
Abstract
In the past decade, interest in studying psychedelic compounds as potential therapeutic agents has resurged. These studies carefully exclude individuals at risk for developing psychotic symptoms in response to psychedelic use. Given the potential for psychedelics to be established as treatments in psychiatry, it is important to more robustly understand their link with psychosis and schizophrenia spectrum disorders (SSDs). In this narrative review, we examine the historical and theoretical relationship between psychedelic drugs and SSDs, including the origins of the psychotomimetic hypothesis. For key psychedelic compounds, we review their phenomenological manifestations in relation to the experiential alterations characteristic of SSDs, revealing both areas of overlap and important qualitative differences that challenge the uniform psychotomimetic classification. We also review putative neural mechanisms underlying altered experiential states associated with psychedelic use and SSDs, with attention to serotonergic, dopaminergic, and glutamatergic contributions. Clinical evidence demonstrates that psychedelics can exacerbate pre-existing psychotic illness and may trigger psychosis in vulnerable individuals, though the magnitude of these risks remains inadequately quantified. However, phenomenological and mechanistic distinctions suggest that potential therapeutic applications may exist for carefully selected symptoms (negative symptoms, depression) in stable patients using low-dose, controlled approaches. Based on published work, we provide recommendations regarding psychosis-related risk and potential avenues for the treatment of SSDs as psychedelics gain traction as therapeutics.
Introduction
Recent years have witnessed a revitalized and accelerated interest in the use of psychedelic compounds as therapeutic agents (Nutt and Carhart-Harris, 2021; Solmi et al., 2022). This resurgence is reflected through a growing mental health and addiction crisis, driving research into additional therapeutic modalities, including psychedelics. In the past decade, psychedelic research has been spurred by the backing of non-governmental sources (e.g., foundations and private equity), and, most recently, with federal support (Phelps et al., 2022). The accumulating number of recent clinical trials that have formally examined therapeutic applications of psychedelic compounds highlights both a broad interest in the therapeutic potential of these powerful drugs and an important shift in attitudes both in the public domain and in the psychiatric community.
Much of the recent work with psychedelics recapitulates the robust history of studies conducted through the 1960s, prior to restrictive drug rescheduling and cultural stigmatization (Busch and Johnson, 1950; Cohen, 1967; Hoch et al., 1952; Nichols and Walter, 2021; Sandison et al., 1954). During this nascent period, psychotic illness and psychedelic drugs converged in discussions of phenomenology, pathophysiology, risk, and therapeutic potential (Bowers, 1968; Savage and Cholden, 1956; Vollenweider and Geyer, 2001). However, the presence of psychosis or a schizophrenia spectrum disorder (SSD) is, categorically, a strict contraindication in recent studies examining psychedelic drugs as therapeutic agents (Johnson et al., 2008; Nutt and Carhart-Harris, 2021; Reiff et al., 2020). Given that the early studies highlight a complex and integrated relationship between the schizophrenia spectrum and psychedelic research, the rigorous exclusion of psychosis in psychedelic research today warrants a broader dialogue on the widespread therapeutic considerations of these drugs (Paparelli et al., 2011; Sabé et al., 2024; Simonsson et al., 2023).
To contribute to this dialogue, this narrative review aims to synthesize several strands of research and evidence to explore how available phenomenological, neurophysiological, and clinical knowledge allows for evaluation of the risk and potential of psychedelic drugs in SSDs. In contrast to other systematic reviews examining psychedelic applications across psychiatric disorders (Nutt and Carhart-Harris, 2021; Reiff et al., 2020), our aim is not to comprehensively review therapeutic evidence for these broader applications. Rather, we focus specifically on the intersection with SSDs. First, we lay a historical and theoretical foundation by discussing the origins of the psychotomimetic hypothesis and the empirical evidence initially thought to support it. We then turn to comparative phenomenological analyses, comparing available data on the experience of psychedelics to the distinct qualitative features of SSDs, as informed by the contemporary phenomenological self-disorder model (Sass and Parnas, 2003). These analyses prepare us to offer remarks that reevaluate the experiential basis for the psychotomimetic status of psychedelics. We then review putative neural mechanisms underlying altered experiential states associated with psychedelic use and inherent to SSDs. Finally, we integrate empirical findings on psychedelic exposure in individuals with preexisting SSDs to illustrate potential risks, therapeutic implications, and recommendations for ongoing clinical research.
Historical and theoretical background
Most prominent in contemporary psychedelic research are the so-called “classic psychedelics,” grouped by their similar altering effects on subjective experiences (e.g., changes in perception, induction of spiritual or mystical experiences) and their primarily serotonergic effects achieved by means of serotonin 5-HT2A receptor agonism (Ley et al., 2023). These substances include psilocybin, a naturally produced species of fungi, which has been examined as a treatment for a range of psychiatric conditions (Bogenschutz et al., 2022; Carhart-Harris et al., 2021; Davis et al., 2021a; Goodwin et al., 2022; Griffiths et al., 2016; Moreno et al., 2006; Raison et al., 2023; Ross et al., 2016). Other serotonergic psychedelics include mescaline; d-lysergic acid diethylamide (LSD), a synthetic psychedelic; N,N-dimethyltryptamine (DMT) found naturally in ayahuasca brews; and 5-methoxy-N,N-dimethyltryptamine, extracted from river toad glands. Another compound, often grouped as a psychedelic and similarly experiencing a resurgence of attention for its therapeutic utility (e.g., Mitchell et al., 2023), is 3,4-methylenedioxymethamphetamine, commonly known as MDMA. Finally, ibogaine, a psychoactive substance found in the bark of the iboga tree, is also a psychedelic with mechanisms of action distinct from 5-HT2A agonism.
The early enthusiasm for psychedelic drugs in psychiatric research revolved around two aims. Initially, psychedelic drugs were investigated as psychotomimetic (or psychosis-mimicking) agents to better understand psychosis-related phenomena (Nichols and Walter, 2021). This was motivated by the observation of phenomena in mescaline intoxication that were thought to be consistent with psychotic states, including: loss of ego boundaries (breakdown between the boundaries of self and world), disturbances in perception (i.e., visual hallucinations) and thought (i.e., impaired concentration and reasoning abilities), and increased sensitivity to stimuli (Jay, 2019; Mogar, 1970). However, interest in the therapeutic potential of classic psychedelics for SSDs soon emerged. By bringing about experiences presumed to be psychotic, researchers hoped that substances such as mescaline and LSD would facilitate a therapeutic process of “working through” unconscious conflicts (Arieti, 1955; Nichols and Walter, 2021).
Psychomimetic hypothesis
Systematic study of mescaline began in 1888, when Louis Lewin, a toxicologist from Berlin, obtained dried peyote samples from the Parke-Davis Pharmaceutical Company. Working with his colleague Arthur Heffter, he isolated and characterized several alkaloids, including anhalonidine, anhalonine, pellotine, lophophorine, and mescaline. Using both animal and self-experimentation, Heffter published a seminal 1894 report establishing mescaline as the principal alkaloid responsible for the psychedelic effects of peyote (Heffter, 1894).
This line of inquiry catalyzed research that linked psychedelic compounds and psychosis, driven by similarities in the perceptual and psychological experiences of mescaline use and psychotic symptoms (Jay, 2019). Mescaline’s psychotomimetic properties were further documented in Kraepelin’s early psychopharmacologic experiments. During this era, Kraepelin contributed important work that conceptualized the need for “model psychoses” that could be derived from a pharmacologic induction of disease states (Kraepelin, 1882; Müller et al., 2006; Savage and Cholden, 1956). Across Europe, investigations by researchers—including Kraepelin himself—examined mescaline’s potential for producing experimental psychopathological states. This included detailed first-person accounts of intoxication to deliberate attempts to reproduce the presentations of psychotic illness (Beringer, 1923; Fernberger, 1923; Knauer, 1913; Lewin, 1931; Rouhier, 1927).
Guttman and colleagues summarized many of these observations, reporting on subjects administered synthetic mescaline sulfate (Guttmann, 1936). They further advanced the view that psychedelic agents could serve as experimental models for elucidating “the complicated interplay of aetiological factors in the origin of psychoses.” This first wave of mescaline research culminated in the influential 1940 report by Stockings et al., which drew explicit parallels between mescaline-induced states and schizophrenia through contemporaneous clinical descriptions. Critically, Stockings (1940) emphasized the concept of a psychogenic psychosis, underscoring mescaline’s utility as a research tool. In addition, the report anticipated brain-based approaches to experimental psychoses by highlighting the involvement of auditory, visual, and “higher” cortical processes (Stockings, 1940).
