
Abstract
Early intervention providers (EI) have a responsibility to enact recommended practices to best support young children with disabilities and their families. However, pre-service and in-service preparation of early intervention providers is complex and often lacking, leading to gaps in practice. In this qualitative study, we aimed to understand what supports and barriers EI providers in the U.S. state of Illinois experience that they believe influence their practices. Overall, we developed four themes that represent the data: (1) systemic barriers, (2) collaboration as a support and barrier, (3) key experiences as supports, and (4) the need for meaningful professional development. Implications include the need for policies that address financial concerns and collaborative teaming, as well as personnel development focused on effective teaming and responding to diverse family needs.
Keywords
Under Part C of the Individuals with Disabilities Education Improvement Act (IDEA, 2004), infants and toddlers with delays and disabilities can receive early intervention (EI) services. EI services aim to reduce the need for special education and disability services later in an individual’s life by intervening early. These services differ from school-based services as they typically occur in the child’s home or community settings (rather than a school), and professionals focus on building the family’s capacity to promote their child’s development, rather than intervening directly with the child (Early Childhood Technical Assistance [ECTA], 2023). Professionals who deliver EI services (i.e., EI providers) come from a variety of disciplines and educational backgrounds, such as early childhood special education, speech-language pathology, occupational therapy, and physical therapy (IDEA, 2004). The federal law provides overarching requirements for Part C EI services, but individual states oversee implementation of the EI program (ECTA, 2023). For example, IDEA requires that children with disabilities and delays receive EI services, but states determine the specific eligibility requirements, such as the percentage of delay needed. Similarly, the law requires that states develop a comprehensive system of personnel development (CSPD); however, each state determines what the CSPD entails.
The purpose of a CSPD is to ensure that EI providers are qualified and trained to use recommended practices in the field to support families (IDEA, 2004). Recommended practices in EI derive from a variety of sources, including the Division for Early Childhood (DEC)’s (2014) recommended practices, the Workgroup on Principles and Practices in Natural Environments (2008), and the Early Childhood Personnel Development’s cross-disciplinary competencies (Bruder et al., 2019). Recommended practices cross multiple topic areas, such as collaboration, family-centered practice, assessment, transition, and professionalism (Bruder et al., 2019; DEC, 2014; Whipple, 2014; Workgroup on Principles and Practices, 2008). Specific examples of recommended practices include building families’ capacities to support their children, using a transdisciplinary teaming model, and embedding intervention into daily routines (Boyer & Thompson, 2014; DEC, 2014; Workgroup on Principles and Practices, 2008).
Personnel development for both in-service and pre-service practitioners is essential for ensuring recommended practices are implemented. Several researchers have found that participants need high-quality training on topics related to recommended practices, such as how to build families’ capacities (e.g., Douglas et al., 2020; Stewart & Applequist, 2019). However, years of research have indicated that personnel development in EI is complex and often lacking (Bruder & Dunst, 2005; Chen & Mickelson, 2015). Given that EI providers represent various disciplines, there are inconsistencies across their personnel preparation and training, often leading to gaps in EI providers’ knowledge and skills (Bruder, 2010; Bruder & Dunst, 2005; Bruder et al., 2019; Campbell & Sawyer, 2009; Catalino et al., 2015; Childress et al., 2019; Malone et al., 2000). Professional development (PD) for in-service providers often focuses on single-event trainings, which are not sufficient for improving EI providers’ practices (Dunst et al., 2011; Malone et al., 2000). Instead, ongoing, capacity-building PD is needed to increase EI providers’ use of recommended practices (Dunst et al., 2020; Meadan et al., 2020).
EI providers’ use of recommended practices is also influenced by factors aside from formal training. For example, researchers have found that EI providers report learning how to implement family capacity-building practices by seeking information from current research, engaging in reflection, and collaborating with other professionals (Douglas et al., 2020; Williams & Ostrosky, 2023). Additionally, several studies indicated that participants believed that the quality of their services and use of family-centered practices were dependent on families, such as the caregiver’s level of involvement, the composition of the family, and the family’s culture (Douglas et al., 2020; Fleming et al., 2011; Meadan et al., 2018, 2020; Spence et al., 2022; Stewart & Applequist, 2019; Tomczuk et al., 2022).
