
Abstract
This article examined the reporting of four elements of fidelity of implementation (FOI) in parent-mediated early communication treatment studies. Thirty-five studies were reviewed to extract information regarding reporting of dosage, adherence, quality, and participant responsiveness for both practitioners and parents involved in parent-delivered communication treatment for children birth to 6 years of age. Results indicate relatively low reporting practices across the four elements of FOI for both practitioners and parents. Most studies (71%) reported dosage at the practitioner level (e.g., number and length of parent-training sessions), while few studies (14%) reported dosage at the parent level (i.e., amount of intervention implemented by parents outside of treatment sessions). Results also found 60% of studies reported adherence for parent implementation, but only 34% of studies reported adherence for practitioners. Implications for low reporting in the research literature, as well as recommendations for future reporting and research on FOI, are provided.
Keywords
Accurate implementation of interventions that have been shown to be efficacious in controlled research contexts is one way we bridge the gap between scientific research and improved outcomes for children with disabilities and their families (Bellg et al., 2004; Breitenstein, Robbins, & Cowell, 2012; Halle, 1998). However, limited measurement of fidelity of implementation (FOI) in research (Kaderavek & Justice, 2010; Smith, Daunic, & Taylor, 2007) is a roadblock in linking research to the practices carried out across treatment research fields (Gresham, 2009). In addition, measurement of FOI in practice presents a unique set of challenges. This may be particularly true when an indirect service delivery model is used—a model often used with young children with special needs. Understanding how implementation of teaching and coaching strategies with parents, and parents’ subsequent use of learned strategies with children, affects child outcomes both in and out of the lab requires fidelity measurement at the practitioner and parent levels, and is necessary for development and dissemination of evidence-based practices in early childhood intervention. The purpose of the current article is to conduct a systematic review of reporting practices of FOI in parent-mediated communication intervention studies for young children with disabilities as an illustration of where we are as a field in the collection and reporting of FOI data, and provide a framework for how we might best measure FOI in research and practice involving young children with disabilities and their families.
The current article uses the term FOI to refer to practitioner implementation of teaching and coaching strategies with parents (referred to as implementation fidelity by Barton & Fettig, 2013), and to parent implementation of newly acquired strategies with their children (referred to as intervention fidelity by Barton and Fettig). FOI has been defined as the degree to which a treatment is carried out as intended (Carroll et al., 2007), and may be viewed as a complex, multidimensional construct that includes measurement of the implementation of an intervention, as well as engagement in the intervention by treatment recipients (Zvoch, 2012). It is likely that FOI affects the association between a treatment and outcome (i.e., acts as a mediator and/or moderator; Carroll et al., 2007), and that other variables may act as mediators or moderators of FOI (Sanetti & Kratochwill, 2009). Although there is growing consensus among researchers of the importance of addressing this construct in research and practice, there continue to be limitations in defining, measuring, and reporting FOI in the literature (Sanetti & Kratochwill, 2009; Zvoch, 2012). Lack of attention to FOI has implications for identification of causal influences of treatment on important child outcomes, establishment of evidence-based practices, and evaluation of how those practices are carried out in the field.
A Triadic Model of Early Intervention
Contemporary early intervention practice for young children involves use of a family-centered model. In such a model, professionals often teach and coach parents to use specific strategies for supporting their children’s development during their daily activities and routines. It is expected that caregivers will be the primary implementers of intervention strategies with their children. A triadic model of early intervention is one way to deliver services that meet these specifications (Salisbury & Cushing, 2013). In a triadic model of early intervention, the service provider works with the parent, who then implements strategies with the child, thereby impacting developmental outcomes. This model of early intervention practice requires parents to use the knowledge and skills they have acquired during home visits across routines and activities in their day to day lives. There are three key assumptions in this cascading model of intervention: (a) the provider effectively teaches and coaches the parent to use specific strategies for supporting child development; (b) parents learn these development supporting strategies during the home visit; and (c) parents apply these strategies accurately, consistently, and often enough to make a difference in the course of their child’s development (Roberts, Kaiser, Wolfe, Bryant, & Spidalieri, 2014).
A Framework for Measurement of FOI Within a Triadic Model of Intervention
The triadic model of early intervention is an indirect service delivery model where a second individual (i.e., the parent) implements intervention with the intended recipient (i.e., the child). This model must therefore involve measurement at two levels of implementation (Sanetti & Kratochwill, 2009; Sheridan, Swanger-Gagné, Welch, Kwon, & Garbacz, 2009). Because strict adherence to an intervention protocol may or may not be related to outcomes (Perepletchikova, 2011), it is necessary to conceptualize and measure FOI using multiple dimensions. Four aspects of FOI most relevant to the triadic model of early intervention practice include (a) dosage, (b) adherence, (c) quality (i.e., skill) of intervention delivery, and (d) participant responsiveness (Dane & Schneider, 1998; Dusenbury, Brannigan, Falco, & Hansen, 2003; Knoche, Sheridan, Edwards, & Osborn, 2010). (A fifth dimension, program differentiation, has been excluded because the focus of the current review is on specific parent and practitioner behaviors, not necessarily program or condition comparisons.) Dosage pertains to the actual amount of intervention provided. Adherence may be defined as a measure of whether all prescribed elements of an intervention were delivered accurately. Quality of intervention delivery indicates how well intervention strategies were delivered, and has been measured by looking at enthusiasm of the practitioner and interactions of the practitioner with participants (Dusenbury et al., 2003). Finally, participant responsiveness relates to the participant’s engagement in the intervention (Dusenbury et al., 2003; Knoche et al., 2010).
