
Abstract
Introduction:
Schizophrenia is a severe mental disorder that impacts thoughts, emotions, and behavior, affecting 0.32% of the global population. While antipsychotic medications are crucial for managing symptoms, nearly half of individuals with schizophrenia experience weight gain, leading to treatment non-compliance and further health complications. Our systematic review and network meta-analysis aim to provide comprehensive evidence on the safety and efficacy of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain.
Methods:
We conducted this study in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement, following our protocol (CRD42024599597). We searched PubMed, Scopus, Web of Science, and Cochrane Library until July 2025. Only randomized placebo-controlled trials were included. We focused on anthropometric measurements and safety profiles. The primary outcome was weight change, while the secondary outcomes included waist-hip ratio, waist circumference, and hip circumference.
Result:
Fifty-five studies were included in the meta-analysis, with a total of 2977 individuals. Regarding the weight change, the highest three interventions hold the highest probability of being the most effective therapy in weight loss compared to the Usual care group were Semagultide (MD: −13.5 [−17.3, −9.57], followed by Metformin + NutriEx (MD: −6.34, [−9.85, −2.9]), then Nizatidine (MD: −5.46 [−7.77, −2.76]). According to non-pharmacological interventions, all interventions showed significant reductions in weight (p-value < 0.05).
Conclusion:
We found that Semaglutide has the highest probability of being the most effective therapy in the reduction of weight gain and BMI. Liraglutide was associated with mild adverse effects. Additional trials focusing on non-pharmacological approaches are essential.
Introduction
Schizophrenia is a serious long-term mental condition that affects how people think, feel, and behave, with a global prevalence of 0.28% (Charlson et al., 2018). It is characterized by a wide range of symptoms, including hallucinations, delusions, disorganized speech, and cognitive impairments. These symptoms can be classified into positive symptoms, such as hallucination, delusion, and disorganized behavior, and negative symptoms, such as anhedonia and alogia, which means talking less (Bitter, 2020). The cornerstone of schizophrenia management is pharmacotherapy, mainly involving antipsychotic medications; these drugs are designed to mitigate the most distressing symptoms, particularly positive symptoms (Patel et al., 2014; Savill, 2020). Despite their effectiveness, antipsychotics can lead to significant side effects, including metabolic syndrome and neurological complications, necessitating careful monitoring and management (Sabe et al., 2022; Stępnicki et al., 2018).
The impact of schizophrenia and its treatment on individuals extends beyond psychiatric disabilities, significantly affecting their physical health as well. One concerning physical issue faced by individuals with schizophrenia is weight gain, which can lead to a range of associated health complications (Connolly and Kelly, 2005; Gordon et al., 2013). This weight gain is often exacerbated by the adverse effects of antipsychotic medications, making it a clinically important concern that requires careful management to ensure the overall well-being of those affected (Qureshi et al., 2018; Varley, 2009). A meta-analysis conducted by Mitchell et al. (2013) reported that 49.4% of individuals with schizophrenia experience weight gain. Weight gain is also associated with metabolic syndrome, which includes an impairment in glucose tolerance of 19.5%, a decrease in HDL of 42.6%, and an increase in triglyceride level of 39.3% (Mitchell et al., 2013). These changes increase with the dose, and can contribute to the risk of developing hypertension, stroke, cardiovascular diseases, and even death (Olfson et al., 2015; Sabé et al., 2023). The factors that contribute to the previous problems are a sedentary lifestyle, unhealthy food habits, genetic contribution, and antipsychotic treatment.
Antipsychotic-induced weight gain (AIWG) holds significant clinical relevance due to its iatrogenic nature, resulting from the very medications prescribed to manage psychiatric symptoms (Allison et al., 1999; Lee et al., 2022; Xiao and Baker, 2010). A meta-analysis conducted by Pillinger et al. (2020) reported a maximum weight gain of 3.01 kg with clozapine and olanzapine. AIWG leads to further undesirable effects by increasing the risk of poor adherence to antipsychotic medications (Castle et al., 2017; Goff and Kreyenbuhl, 2012; Pillinger et al., 2020). Research indicates that individuals who experience weight gain are more likely to discontinue their antipsychotic treatment compared to those who maintain a stable weight (De et al., 2025). This discontinuation can lead to deteriorating clinical outcomes, compromising these individuals’ overall quality of life (Weiden et al., 2004).
Several studies have addressed the efficacy and safety of many options for managing AIWG, comprising pharmacological and non-pharmacological options (Alvarez-Jiménez et al., 2008; Baptista et al., 2006, 2007). Common pharmacological options comprise metformin, berberine, bupropion, naltrexone, naltrexone-bupropion combination, fluoxetine, amantadine, sibutramine, nizatidine, topiramate, alpha lipoic acid, topiramate, betahistine, rosiglitazone, liraglutide, fluvoxamine, phenylpropanolamine, orlistat, exenatide, probiotic, plus dietary fibers. Non-pharmacological options include behavioral therapy (BT), lifestyle, physical exercise, educational programs, and weight management programs.
Previous evidence, mainly randomized controlled trials (RCTs), focused on determining the efficacy and safety of each option compared to placebo. A comprehensive study explored the efficacy of various pharmacological options in the prevention of weight gain in individuals with schizophrenia; it only focused on pharmacological options (Agarwal et al., 2022). Systematic evidence discussed the efficacy of metformin only in the prevention and management of AIWG (de Silva et al., 2016; Fitzgerald et al., 2022). Another systematic review aimed to summarize the evidence on a limited scope, with only four options discussed in varying doses (Bak et al., 2024; Lee et al., 2022). Another systematic review discussed the evidence about the glucagon-like peptide 1 receptor (GLP-1) agonist class, especially exenatide and liraglutide (Bak et al., 2024).
