
Abstract
Ketamine has emerged as a promising rapid-acting treatment for mood disorders and suicidality. Notwithstanding its replicated antidepressant efficacy, ketamine-associated risk for abuse, dependence, and misuse remain. We conducted a systematic review of clinical and preclinical studies from database inception to August 2025, including randomized and observational trials, open-label extensions, case reports, and preclinical animal research, assessing ketamine or its enantiomers for outcomes related to abuse potential including craving, drug liking, tolerance, withdrawal, or dependence. A total of 30 studies (25 clinical and 5 preclinical) met the inclusion criteria. Clinical studies consistently reported minimal evidence of craving, dose escalation, misuse, or illicit use when ketamine or esketamine was administered in controlled, clinically supervised settings. Preclinical findings demonstrated that (S)-ketamine produces reward-related behaviors and locomotor sensitization, racemic ketamine shows reinforcing effects at higher doses, whereas (R)-ketamine demonstrates minimal reinforcing effects. Overall, the body of reviewed literature suggests that ketamine and esketamine carry low abuse liability when delivered in a monitored clinical setting while risk of abuse and misuse was identified largely in case reports and series in which appropriate monitoring was often not conducted. These findings support the safe incorporation of ketamine into treatment protocols for mood disorders while emphasizing the importance of structured administration and ongoing patient monitoring both throughout treatment and follow-up. Further research using longitudinal, prospective designs is warranted to assess potential misuse over extended treatment periods and across diverse patient populations, to optimize clinical safety and further inform evidence-based clinical practice guidelines.
Keywords
Introduction
Mood disorders are complex conditions associated with substantial personal, social, and economic burdens, including impaired functioning, decreased quality of life, and increased risk of suicide (Maj et al., 2020; McIntyre et al., 2020). The heterogeneity in symptoms and variable treatment response further complicates the management of mood disorders. Notwithstanding the current availability of treatment options (e.g., conventional monoamine-based antidepressants), therapeutic outcomes often remain suboptimal for many individuals. For instance, approximately 30% of individuals with major depressive disorder (MDD) do not achieve remission after treatment with two or more first-line monoaminergic antidepressants (McIntyre et al., 2023). Similar challenges exist in the treatment of bipolar depression, wherein treatment-resistant presentations continue to respond poorly to clinical interventions (Diaz et al., 2022). These limitations have increased interest in novel, rapidly acting treatments for patients who do not respond to conventional interventions.
Ketamine, a non-competitive N-methyl-
Notwithstanding ketamine’s therapeutic potential, its pharmacological properties raise concerns regarding abuse liability. Recreational use has been associated with compulsive intake, craving, dose escalation, and withdrawal-like symptoms (Kwan et al., 2024b; Le et al., 2022; Liu et al., 2016). Additionally, population surveillance data have also reported increasing rates of non-medical ketamine use in recent years (Palamar et al., 2025). Although these trends cannot be directly attributed to the clinical use or approval of esketamine, they highlight a broader population-level context for the abuse liability of ketamine. With the expanding clinical application of ketamine and the increasing use of repeated administration protocols, systematic evaluation of its potential for abuse, misuse, tolerance, and dependence is warranted. A thorough understanding of these risks is essential for the safe integration of ketamine into clinical practice for mood disorders.
The abuse liability of ketamine was previously reviewed by our group (Le et al., 2022), however, substantial new evidence has emerged in recent years, meriting an updated synthesis. This review incorporates additional datasets and a particular focus on mood disorders with the inclusion of esketamine. We will evaluate findings from clinical trials, observational studies, case reports, and preclinical research, with emphasis on indicators of misuse, craving, tolerance, and dependence in individuals with a mood disorder. Furthermore, it aims to provide a framework for understanding ketamine-related risks in clinical practice, guide evidence-based prescribing and monitoring strategies, and identify priorities for future research.
Methods
Search string and strategy
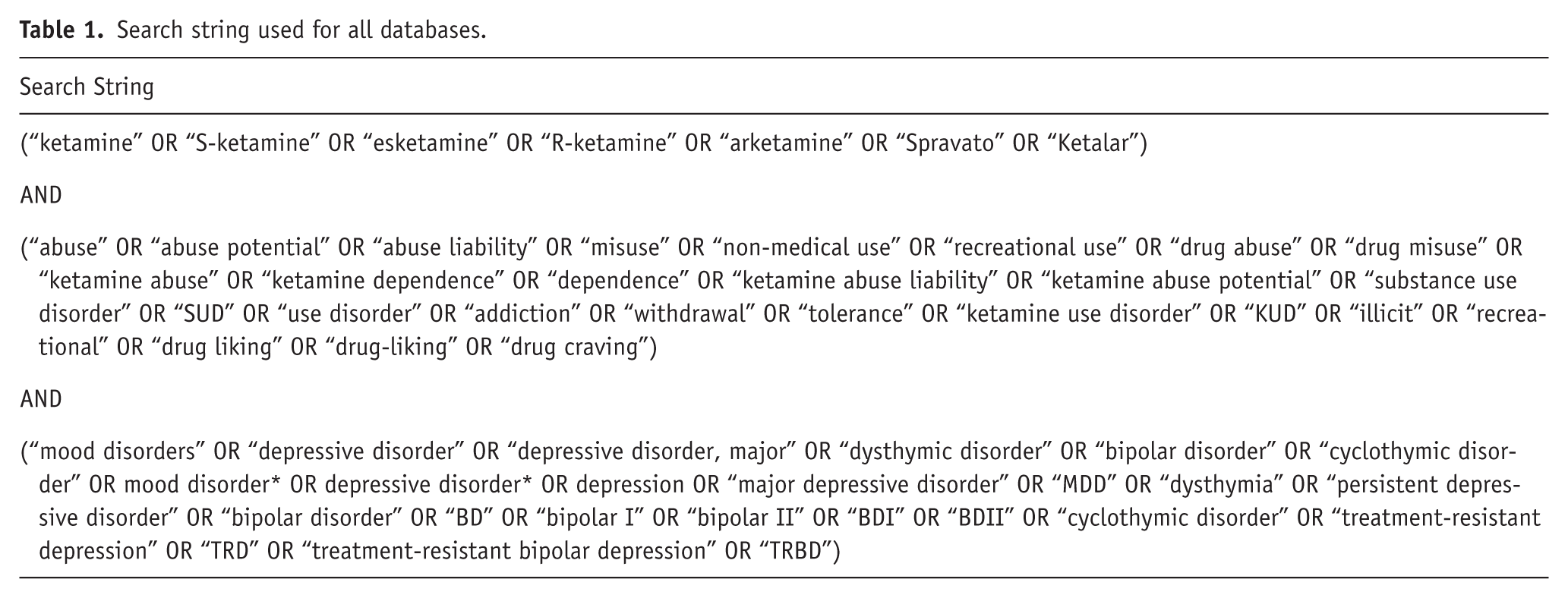
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (Page et al., 2021) and registered with the international prospective register of systematic reviews (PROSPERO ID: CRD420251130843). A comprehensive literature search was carried out in PubMed and OVID databases, including MEDLINE, Embase, and PsycINFO, from inception through August 2025. The full search string is provided in Table 1 and was applied consistently across all databases to ensure uniformity. No additional filters or limits were applied during the database search. To capture additional relevant studies, supplementary searches were performed using Google Scholar and by reviewing the reference lists of included articles. Specifically, the first 10 pages of Google Scholar results were screened by title and abstract, duplicates were removed, and potentially eligible full texts were assessed using the same inclusion and exclusion criteria as applied to the primary database searches.