Given the legal and professional requirements in place to ensure the quality of EI services, this qualitative study aimed to identify specific facilitators and barriers of EI providers’ understanding and use of best practices. Identifying facilitators and barriers from practitioners’ viewpoint helps the field in several ways, including (1) supporting continual improvement of CSPD programs, (2) influencing EI policies and procedures, and (3) guiding researchers in critical issues to investigate. The following research question guided the study: What supports and barriers do EI providers in one state report as impacting how they deliver EI services?
Method
This research study is part of a larger mixed methods study that explored EI providers’ beliefs about and use of recommended practices in EI (Hardy et al., 2024). In this paper, we present only the qualitative data related to EI providers’ beliefs about what supports and hinders their use of recommended practices. We combined qualitative survey data and qualitative interview data to answer the research question.
Positionality
Reporting on positionality is one indicator for high-quality qualitative research, in which researchers reflect on how their positions (e.g., beliefs, experiences, position of power) affect their decisions and interactions throughout the research process (Brantlinger et al., 2005; The QR Collective, 2023). The research team for this study included two graduate students and two special education faculty, all of whom are white women. Each team member brought experience and knowledge that were essential to the study. Collectively, we had representation from a practicing EI provider (first author), a pre-service EI provider (third author), and individuals who help prepare EI providers (second and fourth author). All authors have experience providing in-service training to practicing EI providers. We used our experiences in these areas to design the study, recruit participants, develop rapport with participants, and analyze the data. For example, as a practicing professional, the first author was a member of several EI provider social media groups that we used for recruitment. Also, the third author who conducted the interviews had recently completed a field placement in EI. Her curiosity and recent experience in the field likely contributed to participants viewing her as a peer with whom they were sharing their expertise.
Participants and Setting
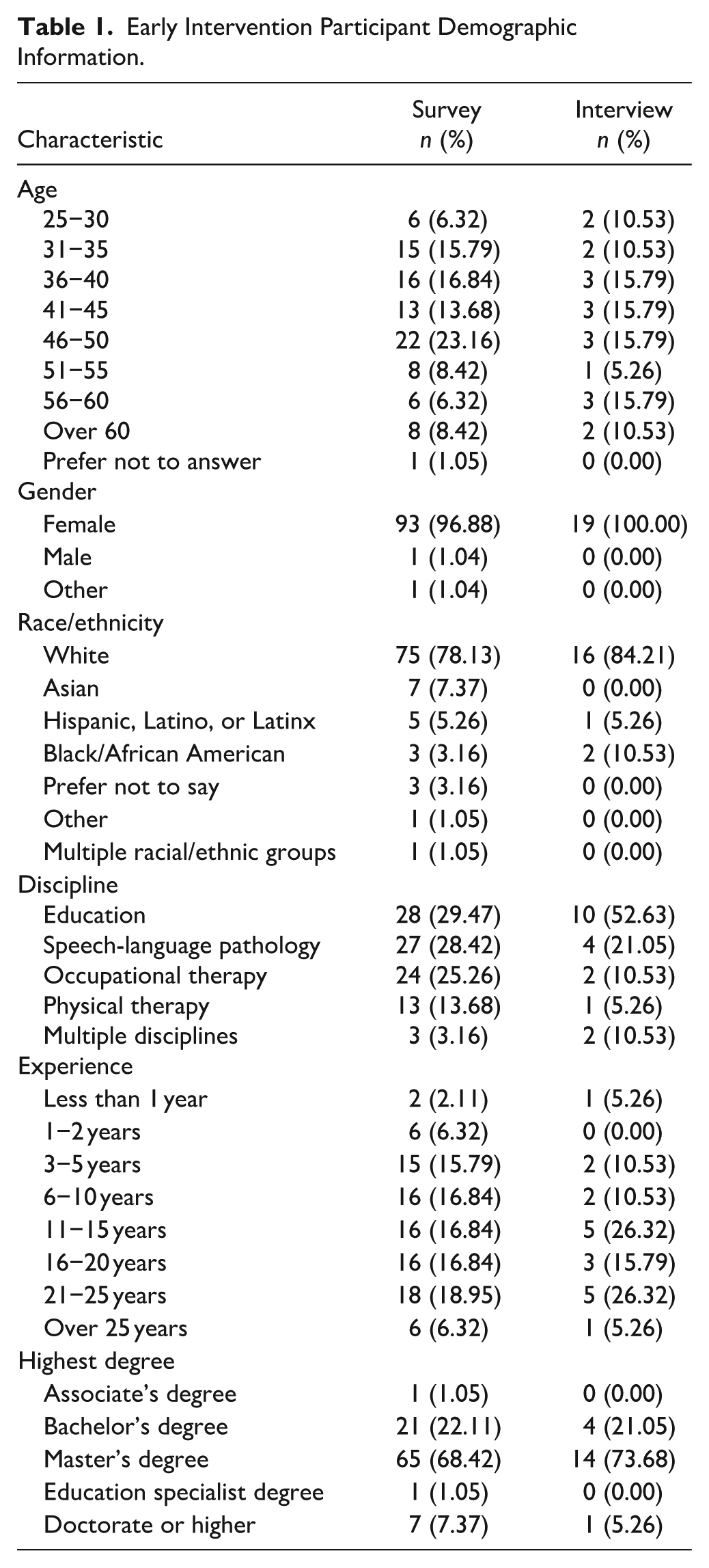
This study included two sets of participants: 95 survey participants and 19 interview participants (a subset of the survey participants). To be included in the survey, participants had to be an EI provider in Illinois and represent one of four main disciplines. These disciplines included EI educators, speech language pathologists (SLPs), occupational therapists (OTs), and physical therapists (PTs). EI educators are EI personnel who provide the service special instruction; these providers are known by various