This convergence ultimately informed broader biochemical hypotheses. Osmond and Smythies (1952) proposed that schizophrenia and mescaline intoxication share a striking phenomenological overlap via a biochemical link through adrenaline metabolism (Osmond and Smythies, 1952). Both conditions produce vivid hallucinations, thought disorder, catatonia, mood disturbance, and distortions of self and reality, though schizophrenia arises spontaneously and can be chronic, while mescaline intoxication is acute and time limited. The authors highlight mescaline’s close structural similarity to adrenaline and hypothesize that a pathological error in adrenaline’s methylation pathway could generate mescaline-like compounds (“M-substance”) endogenously. Such toxins might emerge under stress when the adrenal system is overworked, explaining why psychosis is often precipitated by stress and why its presentation varies widely. This mechanism could also account for the therapeutic effects of insulin, which antagonizes adrenaline and alters glucose metabolism, counteracting mescaline-like activity. Thus, schizophrenia is framed as a “synthetic illness” (Osmond and Smythies, 1952), potentially caused by abnormal adrenal metabolism producing mescaline analogues.
Albert Hofmann’s accidental discovery of LSD’s psychedelic properties in 1943 further propelled Kraepelin’s conception of a pharmacologically induced, experimental model of psychosis, while simultaneously opening the door to therapeutic investigations (Hofmann, 1979; Nichols, 2018). Promoted by Sandoz, LSD offered distinct advantages over mescaline: it produced effects of shorter duration but far greater potency, allowing for tighter experimental control in eliciting both psychedelic experiences and purported psychotomimetic states. By 1960, psilocybin was studied experimentally and classified as a psychotogenic compound, as its effects were considered largely similar to those of LSD and mescaline (Figure 1; Rinkel et al., 1960). The purported psychotomimetic properties of psilocybin were further considered in subsequent decades (Kleinman et al., 1977). For instance, studies in healthy volunteers using 5-HT2A antagonists have demonstrated that blocking psilocybin’s effects can prevent its psychotic-like symptoms (Vollenweider et al., 1998).
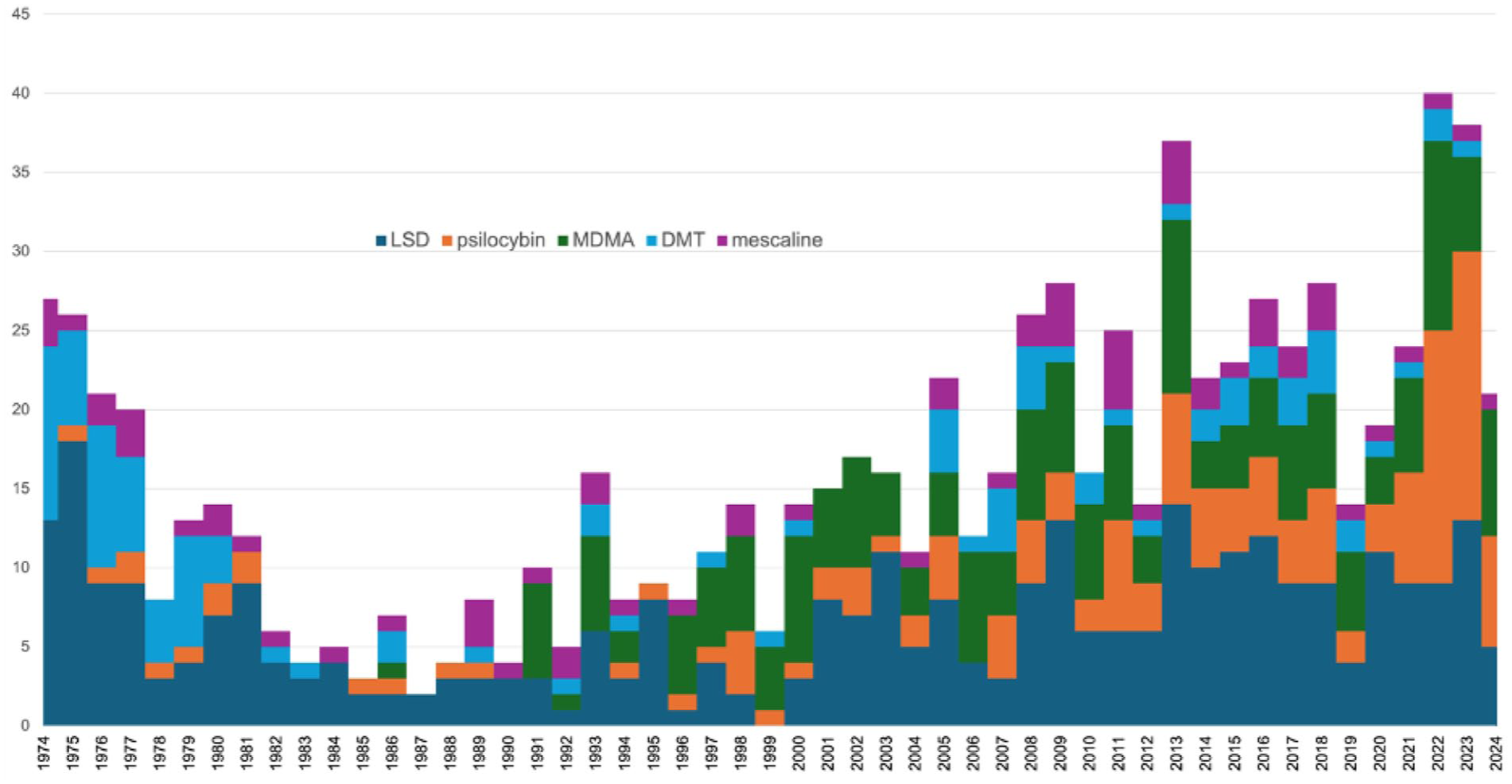
Distribution of MEDLINE publications by psychedelic compound with keywords “psychosis” or “schizophrenia.” LSD has been the most prominent compound in psychedelic research focused on psychosis or SSDs. However, in recent years, there has been a larger representation of studies focused on psilocybin.
Today, promising results on the efficacy of psychedelic-assisted therapy for depression and anxiety have prompted a need to reevaluate the psychotomimetic status of psychedelics; the potential of such substances to mitigate the negative symptoms and the mood components of SSDs must first be weighed against an evaluation of their risk for activating psychotic symptoms. We argue that carefully attending to and comparing the first-person experience of both psychotic and psychedelic experiences (taken with other strands of evidence) can be in service of this need. Of particular relevance to this comparative aim is the phenomenological self-disorder model of SSDs (Sass and Parnas, 2003). Given that this model of SSDs provides detailed and qualitatively rich descriptions of the overall context of patient experiences, examining the varieties of psychedelic experiences side-by-side with phenomenological descriptions of SSDs is useful for looking past superficial similarities between both types of experiences (e.g., the presence of “hallucinations” or impaired thinking).
Comparative phenomenology: Mescaline, LSD, psylocibin, DMT, and SSDs
Relevance of the self-disorder model of SSDs
SSDs are typically understood in terms of a combination of four core symptom dimensions: positive symptoms (hallucinations, delusions), negative symptoms (e.g., diminished emotional expression or motivation), thought disorders (e.g., tangential or incoherent speech), and disorganized behavior (e.g., rigid posture; American Psychiatric Association, 2013). The self-disorder model conceptualizes the core symptoms of SSDs as emerging within broader experiential shifts that precede the onset of psychosis (Feyaerts and Sass, 2024; Sass et al., 2018).
Central to the self-disorder model is the notion of basic or minimal selfhood: the implicit sense that experience is given as one’s own (Zahavi, 2005) The self-disorder model proposes that this most basic level of self is disrupted in SSDs. Experientially, this instability manifests in a range of anomalous transformations that can be organized within two interconnected domains: self-experience and world experience. Anomalous experiences are hypothesized as preceding and accompanying the core symptoms of SSDs (Brar et al., 2025; Parnas, 2011; Parnas and Henriksen, 2014).
Anomalies of self-experience can be understood in terms of complementary alterations: hyperreflexivity and altered self-presence (Feyaerts and Sass, 2024; Sass et al., 2018). Hyperreflexivity includes anomalies that result from the transformation of normal processes that are typically tacitly experienced, such as inner speech and bodily sensations, into objects of intense awareness. This transformation of processes that are typically the medium of experience into the objects of experience coincides with a loss of ownership and control over these processes. Alterations in self-presence can involve both a diminished sense of being a subject of experience directed toward the world, for example, the sense that one is somehow nonexistent, or a heightened self-presence, for example, the sense that one creates everything that exists or that all occurrences in the world refer to one’s mental activities. Hyperreflexivity and altered self-presence have been proposed as explaining the emergence of specific symptoms in SSDs. For instance, an increased alienation from one’s stream of cognition or bodily events, taken with increased tension and acute awareness of these abnormalities, may eventually amount to the experience of such phenomena as imposed upon the individual from the external world (i.e., thought insertion or delusions of control; Klosterkötter, 1992; Nordgaard et al., 2020).