Search string used for all databases.
Eligibility criteria
All retrieved studies were screened against the following eligibility criteria: (1) Participants were required to have a primary diagnosis of a mood disorder, established through clinical assessment or standardized diagnostic criteria (e.g., Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR)), including MDD and TRD, persistent depressive disorder (dysthymia), bipolar disorders (i.e., TRBD, Bipolar Disorder I, Bipolar Disorder II), cyclothymic disorder, or other specified or unspecified depressive disorders. Preclinical studies using animal models in which a mood disorder was replicated (e.g., chronic social defeat stress, chronic mild stress) to assess ketamine self-administration, reinforcement, reinstatement, or other abuse liability endpoints were also eligible, (2) Studies had to investigate ketamine or related formulations (i.e., racemic ketamine, esketamine ((S)-ketamine), arketamine ((R)-ketamine), Spravato, or Ketalar), (3) Studies were required to report at least one outcome related to ketamine’s abuse liability or misuse potential, including drug craving, drug liking, behavioral measures of abuse potential, dependence, tolerance, withdrawal, or adverse event reporting; secondary outcomes included substance use disorder (SUD) or non-medical/illicit ketamine use following treatment, (4) Eligible study designs included randomized controlled trials (RCTs), open-label trials, cross-over trials, cohort studies (prospective or retrospective), case-control studies, case reports/series, and preclinical animal studies.
Studies were excluded if (1) the population did not include individuals with a mood disorder or mixed populations without separate data for mood disorders, (2) interventions did not involve ketamine or its related formulations, (3) outcomes did not assess abuse, misuse, or dependence, or (4) the study was not primary research, including reviews, editorials, abstracts without full text, study protocols, or unpublished manuscripts.
Study selection
Retrieved studies were screened independently by two reviewers (S.V. and G.F.M.L.) using the Covidence platform (Covidence, n.d.). Initial screening was conducted based on titles and abstracts. Studies deemed potentially relevant by at least one reviewer were then assessed in full text against the eligibility criteria outlined in section “Eligibility criteria.” Inclusion required agreement between both reviewers, with any discrepancies resolved through discussion. Records were excluded at the full-text stage if they did not meet the predefined eligibility criteria (e.g., population, intervention, outcomes, or study design).
Data extraction
Data extraction was independently performed by two reviewers (S.V. and G.F.M.L.) using a piloted template, with discrepancies resolved through discussion. For clinical studies, predefined elements included: study authors and year of publication, study design, sample population (i.e., diagnosis, age, and sex for case reports), sample size, intervention/exposure, outcomes related to abuse liability or misuse, assessment tools/measures, and primary and secondary results. For preclinical (animal) studies, predefined elements included: study authors and year of publication, study design, animal model, sample size, intervention/exposure, outcomes related to abuse liability or misuse, assessment tools/measures, and primary and secondary results. When outcome data were missing or incomplete, supplementary materials and trial registries were consulted, and unresolved gaps were documented. Diagnostic criteria for psychiatric disorders were also recorded when applicable. Extracted information from clinical and preclinical studies is presented in Tables 2 and 3, respectively. Given the heterogeneity in study designs, populations, and outcome measures across the included clinical and preclinical studies, results were synthesized using a qualitative systematic review approach, and no quantitative pooling or meta-analysis was conducted.
Clinical data extraction for studies on ketamine abuse liability in mood disorders.
