
Abstract
Background:
One of the most robust acute effects of cannabis is impaired memory. Although memory is not a unitary construct, most cannabis research has focused on verbal memory. Less is known about its effects on more ecologically valid domains of memory, such as prospective and temporal order memory.
Methods:
We conducted a randomized, double-blind, placebo-controlled study to map out which aspects of memory are impaired following acute cannabis use. Cannabis-using participants (N = 120) were randomly assigned to vaporize flower containing 0 mg Δ-9-tetrahydrocannbinol (THC; placebo), 20 mg THC (moderate dose) or 40 mg THC (high dose) before completing a battery of memory tests, including tests of verbal memory (immediate, delayed, short-term, working), visuospatial memory (immediate, delayed, short-term, working), prospective memory (event-cued, time-cued), source memory, false memory, episodic content memory, and temporal order memory.
Results:
Relative to placebo, cannabis increased susceptibility to false memories and detrimentally impacted verbal memory (immediate, delayed, working), visuospatial memory (immediate, delayed), event-cued prospective memory, source memory, and temporal order memory. There were no significant differences between the moderate and high dose groups.
Conclusion:
This is the first study to detect acute effects of cannabis on prospective memory and temporal order memory, which is important because these tests better reflect everyday memory and predict daily functioning. Collectively, these results indicate that acute cannabis use has broad detrimental effects on most domains of memory rather than selectively impairing a limited number of these domains. The study was pre-registered on clinicaltrials.gov (#NCT05488509) at https://clinicaltrials.gov/study/NCT05488509.
Introduction
One of the most robust detrimental effects of acute cannabis intoxication is on memory. However, memory is not a unitary construct. Rather, memory is a complex system comprised of multiple, distinct, subsystems that are interrelated, have unique characteristics and developmental courses, employ different neural mechanisms, and can be selectively impaired (Cowan, 1995, 2008; Schacter & Tulving, 1994; Squire, 2004; Tulving, 1985). Nevertheless, the overwhelming bulk of previous research on humans has rather narrowly focused on the impacts of acute cannabis intoxication using verbal memory tests, which involve remembering lists of words, and working memory tests, which require temporarily storing and manipulating information (for reviews see Broyd et al., 2016; Crane et al., 2013; Dellazizzo et al., 2022). Far fewer studies have considered impacts of acute cannabis use on more ecologically valid memory tests that better reflect the events and tasks people need to remember in everyday life, such as temporal order memory (the ability to remember the order in which past events occurred), prospective memory (the ability to remember to execute tasks in the future), source memory (the ability to remember the source of previously learned information), false memory (falsely recalling information that was not previously presented), and episodic content memory (the ability to recall personally experienced events in which the participant was actively engaged).
Specifically, only one prior study has examined the acute effects of cannabis on temporal order memory (Cuttler et al., 2021) and prospective memory (Cuttler et al., 2021). Although that study failed to detect significant effects on either domain of memory, it was only powered to detect large-sized effects. Moreover, it did not include a placebo control group, and it focused on event-cued prospective memory, which requires participants to remember to perform tasks upon the occurrence of a specific event (Cuttler et al., 2021). The potential impact of cannabis on time-cued prospective memory, which requires participants to remember to perform tasks at a specific time or after a specific amount of time has elapsed, is unknown. Similarly, only a handful of studies have examined the acute effects of cannabis on source memory (Cuttler et al., 2021; Ilan et al., 2004; Morgan et al., 2010) and false memory (Cuttler et al., 2021; Ballard et al., 2012; Doss et al., 2018; Kloft et al., 2019, 2020), with mixed evidence of impairments for each domain. To our knowledge, no prior studies have examined the impacts of cannabis on the ability to recall personally experienced events. Impoverished knowledge of the impacts of cannabis on more naturalistic memory domains is problematic as they are highly relevant to daily life and predict everyday functioning better than more traditional verbal memory tests (Schmitter-Edgecombe et al., 2009).
To our knowledge, no prior research has examined all these aspects of memory in a single study. This is concerning because considerable variability in methodologies exists across studies, including location (lab vs field), method of administration (oral, smoked, vaped), potency of cannabis, and lack of inclusion of a placebo control group, which complicates cross-study comparisons within different memory domains. Thus, the purpose of the present study was to utilize a comprehensive battery of memory tests to determine which domains of memory are impaired and which are spared under conditions of acute cannabis intoxication. Specifically, we examined the impacts of a moderate (20 mg Δ-9-tetrahydrocannbinol (THC)) and high dose of cannabis (40 mg THC) on verbal memory (immediate, delayed, short-term, working), visuospatial memory (immediate, delayed, short-term, working), prospective memory (event-cued, time-cued), source memory, false memory, temporal order memory, and episodic content memory using a large sample and a randomized, double-blind, placebo-controlled design.
Methods and materials
Design
A randomized, double-blind, placebo-controlled, parallel group study was conducted to examine acute effects of cannabis on multiple memory domains. Participants were randomly assigned to vaporize placebo, a moderate dose of cannabis, or a high dose of cannabis. RJM used Excel’s random number generator to randomly assign participants to conditions with a 1:1:1 allocation ratio and kept the experimenter (CC) blind to this list.
Approvals
The study was approved by Washington State University’s Institutional Review Board, an Investigational New Drug (IND) application was approved by the FDA (#164993), and RJM has a Schedule 1 license from the Drug Enforcement Agency (DEA) to handle and administer cannabis. The study was pre-registered on clinicaltrials.gov (#NCT05488509) on June 6, 2023 and a certificate of confidentiality was obtained from the National Institutes of Health to protect participants’ confidentiality. Participants were tested between August 21, 2023 and May 17, 2025.
Power
A power analysis conducted using G-Power (Erdfelder et al., 1996) indicated that a sample size of 156 participants would afford power of 0.80 to detect medium-sized effects (i.e.,
Inclusion/exclusion criteria
Participants were required to be at least 21 years of age, fluent in English, and to use cannabis ⩾ once a week for ⩾1 year. Participants were not eligible if they reported being diagnosed with a serious psychiatric condition (psychosis, bipolar I, panic disorder) or a family history of psychosis. Participants were also not eligible if they reported having any learning disorders, neurological disorders, heart disease or medical conditions impacting cognition (e.g., diabetes), multiple concussions or head injury with loss of consciousness, pregnancy or lactation, a body mass index (BMI) > 34 (computed by investigators using height and weight data), use of illicit drugs in the past 6 months, current tobacco or nicotine use (given the memory-enhancing effects of nicotine), heavy alcohol use (>4 drinks, ⩾4 times/week), or a history of serious adverse reactions to cannabis (e.g., panic attacks, psychosis). One participant who did not typically inhale cannabis had an adverse event, and therefore regular inhalation of cannabis was added as an inclusion criteria mid-way through the study.