These four elements can be incorporated into the triadic model of early intervention service delivery to show the potential influences of FOI on child outcomes at the practitioner, parent, and child levels (see Figure 1). Figure 1 depicts the dimensions and levels of FOI that may be particularly important to measure in early intervention research to determine within the process how and why an intervention may or may not be affecting child outcomes, and where breakdowns in implementation may occur. Parent and child responsiveness are contained on the directional arrows to indicate the unique position of representing a dimension of FOI and engaging as a member of the triadic model of early intervention with measureable outcomes (i.e., parent FOI and child communication). It should be noted that implementing an intervention with fidelity across all dimensions at both practitioner and parent levels does not guarantee meaningful child and family outcomes. However, engaging in comprehensive measurement of FOI enables examination of those variables that may impact outcomes, and identification of potential problems within an indirect intervention delivery model.
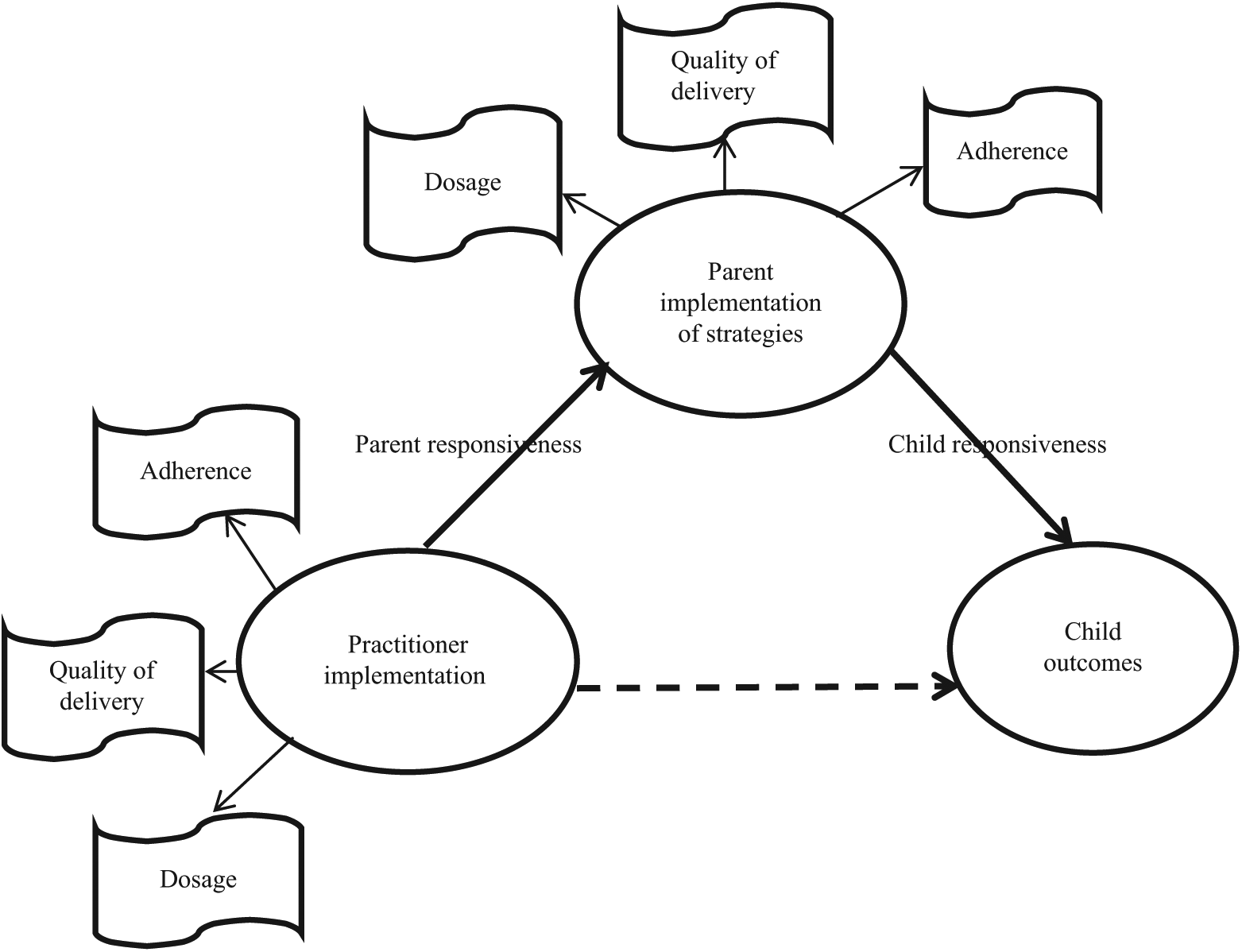
Triadic model of early intervention incorporating four elements of fidelity of implementation at practitioner and parent levels.
Current Measurement of FOI in Early Intervention Research
A 2002 review of the quantitative research examining early childhood intervention practices found that only 12.6% provided specific FOI data (Snyder, Thompson, McLean, & Smith, 2002). A more recent review of parent-implemented interventions in early intervention and early childhood special education found 79% of studies reported some measure of fidelity of parent implementation; however, only 29% of studies reviewed reported practitioners’ fidelity in training parents to implement intervention strategies (Barton & Fettig, 2013). In addition, in a meta-analysis of parent-implemented communication interventions, Roberts and Kaiser (2011) reported that 72% of studies did not report treatment fidelity, and that 50% of studies did not clearly describe parent-training procedures. However, neither Barton and Fettig (2013) nor Roberts and Kaiser differentiated between elements of FOI (i.e., dosage, adherence, quality, and responsiveness) for both practitioners and parents.