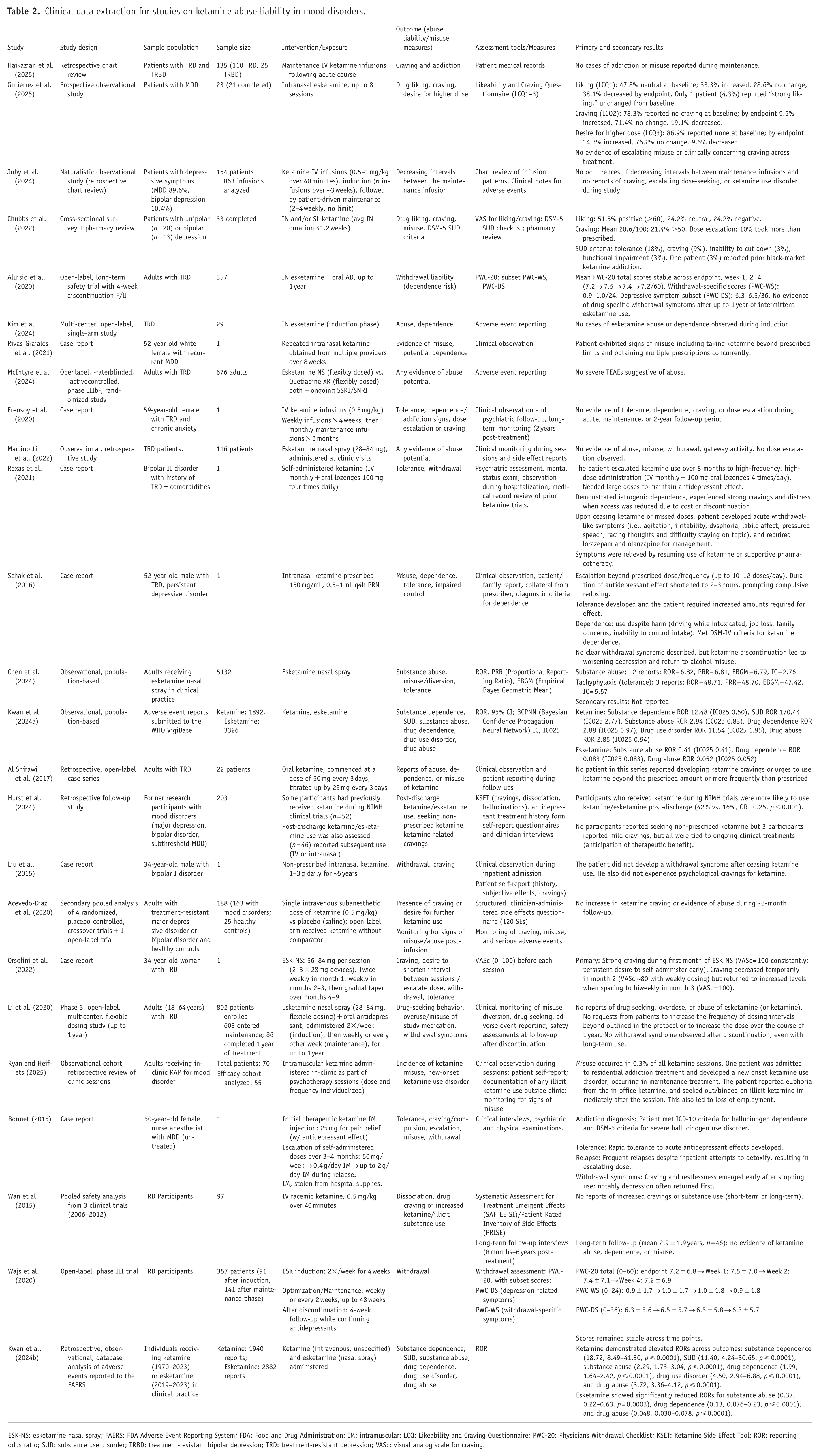
ESK-NS: esketamine nasal spray; FAERS: FDA Adverse Event Reporting System; FDA: Food and Drug Administration; IM: intramuscular; LCQ: Likeability and Craving Questionnaire; PWC-20: Physicians Withdrawal Checklist; KSET: Ketamine Side Effect Tool; ROR: reporting odds ratio; SUD: substance use disorder; TRBD: treatment-resistant bipolar depression; TRD: treatment-resistant depression; VASc: visual analog scale for craving.
Preclinical data extraction for studies on ketamine abuse liability in mood disorders.
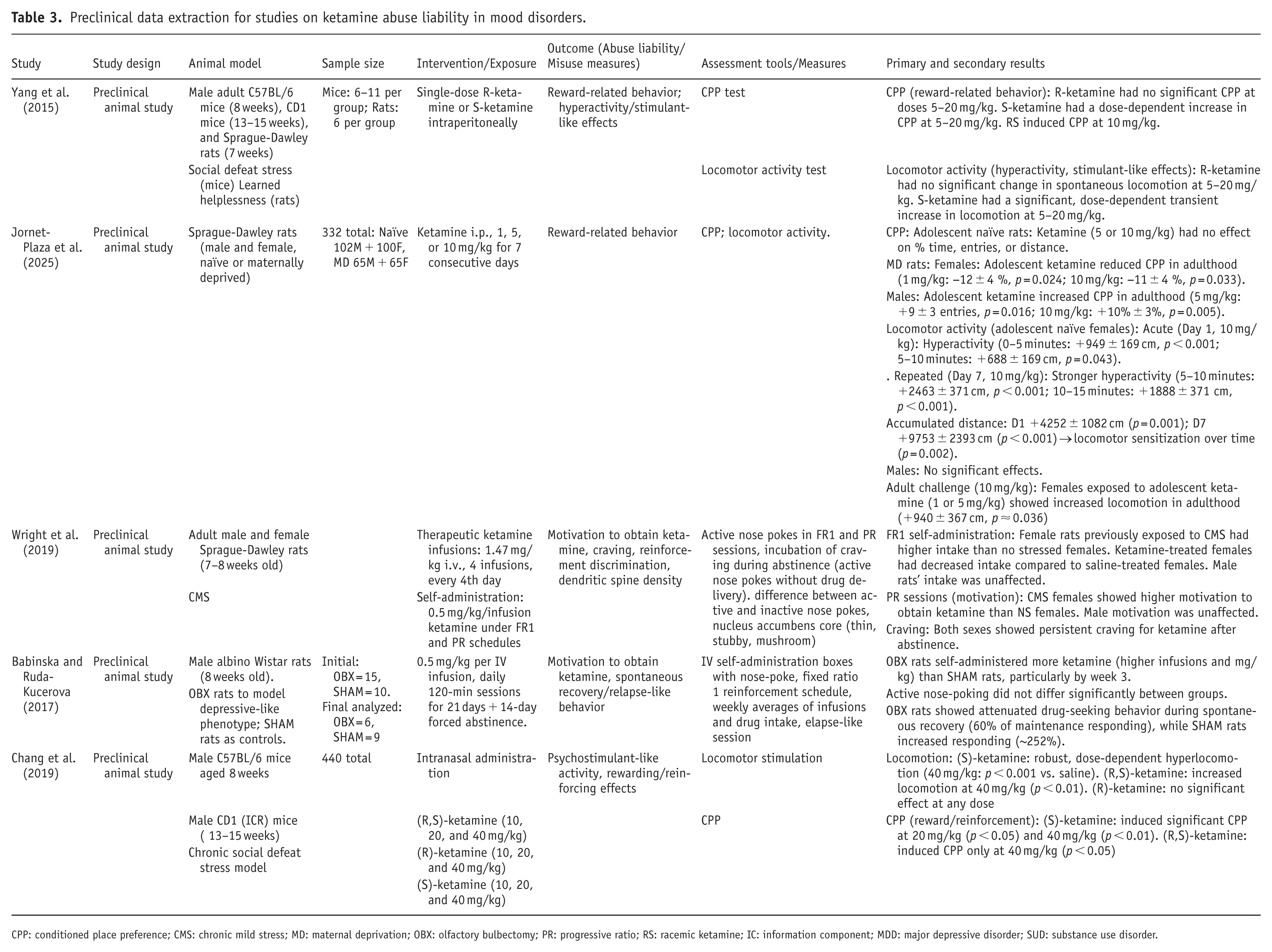
CPP: conditioned place preference; CMS: chronic mild stress; MD: maternal deprivation; OBX: olfactory bulbectomy; PR: progressive ratio; RS: racemic ketamine; IC: information component; MDD: major depressive disorder; SUD: substance use disorder.