Although there are a couple of RCTs and systematic reviews, there is a lack of comprehensive systematic evidence pooling the effects of all available options and comparing them to each other. In our systematic review and network meta-analysis (NMA), we aim to provide tailored evidence about the various AIWG options by providing comprehensive evidence about the efficacy and safety of the numerous options for managing AIWG compared to each other.
Methods
Registration
We followed the guidelines of PRISMA statements in this systematic review and NMA (Page et al., 2021). We conducted this study using the Cochrane Handbook of Systematic Reviews of Interventions (Cochrane Handbook for Systematic Reviews of Interventions, n.d.). This study was prospectively registered on PROSPERO (CRD42024599597).
Search strategy
Three authors independently conducted the literature search and screening (MEM, KRA, and MMH). Eligibility screening was done using Rayyan, a web-based tool designed for systematic review (Rayyan – Intelligent Systematic Review, n.d.). Studies were screened at two levels. The first level involved screening the title and abstract to ensure matching the inclusion criteria. The second level involved checking the full-text articles for eligibility to our meta-analysis criteria. In cases of disagreement between screeners, a joint review of the conflicting papers was conducted with all three authors present to reach a consensus. The search terms were a combination of keywords and MeSH terms, such as schizophrenia or psychosis, and a list of pharmacological and non-pharmacological interventions (e.g., “anti-Obesity Drugs” or physical activity). The full list of search terms can be found in the PROSPERO protocol.
Inclusion criteria and study selection
The systematic review included human studies on adult individuals (18–65 years old) with schizophrenia diagnosed with the Diagnostic and Statistical Manual of Mental Disorders criteria. The experimental groups in these studies received pharmacological interventions such as (Metformin, Metformin plus Sibutramine, Berberine, Betahistine, Nalterxone, Naltrexone plus Bupropion, Exenatide, Nizatidine, Sibutramine, Alphalipoic acid, Topiramate, Rosiglitazone, Orlistat, Fluoxetine, Amantadine, Liraglutide, Fluvoxamine, Phenylpropanolamine, Semaglutide). Some studies also involved non-pharmacological interventions, including BT, psychological nutritional education (PsyNut), and nutritional education combined with exercise (NutriEx). Control groups were given either a placebo or the standard care provided for schizophrenia, which is referred to as usual care (UC). Included studies reported outcomes related to changes in weight or BMI from baseline to the end of the study, and were all RCTs. We excluded articles that were case reports/case series, theses, conference abstracts, non-randomized trials, observational studies, healthy control studies, and studies that used preventive methods rather than therapeutic protocols, which are focused on reducing weight. Articles not available in English were excluded.
Data extraction
All authors extracted the data independently using an online data extraction form. The extracted data were mainly divided into four domains: (1) study characteristics, (2) characteristics of the included study population, (3) risk of bias (ROB) domains, and (4) study outcomes. Data were exported as a Microsoft Excel sheet. Any conflicting error was resolved by the supervisor author (MS).
Assessment of the ROB in included studies
Four authors (FA, KRA, MM, and AB) independently assessed the quality of each included study using the Cochrane ROB tool (Higgins et al., 2011). The Cochrane ROB tool was designed to assess the probability of bias in seven study scopes, including (1) random sequence generation, (2) allocation concealment, (3) blinding of the investigators and individuals, (4) blinding of the outcome assessors, (5) incomplete outcome data, (6) selective outcome reporting, and (7) other sources of bias. After careful screening of the structure and data presented in the published RCTs, in each domain, each study was stamped as “low ROB,” “high ROB,” or “unclear.” In case of disagreements between the two authors, an examination of the article was conducted in the presence of a Fifth author (MEM) to reach a consensus.
Measures of treatment effect
In studies assessing the efficacy of pharmacological and non-pharmacological interventions on anthropometric measurements. The primary outcome measurement was weight change, which is the difference in body weight from the baseline (pre-treatment) to the endpoint (post-treatment), expressed in kilograms (kg). The secondary outcomes were BMI, waist circumference, hip circumference, and waist-hip ratio. The BMI was calculated as “kg/m,” and the other outcomes were measured as “cm.”
Dealing with missing data
When the standard deviation (SD) of the mean change of included outcomes was not available, we reached by email to the corresponding authors of the given studies. In the absence of response, we imputed the SD from the 95% confidence interval (CI) according to Altman’s methods (Altman and Bland, 2005).
Data synthesis
All statistical analyses and plotting were performed using MetaInsight software version 6.4.0. We conducted a Bayesian NMA for primary and secondary outcomes using the “gemtc” R package. For safety outcomes, a frequentist framework was applied using the “netmeta” R package. Continuous data were pooled as mean differences (MDs) in the meta-analysis, while binary outcomes were analyzed using risk ratios (RRs). Both MD and RR were reported with 95% CIs to estimate effect sizes. Due to the expected high heterogeneity among the studies included, all analyses were conducted using a random-effects model.
Assessment of inconsistency and heterogeneity
We assessed inconsistency using residual plots by comparing each study’s deviation from the standard NMA model against its deviation from the Unrelated Mean Effects (UMEs) model (Spineli, 2022). This visualization facilitates the detection of inconsistency by highlighting differences in study deviations between the two models. Studies clustered closely around the origin suggest minimal deviation and indicate consistency between the NMA and UME models. Conversely, studies with larger deviations from the origin may signal inconsistency within the network.