Materials
Study drug
Placebo and dried cannabis flower were obtained from the National Institute on Drug Abuse Drug Supply Program. We obtained cannabis (barrel #1592) containing 11.86% Δ9 THC, 1.12% cannabidiol (CBD), 0.32% cannabichromene (CBC), 0.41% cannabigerol (CBG), 0.77% cannabinol (CBN), and 0.10% tetrahydrocannabivarin (THCV). The placebo (Lot #1004-1904-01) contained <0.025% Δ9 THC, 0.03% Δ8 THC, 0.14% CBD, <0.025% CBC, and <0.01% CBG, CBN, and THCV. Participants in the moderate dose condition were administered 20 mg THC (0.17 g of 11.86% THC cannabis flower) and those in the high dose condition were administered 40 mg THC (0.34 g of 11.86% THC cannabis flower). Participants in the placebo condition were administered 0.17 g of placebo plant material. Cannabis and placebo were stored in a DEA-approved locked refrigerator, and each dose was removed and weighed a maximum of 24 hour prior to each testing session.
Weschler Test of Adult Reading
The Weschler Test of Adult Reading (WTAR) is a brief measure of premorbid verbal IQ (Holdnack, 2001). The test consists of a list of 50 words that participants pronounce aloud. They are given 1 point for each correctly pronounced word; therefore, total scores can range from 0 to 50 with higher scores reflecting better premorbid verbal IQ. This test was used to ensure the three groups had comparable cognitive abilities at baseline.
Prospective memory tests
Participants’ ability to remember to execute tasks in the future was assessed with two prospective memory tests: the Difficulty Ratings Test (Cuttler et al., 2021, 2023) and the Bell Test (Einstein and McDaniel, 1996). The Difficulties Ratings Test is an event-cued prospective memory test that requires participants to rate the difficulty of each test they completed immediately after completing it, using a 0 (not at all difficult) to 10 (extremely difficult) scale. The percentage of tests each participant provided difficulty ratings for was computed as an index of event-cued prospective memory test performance; therefore, scores can range from 0 to 100, with higher scores reflecting better event-cued prospective memory.
The Bell Test is a time-cued prospective memory test that required participants to ring a bell every 10 minutes. Participants had continual access to a clock positioned next to the bell to keep track of the time. Participants received 0 points if they failed to ring the bell, 1 point if they rang it late, and 2 points if they rang the bell in precisely 10 minutes (based on minutes not seconds). These points were summed and converted to a percentage as an index of time-cued prospective memory test performance; therefore, scores can range from 0 to 100 with higher scores reflecting better time-cued prospective memory.
California Verbal Learning Test-II
The California Verbal Learning Test II (CVLT-II; Delis et al., 2000) was used to assess immediate and delayed verbal free recall. Participants were asked to listen to and immediately recall a list of 16 words 3 times in a row (List A). This was slightly modified from the standardized version, which requires presentation and recall of List A five times in a row, to reduce the potential for ceiling effects. They were then asked to listen to, and immediately recall, a list of 16 new words (List B). Immediately following recall of List B, participants were required to recall the words from List A without re-presentation of the list. The mean number of words they were able to recall across these four trials was used as an index of immediate verbal memory. As such, scores can range from 0 to 16, with higher scores reflecting better immediate verbal memory. Approximately 12 minutes later, participants were asked to recall List A without re-presentation. The number of words they correctly recalled (out of 16) on this trial served as an index of delayed verbal memory. We also summed the total number of intrusions (false recall of words not on the lists) across all six trials of the CVLT-II as an index of susceptibility to false memories.
Brief Visuospatial Memory Test—Revised
The Brief Visuospatial Memory Test—Revised (BVMT-R) was used to assess visuospatial memory (Benedict, 1997). For this test, participants were shown an array of 6 geometric figures for 10 seconds and then were asked to draw as many of the figures as they could in their correct location on the page. This trial was repeated a second time. They were given 1 point for each correct figure they drew and 1 point if the figure was in its correct location (for a total of 12 points per trial). Scores on these two trials were averaged to derive the index of immediate visuospatial memory. As such, scores can range from 0 to 12, with higher scores reflecting better immediate visuospatial memory. Participants were also asked to reproduce the figures in their correct locations approximately 10 minutes after the second immediate recall trial (without re-presentation of the figures) for an index of delayed visuospatial memory. Scores on this trial could also range from 0 to 12.
Corsi Block Tapping Test
An online version of the Corsi Block Tapping Test (Corsi, 1972) forward was used to measure visuospatial short-term memory, and the backwards version of the test was used to measure visuospatial working memory. For the forward version, participants saw a series of blocks light up in a sequence, and they had to click the same blocks in the same sequence in which they lit up. For the backward version, participants had to click the same blocks in the reverse sequence in which they lit up. The tests started with sequences of two and became increasingly longer until the participant failed two trials of the same length. Scores reflected the highest sequence lengths they could accurately complete for each test.
Picture/word test
For the encoding portion of the picture/word test (Schmitter-Edgecombe et al., 2009), participants saw 32 basic pictures (e.g., black and white line drawings of common objects and animals such as an envelope, hat, and horse) and printed words for 2 seconds each. They were asked to read the words aloud and identify the pictures aloud. After an approximate 7 minutes retention interval, they completed a free recall trial where they were asked to freely recall as many items as possible as an index of delayed verbal free recall. Next, to assess source memory, they completed a recognition test for which they were presented with 64 words and were asked to identify whether each was presented previously as a picture or a word or whether the item was not presented earlier. Source memory discrimination indices were computed based on the single-source conditional-source identification measure (Schmitter-Edgecombe et al., 2009). Specifically, the discrimination index for picture memory was calculated as (Correctpic/(Correctpic + False Alarmspic)), and the discrimination index for word memory was calculated as (Correctword/(Correctword + False Alarmsword)) where Correct represents the number of pictures/words that were correctly identified, and False Alarms represents the number of pictures/words that were incorrectly identified. Therefore, the discrimination indices for picture and word memory can range from 0 to 1 and represent the proportion of total pictures/words that were accurately identified.
False Memory Test
The Deese–Roediger–McDermott Paradigm was used to assess susceptibility to false memories (Roediger and McDermott, 1995). Participants heard 6 lists of 12 words that each related to 1 critical lure word that was not on the list. For example, a list might include the words: tired, pillow, bed, dream, and night, while the critical lure word “sleep” that directly relates to each of the words in the list is never presented. For the immediate free recall trial, participants recalled as many words as they could from each list immediately after hearing each. After a 5-minute retention interval, participants completed a recognition test that contained 42 words, including 12 old words, 6 critical lures, 12 new related words (i.e., words which were related to the theme of an original list, but not as directly related as the critical lure word), and 12 new unrelated words (i.e., words that were completely unrelated to the theme of the original lists). False identification of critical lures, related words, and unrelated words was used to measure false memory. We computed the average number of words they recalled on each trial of the free recall portion of the test as an index of immediate verbal memory; therefore, scores on the free recall trial could range from 0 to 12. We computed the total number of intrusions on the free recall trials as an index of false memories. Finally, we computed the proportion of critical lures (total number of critical lures identified as old/total number of critical lures), related words (total number of related words identified as old/total number of related words), and unrelated words (total number of unrelated words identified as old/total number of unrelated words), they falsely recognized as primary indices of false memories. Scores on these could range from 0 to 1.