Despite calls for better reporting of implementation fidelity, limited information continues to exist across published studies in the early intervention literature. Such a lack of information regarding FOI limits what we know and understand regarding efficacious interventions for very young children with disabilities. A first step in understanding FOI reporting needs in applied settings is knowing how and to what extent FOI is reported in treatment research where parents are implementing part or all of treatment (i.e., when efficacy of a treatment is examined within a triadic model of intervention). Communication is an area of development particularly impacted in children with special needs across diagnostic categories. In addition, it is known that parents play an important role in their children’s communication and language development (Hart & Risley, 1995; Kaiser, Hancock, & Trent, 2007; Roberts & Kaiser, 2011). Hence, communication intervention research is well-suited for examining measurement of fidelity within a triadic model of intervention. The following review of the literature focuses on FOI reporting in parent-mediated communication interventions for young children with developmental delays and disabilities, and examines the four elements of FOI (dosage, adherence, quality, and responsiveness) at the practitioner and parent level.
Method
An electronic keyword search was conducted in the ERIC and Psycinfo databases of peer-reviewed articles using the phrases early intervention, early childhood, and language. A total of 509 abstracts were examined for the following criteria: (a) children 0 to 60 months were included in the sample; (b) single subject, group experimental, or quasi-experimental designs were used to examine research questions; and (c) studies involved parent training or parent implementation of communication intervention strategies. In addition, a hand search of references was conducted for McConachie and Diggle (2007), Roberts and Kaiser (2011), and Kong and Carta (2013). A total of 38 studies were eligible for review based on the above search and criteria. Two studies were excluded because they were not communication intervention studies. Two additional studies were excluded because they reported on the same sample as two other eligible studies (Girolametto, Pearce, & Weitzman, 1997; Warren et al., 2008). One study not captured during the original search due to recency of the publication date was included in the final review (Roberts et al., 2014).
Thirty-five studies were coded using a system adapted from Swanson et al. (2011) and Wheeler, Baggett, Fox, and Blevins (2006). Primary coding was conducted by the author of the current article. A second observer was trained in the use of the coding scheme, which involved meeting with the primary coder to review coding categories, joint coding of two studies, and independent coding of practice studies. Discrepancy discussions were held after each independently coded practice study. Once a criterion of 80% agreement across three studies was reached (calculated by dividing the number of agreements by the number of agreements plus disagreements and multiplying by 100), 31% of remaining, randomly selected studies were coded for agreement.
Results
Inter-Observer Agreement (IOA)
Eleven studies (31%) were independently reviewed by a second coder. Percentage agreement was calculated for (a) general characteristics (e.g., design, sample size, age of sample) and FOI study characteristics together and (b) study characteristics related only to FOI (e.g., FOI on practitioner and/or parent implementation, whether FOI scores were reported or used in analyses, etc.). Average IOA across all study characteristics was 85% (SD = 12); average IOA on FOI study characteristics alone was 80% (SD = 19). Discrepancy discussions and consensus coding were conducted for studies where IOA fell below 80% (n = 3).
General Study Characteristics
A total of 1,148 children participated in the 35 studies reviewed in the current article. Four studies reported the smallest sample size across studies (n = 3; Gillett & LeBlanc, 2007; Peterson, Carta, & Greenwood, 2005; Rocha, Schreibman, & Stahmer, 2007; Schertz & Odom, 2007). Green et al. (2010) and Ward (1999) reported the largest sample sizes with 152 and 122 participants, respectively. Participants ranged in age from 10 months to 6 years, with 27 studies (77%) including children below the age of 3 years. Twenty studies (57%) used a randomized controlled design, 5 (14%) used a quasi-experimental group design, and 10 studies (29%) used a single case design. The parent was the primary implementer in 29 studies (83%). Both parents and practitioners implemented intervention with children in 5 studies (14%), and the therapist was the primary implementer of intervention in 1 study (3%). This study was included in the current review because the intervention involved parent training of responsive communication behaviors.
Eight studies (23%) implemented parent training in the home, 12 studies (34%) implemented parent training in a community setting such as a clinic or classroom, 11 studies (31%) implemented parent training in a combination of home and community settings, and 3 studies (9%) implemented parent training in a home or community setting, which varied by participant. One study did not specify where parent training occurred. Twenty-six studies (74%) measured child outcomes using norm-referenced, standardized assessments; 31 studies (89%) measured child outcomes using observational measures (e.g., parent–child interaction); and 9 studies (26%) reported Mean Length of Utterance as a child outcome (see Table 1 for general study characteristics). All studies reported an increase in at least one child communication or language outcome, although because studies were not reviewed in the current article for methodological rigor, interpretation of meaningfulness of child outcomes is limited.
General Study Characteristics.
