
Abstract
Background:
Whether starting antidepressants (ADs) precipitates treatment-emergent mania (TEM) in young people with major depressive disorder (MDD) is still debated. A recent nationwide cohort study found no short-term risk, but its transferability to more diverse settings is unknown.
Methods:
Using the TriNetX global electronic-health-record network, we emulated a target trial in children and adolescents aged 6–17 years with a first MDD diagnosis (2016–2024). Patients who initiated an AD within 3 months formed the exposed cohort, and those who did not served as controls. After 1:1 propensity-score matching, 105,728 participants (52,864 per group) were followed for 3 months. The primary outcome was a composite of new mania/bipolar diagnosis or lithium initiation.
Results:
The exposed group had a significantly higher risk of the primary composite outcome compared to the unexposed group (45 vs. 27 events; Hazard ratio = 1.64, 95% confidence interval, 1.01–2.63, p = 0.041). However, it lost statistical significance when disaggregating the composite outcome, in landmark time-split analyses, and when restricting the cohort to patients with a prior history of healthcare encounters.
Conclusion:
In a large, multinational real-world cohort, AD initiation was associated with a non-robust increase in short-term TEM risk. The observed association appeared susceptible to unmeasured confounding factors. These results underscore the importance of careful assessment and monitoring rather than indiscriminate AD use or avoidance in this population.
Keywords
Introduction
Major depressive disorder (MDD) in children and adolescents is a pressing global public health challenge, characterized by its escalating prevalence and status as a leading cause of disability (Ferrari et al., 2024; Yang et al., 2024). The severity of this issue is underscored by rising suicidality and its link to psychosocial risk factors such as bullying (Bertuccio et al., 2024; Serafini et al., 2023). Antidepressants (ADs) are a cornerstone of pharmacotherapy for moderate-to-severe MDD, and their use in specific contexts is supported by numerous guidelines, such as the National Institute for Health and Care Excellence (NICE) and American Academy of Child and Adolescent Psychiatry (NICE Guidance, 2019; Walter et al., 2023). However, clinicians face a profound dilemma in prescribing them, weighing the potential benefits against known risks. The most prominent of these is the U.S. Food and Drug Administration black box warning regarding an increased risk of suicidality (Center for Drug Evaluation and Research, 2018). A parallel and critical concern is the potential for antidepressants to induce treatment-emergent mania (TEM) or hypomania a complication that not only challenges the therapeutic course but may also unmask an underlying bipolar diathesis.
For decades, the evidence linking antidepressant use to the risk of TEM in children and adolescents has been conflicting. While many observational studies and even systematic reviews have suggested an increased risk (Barbuti et al., 2023; Martin et al., 2004; Melhuish Beaupre et al., 2020), they have often been hampered by methodological limitations, including small sample sizes, and many residual confounders. Against this backdrop, a recent nationwide cohort study from Sweden in 2024 challenged this prevailing view using target trial emulation (Virtanen et al., 2024). Leveraging comprehensive linked national registries, the study found no significant association between antidepressant use and an increased risk of mania within a 12-week follow-up period, observing only a weak signal at 52 weeks.
However, the generalizability of the Swedish study’s findings to other healthcare systems and populations remains an open question. Its conclusions were derived from a relatively homogeneous Swedish population, and with data ending in 2019, may not fully reflect recent shifts in clinical practice. When a well-designed study presents findings that contradict conventional wisdom, independent external validation becomes paramount. Given the ethical impediments to investigating this harm outcome through a randomized controlled trial, large-scale real-world evidence emerges as the most viable alternative. Therefore, this study aims to leverage a large, contemporary, and multi-regional electronic health record (EHR) network (TriNetX, LLC, Cambridge, MA, USA) to apply a similar target trial framework in a more diverse, global cohort of children and adolescents with depression. We hypothesize that antidepressant initiation is associated with an increased risk of mania or hypomania within 3 months in this population.
Methods
Data source and ethical considerations
This study used data from the TriNetX global federated health research network, a system that provides access to patient-level EHRs from a diverse array of healthcare organizations (HCOs). As of the data query date, TriNetX encompassed over 120 HCOs, including academic medical centers, community hospitals, and specialty care providers, primarily across the United States, but also spanning 19 other countries, representing over 275 million patient lives. The data for this study were sourced from the TriNetX “Research Network,” which includes HCOs that have agreed to participate in secondary research analyses. As a secondary analysis of pre-existing, de-identified data with no patient interaction, the study was exempt from informed consent. The study protocol received institutional review board approval through an expedited review process at Chung Shan Medical University Hospital (No. CS2-25111).
Study design and population
We conducted a retrospective cohort study using a target trial emulation framework to assess the association between antidepressant initiation and the risk of TEM or hypomania (Hernán and Robins, 2016). TEM will be defined as the first recorded International Classification of Diseases, Tenth Revision (ICD‑10) code for mania or hypomania within 3 months of antidepressant initiation (Nuñez et al., 2023). The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (Supplemental eMethod).
