
Abstract
Background:
Psychedelic microdosing—repeated sub-perceptual doses of lysergic acid diethylamide (LSD) or psilocybin—has attracted scientific interest as a potential mood and cognitive intervention. The evidence base remains methodologically heterogeneous and vulnerable to expectancy bias.
Methods:
We conducted an umbrella review with narrative synthesis following Joanna Briggs Institute guidance and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 standards (International Prospective Register of Systematic Reviews [PROSPERO]: 2020 standards (PROSPERO: CRD420251077340). Six databases were searched through February 2026. Eligible studies were systematic reviews and/or meta-analyses examining microdosing effects (⩽20 μg LSD or ⩽3 mg psilocybin per session) on mood or cognitive outcomes in adults. Quality was appraised with A Measurement Tool to Assess Systematic Reviews-2; primary-study overlap was quantified via corrected covered area (CCA).
Results:
Three meta-analyses met quantitative criteria, drawing on 14 studies (13 unique samples, N = 1614); three reviews contributed to narrative synthesis. Primary-study overlap was very high (CCA = 0.29). The sole significant pooled effect was a small decrease in cognitive control (d = −0.34, 95% CI: −0.62 to −0.06); all other domains were non-significant. No eligible meta-analysis provided pooled mood-outcome effect sizes within the microdose threshold; narrative evidence indicates that self-reported mood benefits are largely attenuated under placebo-controlled conditions. Short-term tolerability was acceptable, though cardiovascular signals and long-term risks via 5-HT2B activation remain uncharacterized.
Conclusions:
Current evidence does not support cognitive enhancement through microdosing; the only consistent controlled finding runs counter to popular claims: microdosing was associated with a small but reliable impairment of cognitive control. Observed mood benefits are not replicated under blinded conditions, consistent with expectancy-driven responding. Adequately powered, preregistered, expectancy-controlled trials are required before clinical recommendations can be made.
Keywords
Introduction
Psychedelic microdosing refers to the regular, repeated use of very low doses of classic psychedelics—most commonly LSD and psilocybin—typically around 1/10 to 1/20 of a standard dose (Johnstad, 2018; Polito and Stevenson, 2019). These subthreshold doses are generally intended to avoid a full psychedelic “trip” while remaining compatible with daily functioning (Lea et al., 2020; Polito and Stevenson, 2019). Observational studies frequently report perceived improvements in mood, anxiety, focus, and creativity among users (Anderson et al., 2019; Hutten et al., 2019; Lea et al., 2020). Mechanistic accounts often emphasize serotonergic signaling—especially 5-HT2A-related pathways—and potential links to neuroplasticity-relevant processes (Carhart-Harris and Nutt, 2017; Nichols, 2016).
However, the early evidence base is dominated by observational and self-report designs with important inferential limitations (Johnstad, 2018; Polito and Liknaitzky, 2022). Expectancy and placebo effects represent a pervasive methodological challenge in this literature, one that is not resolved by the adoption of placebo-controlled designs: given that psychedelic effects are subjectively distinctive, participant blinding is difficult to maintain even in randomized controlled trials (RCTs), and expectancy inflation may be particularly pronounced in microdosing research where perceptual cues are subtle and participant beliefs are strong (Szigeti et al., 2021). Placebo-controlled and self-blinding studies suggest that many reported benefits are small, mixed, or not clearly separable from expectancy effects (Cavanna et al., 2022; Szigeti et al., 2021). Thus, whether microdosing produces robust pharmacological benefits beyond expectancy-enhanced responses remains debated (Polito et al., 2024).
Recent evidence syntheses differ considerably not only in focus—with some emphasizing mood and mental-health outcomes and others prioritizing cognition, acute effects, or safety (Lo et al., 2024; Polito and Liknaitzky, 2022; Polito et al., 2024)—but also in the methodological approaches they adopt. Thus umbrella-review approach is, therefore, appropriate for integrating review-level evidence, mapping overlap, and appraising methodological quality within a unified framework (Aromataris et al., 2015).
In this regard, we aimed to systematically synthesize the heterogeneous findings in the microdosing literature and present the quality of evidence within an unbiased framework.
Methods
Review design and protocol registration
This study used a two-component mixed-methods design integrating (1) a quantitative umbrella review of eligible meta-analyses reporting microdose-specific effect sizes and (2) a systematic narrative synthesis of methodologically relevant reviews that did not meet quantitative inclusion thresholds but provide essential interpretive context. The review was conducted in line with Joanna Briggs Institute umbrella-review guidance and reported according to PRISMA 2020 standards (Aromataris et al., 2015; Page et al., 2021). The protocol was prospectively registered in PROSPERO (CRD420251077340).
Eligibility criteria
Quantitative umbrella component
Inclusion criteria were: (1) systematic reviews and/or meta-analyses examining effects of classical psychedelics at microdose-range doses (⩽20 µg LSD-equivalent; see Dose Normalization); (2) at least one extractable quantitative outcome in mood (depression, anxiety, and well-being) or cognitive function (attention, memory, executive functioning, and creativity); (3) clinical or healthy adult populations; and (4) a systematic search with at least one reportable pooled effect size. Exclusion criteria were: exclusive full-dose (macrodose) data without separable microdose subgroup; preclinical focus; narrative/scoping design; and non-English publication.
Narrative synthesis component
Reviews meeting all criteria except pooled effect-size reporting (e.g., systematic narrative reviews, qualitative meta-syntheses, and methodological appraisals) were included in narrative synthesis.
Dose normalization
The ⩽20 µg LSD-equivalent threshold was operationalized as follows. For LSD, eligible doses were those explicitly reported as ⩽20 µg per session (e.g., 5, 10, 13, 20 µg); studies reporting 25 µg or above were excluded from quantitative synthesis. For psilocybin, a pragmatic operational boundary of 1 mg psilocybin = 10–15 µg LSD was used solely as an eligibility screening rule, corresponding approximately to 1–3 mg psilocybin under the present framework. This conversion was applied as an operational criterion for study selection only and does not imply true pharmacological equivalence between LSD and psilocybin, which differ in receptor binding profiles, potency, and duration of action. No eligible studies were identified for other classical psychedelics; a priori eligibility thresholds for dimethyltryptamine (DMT; ⩽5 mg vaporized, or ayahuasca ⩽0.1 mg/kg DMT-equivalent) and mescaline (⩽50 mg) were pre-specified in the registered protocol but are not reported further given the absence of qualifying reviews.
Information sources and search strategy
PubMed/MEDLINE, Embase, PsycINFO, Web of Science, Scopus, and the Cochrane Library were searched using Boolean combinations of “microdose*,” “low dose,” “psychedelic*,” “LSD,” “lysergic acid diethylamide,” “psilocybin,” “serotonin 5-HT2A,” “meta-analysis,” and “systematic review.” Initial searches were completed in February 2026 to capture newly published studies. Records identified through this update are reported under “studies identified through other methods” in the PRISMA flow diagram.
Study selection
Title/abstract screening and full-text eligibility assessment were performed independently by two reviewers (YÖ and BCÖ). Full-text disagreements were resolved through blinded adjudication by two independent child and adolescent psychiatry specialists (UU and HB) who did not meet authorship criteria and were blinded to each other’s assessments.
Study overlap
Overlap of primary studies across included meta-analyses was assessed by systematic cross-referencing of included-study lists. Corrected covered area (CCA) was calculated as proposed by Pieper et al. (2014):

where
Data extraction
Data extraction was performed independently by both authors (YÖ and BCÖ) using a pre-specified form. Extracted items were: number and design of included primary studies (RCT vs observational), total sample size and demographics, substance and dosage regimen, mood outcomes (depression, anxiety, and well-being), cognitive outcomes (attention, memory, executive functioning, and creativity), effect sizes (Hedges’ g and Cohen’s d), heterogeneity indices (I2, τ2), prediction intervals (if reported), and adverse-event profile.