Risk of bias assessment
Two independent reviewers (S.V. and G.F.M.L.) assessed the potential risk of bias across included studies. Preclinical animal studies were evaluated using the SYRCLE Risk of Bias tool for Animal Studies (Hooijmans et al., 2014). RCTs were assessed using the Cochrane Risk of Bias Tool for Randomized Studies (RoB 2; Higgins et al., 2011). Non-randomized clinical studies were assessed using the Risk of Bias in Non-randomized Studies – of Interventions (ROBINS-I V2) tool (Sterne et al., 2019). Case reports and case series were assessed using the tool for evaluating the methodological quality of case reports and case series proposed by Murad et al. (2018). Discrepancies between reviewers were resolved through discussion and consensus.
Results
Study selection and characteristics
Five thousand three hundred ninety-three studies were identified through the systematic search. Following the removal of duplicates (n = 2104), 3289 studies underwent title and abstract screening by two independent reviewers, of which 3233 were excluded for not meeting the eligibility criteria (e.g., not involving ketamine or related formulations, not including mood disorder populations, not assessing abuse-related outcomes, or not representing primary research). The remaining 56 studies underwent full-text screening, and 30 studies (25 clinical studies and 5 preclinical studies) met eligibility criteria and were included in the qualitative synthesis (see PRISMA flow diagram in Figure 1).
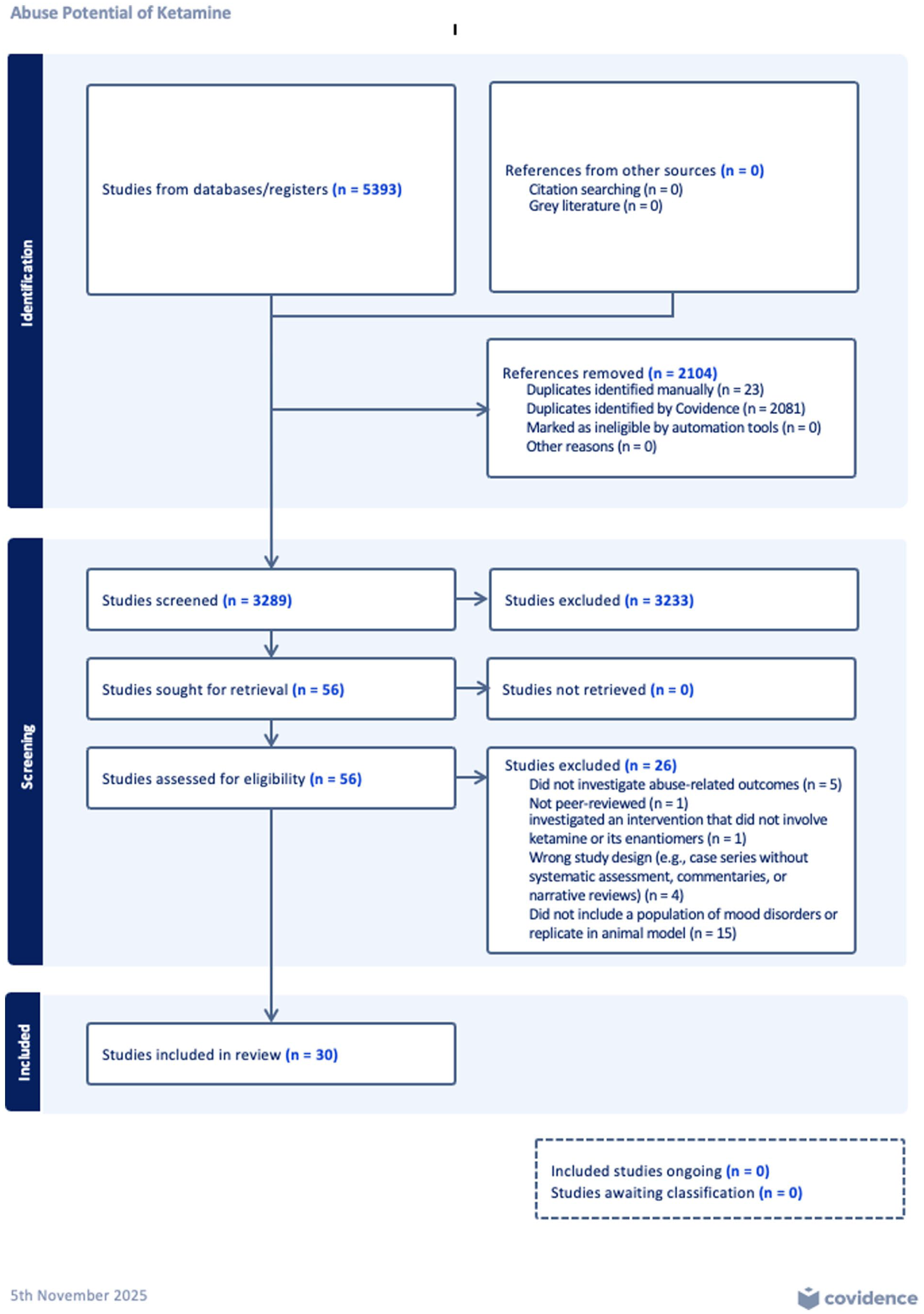
PRISMA flow diagram for study selection process of systematic review of preclinical and clinical studies evaluating the abuse liability of ketamine in the treatment of mood disorders (Covidence, n.d.).
Following full-text review, 26 studies were excluded for the following reasons: 15 studies did not use animal models of mood disorders or did not include a population with mood disorders, 5 studies did not investigate an abuse-related outcome, 4 studies employed an ineligible study design (e.g., case series without systematic assessment, commentaries, or narrative reviews), 1 study was excluded because it was not peer-reviewed (i.e., preprint without formal review), and 1 study investigated an intervention that did not involve ketamine or its enantiomers.