We extracted the study cohort data from the TriNetX Research Network between July and September 2025. We included patients aged 6–17 years who received a first-ever diagnosis of unipolar depression (MDD, single or recurrent episode; ICD-10-CM codes F32, F33.0, F33.1, F33.2, F33.3, F33.8) between January 1, 2016 (to coincide with the formal adoption of ICD-10-CM) and December 31, 2024. To identify incident antidepressant users, we required a 1-year washout period prior to the diagnosis date, during which patients had no recorded antidepressant prescriptions (Anatomical Therapeutic Chemical (ATC) code N06A).
We applied exclusion criteria to create a cohort naive to manic or psychotic symptoms. Patients with any prior diagnosis of bipolar disorder (F30, F31) or schizophrenia spectrum disorders (F2x) before the index date were excluded. Furthermore, patients with a history of lithium prescription (ATC code N05AN) at any time before the index date were also excluded. This exclusion was implemented because lithium is predominantly indicated for bipolar disorder, and its prior use may signal an underlying bipolar diathesis, even without a formal diagnosis. By contrast, aripiprazole is a more common first-line augmentation strategy for treatment-resistant depression in many settings, thus excluding lithium users helps to isolate a cohort more representative of pure unipolar depression. We did not use valproate as a proxy for mood stabilization due to the difficulty in ascertaining its specific indication (e.g., epilepsy versus mood disorder) within the database.
Exposure
The exposure group consisted of patients who initiated an antidepressant medication within 3 months of this diagnosis. For the exposure group, the index date was defined as the date of the first antidepressant initiation. The control group comprised patients who did not receive an antidepressant prescription within the same 3-month window. For the control group, the index date was the date of their initial depression diagnosis.
Outcomes and follow-up
The primary outcome was a composite event defined as either a new diagnosis of manic episode (ICD-10-CM F30, including F30.0 for hypomania) or bipolar mania (ICD-10-CM F31.0, F31.1, F31.2, F31.6, not including bipolar depression), or the initiation of lithium treatment. To enhance sensitivity and mitigate potential misclassification bias from uncoded diagnoses, a common limitation in medical record studies, lithium initiation was included as a proxy for a manic episode. The follow-up period for the outcome began at the start of exposure (or the corresponding diagnosis date for the control group) and continued for 3 months. This timeframe was chosen to capture proximate treatment-emergent events and to minimize the risk of attrition common in long-term EHR-based studies.
Covariates and propensity score matching
The baseline period for covariate assessment extended from the day before the index date up to 12 months prior. To control for confounding by indication and other baseline differences, we implemented 1:1 propensity score matching (PSM). The propensity score model included covariates selected for being potential confounders or strong predictors of the outcome. These variables included the following: demographics (age at index as continuous covariates, sex, race), socioeconomic status indicators (ICD-10-CM Z55-Z65, Persons with potential health hazards related to socioeconomic and psychosocial circumstances), healthcare utilization patterns (inpatient, outpatient, emergency, preventive, and psychiatric services), a history of suicidal ideation, suicide attempt, or intentional self-harm (ICD-10-CM R45.851, T14.91, X71-83), other psychiatric comorbidities except for mood disorder [F3x] (e.g., mental and behavioral disorders due to psychoactive substance use [F1x], neurotic, stress-related and somatoform disorders [F4x], etc.), and concomitant use of key psychotropic medications (opioids, antipsychotics, psychostimulants, antiepileptics, anxiolytics, and hypnotics/sedatives).
Negative control outcomes
To assess for potential residual confounding or systematic bias inherent in the study design, we analyzed two negative control outcomes (NCOs): acute appendicitis (ICD-10-CM K35) and fracture of the forearm (ICD-10-CM S52). These conditions are considered mechanistically unrelated to antidepressant exposure or depression. A null finding for the association between antidepressant use and these NCOs would strengthen confidence in the validity of our primary results.
Statistical analysis
Baseline characteristics were summarized for both the unmatched and matched cohorts. Balance after PSM was assessed using the absolute standardized mean difference (aSMD), with aSMD < 0.1 indicating negligible imbalance (Austin, 2009). We used a Cox proportional hazards model for the primary analysis to estimate the hazard ratio (HR) and its 95% confidence interval (CI) for the primary composite outcome. Kaplan–Meier curves were generated to visualize the cumulative incidence over the 12-week follow-up, and differences between curves were tested using the log-rank test. Patients were censored at the time of their last recorded activity in the database. We tested the proportional hazards assumption of the Cox model. A non-significant Chi-square test was interpreted as the assumption that the HR remained consistent throughout the follow-up period being met (Grambsch and Therneau, 1994). To quantify the robustness of our results, we calculated an E-value for the primary HR estimate (VanderWeele and Ding, 2017). This analysis assesses how susceptible our findings are to potential unmeasured confounding by estimating the minimum strength a hidden variable would need to have with both antidepressant use and mania to negate our results. All two-sided p-values of <0.05 were considered statistically significant. All primary statistical analyses were conducted within the TriNetX platform. The aggregate outputs used in this study reflect the platform-level handling of missing data without imputation by TriNetX.
