
Abstract
Previous research presented mixed results on the relationship between mental resilience, that is, the ability to adapt to stress of major life events, and the frequency and severity of experiencing alcohol hangovers. An online survey among n = 854 UK and Irish adults who consume alcohol was conducted to investigate this relationship. Mental resilience was assessed with the Brief Resilience Scale (BRS) and the Connor–Davidson Resilience Scale (CD-RISC 2). No significant correlations were found between mental resilience and alcohol consumption outcomes. Correlations between mental resilience and hangover frequency and severity were small and not significant (all: |r| < −0.1). Multiple linear regression analyses showed that mental resilience was not a significant predictor of hangover severity (BRS: B = 0.039; 95% CI: −0.127, 0.205; p = 0.644, and CD-RISC 2: B = −0.008; 95% CI: −0.077, 0.092; p = 0.841) or hangover frequency (BRS: B = −0.078; 95% CI: −0.168, 0.012, p = 0.091, and CD-RISC 2: B = −0.043; 95% CI: −0.089, 0.003; p = 0.065).Together, these findings suggest that any association between mental resilience and alcohol hangover outcomes is likely to be small and of limited practical relevance.
Introduction
The alcohol hangover is defined as the combination of mental and physical symptoms experienced the day after a single episode of heavy drinking, starting when blood alcohol concentration (BAC) approaches zero (Verster et al., 2020). Several factors may influence the frequency and severity of alcohol hangovers (Verster et al., 2023). These can be related to not only amount of alcohol consumed over a certain period of time but also characteristics of the alcoholic beverages (e.g. congener content), the drinker (e.g. health status, including psychological state) (Verster et al., 2023). Further, in particular when coping strategies are inadequate, alcohol consumption may be influenced by external causes such as stress or major life events (Sanchez et al., 2022), and as such influence the frequency or severity of hangovers. It is crucial to further investigate factors that may increase its frequency and severity, as experiencing hangovers has been associated with systemic inflammation, which increases the susceptibility to disease (Išerić et al., 2024). Previous research revealed mixed results on a possible relationship between mental resilience and experiencing hangovers (Terpstra et al., 2022; Verster et al., 2023). However, the conflicting evidence may be due to methodological shortcomings discussed elsewhere (Verster et al., 2023), including that hangover severity and drinking measures were not necessarily aligned to the same event in the study from Terpstra et al. (2022). Therefore, it was hypothesized that there was no significant relationship between mental resilience, alcohol consumption, and experiencing hangovers. The present exploratory study evaluated this hypothesis using an online survey conducted among a convenience sample of adults living in the United Kingdom or Ireland. They were recruited among individuals that followed a psychology course at The Open University. The study was approved by The Open University Human Research Ethics Committee, HREC (approval code: HREC/4628, date of approval: 20 March 2023), and all participants provided informed consent. A detailed description of the study methodology, survey content, and the dataset are published elsewhere (Verster et al., 2025).