Data synthesis
Effect sizes were extracted and tabulated at the meta-analytic level. Exploratory meta-regression analyses of dose-by-population interactions were reported descriptively. Prediction intervals were extracted where reported; intervals crossing the null were interpreted as indicating that future well-controlled studies may plausibly observe no effect.
For the narrative component, findings were synthesized thematically across included reviews by consistency of evidence, methodological quality of the underlying evidence base, and convergence/divergence with the quantitative umbrella findings.
Results
Study selection
Database searches across six electronic sources (PubMed/MEDLINE, Embase, PsycINFO, Web of Science, Scopus, and the Cochrane Library), updated through February 2026, identified 2,024 records. Following deduplication, 348 records underwent title and abstract screening; 326 were excluded for irrelevance. Twenty-two full-text articles were assessed for eligibility; 16 were excluded. Three systematic reviews and meta-analyses met criteria for the quantitative umbrella component; three additional reviews met criteria for the narrative synthesis component. A detailed overview of the identification, screening, and eligibility assessment stages is presented in the PRISMA flow diagram (Figure 1).
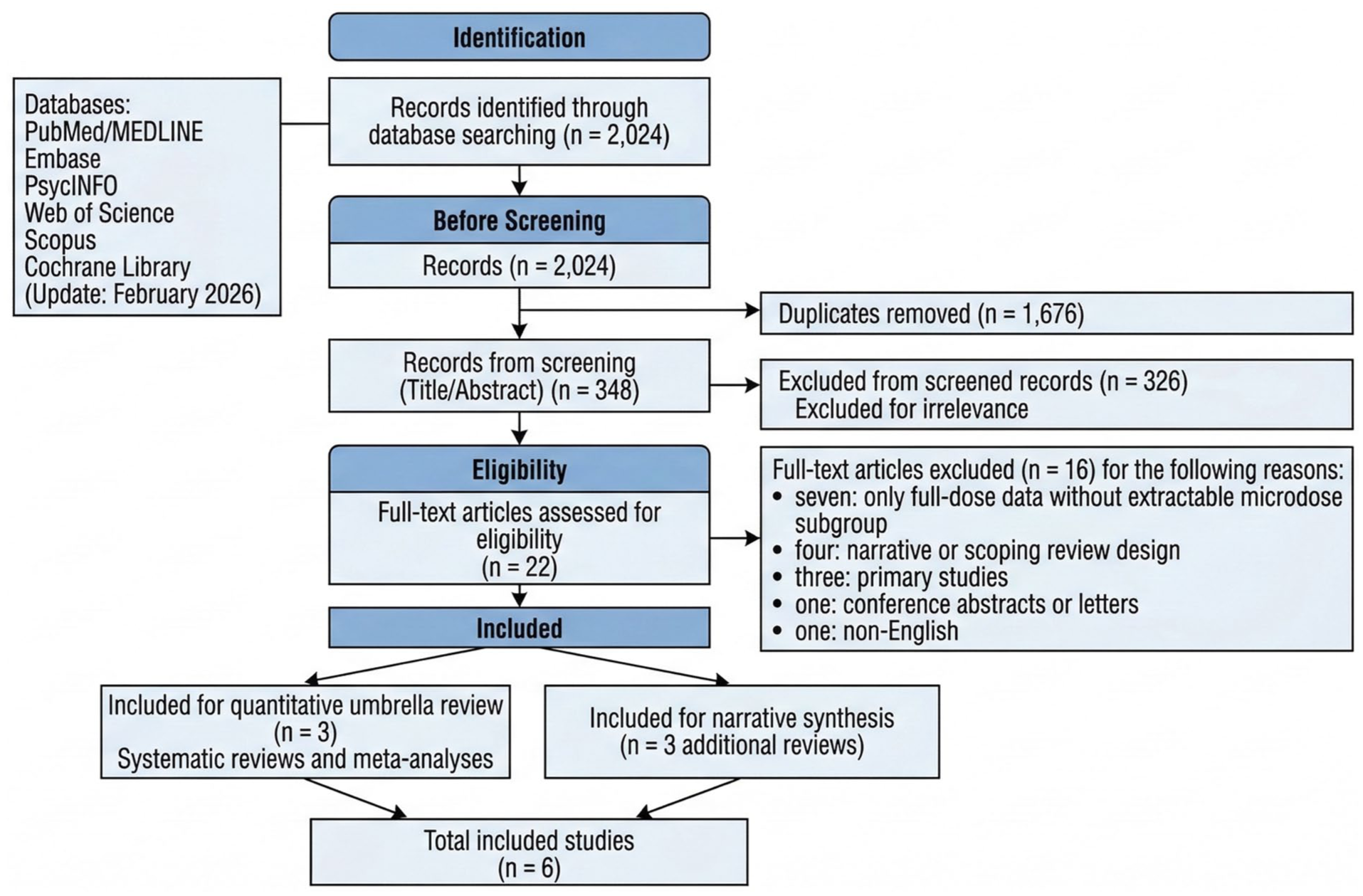
PRISMA 2020 flow diagram of the study selection process. The systematic search, updated through February 2026, identified 2024 records across 6 electronic databases. After removal of duplicates and title–abstract screening, 22 full-text articles were assessed for eligibility. Six reviews met inclusion criteria: three systematic reviews with meta-analyses contributing to the quantitative umbrella synthesis and three additional reviews retained for narrative synthesis to provide methodological and interpretive context. Most exclusions occurred because psilocybin doses exceeded the predefined microdosing threshold (>3 mg) or because studies did not report extractable results for microdose-specific subgroups.
Of the 16 excluded full-text articles, the majority were excluded for reasons unrelated to study outcomes or directionality of findings specifically, seven were excluded for containing exclusively full-dose data without an extractable microdose subgroup, four for lacking a systematic search strategy, three for being primary rather than review-level studies, one for being a conference abstract or letter, and one for non-English publication. No excluded review was identified as reporting systematically more positive or negative microdosing outcomes than those included; exclusions reflected pre-specified design and eligibility criteria rather than result-based selection. Accordingly, no evidence of directional inclusion bias attributable to the exclusion process was identified.
Characteristics of included studies
Of the six included reviews, three contributed to the formal quantitative umbrella component (Basedow et al., 2024; Li et al., 2022; Pinhas et al., 2026) and three were retained for narrative synthesis only (Beaton, 2026; Petranker et al., 2024; Totomanova et al., 2025). As detailed below, Li et al. (2022) is classified under the quantitative component by design but contributed only to narrative synthesis in practice, because its microdose-range subgroup did not yield individually extractable effect sizes at or below the ⩽20 µg threshold; it was, therefore, excluded from all pooled quantitative estimates. This distinction is reflected throughout the results and is summarized in Table 1.The quantitative umbrella component comprised three meta-analyses (Table 1). Pinhas et al. (2026) incorporated 14 studies (13 unique samples, N = 1614) and 59 effect sizes across 7 cognitive domains using a preregistered multilevel meta-analytic framework. Basedow et al. (2024) included 8 microdose-specific primary studies (N = 209) within a broader meta-analysis of acute and subacute psychedelic and 3,4-methylenedioxymethamphetamine (MDMA) effects. Li et al. (2022) synthesized five LSD RCTs (N = 132); the sole microdose-relevant subgroup (Family et al., 2020; LSD 5–20µg; n = 48; mean age 62.9 years) was retained for narrative synthesis only, as individual-dose effect sizes were not separately reported. Mood data within Li et al. (2022) at the lowest dose level (25µg; Holze et al., 2020) nominally exceeded the ⩽20µg threshold and are therefore reported descriptively.