Sensitivity analyses
To evaluate the robustness of our findings, we conducted several pre-specified sensitivity analyses. First, to address potential bias from incomplete care records, we restricted the analysis to patients with at least one recorded healthcare visit in the year prior to the first diagnosis date. Second, we performed a landmark analysis, splitting the follow-up period into 1 day to 1 month and 1–3 months, with follow-up extended to 12 months to examine the timing of risk. Third, we disaggregated the composite outcome to analyze the risk of a new mania/bipolar diagnosis separately from the risk of lithium initiation. Fourth, we repeated the analysis in the full unmatched cohort. Finally, we tested the sensitivity of the exposure definition by shortening the grace period for antidepressant initiation from 3 to 2 months.
Results
Study population and cohort selection
The cohort selection process is outlined in Figure 1. The initial query of the TriNetX database identified 149,121,297 patients. After applying age criteria (6–17 years) and requiring a diagnosis of MDD, 326,492 patients remained. The cohort was further refined by restricting the diagnosis date between January 1, 2016, and December 31, 2024, resulting in 296,472 patients. After excluding patients with a prior history of mania/schizophrenia/lithium use (N = 7720) and those with antidepressant exposure in the year prior to the index date (N = 55,760), the final eligible cohort comprised 232,992 patients. Of these, 63,913 patients initiated an antidepressant within 3 months of their MDD diagnosis and were assigned to the exposed cohort, while the remaining 169,079 patients who did not receive an antidepressant within this window formed the unexposed cohort.
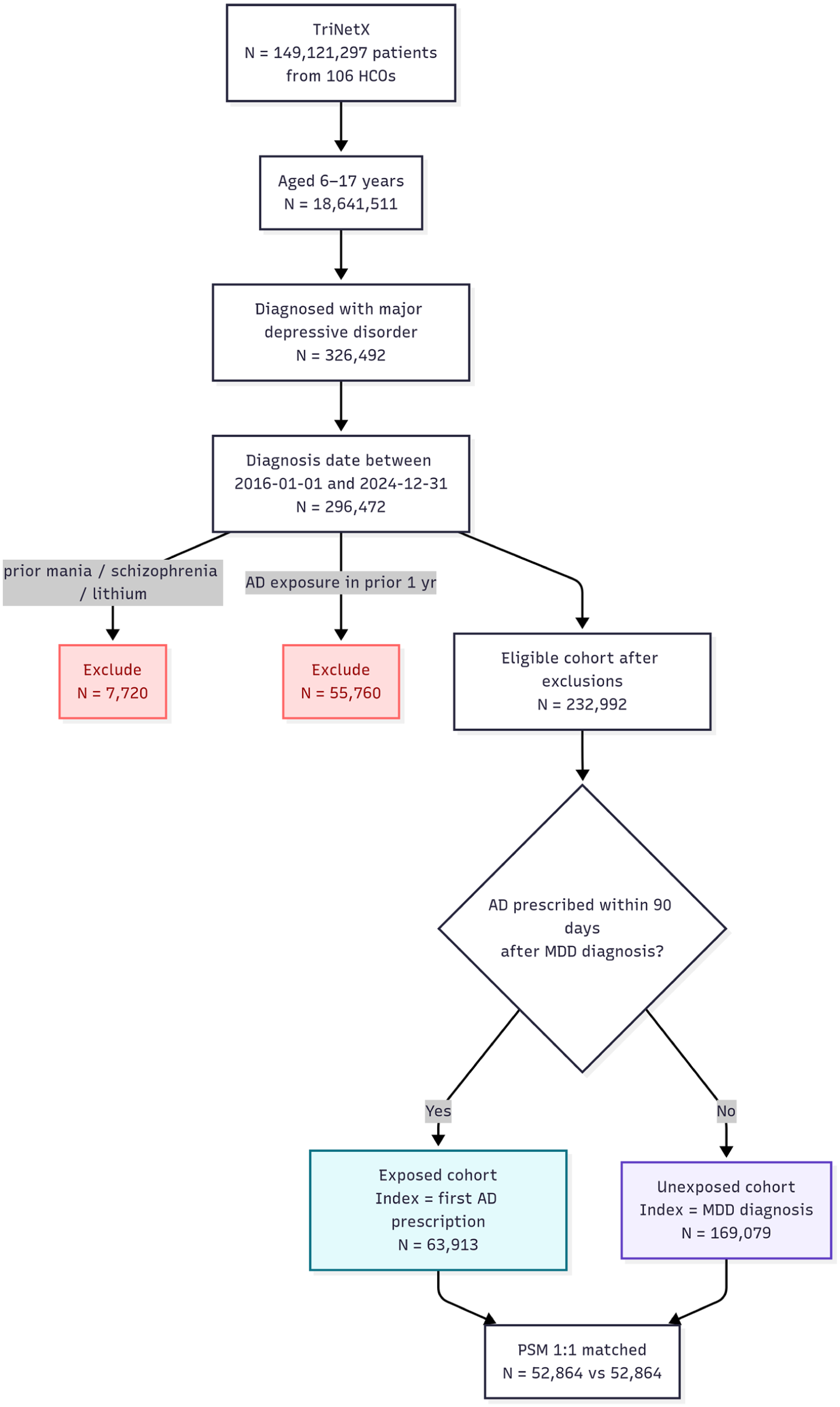
Flow diagram of study cohort selection.
