
Abstract
Background:
Lysergic acid diethylamide (LSD) has been considered as a potential treatment for depression for over 75 years, but its therapeutic potential has only recently been considered in mainstream psychiatry. Repeated ingestion of low doses of LSD (“microdoses”) is thought to reduce depression, but the neurobiology underlying this effect is unknown. We previously reported that low doses of LSD increased event-related potentials (ERPs) during receipt of monetary rewards in healthy adults. LSD also produced more positive subjective effects in participants with mild-to-moderate baseline symptoms of depressed mood, compared to controls.
Aim:
In this report, we examined the effects of LSD on reward ERPs in participants with mild-to-moderate depressed mood and in non-depressed controls.
Methods:
Participants with subclinical mild-to-moderate depression (N = 20) or controls with minimal symptoms (N = 19) received LSD (26 μg tartrate) or placebo on two sessions. Primary measures were ERPs during a reward task, and secondary measures included self-reported mood during and 48 hours after the sessions.
Results:
LSD (vs placebo) increased late positive potential (LPP) amplitude to loss (vs win) reward feedback only in participants with higher baseline depressed mood, suggesting enhanced affective processing given the role of LPP in emotional valuation of reward. This effect of LSD on LPP was associated with its acute positive mood effects, and with lower depressed mood 48-hour after the LSD (vs placebo) session. In the full sample, LSD (vs placebo) decreased feedback-P3 and LPP amplitude to reward (vs neutral) feedback.
Conclusion:
Although findings must be interpreted with caution, results support the idea that low doses of LSD have potential anti-depressant effects.
Introduction
There has been substantial public interest in the idea that low doses of psychedelic drugs, especially lysergic acid diethylamide (LSD), can have beneficial mood and behavioral effects (Fadiman et al., 2011). Specifically, users claim that “microdosing,” or taking very small doses of LSD once every 3–4 days, improves mood, cognitive function, and even creativity (Kuypers, 2020; Passie, 2019). However, the beneficial effects of this practice have been difficult to demonstrate in controlled studies (Cavanna et al., 2022; De Wit et al., 2022; Murphy et al., 2023; Polito and Liknaitzky, 2022; Szigeti et al., 2021). One reason for the difficulty may be that the self-report and behavioral measures are not sensitive enough to detect subtle effects. Measures of brain function may reveal underlying changes that are not detectable by self-report. Our laboratory has investigated the idea that low doses of LSD affect brain responses to reward, even at doses that produce minimal mood or behavioral effects (Glazer et al., 2023; Murray et al., 2022a).
Event-related potentials (ERPs) offer an efficient way to study acute effects of psychedelic drugs on brain responses to reward. The strong temporal resolution of electroencephalography (EEG) is well-suited to measure three distinct ERP components during feedback processing of rewards (Glazer et al., 2018). Each ERP component reflects a distinct psychological function that sequentially encodes hedonic, motivational, and affective aspects of reward feedback. First, the Reward-Positivity (RewP) encodes the immediate impact of positive (vs negative) feedback (Holroyd et al., 2008). The RewP is thought to reflect reward prediction errors associated with phasic mesencephalic dopamine in the ventral striatum and is attenuated in depression (Carlson et al., 2011; Holroyd and Coles, 2002; Proudfit, 2015). Next, the Feedback-P300 (FB-P3) encodes the motivational salience of feedback and likely reflects attentional processes that categorize feedback stimuli and update working memory with important contextual information, such as the size or likelihood of rewards (San Martín, 2012). Lastly, the Late Positive Potential (LPP) reflects the emotional value of negative (vs positive) feedback and has been called the “affective counterpart” of the FB-P3 (Groen et al., 2008; Glazer et al., 2018). Stronger emotional processing after negative feedback can help motivate behavioral change and quicken responses on subsequent trials (Glazer et al., 2018, Pornpattananangkul and Nusslock, 2016). The FB-P3 and LPP both covary with activation in the amygdala (Nieuwenhuis et al., 2005; Olofsson et al., 2008), a region associated with abnormal emotional processing in depression (Groenewold et al., 2013) and impacted by LSD (Bershad et al., 2020; Mueller et al., 2017). Together, these three ERP components reflect independent psychological processes that sequentially encode the hedonic (RewP), motivational (FB-P3), and affective (LPP) value of reward feedback.
One task used to study ERPs during reward processing is the electrophysiological monetary incentive delay (eMID) task (Broyd et al., 2012). The eMID is a well-validated measure of reward processing that is sensitive to symptoms of depression (Novak et al., 2016). On each trial, a reward or neutral cue indicates whether the participant can win money. Then, the participant quickly responds to a target stimulus. Lastly, a feedback stimulus indicates whether their response was quick enough (positive feedback) or too slow (negative feedback). Several eMID studies have reported lower RewP and FB-P3 amplitudes to positive feedback on reward trials are associated with higher depressive symptoms in depressed patients and greater subthreshold symptoms in healthy adults (Ait Oumeziane et al., 2019; Novak et al., 2016; Pegg et al., 2021; Wen et al., 2024; White et al., 2021; Zhou et al., 2019), likely reflecting blunted reward sensitivity (Nusslock and Alloy, 2017). Some eMID studies have also reported associations between higher depressive symptoms and enhanced FB-P3 amplitudes to positive and negative feedback on neutral trials (Gao et al., 2024; Wen et al., 2024). This effect could be related to motivational deficits and inefficient effort allocation to neutral trials where monetary rewards are not possible. Finally, although few eMID studies have measured the LPP, several reward processing studies have observed a greater anterior LPP amplitude to negative (compared to positive) feedback (see Glazer et al., 2018). Lower LPP amplitudes to negative feedback are associated with higher depressive tendencies in healthy adults (Glazer et al., 2019) and adolescents with major depressive disorder (Webb et al., 2021). Thus, lesser LPP amplitude (i.e., a smaller difference between negative and positive feedback) in the eMID may also capture blunted emotional processing of reward feedback typically associated with higher depressive symptoms.
We recently reported that low doses of LSD (13 and 26 µg LSD tartrate) increased neural responses to monetary rewards in the eMID task as measured by the three ERPs involved in reward feedback processing (Glazer et al., 2023). These low doses of LSD are in the range used for microdosing and are a fraction of doses used for hallucinogenic effects and in most clinical trials (75–200 µg; Dos Santos et al., 2021). Glazer et al (2023) found that 13 µg (but not 26 µg) LSD increased the immediate impact (RewP) and the emotional consequences (LPP) of reward (vs neutral) feedback in healthy adults. Both 13 and 26 µg LSD increased the motivational salience (FB-P3) of positive (vs negative) feedback. Interestingly, these neural effects were not strongly associated with modest subjectively reported drug effects (Murray et al., 2022b), suggesting that the drug may affect reward processing in the brain at doses below those needed to produce self-reported effects. It is not clear why 13 µg, but not 26 µg LSD increased the RewP. However, we previously speculated that this may relate to a “sweet spot” described in anecdotal reports of microdosing, that is, an optimal dose for desired effects (Spotswood, 2022). This interesting question must await future studies with the effect of low doses of LSD on reward ERPs in humans.