Anomalies of world experience include a range of transformations in the salience of the perceptual field (Kapur, 2003; Pienkos et al., 2017). In basic self-disturbance research, these anomalies are also sometimes referred to as disturbances or alterations in grip. These can include objects appearing as unreal, fake, and lacking their everyday “affordances” for action, or the encountering of benign events in one’s environment as having a special yet unknown significance. Anomalies of world experience have also been linked to certain core symptoms in SSDs. For example, a gradual sense of anxious anticipation associated with finding one’s surroundings as unreal may motivate a search for meaning, culminating in the sudden appearance of a paranoid idea that grants coherence to perplexing changes in the perceptual field (Conrad, 2012; Feyaerts et al., 2021; Fuchs, 2020).
We begin our comparative phenomenological analyses below by first attending to transformations of world experience during the acute effects of classic psychedelics and in SSDs. This is because such transformations are perhaps those most frequent and salient during the effects of psychedelics (Ley et al., 2023), and for this reason offer a starting point for comparison with the states characteristic of SSDs. We will then consider transformations of self-experience.
Transformations of world experience: Meaning, the sense of reality, and revelation
First-person accounts of the effects of classic psychedelics and SSDs draw attention to striking similarities—and subtle differences—in the meaning or significance of everyday objects, and in the overall “feel” or “atmosphere” of reality. These transformations can, as we will see, amount to moments of revelation or insight. First, let us consider changes in the meaning of everyday objects.
Key examples of such changes have been described by Nelson and Sass (2008) in their analysis of Huxley’s (1963) experience of mescaline use, as recounted in The Doors of Perception. Here, Huxley describes encountering objects in their “mere-being”: there is no longer the immediate understanding of a chair as a thing for sitting, but as a “pure object” (Huxley, 1963). Similarly, in a mescaline experience reported by Osmond (1970), the subject writes: “a sense of special significance began to invest everything in the room . . . A plain wooden chair was invested with a ‘chairliness’ which no chair ever had for me before” (p. 24). In Huxley’s account, this experience of the “mere-being” of objects was associated with a dissolving of spatial relations between objects; rather than apprehending a visual field of related entities, objects were encountered in an individuated manner, each glowing with an “inner light,” and imbued with an almost ineffable beauty and significance. Experiences of awe, beauty, and novelty inherent to objects—and accompanied by euphoria—have likewise been observed under the effects of LSD, psilocybin, and DMT (Aaronson and Osmond, 1970; Huxley, 1963; Krippner, 1970; Wasson and Wasson, 1957).
As Nelson and Sass (2008) note, the experience of the mere-being of objects may be particularly characteristic of the prodromal stages of schizophrenia, where it is often accompanied by a frightful affective tone (Nelson and Sass, 2008). In the memoir Autobiography of a Schizophrenic Girl, for example, Renee states: “I looked at a chair or a jug, I thought not of their use or function . . . but as having lost their names, their functions and meanings,” elaborating that this strange experiential transformation filled her with terror (Sechehaye, 1962). A loss of spatial relations, or a “fragmentation of perception,” has also been described in classic phenomenological writings on schizophrenia. Matussek (1987) described how patients with schizophrenia are given to captivation by isolated objects or details in the perceptual field: “I may look in the garden . . . I can only see details . . . I can lose myself looking at a bird on a branch, but then I don’t see anything else” (p. 92). Other affinities and dissimilarities in world experiences can be construed in terms of changes in the sense of reality.
In SSDs, the stripping away of everyday significances can also take the form of a profound sense of unreality (hypo-reality): everyday surroundings can lose their sense of objective presence in the world, an experience that individuals may describe by saying that objects appear illusory, false, or somehow fake (Conrad, 2012; Feyaerts et al., 2021). Stockings (1940) reports experiences of derealization in mescaline intoxication that may bear some possible resemblance to those in pre- and sub-psychotic changes: “it appears to the subject as if . . . a veil of unreality had been laid over everything . . . objects appear more or less unchanged . . . and yet they are completely different” (p. 33). However, it is unclear just how prevalent experiences of unreality are in mescaline use, and whether they are induced by other classic psychedelics. In addition to the sense of unreality, psychedelic and psychotic experiences can be characterized by hyperreality. This involves an intensification of the presence (e.g., vividness) and significance of percepts, such that they feel more real than usual, command the perceiver’s attention, and appear to disclose a revelation or insight.
In hyperreal changes in reality in SSDs, patients experience nothing as a mere coincidence, but as deeply interconnected necessities that give the impression of penetrating to the deeper layers of reality (Conrad, 2012; Feyaerts et al., 2021): “At that moment, I believe you are in contact with the universe. Every step that I took was rhythmical . . . everything was rhythmical” (Feyaerts et al., 2021: 9). These changes in the sense of reality, and the revelatory experiences they bring about, are sometimes expressed by patients in mystical or religious terms—patients can, for example, describe a state of divine unity or access to the secrets of the universe. Nelson and Sass (2008) likewise note how the transformations of mere-being and heightened significance reported by Huxley were experienced as providing unmediated access to a “truer” reality. Questionnaire-based studies suggest that experiences of mystical union or connection with “ultimate reality” may also be prevalent across the effects of other psychedelics, such as psilocybin and DMT (e.g., McCulloch et al., 2022; Timmermann et al., 2018).
The perceptual field in psychedelic experiences and SSDs, then, seems to undergo similar changes in its overall salience (i.e., the meaning of objects) and quality (realness), and what it discloses (revelation) (Kapur, 2003). While further analyses are required for a finer-tuned comparison, some distinctions can be made. In SSDs, the changes described above eventually take on a self-referential quality; that is, the sense that these mysterious changes in the perceptual field concern the individual, or refer to them, in some indeterminate manner—a hypothesized pathway to delusions (discussed in more detail below; Fuchs, 2020; Jaspers, 1913). Similarly, Matussek (1987) argued that in the fragmentation of perception, the “splitting of individual perceptual components from their natural context” (p. 90) allows for a new meaning of objects to emerge. These new meanings, in SSDs, can include nihilistic (impending catastrophes) or self-referential and paranoid themes. This phenomenological observation is consistent with the hypothesis that while both psychedelic and psychotic experiences involve an “entropic-broadening” process (widened attentional scope and decreased predictability of stimulus processing), the latter type of experience is distinguished by an exaggerated self-focus (Dourron et al., 2022).
Transformations of self-experience: Dissolution of ego boundaries and depersonalization
Resemblances in alterations of self-experience across the classic psychedelics and psychotic experiences are also notable. Huxley (1963) writes of a loss of distinction between himself and the perceived object, as if gazing at bamboo legs or a chair merged him with these objects. Comparable experiences have been reported under the effects of psilocybin. For example, Krippner (1970) writes: “I sniffed the cloves, and their fragrance seemed to envelop my whole being. I became the odor . . . I became the taste” (p. 37). Such a description, characterized by heightened tactile and olfactory sensitivity, may suggest a kind of pleasant merging of the experiencer and what is experienced as sensations. This experience of expanding ego boundaries may not always be pleasant or experienced as a mystical union; one experimental study on psilocybin reported an anxiously experienced loss of ego boundaries in participants along with paranoid ideation (the content of such ideation, however, was not reported). Experiences of joining with objects and the environment have long been described in SSDs (Bleuler, 1911). Such experiences may likewise be accompanied by an elated affective tone and elaborated in a mystical manner, or may alternatively be experienced as threatening or annihilating. A fragility in ego boundaries in SSDs can also involve an experience of the other’s gaze as threatening, as if this mere gaze was exposing the individual, or risking engulfment by and with the other (Laing, 1959). Such experiences, from a phenomenological perspective, are interpreted as a manifestation of diminished self-presence: a weakened sense of being a “real” self renders this unstable self vulnerable to dissolution or merging with the surroundings (Parnas and Sass, 2001).
Degrees of depersonalization are also possible under the effects of the classic psychedelics (Huxley, 1963; Hofmann, 1959; Lawrence et al., 2022; McCulloch et al., 2022), Huxley describes—again, mainly in mystical terms—a sense of the self as separate from his body, experienced almost as an object. Hofmann (1959), describing effects of LSD, reports a more extreme and frightening out-of-body experience: “I felt as if I were out of my body. I thought I had died. My ego seemed suspended somewhere in space, from where I saw my dead body lying on the sofa” (p. 246). Experiences of depersonalization in classic psychedelic use should be compared with those in SSDs with caution. The hyperreflexive forms of depersonalization that appear more frequently in SSDs (Raballo et al., 2021)—and which may serve as precursors to certain first-rank symptoms (i.e., delusions of control, thought insertion)—tend to be more subtle forms of alienation from one’s body. Such experiences can take the form of feeling that one’s body is somehow strange or alien, that one is not fully in control of one’s movements, or at a distance from one’s actions (Klosterkötter, 1992; Nordgaard et al., 2020).