Baseline characteristics and follow-up duration
Before matching, the exposed (N = 63,981) and unexposed (N = 169,106) cohorts exhibited significant differences across numerous baseline characteristics (Table 1). The exposed cohort was slightly older (mean age 13.2 vs. 12.9 years; aSMD = 0.143), had a higher proportion of White patients (67.7% vs. 56.3%; aSMD = 0.236), and a lower proportion of Black or African American patients (11.1% vs. 17.9%; aSMD = 0.194). The prevalence of comorbidities was notably higher in the exposed group, particularly for anxiety, dissociative, stress-related, and somatoform disorders (38.9% vs. 12.2%; aSMD = 0.643) and suicidal ideation (20.8% vs. 3.1%; aSMD = 0.564). The exposed group also had higher rates of healthcare utilization and concomitant use of other psychotropic medications. The propensity score distributions of the two groups were distinct before matching and showed substantial overlap after matching (Supplemental Figure 1(a) and 1(b)). After 1:1 PSM, two well-balanced cohorts of 52,864 patients each were created. Post-matching, all baseline covariates, including demographics, comorbidities, and healthcare utilization, had aSMDs below 0.1, indicating negligible imbalance between the groups. In the matched cohorts, the mean follow-up time was 75.1 days (standard deviation (SD) = 30.8) for the antidepressant group and 74.0 days (SD = 32.6) for the non-antidepressant group. The median follow-up was the full 3 months for both groups (Table 2).
Baseline characteristics of cohorts before and after propensity score matching.
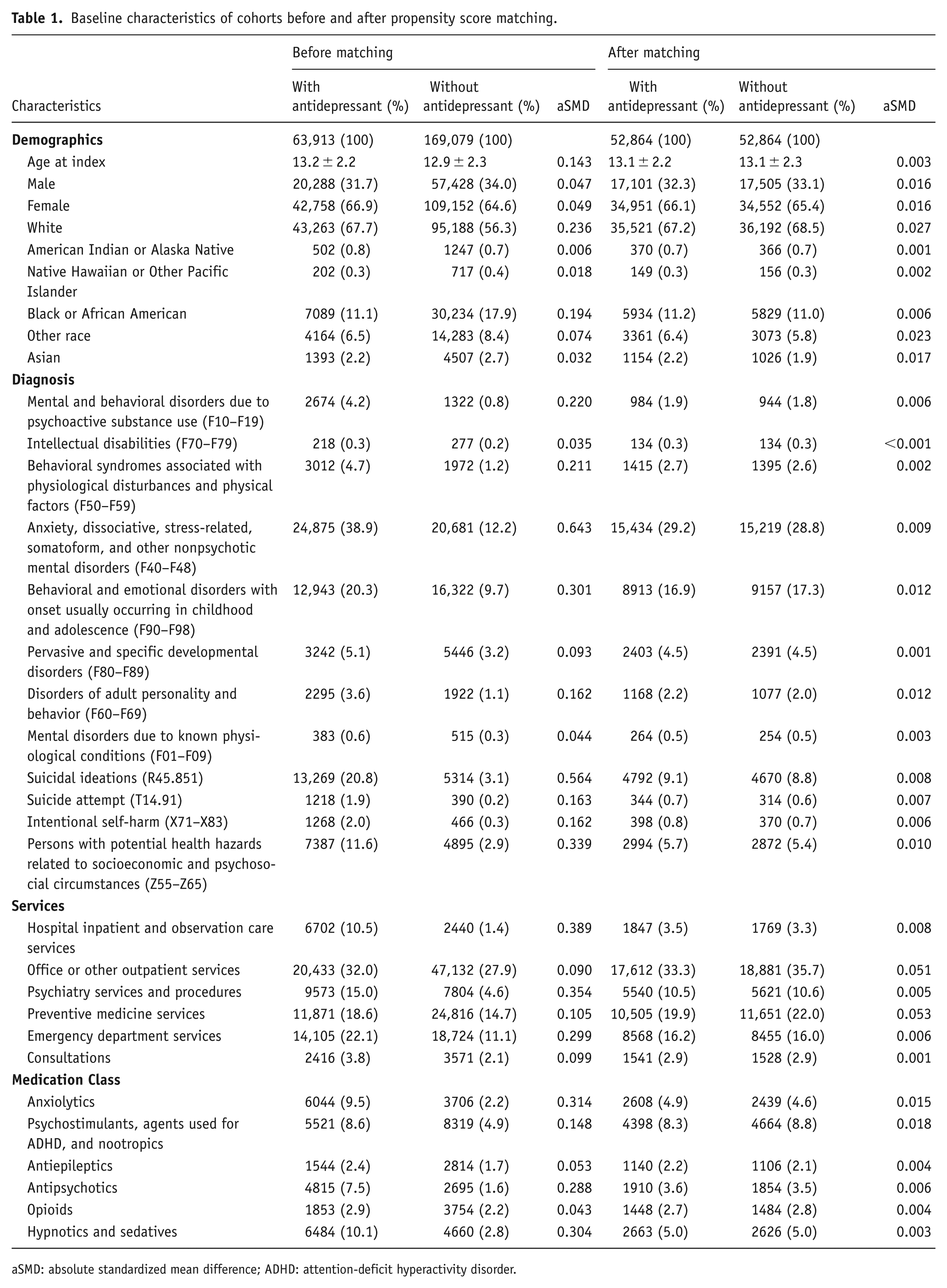
aSMD: absolute standardized mean difference; ADHD: attention-deficit hyperactivity disorder.