In addition to demographics (e.g. sex, age, bodyweight), the survey comprised questions on weekly alcohol (drinks per week and number of drinking days), and for the past month’s heaviest drinking occasion information was gathered on the number of drinks and the duration of drinking. Respondents were given information about standard serving sizes of alcohol and were asked to convert the consumed beverages into standard alcoholic drink sizes (units). Subjective intoxication and next-day hangover severity were assessed on a scale ranging from 0 (absent) to 10 (extreme). The estimated blood alcohol concentration (BAC) for this drinking occasion was computed using a modified Widmark equation, taking into account the amount of alcohol consumed, drinking duration, bodyweight, and sex (Watson et al., 1981; Mathijssen and Twisk, 2001). In addition, the number of hangovers they experienced per month was recorded. Mental resilience was assessed with two different scales: the Brief Resilience Scale (BRS) (Smith et al., 2008) and the abbreviated version of the Connor–Davidson Resilience Scale (CD-RISC), the CD-RISC 2 (Vaishnavi et al., 2007). The BRS has 6 items using 5-point Likert scales and reports excellent internal consistency reliability, whereas the CD-RISC 2 has 2 items, each with 5 answering options (from 0 to 4), with a total sum of 0–8. For both measures, higher scores indicate greater ability to bounce back. Statistical analyses were conducted with SPSS (IBM Corp, 2013. Released 2013). Since the data were not normally distributed, nonparametric tests were applied. Possible sex differences were evaluated with the Independent-Samples Mann–Whitney U test (p < 0.00625, applying a Bonferroni’s correction for multiple related comparisons). Spearman’s correlations were computed between the alcohol and metal resilience outcomes. A partial Spearman’s correlation, controlling for estimated BAC, was computed between mental resilience and subjective intoxication and between mental resilience and hangover severity. Correlations were considered significant if p < 0.0031, applying a Bonferroni’s correction for multiple related correlations. Finally, multiple linear regression analyses were conducted to identify predictors of hangover severity and hangover frequency. Mental resilience was included as a continuous predictor, and all variables listed in Table 1 were entered simultaneously into the model (enter method). The unstandardized regression coefficient (slope estimate; B), representing the expected change in the outcome variable associated with a one-unit increase in the predictor variable, was computed, along with its 95% confidence interval (CI). Separate analyses were conducted for the BRS and the CD-RISC2.
Study outcomes and their relationship with mental resilience.
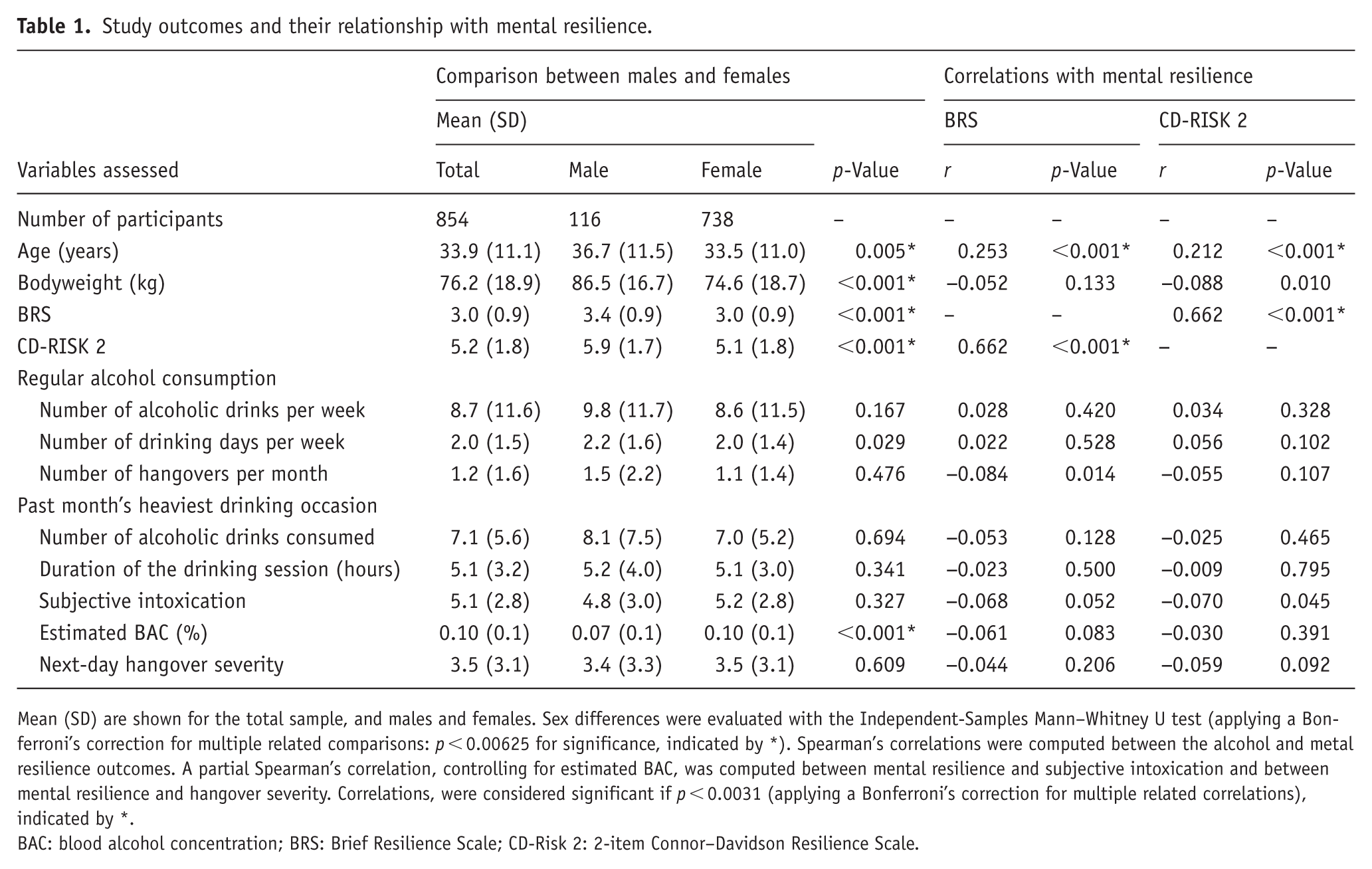
Mean (SD) are shown for the total sample, and males and females. Sex differences were evaluated with the Independent-Samples Mann–Whitney U test (applying a Bonferroni’s correction for multiple related comparisons: p < 0.00625 for significance, indicated by *). Spearman’s correlations were computed between the alcohol and metal resilience outcomes. A partial Spearman’s correlation, controlling for estimated BAC, was computed between mental resilience and subjective intoxication and between mental resilience and hangover severity. Correlations, were considered significant if p < 0.0031 (applying a Bonferroni’s correction for multiple related correlations), indicated by *.