The present study extended the findings of the Glazer et al. (2023) study, by testing effects of a low dose of LSD (26 µg) in individuals with mild-to-moderate levels of depressed mood, compared to controls with minimal symptoms (Molla et al., 2023). We found that the mildly depressed participants exhibited more pronounced subjective responses to LSD. Participants in the Molla et al. (2023) study also completed the eMID with EEG recordings, which are presented here (Molla et al., 2003). The goal of the present study is to examine whether neural effects of the drug are related to symptoms of depressed mood before receiving LSD, during the sessions, or 48 hours later. Whereas Molla et al. (2013) assessed depressed mood using traditional diagnostic cutoffs (i.e., BDI scores of 0–13 Minimal; 14–19 Mild; 20–28 Moderate, and 29–63 Severe), the present study examined depressed mood as a continuous variable. This dimensional approach is consistent with contemporary models of depression that argue few qualitative differences exist between sub-clinical and clinical symptomatology (Cicchetti et al., 2009). Numerous studies support the view that depressive symptomatology is a spectrum rather than a discrete category (Hankin et al., 2005; Ruscio and Ruscio, 2002). In the present study, current symptoms of depressed mood were assessed at baseline, 48 hours after an LSD session, and 48 hours after a placebo session using a continuous measure. We hypothesized that compared to placebo, LSD would increase neural responses to reward feedback for the RewP, FB-P3, and LPP to a greater extent in individuals with higher symptoms of depressed mood at baseline. We also examined these neural effects in relation to the acute subjective effects of LSD (vs placebo) and the reduction in baseline symptoms of depressed mood from 48-hour after LSD (vs 48-hour after placebo).
Materials and methods
Study design
Healthy men and women with a range of scores on a modified version of the Beck Depression Inventory-II (M-BDI; see below) participated in two 5-hour study sessions, one with LSD (26 µg), the other with placebo (Molla et al., 2023). The drug and placebo were administered under double-blind conditions, separated by at least 7 days. EEG recordings were obtained during the peak time of drug effect, while participants completed the eMID reward task. Participants completed the M-BDI questionnaire at baseline (during orientation) and 48-hour after both study sessions, and subjective effects questionnaires during each session at regular intervals. The specific times for each study session and activity are outlined below in subsequent sections.
Participants
Thirty-nine volunteers (age 18–35 years) were recruited via posters and internet advertisements (N = 34 after participant exclusion). Study inclusion criteria were fluency in English, minimum high school education, BMI 19–30 kg/m2, no current medications, and at least one experience with a psychedelic drug. Screening included a physical exam, electrocardiogram, semi-structured psychiatric interview, and drug use history questionnaire. Exclusion criteria included current suicidal ideation, severe post-traumatic stress disorder, obsessive compulsive disorder, panic disorder, lifetime psychotic disorder, past year history of severe substance use disorder or adverse responses to psychoactive drugs, medical conditions contraindicating study participation and pregnancy or planned pregnancy in women.
Orientation session
Participants were familiarized with procedures, and provided informed consent. They were told that they might receive a placebo, a stimulant, a sedative, or a hallucinogen, and instructed to abstain from drugs before the study sessions. The study was approved by the Institutional Review Board of the Biological Sciences Division of the University of Chicago. Participants completed the M-BDI during orientation to determine baseline symptoms of depressed mood.
Experimental sessions
Two 5-hour sessions were conducted from 9:00 am to 2:00 pm, separated by at least 7 days. Before drug was administered, breathalyzer (Alco-Sensor III, Intoximeters, St Louis, MO, USA) and urine drug tests were obtained (CLIAwaived Instant Drug Test Cup), and women were tested for pregnancy. Participants completed pre-drug questionnaires and cardiovascular measures (see below) were obtained, and then received LSD (26 µg) or placebo sublingually under double-blind conditions. The order of placebo and drug sessions was counterbalanced (placebo first: N = 16, drug first: N = 18). At 11:30 am, EEG electrodes were applied, and the eMID task was initiated. Mood and cardiovascular measures were obtained at regular intervals throughout the session. Participants completed the M-BDI 48-hour after each session.
Drug
LSD tartrate (Organix Inc) in a tartaric acid solution was prepared by the University of Chicago Investigational Pharmacy. The 26 µg dose of LSD was administered sublingually in 0.4 mL of solution, and 0.4 mL of distilled water was administered during placebo sessions.
Questionnaires
M-BDI (Beck et al., 1996): The BDI is a 21-item inventory that assesses symptoms of depression in the last 2 weeks. To assess current symptoms of depressed mood, the present study used a variant of this questionnaire, asking participants how they felt “at the moment” and is referred to as the M-BDI, or “Momentary-BDI.” Participants completed the M-BDI at baseline (orientation) and 48 hours after each experimental session. Importantly, the M-BDI did not provide information needed for a formal diagnosis, which requires the symptoms to persist for at least 2 weeks (American Psychiatric Association, 2022). 1 The M-BDI captured depressed mood states at-the-moment, before participation (baseline) and 48 hours after each session. Continuous M-BDI scores were used as a dimensional measure of current depressed mood. M-BDI change scores were calculated by subtracting baseline M-BDI scores from M-BDI scores assessed 48-hour after LSD (ΔM-BDI-LSD: baseline minus LSD) and placebo (ΔM-BDI-placebo: baseline minus placebo) sessions.
Profile of Mood States
(POMS; (McNair et al., 1971): The POMS consists of 72 adjectives commonly used to describe momentary mood states induced by drugs (De Wit and Griffiths, 1991). For this analysis, we examined the following subscales associated with positive and negative emotional experience: Positive Mood, Elation, Vigor, and Depression. Peak subjective effects were calculated by subtracting initial values measured just before drug administration from the highest or lowest value measured during the session (60, 120, 180, and 240 minutes after drug or placebo administration).
EEG measures
Electrophysiological Monetary Incentive Delay
The eMID task was administered using E-Prime (Psychology Software Tools, Pittsburgh, PA, USA). Each trial consisted of a cue stimulus (trial-type: reward or neutral), followed by a rapid response requirement, followed by a feedback stimulus (feedback-type: “WIN” or “LOSE”). Reward cues indicated participants could win $1.50 on these trials. Neutral cues indicated participants could not win or lose any money on these trials. Punishment trials were also included (indicating participants could lose $0.75 on these trials) but were not analyzed here because the study focused on reward processing (see Supplemental materials for analysis of punishment trial types). Next, a fixation cross was displayed (jittered from 2–2.5 seconds) followed by a white square. Participants responded as-quickly-as-possible to the square with their right index finger on a response box. After this response, another fixation cross was displayed (2 seconds). Finally, a feedback stimulus was presented (1.5 seconds) consisting of the words “WIN” or “LOSE.” If participants responded before the square disappeared (“fast enough”), they received “WIN” feedback. Otherwise, they received “LOSE” feedback (“too slow”). On reward trials, “WIN” feedback resulted in a monetary gain of $1.50, and “LOSE” feedback resulted in $0.00 (e.g., “missed” monetary gains). Subjects still received “WIN” or “LOSE” feedback on neutral trials if their response was fast enough or too slow, but there was no monetary outcome (see Figure S1 in Supplemental materials for trial structure). Unbeknownst to participants, an adaptive algorithm adjusted the square duration after each trial to ensure “WIN” and “LOSE” feedback were presented an equal number of times after reward and neutral cues (Broyd et al., 2012; Novak et al., 2015, 2016; Murray et al., 2022b). The starting square duration was determined during a practice task (32 trials). The 30-minute task consisted of six blocks of 20 trials. EEG measures of reward processing after feedback presentation were the primary outcome measures (Glazer and Nusslock, 2022; San Martín, 2012).
Electrophysiological acquisition
An Electro-Geodesic net with 64 active electrodes was used (Magstim, EGI). Electrodes were soaked in saline before head placement (nasion-to-inion, mastoid-to-mastoid). Additional electrodes were placed on the chest for EKG and around the eyes for ocular movements. EEG data were sampled online (1024 Hz) and acquired continuously, amplified, and digitized using Netstation software (Magstim, EGI). Electrode impedance was kept under 10 kΩ.