Thus, while the self undergoes transformations in both psychedelic and psychotic experiences, caution should be exercised when interpreting the former as involving a disturbance in the basic sense of self. Indeed, descriptions of a loss of ego boundaries in psychedelic experiences are not reported as coinciding with a diminution of self-presence or a sense of non-existence. On the contrary, Dourron et al. (2022) note how at least one first-person account of psilocybin indicates the potential of psychedelics to make the ordinarily implicit sense of self-presence explicit and amenable to thematic description: “I had just found the ‘I’—that perceptual point of view . . . that place of awareness beyond form” (Dourron et al. 2022). Further, while psychedelic users may find themselves as disconnected or separated from their bodies, missing from these descriptions is a loss of ownership over the medium of selfhood—that is, one’s thoughts and bodily sensations. Also notably absent from descriptions of classic psychedelic experiences is the extreme exaggeration of self-presence sometimes described in SSDs: “A young patient reported that he had . . . a feeling that only the objects in his current field of vision were real, as if the rest of the world . . . did not exist” (Parnas and Sass, 2001). Important here is the solipsistic quality of this experience: the world is felt to have no existence independent from the experiencer. Contrast this with how, under the effects of classic psychedelics, the individual feels to have discovered a fundamental insight into shared reality and communal human existence.
Comparative phenomenology of other psychedelic compounds with SSDs
3,4-Methylenedioxymethamphetamine
Perhaps the starkest differences with SSDs are to be found in comparison with MDMA, which many researchers do not classify as a psychedelic at all given its distinct pharmacological and phenomenological profile (Nichols, 1986). MDMA has been described as an “entactogen” or “empathogen”—a substance with a distinct ability to aid users’ access to their emotions and increase their sense of interpersonal connectedness (Nichols, 1986). Indeed, studies of the subjective experience of MDMA across users emphasize largely positive changes in emotional (elation, euphoria) and interpersonal experience (increased interpersonal connections; Baylen and Rosenberg, 2006; Hysek et al., 2014; Kirkpatrick et al., 2014). While studies reporting on the subjective experience of MDMA do report “loss of ego boundaries” and experiences of “unity,” the experiences at hand are likely to be qualitatively distinct from the transformations of self-experience characteristic of SSDs (Leneghan, 2013; Liester et al., 1992). In MDMA intoxication, expressions of “unity” with others may rather reflect increased awareness of emotions in interpersonal contexts (empathy, love, care) and a sense of closeness or intimacy with others. Based on available reports, there is little reason to contend that such experiences of “loss of ego boundaries” express confusion between oneself, others, and the external world—as is characteristic of SSDs. Among the notable adverse reactions to MDMA are the sequelae of serotonergic neurotoxicity (McCann et al., 2000). These reactions are largely functional, however, manifesting as changes in attention, reasoning, and memory, in addition to potential changes in sleep patterns.
Ibogaine
While described as a hallucinogen, ibogaine intoxication—at high doses—may be more akin to vivid waking dreams than the “hallucinogenic” experiences or visual alterations found in classic psychedelics (Alper and Lotsof, 2007). This is due to users reporting intense, closed-eye visual imagery, much like viewing a film, often involving navigation of some visual landscape. The imagery experienced may relate to an individual’s autobiography or may be more surreal, comical, or spiritually themed. At lower doses, ibogaine has been described as having stimulant effects (Lecomte, 1864). It is therefore not apparent that typically schizophrenic transformations in the everyday understanding of the perceptual field, and experiences of alienation from one’s bodily actions, or dissolution between self and world, which sometimes overlap with other psychedelic experiences, figure centrally in ibogaine intoxication. Available evidence on adverse psychiatric reactions is limited and does not allow rigorous comparison with schizophrenic psychosis (Rocha et al., 2023).
Reconsidering the phenomenological basis of the psychotomimetic hypothesis
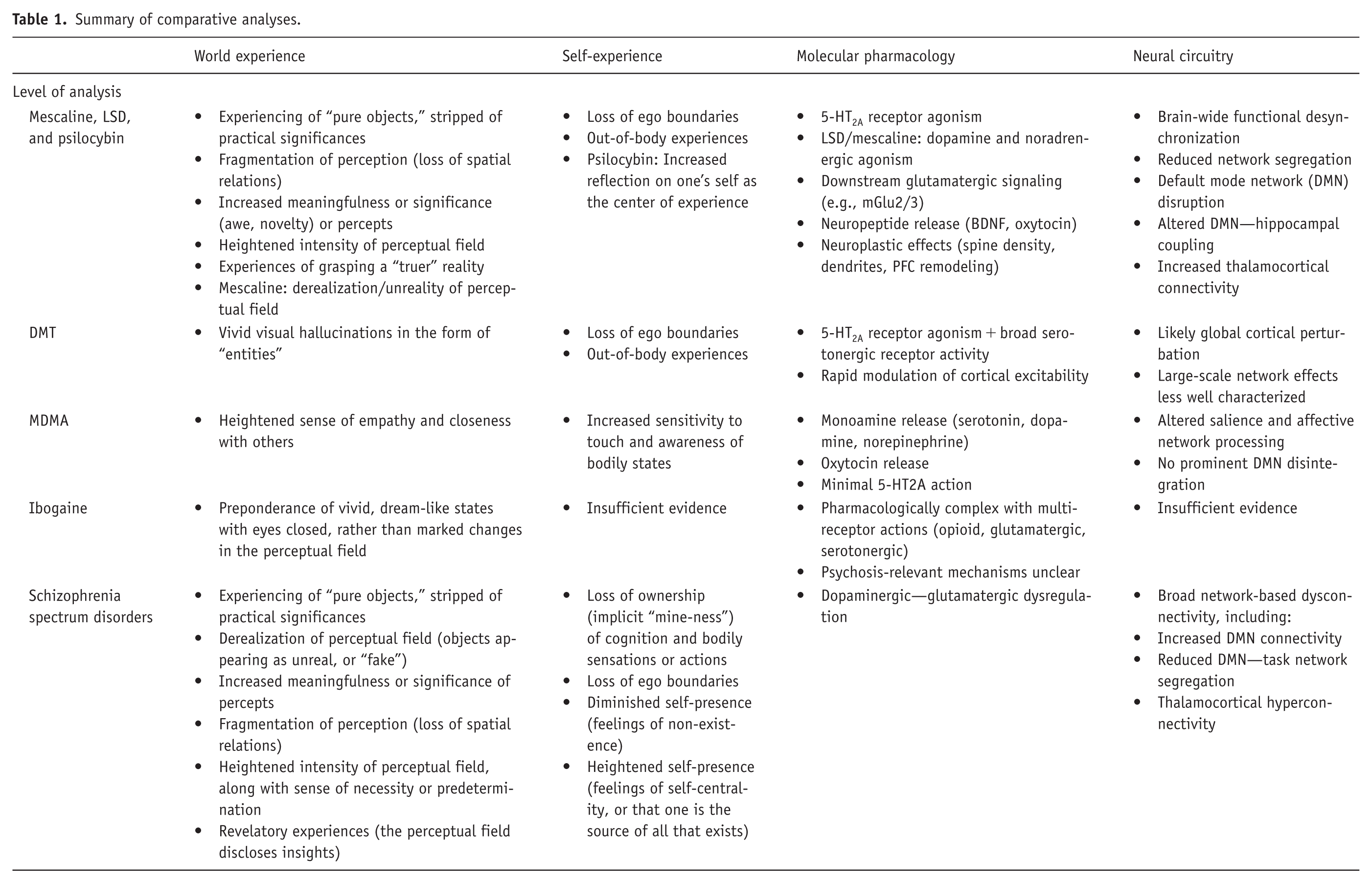
Above, we first discussed the psychotomimetic hypothesis, reviewing how this position was motivated by the observation of certain clinical similarities between psychedelic states and psychotic experiences, including hallucinations, thought disturbances, depersonalization, loss of ego boundaries, and delusions. Having now laid a broader phenomenological ground by framing the experiences at hand in terms of transformations of world and self (see Table 1 for summary), we argue that it remains dubious whether psychotic symptoms—if and when they emerge during the psychedelic experience—genuinely resemble psychotic experiences in SSDs.
Summary of comparative analyses.