BAC: blood alcohol concentration; BRS: Brief Resilience Scale; CD-Risk 2: 2-item Connor–Davidson Resilience Scale.
Data of n = 854 participants who consume alcohol were included in the analyses. The study results are summarized in Table 1. Compared to males, females were significantly younger, had a lower bodyweight, and scored significantly lower on both resilience scales. Regarding alcohol consumption, compared to males, females had a significantly higher estimated BAC on their past month heaviest drinking occasion.
No significant correlations were found between hangover severity and mental resilience, assessed with either the BRS (r = −0.044, p = 0.206) or the CD-RISC 2 (r = −0.059, p = 0.092). The observed correlations were small, with 95% confidence intervals spanning values close to zero (i.e., hangover severity and BRS: −0.120, 0.018, and hangover severity and CD-RISC 2: −0.129, 0.010). These results indicate no evidence for a meaningful positive association between mental resilience and hangover severity. While the data do not exclude the possibility of a small negative relationship, any such effect is likely to be limited in magnitude.
Significant positive correlations were found between age and mental resilience. There was good agreement between the two scales assessing mental resilience (r = 0.622, p < 0.001). None of the alcohol consumption variables correlated significantly with the two mental resilience scales, and the magnitude of the correlations was weak (all between −0.1 and 0.1).
Two multiple linear regression analyses were conducted, including all variables listed in Table 1, to identify potential predictors of hangover severity. The analyses were performed separately for the Brief Resilience Scale (BRS) and the CD-RISC2. When including the BRS, the model was significant (F(11, 801) = 83.98, p < 0.001), explaining 53.6% of the variance in hangover severity. Subjective intoxication (B = 0.602; 95% CI: 0.531, 0.673; p < 0.001), number of alcoholic drinks consumed (B = 0.138; 95% CI: 0.006, 0.274; p = 0.041), and hangover frequency (B = 0.628; 95% CI: 0.508, 0.748; p < 0.001) emerged as significant predictors. When including the CD-RISC2, a model was observed (F(11, 801) = 83.94, p < 0.001), explaining 53.5% of the variance. Subjective intoxication (B = 0.601; 95% CI: 0.530, 0.672; p < 0.001), number of alcoholic drinks consumed (B = 0.138; 95% CI: 0.005, 0.271; p = 0.042), and hangover frequency (B = 0.627; 95% CI: 0.507, 0.747; p < 0.001) were the significant predictors. Mental resilience was not a significant predictor of hangover severity. Both the Brief Resilience Scale (B = 0.039; 95% CI: −0.127, 0.205; p = 0.644) and the CD-RISC2 (B = −0.008; 95% CI: −0.077, 0.092; p = 0.861) showed small effect estimates with confidence intervals centered near zero, suggesting that any association is likely to be minimal.