Characteristics of included reviews.
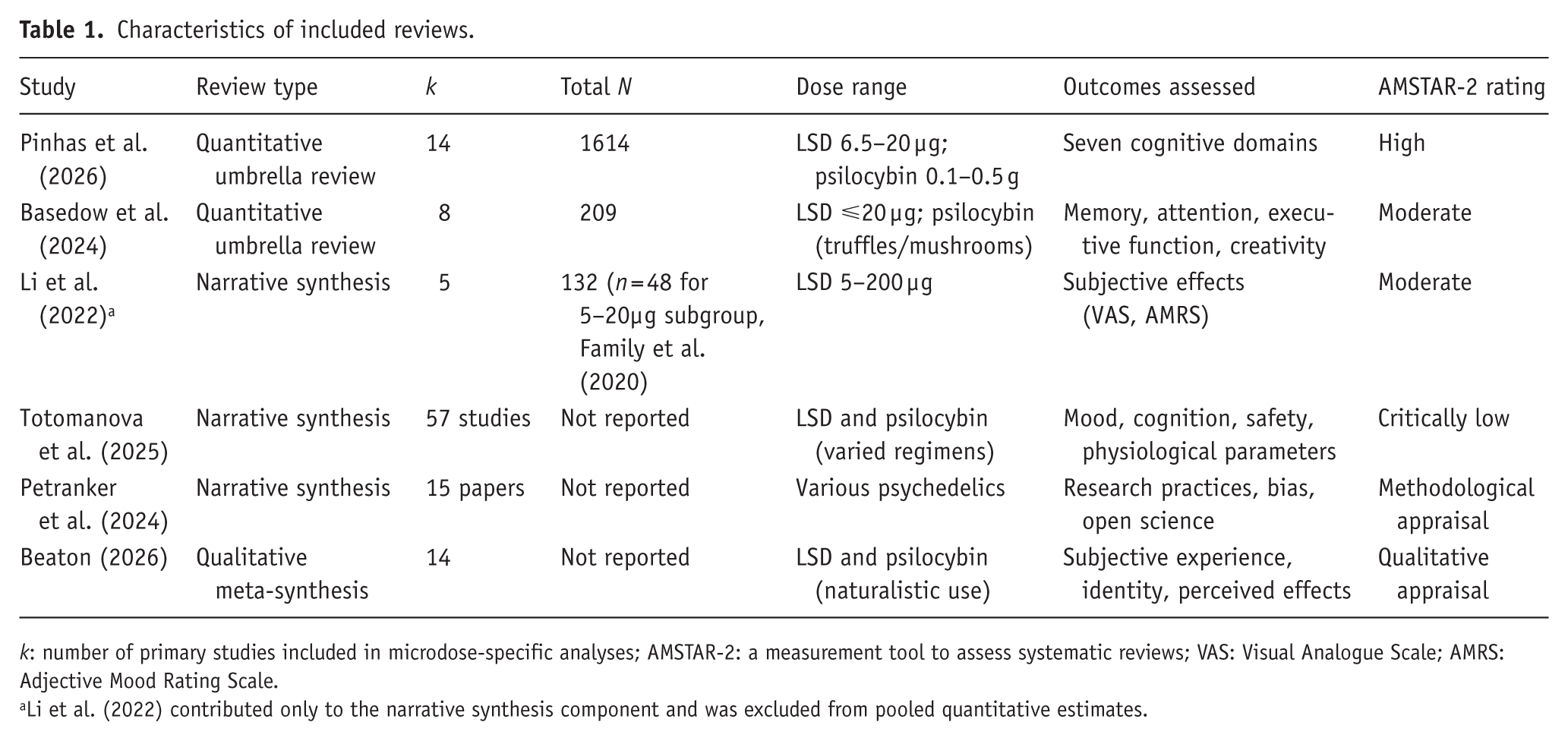
k: number of primary studies included in microdose-specific analyses; AMSTAR-2: a measurement tool to assess systematic reviews; VAS: Visual Analogue Scale; AMRS: Adjective Mood Rating Scale.
Li et al. (2022) contributed only to the narrative synthesis component and was excluded from pooled quantitative estimates.
The narrative synthesis component comprised three reviews. Totomanova et al. (2025) critically synthesized 57 human studies examining psychological and physiological outcomes across clinical and non-clinical populations. Petranker et al. (2024) appraised research practices across 15 experimental and quasi-experimental microdosing papers published before March 2022. Beaton (2026) employed a qualitative meta-synthesis of 14 naturalistic studies examining subjective microdosing experiences outside controlled settings.
Study overlap
Overlap of primary studies across the two quantitative umbrella reviews was assessed by systematic cross-referencing. Using Pinhas et al. (2026; k = 14) and Basedow et al. (2024; k = 8), five studies were confirmed as common to both reviews: Bershad et al. (2019), Family et al. (2020), Yanakieva et al. (2019), Cavanna et al. (2022), and Prochazkova et al. (2018). The CCA (Pieper et al., 2014) was 0.29 (29.4%), indicating very high overlap (classification: slight ⩽5%; moderate 6%–10%; high 11%–15%; very high >15%). Li et al. (2022) was excluded from this calculation.
As shown in Figure 2, a substantial degree of overlap exists between the included reviews, indicating reliance on a largely shared pool of RCTs.
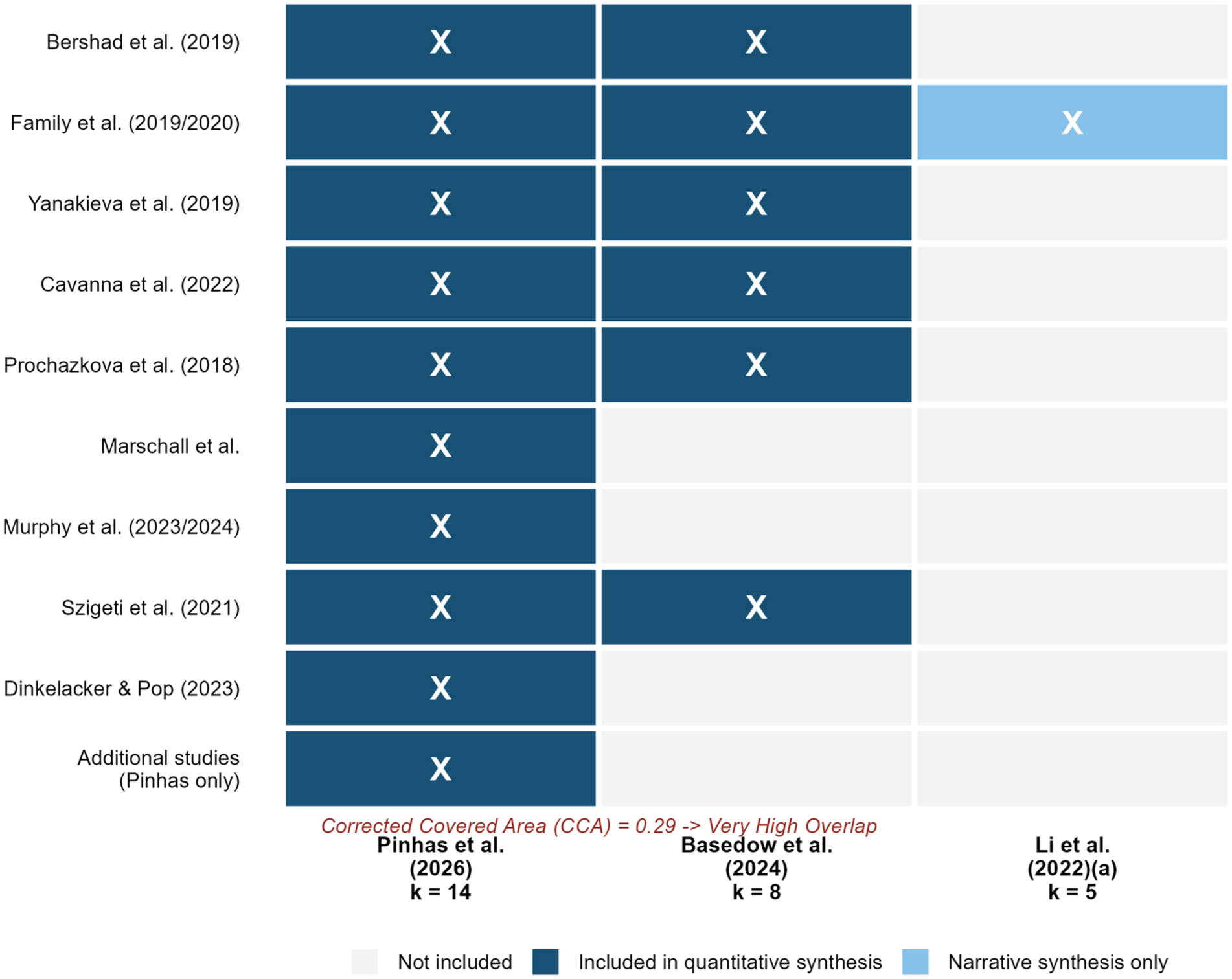
Primary study overlap matrix across included quantitative reviews. Overlap between primary studies included in the quantitative reviews was quantified using the corrected covered area (CCA) method proposed by Pieper et al. (2014). The calculated CCA = 29.4%, indicating very high overlap and, therefore, substantial evidentiary dependence across the included meta-analytic sources. Dark blue cells denote studies included in the quantitative umbrella synthesis, whereas the light blue cell denotes studies included only in the narrative synthesis component (Li et al., 2022). The matrix demonstrates that most reviews draw on a shared core of randomized controlled trials, including Bershad et al. (2020), Family et al. (2020), and Yanakieva et al. (2019).