names depending on their state, including developmental therapists, developmental specialists, or early childhood special educators (DEC, 2024). A few participants served in one of the four main roles in addition to another role, which they wrote in a comment on the survey (e.g., EI educator and behavior). Overall, both sets of participants were primarily white females with master’s degrees. Each of the main disciplines were represented across the survey and interview. Participants also represented a variety of age ranges and years of experience in EI. More than half of the survey participants (n = 53, 55.79%) and interview participants (n = 11, 57.89%) were independent providers, who worked directly for the state, rather than an EI agency (see Table 1 for additional information).
Early Intervention Participant Demographic Information.
In llinois, EI services are housed in the Department of Human Services, and there are 25 regional points of entry. All EI providers hold a credential with core knowledge in four competencies: typical/atypical development, working with families, intervention strategies, and assessment (Provider Connections, n.d.). EI providers can work “independently” through the state as contractors or for private agencies who contract with the state. Families often receive ongoing services from multiple providers, rather than from one primary service provider. Also, EI providers in the state have the option to co-treat together, in which two members on the team deliver services at the same time. In 2022, the state permanently authorized telepractice as a service delivery option (Illinois Department of Human Services, 2022).
Data Collection
Instruments
We used a survey and interview protocol to collect data, which were developed in collaboration by the research team. The survey had quantitative and qualitative questions. In this paper, we focus on three qualitative items: (1) Briefly describe the biggest challenges you face as an EI provider, (2) Briefly describe the biggest benefits or successes you experience as an EI provider, and (3) Briefly describe what a successful EI session looks like for you. Participants were asked to leave their contact information if they were interested in completing an interview. The interview protocol included seven broad questions, three of which are the focus of this paper: (1) What challenges have you experienced with applying best practices? (2) What are the best opportunities you have received to expand your knowledge and skills related to EI best practices? (3) What opportunities have you provided to expand other practitioners’ knowledge and skills related to EI? We used the term “best practices” during interviews to avoid confusion with any specific recommended practices (e.g., DEC Recommended Practices) and to encourage participants to construct what they believe is best in the field. We report additional detail on the survey instrument and interview protocol in another paper (Hardy et al., 2024).