Follow-up duration in matched cohorts.

Primary outcome
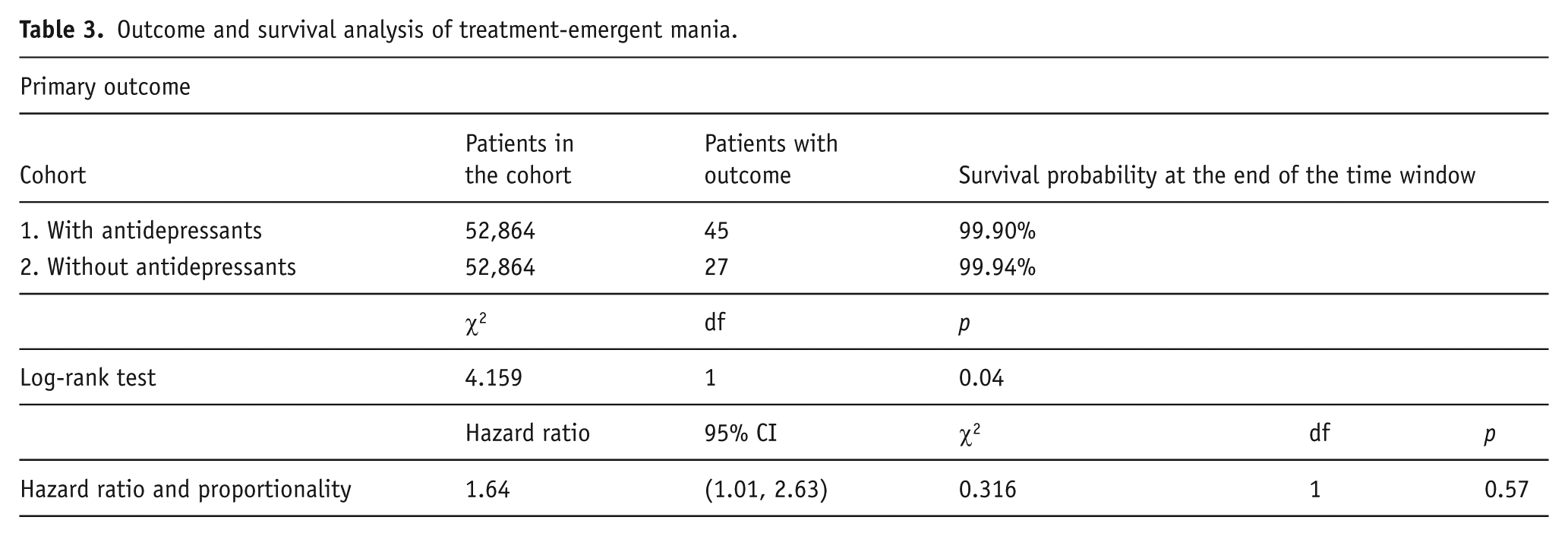
During the 12-week follow-up period in the matched cohorts, the primary composite outcome (a new diagnosis of mania/bipolar disorder or a new lithium prescription) occurred in 45 patients in the antidepressant group and 27 patients in the non-antidepressant group (Table 3). The Kaplan–Meier curve for mania-free survival (Figure 2) showed that the cumulative survival probability was lower in the antidepressant group compared to the non-antidepressant group over time. A log-rank test indicated a statistically significant difference between the two survival curves (χ² = 4.159, p = 0.041). The Cox proportional hazards model yielded a HR of 1.64 (95% CI, 1.01–2.63) for the primary outcome. The test for the proportional hazard assumption was not significant (χ² = 0.316, p = 0.574), indicating that the assumption was met. The E-value was 2.65 for the point estimate and 1.13 for the lower bound of the CI.