Methodological quality
AMSTAR-2 ratings ranged from moderate to high. Pinhas et al. (2026) received a high rating, reflecting preregistration, comprehensive search strategy, independent dual screening and extraction, and rigorous statistical procedures including sensitivity and publication bias analyses. Basedow et al. (2024) and Li et al. (2022) each received moderate ratings, primarily due to the absence of prospective registration and limited publication bias assessment. At the primary study level within Pinhas et al. (2026), seven of ten RCTs were rated at high risk of bias (RoB 2.0, Sterne et al., 2019), predominantly for selective outcome reporting and uncontrolled participant expectancy; two (Bershad et al., 2019; Marschall et al., 2022) were low risk and one (Murphy et al., 2023) showed some concerns. All primary studies within Basedow et al. (2024) were rated at high risk, primarily reflecting the structural difficulty of maintaining participant blinding in psychedelic research (Table 2).
Summary of findings and GRADE certainty of evidence by outcome.
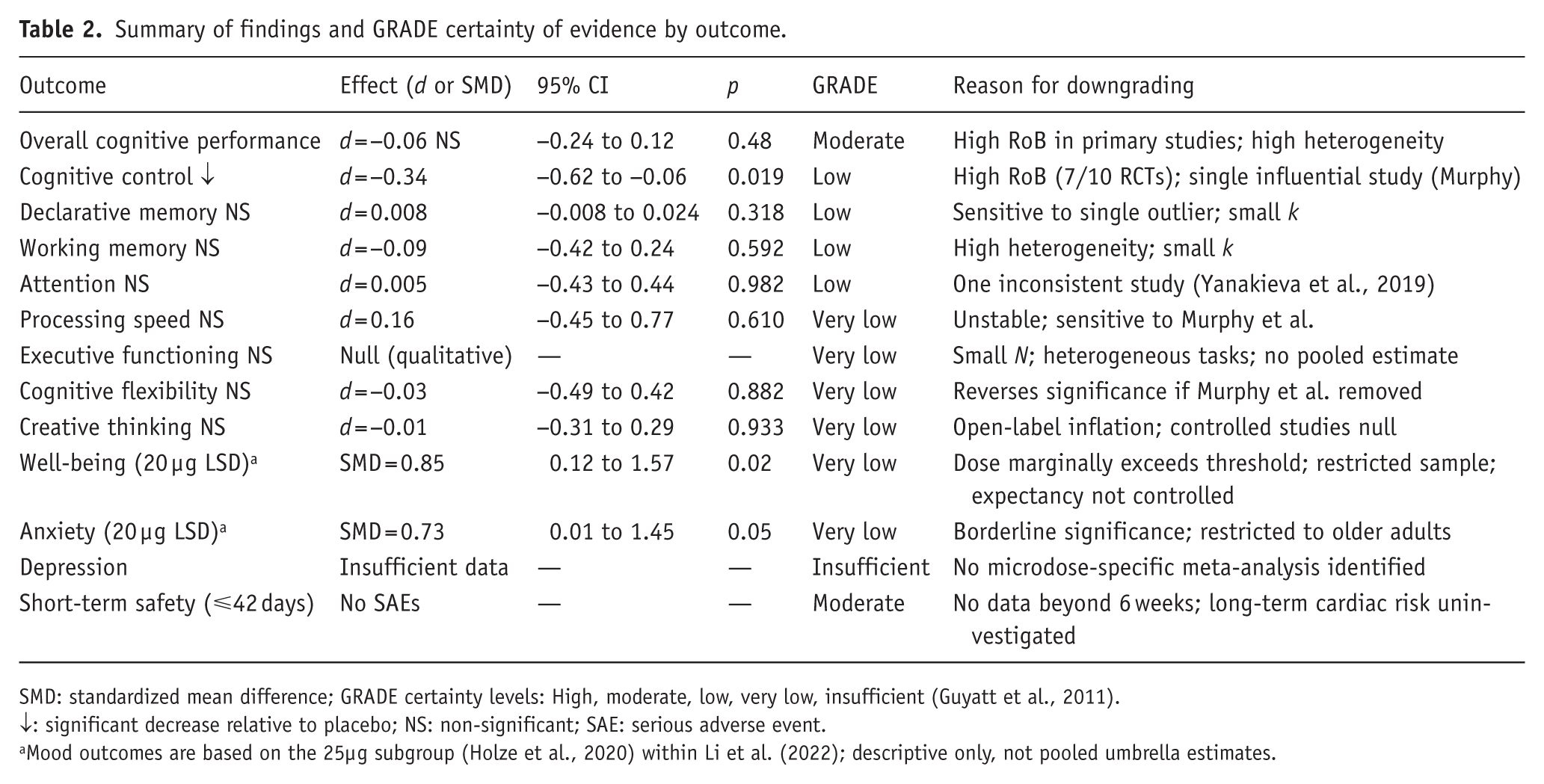
SMD: standardized mean difference; GRADE certainty levels: High, moderate, low, very low, insufficient (Guyatt et al., 2011).
↓: significant decrease relative to placebo; NS: non-significant; SAE: serious adverse event.
Mood outcomes are based on the 25µg subgroup (Holze et al., 2020) within Li et al. (2022); descriptive only, not pooled umbrella estimates.
Cognitive outcomes
Overall cognitive performance
The multilevel meta-analysis by Pinhas et al. (2026), incorporating 59 effect sizes from 14 studies (N = 1614), revealed no significant overall effect of classical psychedelic microdosing on cognitive performance (d = −0.06, 95% CI: −0.24 to 0.12, p = 0.48). Significant heterogeneity was present (Q(58) = 935.59, p < 0.001; σ2 = 0.074; SD = 0.27). Leave-one-out sensitivity analyses confirmed robustness of the null conclusion (d range: −0.11 to −0.01; all p > 0.20). Egger’s test indicated significant funnel asymmetry (b = −0.30, p = −0.008); trim-and-fill correction, imputing two studies, did not alter the conclusion (adjusted d = 0.08, 95% CI: −0.26 to 0.10, p = 0.37).