Statistical heterogeneity among studies was evaluated using the chi-square test (Cochrane Q test). The Cochrane Q statistic was subsequently used to calculate the I-squared (I²) value according to the formula: I² = (Q − df)/Q × 100%, where df represents degrees of freedom. Heterogeneity was considered significant when the Chi-square test yielded a p-value less than 0.1.
Ranking of interventions and publication bias
We employed Surface Under the Cumulative Ranking (SUCRA) scores to rank each intervention based on its effectiveness. SUCRA values range from 0% to 100%, representing the probability that a given treatment is the most effective among all interventions. These scores are visualized using a cumulative ranking plot, where each line corresponds to a specific intervention and depicts its cumulative probability across all possible ranks. Variations in ranking over time or across scenarios indicate fluctuations in intervention effectiveness. This analysis helps distinguish interventions with consistently stable efficacy from those whose effectiveness may depend on specific contexts. We utilized funnel plots to visualize and assess asymmetry and potential publication bias, complemented by Egger’s test, where a p-value < 0.05 indicates a risk of publication bias.
Results
Results of the literature search
A total of 5844 unique articles were included in the process of literature review. Two thousand, nine hundred seventy-seven of them were identified as duplicates by Rayyan. We excluded 2777 articles by screening titles and abstracts. Ninety unique full texts were reviewed and screened for the eligibility criteria. Overall, this NMA included 55 RCTs, published between 2001 and 2025. All article references are provided in the Supplemental tables file. The PRISMA flow diagram of the study selection process is shown in Figure 1.
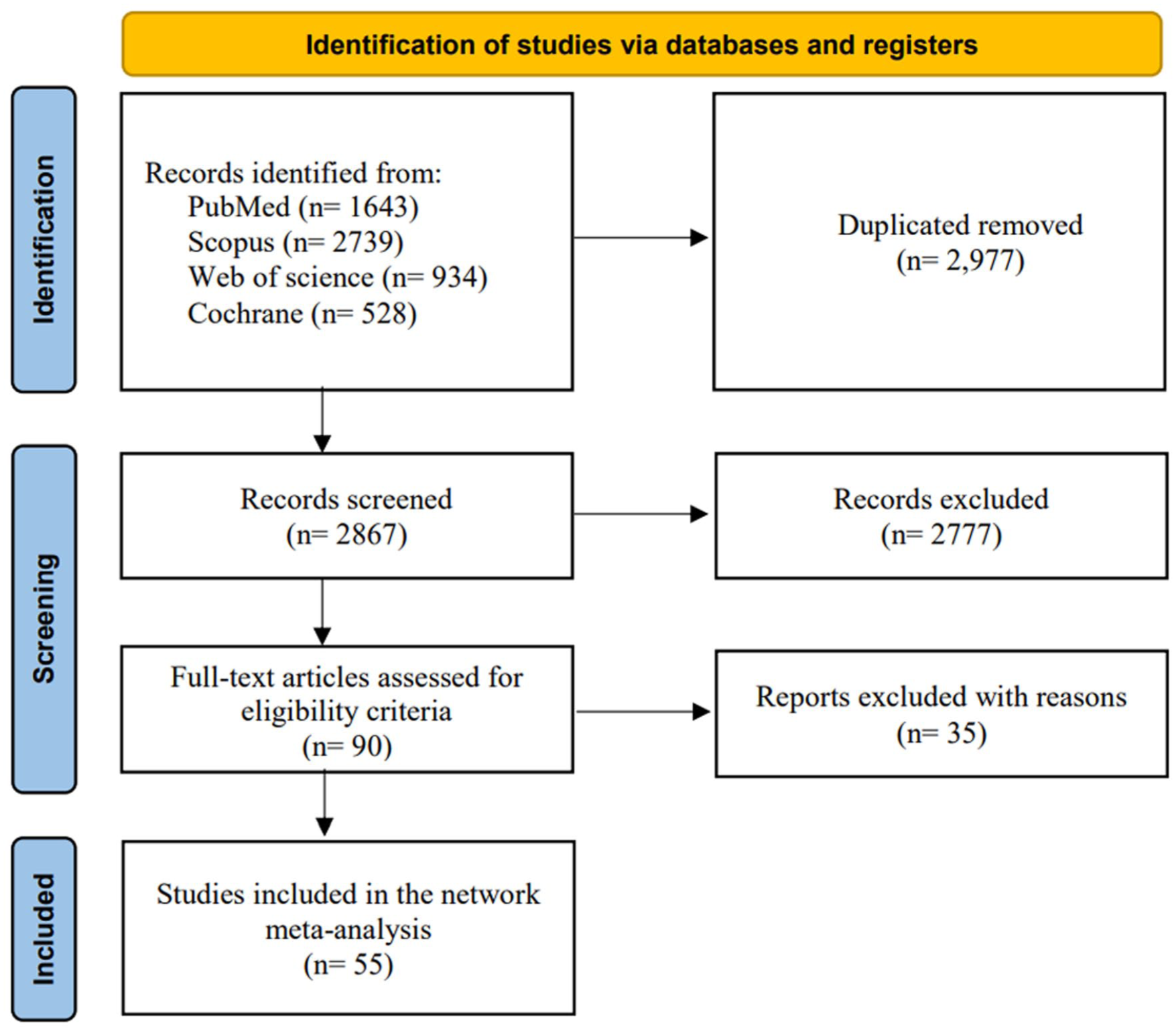
The PRISMA flow diagram.