Procedures
Pilot
Prior to data collection, we received institutional review board approval and piloted the study in April 2022. Seven practicing EI providers in Illinois participated in the pilot. We asked the participants to provide feedback on the time it took to complete the survey and interview, how easy it was to navigate the survey, how easy it was to understand the survey and interview questions, and any other suggestions they had. Pilot participants gave only positive feedback about the survey. Suggestions related to the interview questions were related to clarity, which we addressed by adding words, providing examples, breaking questions into multiple parts, and displaying the questions on the screen during interviews.
Survey recruitment and compensation
Recruitment began in May 2022 using social media, email, and phone calls. We contacted regional EI coordinators by email and phone to ask them to share our recruitment flyer to EI providers in their region. We also posted the flyer in EI-related Facebook groups. The recruitment flyer included a link/QR code to a screening survey, which prevented bots or individuals who were not EI providers from doing the survey. Each participant read a consent form and consented to participate before moving on to the survey questions. After 10 weeks of collecting responses, we closed the survey and began recruiting for the interview. Twenty randomly-selected survey participants received a $15 gift card.
Interview recruitment and compensation
We purposefully selected participants with the highest and lowest mean scores on the survey rating scale questions to participate in the interviews to understand a wide range of perspectives. We contacted 36 survey participants by email; 19 agreed and completed the interviews. Each interview participant received a $20 gift card as compensation. The interviews were conducted via Zoom in July and August of 2022 by the third author. Each participant verbally consented to participate and have their interview recorded. The interviews were recorded and transcribed using Zoom and lasted between 18.50 minutes and 50.00 minutes (M = 30.75). A graduate research assistant and professional transcriber reviewed the transcripts for errors and corrected them. After each interview, the third author wrote a reflexive memo summarizing her initial thoughts and key quotes. The first author completed a member check with participants. She read each transcript as soon as possible after the interview, wrote a one-page summary of the interview, and emailed the summary to the participant. Participants were prompted to review the summary and provide clarifications or confirm its accuracy. Of the 18 participants who responded, two made minor clarifications to their summaries. All the data associated with the study (e.g., survey responses, transcripts, summaries) were de-identified and stored securely in a password-protected FERPA-compliant cloud-based folder. Participants’ names were replaced with their participant number.
Data Analysis and Credibility
We used Braun and Clarke’s (2006) six-phase thematic analysis process to analyze the qualitative survey and interview data. First, we familiarized ourselves with the data by reading through the data, conducting member checks, and writing reflective memos. In the second phase, we developed initial codes for the data. All four authors coded the three qualitative survey questions. Then, the second and fourth author met to come to agreement on the codes and develop a codebook. The first and third authors coded the interview data. They independently coded each interview one at a time—continually meeting to discuss codes, reach consensus, and develop/refine the codebook. Throughout data analysis, all four authors met to debrief. After all the data were coded, all four authors reviewed both the survey and interview codebooks and data, took notes about potential themes, and met to develop initial themes. The first and second author refined the themes, referring to the data to ensure the themes represented the data. We also created a thematic map, which shows each code that represents each theme (see Figure 1).