Outcome and survival analysis of treatment-emergent mania.
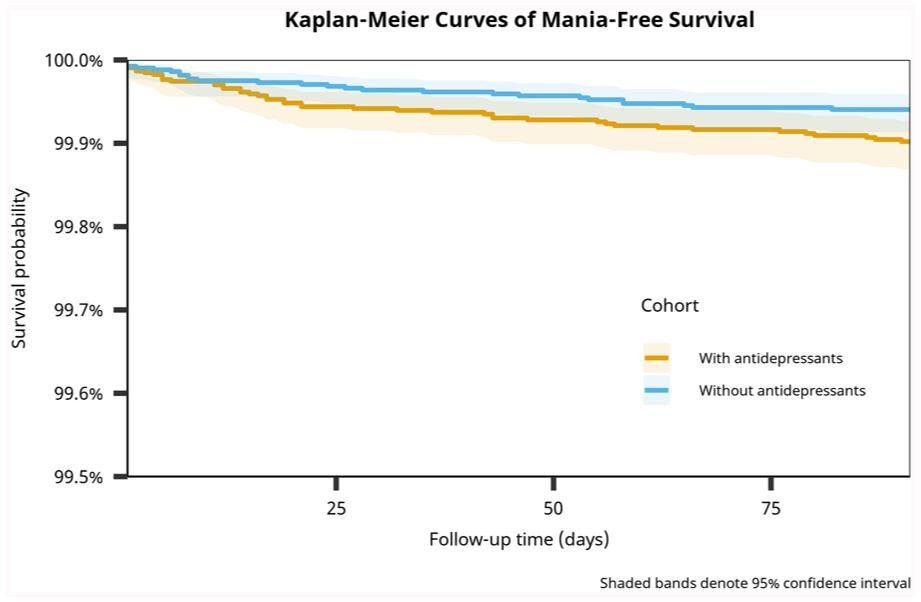
Kaplan–Meier curves of mania-free survival.
Negative control outcomes
The first negative control outcome, acute appendicitis, occurred in 28 patients in the antidepressant group versus 30 in the non-antidepressant group, with no significant difference (HR = 0.91; 95% CI, 0.55–1.53; log-rank p = 0.730) (Table 4, Supplemental Table 1). For fracture of the forearm as the second negative control outcome, there were 101 events in the antidepressant group and 108 in the non-antidepressant group, also with no significant difference (HR = 0.92; 95% CI, 0.70–1.20; log-rank p = 0.526) (Supplemental Table 2).
Summary statistics of NCOs and sensitivity analysis.
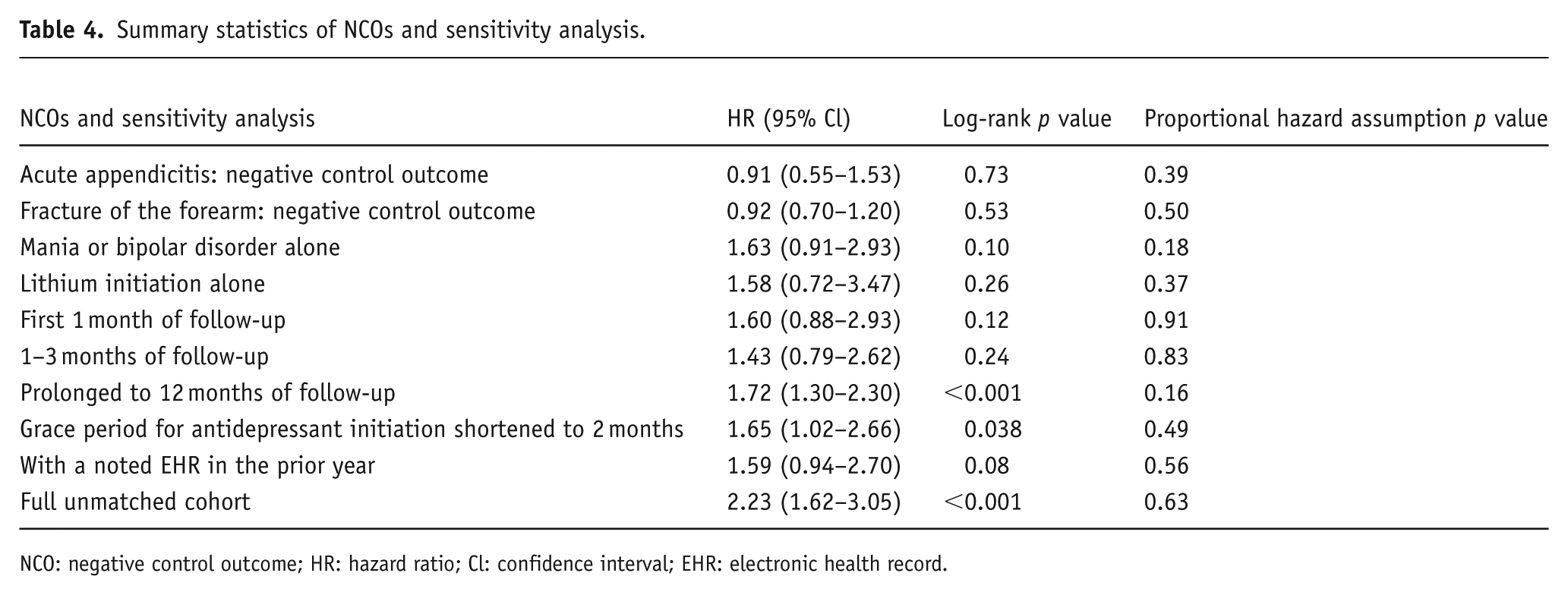
NCO: negative control outcome; HR: hazard ratio; Cl: confidence interval; EHR: electronic health record.