Characteristics of included studies
A total of 2752 individuals were included in 55 articles. Of them, 40 studies used Pharmacological therapies (Assunção et al., 2006; Atmaca et al., 2003, 2004; Baptista et al., 2007, 2009; Biedermann et al., 2014; Borovicka et al., 2002; Bustillo et al., 2003; Carrizo et al., 2009; Chan et al., 2022; Chiu et al., 2016; de Silva et al., 2015; Deberdt et al., 2005; Graham et al., 2005; Henderson et al., 2005, 2007; Ishøy et al., 2017; Jarskog et al., 2013; Joffe et al., 2008; Kim et al., 2016; Ko et al., 2005; Larsen et al., 2017; Lu et al., 2004; Lyu et al., 2018; Nickel et al., 2005; Patino et al., 2025; Poyurovsky et al., 2002; Pu et al., 2021; Qiu et al., 2022; Siskind et al., 2025; Smith et al., 2018; Tang et al., 2021; Taveira et al., 2014; Tek et al., 2014; Wang et al., 2012; Weizman et al., 2021; Whicher et al., 2021; Wu et al., 2008, 2012; Xie et al., 2024), and 15 used non-pharmacological therapies (Brar et al., 2005; Iglesias-García et al., 2010; Khazaal et al., 2007; Kwon et al., 2006; Mauri et al., 2008; McKibbin et al., 2006; Melamed et al., 2008; Menza et al., 2004; Ratliff et al., 2012; Skrinar et al., 2005; Sugawara et al., 2018; Usher et al., 2013; Vreeland et al., 2003; Weber and Wyne, 2006; Wu et al., 2007). Most recruited individuals in these studies were adult individuals diagnosed with schizophrenia who were treated with atypical antipsychotics. Most of the individuals were overweight or presented with a BMI that was higher than 25. The duration of intervention in each trial ranged from 6 to 52 weeks. The summaries of the included studies are shown in Table S1-2, and the baseline characteristics of the included studies are shown in Table S3.
ROB of included studies
The quality of each study was assessed according to the Cochrane Handbook of Systematic Reviews of Interventions by all authors. According to pharmacological interventions, 10 studies were rated as low ROB, 14 were rated as some concern, and the others were rated as high ROB. According to non-pharmacological interventions, 4 studies were rated as some concern and 11 as high risk. The summaries of quality assessment domains are shown in Figures S14–S15.
Primary outcome
Weight change
Among 53 studies included, 25 different interventions (UC, Metformin, Metformin plus NutriEx. Metformin plus Sibutramine, Berberine, Betahistine, Naltrexone, Naltrexone plus Bupropion, Exenatide, Nizatidine, Sibutramine, Alphalipoic acid, Topiramate, Rosiglitazone, Orlistat, Fluoxetine, Amantadine, Liraglutide, Fluvoxamine, Phenylpropanolamine, Semaglutide, BT, NutriEx. PsyNut) were proposed to 2693 individuals. We present in Figure 2 network estimates of the intervention’s effect on weight compared to UC. The network plot of weight change is shown in Figure 2(c); each node represents a different intervention; UC was the most common intervention, well connected with all other interventions directly linked to it. UC was considered a reference for comparison in all outcomes. According to the pharmacological interventions, all liraglutide (MD: −5.38 [−8.24, −2.57]), Metformin (MD: −3.16 [−4.71, −1.78]), metformin plus NutriEx (MD: −6.34 [−9.85, −2.90]), nizatidine (MD: −5.46 [−7.77, −2.76]), and semaglutide (MD: −13.5 [−17.3, −9.57] showed statistically significant reduction of weight, as shown in Figure 2(a). In non-pharmacological interventions, both BT (MD: −2.46 [−4.05, −0.910]) and NutriEx (MD: −2.92 [−4.78, −1.23]) showed statistically significant differences, as shown in Figure 2(a). After testing the ranking using SUCRA scores, we found that semaglutide holds the highest probability of being the most effective therapy in weight loss. While rosiglitazone had the highest probability of being the least effective in weight loss, as shown in Figure 2(b). The SUCRA score rankings for all interventions are shown in Table S4. According to the inconsistency, the trials with the highest residual deviances in both the consistency (NMA) and inconsistency (UME) models were Assuncao 2006 (Nizatidine arm), Assuncao 2006 (UC arm), and Biedermann 2014 (Sibutramine arm) Under the NMA model, their deviances were 2.63, 2.5, and 1.81, respectively, and under the UME model, they were 2.56, 2.42, and 1.75, showing they are poor fits under both models and are key drivers of the network’s heterogeneity, as shown in Figure 2(d). We conducted a sensitivity analysis by excluding studies with a high ROB. We found that semaglutide has the highest probability of being the most effective therapy in weight loss. As shown in Figure S16–S17.