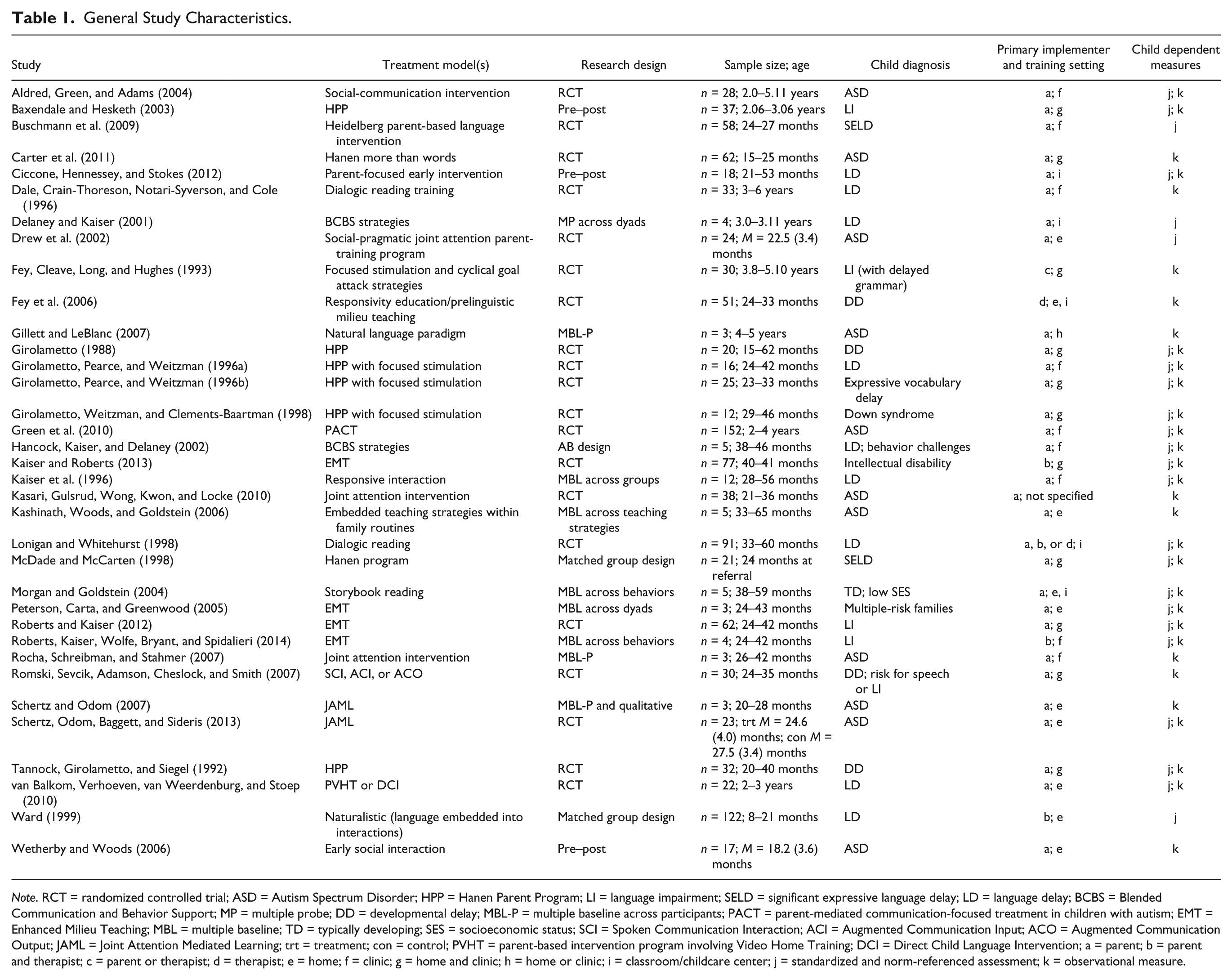
Note. RCT = randomized controlled trial; ASD = Autism Spectrum Disorder; HPP = Hanen Parent Program; LI = language impairment; SELD = significant expressive language delay; LD = language delay; BCBS = Blended Communication and Behavior Support; MP = multiple probe; DD = developmental delay; MBL-P = multiple baseline across participants; PACT = parent-mediated communication-focused treatment in children with autism; EMT = Enhanced Milieu Teaching; MBL = multiple baseline; TD = typically developing; SES = socioeconomic status; SCI = Spoken Communication Interaction; ACI = Augmented Communication Input; ACO = Augmented Communication Output; JAML = Joint Attention Mediated Learning; trt = treatment; con = control; PVHT = parent-based intervention program involving Video Home Training; DCI = Direct Child Language Intervention; a = parent; b = parent and therapist; c = parent or therapist; d = therapist; e = home; f = clinic; g = home and clinic; h = home or clinic; i = classroom/childcare center; j = standardized and norm-referenced assessment; k = observational measure.
FOI Reporting
The following sections examine reporting of four elements of FOI across the practitioner and parent levels: (a) dosage, (b) adherence, (c) quality, and (d) participant responsiveness (see Table 2). Dosage was evaluated based on reporting of the amount of training delivered by providers to parents, and the amount of strategy use by parents with their children. Adherence was evaluated based on reporting of the use of self- or other-completed checklists to track accuracy of implementation, observational coding of parent-training sessions and/or parent–child sessions, and/or measurement of parent implementation as a dependent variable. Quality was evaluated based on the reporting of additional information pertaining to skill of delivery, use of a criterion for mastery, and/or frequency or rate of strategy delivery. Rate of strategy use has been defined elsewhere as adherence (e.g., Knoche et al., 2010); however, it was felt that frequency or rate of strategy use differs from adherence in that two individuals could carry out a language-promoting strategy with sufficient adherence, but an individual providing a higher frequency of those strategies during a treatment session may be providing the child more opportunities for language learning (and hence implementing at a higher quality). Finally, participant responsiveness was evaluated based on the reporting or observation of engagement of participants during training or treatment sessions. This may include parent attendance data, report of parent satisfaction for the intervention through questionnaires or interviews, and/or parent-report or direct observation of the child as the parent implemented newly learned strategies.
Aspects of FOI Reported at Practitioner and Parent Levels.