Digit span forward and backwards tests
The digit span forward test was administered as a measure of verbal short-term memory and the digit span backwards test was administered as a measure of verbal working memory (Wechsler, 1997). For the forward version, participants hear sequences of numbers and repeat/recall each in the same order in which they were presented. For the backwards version, participants hear sequences of numbers and repeat/recall each in the reverse order in which they were presented. The number of digits in the sequence begins with 2 and increases one at a time up to a length of 8 numbers for the forward version and 7 numbers for the backwards version. Each test includes two sequences of each length, and testing ceases if a participant fails to correctly recall any two sequences of the same length. The total number of sequences successfully recalled on each version of the test served as our measures of verbal short-term and working memory, respectively. Possible scores on the short-term memory test range from 0 to 16, while scores on the working memory test range from 0 to 14.
Episodic Content Memory Test
To assess the ability to recall events participants actively engage in, participants were asked to freely recall and describe all the tasks they completed during the testing session (Schmitter-Edgecombe et al., 2009). There were a total of 15 distinct tests and subtests that could be recalled. Participants received 1 point for each test or subtest they correctly recalled and/or accurately described. When participants’ descriptions of tasks were ambiguous or unclear, the experimenter asked neutral clarification questions (e.g., “Can you tell me more about that task?”) until it was evident which specific test or subtest they were referring to. The experimenter gave 1 point for each correctly identified task/subtask, and the total number was summed as a measure of episodic content memory; thus, scores could range from 0 to 15.
Temporal Order Memory Test
To assess memory for the sequential order of past events, participants were presented with 15 cards, each describing a test/subtest, and were asked to organize them in the order in which they were administered (Schmitter-Edgecombe et al., 2009). Participants’ responses were individually scored from 0 to 2. Participants received a score of 2 for each test they recalled in the correct sequence. They received a score of 1 for each test they switched the order with an adjacent test. If participants recalled tests in an order that was completely out of sequence, they received a score of 0 for the test. Individual scores were then summed to create a total temporal order memory score. Scores could range from 0 to 30.
Supplemental Table 1 shows the correlations between each of the various memory test outcomes. The shaded areas of the table highlight that, with a couple of minor exceptions, tests within each memory domain (verbal memory, visuospatial memory, prospective memory, source memory, false memory) are significantly correlated with one another. One exception to this trend is the verbal short-term memory test, which was only significantly correlated with the verbal working memory test and delayed free recall trial of the false memory test.
Procedure
Participants were recruited using advertisements posted in cannabis dispensaries, on Washington State University campus, in the community, and on social media, as well as by emailing cannabis-using participants from recent prior studies. Advertisements and emails contained links to an online Qualtrics screening survey that contained questions probing the various inclusion/exclusion criteria reported above to determine eligibility. Eligible participants were contacted and instructed to abstain from using cannabis on the day of their scheduled testing session (from midnight until their session).
Upon arrival at The Health and Cognition lab at Washington State University, participants provided written informed consent. They were then asked to show ID verification of their age and report when they last used cannabis. They next completed a 12-panel urine drug test to ensure they had not recently used illicit drugs. Next, they rated their level of intoxication (T0) using a 0 (not at all) to 10 (extremely) visual analogue scale. All participants gave baseline intoxication ratings of 0 consistent with the required abstinence period. Participants then completed the WTAR (Holdnack, 2001) as an index of premorbid verbal IQ. Participants then completed an online survey that contained demographic questions and the Daily Sessions, Frequency, Age of Onset, and Quantity of Cannabis Use Inventory (DFAQ-CU; Cuttler and Spradlin, 2017) to measure cannabis use patterns.
Participants were brought to a vaping room that contained a fume hood to evacuate residual vapor. Cannabis or placebo was pre-loaded into the chamber of a Volcano MEDIC 2 vaporizer (donated to the THC lab by Storz & Bickel, GmbH, Tuttlingen, Germany) by RJM with the appropriate dose, a maximum of 24 hours prior to each participant’s arrival. The experimenter (CC) and participants were blinded to the product in the sealed chamber, and a black cloth was placed on the Volcano whip to help with blinding. After heating the vaporizer to 210°C, participants were instructed to inhale for a minimum of 2 seconds, hold for a minimum of 2 seconds, and then exhale into a carbon filter “sploofy.” They were instructed to inhale the full dose but were informed that they could discontinue the session if the effects became too strong or uncomfortable. The experimenter observed the participant during the vaping session and timed the duration of each inhalation and hold and recorded the number of puffs each participant took.
After the vaping session was complete, participants were brought back to a testing room and were asked to rate their level of intoxication (T1) using a 0 (not at all) to 10 (extremely) visual analogue scale. They then completed approximately 1 hour of memory tests (they started the memory tests approximately 7 minutes after the vaping session ended). Specifically, participants completed the following tests in the following fixed order: Difficulties Rating Test (event-cued prospective memory), Bell Test (time-cued prospective memory), CVLT-II (immediate verbal memory), BVMT-R (immediate visuospatial memory), Picture/Word Test Encoding, Corsi Block Tapping Test Forward (visuospatial short-term memory), Corsi Block Tapping Test Backwards (visuospatial working memory), CVLT-II Delayed Recall (delayed verbal memory), BVMT-R Delayed Recall (delayed visuospatial memory), Picture/Word Test Delayed Free Recall (delayed verbal memory), Picture/Word Test Recognition (source memory), False Memory Test Free Recall (verbal memory and intrusions), Digit Span Forwards (verbal short-term memory), Digit Span Backwards (verbal working memory), False Memory Recognition Test (false memory), Episodic Content Memory Test (episodic content memory), Temporal-Order Memory Test (temporal order memory). Participants were asked to rate their level of intoxication and drug effects using a 0 (not at all) to 10 (extremely) visual analogue scales midway through the tests (T2) and immediately after completing these tests (T3). They were also asked to rate how much they liked the drug effects using a 0 (dislike very much) to 10 (like very much) visual analogue scales at these same two time points (T2 and T3).
Participants were then brought to an adjacent “chill out room” furnished with couches and chairs, a TV, a PlayStation 4, video games, books, and magazines and containing a wide variety of snacks and beverages. Participants remained in the chill out room for a minimum of 3 hours (until it had been a minimum of 4 hours since the vaping session ended and they gave a 0 intoxication rating) and then were debriefed and compensated with a $100 MasterCard gift card. A small number of participants reported feeling intoxicated after 3 hours in the chill out room and remained in the lab until they gave a 0 intoxication rating.