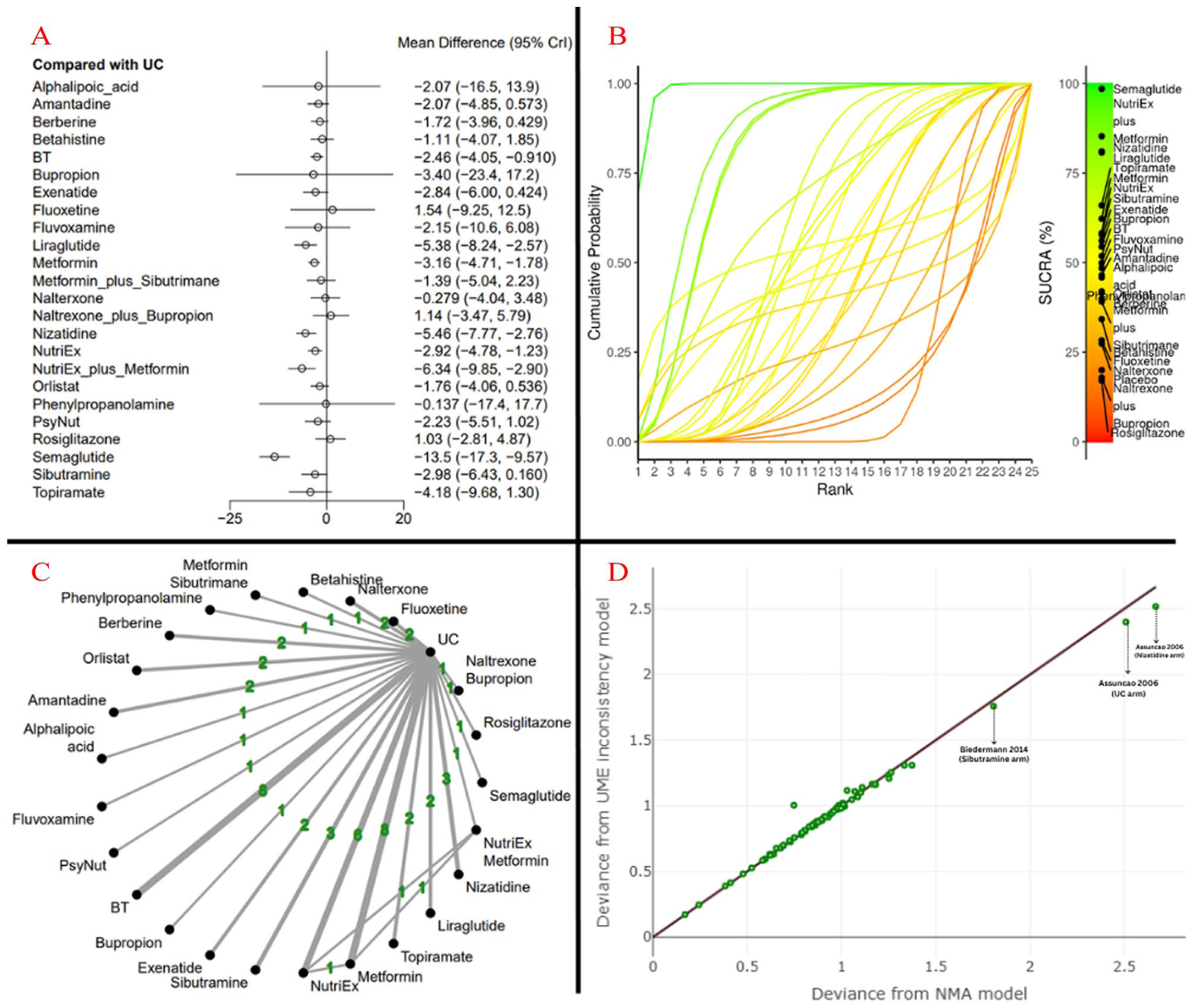
Results of weight change. (a) Forest plots, (b) Ranking with SUCRA scores, (c) Network plot, (d) Inconsistency model.
Secondary outcomes
BMI
Among 45 studies included, 22 different interventions (UC, Metformin, Metformin plus NutriEx, Metformin plus Sibutramine, Berberine, Betahistine, Exenatide, Nizatidine, Sibutramine, Alphalipoic acid, Rosiglitazone, Orlistat, Fluoxetine, Amantadine, Liraglutide, Fluvoxamine, Semaglutide, BT, NutriEx. PsyNut) were proposed to 2349 individuals. We present in Figure 3 network estimates of the intervention’s effect on BMI compared to UC. The network plot of weight change is shown in Figure 3(c); each node represents a different intervention. UC was the most common intervention, well connected with all other interventions directly linked to it. UC was considered a reference for comparison in all outcomes. According to the pharmacological interventions. All liraglutide (MD: −1.69 [−3.32, −0.04], metformin (MD: −1.08 [−1.71, −0.477]), nizatidine (MD: – 2.89 [−4.45, −1.33]), semaglutide (MD: −4.83 [−6.56, −3.11]), as shown in Figure 3(a), in non-pharmacological interventions, both BT (MD: −0.946 [−1.65, −0.254]) and NutriEx (MD: −0.902 [−1.82, −0.172]) showed statistically significant differences, as shown in Figure 3(a). After testing the ranking using SUCRA scores, we found that semaglutide holds the highest probability of being the most effective therapy in weight loss. While rosiglitazone had the highest probability of being the least effective therapy in weight loss, as shown in Figure 3(b). The SUCRA score rankings for all interventions are shown in Table S4. According to the inconsistency, the trials with the highest residual deviances in both the consistency (NMA) and inconsistency (UME) models were Menza 2004 (UC arm), Menza 2004 (NutriEx arm), Pu 2021 (UC arm), and Pu 2021 (Berberine arm). Under the NMA model, their deviances were 2.16, 1.75, 1.53, and 1.4, respectively, and under the UME model, they were 1.76, 1.49, 1.57, and 1.43, showing they are poor fits under both models and are key drivers of the network’s heterogeneity. As shown in Figure 3(d).