Electrophysiological preprocessing
EEG data were analyzed offline using EEGLab (Delorme and Makeig, 2004) and ERPLAB (Lopez-Calderon and Luck, 2014) in MATLAB (The Math Works, Inc.). Raw data were resampled (256 Hz) and mastoid re-referenced (left/right average). Line noise and bad channels were removed (PREP, CleanRawData; Bigdely-Shamlo et al., 2015). Unfiltered data were saved. Next, independent component analysis (ICA) was performed. Before ICA, data were high pass filtered (1.0 Hz) and large artifacts were removed (any electrode >500 µV, 500 ms windows, 250 ms overlap). ICA weights were applied to unfiltered data saved previously and bad channels were interpolated. 2 Artifactual ICA components (ocular/muscular) were identified using visual inspection and removed. Data were then bandpass filtered (0.1–30 Hz), segmented into epochs (−200 to −1000 ms) time-locked to feedback stimulus onset, and baseline corrected using the pre-stimulus interval (−200 to 0 ms). Artifacts were removed using automated methods (any electrode >100 µV, 200 ms windows, 100 ms overlap). Accepted epochs were averaged together separately to extract four feedback bins: Reward “WIN,” Reward “LOSE,” Neutral “WIN,” and Neutral “LOSE.” Five participants were removed: excessive artifact rejection (N = 1), not following task instructions (N = 2), and incomplete EEG data (N = 2). All remaining participants retained acceptable artifact rejection rates (trials-per-bin accepted: Reward WIN: M = 27.87, SD = 3.43, Reward LOSE: M = 26.06, SD = 3.47, Neutral WIN: M = 28.04, SD = 3.55, Neutral LOSE: M = 26.32, SD = 3.30). Baseline depressed mood did not significantly impact artifact rejection rates (2 × 2 analysis of variance (ANOVA): trial-type (reward, neutral) × feedback type (WIN, LOSE) × M-BDI scores: ps > 0.87). Thirty-four participants were retained for analysis (17 female and 16 with placebo session first).
ERP measurement
Average activity for each ERP component was measured after feedback presentation. Electrode averages were used around FCz (FC1/FC2/FCz) and Pz (P1/P2/Pz) to reduce noise. Three ERPs were extracted from average activity in each bin: RewP from 287–337 ms around FCz (±25 ms around peak LOSE–WIN difference wave), FB-P3 from 337–387 ms around Pz (±25 ms around peak positivity), and LPP from 700 to 1000 ms around FCz (where positivity was maximal).
Statistical analyses
Symptoms of depressed mood
Participants completed the M-BDI to assess symptoms of depressed mood at baseline (orientation) and 48-hour after each session (ΔM-BDI-LSD and ΔM-BDI-Placebo). ANOVA was performed with drug as the within-person factor (drug: ΔM-BDI-placebo, ΔM-BDI-LSD). To maximize statistical power, continuous M-BDI scores were used in all analyses (Hankin et al., 2005; Ruscio and Ruscio, 2002).
Subjective effects
Complete subjective effects data are presented in Molla et al. (2023). Separate ANOVAs were performed for each subjective measure with one within-person factor (drug: placebo, LSD) and one continuous covariate (baseline M-BDI scores). If significant effects of baseline M-BDI scores and drug emerged in the omnibus ANOVA, the same statistical procedure was performed with ΔM-BDI-LSD scores as the continuous covariate (controlling for ΔM-BDI-placebo scores).
ERP analyses
Primary ERP outcome measures were the RewP, FB-P3, and LPP measured after feedback presentation. The analysis was first conducted without M-BDI scores as a covariate. Separate ANOVAs were performed for each ERP with three within-person factors: Drug (LSD, Placebo) × Trial-Type (Reward, Neutral) × Feedback-Type (WIN, LOSE). Follow-up t-tests were performed to examine significant effects. Then, to determine whether associations were moderated by symptoms of depressed mood, the same analysis was conducted with one additional continuous covariate: baseline M-BDI scores. Only significant effects involving baseline M-BDI scores and drug in the omnibus ANOVA were considered, and linear regressions were performed to examine significant interactions. The same statistical procedure was performed with ΔM-BDI-LSD (controlling for ΔM-BDI-placebo) only if significant effects of baseline M-BDI and drug emerged in the omnibus ANOVA.
ERPs × Subjective Effects
Associations between ERPs and subjective measures were analyzed only for variables on which there were significant effects of drug and baseline M-BDI scores in the omnibus ANOVA. ANOVA was performed with three within-subject factors (drug, trial-type, and feedback-type) and one continuous covariate (subjective measure difference score: LSD minus placebo).
Several steps were taken to minimize multiple comparisons. First, Fisher’s protected t-tests were utilized to minimize family-wise error rate, which requires a significant omnibus ANOVA F-test to proceed to pairwise comparisons (Patricia Cohen et al., 1983). Second, follow-up t-tests were performed only to examine significant effects involving drug in the omnibus ANOVA. Third, significant ERP effects were evaluated using difference waves calculated between feedback-types (LOSE minus WIN feedback), trial-types (reward minus neutral trials), and drug (LSD minus placebo). All analyses controlled for two between-person factors (drug order: placebo-LSD or LSD-placebo, and sex: male or female), which had no effects beyond what might be expected by chance.
Results
Demographic characteristics
Participant demographic characteristics and drug use patterns are shown in Table S1 (Supplemental materials).
Symptoms of depressed mood
Compared to baseline (M-BDI-baseline: M = 11.97, SD = 9.34, median = 12, range = 0–33), M-BDI scores declined to a greater degree 48-hour after the LSD session (M-BDI-LSD: M = 6.62, SD = 6.67, median = 3.5, range = 0–23; ΔM-BDI-LSD: M = 5.35, SD = 5.52, median = 4, range = −3 to 20) compared to after the placebo session (M-BDI-placebo: M = 8.53, SD = 7.86, median = 7.5, range = 0–28; ΔM-BDI-placebo: M = 3.44, SD = 4.22, median = 3, range = −3 to 16) (F = 4.51, p = 0.042, ηp2 = 0.13).
Subjective effects
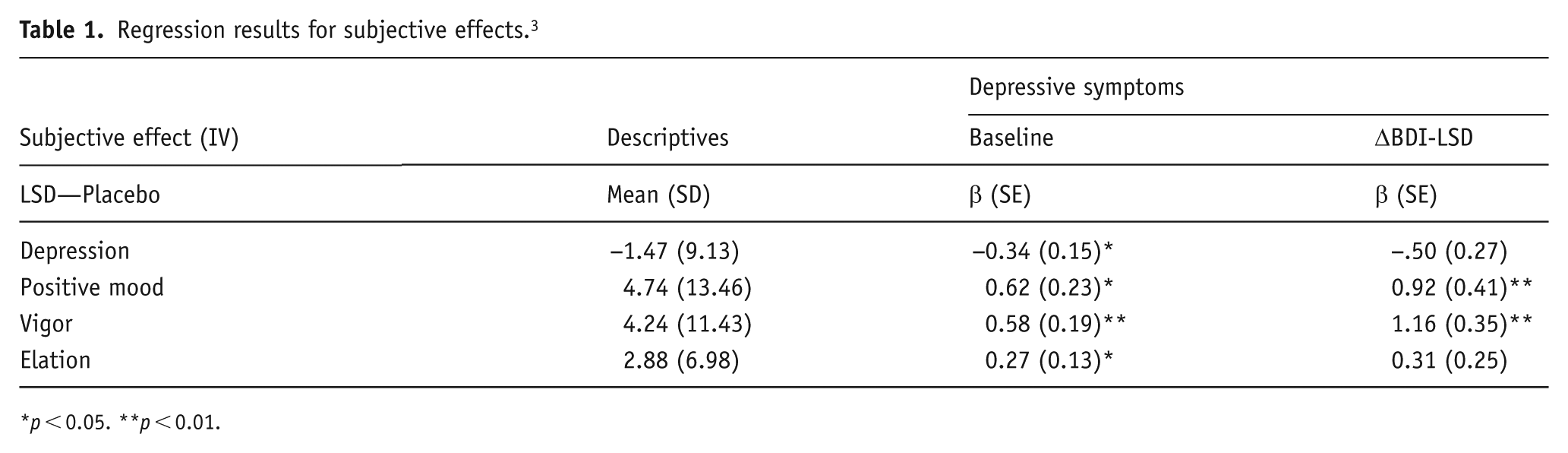
Higher baseline M-BDI scores were significantly associated with greater increases in POMS positive mood, vigor, and elation and decreased POMS depression ratings during the session after LSD, compared to placebo (significant baseline M-BDI × Drug interaction; see Table 1 for regression results). When ΔM-BDI-LSD scores were entered as a covariate (controlling for ΔM-BDI-placebo scores), greater reductions in M-BDI scores 48-hour after the LSD session were significantly associated with increased POMS positive mood and vigor for LSD during the sessions, compared to placebo (significant ΔM-BDI-LSD × drug interaction; see Table 1 for regression results).