Data analysis
Data were screened for outliers defined as values more than ±3.29 standard deviations from the mean (Tabachnick and Fidell, 2013). A total of 0.5% of the data were identified as outliers and were trimmed to one unit higher or lower than the closest non-outlying raw score value (Tabachnick and Fidell, 2013).
Chi-square tests were used to ensure the three groups were comparable with respect to gender, ethnicity/race, education, income, and employment status. One-way between-group analyses of variance (ANOVA) were used to ensure the groups were similar with respect to age, BMI, duration of abstinence from cannabis (hour), frequency of cannabis use, quantity of cannabis use, years of cannabis use, and age of onset of cannabis use.
Cannabis exposure was quantified by total number of puffs, mean duration of inhalations (seconds), and mean duration of holds (seconds). One-way between-group ANOVAs were used to examine differences in each of these metrics across the three drug conditions.
A 3 × 3 mixed factorial ANOVA, with drug condition (placebo, moderate dose, high dose) as a between-subjects factor and time (T1, T2, T3) as a within-subjects factor was used to examine post-vaping intoxication, drug effect, and drug liking ratings. When the assumption of sphericity was violated, Greenhouse–Geisser adjusted statistics are reported. Significant drug condition × time interactions were decomposed by conducting separate one-way between-subjects ANOVAs at each of the three timepoints. Significant one-way ANOVAs were followed up with Tukey’s post hoc tests (which control for multiple comparisons) to determine which drug conditions differed significantly from one another at each time point.
To assess the impacts of cannabis use on memory test performance, one-way ANOVAs were conducted with condition (placebo, moderate dose, high dose) as a between-subjects factor and memory test outcomes as dependent variables. Significant main effects were probed using Tukey’s post hoc tests. Alpha was set to 0.05, and the Benjamini–Hochberg procedure was used to adjust p-values to reduce false discovery rate across all 21 memory test outcomes.
A sensitivity analysis was conducted after excluding the participants in the cannabis conditions that did not inhale the full dose. The Benjamini–Hochberg procedure was used to independently adjust p-values for this series of analyses. Finally, to probe for potential dose effects, correlations between intoxication ratings at T1, number of inhalations, and each of the memory test outcomes were computed. Alpha was set to 0.05 for these correlation analyses.
Results
Participants
One participant in the high dose condition experienced a mild adverse event (vomiting) prior to completing the memory tests and was excluded. There were no other adverse events. The final sample comprised 120 regular cannabis users (56 men, 52 women, 12 non-binary/transgender), with 40 participants in each group. See Figure 1 for a consort flow diagram detailing exclusions.
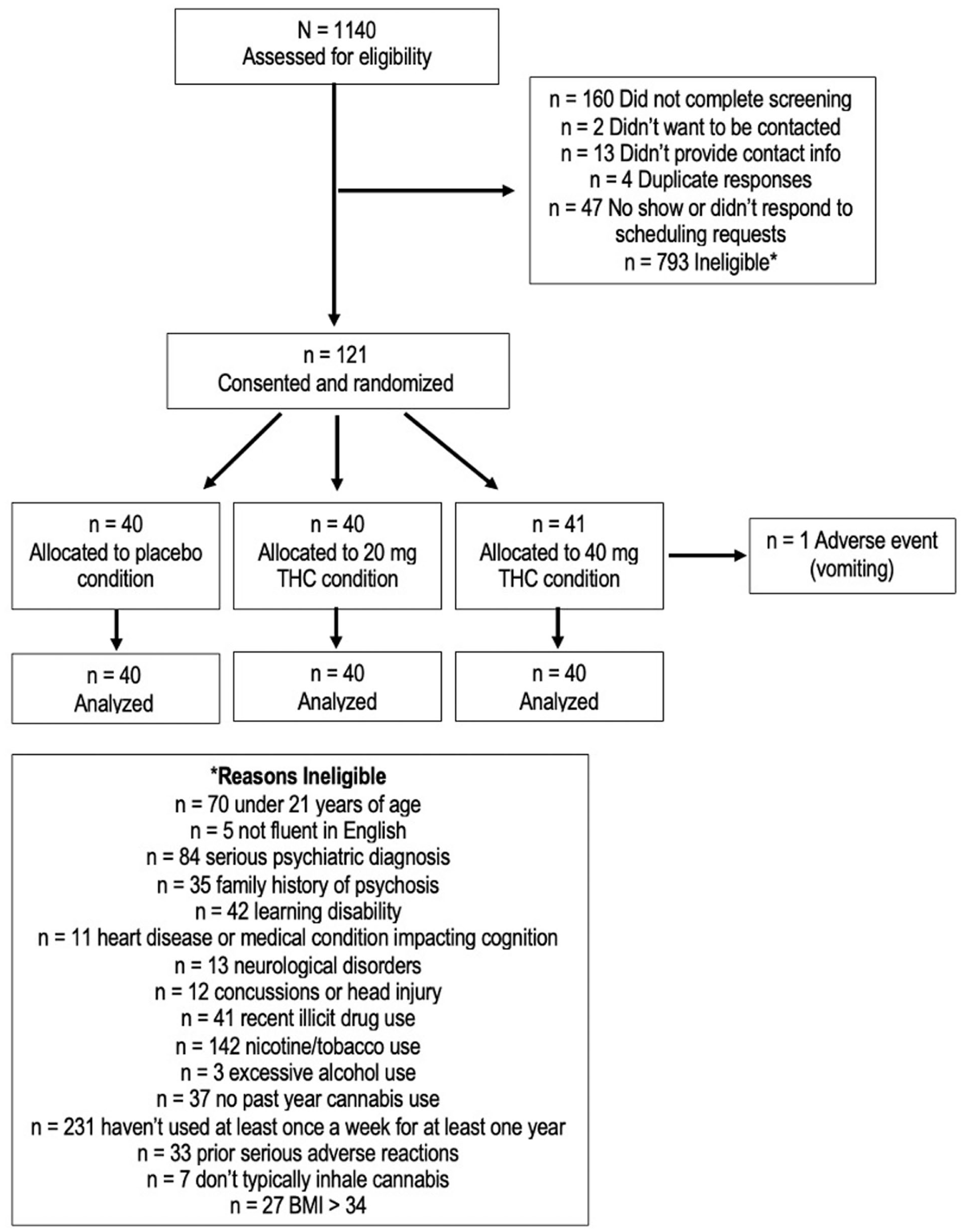
Consort flow diagram showing the total number of people assessed for eligibility, randomized, tested, and analyzed with reasons for exclusions.