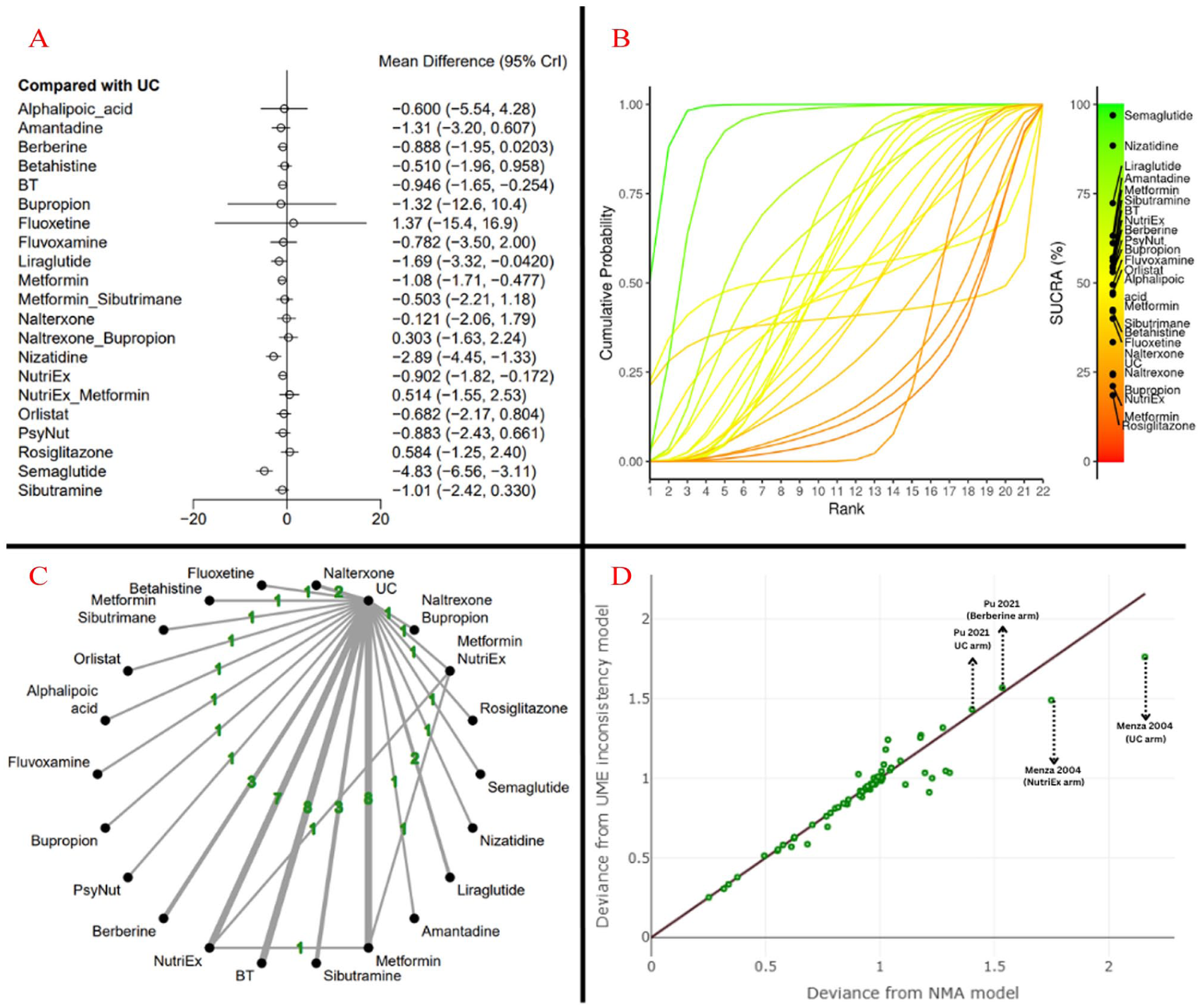
Results of BMI. (a) Forest plots, (b) Ranking with SUCRA scores, (c) Network plot, (d) Inconsistency model.
Waist circumference
Among 21 studies included, 13 different interventions (UC, Metformin, Metformin plus NutriEx, Metformin plus Sibutramine, Berberine, Betahistine, Exenatide, Sibutramine, Rosiglitazone, Liraglutide, BT, NutriEx, PsyNut) were proposed to 1341. We present in Figure S1 network estimates of the intervention’s effect on BMI compared to UC. All studies were well connected to UC, which was therefore selected as the reference comparator, as shown in Figure S1(c). According to the pharmacological interventions, all liraglutide (MD: −5.01 [−8.01, −2.44]), metformin (MD: −1.78 [−3.64, −0.063], and sibutramine (MD: −3.94 [−6.98, −0.757] showed statistically significant differences. In non-pharmacological interventions, both BT (MD: −5.6 [−10.7, −0.723]) and NutriEx (MD: −2.62 [−4.97, −0.278]) showed statistically significant differences. As shown in Figure S1(a). After testing the ranking using SUCRA scores, we found that liraglutide holds the highest probability of being the most effective therapy in weight loss. UC holds the highest probability of being the least effective therapy in weight loss. As shown in Figure S1(b). According to the inconsistency, the trials with the highest residual deviances in both the consistency (NMA) and inconsistency (UME) models were Pu 2021 (UC arm), Pu 2021 (Berberine arm), Wu 2008 (Metformin + NutriEx arm), and Wu 2008 (UC arm). Under the NMA model, their deviances were 1.64, 1.47, 1.5, and 0.67, respectively, and under the UME model, they were 1.71, 1.55, 1.2, and 1.17, showing they are poor fits under both models and are key drivers of the network’s heterogeneity, as shown in Figure S1(d).
Hip circumference
Among the seven studies included, seven different interventions (UC, Sibutramine, Exenatide, Betahistine, Topiramate, Berberine, and NutriEx) were proposed to 389 individuals. We present in Figure S2 network estimates of the intervention’s effect on hip circumference compared to UC. All studies were well connected to UC, which was therefore selected as the reference comparator, as shown in Figure S2(c). No interventions showed a significant reduction in hip circumference, as shown in Figure S2(a). After testing the ranking using SUCRA scores, we found that Berberine holds the highest probability of being the most effective therapy in weight loss. UC holds the highest probability of being the least effectivetherapy in weight loss, as shown in Figure S2(b). The SUCRA score rankings for all interventions are shown in Table S4. According to the inconsistency, most studies showed high but comparable residual deviances in both (NMA) and (UME) models, indicating no substantial inconsistency.