Consider one proposed pathway to paranoia in SSDs according to self-disorder theory in which anomalous world experiences figure centrally (Brar et al., 2025; Fuchs, 2020; Jaspers, 1913). The isolated, “mere object” quality of entities in the perceptual field may grasp the individual with a strange and indeterminate meaning, and the quality of being unreal or constructed (derealization). As affective tension rises, the individual increasingly relates to these strange transformations as somehow referring to themselves, until a delusional idea emerges as revelation or insight. However, as we saw above, further phenomenological data are required to determine if the breakdown of conventional meanings of everyday objects and events in classic psychedelic experiences can indeed take on the derealized texture, anxious affective tone, and self-referential dimension that give way to delusional episodes in SSDs. Further, alterations in world- and self-experience brought on by non-classic psychedelics (MDMA and ibogaine) also do not seem consistent with those proposed as preceding the positive symptoms of SSDs.
Moreover, both psychedelic and psychotic experiences can involve mystical experiences of a revelatory character. In SSDs, these tend to manifest as delusions with metaphysical and even grandiose content and may emerge from a form of hyperreality. The individual experiences all happenings as necessary or predetermined; in other instances, those characterized by experiences of heightened self-presence, the individual feels themselves to be the creator, influencer, or referent of all happenings in the world (Feyaerts et al., 2021). These experiences may give rise to the impression that one has been chosen for a secret mission or has divine powers. While psychedelic experiences do also tend to produce lasting changes in metaphysical and spiritual beliefs in the individual (Timmermann et al., 2021), further phenomenologically informed inquiry must clarify whether these emerge from similar transformations of world and self. For instance, in experiences of psilocybin, an increased sense of interpersonal connection and empathy might contribute to a sense of unity or revelatory understanding (Metastasio et al., 2025). Further, DMT users report encountering and communicating with unworldly “entities,” which can include figures described as mythological beings, aliens, or machine-like entities (Lawrence et al., 2022). Also reported are near-death-like experiences, such as traveling through dark voids and to another realm beyond this earth, and experiences of approaching a “bright light” (Timmermann et al., 2018). These forms of experience may constitute a unique experiential pathway to the sense that one now possesses new insights into reality.
Lastly, another consistent apparent overlap between psychedelic and psychotic experience is a loss of ego boundaries. In some psilocybin studies, this experience has indeed been reported as anxiety-provoking and associated with delusional ideation (Yerubandi et al., 2024; Vollenweider et al., 1998). Again, further inquiry is needed here for phenomenological clarity. Nelson and Sass (2008) argue that such transformation in self-experience, as it occurs in psychedelic experience, is better characterized in terms of a fusion (experiencing the self in all). This can be contrasted with the dissolution of self-boundaries in SSDs, which may be associated with diminished self-presence, rendering the self vulnerable to being engulfed by, or annihilated by, the external world.
The above potential phenomenological overlaps and differences raise the question of whether the range of experiential features at hand reflects common neurobiological substrates or distinct mechanisms. Thus, we now turn to considering brain-based models of psychedelic action.
Brain-based mechanisms
Molecular pharmacology
A starting point for examining the neurobiological basis for psychedelic action is agonism at the serotonin 5-HT2A receptor, which is quintessentially linked with classic indoleamine-grouped psychedelic compounds, including psilocybin, LSD, and DMT, and the phenethylamine, such as mescaline (Figure 2). Occupancy of 5-HT2A receptors in the brain has been linked to the intensity of psychedelic experience, illustrating its central role (Madsen et al., 2019; Stenbæk et al., 2021). In addition, pretreatment with ketanserin, a second-generation antipsychotic and a 5-HT2A receptor antagonist, blocks the subjective psychedelic effects of both psilocybin and LSD (Preller et al., 2017; Vollenweider et al., 1998). In addition, second-generation antipsychotic medications have been found to be more effective than first-generation medications (D2 receptor antagonists) in treating psychedelic-induced psychosis (Sulstarova et al., 2025). These findings further support the role of 5-HT2A receptors in psychedelic experiences. Meanwhile, 5-HT2A receptor action has been linked with a variety of neuroplastic effects, including changes in neuronal spine density, the proliferation of dendrites, and broader structural remodeling in the prefrontal cortex (Ly et al., 2018; Vargas et al., 2023). These preclinical findings have been putatively linked with the therapeutic effects of psychedelics as psychiatric treatments.
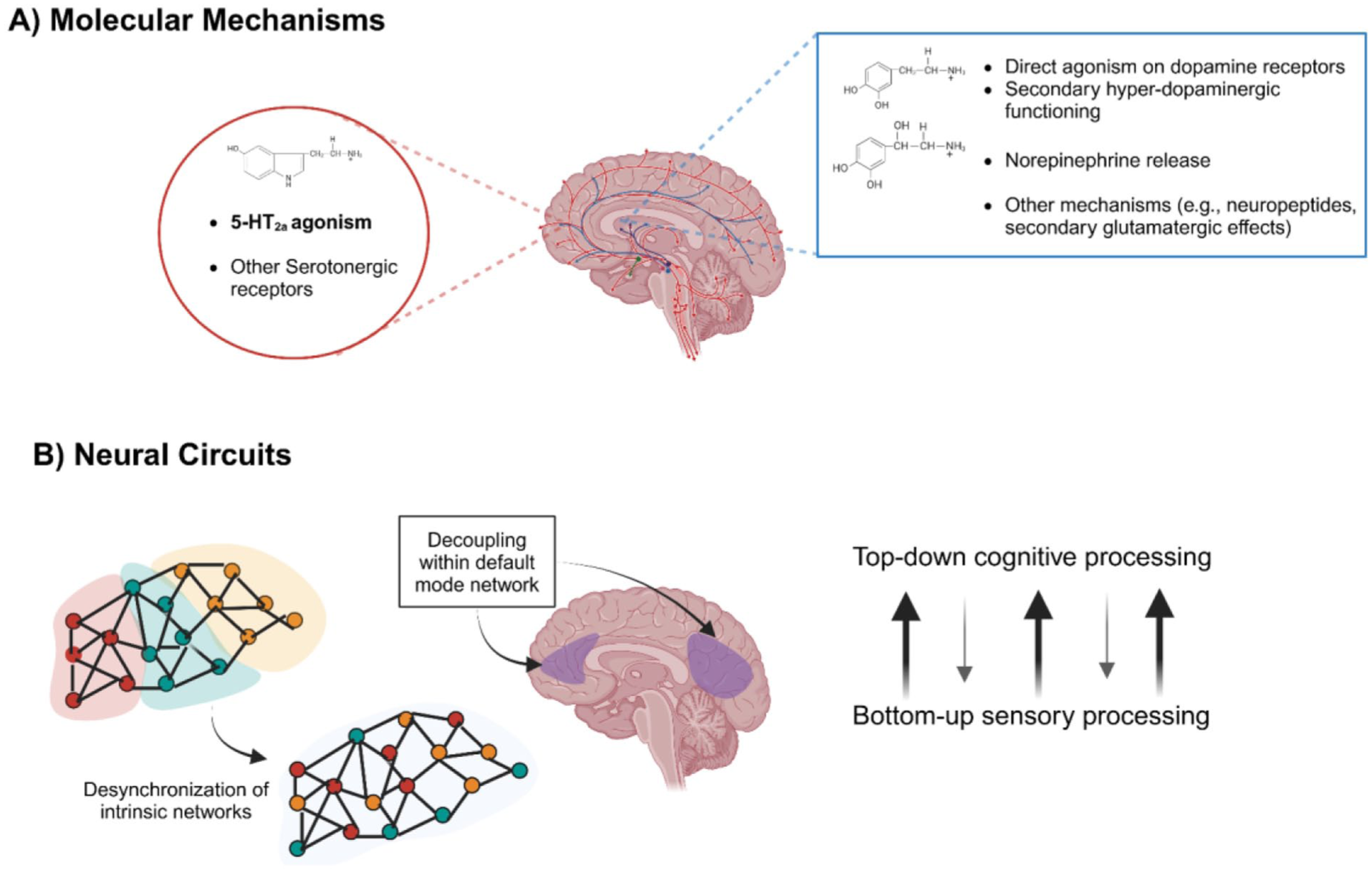
Brain-based mechanisms underlying psychedelic action and psychosis risk. Putative neural mechanisms of psychedelic action are displayed. Differences exist across core psychedelic agents in their individual molecular mechanisms. However, collectively, psychedelic agents work through 5-HT2A agonism and action on a variety of other serotonergic receptors (a). LSD and mescaline also directly or indirectly act as dopamine agonists, binding to a range of dopaminergic receptors and on the norepinephrine system, leading to its release. Downstream effects include action of neuropeptides, such as BDNF and oxytocin, and glutamatergic action. At the level of neural circuitry (b), psychedelic effects result in widespread dysconnectivity and reduced modularity of functional networks, with prominent effects within the default mode network, which is linked with one’s sense of self and internal processing. Likely these large-scale effects result in a net decrease in top-down cognitive processing relative to the processing of bottom-up limbic and perceptual input. Many of these findings, representing acute effects of psychedelics, overlap with pathophysiologic findings of SSDs.