The clinical literature included retrospective chart reviews, prospective observational cohorts, open-label extensions of randomized trials, pharmacovigilance database analyses, and case reports or case series. Collectively, these studies included approximately 3000 patients who received intravenous (IV) racemic ketamine, intranasal (IN) esketamine, or related formulations for mood disorders. Sample sizes varied from single-patient case reports to large population-based analyses, with treatment regimens ranging from acute induction courses to long-term maintenance therapy.
Outcomes assessed included craving, liking, dose escalation, misuse, SUD criteria, and withdrawal potential, measured using clinical observation, patient self-report questionnaires, structured assessment tools (e.g., Likeability and Craving Questionnaire (LCQ), Physicians Withdrawal Checklist (PWC-20), Ketamine Side Effect Tool (KSET)), and adverse event databases (e.g., WHO VigiBase, FDA Adverse Event Reporting System (FAERS)). The preclinical literature consisted of rodent studies investigating ketamine’s abuse liability using conditioned place preference (CPP), self-administration paradigms, locomotor activity, and relapse- or craving-like behavior. Studies examined (R)-ketamine, (S)-ketamine, and racemic formulations across varying doses and models of depression such as chronic social defeat.
Results from risk of bias assessments
The risk of bias across the included studies was assessed using established tools appropriate to each study design. Overall, 1 RCT was rated as low risk of bias; among the non-randomized studies, 4 were rated as low risk and 13 as moderate risk; and among case reports and case series, 3 were rated as high risk and 4 as moderate risk. RCTs were evaluated against the Cochrane Risk of Bias 2 (RoB2) tool (Supplemental Table 1). McIntyre et al. (2024) was rated as low risk across the five domains, demonstrating proper randomization, blinding, data reporting and outcome assessment.
Four studies (Acevedo-Diaz et al., 2020; Gutierrez et al., 2025; Juby et al., 2024; Wan et al. 2015) were assessed utilizing the ROBINS-I-V2 tool (Supplemental Table 2) and were rated to contain a low risk of bias. These studies generally included appropriate handling of confounding variables, well-defined intervention groups, and thorough outcome measurement and reporting. In contrast, most studies (Al Shirawi et al., 2017; Aluisio et al., 2020; Chen et al., 2024; Chubbs et al., 2022; Haikazian et al., 2025; Hurst et al., 2024; Kim et al., 2024; Kwan et al., 2024a, 2024b; Li et al., 2020; Martinotti et al., 2022; Ryan and Heifets, 2025; Wajs et al., 2020) were rated at a moderate risk of bias. Common limitations of these studies included inadequate handling of confounding variables, lack of blinding, and incomplete outcome data, potentially impacting the validity of their results.
The five preclinical animal studies (Babinska and Ruda-Kucerova, 2017; Chang et al., 2019; Jornet-Plaza et al., 2025; Wright et al., 2019; Yang et al., 2015) were assessed using the SYRCLE Risk of Bias tool (Supplemental Table 3). Across all studies, some concerns were noted. These generally consisted of inadequate sequence generation, allocation concealment, and random housing, and blinding was mostly absent or unclear. Finally, risk of bias in case reports and series were assessed using the Murad et al. (2018) tool (Supplemental Table 4). Most case reports (Rivas-Grajales et al., 2021; Roxas et al., 2021; Schak et al., 2016) were judged to have high risk of bias due to unclear or incomplete selection criteria, limited ascertainment of exposure and outcomes, and lack of consideration for alternative explanations of findings. Moderate risk was noted in the other reports (Bonnet, 2015; Erensoy et al., 2020; Liu et al., 2015; Orsolini et al., 2022), where better ascertainment and more detailed reporting mitigated some bias but concerns persisted in regard to causality assessment and selection processes. Overall, most studies exhibited moderate risk of bias, commonly related to a lack of blinding and incomplete outcome data, which may limit the strength of conclusions drawn from the available evidence.
Results of clinical studies
Retrospective and prospective observational studies
Across the included clinical studies, 13 studies evaluated ketamine or esketamine administered under closely supervised medical conditions. Retrospective chart reviews consistently described low or absent rates of apparent misuse or dependence. For example, Haikazian et al. (2025) reviewed the medical records of 135 patients (110 TRD and 25 TRBD) undergoing maintenance IV ketamine infusions following an acute treatment course. No evidence of craving, compulsive use, or addiction-related behaviors was identified during the monitored maintenance period. Similar findings were reported in earlier chart reviews, including Juby et al. (2024), which examined 863 infusions across 154 patients, and Al Shirawi et al. (2017), which described long-term IV ketamine administration without evidence of dose escalation, shortened intervals between infusions, or clinically significant craving.
A retrospective observational study by Martinotti et al. (2022) assessed 116 patients receiving intranasal esketamine (28–84 mg) in routine clinical practice. No evidence of clinically apparent misuse, withdrawal symptoms, dose escalation, or other indicators of abuse liability were reported within the limits of clinical monitoring and adverse event documentation. Similarly, Wan et al. (2015) evaluated the pooled safety analysis from 97 patients receiving IV ketamine for TRD across three clinical trials from 2006 to 2012 and observed no compulsive use, dose escalation, or clinically significant craving occurred over the course of treatment.
A prospective observational study by Gutierrez et al. (2025) followed 23 patients who received up to eight sessions of IN esketamine, assessing measures of “liking,” “craving,” and “desire for a higher dose” at baseline and at the treatment endpoint. The baseline LCQ assessment was conducted up to 24 hours after the first session, and the follow-up assessment was completed within 24 hours after the eighth session. Only one patient (4.3%) reported “strong liking,” which remained unchanged from baseline. Regarding craving, 78.3% reported none at baseline, and by endpoint, 9.5% experienced increased craving and 19.1% decreased. Similarly, 86.9% reported no desire for a higher dose at baseline, with 14.3% increasing and 9.5% decreasing by endpoint. Overall, these measures remained stable or decreased throughout treatment, and there was no reported indication of loss of control or clinically significant misuse (Gutierrez et al., 2025). Additional detailed values are provided in Table 1.