Waist-hip ratio
Among 11 studies included, 9 different interventions (UC, Berberine, Betahistine, Metformin, Orlistat, Semaglutide, Sibutramine, BT, and NutriEx) were proposed to 389 individuals. We present in Figure S3 network estimates of the intervention’s effect on the waist-hip ratio compared to UC. All studies were well connected to UC, which was therefore selected as the reference comparator, as shown in Figure S3(c). No interventions showed a significant reduction in the waist-hip ratio, as shown in Figure S3(a). After testing the ranking using SUCRA scores, we found that Berberine holds the highest probability of being the most effective therapy in weight loss. UC holds the highest probability of being the least effective therapy in weight loss, as shown in Figure S3(b). The SUCRA score rankings for all interventions are shown in Table S4. According to the inconsistency, most studies showed high but comparable residual deviances in both (NMA) and (UME) models, indicating no substantial inconsistency.
Safety
We conducted a network analysis among the Following Symptoms: Abdominal pain, Constipation, Diarrhea, Dizziness, Dry mouth, Fatigue, Headache, Nausea, Tachycardia, and Vomiting. Abdominal pain and nausea were associated with an increased risk of both conditions (RR: 1.77 [1.01, 3.08]) and (RR: 1.94 [1.22, 3.06]), respectively. In Constipation, the analysis model favored betahistine over the UC group (RR: 0.21 [0.05, 0.84]). No group showed a significant difference in the other safety outcomes. Safety results are shown in Figures S4–S13.
Discussion
Summary of the findings
To the best of our knowledge, this is the first systematic review and NMA comparing the efficacy of both pharmacological and non-pharmacological interventions for AIWG. The essentiality of this study is not only to comprehensively evaluate the efficacy of the different interventions but also to rank them from the most effective to the least effective according to the different frequencies.
Explanation of the results
As demonstrated in the weight change results, the top four significantly ranked interventions were Semaglutide Metformin + NutriEx, followed by Nizatidine, and then liraglutide. Our discussion will focus solely on the significant interventions among these. First, Semaglutide exhibits potent GLP-1 receptor agonist activity, targeting key mechanisms involved in appetite regulation, delaying gastric emptying, and promoting feelings of fullness and energy balance (Wilding et al., 2021). Unlike other weight management options, semaglutide not only reduces hunger and increases satiety but also improves insulin sensitivity and glycemic control. Clinical studies have shown significant and sustained weight loss in individuals using semaglutide, even in those who had previously struggled with weight management due to medications such as olanzapine or clozapine (Khaity et al., 2023). In addition, semaglutide may reduce cardiovascular risk, making it particularly valuable in individuals with comorbidities commonly associated with psychiatric illness (Marso et al., 2016). Second, many studies have demonstrated the effectiveness of metformin in promoting weight loss. Metformin, the first-line therapy for type 2 diabetes mellitus, primarily acts by reducing insulin resistance (Foretz et al., 2023). It enhances insulin sensitivity by suppressing hepatic gluconeogenesis and improving peripheral glucose uptake. This mechanism is particularly relevant for addressing AIWG, as many antipsychotics, especially atypical agents such as olanzapine and clozapine, induce insulin resistance, contributing to weight gain. Metformin counteracts this metabolic dysregulation (Carli et al., 2021). Improved insulin sensitivity also helps prevent postprandial hypoglycemia caused by sluggish insulin secretion and delayed insulin peaks, which often trigger carbohydrate cravings and compensatory overeating (Luyckx and Lefebvre, 1971; Schultes et al., 2003). As a result, metformin may help mitigate this cycle of excessive carbohydrate intake. Emerging research has also identified complex mechanisms and additional targets of metformin beyond the liver, including its effects on the gut microbiota and tissue-resident immune cells. These findings suggest further potential benefits in addressing weight gain induced by antipsychotics (Foretz et al., 2023). The combination of Metformin, nutrition education, and exercise offers a comprehensive approach to weight loss. Metformin helps regulate blood sugar levels and control appetite, while nutrition education and exercise promote sustainable habits, improve body composition, and increase calorie expenditure; importantly, long-term use of these non-pharmacological strategies has been shown to maintain weight loss in individuals with severe mental illness, including those with schizophrenia (Pendlebury et al., 2007). Together, these elements create a more effective and lasting solution compared to using metformin alone. Liraglutide, the third most effective drug in our analysis, also demonstrated significant efficacy in reducing body weight and BMI in AIWG management. Third, Nizatidine, a histamine H2-receptor antagonist, has shown potential benefits in managing AIWG. Unlike other weight loss agents, nizatidine may reduce weight by modulating central and peripheral histaminergic pathways that influence appetite and metabolism (Roerig et al., 2011). Some studies suggest that nizatidine can attenuate weight gain caused by atypical antipsychotics, particularly olanzapine, possibly through effects on leptin sensitivity and reduced fat accumulation (Pae et al., 2003). Its relatively favorable safety profile, low cost, and minimal interaction with psychiatric medications make it a practical choice for long-term adjunctive therapy. Fourth, liraglutide, as a GLP-1 receptor agonist, works by enhancing insulin secretion, inhibiting glucagon release, and slowing gastric emptying, which leads to reduced appetite and food intake. Additionally, liraglutide has been shown to improve satiety and promote weight loss through its central effects on the hypothalamus (Imbernon et al., 2022). Previous systematic reviews have supported liraglutide’s efficacy and safety as an option for managing AIWG (Bak et al., 2024; Barnard-Kelly et al., 2022), and our findings are consistent with this body of evidence. In the included trials, liraglutide led to a mean reduction in body weight from baseline of 5.7 and 4.7 kg and a mean reduction in BMI of 1.7 and 1.6, respectively. These results align with those from a prior meta-analysis that incorporated cohort studies, which reported a mean weight reduction of 4.7 kg and a BMI reduction of 1.21. However, given that only two RCTs were included in our analysis, the confidence in the pooled effect estimate remains limited. Therefore, we recommend conducting additional RCTs to further assess the efficacy of liraglutide in managing AIWG and strengthen the evidence base for its use in this population. For safety outcomes, the results showed no significant difference between the intervention and control groups in most measures. However, liraglutide was associated with worsening symptoms of abdominal pain and nausea, as illustrated in Figures S1–S10.