An important consideration is whether 5-HT2A agonism is also a putative mechanism underlying either the psychotic effects of psychedelic use or the manifestations of SSDs. Dating back to 1956, Manfred Bleuler disagreed that LSD induces a psychotomimetic state and cautioned against the simplified psychotomimetic psychedelic model for schizophrenia (Bleuler, 2009). Many antipsychotic drugs, especially second-generation agents, demonstrate antagonism at 5-HT2A receptors in addition to their canonical dopamine D2 receptor antagonism (Kapur and Mamo, 2003). Risperidone, for example, a drug with considerable 5-HT2A receptor activity, attenuates the effects of psilocybin relative to haloperidol (Vollenweider et al., 1998). However, when examining SSDs, data do not support a central role for 5-HT2A receptors. Postmortem studies examining changes in the distribution of 5-HT2A receptors in SSDs are equivocal: some studies report a decrease in these receptors, while others show no significant changes (García-Bea et al., 2019; Muguruza et al., 2013; Selvaraj et al., 2014). In addition, 5-HT2A antagonists, putative antipsychotic treatments, have not demonstrated a significant reduction in psychosis in people with schizophrenia to date, but have been beneficial for non-psychotic illness domains such as negative symptoms (Bugarski-Kirola et al., 2022; Davis et al., 2021b; Romeo et al., 2023).
Thus, the psychotic manifestations of SSDs, which are classically linked to dopaminergic or glutamatergic systems, cannot singularly be distilled to 5-HT2A receptor-like psychedelic effects (McCutcheon et al., 2020). It also remains undetermined whether the more psychotic manifestations of psychedelic use, described above, are also linked to 5-HT2A receptor action, or whether other systems are involved. Pharmacologic studies of psychedelic compounds demonstrate that their interactions are more diverse and robust than simply targeting the 5-HT2A receptor. For example, LSD exhibits action on a wide range of serotonergic receptors that have a broad distribution across the brain, in addition to agonism of a range of dopamine receptors at moderate to high doses (e.g., D1, D2, D3, and D4), and noradrenergic receptors (Kroeze et al., 2015; Marona-Lewicka et al., 2005). A similar diverse array of actions is observed for mescaline and DMT, while a diverse pharmacologic profile is also implicated for psilocybin (Pierce and Peroutka, 1989; Ray, 2010; Vamvakopoulou et al., 2023; Vollenweider et al., 1999). Broadly, psychedelic compounds have a wide range of molecular effects, from interactions with major neurotransmitter systems to the release of neuropeptides such as BDNF and oxytocin (Holze et al., 2022; Kirkpatrick et al., 2014; Moliner et al., 2023). It is also important to note that agonism of the 5-HT2A receptor is associated with downstream glutamatergic activity, including activation of glutamatergic mGlu 2/3 receptors, which may trigger overlapping mechanisms with psychotic states of SSDs (Wischhof and Koch, 2016).
The psychotic effects of psychedelics and associated risk for psychotic relapse in people who have schizophrenia may result from non-5-HT2A receptor action of these drug systems that are implicated in SSDs. As novel compounds with 5-HT2A receptor action are developed, it may be possible to leverage potential neuroplastic action without detrimental effects on non-serotonergic systems (e.g., dopamine and norepinephrine), inducing a physiologic effect without the psychedelic experience. Critically, ongoing antipsychotic therapy with adequate D2-receptor blockade and coinciding symptomatic stability is likely to counteract some elements of psychedelic experiences, providing a safer background for any potential therapeutic trial. However, this remains theoretical, holding promise for non-psychotic illness domains of schizophrenia, such as negative symptoms, coinciding with the low-dose mescaline studies described above.
Neural circuitry
At the level of large-scale neural circuitry, 5-HT2A receptors are largely expressed in the neocortex, and to a lesser extent, in the hippocampus and subcortical regions, including the thalamus and basal ganglia (Burnet et al., 1995; Carhart-Harris and Nutt, 2017; Gross-Isseroff et al., 1990; Hall et al., 2000). Excitability of 5-HT2A induces brain-wide changes from the prefrontal cortex through the visual system and subcortical regions (Kwan et al., 2022). Thus, it is likely that psychedelics have a broad effect on neural systems, which is supported by an array of neuroimaging findings. Early positron emission tomography and neurometabolic studies of psilocybin and mescaline demonstrated frontal and thalamocortical metabolic alterations accompanied by transient psychosis-like phenomenology, reinforcing the utility of these compounds as experimental models of altered cortical—subcortical integration rather than direct analogues of schizophrenia (Hermle et al., 1992; Vollenweider et al., 1997).
Recent neuroimaging work focused on psychedelic effects, relative to placebo and other compounds, has demonstrated that psychedelics induce a widespread desynchronization of the brain’s intrinsic functional architecture, partly corresponding with the distribution of 5-HT2A receptors (Figure 2; Carhart-Harris et al., 2016; Delli Pizzi et al., 2023; Preller et al., 2017, 2018, 2020; Siegel et al., 2024; Soares et al., 2024; Tagliazucchi et al., 2016; Tolle et al., 2024). This includes prominent abnormalities in functional interactions and oscillatory power of the default mode network (DMN) with regions such as the hippocampus, possibly underlying neuroplastic effects that may link with longer-lasting psychedelic-induced phenomena (Muthukumaraswamy et al., 2013; Siegel et al., 2024). The DMN is compelling in the mechanism of psychedelics, given its established role in self-reflection and internal monitoring (Davey et al., 2016). Gross abnormalities within the DMN and between the DMN, prefrontal, and somatosensory networks have been reported during use of psilocybin, LSD, and ayahuasca (Carhart-Harris et al., 2012, 2016; Palhano-Fontes et al., 2015; Stoliker et al., 2023).
Notably, increased DMN connectivity with task-active executive networks with less network segregation (less anticorrelation) between the two, in addition to global desynchronization, has been implicated in the pathophysiology of schizophrenia and as a critical component of antipsychotic response (Maximo et al., 2021; Sambataro et al., 2010; Sheffield and Barch, 2016; Uhlhaas, 2013; Unschuld et al., 2014). In separate studies, brain-wide changes in functional connectivity have been linked with sensory circuits, including hyperconnectivity of thalamic circuitry during the acute effects of LSD (Müller et al., 2017; Preller et al., 2020). Increased thalamocortical connectivity with somatosensory regions has emerged in recent years as a pathophysiological marker of schizophrenia (Anticevic et al., 2014; Woodward and Heckers, 2016). Directly addressing similarities and differences between psychedelic and psychotic states, Avram and colleagues demonstrated that LSD induces thalamocortical dysconnectivity patterns that partially overlap with, but remain distinct from, those observed in schizophrenia, particularly when contrasted with dopaminergic challenge, highlighting both shared circuit-level perturbations and important mechanistic divergences (Avram et al., 2022). Coinciding with these findings, a putative model for psychedelic effects on neural circuitry, the relaxed beliefs under psychedelics, and the anarchic brain model (i.e., the relaxed beliefs under psychedelics (REBUS) model), proposes that disrupted intrinsic functioning across the brain deemphasizes “top-down” associative control over “bottom-up” sensory and limbic signaling (Carhart-Harris and Friston, 2019; Kwan et al., 2022; Vollenweider and Geyer, 2001). Links between these findings and proposed models with the schizophrenia neuroimaging literature, however, remain speculative and have not been directly examined.
Much like the comparative phenomenological analyses above, discussion of the brain-based models of psychedelics and SSDs shows broad similarities and yet calls for more granular analyses to clarify uncertainties and potential key differences (see also summary in Table 1). We now turn to studies that speak to the potential adverse, psychosis-triggering effects of psychedelics on SSDs to explore how available clinical evidence contributes to the phenomenological and neurophysiological nuances illustrated above.
The effects of psychedelics on SSDs
Focusing on whether negative reactions of mescaline use approximate psychosis in SSDs, Hoch et al. (1952) observed that mescaline induced anxiety in those with a schizophrenia diagnosis and paranoia in both those with and without schizophrenia. Denber and Merlis (1955a) investigated the impact of mescaline on individuals with schizophrenia to clarify whether psychedelic-induced states could serve as experimental models of psychosis and to probe how electroconvulsive therapy (ECT) altered the underlying structure of the illness. They reasoned that because mescaline induces a psychotomimetic state, its administration before and after ECT could reveal whether the treatment produced qualitative changes in psychotic processes or merely quantitative symptom reductions, with the possibility that mescaline might even function as an objective prognostic test. In a series of studies, they administered mescaline to patients undergoing ECT and observed varied clinical responses, including reactivation of psychotic symptoms and symptom exacerbation, concluding that mescaline could induce a state “indistinguishable from the schizophrenic state.”