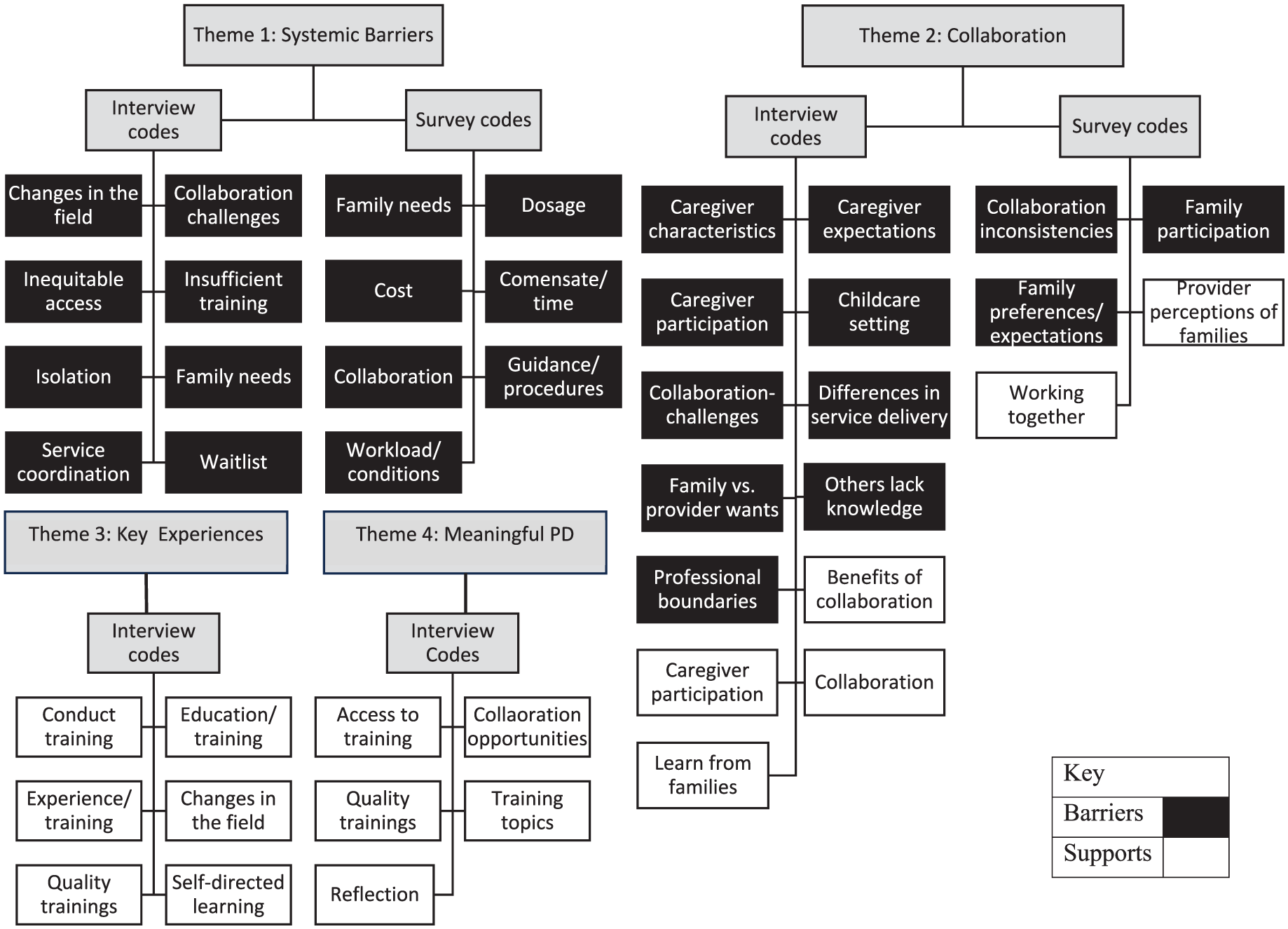
Thematic map.
We used quality indicators for qualitative research to ensure our analysis was credible. These indicators include reflexivity, collaborative work, member checks, and providing rich descriptions (Brantlinger et al., 2005; The QR Collective, 2023). We engaged in reflexivity by reporting our positionality and writing reflective memos during interview data collection. Our collaborative work included developing the research instruments as a team, piloting our materials and eliciting feedback from multiple individuals, and coding the data in groups, not individually. By conducting member checks, we ensured that our understanding of participants’ comments was accurate and unbiased. Finally, in the results section, we provide rich descriptions of each theme and include multiple supportive quotes as evidence, using both survey and interview data.
Results
We developed four themes that represent the data related to supports and barriers. These themes include: (1) systemic barriers in service delivery, (2) collaboration as a support and barrier, (3) experiences that support best practice, and (4) the need for meaningful PD. Next, we discuss each theme with supporting participant quotes. To give context, we provide the participant’s discipline and the quote source (i.e., survey, interview) next to each quote.