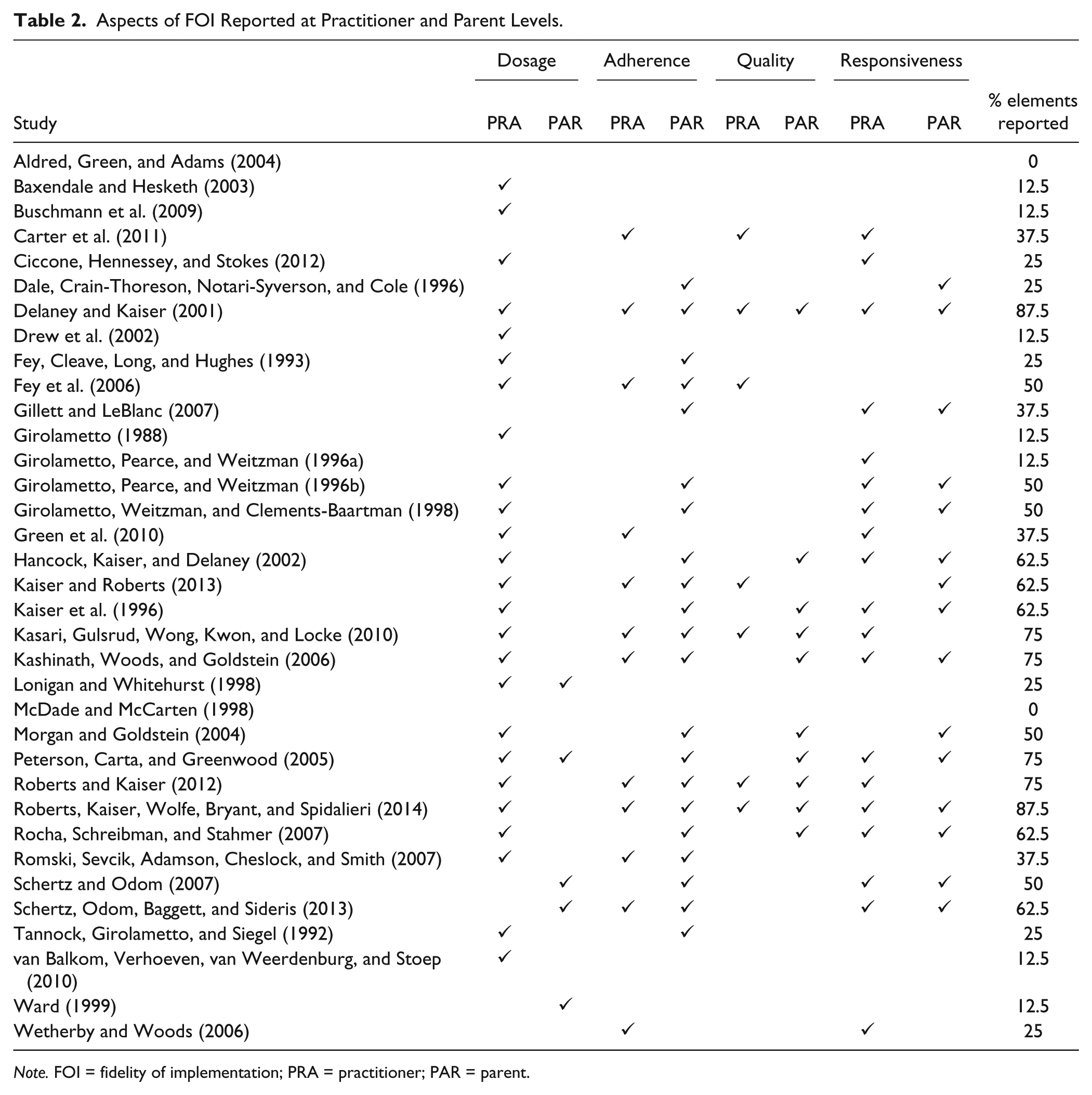
Note. FOI = fidelity of implementation; PRA = practitioner; PAR = parent.
Dosage
Seventy-one percent of studies (n = 25) reported adequate information on treatment dosage at the training or practitioner level, defined here as reporting the number of sessions and session length, with either the length of treatment reported or the frequency of intervention. For those studies that did not meet the criteria for adequate dosage reporting, 9 out of the 10 did not report the length of the sessions.
Fourteen percent of studies (n = 5) included information regarding how often parents implemented learned strategies with their children outside of the parent-training context (i.e., dosage at the parent level; Lonigan & Whitehurst, 1998; Peterson et al., 2005; Schertz & Odom, 2007; Schertz, Odom, Baggett, & Sideris, 2013; Ward, 1999). On their study of parent and teacher-implemented dialogic reading, Lonigan and Whitehurst (1998) had parents and teachers fill out daily logs of when they used dialogic reading and the books that were used during these sessions. Peterson et al. (2005) asked parents to practice milieu language teaching skills twice a week and record the date and time of their sessions. Parents were asked to tape record the sessions for verification by researchers. Schertz and Odom (2007) asked parents to engage in approximately 1 hr of strategy use from Joint Attention Mediated Learning (JAML) per day, and record daily notes on those sessions. In a second study of the JAML intervention, parents committed to 30 min a day of engagement with their toddler using intervention strategies within daily activities and wrote down the approximate time spent within such activities (Schertz et al., 2013). Finally, Ward (1999) reported the average time each day parents spent carrying out play sessions and other activities with their children based on parent-report.