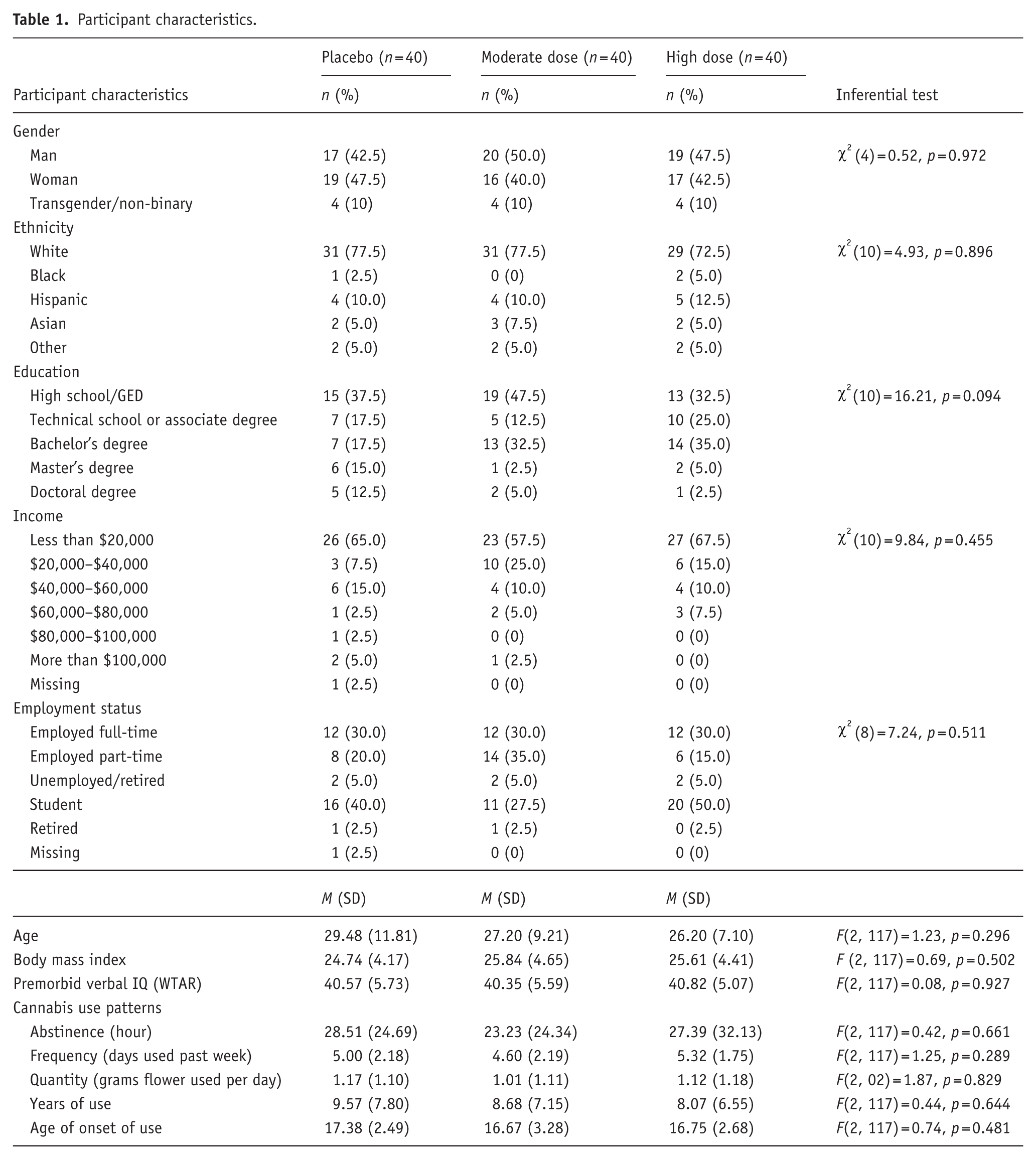
As shown in Table 1, participants in the three conditions were comparable with respect to demographic characteristics and cannabis use patterns. Furthermore, there were no significant differences across the groups in the reported hours since they last used cannabis with an overall mean abstinence period of 26.4 hour (see Table 1).
Participant characteristics.
Cannabis exposure
A total of 10 participants in the high dose condition, 3 participants in the moderate dose condition, and 1 participant in the placebo condition refused to inhale the full dose because they found the effects too strong/uncomfortable.
As depicted in Supplemental Figure 1A, there was a large-sized significant difference in the number of inhalations participants took across the three conditions, F(2, 117) = 18.09, p < 0.001,
Drug effect ratings
As shown in Figure 2(a), there was a large-sized significant drug condition × time interaction on intoxication ratings, F(3.24, 189.44) = 7.69, p < 0.001,
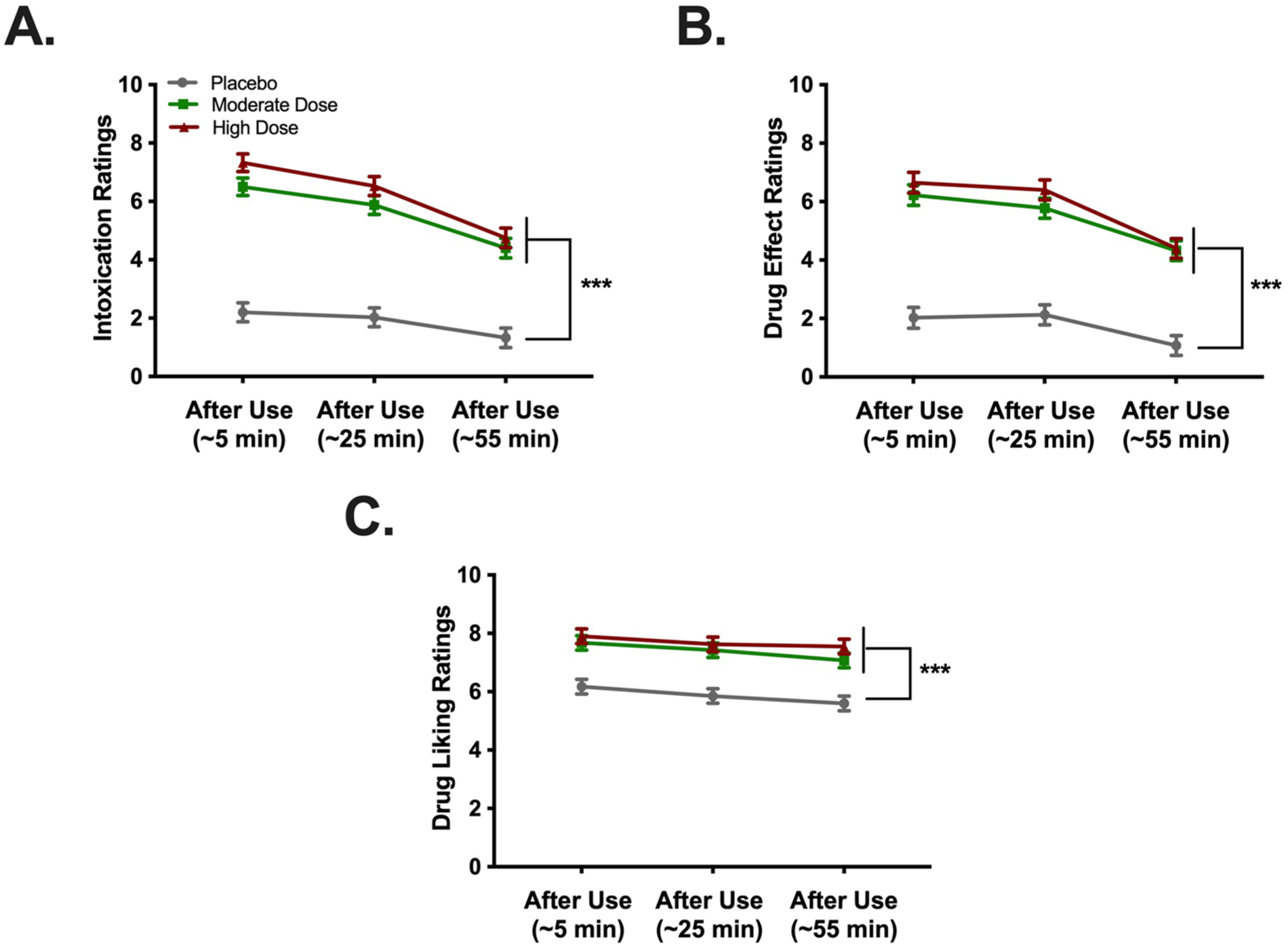
Intoxication, drug effect, and drug liking ratings for participants assigned to vaporize placebo (n = 40), a moderate dose (n = 40), or a high dose (n = 40) of cannabis. Participants in the moderate (green) and high dose (red) conditions gave significantly higher intoxication ratings (a), drug effect ratings (b), and drug liking ratings (c) at each time point compared to participants assigned to vaporize placebo (grey). No differences in any ratings were observed between moderate and high dose conditions at any time point. Error bars represent mean ± SEM.