Strength points and limitations
Our analysis provides the most comprehensive evidence on the efficacy and safety of various anti-obesity interventions for individuals with schizophrenia who experience AIWG. The inclusion criteria were broad, with no restrictions based on the year of dissemination, geographical location, or the specific type of intervention. This broad approach also allowed us to incorporate more than 24 interventions, covering a wide spectrum of treatment options, from BT and lifestyle modifications to pharmacological treatments. The large number of individuals included in the quantitative synthesis further strengthens our findings and enhances the generalizability of the results. However, some limitations must be considered. There is variety in outcome assessment time points across trials, which may have introduced unit-of-analysis errors into our synthesis. In addition, most of the included studies have a high ROB.
Implications
A dual-approach strategy is recommended for the effective management of AIWG. Semaglutide appears to be the most effective pharmacological agent for achieving significant and rapid weight reduction, particularly in individuals with substantial weight gain. However, its use requires careful patient selection and ongoing monitoring to mitigate potential adverse effects. At the same time, non-pharmacological interventions—such as BT, nutritional education, and structured exercise—remain essential for promoting sustainable, long-term weight control. These should be considered a foundational component of treatment for all individuals. When combined with pharmacological therapy, these interventions can have synergistic effects, enhancing overall treatment outcomes. Managing AIWG effectively demands an integrated, multidisciplinary care model. Healthcare systems must establish clear protocols that support collaboration among psychiatrists, endocrinologists, dietitians, and behavioral specialists. This includes creating streamlined referral pathways to lifestyle intervention programs and providing targeted training for healthcare providers. Implementing such coordinated, patient-centered care plans is crucial for addressing both the immediate and long-term metabolic health challenges faced by individuals with schizophrenia. Future research should aim to optimize and personalize treatment strategies. Key priorities include determining the optimal timing and sequencing of combined interventions, identifying predictors of individual treatment response, and developing tailored approaches that maximize the benefits of both semaglutide and lifestyle modification. Ongoing investigation is essential to refine evidence-based guidelines and improve long-term outcomes and quality of life for individuals affected by AIWG.
Conclusion
Our study provides a comprehensive evaluation of the efficacy of anthropometric measurements and safety profiles to synthesize evidence for the best practices in treating AIWG. We showed that the most effective approach is Semaglutide. We encourage further exploration of non-pharmacological approaches and the conduct of new studies in this area.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251399544 – Supplemental material for Efficacy and safety of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain in individuals with schizophrenia: A systematic review and network meta-analysis of 55 clinical trials
Supplemental material, sj-docx-1-jop-10.1177_02698811251399544 for Efficacy and safety of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain in individuals with schizophrenia: A systematic review and network meta-analysis of 55 clinical trials by Mohamed Ezzat M. Mansour, Khalid Radwan Alsaadany, Mohamed M. M. Mustafa, Mohamed Awad E. Ahmed, Ahmad Beddor, Mohamed Mohsen Helal, Ali Salah Elgahamy, Omar Kassar, Fares Abdelsalam, Ahmed Ezzat Elmetwalli and Michel Sabé in Journal of Psychopharmacology
Supplemental Material
sj-docx-2-jop-10.1177_02698811251399544 – Supplemental material for Efficacy and safety of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain in individuals with schizophrenia: A systematic review and network meta-analysis of 55 clinical trials
Supplemental material, sj-docx-2-jop-10.1177_02698811251399544 for Efficacy and safety of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain in individuals with schizophrenia: A systematic review and network meta-analysis of 55 clinical trials by Mohamed Ezzat M. Mansour, Khalid Radwan Alsaadany, Mohamed M. M. Mustafa, Mohamed Awad E. Ahmed, Ahmad Beddor, Mohamed Mohsen Helal, Ali Salah Elgahamy, Omar Kassar, Fares Abdelsalam, Ahmed Ezzat Elmetwalli and Michel Sabé in Journal of Psychopharmacology
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
This study was prospectively registered on PROSPERO (CRD42024599597).
Author contributions
Mohamed Ezzat M. Mansour conceived and designed the project idea. All authors were responsible for data extraction. Mohamed Ezzat M. Mansour, Mohamed Mohsen Helal, and Khalid Radwan Alsaadany conducted the literature search. Mohamed Ezzat M. Mansour and Khalid Radwan Alsaadany acquired and analyzed the data. Mohamed Ezzat M. Mansour, Khalid Radwan Alsaadany, Mohamed M. M. Mustafa, and Mohamed Mohsen Helal were responsible for writing. All authors have reviewed and approved the final version of this manuscript and consent to its publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All authors had full access to the data we used in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.