Cognitive control
The sole domain yielding a statistically significant effect was cognitive control. Pinhas et al. (2026) reported a significant decrease in performance (d = −0.34, 95% CI: −0.62 to −0.06, p = 0.019), the only domain for which confidence intervals excluded zero. Leave-one-out estimates ranged consistently from d = −0.41 to d = −0.26. Cook’s distance analysis identified Murphy et al. (2023, 2025) as a moderately influential case (Cook’s D = 0.29), though removal did not alter significance or direction. Assessment timing did not significantly moderate the effect (on- vs off-drug Δd = 0.29; 95% CI: −0.29 to 0.86, p = 0.33; off-drug: d = −0.50; 95% CI: −0.93 to −0.07; on-drug: d = −0.21; 95% CI: −0.59 to 0.16). Substance type (psilocybin: d = −0.14, p = 0.436; LSD: d = −0.085, p = 0.496), dosage (psilocybin: b = −0.26, p = 0.684; LSD: b = −0.006, p = 0.664), and microdosing duration (b = −0.0009, p = 0.895) were non-significant moderators in exploratory meta-regression analyses.
Memory
Basedow et al. (2024) identified four controlled LSD microdose studies (N = 124) evaluating memory across five tests; none reported significant effects relative to placebo. Within Pinhas et al.’s (2026) study, declarative memory (d = 0.008, 95% CI: −0.008 to 0.024, p = 0.318; Egger’s b = 0.01, p = 0.314) and working memory (d = −0.09, 95% CI: −0.42 to 0.24, p = 0.592; Egger’s b = 0.26, p = 0.420) were both non-significant. Dinkelacker and Pop’s (2023) study was identified as an influential case for declarative memory (Cook’s D = 67.0).
Attention and processing speed
Basedow et al. (2024) identified four controlled microdose studies (N = 106) evaluating attention; three reported null effects and one (Yanakieva et al., 2019) reported reduced attention under LSD microdose. In Pinhas et al.’s (2026) study, neither attention (d = 0.005, 95% CI: −0.43 to 0.44, p = 0.982) nor processing speed (d = 0.16, 95% CI: −0.45 to 0.77, p = 0.610) was significant. Processing speed was sensitive to removal of Murphy et al. (2023, 2025), yielding d = 0.42 (p = 0.062) on removal, though remaining non-significant.
Executive functioning and cognitive flexibility
Basedow et al. (2024) identified five controlled microdose studies (N = 161) evaluating executive functioning across nine tasks; two reported mild impairments, one reported improved performance, and the remainder found no significant effects. Cognitive flexibility in Pinhas et al. (2026) was likewise non-significant (d = −0.03, 95% CI: −0.49 to 0.42, p = 0.882); leave-one-out analysis revealed instability, with removal of Murphy et al. (2023, 2025) yielding a significant positive estimate (d = 0.06, p < 0.001) contrasting with non-significant negative estimates upon removal of all other individual studies.
Creative thinking
Pinhas et al. (2026) reported a non-significant effect (d = 0.01, 95% CI: −0.31 to 0.29, p = 0.933), with Cavanna et al.’s (2022) study identified as an influential case (Cook’s D = 1.21). Basedow et al. (2024) similarly reported a non-significant pooled estimate across three studies (Bershad et al., 2019; Cavanna et al., 2022; Prochazkova et al., 2018; N = 81; Z = 0.37; 95% CI: −2.51 to 3.24, p = 0.64; I2 Level2 = 54.46%). The pooled estimate was dominated by Prochazkova et al. (2018), an open-label observational study reporting a large effect on the Alternate Uses Task (g = 2.40); double-blind placebo-controlled studies reported near-zero or negative effects (Cavanna et al., 2022: AUT g = −1.13, RAT g = −1.03; Bershad et al., 2019: RAT g = 0.22).
As illustrated in Figure 3 and Table 3, pooled estimates across cognitive domains were largely non-significant, except for a small negative effect observed for cognitive control.
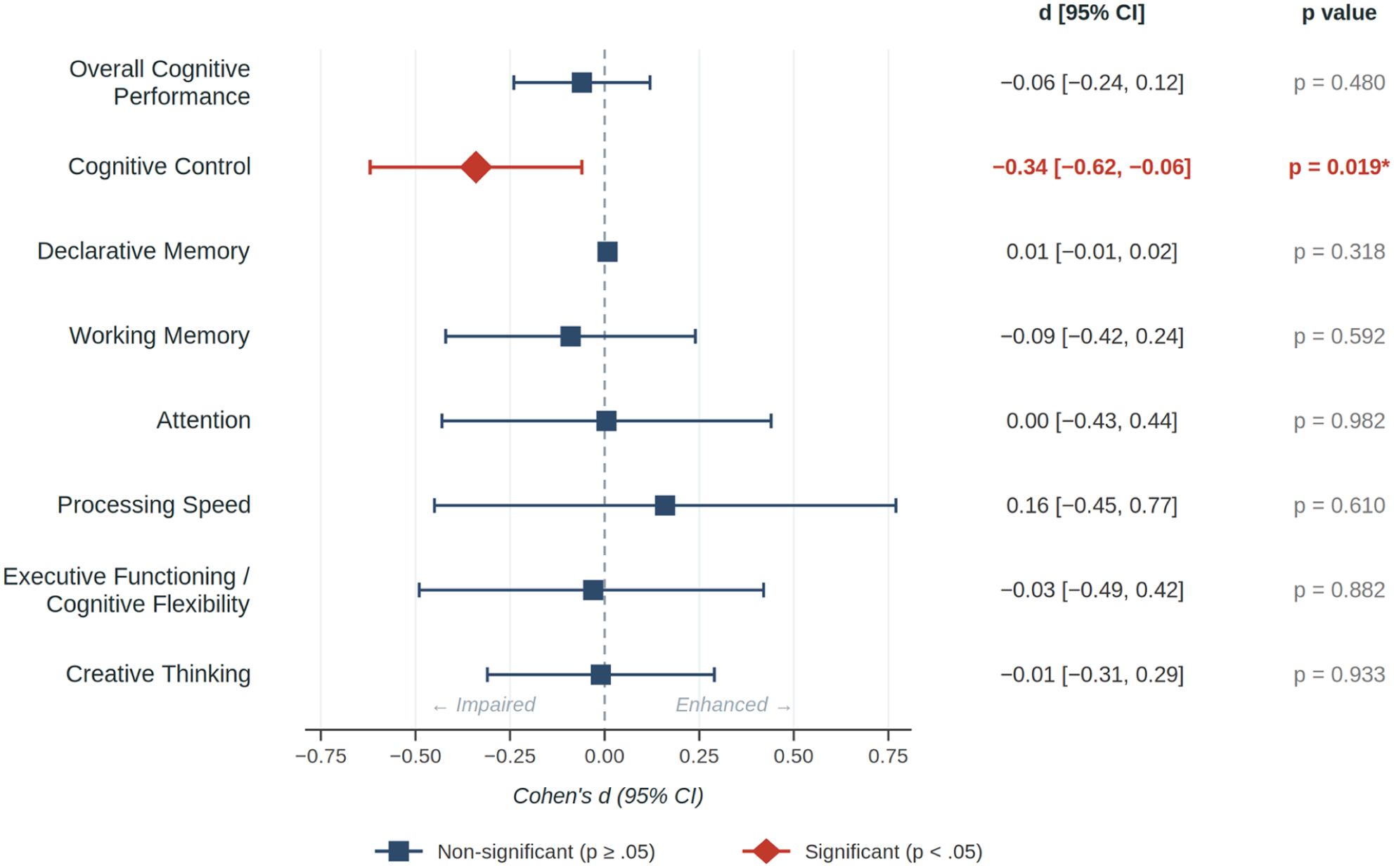
Forest plot of classical psychedelic microdosing effects on cognitive domains. Effect sizes (Cohen’s d) are derived from the multilevel meta-analysis conducted by Pinhas et al. (2026), which incorporated 59 effect sizes from 14 studies (N = 1614). Negative values represent performance decrements relative to placebo, whereas positive values represent performance enhancement. The only statistically significant pooled effect was a small reduction in cognitive control performance (d = −0.34, 95% CI: −0.62 to −0.06, p = 0.019). All other cognitive domains—including memory, attention, and creative thinking—showed non-significant pooled effects, with confidence intervals crossing the null value.