Figure 2(b) depicts a medium-sized significant drug condition × time interaction on drug effect ratings, F(3.75, 219.52) = 3.72, p = 0.006,
Figure 2(c) shows a large-sized significant main effect of condition on drug liking ratings, F(2, 117) = 20.89, p < 0.001,
Acute effects of cannabis on memory
As shown in Table 2, there were significant main effects of drug condition on five of the six verbal memory test outcomes, two of the four visuospatial memory test outcomes, one of the two prospective memory tests, both measures of source memory, four of the five measures of false memory, and the temporal order memory test. The only domain that failed to reveal a significant effect of cannabis exposure was episodic content memory. Furthermore, both tests of short-term memory and the verbal working memory test failed to reveal a significant effect. In total, 15 of the 21 (71%) outcomes revealed significant effects of acute cannabis use.
Acute effects of cannabis on memory.
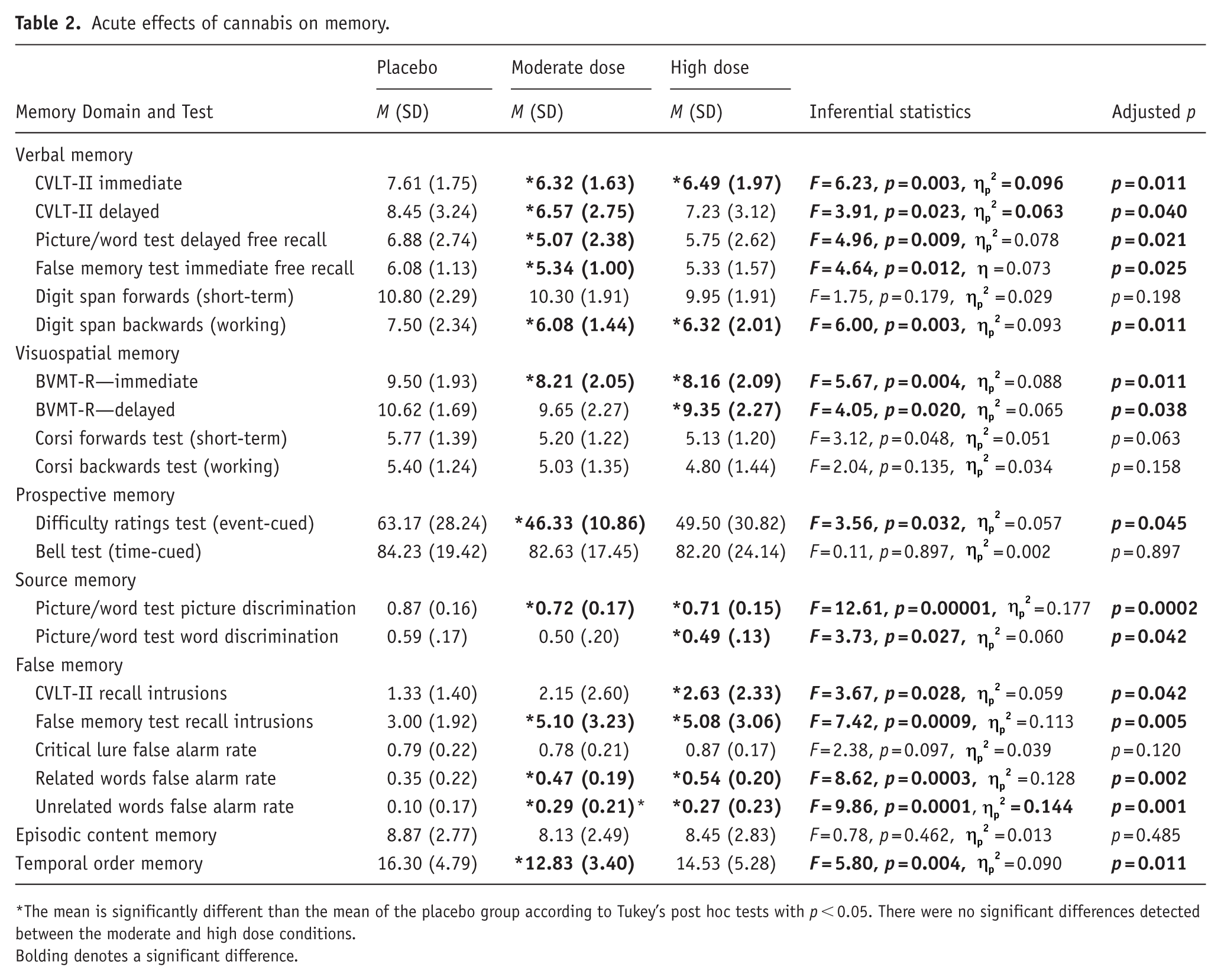
The mean is significantly different than the mean of the placebo group according to Tukey’s post hoc tests with p < 0.05. There were no significant differences detected between the moderate and high dose conditions.
Bolding denotes a significant difference.