Chubbs et al. (2022) surveyed 33 patients with unipolar (n = 20) or bipolar (n = 13) depression receiving IN or sublingual (SL) ketamine. Positive drug liking was reported by 17 participants, neutral by 8, and negative by 8. Cravings were generally low (mean 20.6/100), with 6 participants reporting scores above 50. Dose escalation occurred in 10 participants across IN and SL formulations. DSM-5SUD criteria was rarely met including 6 participants that reported tolerance, 3 reported cravings, 1 reported inability to cut down use, and 1 reported functional impairment. In addition, 1 participant had a previous history of black-market ketamine use (Chubbs et al., 2022).
Hurst et al. (2024) observed that individuals exposed to ketamine in earlier clinical trials were more likely to pursue subsequent ketamine treatment; however, none sought illicit ketamine, and the three participants that reported cravings experienced them only during participation in supervised protocols in anticipation of clinical benefit. Finally, Ryan and Heifets (2025) examined 55 adults receiving in-clinic intramuscular ketamine as part of psychotherapy sessions. Misuse occurred in 0.3% of all sessions. One patient developed a new-onset ketamine use disorder during maintenance, reporting euphoria from in-clinic ketamine and subsequent illicit use, which contributed to loss of employment (Ryan and Heifets, 2025).
Open-label studies
Long-term open-label and extension studies of IN esketamine provided additional data. Pooled analyses from multicenter trials (Aluisio et al., 2020; Wajs et al., 2020) demonstrated no systematic increase in dosing frequency, no increase in dose beyond approved limits, and no rise in Physician Withdrawal Checklist (PWC-20) scores over months of maintenance ketamine treatment. Similarly, Li et al. (2020) and Kim et al. (2024) reported stable dosing of ketamine, and no observed dependence during ketamine use in open-label extensions up to and longer than 1 year. Even in randomized, active-controlled trials such as that of McIntyre et al. (2024), severe adverse events resembling withdrawal or drug-seeking were not observed.
Pharmacovigilance and post-marketing data
Chen et al. (2024) analyzed post-marketing safety data from over 5000 esketamine-treated patients and identified 12 reports of “substance abuse” and three reports of “tolerance.”
Similarly, two large pharmacovigilance analyses by Kwan et al. (2024a, 2024b) examined spontaneous reporting databases from both global and U.S. reporting systems, with acetaminophen serving as the comparator. In their WHO VigiBase study (Kwan et al., 2024a), which included 1892 ketamine and 3326 esketamine reports, ketamine was associated with increased reporting signals for substance dependence, SUD, and drug abuse. In contrast, esketamine reduced reporting signals for comparable outcomes, suggesting a reduced signal for misuse when compared with ketamine although interpretation should remain cautious given the limitations of spontaneous reporting systems. (Kwan et al., 2024a). The complementary analysis of FAERS data (Kwan et al., 2024b) also showed similar results. Of the 1940 ketamine and 2882 esketamine reports, ketamine exhibited increased reporting signals for misuse-related outcomes. In contrast, esketamine showed lower reporting signals for similar outcomes (Kwan et al., 2024b) Detailed numerical values for these analyses are provided in Table 1.
Case reports and case series
Case reports and case series provided qualitative data about the contexts under which ketamine misuse and dependence can emerge. For instance, Roxas et al. (2021) described a patient who transitioned from clinic-administered IV ketamine to unsupervised high-dose oral lozenges, developing iatrogenic dependence characterized by craving, tolerance, and withdrawal-like symptoms. Schak et al. (2016) reported compulsive intranasal ketamine use up to 10–12 times per day with functional impairment, while Bonnet (2015) detailed a nurse anesthetist escalating from therapeutic intramuscular ketamine to 2 g/day stolen from hospital supply, meeting DSM-5 criteria for severe hallucinogen use disorder. Rivas-Grajales et al. (2021) described a patient taking IN ketamine beyond prescribed limits and obtaining multiple prescriptions concurrently, and Orsolini et al. (2022) reported a patient receiving esketamine nasal spray who exhibited strong craving during early treatment (visual analog scale for craving = 100), which fluctuated with the dosing schedule. In contrast, two case reports (Erensoy et al., 2020; Liu et al., 2015) documented repeated ketamine or esketamine administration without craving or withdrawal phenomena. Across these reports, misuse was most often associated with contexts involving unsupervised dosing or dose escalation outside structured treatment protocols.
Results of preclinical studies
Overall, preclinical findings indicate that ketamine exhibits reinforcing and stimulant-like properties, with effects influenced by enantiomer, sex, developmental stage, and stress-related vulnerability. Detailed numerical values are provided in Table 2.
Reward-Related behavior (conditioned place preference)
CPP was the most frequently used measure of reward-related behavior and served as a key marker of abuse liability in the included preclinical studies. Yang et al. (2015) demonstrated this pattern across C57BL/6 and CD1 mice and Sprague-Dawley rats, showing dose-dependent CPP for S-ketamine (5–20 mg/kg), CPP for racemic ketamine at 10 mg/kg, and no effect for R-ketamine. Chang et al. (2019) replicated these findings in a large cohort of mice (n = 440) using intranasal administration, with S-ketamine producing significant CPP at 20 and 40 mg/kg, racemic ketamine at 40 mg/kg, and R-ketamine showing no effect. Developmental exposure and early-life stress further modulated CPP outcomes. Jornet-Plaza et al. (2025) found that adolescent ketamine exposure produced sex- and stress-dependent long-term effects. In naïve adolescent rats, ketamine did not induce significant CPP. In maternally deprived rats, which is known to induce depression-like phenotypes (Mourlon et al., 2010), tested in adulthood, females exposed to adolescent ketamine showed reduced CPP, whereas males exhibited increased CPP. Overall, CPP findings suggest that (S)-ketamine and racemic ketamine demonstrate dose-dependent reward-related effects, whereas (R)-ketamine shows minimal reinforcing properties across preclinical models.
Locomotor activity (stimulant-like effects)
Locomotor activity, a known proxy for stimulant-like effects, further paralleled CPP findings. Jornet-Plaza et al. (2025) found that adolescent naïve females showed significant hyperactivity following acute ketamine exposure, thereby suggesting locomotor sensitization. Contrastingly, males showed no significant locomotor effects. Importantly, females previously exposed to adolescent ketamine (1 or 5 mg/kg) exhibited increased locomotion in adulthood following a challenge dose. Finally, Chang et al. (2019) similarly reported that S-ketamine produced dose-dependent hyperlocomotion at 40 mg/kg, racemic ketamine increased locomotion at 40 mg/kg, and R-ketamine had no significant effect. Together, these findings suggest stimulant-like and sensitization effects associated with (S)-ketamine and racemic ketamine, with variability observed across sex and developmental exposure.