Regression results for subjective effects. 3
p < 0.05. **p < 0.01.
Feedback-related ERPs
Neither LSD nor M-BDI affect RewP
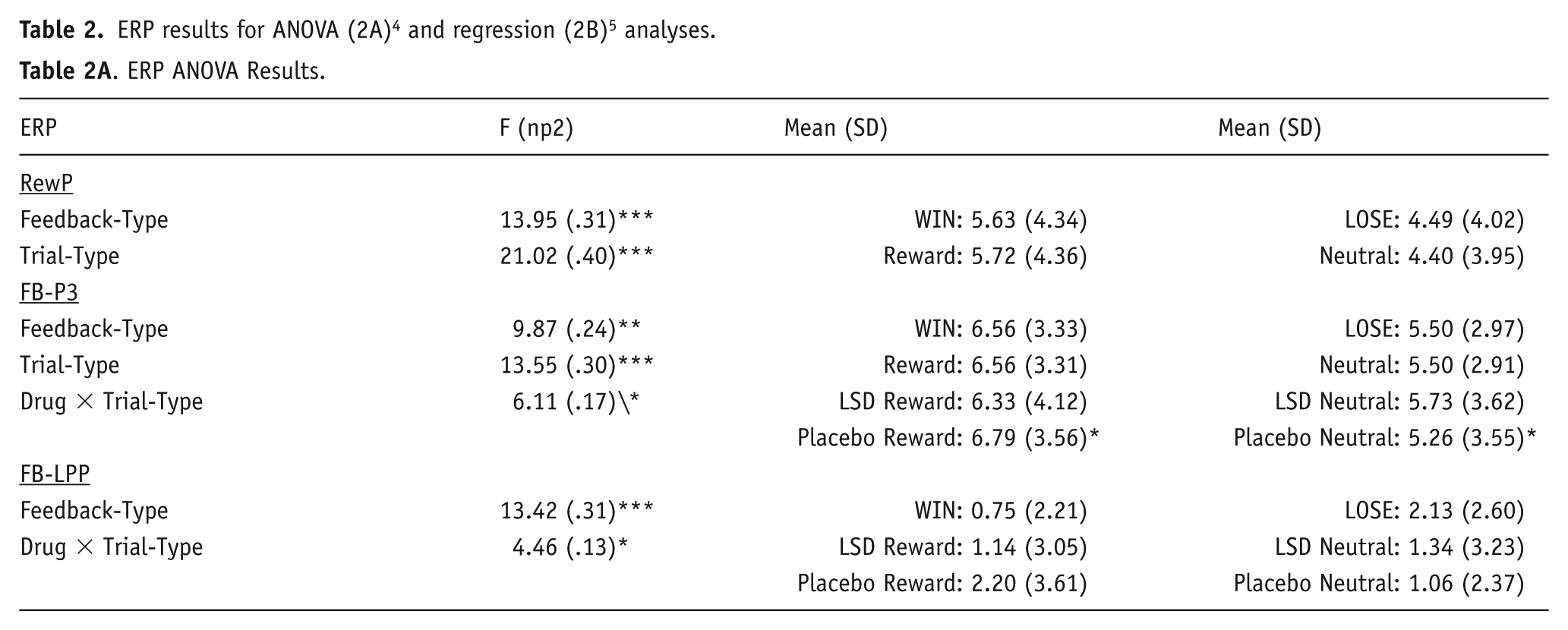
LSD did not alter RewP amplitude. Although there were significant main effects of trial-type and feedback-type on RewP amplitude (see Table 2 for ANOVA results), the drug did not affect this measure, and there were no significant effects of baseline M-BDI scores.
p < 0.05. **p < 0.01. ***p < 0.001.
LSD but not M-BDI affects FB-P3
LSD significantly decreased the differences in FB-P3 amplitude between reward and neutral trials (Significant Drug × Trial-Type interaction), regardless of WIN or LOSE feedback. Although there was a significant main effect of feedback-type on FB-P3 amplitude (see Table 2 for ANOVA results), there were no significant effects of baseline M-BDI scores. 6
LSD and M-BDI affect LPP
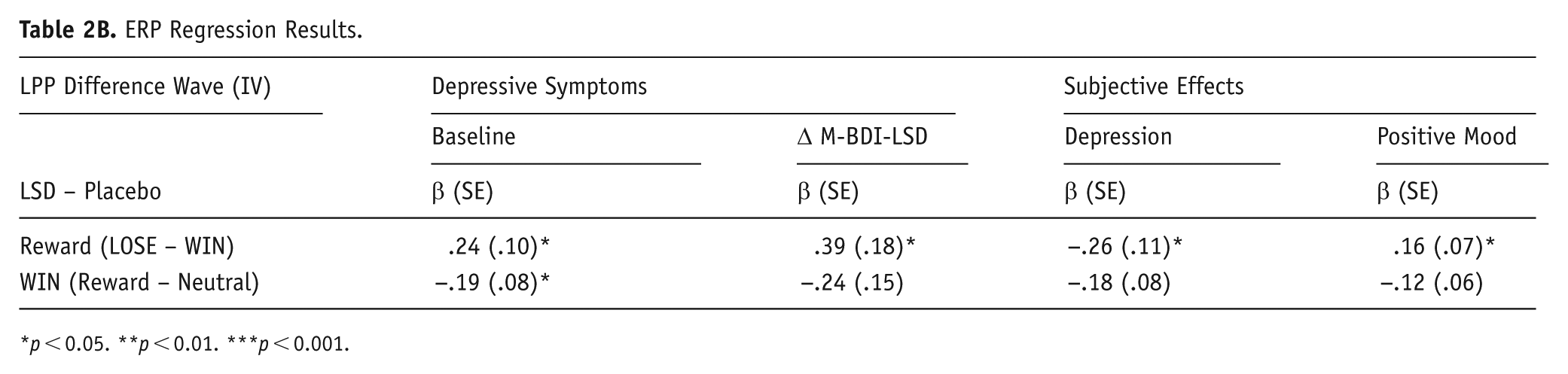
Higher baseline M-BDI scores were significantly associated with greater LPP amplitude to reward feedback (LOSE–WIN difference wave) after LSD compared to placebo (Significant Baseline M-BDI × Drug × Trial-Type × Feedback-Type interaction (F = 5.76, p = 0.023, ηp2 = 0.16, B = 0.29, SE = 0.12); see Table 2 for regression results). The differences in LPP amplitude between reward and neutral trials were significantly smaller after LSD compared to placebo (Significant Drug × Trial-Type interaction), regardless of baseline M-BDI scores or feedback-type. LPP amplitude was also significantly greater for LOSE compared to WIN feedback (significant main effect of feedback-type), regardless of trial-type or drug (see Table 2 for ANOVA results).