Sensitivity analyses
In the disaggregated outcome analysis, the risk for a new diagnosis of mania or bipolar disorder alone (30 events vs. 18 events) was not statistically significant (HR = 1.63; 95% CI, 0.91–2.93; log-rank p = 0.098) (Supplemental Table 3). Similarly, the risk for lithium initiation alone (16 events vs. 10 events) was not statistically significant (HR = 1.58; 95% CI, 0.72–3.47; log-rank p = 0.255) (Supplemental Table 4). A landmark analysis showed no significant difference in risk between groups during either the first 1 month of follow-up (HR = 1.60; 95% CI, 0.88–2.93; p = 0.121) (Supplemental Table 5) or from 1 to 3 months (HR = 1.43; 95% CI, 0.79–2.62; p = 0.238) (Supplemental Table 6). An extended follow-up to 12 months revealed a more significant effect (HR = 1.72; 95% CI, 1.30–2.30; log-rank p < 0.001) (Supplemental Table 7). When the grace period for antidepressant initiation was shortened to 2 months, the association with the primary outcome remained statistically significant (HR = 1.65; 95% CI, 1.02–2.66; log-rank p = 0.038) (Supplemental Table 8). The association became non-significant when restricting the analysis to patients with a noted EHR in the prior year (HR = 1.59; 95% CI, 0.94–2.70; log-rank p = 0.083) (Supplemental Table 9). Finally, an analysis of the full unmatched cohort yielded a significant association with a larger effect size (HR = 2.23; 95% CI, 1.62–3.05; log-rank p < 0.001) (Supplemental Table 10).
Discussion
In this large, global cohort study, we found an association between antidepressant initiation and the short-term risk of TEM in children and adolescents. However, this modest association was not robust across a series of sensitivity analyses. The persistence of HRs greater than 1.0 (≈1.4–2.2) across these analyses, even without statistical significance, may raise the possibility of an underlying effect within a specific subgroup. This instability provides a nuance to the existing literature, particularly when contrasted with the mentioned Swedish nationwide study that found no significant short-term risk (Virtanen et al., 2024).
A primary strength of the Swedish study was the homogeneity and comprehensive data linkage of its national registries, which enabled excellent control over crucial confounders like family history and socioeconomic status. This level of control likely contributed to its null finding. By contrast, while our EHR database offers advantages in population diversity and data timeliness, it cannot capture the same granular variables. The association lost statistical significance in time-stratified analyses (1 day–1 month and 1–3 months), weakening the hypothesis of a strong, time-specific effect, such as an activation syndrome (Luft et al., 2018). When the observation period was extended to 12 months, the association regained statistical significance, suggesting that different selection mechanisms may be at play over a longer timeframe. Furthermore, the association disappeared when we restricted the analysis to patients with a prior history of care. This suggests our primary result was susceptible to bias, where patients presenting for the first time with severe depression may inherently be at a higher risk for mood instability.
Although our data did not establish a robust statistical association, the clinical concern may stem from its biological plausibility. Several hypotheses provided a theoretical basis for how antidepressants might trigger mood instability in susceptible individuals. At the receptor level, the rapid increase in synaptic serotonin from selective serotonin reuptake inhibitors can over-activate receptors like 5-HT2A/2C, potentially increasing excitability in cortico-limbic circuits (Celada et al., 2013). This may be particularly relevant in adolescents, whose brains exhibit peak 5-HT2A receptor expression (Crews et al., 2007), making their excitatory/inhibitory balance more vulnerable to pharmacological perturbation. On a cellular level, antidepressants promote neuroplasticity, often via pathways like brain-derived neurotrophic factor (Madsen et al., 2024; Yang et al., 2020), but in certain individuals, this effect might be excessive, destabilizing mood-regulating circuits. At the network level, neuroimaging studies have shown that patients who experience TEM exhibit abnormal connectivity patterns such as hyperactivation of the amygdala similar to those seen in bipolar mania (Cotovio and Oliveira-Maia, 2022; Nery et al., 2020; Wang et al., 2020).