Effect sizes by cognitive domain (Pinhas et al., 2026) and qualitative summary (Basedow et al., 2024).
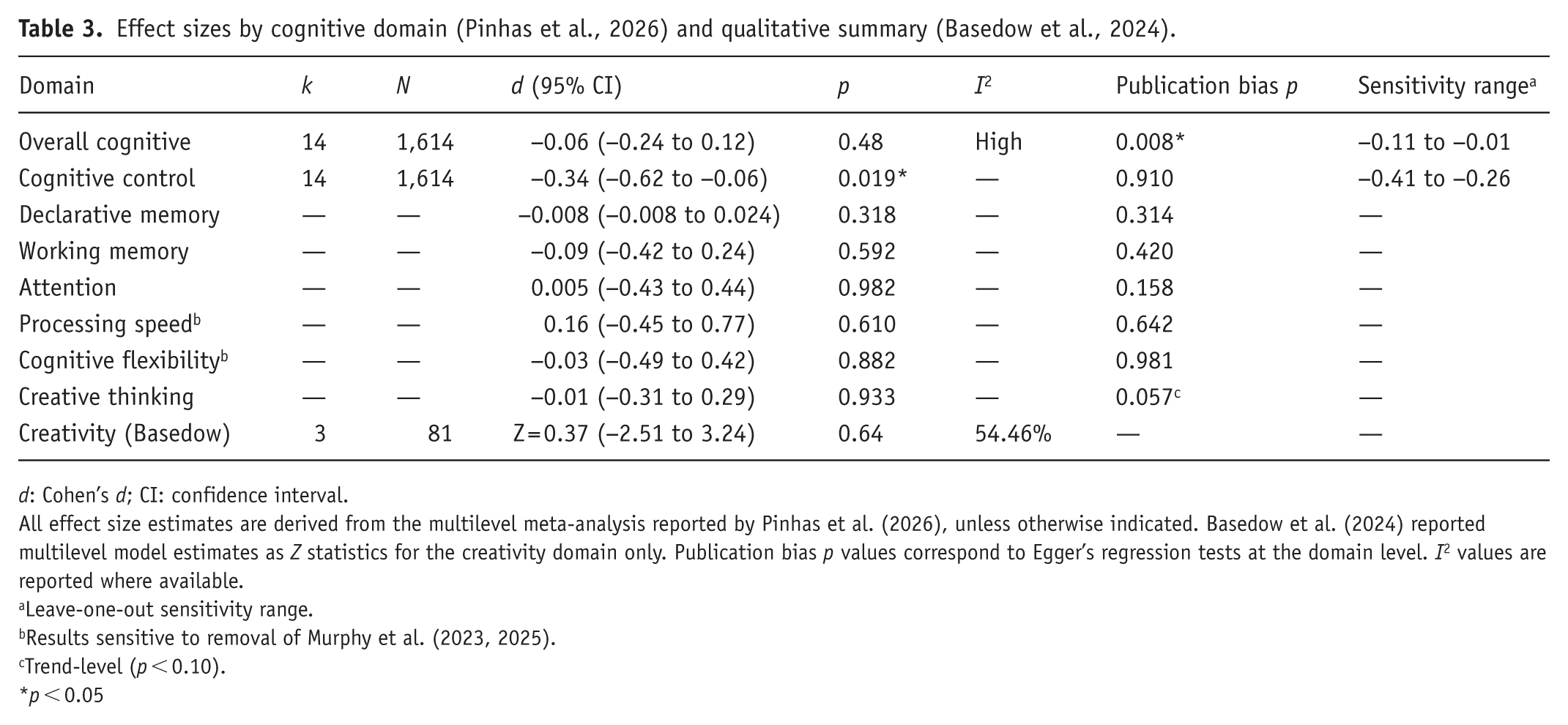
d: Cohen’s d; CI: confidence interval.
All effect size estimates are derived from the multilevel meta-analysis reported by Pinhas et al. (2026), unless otherwise indicated. Basedow et al. (2024) reported multilevel model estimates as Z statistics for the creativity domain only. Publication bias p values correspond to Egger’s regression tests at the domain level. I2 values are reported where available.
Leave-one-out sensitivity range.
Results sensitive to removal of Murphy et al. (2023, 2025).
Trend-level (p < 0.10).
p < 0.05
Mood-related outcomes
Li et al. (2022), the sole review providing mood relevant data near the microdose range, reports its lowest dose subgroup at 25µg LSD (contributed by Holze et al., 2020) a dose nominally exceeding the ⩽20µg threshold. Estimates for the 5, 10, and 20µg arms (Family et al., 2020) were not separately reported. Data are, therefore, presented descriptively and excluded from pooled estimates.
Well-being and subjective drug effects
At the 25-µg LSD subgroup level (Holze et al., 2020, within Li et al., 2022), significant subjective effects were observed on the Visual Analogue Scale: any drug effect (SMD=1.71, 95% CI: 0.89–2.54, p <0.001) and good drug effect (SMD=1.56, 95% CI: 0.75–2.36, p <0.001). Bad drug effect did not reach significance (SMD=0.64, 95% CI: −0.07 to 1.35, p =0.08). On the Adjective Mood Rating Scale, well-being was significantly elevated (SMD=0.85, 95% CI: 0.12–1.57, p =0.02).
Anxiety
The anxiety subscale of the Adjective Mood Rating Scale reached borderline significance at the 25µg subgroup level (SMD=0.73, 95% CI: 0.01–1.45, p=0.05); remaining subscales were non-significant (all p⩾0.13). These findings should be interpreted with caution given the small single-study subgroup (Holze et al., 2020), the absence of expectancy controls, and the dose level nominally exceeding the review threshold.
Depression
No eligible meta-analysis examined depression symptom reduction as a primary outcome at microdose-range doses (⩽20 µg LSD-equivalent), constituting a critical gap in the evidence base.
Safety and adverse events
No serious adverse events (SAEs) causally attributable to microdosing were reported across included studies within exposure periods of up to 42 days. Adverse events were mild and transient, including headache, anxiety, restlessness, fatigue, and gastrointestinal discomfort. In Li et al. (2022), List-of-Complaints and autonomic effects (systolic and diastolic blood pressure, heart rate, body temperature) were significant in the overall pooled analysis across the 25–200µg range (acute LC SMD=0.96; systolic 0.89; diastolic 1.08; heart rate 0.81; body temperature 0.66). However, in dose-stratified subgroup analyses these effects were non-significant at 25µg and reached significance only at 100–200µg, indicating that the pooled signal is driven by the higher, non-microdose levels.