When ΔM-BDI-LSD scores were entered as a covariate (controlling for ΔM-BDI-placebo scores), greater reductions in ΔM-BDI-LSD scores were significantly associated with greater LPP amplitude to reward feedback (LOSE–WIN difference waves) after LSD compared to placebo (Significant ΔM-BDI-LSD × Drug × Trial-Type × Feedback-Type interaction (F = 4.50, p = 0.043, ηp2 = 0.14, B = 0.50, SE = 0.24); see Table 2 for regression results)). There were no significant effects of ΔM-BDI-placebo scores (ps > 0.063).
Interaction between LSD and subjective effects affects LPP
Higher POMS positive mood scores after LSD (compared to placebo) were significantly associated with greater LPP amplitude to reward feedback (LOSE–WIN difference waves; Significant POMS Positive Mood × Drug × Trial-Type × Feedback-Type interaction (F = 5.29, p = 0.029, ηp2 = 0.15, B = 0.21, SE = 0.09)). Smaller changes in POMS depression scores during the sessions were significantly associated with greater LPP amplitude to reward feedback (LOSE–WIN difference waves) after LSD compared to placebo (Significant POMS Depression × Drug × Trial-Type × Feedback-Type interaction (F = 6.81, p = 0.014, ηp2 = 0.19, B = −0.35, SE = 0.14); see Table 2 for regression results). There were no significant effects for POMS vigor or POMS elation (ps > 0.133).
Discussion
This study presents new evidence that baseline symptoms of depressed mood are associated with altered brain and subjective responses to a low dose of LSD. We examined the effects of a single, low dose of LSD (26 µg tartrate) on reward processing in the brain using EEG measures during a reward task, in participants who presented with mild-to-moderate versus minimal symptoms of depressed mood as measured by the M-BDI. LSD differentially affected LPP amplitude in participants with differing levels of depression: Compared to placebo, LSD increased LPP amplitude to reward feedback (LOSE–WIN difference waves) only in participants with higher M-BDI scores at baseline (Figure 1(a)–(d)). Higher baseline depressed mood was also associated with improved subjective mood states during the LSD (vs placebo) session. These acute neural and subjective effects of LSD were both associated with greater reductions in baseline depressed mood 48-hour after LSD (but not placebo) and were correlated with each other (Figure 1(d)–(g)). Higher depressed mood at baseline was also associated with increased LPP amplitude to WIN feedback on neutral trials at the LSD (vs placebo) session. Finally, compared to placebo, LSD decreased FB-P3 and LPP amplitude on reward (vs neutral) trials. Together, these results are the first to demonstrate that the neural effects of a single, low dose of LSD on LPP amplitude are associated with baseline symptoms of depressed mood. Findings provide important initial evidence that low doses of LSD may enhance emotional processing of reward in the brain, and have implications for its potential use as an anti-depressant.
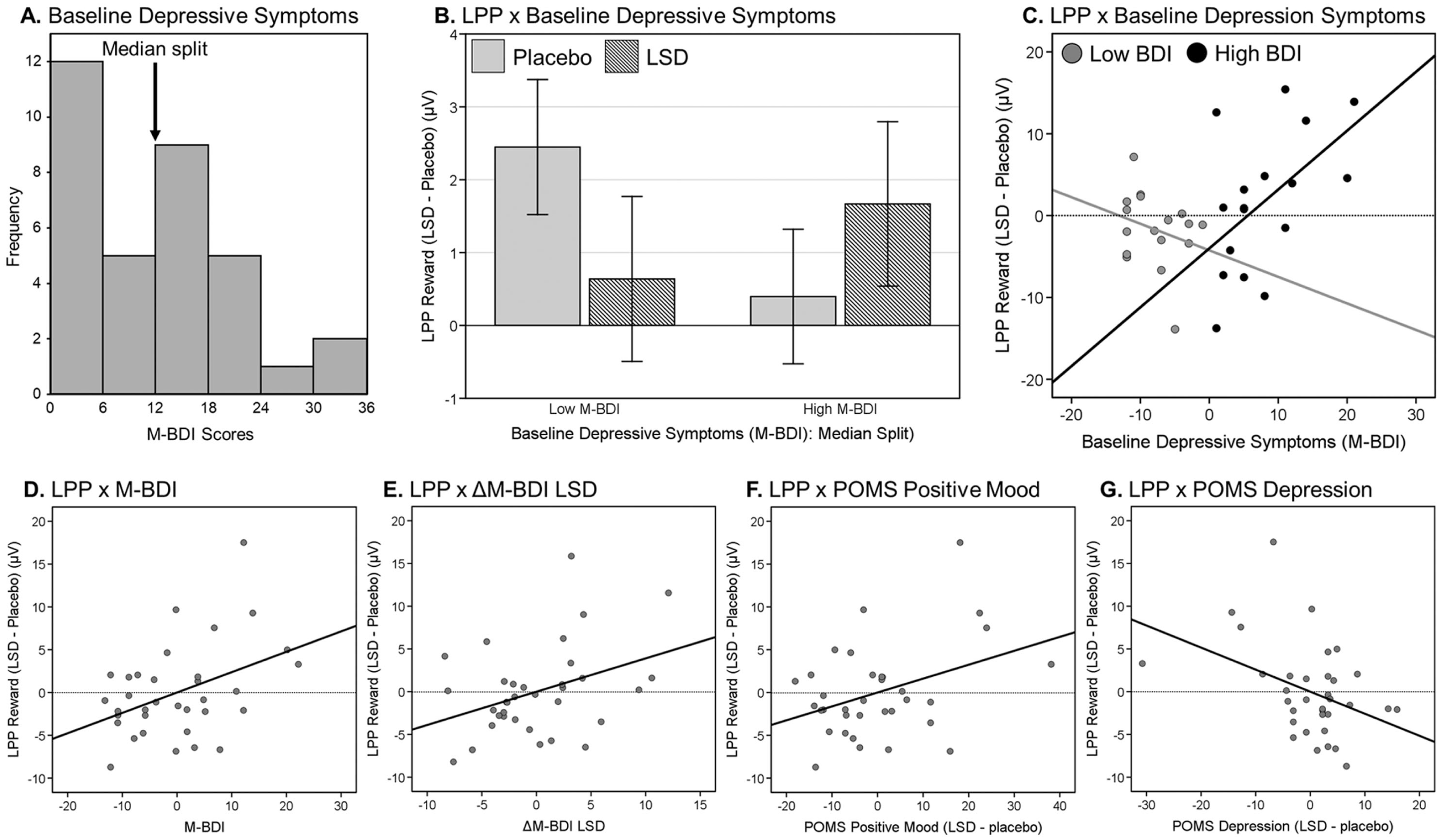
Relationships between LPP difference waves (Reward: LOSE–WIN) after LSD and depression ratings or subjective responses to LSD. (a) Displays a histogram of baseline symptoms of depressed mood (x-axis: M-BDI scores, y-axis: frequencies) with arrow showing median split (for visualization purposes only). (b) Displays bar graph of LPP difference wave (Reward: LOSE–WIN feedback) separately for LSD (dark grey bars) and placebo (light grey bars) median split for low M-BDI (left) and high M-BDI (right). (c) Displays the LPP difference wave (Reward: LOSE–WIN feedback) between LSD and Placebo sessions (LSD–Placebo) on the y-axis (voltage) and baseline depressed mood scores on the x-axis (M-BDI) with separate lines that are median split for low M-BDI (grey dots) and high M-BDI (black dots). (d)–(g) display partial regression scatterplots for LPP difference waves (Reward: LOSE–WIN feedback) between LSD and placebo sessions (LSD–placebo) on the y-axis (voltage). X-axis for panels (d) and (e) display baseline depressive symptoms (e.g., baseline M-BDI scores: panel (d)) and ΔM-BDI-LSD scores (e.g., M-BDI scores at baseline—M-BDI scores 48-hour after LSD session: panel (e)). X-axis for panels (f) and (g) display peak-change scores for subjective effect of LSD compared to placebo (LSD–placebo difference) for positive mood (panel (f)) and depression (panel (g)). All regression variables in panels (d)–(g) are mean-centered.