Theme 1. Systemic Barriers in Service Delivery
There are several systemic challenges that participants believed negatively impacted their delivery of EI services. Many of these challenges were related to the financial burden of working in EI. Participants discussed having low and inconsistent compensation and not being reimbursed for specific costs (e.g., cancelations, trainings, assessment tools, collaboration time). Participant 84 discussed the financial burden, sharing, “I love my clients, my job. The pay makes it hard to stay. It’s really low for all the hoops and difficulties we deal with (no pay for no shows, cost of driving around, monitoring our files, etc)” (SLP, Survey). Some participants believed that low compensation led to providers leaving the field. One provider, participant 60, explained, “Another challenge is providers leaving the system. Providers are leaving left and right because of not – we’ve only had three raises in the last 20 years because of funding” (EI educator, Interview). Because of the lack of EI providers in the state, many participants felt overworked and said the waitlist for children to receive services was long. While participants across disciplines shared concerns about compensation, some EI educators believed that their discipline specifically was undervalued, as they are compensated at a lower rate than every other EI discipline. Participant 134 explained, “As [an EI educator] that [we’re] not paid at a comparable rate to other providers” (EI educator, Survey). Participant 122 echoed this sentiment, saying, “a [EI educator] with a [master’s in education] and 30 years experience makes the same pay as a new grad and less than new grads in other disciplines” (EI educator, Survey). Related to financial burden, Participant 111 noted that EI providers’ use of best practices is impacted by their access to training, which unfortunately, is not always available at low cost or convenient times.
Some courses can be costly and timely, and I know I’ve worked with other therapists that don’t want to take the time off work to gain the knowledge necessary to do the job or don’t want to spend the money and prefer to do online courses. (PT, Interview)
Other systemic challenges were related to inconsistencies across the state and inequitable opportunities for both providers and families. In the following quote, Participant 60 explained how there is favoritism when it comes to EI providers receiving referrals.
In the 23 years I have been a provider, parents have NEVER been given the opportunity to choose providers as it is described in the rules. If you are in good with the Service coordinators then you get work, if not, you are rarely given a chance. (EI educator, Survey)
Participants also cited inequities that families experience. For example, Participant 48 explained, If you’re a parent that like is white and can get on that phone and harass the service coordinator, you’re going to get what you want. If you’re a lower, lower income client and they’re working multiple jobs and they don’t speak the language, like, they’re less likely to have access to these kinds of things. (EI educator, Interview)
Another challenge reported by participants was that the system is not responsive to families’ needs. Participant 43 explained that providers having the option not to provide in-person services is challenging for some families.
There is a lack of providers in my area, so the waitlists are very long and of the providers available, many of them will not provide face-to-face services, which is challenging for several of the families I service that have very significant needs. (SLP, Interview)
Others expressed difficulty connecting families to mental health or other services. Participant 29 said, “The biggest issue that I have received recently is dealing with parents mental health issues and trying to find help” (SLP, Survey). Likewise, Participant 54 said, “The needs of the families are larger of what we can provide help with” (EI educator, Survey) and explained during the interview “challenges in getting [families] the services that they need and the state not being, not having the best avenues to do that” (EI educator, Interview).
Finally, participants noted that their work is often done in isolation, and there is a lack of systemic support for EI providers to engage in collaboration. Participant 72 shared, “Few systems supports for true collaborative teaming with all the professionals who are serving a family” (EI educator, Survey). She further explained in the interview that she cannot find time to collaborate with some providers due to their caseload size and lack of time.
I then wanted to have a conversation with the speech pathologist. She’s seeing like 30 kids a week . . . and she has children of our own. So, it’s kind of like okay, well when, you know, is it the five minutes when, when they’re driving? You know, people who are trying to maximize their income, don’t have time. (EI educator, Interview)
Participant 156 explained that Illinois is more isolated compared to another state she worked in previously. She shared, Here in Illinois, especially, I don’t necessarily work with those providers here in my office. I don’t know them very well. It’s an awkward relationship. I can’t really talk to them about it and maintain a professional relationship, versus when I was in Seattle, we were all part of one team altogether—SLPs, PTs, OTs, special educators, nutritionists, like all part of one team. And as a team, we could talk about like, “Oh, how are we doing, X, Y, or Z? How are we supporting the families?” and here in Illinois, feels a little bit more piecemeal. (SLP, Interview)
Overall, this theme illustrates the systemic barriers that EI providers reported facing. The specific barriers were related to the financial burden of being an EI provider, inconsistences and inequities with referrals, and a lack of systems support to meet the demands of the job, such as supporting family’s mental health, accessing training, and having time to collaborate. The following theme addresses collaboration more specifically.