Follow-up Tukey’s post hoc tests revealed that participants in the moderate and high dose conditions performed significantly worse than those in the placebo condition on the CVLT-II immediate recall trials (immediate verbal memory), the digit span backwards test (verbal working memory), and the BVMT-R immediate recall trials (immediate visuospatial memory), Furthermore, both cannabis groups demonstrated worse source memory discrimination for pictures, more intrusions on the recall trial of the false memory test, as well as more false memories for related words and unrelated words on the recognition portion of the false memory test.
Furthermore, participants in the moderate dose condition performed significantly worse than participants in the placebo condition on the delayed recall trial of the CVLT-II (delayed verbal memory), picture/word test free recall (delayed verbal memory), the recall trials of the false memory test (immediate verbal memory), the difficulties ratings test of prospective memory (event-cued prospective memory), and the temporal order memory test.
Finally, participants in the high dose condition performed significantly worse than those in the placebo condition on the delayed recall trial of the BVMT-R (delayed visuospatial memory) and they had worse source memory discrimination for words. There were no significant differences in the performance of participants assigned to the moderate and high dose conditions on any of the memory outcomes.
Sensitivity analyses
The results of these same analyses after excluding the 10 participants in the high dose condition and 3 participants in the moderate dose condition who refused to inhale the full dose are shown in Supplemental Table 2. The results were largely consistent with those reported above, with a few minor exceptions. First, the main effect on the event-cued prospective memory test fell just shy of statistical significance prior to correction (p = 0.053); however, the post hoc analyses continued to indicate that the moderate dose group performed significantly worse than the placebo group. Second, the main effect on the visuospatial working memory test increased and was statistically significant, with the high dose group demonstrating significantly worse performance than the placebo group. In contrast, the difference between the high dose and placebo group on verbal working memory was no longer statistically significant (although the overall main effect and the effect in the moderate dose group remained statistically significant). Finally, significant differences between the placebo group and moderate dose group on the delayed recall trial of the BVMT-R and source memory discrimination for words emerged, with this group performing significantly worse than the placebo group on both outcomes. In total, 14 of the 21 (66.7%) main effects revealed a significant effect of acute cannabis use.
Correlations between intoxication ratings at T1, number of inhalations, and performance on the memory test outcomes in the cannabis exposed groups (n = 80) are provided in Supplemental Table 3. They largely corroborate the absence of dose effects with a small number of exceptions: there was a moderate sized significant correlation between intoxication ratings and worse performance on the digit span forwards test (verbal short-term memory) and small but significant correlations between intoxication ratings and more intrusions on the free recall trial of the CVLT-II and false memory test. Total number of puffs only demonstrated a small but significant correlation with more intrusions on the CVLT-II.
Discussion
The overwhelming majority of prior investigations examining the acute effects of cannabis on memory have narrowly focused on verbal memory and working memory. The present study was conducted to broadly examine the impacts of cannabis on multiple memory domains, especially more ecologically valid domains of memory, in order to determine whether cannabis has global detrimental effects on memory or whether the effects of cannabis use are specific to a limited number of memory domains. Results of the present study revealed evidence of broad impacts with moderate-to-large-sized effects across most domains, suggesting the detrimental effects of acute cannabis intoxication on memory are more global in nature and impact a fairly wide variety of memory tasks.
More precisely, we detected detrimental acute effects of cannabis on multiple measures of verbal memory, visuospatial memory, source memory, and false memory, as well as on measures of temporal order memory and prospective memory. Findings from the present study are consistent with well-established effects of cannabis on verbal memory, as well as with less reliably detected effects on visuospatial memory (Broyd et al., 2016; Crane et al., 2013; Dellazizzo et al., 2022). Furthermore, findings from the present study help corroborate prior findings that acute cannabis intoxication increases susceptibility to false memories (Cuttler et al., 2021; Kloft et al., 2020) and interferes with source memory (Cuttler et al., 2021), using a randomized, double-blind, placebo-controlled design. To our knowledge, this is the first study to detect significant effects of acute cannabis intoxication on either temporal order memory or prospective memory, as the only other prior investigation to include these outcomes was somewhat underpowered (Cuttler et al., 2021). The largest effects detected were regarding the false memory outcomes and source memory for pictures, suggesting that these domains of memory are most heavily impacted by acute cannabis intoxication. This is important as the spread of misinformation is becoming increasingly prominent in today’s society, especially on social media. Not only could false memories further contribute to the spread of misinformation but disruptions to source memory would undermine the ability to recall whether the information was obtained from a credible or questionable source.
The significant effect of acute cannabis intoxication on prospective memory was limited to the event-cued test. However, there was an evident ceiling effect on the time-cued prospective memory test that decreased sensitivity to detect a significant effect (see Supplemental Figure 2). Furthermore, although acute cannabis intoxication is known to alter time perception (Atakan et al., 2012), participants had continuous access to a clock they could check, which may have contributed to the ceiling effect and would mitigate the influence of time perception on task performance. Future research should employ a more difficult time-cued task and measure clock-checking behavior, in addition to overall task performance, to understand whether intoxicated participants engage in increased clock-checking to support task performance. Similarly, there was a ceiling effect on the false recollection of the six critical lures on the false memory test that reduced sensitivity to detect a significant effect on that specific outcome (see Supplemental Figure 2). We also failed to detect significant effects on the verbal short-term memory, visuospatial short-term, and visuospatial working memory tests despite an absence of ceiling effects on these tests, although low trial counts may have contributed to a lack of sensitivity to detect effects (see Adam et al., 2020). Nevertheless, we did detect effects on the verbal working memory test. These findings are consistent with the conclusions of major review papers and meta-analyses indicating that evidence for the acute effects of cannabis on working memory is largely mixed (Broyd et al., 2016; Dellazizzo et al., 2022); however, this mixed evidence may be due to sensitivity issues such as low sample sizes and low trial counts (Adam et al., 2020). Finally, we failed to detect a significant effect on the episodic content memory test, which assessed memory for personally experienced events. Additional research should attempt to further establish the acute effects of cannabis on the ability to recall personally experienced events using more complex autobiographical memory tasks such as the Autobiographical Interview (Levine et al., 2002) that requires participants to recall specific life events experienced outside of the context of the lab environment.
From a pharmacological perspective, THC, the primary psychoactive component of cannabis, exerts its effects primarily through activation of type-1 cannabinoid receptors (CB1Rs), which are widely expressed in brain regions critical for memory. In the human hippocampus, CB1Rs are present across all major subfields, including the dentate gyrus, CA1, CA3, and subiculum, with dense localization in axon terminals of both excitatory and inhibitory neurons (Glass et al., 1997; Mato et al., 2003). This broad distribution positions the endocannabinoid system to regulate synaptic transmission and network dynamics essential for memory encoding and retrieval (Figueiredo & Cheer, 2023). Recent work has further identified a population of CB1Rs on mitochondria in hippocampal neurons, where activation by THC reduces mitochondrial respiration and impairs memory formation (Hebert-Chatelain et al., 2016). Collectively, these findings suggest that acute cannabis intoxication results in rather global memory distruptions primarily through hippocampal CB1R activation.