Narrative synthesis
Overview of included reviews
The three narrative synthesis reviews approached the microdosing literature from distinct methodological standpoints. Totomanova et al. (2025) critically synthesized 57 human studies examining psychological and physiological outcomes across clinical and non-clinical populations. Petranker et al. (2024) appraised research practices across 15 experimental and quasi-experimental papers published before March 2022. Beaton (2026) conducted a qualitative meta-synthesis of 14 naturalistic studies examining subjective microdosing experiences outside controlled settings. Together, these reviews span observational, experimental, and qualitative traditions, enabling a broad appraisal of the evidence base and its structural limitations.
Consistency of findings across reviews
All three reviews converged on mood, mental health, and well-being as the most consistently reported perceived benefits. Totomanova et al. (2025) found that observational studies consistently reported positive self-reported effects on mood and reductions in depression, anxiety, and stress; Beaton (2026) similarly reported that naturalistic users commonly described improved mood, reduced anxiety and depressive symptoms, heightened creativity, and greater mood awareness. Both reviews noted, however, that adverse effects—including anxiety, physical discomfort, and cognitive disruption—were also frequently reported, and that outcomes were highly individual and context-dependent.
Cognitive outcomes were considerably less consistent. Among observational studies reviewed by Totomanova et al. (2025), 10 of 11 reported perceived enhancements in cognitive functioning, focus, and productivity; yet six of those same studies simultaneously noted self-reported cognitive difficulties, including concentration problems, racing thoughts, and disorientation. Placebo-controlled experimental studies were more equivocal, with the majority failing to demonstrate objective cognitive enhancement—a systematic divergence between self-reported and objectively measured effects that recurs throughout the literature.
Methodological quality of the underlying evidence base
Petranker et al. (2024) concluded that the majority of published microdosing research should be considered preliminary, noting a near-total absence of pre-registration (two of 14 surveyed papers), widespread failure to share data (4 of 14 papers had data available online; several authors declined data-sharing requests), biased and non-representative samples, inconsistent dosing particularly in psilocybin studies, and inappropriate statistical inferences. Totomanova et al. (2025) identified a systematic pattern whereby observational studies report substantially more benefits than experimental trials, attributable to self-selection, expectancy, and personalized dosing rather than pharmacological efficacy. Beaton (2026) demonstrated that microdosers’ self-narratives are shaped by identity and boundary maintenance processes users frame microdosing as rational and conventional rather than recreational in ways that may systematically inflate self-reported benefits in naturalistic settings.
Relationship to quantitative umbrella findings
The narrative evidence reinforces the quantitative umbrella findings. The single statistically significant pooled effect a decrease in cognitive control performance (d = −0.34) is consistent with the cautionary pattern emerging across all three narrative reviews: where experimental, placebo-controlled designs are employed, reported benefits attenuate or disappear and adverse cognitive effects become more visible. Self-reported enhancements prominent in observational and qualitative data are not corroborated by objective measurement in controlled conditions. Beaton’s (2026) identification of identity-based narration as a systematic driver of perceived benefit provides a plausible mechanism for this discrepancy and underscores the interpretive limitations of self-report data in this literature.
Discussion
This umbrella review synthesized review-level evidence on classical psychedelic microdosing across cognition, mood, and safety. Under strict microdose-focused eligibility criteria, the quantitative component relied primarily on available meta-analytic evidence for cognitive outcomes (Pinhas et al., 2026), while complementary systematic and critical reviews were incorporated narratively to contextualize methodological constraints and interpretability limits (Petranker et al., 2024; Polito and Liknaitzky, 2022; Totomanova et al., 2025). Primary-study overlap across review-level sources was substantial, indicating limited evidentiary independence and warranting cautious interpretation of aggregate conclusions (Pieper et al., 2014; Polito and Liknaitzky, 2022); across cognitive domains, current pooled evidence does not support consistent cognitive enhancement, with the only significant signal being a small decrement in cognitive control (approximately d = −0.34), while other domains are largely null (Pinhas et al., 2026). For mood outcomes, robust quantitative synthesis remains constrained under strict dose boundaries, so conclusions depend more heavily on convergent narrative evidence (Petranker et al., 2024; Totomanova et al., 2025). Short-term tolerability in controlled settings appears acceptable within observed exposure windows, but adverse effects are reported and long-term safety remains insufficiently characterized (Cavanna et al., 2022; Hutten et al., 2019; Totomanova et al., 2025); overall, the field remains early-stage, and stronger inference requires larger preregistered trials, harmonized dose definitions, and longer follow-up (Petranker et al., 2024; Polito and Liknaitzky, 2022; Pinhas et al., 2026).
Effects on mood
No eligible meta-analysis provided pooled mood-outcome effect sizes exclusively within the ⩽20 µg LSD-equivalent threshold in a form suitable for quantitative synthesis. Li et al. (2022), the sole review reporting mood data within the approximate microdose range, reported significant subjective effects at 25-µg LSD in a healthy older adult sample (n = 48; mean age 62.9 years): well-being was significantly elevated (SMD = 0.85, p = 0.02) and the anxiety subscale reached borderline significance (SMD = 0.73, p = 0.05). The absence of individually reported effect sizes for 5, 10, and 20 µg within this review precluded extraction at the pre-specified threshold. These findings should be interpreted with caution: the sample was restricted to healthy older adults with no baseline affective pathology, expectancy was not experimentally controlled, and the dose level nominally exceeded the review threshold. No eligible meta-analysis examined depression symptom reduction as a primary outcome at microdose-range doses, constituting a critical gap in the evidence base.
Across all three narrative synthesis reviews, self-reported improvements in mood, well-being, and reductions in anxiety and depressive symptoms emerged as the most consistently reported perceived benefits of microdosing (Beaton, 2026; Totomanova et al., 2025). However, these reports derive predominantly from observational and naturalistic designs in which expectancy is uncontrolled. Totomanova et al. (2025) identified a systematic divergence between observational studies—which consistently report positive mood outcomes—and placebo-controlled trials, which yield attenuated or null effects. Beaton (2026) demonstrated that this divergence is at least partly attributable to identity-based narration: naturalistic microdosers systematically frame their experiences in ways that emphasize benefit and minimize harm, inflating self-reported outcomes relative to controlled conditions. The absence of an eligible pooled mood estimate in the present review, therefore, reflects not only a dose-boundary constraint but the broader evidentiary problem of disentangling pharmacological from expectancy-driven mood effects in this literature.
Clinical versus healthy populations
Available evidence does not permit firm conclusions regarding differential effects of microdosing across clinical and healthy populations, as no eligible quantitative meta-analysis directly examined mood outcomes in diagnosed samples at doses ⩽20 µg LSD-equivalent. The Li et al. (2022) subgroup was restricted to healthy older adults, precluding generalization to clinical populations. Narrative synthesis evidence from Totomanova et al. (2025) suggests that observational studies reporting the largest mood benefits tend to include self-selected samples with pre-existing mental health difficulties, consistent with regression-to-the-mean and expectancy amplification in symptomatic individuals. Whether microdosing confers pharmacologically distinct mood benefits in clinical populations—as suggested by full-dose psychedelic-assisted therapy findings, including a randomized trial comparing psilocybin with escitalopram (serotonin reuptake inhibitor; SERT) for depression (Carhart-Harris et al., 2021)—remains an open empirical question requiring prospective, expectancy-controlled trials in diagnosed samples.
Placebo and expectancy effects
The role of expectancy and placebo mechanisms in shaping observed outcomes was a convergent theme across all included reviews and constitutes the primary interpretive challenge for the field. Expectancy effects in psychedelic research are not confined to uncontrolled or observational designs: even within RCTs, the subjective salience of psychedelic administration—including at sub-perceptual microdose levels—renders conventional double-blind procedures structurally unreliable, as participants frequently identify their allocation based on subtle physiological or perceptual cues (Petranker et al., 2024; Szigeti et al., 2021). Petranker et al. (2024) demonstrated that this problem is compounded by systematic methodological failures: near-universal absence of pre-registration, widespread non-disclosure of data, and biased recruitment at psychedelic-enthusiast events collectively ensure that expectancy inflation is maximized and undetectable in the majority of available studies. Beaton (2026) extended this analysis to the sociocultural level, demonstrating that microdosers’ identity and community membership actively shape outcome narration in ways that are indistinguishable from pharmacological response in self-report data. Taken together, these findings indicate that the pharmacological contribution of microdosing above and beyond expectancy-driven responses cannot be reliably estimated from the currently available evidence base.