The biological mechanisms behind our statistical signal are likely not universally applicable to all children and adolescents with depression. Rather, they may pertain to a specific subgroup with a pre-existing biological vulnerability. This vulnerability may be defined by factors our data cannot identify, such as specific genotypes (Daray et al., 2010; Nuñez et al., 2023), a family history of bipolar disorder, or a depressive episode with mixed features (Bottlender et al., 2004; Olgiati and Serretti, 2023). The very individuals with this underlying vulnerability may be the first to receive pharmacotherapy, creating a biased association. Given that the reported influence of parental psychiatric history (HR ≈ 4.1 in the Sweden cohort) can exceed this threshold ( E-value ≈ 2.65 for the primary finding) (Birmaher et al., 2009; Virtanen et al., 2024), we cannot rule out that such unmeasured factors are the primary driver of the weak association we observed. Crucially, these factors likely play a dual role. While they act as confounders that can create a spurious association in our statistical model, they may also function as effect modifiers that identify the very subgroup of patients in whom a true risk may exist. In adults, meta-analytic evidence reports variable, largely context-dependent TEM risk, and a 2025 network meta-analysis found no antidepressant with a significantly higher switch risk than placebo, aligning with our data showing only a weak, non-robust short-term signal (Fornaro et al., 2018; Oliva et al., 2025).
Despite the limitations on causal inference, the clinical principle of “do no harm” remains paramount. In the face of uncertain evidence, the need to weigh potential benefits and risks when prescribing antidepressants to children and adolescents becomes even more critical. This includes the potential for mood destabilization, balanced against the known functional impairment and worsening illness course associated with untreated depression. The number needed to harm (NNH) of 2937 indicates that the absolute impact of antidepressant initiation is modest. Our findings further suggest that the risk of TEM is not a universal constant but a variable highly dependent on an individual’s baseline characteristics. This shifts the clinical focus from asking, “Will this antidepressant cause mania?” to a more nuanced question: “Is this particular patient part of a high-risk subgroup?” Given the debate about Blackbox warnings, expert reviews emphasize monitoring rather than avoiding effective antidepressants in youth (Fornaro et al., 2019). This reinforces the importance of a comprehensive pre-treatment evaluation, including careful inquiry about symptom severity and characteristics, family history, past hypomanic symptoms, and close monitoring for activation signs like agitation, insomnia, and impulsivity during the initial phase of treatment. This process is an indispensable component of shared decision-making with patients and their families.
Limitations
This study has several limitations. Our most important limitation is confounding by indication. In other words, clinical factors such as high depression severity or a family history of bipolar disorder may drive both the decision to start antidepressants and the subsequent risk of mania, yet these variables were not captured in our dataset. An additional larger dataset would allow for stratification to better address this limitation. Second, our use of a diagnosis date for the comparator group and a prescription date for the treatment group may have introduced immortal time bias. Future research could utilize individual-level data to apply methods such as marginal structural models. Third, misidentification bias is an inherent concern given the limited accuracy of EHR data. In addition, the risk of loss to follow-up poses a further challenge due to potential bias from administrative censoring. Finally, our study estimates the average treatment effect only for the specific subpopulation created by PSM, not for the entire patient population. Consequently, this design limits our ability to assess whether concomitant medications have a protective effect against TEM.
In conclusion, this study, using a large, global real-world database, found a weak and non-robust statistical association between antidepressant initiation and short-term mania risk in children and adolescents. This finding should not be interpreted as an absence of risk, but rather as one that may be concentrated within a vulnerable subgroup. Accordingly, while our results do not provide strong evidence for a causal risk, they should not discourage the use of antidepressants when clinically indicated. Vigilance remains warranted, particularly for patients with a potential underlying bipolar diathesis. Our results highlight the critical need for future research to capture more detailed clinical features to enable better risk stratification.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251389541 – Supplemental material for Antidepressant initiation and the risk of treatment-emergent mania in children and adolescents with depression: A real-world cohort study
Supplemental material, sj-docx-1-jop-10.1177_02698811251389541 for Antidepressant initiation and the risk of treatment-emergent mania in children and adolescents with depression: A real-world cohort study by Yu Chang, Ming-Hong Hsieh, Po-Chung Ju and Cheng-Chen Chang in Journal of Psychopharmacology
Footnotes
Ethical considerations
This study was conducted using de-identified patient data from the TriNetX global federated health research network. The de-identification process complies with the standards defined in Section §164.514(a) of the U.S. Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. As the research involved a secondary analysis of pre-existing, de-identified data with no direct patient interaction, it was exempt from the requirement for informed consent. The study protocol received institutional review board (IRB) approval through an expedited review process at Chung Shan Medical University Hospital (No. CS2-25111).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the TriNetX research network, but restrictions apply to the availability of these data. Data may be available from the authors upon reasonable request and with permission of TriNetX.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.