Self-administration and motivation to obtain ketamine
Preclinical studies including operant self-administration experiments further demonstrated ketamine’s reinforcing properties. Wright et al. (2019) found that adult male and female Sprague-Dawley rats exposed to chronic mild stress self-administered ketamine (0.5 mg/kg/infusion) under fixed-ratio 1 schedules. In addition, females exposed to stress showed increased intake and greater motivation under progressive ratio schedules when compared to non-stressed females. Previous therapeutic ketamine infusions (1.47 mg/kg IV. four infusions) reduced reinforcement during subsequent trials in females, but this effect was not observed in males. Both sexes demonstrated persistent craving after forced cessation of ketamine use (Wright et al., 2019). In addition, Babinska and Ruda-Kucerova (2017) reported that male olfactory bulbectomy (OBX) rats self-administered more ketamine than SHAM controls, particularly by week 3, but showed decreased drug-seeking during spontaneous recovery, responding at about 60% of maintenance levels compared to about 252% in SHAM rats. During operant conditioning, the rats’ active nose-poking (the action used to obtain ketamine) did not differ significantly between the two groups (Babinska and Ruda-Kucerova, 2017). Collectively, self-administration studies indicate that ketamine possesses reinforcing properties in rodent models, particularly under stress-related conditions.
Discussion
This systematic review synthesizes clinical literature examining the abuse potential of ketamine and esketamine in individuals with mood disorders as well as in preclinical models. Overall, the current body of evidence indicates that when used therapeutically (i.e., administered under clinical supervision and at evidence-based recommended doses), ketamine and esketamine appear to be associated with a relatively low risk of abuse, misuse, dependence, or compulsive drug-seeking within the limits of available evidence. Evidence obtained from retrospective chart reviews, prospective observational studies, and long-term open-label trials, consistently support little to no cases of craving, intentional dose escalation, or illicit use following treatment. Moreover, no clinically significant cases of ketamine or esketamine abuse were reported in large clinical cohorts during maintenance treatment periods of up to 1 year (Aluisio et al., 2020; Haikazian et al., 2025; Li et al., 2020). Notwithstanding, some case reports show instances of misuse or dependence, primarily in situations of unsupervised or self-administered ketamine (Bonnet, 2015; Roxas et al., 2021; Schak et al., 2016), which accord with extant literature highlighting the importance of careful and routine monitoring as well as patient education throughout ketamine/esketamine-based treatment (Le et al., 2022; McIntyre et al., 2021).
Preclinical studies provide insights into the differential abuse liability of ketamine formulations. Specifically, CPP experiments suggest that (S)-ketamine is associated with dose-dependent rewarding effects, whereas (R)-ketamine lacks reinforcing properties (Chang et al., 2019; Yang et al., 2015). Notably, the doses used in these studies (5, 10, or 20 mg/kg; Yang et al., 2015) when scaled based on body surface area to an approximate human equivalent dose, as outlined by the U.S. Food and Drug Administration (2005), indicates that rodent doses must be adjusted by a species-specific conversion factor (kₘ). For rats, this corresponds to an approximate six-fold difference, such that rodent doses in the range of approximately 5–10 mg/kg would translate to a human equivalent dose of approximately 0.8–1.6 mg/kg, consistent with subanesthetic doses used in clinical settings subanesthetic exposures (Li et al., 2010, 2025). Despite this, caution is warranted when extrapolating findings from animal models to clinical safety, as preclinical paradigms primarily assess reinforcing properties under controlled conditions and may not fully reflect the complexity of human clinical populations including comorbid psychiatric conditions (e.g., depression or post-traumatic stress disorder), prior substance use history, aging, or other medical factors that may influence real-world abuse liability.
In addition, early-life stressors that are used as a model of a depression phenotype, such as maternal deprivation, impact CPP responses in a sex-dependent manner (Jornet-Plaza et al., 2025). Jornet-Plaza et al. (2025) found that male rats often showed increased sensitivity while females exhibited attenuated or altered reward responses. In addition, locomotor sensitization studies align with CPP findings. (S)-ketamine was reported to induce hyperlocomotion and sensitization over repeated dosing, while (R)-ketamine was not found to have these effects (Chang et al., 2019). Adolescent females show hyperactivity and sensitization, substantiating the influence of developmental stage and sex on ketamine’s stimulant-like effects (Jornet-Plaza et al., 2025). In addition, operant self-administration and relapse experiments further clarify ketamine’s differential abuse potential, wherein rats self-administer ketamine readily under fixed-ratio schedules, and stressed female rats display potentiated intake and motivation to consume ketamine under progressive-ratio schedules (Wright et al., 2019). OBX rats, another model of depressive-like phenotypes, used more ketamine than the sham controls, however demonstrated attenuated relapse-like behavior during forced cessation of the drug (Babinska and Ruda-Kucerova, 2017). The aforementioned triangulation of evidence suggests that abuse liability is impacted by drug enantiomer, sex, and neurodevelopmental stage.
Integrating clinical and preclinical evidence provides a broader understanding of ketamine abuse liability. Preclinical studies demonstrate that ketamine can produce reinforcing and stimulant-like effects under experimental conditions, which may help explain rare clinical reports of compulsive use, dose escalation, or illicit acquisition following treatment. Data from clinical studies further suggests that inadequately controlled and monitored ketamine/esketamine use may further exacerbate pre-existing risk from biological factors contributing to abuse potential, whereas supervised administration, structured dosing schedules, and ongoing monitoring may help mitigate these risks in therapeutic settings. The foregoing suggests that while the potential for ketamine addiction and the development of ketamine use disorder exists, clinical context and monitoring appear to play an important role in limiting misuse during therapeutic use. These findings also highlight the importance of patient education, ongoing monitoring for misuse-related behaviors, and adherence to structured treatment protocols when administering ketamine-based therapies in clinical settings.