Related work examined electroencephalographic patterns during administration of chlorpromazine following a mescaline challenge, finding antagonistic interactions that supported the use of psychedelic-induced psychosis as a mechanistic model for research (Merlis and Denber, 1956). Finally, they explored the combined use of mescaline and chlorpromazine, reporting mixed outcomes that pointed both to the theoretical promise of psychedelic-based frameworks and to the risk that mescaline could worsen psychotic illness (Denber and Merlis, 1955b).
Research on LSD use in individuals with SSDs in the 1950s and 1960s echoes the complex therapeutic potential and symptomatic exacerbation illustrated by Denber and Merlis’s mescaline-chlorpromazine work. Stoll (1947) first reported that LSD is well-tolerated in people with schizophrenia and introduced the idea that lower doses of LSD might facilitate psychotherapeutic processes. In similar studies across 2 decades, LSD was administered to individuals with schizophrenia, noting a variety of effects, including catatonia, more robust expressions of emotion, greater engagement with environmental stimuli, and facilitation of conversation for psychotherapeutic processes, particularly with lower doses (Busch and Johnson, 1950; Condrau, 1949; Katzenelbogen and Fang, 1953; Shirvaikar and Kelkar, 1966). Several of these studies highlight both a differential response to LSD in people with schizophrenia between lower and higher doses, or an overall greater amount of variability in dose needed to achieve psychedelic effects (20–130 μg; Busch and Johnson, 1950; Cline and Freeman, 1956; Katzenelbogen and Fang, 1953; Stoll, 1947). While these LSD studies largely focus on the link with psychosis while beginning to examine dosing, it is important to note that they were open-label, observational studies, without rigorous and quantitative clinical measures, strict dosing paradigms, or systematic descriptions of adverse effects.
In contrast to findings illustrating potential therapeutic benefits of LSD, other studies highlight acute risks for psychotic illness associated with LSD. In a large cohort of individuals with serious mental illness, including schizophrenia, Fink et al. (1966) examined the effects of LSD administration. They report an estimated 2% rate of prolonged presentations of psychosis mirroring prior episodes of their established illness. Other studies suggest that more prolonged psychotic symptoms and more significant destabilization are present in individuals at higher risk for serious mental illness (Anastasopoulos and Photiades, 1962; Vardy and Kay, 1983).
Moreover, exposure to LSD in people with relatives who have a diagnosis of schizophrenia is more likely to lead to the development of psychotic symptoms (e.g., paranoid delusions, derealization; Anastasopoulos and Photiades, 1962; Vardy and Kay, 1983). Other studies have proposed leveraging psychotogenic properties of LSD for diagnostic confirmation, given differences in manifestations during intoxication between patient groups and control participants, or symptom provocation, to induce treatment responsiveness in refractory schizophrenia (Itil et al., 1969; Sedman and Kenna, 1965).
Overall, findings from studies of LSD paint a complex relationship with SSDs. As reviewed above, dosing of LSD further obfuscates this relationship, with higher doses more likely to induce psychotic states in healthy individuals and exacerbate existing psychotic illness (Cline and Freeman, 1956; De Gregorio et al., 2016; Kuramochi and Takahashi, 1964; Sandison et al., 1954). Such findings coincide with the broader recoil from psychedelic use that led to the prohibition and reclassification of LSD as a Schedule I drug in 1970 (Cohen, 1966; Nichols, 2018; Nichols and Walter, 2021). A follow-up study from Denmark characterized outcomes in a cohort of 151 individuals with preexisting psychiatric illness, including both psychotic and non-psychotic illness, who received LSD in early trials, and subsequently underwent a tribunal to receive compensation for damages due to psychedelic exposure (Larsen, 2017). The study found that the short and long-term effects of exposure to LSD are dependent on the duration and dose of psychedelic exposure. Thus, current recommendations support the risk of prolonged and delayed psychotic symptoms to LSD use, framing exposure as a risk factor that interacts with a background propensity for SSDs (Abraham and Aldridge, 1993; Nichols, 2018; Paparelli et al., 2011).
Moreover, the current “psychedelic renaissance” has produced high-profile trials investigating psilocybin for conditions such as end-of-life distress, major depressive disorder, anxiety, alcohol use disorder, and obsessive-compulsive disorder (Bogenschutz et al., 2022; Carhart-Harris et al., 2021; Davis et al., 2021a; Goodwin et al., 2022; Griffiths et al., 2016; Moreno et al., 2006; Raison et al., 2023; Ross et al., 2016). These modern trials report groundbreaking findings and benefit from improved methodological rigor over earlier studies, particularly regarding randomization, blinding, and outcome measurement. However, based on lessons from earlier research, modern trials uniformly exclude individuals with a personal or family history of psychotic disorders (e.g., schizophrenia, bipolar disorder, and schizoaffective disorder) to mitigate risk. This conservative approach reflects concerns about the potential for psychedelics to induce or exacerbate psychotic symptoms—risks that remain poorly quantified because of inherent limitations in available data.
Recent data support this caution. Longitudinal analyses suggest that associations between psychedelic use and psychotic symptoms are conditional rather than uniform, with differential patterns emerging as a function of psychiatric history: symptom increases have been observed in individuals with certain familial risk profiles, including bipolar disorder, whereas symptom reductions have been reported among those with a personal, but not familial, history of psychotic disorders (Honk et al., 2024). Survey-based findings similarly indicate elevated psychotic symptoms following psychedelic use among individuals with a family history of psychotic or bipolar disorders, alongside contrasting patterns in those without such histories, underscoring heterogeneity in vulnerability rather than a single risk trajectory (Simonsson et al., 2023). A recent qualitative study likewise presents contrasting results, with use resulting in increased insight into positive symptoms in some individuals, but also hospitalizations in the case of high dosages and/or polysubstance use (Dourron et al., 2025). However, one case study on a patient with schizoaffective disorder, whose positive symptoms were in remission, showed improvement in negative symptoms following a session of psilocybin-based psychedelic-assisted therapy (Sabé et al., 2025). Together, these findings highlight important nuances that remain incompletely resolved, particularly regarding which dimensions of risk, exposure, and context drive adverse versus neutral or attenuating outcomes. Finally, emergency room visits linked to psychedelic use have, in some cases, preceded the later development of SSDs (Myran et al., 2024).
In contrast, clinical trials involving carefully screened participants have not observed new cases of psychotic illness following psilocybin treatment, validating the importance of rigorous selection criteria (Studerus et al., 2011). However, individuals with existing psychotic disorders or heightened vulnerability, particularly during sensitive neurodevelopmental periods, remain at significant risk of psychotic relapse or sequelae following psychedelic exposure (Starzer et al., 2018). Given the current lack of robust quantification and detailed characterization of these risks, further research is critical. These uncertainties have important implications for the broader generalization of psychedelics, such as psilocybin, as therapeutic agents in psychiatry.
Other work has demonstrated the potential for MDMA and ibogaine to be effective treatments for post-traumatic stress disorder (PTSD), a condition with limited existing psychopharmacologic options (Cherian et al., 2024; Mitchell et al., 2023). Psychotic illness in relation to other psychedelic compounds, such as ibogaine, remains at the level of case reports and requires further investigation (Houenou et al., 2011).
Finally, emerging evidence has prompted reconsideration of psychedelic applications in SSDs. The prosocial properties of MDMA and its neuroplasticity-promoting effects have generated interest in treating negative symptoms and social deficits (Arnovitz et al., 2022; Wolf et al., 2023). In addition, given psychedelics’ efficacy for treatment-resistant depression in other populations, they may offer promise for co-occurring depression, a disabling feature affecting 30%–70% of individuals with SSDs that responds poorly to conventional treatments (Buckley et al., 2009; Siris, 2000; Upthegrove et al., 2016) However, any therapeutic exploration requires careful risk stratification, conservative dosing, and restriction to clinically stable individuals, as emphasized throughout this review.