Cognitive effects
No included review provided evidence for reliable cognitive enhancement through microdosing at sub-perceptual doses. The multilevel meta-analysis by Pinhas et al. (2026), the largest and most methodologically rigorous synthesis identified, found no significant overall cognitive effect (d = −0.06, p = 0.48) and non-significant estimates across six of seven domains examined. The sole exception was a small, but consistent decrease in cognitive control performance (d = −0.34, 95% CI: −0.62 to −0.06), an effect that persisted in leave-one-out sensitivity analyses, was not moderated by assessment timing, substance type, dose, or duration in exploratory meta-regression analyses reported by Pinhas et al. (2026), and is directionally consistent across both on-drug and off-drug assessment windows. This finding is particularly notable given the widespread popular claim that microdosing enhances executive and attentional functions: the available controlled evidence suggests the opposite directional tendency, at least for inhibitory aspects of cognitive control.
The dissociation between subjective reports of improved focus and concentration—consistently reported in observational studies reviewed by Totomanova et al. (2025)—and null or negative objective findings in controlled designs is a central feature of the microdosing literature. This pattern is consistent with expectancy-driven responding and has been documented across multiple placebo-controlled designs (Cavanna et al., 2022; Yanakieva et al., 2019). Basedow et al. (2024) additionally identified assessment timing as a potential moderator, with acute attentional effects and sub-acute executive facilitation emerging in separate subsets of studies, suggesting that the window of cognitive assessment relative to drug administration may critically determine observed outcomes a variable requiring standardization in future research.
Creativity and divergent thinking
Claims that microdosing reliably enhances creative thinking or divergent cognition are not supported by blinded controlled evidence. The large positive effect on the Alternate Uses Task reported by Prochazkova et al. (2018; g = 2.40) was obtained under open-label conditions and is attributable to expectancy and practice effects; double-blind, placebo-controlled studies yielded near-zero or negative estimates (Bershad et al., 2019: RAT g = 0.22; Cavanna et al., 2022: AUT g = −1.13, RAT g = −1.03), and pooled estimates in both Basedow et al. (2024; Z = 0.37, p = 0.64) and Pinhas et al. (2026; d = 0.01, p = 0.933) were non-significant. This pattern—large effects in open-label designs attenuating to null under blinded conditions—exemplifies the broader subjective–objective dissociation observed across cognitive domains.
Mechanisms of action
Both LSD and psilocybin act as partial agonists at serotonin 5-HT2A receptors, with sub-perceptual doses hypothesized to modulate cortical excitability and synaptic plasticity without producing full hallucinogenic effects (Carhart-Harris and Nutt, 2017; Nichols, 2016). The neurobiological basis for the cognitive control impairment identified in the present review is consistent with 5-HT2A-mediated modulation of prefrontal inhibitory circuits (Celada et al., 2013), though direct neuroimaging evidence specific to microdose-range administration remains sparse. The relative contributions of pharmacological and expectancy mechanisms to observed mood and cognitive outcomes cannot be reliably partitioned with currently available data. Future neuroimaging and biomarker studies employing active placebo controls and verified blinding are required to characterize the neurobiological signature of microdosing independent of expectancy.
Safety
Short-term tolerability within study exposure periods (⩽42 days) was acceptable across all included reviews: no SAEs were causally attributed to microdosing, and adverse events were consistently mild and transient. However, two specific safety signals identified in this review warrant prospective monitoring. Li et al. (2022) reported significant autonomic elevations (systolic and diastolic blood pressure, heart rate, body temperature) in pooled analyses across 25–200µg, but these effects were non-significant at 25µg in dose-stratified analysis and emerged only at 100–200µg. Within the microdose range, LSD therefore appears largely physiologically inert in acute studies; cardiovascular signals are confined to higher doses, while the theoretical 5-HT2B-mediated risk under chronic microdosing (Totomanova et al., 2025) remains uninvestigated. Second, Totomanova et al. (2025) flagged the theoretical risk of cardiac fibrosis through 5-HT2B receptor activation under chronic exposure—a mechanism previously implicated in valvular pathology with other long-term serotonergic compounds acting via 5-HT2B agonism—as remaining largely uninvestigated in human microdosing studies. The majority of available safety data reflect exposure periods of ⩽6 weeks; cumulative and long-term risks are entirely unknown and constitute a critical evidence gap. Future trials should incorporate cardiac monitoring protocols and follow-up periods of sufficient duration to detect delayed adverse effects.
Clinical implications
When patients enquire about psychedelic microdosing, clinicians should convey the following evidence-based summary: mood effects at doses within the established microdose range have not been reliably demonstrated in controlled conditions; there is no convincing evidence of cognitive enhancement in any neuropsychological domain; the sole consistent finding from controlled research is a small impairment of cognitive control; and long-term safety including potential cardiovascular risks remains uncharacterized. Self-reported benefits widely circulated in popular discourse are largely consistent with expectancy-driven responses rather than pharmacological effects. Established treatments for mood and anxiety disorders retain substantially stronger empirical support. Microdosing should be considered investigational and is not currently suitable for clinical recommendation pending adequately powered, expectancy-controlled trials.
Methodological limitations
Several limitations of the present review should be noted. Primary study overlap across the quantitative umbrella component was very high (CCA = 0.29), indicating that the two meta-analyses draw substantially from the same small pool of primary RCTs; effect estimates are, therefore, not independent, and findings should be interpreted accordingly. The absence of an eligible pooled mood effect size reflects both the dose-boundary constraint applied in this review and the broader unavailability of well-controlled mood outcome data at doses ⩽20 µg. Meta-regression analyses reported by Pinhas et al. (2026) and discussed above are strictly exploratory given the small number of primary studies; no causal inferences regarding dose or population-level moderation are warranted. The evidence base is additionally constrained by the predominantly healthy, psychedelic-experienced, and self-selected samples characteristic of existing primary research, limiting generalizability to clinical populations and individuals naïve to psychedelic substances.
Future research directions
All three narrative synthesis reviews converged on the need for pre-registered, double-blind, placebo-controlled trials with adequate sample sizes, verified dosing, active manipulation of participant expectancy, and longitudinal follow-up. Petranker et al. (2024) proposed the establishment of a consortium of psychedelic researchers committed to open science standards preregistration, data sharing, and transparent reporting as a structural prerequisite for meaningful cumulative knowledge. Totomanova et al. (2025) additionally emphasized prospective investigation of neurobiological mechanisms and cardiac safety monitoring under repeated administration. Beaton (2026) argued for dedicated qualitative and mixed-methods research to characterize the sociocultural dimensions of microdosing—including expectancy formation, identity processes, and community norm transmission—as these factors directly shape both self-reported outcomes and the ecological validity of controlled trial findings. Individual participant data meta-analysis, where feasible, would substantially improve the precision of dose-response and population-level moderator estimates.
Footnotes
Acknowledgements
No individuals who do not meet the authorship criteria contributed to the preparation of this article.
Ethical considerations
Not applicable. This umbrella review did not involve the collection or analysis of primary data from human participants and therefore did not require ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This umbrella review is based exclusively on previously published systematic reviews and meta-analyses. All data analyzed are available within the referenced publications.
Editorial board membership disclosure
None of the authors are members of the Editorial Board of the Journal of Psychopharmacology.