The present study demonstrated that a single, low dose of LSD increased neural processing of reward feedback only for individuals with higher baseline symptoms of depressed mood. At the placebo session, higher baseline depressed mood was associated with smaller LPP amplitude to reward feedback (smaller LOSE–WIN difference waves: Figure 2(a)). This pattern may reflect blunted emotional processing of reward feedback in the non-drug state. Smaller LPP amplitudes are linked to suboptimal integration of negative feedback information (Castro et al., 2019) and are associated with psychopathology (Althaus et al., 2010; Abram et al., 2020; Groen et al., 2008, Van Meel et al., 2011). Compared to placebo, LSD produced greater LPP amplitude to reward feedback in individuals with higher baseline depressed mood (larger LOSE–WIN difference waves: Figure 2(b)). This pattern suggests that the drug enhanced emotional processing of reward feedback only for individuals with higher depressed moods at baseline (Glazer et al., 2018). Greater LPP amplitude for LOSE over WIN feedback is thought to reflect an adaptive emotional response that motivates behavioral change after negative feedback (Glazer et al., 2018, Pornpattananangkul and Nusslock, 2016). Together, this pattern of results suggests LSD “normalized” the disturbed emotional processing of reward feedback in individuals with higher depressed mood at baseline, and that it reversed blunted neural responses observed in the absence of a drug (i.e., placebo).
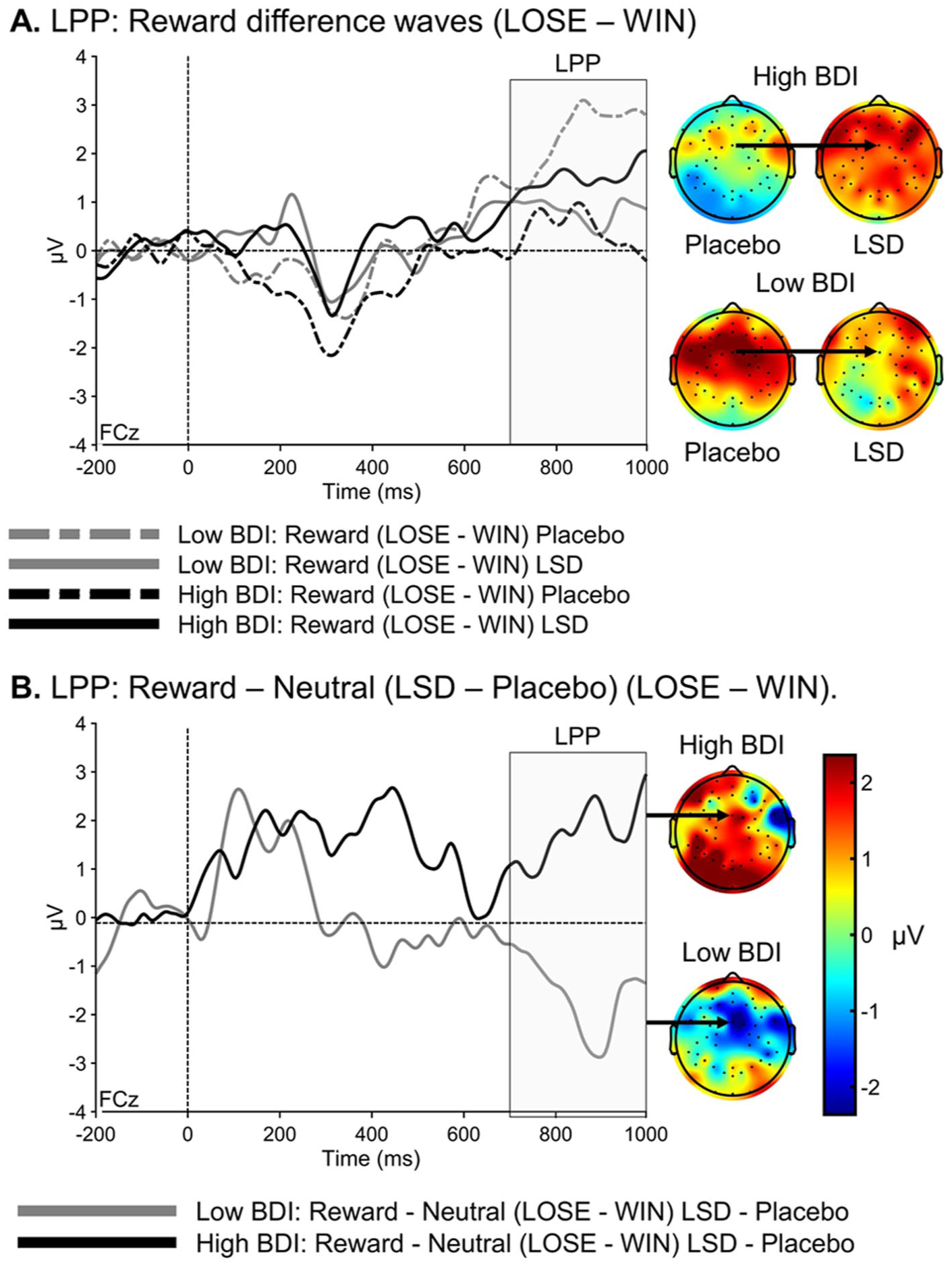
Effects of LSD and placebo on LPP difference waves. Waveforms (left side; x-axis: voltage, y-axis: time) and scalp maps (right side) for the LPP (grey area) difference waves (LOSE–WIN feedback). (a) (top) shows LPP difference waves plotted separately for LSD (solid lines) and placebo (dashed lines) and for high (black lines) and low (grey lines) baseline M-BDI depressive symptoms (median split for visualization purposes only). (b) (bottom) displays the 4-way interaction (Baseline BDI Scores × Drug × Trial-Type × Feedback-Type) separately for low (grey line) and high (black line) BDI groups with the color bar scale shown for all scalp maps.
Larger LPP amplitude to reward feedback after LSD (vs placebo) was also associated with greater decreases in M-BDI scores 48-hour after the LSD session. Thus, one process by which LSD could produce lasting changes in depressed mood is by strengthening emotional responses to reward feedback in the brain. This is consistent with previous reports that greater LPP amplitude after LOSE (vs WIN) feedback is associated with adaptive behavioral patterns that are impaired in depressive disorders (Eshel and Roiser, 2010), such as behavioral adjustments after mistakes (San Martín et al., 2013; Von Borries et al., 2013) and higher reinforcement learning rates (Althaus et al., 2010). It will be of interest to determine whether increases in sensitivity to reward signals are related to the purported long-term beneficial effects of either low (Kuypers, 2020; Passie, 2019) or higher doses of LSD (Nutt et al., 2023).