Adherence
Twelve of the 35 studies (34%) reported information regarding adherence to intervention/treatment at the practitioner level. Four of the 12 studies (33%) reported use of a self-checklist of implementation of intervention (Carter et al., 2011; Morgan & Goldstein, 2004; Schertz et al., 2013; Wetherby & Woods, 2006). Carter et al. (2011) and Schertz et al. (2013) reported agreement data with an independent observer on the self-checklists completed by the interventionists. Two of the 12 studies (17%) reported a second observer completed a checklist of implementation of intervention (Delaney & Kaiser, 2001; Romski, Sevcik, Adamson, Cheslock, & Smith, 2007); 4 of the 12 studies (33%) reported coding practitioner use of specific strategies of implementation (Fey et al., 2006; Kaiser & Roberts, 2013; Roberts & Kaiser, 2012; Roberts et al., 2014). Two studies used a checklist to measure practitioner adherence to intervention procedures, but did not indicate whether the checklists were completed by interventionists or independent observers (Kasari, Gulsrud, Wong, Kwon, & Locke 2010; Kashinath, Woods, & Goldstein, 2006).
Twenty-one of the 35 studies (60%) reported information regarding adherence to intervention/treatment at the parent level (11 single case design and 10 group design studies). Seven of the 11 single case studies (64%) directly measured parent strategy use through visual analysis (Delaney & Kaiser, 2001; Hancock, Kaiser, & Delaney, 2002; Kaiser et al., 1996; Kashinath et al., 2006; Morgan & Goldstein, 2004; Peterson et al., 2005; Roberts et al., 2014). Delaney and Kaiser (2001) also provided mean levels of nine trained parent behaviors during baseline and after training. Eight of the 10 group design studies (80%) measured parent behaviors specifically taught through the intervention as a dependent variable (Dale, Crain-Thoreson, Notari-Syverson, & Cole, 1996; Fey, Cleave, Long, & Hughes, 1993; Fey et al., 2006; Girolametto, Pearce, & Weitzman, 1996b; Girolametto, Weitzman, & Clements-Baartman, 1998; Kaiser & Roberts, 2013; Roberts & Kaiser, 2012; Tannock, Girolametto, & Siegel, 1992). Parent strategy use as a dependent variable was only considered an indicator of adherence if the treatment was well-described in the study and the parent dependent variable was a measure of those strategies explicitly taught to parents. Nine of the 21 studies (43%) measured adherence at the parent level using other-completed checklists or observers of audio- or video-recorded sessions (Gillett & LeBlanc, 2007; Girolametto et al., 1996b; Girolametto et al., 1998; Kasari et al., 2010; Roberts & Kaiser, 2012; Roberts et al., 2014; Rocha et al., 2007; Romski et al., 2007; Schertz et al., 2013). Three of the 21 studies (14%) used parent self-report as a measure of adherence to treatment (Girolametto et al., 1998; Schertz & Odom, 2007; Schertz et al., 2013).
Quality
Seven of the 35 studies (20%) reported information regarding the quality with which treatment was delivered by practitioners. One study did not provide enough information to determine whether their FOI procedures measured quality (Schertz et al., 2013). Carter and colleagues (2011) described their FOI checklist as containing an assessment of “quality of teaching style” (p. 745). Delaney and Kaiser (2001) assessed “management of the training process by the parent educator” and “content provided during the session by the parent educator” in addition to adherence to the actual components of the intervention in their FOI measure. In addition to measuring whether practitioners implemented successful teaching episodes, Fey et al. (2006) enlisted uninformed graduate assistants to judge whether practitioners were implementing prelinguistic milieu teaching or milieu teaching, and identify primary objectives being addressed within the treatment sessions they viewed. Kaiser and Roberts (2013), Roberts and Kaiser (2012), and Roberts et al. (2014) determined a criterion level against which to measure implementation of all treatment strategies. Kasari et al. (2010) used a rating system of practitioner implementation that looked at how well trainers carried out strategies.
Ten of the 35 studies (29%) reported some measure of the quality of parents’ implementation of communication strategies. The majority recorded the frequency or rate of parent strategy use, or used a preset criterion by which to judge strategy use (Delaney & Kaiser, 2001; Hancock et al., 2002; Kaiser et al., 1996; Kashinath et al., 2006; Morgan & Goldstein, 2004; Peterson et al., 2005; Roberts & Kaiser, 2012; Roberts et al., 2014; Rocha et al., 2007). A single study had practitioners report directly on quality of parents’ implementation of intervention strategies, and had parents provide a self-report of whether they felt confident and competent in using strategies taught to them by the practitioner with their children (Kasari et al., 2010).
Participant responsiveness
Nineteen of the 35 studies (54%) provided some measure of participant responsiveness at the practitioner level. Six of the 19 studies (32%) provided information regarding parent attendance to treatment (Girolametto, Pearce, & Weitzman, 1996a, 1996b; Girolametto et al., 1998; Green et al., 2010; Roberts & Kaiser, 2012; Schertz & Odom, 2007). Ten of the 19 studies (53%) provided a parent satisfaction questionnaire (Carter et al., 2011; Ciccone, Hennessey, & Stokes, 2012; Gillett & LeBlanc, 2007; Girolametto et al., 1996a; Girolametto et al., 1998; Kaiser et al., 1996; Kashinath et al., 2006; Peterson et al., 2005; Rocha et al., 2007; Schertz et al., 2013). Six of the 19 studies (32%) provided some other measure of parent engagement information for the intervention (Delaney & Kaiser, 2001; Hancock et al., 2002; Kasari et al., 2010; Roberts & Kaiser, 2012; Wetherby & Woods, 2006). Delaney and Kaiser (2001) and Hancock et al. (2002) used a semi-structured interview to measure parent satisfaction with the intervention. Roberts and Kaiser (2012), Roberts et al. (2014), and Wetherby and Woods (2006) built discussions with parents regarding their satisfaction with programs and engagement into coaching sessions. Kasari et al. (2010) asked parents to report on whether they made time to carry out strategies outside of parent-training sessions.