However, several limitations of this review must be acknowledged. Many of the included clinical studies are observational or retrospective, limiting the ability to make conclusions surrounding the abuse potential of ketamine. In addition, sample sizes in several of the prospective trials are relatively small with variable treatment schedules and follow-up periods, which may result in the underestimation of the presence of delayed or rare abuse/misuse events. Furthermore, case reports, although informative of abuse-related events, are inherently biased due to their sample size pertaining to one individual. In addition, it should be noted that although this review sought to investigate the abuse potential of ketamine across all DSM-5-TR mood disorders, an overwhelming number of the included studies investigated the abuse liability of ketamine for TRD, which a small number of studies investigating the use of ketamine for TRBD. Although this is due to the current landscape of ketamine treatment for these mood disorders in particular, it limits the generalizability of findings across different mood disorder populations. Importantly, pharmacovigilance datasets such as FAERS and WHO VigiBase are designed for signal detection rather than quantitative risk estimation and therefore cannot be used to determine the incidence of adverse events. Accordingly, findings from these systems should be interpreted cautiously given limitations including duplication, incomplete reporting, and reporting bias. Finally, the heterogeneity in study design including differences in dosing, administration route, and monitoring as well as follow-up protocols between preclinical models and clinical studies as well as between clinical studies limit direct comparison between studies.
Regulatory frameworks may also influence abuse risk. IN esketamine is administered under structured monitoring programs in both the United States and Canada, requiring in-clinic dosing and post-administration observation (Sanacora et al., 2025; Janssen Inc, 2024). In contrast, racemic ketamine may be prescribed off-label for mood disorders and delivered through less structured care models, including telehealth-supported or take-home treatment (Mathai et al., 2024). Emerging evidence suggests that differences in regulatory controls, rather than pharmacology alone, may contribute to divergent patterns of misuse between ketamine and esketamine (Dart, 2024). In less regulated settings, the potential for unsupervised dosing may increase the risk of misuse. Supporting this concern, non-peer-reviewed survey data suggest that 55% of individuals receiving at-home ketamine therapy reported accidentally or intentionally exceeding the recommended dose, highlighting a potential public health concern (Plus APN, 2023).
Additional considerations include the impact of comorbidities, which are often overlooked in controlled trials. For instance, patients with comorbid SUDs, which are common in TRD (Brenner et al., 2019), are often excluded from studies (Geller et al., 2024). Consistent with this, several of the included clinical studies excluded individuals with current SUD (Gutierrez et al., 2025; Wajs et al., 2020), while only a subset of observational studies included participants with comorbid SUD (Martinotti et al., 2022; Ryan and Heifets, 2025). Notably, we identified one case report describing a patient with an extensive history of substance abuse beginning in early adolescence (Liu et al., 2015). Overall, reporting of SUD status was limited and inconsistently defined, with few studies reporting the proportion of participants with SUD (e.g., 6% and 49% in Martinotti et al., 2022 and Ryan and Heifets, 2024), limiting the conclusions on ketamine’s abuse potential in at-risk populations. Interactions with concomitant medications such as benzodiazepines or stimulants may also have an impact on both therapeutic outcomes and risk of misuse, yet remain largely underexplored. Moreover, most studies fail to conduct follow-ups longer than 12 months, with most ceasing long before this point. This results in uncertainty about whether tolerance, dose escalation, or misuse might emerge with longer-term treatment. Future research should incorporate regular validated assessments of drug liking and craving during ketamine treatment, investigate abuse potential across diverse patient populations including individuals with TRBD and comorbid SUDs, and extend follow-up periods beyond 12 months to prospectively identify individuals at higher risk of misuse. As well, important unanswered questions remain regarding long-term misuse risk and the real-world safety profile of ketamine-based treatments outside controlled clinical environments. Clinical trials should also consider long-term monitoring, including post-discharge behavior, attempts to obtain the drug beyond clinical use, and potential self-administration outside structured settings. Finally, incorporating translational markers, such as enantiomer-specific effects and sex differences, could lead to improved risk assessment and further improve patient safety in clinical settings.
Conclusion
The results of this review indicate that ketamine appears to be associated with a low risk of abuse potential when administered therapeutically in controlled, supervised conditions. Clinical studies report minimal instances of craving, dose escalation, or illicit use, while preclinical findings highlight factors, including enantiomer, sex, and developmental stage that may influence the drug’s reinforcing effects. Limitations in the literature including small sample sizes, short or variable follow-up, observational study designs, and a focus on TRD highlight the need for longitudinal, prospective studies across diverse populations. Incorporating systematic assessments of craving, drug liking, and post-treatment behavior will improve understanding of abuse liability to inform treatment guidelines. Collectively, these findings suggest that ketamine and esketamine may be administered with manageable risk within rigorously monitored clinical settings.
Supplemental Material
sj-docx-1-jop-10.1177_02698811261453814 – Supplemental material for Evaluating the abuse liability of ketamine in the treatment of mood disorders: A systematic review
Supplemental material, sj-docx-1-jop-10.1177_02698811261453814 for Evaluating the abuse liability of ketamine in the treatment of mood disorders: A systematic review by Shreya Vasudeva, Gabrielle F.M. Lovell, Sabrina Wong, Gia Han Le, Diana K. Orsini, Sara Di Luch, Roger S. McIntyre and Joshua D. Rosenblat in Journal of Psychopharmacology
Footnotes
Author contributions
Conceptualization: S.V. and J.D.R. Data curation: S.V. and G.F.M.L. Investigation: S.V. Methodology: S.V. Project administration: S.V. and J.D.R. Resources: S.V. Supervision: S.V. and J.D.R. Validation: S.V. and G.F.M.L. Visualization: S.V. Writing – original draft preparation: S.V. Writing – review & editing: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Joshua D. Rosenblat has received research grant support from the Canadian Institute of Health Research (CIHR), Physician Services Inc (PSI) Foundation, Labatt Brain Health Network, Brain and Cognition Discovery Foundation (BCDF), Canadian Cancer Society, Canadian Psychiatric Association, Academic Scholars Award, American Psychiatric Association, American Society of Psychopharmacology, University of Toronto, University Health Network Centre for Mental Health, Joseph M. West Family Memorial Fund, Inagene and the Timeposters Fellowship and industry funding for speaker, consultation, and research fees from iGan, Boehringer Ingelheim, AbbVie, Braxia Health (Canadian Rapid Treatment Centre of Excellence), Braxia Scientific, Janssen, Allergan, Lundbeck, Sunovion and COMPASS. Dr. Roger S. McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute; speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Neurawell, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eli Lilly, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, Abbvie, Bristol Myers Squibb (BMS), Teva, Adhere Tech, GH Research, Autobahn Theapeutics and Atai Life Science.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.