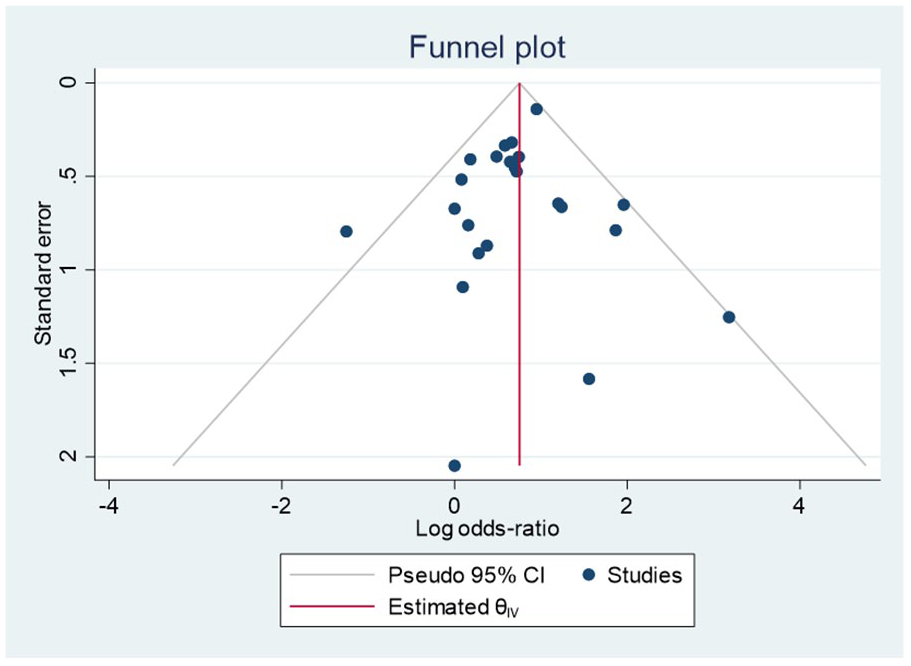
Funnel plot for all studies on the association between clozapine and somnolence.
Discussion
We performed a meta-analytic review of somnolence in RCTs of clozapine compared to other antipsychotics. We found a significant, two-fold increased odds of somnolence in patients with schizophrenia treated with clozapine compared to other antipsychotics (36.3% vs 21.9% prevalence, respectively). In an analysis of individual antipsychotics, clozapine was associated with a significantly increased odds of somnolence compared to risperidone and olanzapine. In meta-regression analyses, age, sex, race, mean clozapine dose, and year of publication were not significantly related to this association.
We believe ours is the first systematic review of somnolence in RCTs of patients with schizophrenia treated with clozapine compared to other antipsychotics. Another strength of the present study is the large sample of subjects with schizophrenia. We also performed meta-regression analyses to consider multiple potential moderating factors. One limitation of our study is that the data do not permit inferences regarding the risk of somnolence in individual patients. The reporting of insomnia in the RCTs was dependent upon investigator judgment and was not defined by research-grade diagnostic criteria for somnolence, or by somnolence severity ratings. There were considerable methodological differences in the clinical population and study design, including clozapine titration and dose. The prevalence of somnolence in individual RCTs ranged from 13% to 100% for clozapine and 3%–100% for other antipsychotics, suggesting variability in data collection procedures across studies. By contrast, several RCTs of clozapine did not report on somnolence as a potential adverse effect, and therefore could not be included in the present meta-analysis. Thus, there is the potential for a residual selection bias. There were also no objective measures of somnolence in any of the included trials. Blood clozapine levels were not available, and inter-individual variability in metabolism could explain negative findings for clozapine dose as a moderator of the association. We were not able to control for other potential confounding factors, such as other concurrent psychotropic medications and medication adherence. Regarding the latter, data were not available for comparisons between clozapine and long-acting injectable antipsychotics. The impact of these factors on the association remains unclear.
Clozapine is the only antipsychotic with an FDA indication for suicide prevention in schizophrenia (Kasckow et al., 2011). The mechanism(s) by which clozapine is associated with decreased suicide are likely complex and multifactorial, and the associated literature in this area is modest. The magnitude of the association between clozapine and somnolence in the present study (OR = 2.06) was similar to that for clozapine and insomnia (OR = 2.20) in our previous meta-analysis (Miller et al., 2023). In these studies, clozapine was associated with less insomnia and more somnolence than both risperidone and olanzapine. There is evidence that discontinuation of clozapine is associated with increases in suicidality (Masdrakis and Baldwin, 2023). A case report describes a patient with a history of highly lethal past suicide attempts stabilized on clozapine for 2 years (Patchan et al., 2015). Subsequently, clozapine was discontinued due to sedation, and the patient died by suicide 8 months later.
In contrast to findings regarding insomnia and suicide in schizophrenia (McCall and Miller, 2023; Vayalapalli et al., 2024), associations between somnolence and suicide risk in this patient population have largely been unexplored. Outside of schizophrenia, somnolence has been associated with incident suicidal behavior in pre-adolescents (Gowin et al., 2024) and excessive daytime sleepiness with incident suicidal ideation in treatment-resistant depression (Maruani et al., 2023). In subjects with a major depressive episode in the past year, those with hypersomnia and co-occurring insomnia and hypersomnia had higher rates of recent suicide attempt (Soehner et al., 2014). In this study, insomnia and hypersomnia symptoms co-occurred in over one-quarter of respondents (28%), whereas only 6% had hypersomnia without co-occurring insomnia.
In conclusion, clozapine is associated with significantly more somnolence compared to other antipsychotics. Future studies should investigate potential associations between somnolence and suicide risk in schizophrenia. A greater mechanistic understanding of associations between sleep changes and suicide risk in patients treated with clozapine is needed.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251364385 – Supplemental material for Meta-analysis of clozapine and somnolence in schizophrenia
Supplemental material, sj-docx-1-jop-10.1177_02698811251364385 for Meta-analysis of clozapine and somnolence in schizophrenia by Matthew R Hopkins and Brian J Miller in Journal of Psychopharmacology
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Matthew R Hopkins has nothing to disclose for the work under consideration. Brian J Miller has nothing to disclose for the work under consideration. In the past 12 months, he received research support from Augusta University, the National Institute of Mental Health, and the Stanley Medical Research Institute, and Honoraria from Psychiatric Times.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.