Fifteen of the 35 studies (43%) provided some measure of participant responsiveness at the parent level. In 10 single case design studies, researchers measured child behaviors as they were interacting with parents during treatment sessions (Delaney & Kaiser, 2001; Gillett & LeBlanc, 2007; Hancock et al., 2002; Kaiser et al., 1996; Kashinath et al., 2006; Morgan & Goldstein, 2004; Peterson et al., 2005; Roberts et al., 2014; Rocha et al., 2007; Schertz & Odom, 2007). In five group design studies, researchers measured targeted child behaviors within parent–child observation contexts (Dale et al., 1996; Girolametto et al., 1996b; Girolametto et al., 1998; Kaiser & Roberts, 2013; Schertz et al., 2013). Delaney and Kaiser (2001) and Hancock et al. (2002) asked parents to talk about the “effectiveness of the intervention strategies with their [children]” as part of a semi-structured interview of parent satisfaction. Finally, Schertz et al. (2013) asked parents to report on their child’s engagement during home strategy use.
Discussion
The above review supports previous findings of limited FOI reporting in parent-mediated early intervention research. Out of eight possible FOI elements (four each at the practitioner and parent levels), 9 studies reported zero or one of the FOI elements, 20 studies reported between two and five of the FOI elements, and 6 studies reported between six and eight of the FOI elements. Regarding possible trends toward increased FOI reporting over time, 73% of studies published between 1988 and 2000 (n = 11) reported between zero and two elements and 0% reported between six and eight elements, whereas 29% of studies published between 2001 and 2014 (n = 24) reported between zero and two elements and 25% reported between six and eight elements. Results of the review indicate that the highest levels of reporting on FOI dimensions occurred for dosage at the practitioner level (71% of studies) and adherence at the parent level (60% of studies). Relatively low rates of reporting of FOI occurred for the remaining elements at both the practitioner and parent levels, including only 34% of studies reporting practitioner adherence to parent-training strategies. The lowest rates of reporting occurred for practitioner quality (20% of studies) and parent dosage (14% of studies). This latter finding is somewhat discouraging as the presumed efficacy of parent-mediated intervention is due in large part to the fact that parents have many more opportunities across the day to implement strategies.
It is clear that collection of FOI data at the practitioner and parent levels is necessary for a rigorous examination of parent-mediated early intervention, and is an important way scientists can bridge the gap from research to practice in the field of early intervention. However, barriers to measurement and reporting of FOI at both levels of a triadic model of early intervention exist. Several important challenges in measurement of FOI often arise with an indirect service delivery model including (a) lack of standardized protocols or manuals for teaching, coaching, and child treatment, (b) interventions involving multiple components conditional on context (e.g., family situation, home environment, parental behavior), (c) implementation of the intervention by individuals (i.e., parents) with limited specialized training in the treatment, (d) complex ecological variables that differ between families and influence child outcomes (e.g., cultural background, socioeconomic status [SES], family structure), and (e) the need for highly individualized services (Sheridan et al., 2009). In addition, valid and reliable tools to measure FOI at the practitioner and parent level are not in widespread use. Indeed, Sanetti and Kratochwill (2009) stated that “despite acknowledgement by researchers and, to a lesser degree, practitioners that treatment integrity assessment is a key feature of intervention evaluation, there has been minimal development of feasible and efficient treatment integrity assessments with adequate psychometric properties” (p. 451). Clearly serious challenges exist in measuring and reporting FOI in a model of service delivery where the parent acts as the primary implementer of often complex intervention strategies.
Recommendations for Measurement of Dosage, Adherence, Quality, and Responsiveness
To optimize child and family outcomes, it is important that FOI data be collected and reported in research and applied settings. A necessary step in this endeavor is development and use of appropriate measurement tools to track the four elements of FOI described above. Thorough reporting of dosage at the practitioner level should involve information regarding the number of parent-training sessions provided, the length of those sessions, and the duration of the intervention. Such detail in the research literature can inform practitioners when determining the best-fitting parent-training model for a particular family, as well as feasibility of implementing the training in applied settings. Dosage at the parent level is vitally important in understanding results of efficacy studies in early intervention. An important assumption of the triadic model is that parents are providing intervention at sufficient levels to affect change in their child’s development. If researchers do not measure the amount of treatment delivered by parents, it will be difficult to determine whether strategies were or were not effective due to amount of implementation on the part of the parent. Admittedly, dosage at the parent level is difficult to measure accurately in research, and perhaps even more so in practice. However, it will serve the field to determine ways to measure this element of fidelity when implementing parent-mediated interventions.
Adherence data at the practitioner level may be collected based on parent-training sessions using methods such as checklists or coding of observational data. Reliable collection of adherence data requires practitioner implementation strategies be well-defined; however, practitioner behaviors such as teaching and coaching have not been well-specified for the field. Therefore, in addition to development of appropriate measurement tools, models of teaching and coaching used with parents involved in early intervention need to be well-described in the literature. At the parent level, researchers and practitioners may also collect adherence data using methods such as checklists or observations of the parent and child during treatment sessions. Information regarding adherence may also be collected outside of the treatment session through parent self-report of use of strategies, or audio or video recording of parent and child outside of the treatment context. Increased availability of recording technology may allow this type of data collection to occur more readily, and could provide valuable insight into whether parents are able to accurately use intervention strategies when the practitioner is not present.