We did not find evidence of dose-dependent effects in the current study, as there were no significant differences in the performance of participants in the moderate and high dose conditions on any of the memory outcomes. Although we anticipated that participants in the high dose condition would experience stronger intoxication, heightened drug effects, and worse memory test performance, ultimately, both groups felt a similar (high level of) drug effects and demonstrated comparable performance. Thus, the absence of dose-dependent effects likely reflects the lack of difference in the high level of intoxication and drug effect ratings of these two groups. Participants were encouraged to inhale the full dose, but for ethical reasons and to mitigate potential adverse events, they were permitted to discontinue the cannabis use session if the effects became too strong or uncomfortable for them. A total of 10 participants in the high dose condition, 3 participants in the moderate dose condition, and 1 participant in the placebo condition refused to inhale the full dose. Nevertheless, most of the participants who discontinued the vaping session reported above-average intoxication ratings, suggesting they were impacted by the lower dose to the same degree as participants who inhaled the full dose. Indeed, excluding the 13 participants who did not inhale the full dose of cannabis produced only minor differences in the findings, and even after these exclusions there were still no significant differences between the performance of the moderate and high dose conditions, suggesting the refusal of some participants to inhale the full dose not account for the absence of dose-dependent effects. We also attempted to correlate intoxication ratings and number of inhalations with performance on each of the memory tests, and the results largely corroborate the absence of dose-dependent effects with a few small exceptions. In future studies, it will be important to test lower dose ranges to determine whether a threshold of intoxication exists for the memory-impairing effects of cannabis. Future studies should also consider using the same amount of product across all conditions by mixing active and placebo cannabis.
We did not manipulate the administration of cannabis across encoding versus retrieval phases of memory, and therefore, it is unclear whether the acute effects of cannabis predominantly affected encoding, consolidation, retrieval, or all three phases of memory. Prior evidence on the potential differential acute effects of cannabis on these stages of memory is somewhat mixed and may depend on the domain of memory tested. Specifically, while Ranganathan and D’Souza’s (2006) past review of the literature indicates that THC impairs encoding rather than retrieval, it predominantly focused on verbal memory, visuospatial memory, and working memory and did not consider more ecologically valid domains of memory, such as false memory, source memory, or prospective memory. In contrast, a review of the effects of cannabis (and other drugs) on false memory specifically indicates that acute cannabis use “can increase false memory proneness and suggestibility, which seems to be driven largely by THC at retrieval elevating response bias” (Kloft et al., 2021: 301). Therefore, future research should systematically examine whether acute cannabis use primarily perturbs encoding or retrieval phases of prospective memory, source memory, and temporal order memory to help fill these gaps in the literature.
Additional limitations of the present study include the use of experienced cannabis users who may be less sensitive to the effects of cannabis on memory (D’Souza et al., 2008), ceiling effects that reduced sensitivity to detect effects on a couple of outcomes, and the decision of some participants to discontinue the cannabis use session before inhaling the full dose. Nevertheless, all three factors would decrease sensitivity to detect acute effects of cannabis on memory, and we revealed broad effects on approximately 70% of the memory test outcomes. It is also important to note that most of the participants were young adults with a mean age of approximately 28. It is possible that these findings may not generalize to an older adult sample. Thus, future research should target this important demographic. The use of a between-subjects design with no baseline assessments of memory is a minor limitation. However, randomization produced groups that were equivalent at baseline in all important respects (including cannabis use history, demographics, and premorbid verbal IQ). Moreover, we opted to use a between-subjects design because it helps with blinding by eliminating potential contrast effects and because several of the memory tests (e.g., prospective, episodic content memory, temporal order) would be impacted by repeated exposure and practice effects. Furthermore, for tasks with more complicated instructions (e.g., prospective memory tasks), participants were asked to repeat the instructions in their own words to ensure they were paying attention and understood the task requirements; however, it is difficult to determine the extent to which issues with attending to the task instructions influenced some of the acute effects of cannabis on memory. Finally, the mean number of inhalations in the high dose condition was also not double the mean number of inhalations in the moderate dose condition; however, force of inhalation may have differed and could not be measured in the present study. These limitations are offset by several strengths of the study, such as the use of a rigorous randomized, double-blind, placebo-controlled design, the large sample that affords ample power to detect moderately large-sized effects, the use of the Benjamini–Hochberg procedure to reduce false discovery rate, and the use of multiple measures of several different memory domains, especially several understudied ecologically valid memory domains.
In conclusion, acute cannabis intoxication produces moderate to large-sized impairments across a range of memory domains, including ecologically valid measures that are closely tied to real-world functioning. These findings are especially consequential given the sharp rise in daily cannabis use amid ongoing legalization across North America. As cannabis becomes increasingly accessible, understanding its immediate cognitive consequences is essential for informing public health policy, shaping responsible use guidelines, and mitigating potential harms to individuals and society.
Supplemental Material
sj-docx-1-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-docx-1-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Supplemental Material
sj-docx-2-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-docx-2-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Supplemental Material
sj-docx-3-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-docx-3-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Supplemental Material
sj-docx-4-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-docx-4-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Supplemental Material
sj-jpg-5-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-jpg-5-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Supplemental Material
sj-jpg-6-jop-10.1177_02698811261416079 – Supplemental material for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study
Supplemental material, sj-jpg-6-jop-10.1177_02698811261416079 for Mapping the acute effects of cannabis on multiple memory domains: A randomized, double-blind, placebo-controlled study by Carrie Cuttler and Ryan J. McLaughlin in Journal of Psychopharmacology
Footnotes
Acknowledgements
We would like to thank Sia Chheda, Connor Chong, Jason Cross, Sania Farooq, Alexus Harris, Taylor Hollis, Pranavi Peddibhotla, Jack Proctor, and Chloe Stein for monitoring participants while they sobered up, collecting intoxication ratings, and debriefing participants.
Ethical considerations
This study was approved by the Washington State University Institutional Review Board (#19425) on April 21, 2022. All participants provided written informed consent.
Author contributions
CC conceived the idea, wrote the grant to fund the study, designed the study, recruited participants, tested participants, analyzed the data, and prepared the manuscript. RJM helped to conceive of the idea, write the grant, and design the study, randomized participants, served as the drug master, and helped to prepare and edit the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant to CC and RJM from Washington State University’s Dedicated Marijuana Account (DMAc). Funds for this account come from the sales of legal cannabis in the state of Washington (WA Initiative 502). The funder had no role in the design, conduct, analysis, or reporting of the data.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CC and RJM received study-related materials from Storz & Bickel. Outside of this work, CC has received research funds from Huxley Health, Healer, CReDO Science, and Terra Matar Botanicals.
Data availability statement
Deidentified data are available upon reasonable request to carrie.cuttler@wsu.edu.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.