The study also revealed novel associations between neural and subjective effects of LSD, related to depressed mood. The increase in LPP amplitude to reward feedback after LSD (vs placebo) was also associated with improved mood within the sessions after LSD (vs placebo). Prior studies have linked LPP amplitude to subjective reports of emotional experience (Hajcak et al., 2010) and changes in emotional states (Klawohn et al., 2021; Proudfit, 2015; Stange et al., 2017). Importantly, the present results suggest greater emotional processing of LOSE (vs WIN) feedback during the LSD session related to improved mood states during the eMID task. Although LOSE feedback is not necessarily a positive experience, enhanced emotional processing is linked to beneficial behavioral changes after negative feedback, and heightened response may play an important role in improving subjective mood states during reward processing. This idea is consistent with prior studies that report lower LPP to negative (vs positive) feedback is associated with symptoms and psychopathology related to blunted affect, such as depressive tendencies and negative symptoms of schizophrenia (Castro et al., 2019; Glazer et al., 2019). Furthermore, both subjective and neural drug effects during the acute drug period were associated with greater reductions in baseline depressed mood 48-hour after LSD (but not placebo). These links between neural and subjective drug effects may underlie the immediate “rapid-acting” anti-depressant effects of LSD (Baumeister et al., 2014; Dos Santos et al., 2021) and contribute to lasting psychological benefit days later (Müller et al., 2017; Roseman et al., 2018).
Our findings are consistent with the idea that symptoms of depressed mood blunt emotional processing and reward sensitivity, and that LSD may reverse these deficits. In one study with healthy volunteers, a low dose of LSD (13 μg) reduced amygdala-middle frontal gyrus connectivity during rest, and this was correlated with greater positive mood (Bershad et al., 2020). Higher doses of LSD reportedly also reduce connectivity between the amygdala, prefrontal cortex, and visual cortex (Mueller et al., 2017, Müller et al., 2017, 2018), regions that covary with LPP amplitude (Bradley et al., 2003; Olofsson et al., 2008) and are disrupted in depressive disorders (Groenewold et al., 2013). The findings are also consistent with reports using psilocybin in depressed patients (Mertens et al., 2020; Roseman et al., 2018; Watts et al., 2017). Thus, there is a growing body of evidence that psychedelic drugs enhance emotional processing. Although speculative, low doses of LSD may relieve depression by reversing deficits in blunted emotional processing, an effect also observed in prior studies at higher doses and in patient populations with depressive disorders.
These findings have implications for the therapeutic effects of LSD at low doses. The findings suggest that low doses of LSD affect brain reward processing, and that these effects are related to baseline levels of depressed mood. This raises the possibility that “microdosing” produces therapeutic benefits for individuals whose baseline neurophysiological state is sub-optimal. The finding extends our report that baseline levels of depression predicted stronger subjective effects from a low dose of LSD, and that the drug improved mood 48-hour after the administration (Molla et al., 2023), by showing that these effects are accompanied by brain changes. LSD increased LPP amplitude only in individuals with mild-to-moderate depressed mood at baseline. These moderately depressed individuals displayed smaller LPP amplitude without the drug (i.e., after placebo), suggesting they may have greater capacity for improvement because of pre-existing deficits in reward feedback processing. A recent study reported that the neural effects of repeated low doses of LSD (15 µg 4 times for 4 weeks) also depended on baseline states (Hutten et al., 2024). In the Hutten study, LSD enhanced arousal and pre-attentive processing, as indexed by lower EEG power (1–13 Hz) at rest, and higher P3a ERP amplitude during an auditory task. These neural effects of LSD were strongest in individuals with lower levels of arousal and pre-attentive performance at baseline (i.e., those starting with higher EEG power and lower P3a amplitude) and persisted at 1-week follow-up. Together, these results provide a good foundation for conducting trials with low doses of LSD in clinical populations. It remains to be determined whether either single or repeated administration of low doses of LSD offers prolonged therapeutic benefit and lasting neural changes for individuals with severe psychiatric symptoms or neuropsychological deficits.
The present results can be compared to our previous studies. In our previous study, 13 µg (but not 26 µg) LSD increased LPP amplitude on reward (vs neutral) trials in healthy individuals (Glazer et al., 2023). In the present study, we found that LSD (26 µg) decreased LPP amplitude on reward (vs neutral) trials. These effects emerged regardless of feedback-type and were not related to subjective drug effects. One possibility for the discrepancy at the 26 μg dose may be differences in depressed mood, which was not measured in the previous study. Indeed, in the current study, we also found that higher depressed mood at baseline was associated with increased LPP amplitude to neutral WIN feedback (above reward WIN feedback) after 26 µg LSD compared to placebo (see Figure 3), suggesting increased emotional value after WIN feedback on neutral trials. It is also possible that the associations between neural and subjective drug effects are related to individual differences in depressed mood at baseline. This idea could explain why some neural and subjective drug effects were correlated in the current study but not in our prior study. These apparent discrepancies underline the need for replications and further studies with symptomatic participants and a range of doses.
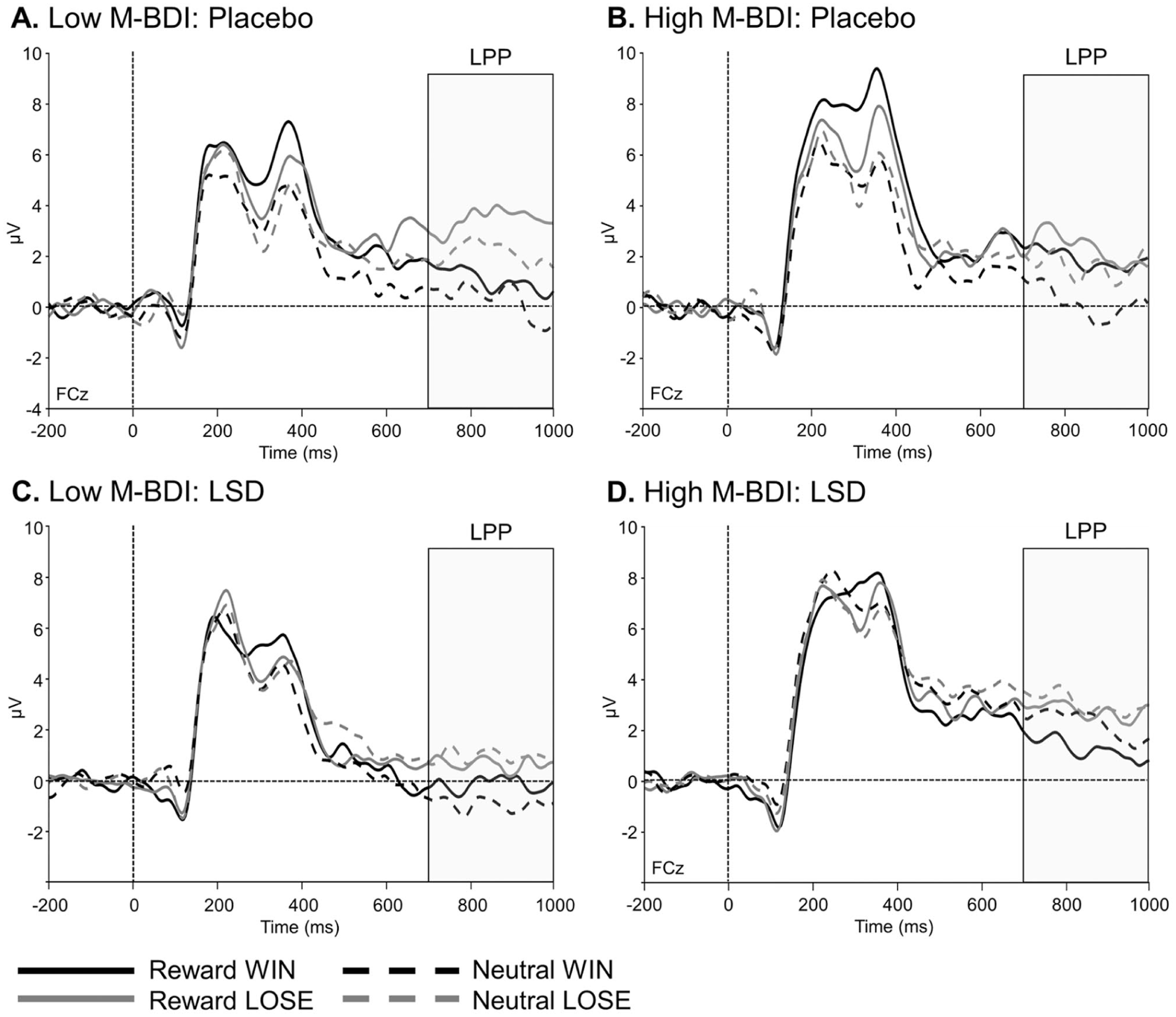
Raw LPP waveforms in different reward conditions. Four waveforms (x-axis: voltage, y-axis: time) are included in each panel on reward WIN (solid black), reward LOSE (solid grey), neutral WIN (dashed black), and neutral LOSE (dashed grey). Panels show waveforms split by baseline M-BDI depressive symptoms (median split for visualization purposes only) for low M-BDI placebo (a), high M-BDI placebo (b), low M-BDI LSD (c), high M-BDI LSD (d).