Two additional multiple linear regression analyses were conducted to identify potential predictors of hangover frequency, again separately for the BRS and CD-RISC2. When including the BRS, the model was significant (F(11, 801) = 41.03, p < 0.001), explaining 36.0% of the variance in hangover frequency. Hangover severity (B = 0.186; 95% CI: 0.155, 0.222; p < 0.001) and the number of drinking days per week (B = 0.172; 95% CI: 0.106, 0.238; p < 0.001) were significant predictors. When including the CD-RISC2, a comparable model was found (F(11, 801) = 41.10, p < 0.001), explaining 36.1% of the variance. Hangover severity (B = 0.186; 95% CI: 0.150, 0.221; p < 0.001) and the number of drinking days per week (B = 0.172; 95% CI: 0.106, 0.237; p < 0.001) were significant predictors. Mental resilience was not a significant predictor of hangover frequency. Both the Brief Resilience Scale (B = −0.078; 95% CI: −0.168, 0.012; p = 0.091) and the CD-RISC2 (B = −0.043; 95% CI: −0.089, 0.003; p = 0.065) showed small effect estimates with confidence intervals close to zero, indicating that any association is likely to be limited in magnitude and not of practical relevance.
Strengths of the study include its large sample size of UK adults following a psychology course at The Open University. In contrast to typical student samples, the current sample comprised a much broader age range. In addition, mental resilience was assessed via two different scales. Limitations include that the majority of participants were female. Second, the retrospective, self-reported data may have been affected by recall bias. Third, the study was conducted in a convenience sample of Open University students. Therefore, the findings may not generalize to the broader population and should be interpreted in the context of this specific sample. Thus, the results should be interpreted with appropriate caution and may serve as a basis for future confirmatory work. Fourth, the analyses did not explicitly account for potential measurement error in the mental resilience scales. Although validated instruments were used, any measurement imprecision in predictor variables may attenuate observed associations. Future studies could consider approaches such as errors-in-variables models to further refine effect estimates. Finally, we used a stringent Bonferroni’s correction because multiple correlations were tested within the same conceptual family of hypotheses (i.e., associations between resilience and several related alcohol-use and subjective response measures). The correction was used to control the familywise error rate and reduce the likelihood of Type I error inflation. Importantly, the overall interpretation of the association between hangover severity and mental resilience remains consistent when examining uncorrected p-values.
In conclusion, the present findings are consistent with previous research (Verster et al., 2023) and suggest that mental resilience is unlikely to be meaningfully associated with the experience of alcohol hangovers. The observed effect estimates were small, indicating that any potential relationship is limited in magnitude and not of practical relevance. Similarly, mental resilience showed no meaningful association with alcohol consumption patterns, including the frequency and quantity of regular alcohol intake and consumption during the past month’s heaviest drinking occasion.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by The Open University Human Research Ethics Committee, HREC (approval code: HREC/4628, date of approval: 20 March 2023).
Consent to participate
Electronic informed consent was obtained from all participants involved in the study.
Consent to publication
All participants provided consent to publish the data.
Author contributions
S.S., L.D., and J.V. contributed to the conceptualization, design, and methodology of the study; L.D. collected the data; S.S. and J.V. conducted the statistical analysis; S.S. and J.V. prepared the original draft. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There are no conflicts of interest in relation to this study. Over the past 3 years, J.V. has acted as a consultant/advisor for KNMP,Komoinvest, Med Solutions, Mozand, Red Bull, and Sen-Jam Pharmaceutical. J.V. received travel support and owns stock from Sen-Jam Pharmaceutical. The other authors have no potential conflicts of interest to disclose.
Data Availability Statement
The data are available as supplementary materials to reference (Verster et al., 2025).