Quality may be the most challenging element to operationalize for measurement. However, it is logical that there is something beyond carrying out steps of an intervention that increases or decreases the efficacy of the treatment. At both the practitioner and parent levels, elements of quality may involve the frequency with which strategies are used during an intervention session, whether a certain percentage of steps are carried out consistently (i.e., a pre-set criterion for strategy use), and/or whether practitioners and parents have confidence and feel competent with their implementation. The above aspects of quality may be measured through self- or other-report, and/or through observation of parent-training sessions or parent–child sessions.
Finally, participant responsiveness is a measure of engagement of the recipient of training or treatment, and can provide insight into how well-received implemented strategies are on the part of the parent and child. Parent engagement (i.e., participant responsiveness at the practitioner level) may be measured by attendance to parent-training sessions, and/or satisfaction with the treatment process as reported through a questionnaire or interview data. Measures of parent satisfaction overlap with the construct of social validity, and may provide insight into the likelihood that parents were highly engaged during sessions and with intervention strategies outside of the treatment context. Child engagement (i.e., participant responsiveness at the parent level) may be measured through direct observation of the child during parent–child sessions, and may also be reported by parents outside of the training context.
Measurement strategies described above were all found within the studies included in the review, although no one study measured all elements of FOI at the parent and practitioner level. Challenges of collecting extensive FOI data are recognized and appreciated, including the introduction of bias and measurement error when using self-report tools. In addition, asking a busy parent to complete a checklist or collect data on strategy implementation may conflict with the model of embedding interventions into family routines to reduce the burden on families of carrying out intervention. However, comprehensive collection and reporting of FOI data is an important step in determining evidence-based practice for providers working within an indirect service delivery model of early intervention. As researchers develop valid, reliable, and less disruptive methods for collecting FOI data, use of such methods will become more readily available and prevalent for practitioners in the field of early intervention, thereby improving outcomes for young children and families involved in early intervention. One important step in that direction includes incorporating technology into collection of FOI data. For example, one device created to assess the language environment of children is the Language ENvironment Analysis (LENA) system. The LENA provides up to 16 hr of continuous recording of the target child’s immediate language environment through a small device inserted into the child’s clothing, and provides information on child utterances, adult words directed to the child, and conversational turns. Used appropriately, this device (or similar unobtrusive methods) may allow for more accurate and extensive collection of FOI data for both practitioners and parents that ultimately lead to better decision making around programs for young children with communication and language delays.
Limitations
The main purpose of this review was to evaluate components of FOI reporting in the parent-mediated communication literature. Therefore, studies involving other types of parent-mediated interventions and child outcomes were not included. In addition, rigor of the study design and overall quality were not rated as part of this review. Therefore, conclusions cannot be drawn regarding overall quality of the studies and impact on child outcomes. Although extensive, it is noted that this review may not be exhaustive of all parent-mediated communication treatment studies. However, it may be considered representative of the extant literature. Finally, complexity of the interventions implemented across the reviewed studies was not examined. Logically, parents may have an easier time implementing interventions that are less complex and/or include strategies that can easily be incorporated into daily routines and activities. How complexity relates to implementation is beyond the scope of this review, but is an important area of future research in FOI.
Future Directions
Future research on parent-mediated intervention should focus on collecting data and reporting the elements of FOI described above, and examining the relationships between dimensions of FOI and participant outcomes. To do this in a systematic fashion, valid and reliable tools that measure implementation at the practitioner and parent level need to be developed and made available. Such FOI tools could be included as part of manualized interventions, and/or could be developed by researchers for use in and out of the lab. A “gold-standard” for measuring FOI involves coding practitioner and provider implementation through direct observation of intervention sessions (Bellg et al., 2004). Use of continuous recording devices such as LENA could allow for direct measures of the child’s language environment without adding much burden to families. Although not an established use for the LENA, research into measurement of FOI could examine the utility of this device for such a purpose. Furthermore, development and evaluation of FOI measures remains an important area of future research in the field. Validity and reliability studies of currently available fidelity tools will help ensure that accurate measures of FOI are readily available for researchers and practitioners alike.
In addition, measuring individual elements of FOI and including them in analyses examining parent and child variables can help tease apart whether certain elements have a greater influence on outcomes than others. It is possible that different dimensions of FOI will impact participant outcomes to different degrees (i.e., some may be more important than others). Understanding the strength of associations between specific dimensions of FOI and parent and child outcomes can provide direction in what to emphasize when implementing parent-mediated interventions. For example, if quality and dosage at the parent level are found to mediate child outcomes, while adherence does not, practitioners may want to focus more on working with families to increase the amount of implementation with their children and the quality of that implementation. Such questions are important areas for future investigation, specifically through the use of randomized controlled trials that can detect mediating and moderating associations among measured variables.
Finally, editors and reviewers of parent-mediated treatment research should consider levels of FOI reporting when making decisions regarding publications of intervention studies. A similar recommendation was made by Snyder and colleagues in their 2002 review, and remains relevant today. Because lack of such data limits interpretability of results, FOI reporting is critical for establishing evidence-based practices for the field of early childhood intervention.
Conclusion
To date, limited FOI data have been reported in the parent-mediated communication literature, as well as the early intervention literature more broadly. A lack of reporting on the four components of FOI described in this article limits our understanding of the implementation and efficacy of parent-mediated interventions, and therefore how best to bridge the gap from research to practice. Attention to dosage, adherence, quality, and participant responsiveness at the practitioner and parent levels is one way researchers can begin to unpack the black box of parent-mediated treatment, and determine evidence-based practices that can be more successfully provided to young children with disabilities and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.