Some of the results in the present study are inconsistent with our previous report. In the previous study, but not the present study, LSD (13 and 26 μg) increased FB-P3 to WIN (vs LOSE) feedback, regardless of reward or neutral trial-type. In the current study, 26 µg LSD decreased FB-P3 amplitude on reward (vs neutral) trials, regardless of WIN or LOSE feedback-type. While feedback on reward trials typically increases motivation compared to neutral trials, this result suggests that the drug “equalized” neural differences in the motivational processing of reward and neutral trials, as indexed by comparable FB-P3 amplitudes. Contrary to our hypotheses, the effect of LSD on FB-P3 amplitude was unassociated with symptoms of depressed mood.
One hotly debated issue is whether widespread anecdotal claims of the subjective benefits of taking repeated low doses of LSD are due to placebo effects (Polito et al., 2024). In an exploratory analysis, we found that the impact of LSD on FB-P3 amplitude was not related to subjective effects of the drug, consistent with our prior study (Glazer et al., 2023). An intriguing possibility is that low doses of LSD may offer subjectively undetected benefits through subtle changes in brain function that cannot be explained by placebo effects. However, whether these effects are beneficial or detrimental may depend on individual differences at baseline. For example, in a recent study, repeated low doses of LSD impaired memory more strongly in individuals with superior memory performance at baseline, as indexed by reduced P200 amplitudes during a visual long-term potentiation paradigm (Hutten et al., 2024). Given the role of FB-P3 in updating working memory, it is possible that low doses of LSD may disrupt reward feedback processing in highly motivated individuals with large FB-P3 amplitudes at baseline by reallocating attentional resources toward neutral trials. Future work is needed to understand the specific effects of LSD on FB-P3 and whether low doses of LSD or other psychedelic drugs may offer subjectively undetectable benefits.
It is notable that LSD (26 µg) failed to affect RewP, an ERP signature associated with reward. In our previous study, we found 13 µg, but not 26 µg, LSD increased RewP amplitude (Glazer et al., 2023). The reason for the non-linear dose effect in the previous study is unclear but, as with some other psychoactive drugs (Karlsson and Roman, 2016; Rubino et al., 2007), there may be a “sweet spot” as described in anecdotal reports of microdosing, for an optimal dose (Spotswood, 2022). Future studies with a range of doses are needed to better understand these effects on RewP amplitude and whether they may differ for individuals with more severe depressed mood or those who meet diagnostic criteria for depressive disorders and psychiatric symptoms.
The study had both strengths and limitations. Strengths included the controlled, double-blind design, the rigorous criteria for inclusion and exclusion, and the use of standardized outcome measures. Another strength is the dimensional assessment of current depressed mood from baseline M-BDI scores (Hankin et al., 2005; Ruscio and Ruscio, 2002), which improve validity and statistical power over traditional categorical models (Cicchetti et al., 2009; Watson, 2005). One limitation is that the study only included individuals with momentary symptoms of depressed mood while formal diagnoses of depression involve symptoms lasting several weeks, which were not assessed here. Another limitation is the modest sample size, limiting power, and the capacity to examine individual differences in responses to the drug. Importantly, the participants reported low levels of depressed mood, leaving open the question of whether individuals with more severe depressed mood or those diagnosed with depressive disorders would exhibit different responses. Further, it is possible that the changes in depressed mood on the drug sessions were the result of chance differences between drug and placebo sessions. Finally, it will be important to extend this type of study from single doses to repeated that are used outside the laboratory.
Studies such as the present one are essential to understand the neural effects of low doses of psychedelic drugs and to investigate their therapeutic potential. There are widespread claims that repeated ingestion of low doses of LSD has beneficial effects on mood and cognition. However, it remains to be determined whether these reports are based on expectancies and context, or the pharmacological effects of the drug, or the neurobiological effects of the drug on neural processing of reward signals. Studies like the present one, examining changes in brain processing of reward feedback in individuals with psychiatric symptomatology, may reveal how these drugs can affect behavior by altering reward processing in the brain.
Supplemental Material
sj-docx-1-jop-10.1177_02698811251405686 – Supplemental material for Reward-related neural activity after low doses of LSD in participants with depressed mood
Supplemental material, sj-docx-1-jop-10.1177_02698811251405686 for Reward-related neural activity after low doses of LSD in participants with depressed mood by James Glazer, Hanna Molla, Royce Lee, Robin Nusslock and Harriet de Wit in Journal of Psychopharmacology
Footnotes
Ethical considerations
The study was approved by the Institutional Review Board of the Biological Sciences Division of the University of Chicago (IRB15-1311 approved on 10/31/2023).
Consent to participate
All participants provided written informed consent to voluntarily participate in this study at the in-person orientation session where they were familiarized with all research activities and procedures. Participants were informed they might receive a placebo, stimulant, sedative, or hallucinogen.
Consent for publication
Not applicable.
Author contributions
James Glazer, Robin Nusslock, Royce Lee, and Harriet de Wit have all significantly contributed to at least one or more of the four criteria described by the International Committee of Medical Journal Editors and Journal of Psychopharmacology (A) the conception and design of the study, acquisition, analysis, and interpretation of data, (B) drafting and revising the present work, (C) final approval of version to published, and (D) accountability agreement for all aspects ensuring the accuracy and/or integrity of any part of the work are appropriately investigated and resolved. Harriet de Wit led the conceptualization, writing of the manuscript, and funding acquisition for the study. James Glazer performed data processing, managed software, conducted formal analysis, contributed to data curation, and led the writing of the manuscript. Hanna Molla led the study methodology, assisted with data collection and investigation, and assisted in the writing of the manuscript. Royce Lee supervised the data processing and data curation, oversaw the study methodology and investigation, and assisted with study methodology. Robin Nusslock supervised statistical analysis and interpretation of data, assisted with study methodology, and contributed to writing the manuscript. All authors contributed to and have approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIDA DA02812. Research reported in this publication was also supported in part by the National Institutes of Health’s National Center for Advancing Translational Sciences, Grant Number TL1TR001423, and NIH grant T32 NS047987. HM was supported by the National Institute of Health T32 GM07019.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Harriet de Wit serves on the Board of Directors of PharmAla Biotech and has served as Scientific Advisor to Awakn Life Sciences, Gilgamesh Pharmaceuticals, and Mind Foundation. These roles are unrelated to the research reported here. Authors have no conflicts of interest to disclose.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.