Clinical and empirical implications
In the historical, phenomenological, and mechanistic work described above, we highlight an inextricable relationship between psychedelic compounds and SSDs. Early research linking psychedelics to SSDs centered on mescaline, aligning with Kraepelin’s pharmacologic model of psychosis. The discovery of LSD shifted the focus of psychedelic studies, but progress stalled following its prohibition and reclassification in 1970 amid broader cultural backlash (Nichols and Walter, 2021). Phenomenologically, while psychedelic experiences and SSDs do show similar alterations in world experience (i.e., breakdown of conventional meanings in percepts, objects disclosing revelatory insights) and self-experience (i.e., changes in the boundaries of the self), this overlap lacks rigorous and direct comparison. Proposed mechanisms underlying these similarities may extend beyond the serotonin system to include drug-specific action on other neurotransmitter systems (e.g., catecholaminergic), reflected in circuit-level neural pathways. Psychedelic compounds may be reclassified and made available for their medicinal properties, yet potential harms are well documented, and modern studies do not factor in serious mental illness, including SSDs. Thus, a conflict is set up that must be resolved with rigorous evidence and appropriate regulation (Smith and Appelbaum, 2022). Based on the existing literature and the emerging findings from modern therapeutic trials, the following conclusions and recommendations are presented.
Psychedelics, preexisting SSDs, and psychosis risk
Evidence, mostly from observational and open-label studies of LSD and mescaline, suggests psychedelics can exacerbate pre-existing psychotic illness (Bowers, 1972; Dewhurst and Hatrick, 1970; Abraham and Aldridge, 1993; Smart and Bateman, 1967; Vardy and Kay, 1983). However, the magnitude of this risk remains unclear due to the limitations of available historical data, including heterogeneous samples, dosing, and ascertainment (Strassman, 1984; Sabé et al., 2024). For other compounds, risk is largely putative and sparse. Rigorous trials or large-scale epidemiologic studies are needed to better quantify this risk (Hinkle et al., 2024; Sabé et al., 2024).
Psychedelics likely trigger in the setting of risk, but do not cause SSDs (Paparelli et al., 2011; Sabé et al., 2024). It is critical to distinguish risk in individuals with preexisting SSDs from the potential for psychedelics to induce de novo chronic psychotic illness. Substantial evidence for the latter is lacking. Persistent psychosis after psychedelic use is documented but remains unquantified and may reflect the unmasking of underlying vulnerability rather than a true delayed reaction (Sabé et al., 2024; Vardy and Kay, 1983). Psychedelics, such as LSD and mescaline, are not pure 5-HT2A agonists; thus, depending on the drug and dose (e.g., LSD), dopamine or norepinephrine receptor binding may also contribute to psychosis risk (Marona-Lewicka et al., 2005). Meanwhile, compounds such as psilocybin and DMT do not exhibit direct dopaminergic activity, illustrating possible heterogeneity in risk among psychedelics.
Phenomenological overlap between psychedelics and SSDs
Psychedelics are not uniformly psychotomimetic, but their effects share pharmacologic and phenomenological features with SSDs. At a broad level, both those experiences induced by classic psychedelics and SSDs involve a breakdown in the everyday and conventional meaning of percepts. However, current evidence suggests that important differences in self- and world experience may exist. More granular qualitative research, drawing on phenomenologically informed interview protocols (Parnas et al., 2005; Sass et al., 2017), is necessary to contribute to our understanding of genuine similarities and differences. Such inquiry can also guide investigation into the neural basis of those experiences respectively characteristic of (sub-)psychotic and psychedelic states.
For example, altered connectivity of the DMN has been proposed as operative in the dissolution of ego boundaries during the acute effects of classic psychedelics, and in SSDs (Carhart-Harris et al., 2012; Feyaerts and Sass, 2024; Nelson et al., 2014). Above, we suggested that a potential difference between psychedelic and psychotic forms of this experience might be that the latter is characterized by an overall unstable sense of self (diminished self-presence). Reduced activity in the temporoparietal junction of the left hemisphere has been proposed as a neural correlate for anomalies of bodily awareness, agency, and self-other differentiation (Salgado-Pineda et al., 2022), and thus may be a candidate for a neural basis contributing to disturbances in self-experience distinct to SSDs. Further neurophenomenological inquiry should also rule out alternative explanations for this apparent overlap in experience—for example, that the transformations of self-experience underlying dissolution of ego boundaries in both psychedelic and psychotic states are one and the same experience, but are interpreted differently and carry different emotional valences (elating versus threatening).
Psychedelics as therapeutic agents in SSDs
Based on the evidence reviewed above, psychedelic compounds may have a potential role in the treatment of SSDs. However, this possibility requires rigorous empirical validation and careful clinical safeguards. Early conceptual and preliminary studies suggest that low-dose, low-intensity regimens, administered under tightly controlled conditions, may mitigate risks while still engaging mechanisms relevant to symptom improvement. Any future clinical exploration will require conservative dosing strategies, stringent patient selection, and restriction to individuals with stable illness courses and well-defined clinical characteristics. Negative symptoms, social withdrawal, and deficits in social cognition appear to be the most rational therapeutic targets, particularly when psychedelic administration is combined with structured psychosocial interventions such as social skills training or cognitive remediation. Observational evidence suggesting that MDMA may offer therapeutic benefit, particularly for negative symptoms, has motivated at least one ongoing clinical trial in schizophrenia (Bershad, 2025). However, MDMA may be a suboptimal candidate for individuals with SSDs, given its substantial sympathomimetic and serotonergic load, which raises safety concerns in vulnerable populations (Hysek et al., 2014; Liechti, 2014; Parrott, 2013). Its effects are likely dose- and receptor-dependent, and available evidence suggests more limited antidepressant efficacy relative to classic serotonergic psychedelics (Rucker et al., 2016). Accordingly, any future research will require conservative dosing, rigorous safety monitoring, and strictly controlled study designs.
Relatedly, co-occurring depression, which represents an often overlooked and disabling element of SSDs, is another core clinical target for psychedelic interventions. Given depression’s strong associations with functional impairment and suicide risk, it constitutes a primary therapeutic target alongside negative symptoms and should be explicitly prioritized in evaluations of novel interventions for SSDs (Buckley et al., 2009; Siris, 2000; Upthegrove et al., 2016).
Mechanistically, ongoing antipsychotic therapy is likely to mitigate psychedelic effects via multiple pathways. For instance, 5-HT2A antagonism (e.g., ketanserin, second-generation antipsychotics) reverses core acute effects of psilocybin and LSD, while D2 receptor blockade (e.g., haloperidol) dampens derealization and boundlessness. Trial designs that combine low doses with antipsychotic continuation, focus on substances with less direct effects on dopamine (e.g., LSD, mescaline), and include structured psychosocial interventions could explicitly test whether clinically meaningful gains (e.g., in negative symptoms, social withdrawal, and social cognition) can be achieved without reliance on intense hallucinogenic or mystical experiences. A departure from conventional paradigms that emphasize profound hallucinogenic or “mystical” experiences, and instead an emphasis on lower-intensity approaches aimed at supporting engagement, affective flexibility, and neuroplasticity, may be more appropriate but remains an area for future research.
Cohort limitations and ethical considerations
Recent psychedelic trials enroll homogeneous populations, excluding individuals with SSDs, obviating the quantification of risk for psychosis (Bogenschutz et al., 2022; Carhart-Harris et al., 2021; Davis et al., 2021a; Goodwin et al., 2022; Griffiths et al., 2016; Moreno et al., 2006; Raison et al., 2023; Ross et al., 2016). Widespread therapeutic use could accelerate or exacerbate psychosis in vulnerable individuals, and it remains unclear how such risks will be systematically measured or how emergent psychotic symptoms will be managed (Carhart-Harris and Goodwin, 2017; Johnson et al., 2008). Meanwhile, in-depth interviews with experts suggest consensus that future studies should carefully examine potential clinical applications of psychedelics in individuals with psychosis (La Torre et al., 2022). Accordingly, caution is warranted as therapeutic applications expand, with an emphasis on rigorous informed consent, conservative dosing, and tightly controlled study designs, particularly in SSD populations (Nutt et al., 2020; Reiff et al., 2020). Regulatory progress will depend on the field’s ability to explicitly address these risks. While current clinical trials increasingly stratify mental illness and have opened new treatment avenues for several psychiatric conditions, individuals with SSDs have yet to experience a comparable therapeutic renaissance.
Conclusion
The link between psychedelics and SSDs is complex and remains unresolved. Early studies emphasized phenomenological overlap and suggested mechanistic connections. Modern research, focused on depression and PTSD, has excluded SSDs, leaving risks poorly defined. Evidence indicates psychedelics can worsen psychosis, yet low-dose, carefully controlled approaches with certain compounds may hold promise for targeting negative symptoms, social withdrawal, and depression. Future work, as psychedelics become mainstream, must use conservative dosing, strict selection, and psychosocial support, while ensuring ethical safeguards and informed consent. Research that utilizes advances in the phenomenological understanding of SSDs should also guide further research into experiential and neurobiological overlap. Rather than excluding SSDs outright, cautious and mechanistically guided inclusion is critical for examining whether compounds that are less likely to cause illness exacerbation can be safely used in this population.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.