Theme 2. Collaborating with Others as a Support and Barrier
Participants said collaborating with families and other professionals was both a support and a barrier to their practice. When participants described working with families as a support, they mentioned learning from families and caregivers participating in EI. Participant 115 summarized how she learned from families over the course of her career. “I feel like the best way to learn is from the families themselves, because every one of them’s unique, everyone’s different and they’re the ones who teach us what they need, and how we can help and support them” (EI educator, Interview). Regarding caregiver participation, Participant 45 said that a successful session is when, “The parent demonstrates activities and strategies that they have been carrying over all week and then is an active participant in our session” (OT, Survey).
In contrast, when participants said that collaborating with families was a barrier, they mentioned a lack of caregiver participation, issues related to caregiver expectations for services, and challenges related to specific family characteristics. Participant 48 explained how some families engage in EI more than others, especially when they are motivated.
Some parents will be very, very specific and have very specific questions or give you very specific examples on how it’s working and then other clients who might get like one-word answers, even if you’re trying to leave it an open-ended question. So, it, it really depends on how much that caregiver, family wants to work on that functional outcome. (EI educator, Interview)
Several participants who mentioned a lack of family involvement seemed to believe that the caregivers needed to do more to be engaged, particularly “carryover strategies” and “follow-through.” However, Participant 100, believed that when she experienced a lack of family engagement, it was her job to help families become engaged.
Some parents are very willing to try and do things, some parents are very nervous and hesitant to do things. Some parents are very engaged, some parents are not as engaged. So when a parent isn’t as engaged or isn’t as comfortable it takes a little more effort on my part. It might take a little more patience. It might take trying many different ways, because sometimes one thing doesn’t really work, so we’ll go, “Okay that’s not working. Let’s figure out another way you can do this.” And having experience, and working with families for a very long time, you know, I can show a child’s parent 10 different ways to get the goal I’m trying to get or the activity I’m trying to get.It doesn’t have to be just one way. So it’s not so much a challenges is, as, it’s, I guess it would be a challenge but it’s a fun challenge you know, like it’s like okay, “That didn’t work what’s the next thing we can try?” (PT, Interview)
Several participants believed that families had expectations for services that did not align with best practices. For example, Participant 38 said that a challenge she experienced is, “When family expects that provider will come in and ‘fix’ the child without participating in therapy or doing any active carryover of strategies” (OT, Survey). Similarly, participants reported that they often experience a mismatch between families’ beliefs and their own. Participant 72 shared, “I’ve had a parent who said, ‘Well I’m trying to potty train her and I spank her when she has an accident.’ You know, how do I respond to something like that?” (EI educator, Interview).
Finally, certain family characteristics were reported as a challenge for EI providers to implement what they consider best practices. Some of these characteristics included having full-time employment, multiple caregivers for a child, mental health concerns, multiple children to care for, or violence in the home. Many believed it was challenging to implement best practices when they don’t see the child’s primary caregivers, such as when the child was watched by other family members or when they attended childcare. For example, Participant 122 said, And then you run into issues like is there a babysitter there, is there the grandparents? So sometimes communication in those situations, when the parents are working full-time and you know, I will leave notes or I will send notes to them and try to communicate over the phone or through videos, but I feel like that’s an area that’s always a challenge is, you know, if the recipients are not dedicated to wanting to learn and follow through with the recommendations that we’re making. (EI educator, Interview)
Participant 48 reported feeling conflicted about how to best support overwhelmed families.
Best practices can be set up at, towards like when we’re starting the therapy and then with a client, it just kind of falls off, cause like, these parents are exhausted. They, a lot of times have multiple children, there’s a lot of stressors going on. So, like, they’re going to use me as an hour to like, take a break and go in the kitchen and make lunch or take care of the baby or fold the laundry or just take a beat for themselves. So, and that I think is really, I feel like that’s something that kind of gets discussed a little bit, but not too much like, you know, am I really supposed to be nagging this exhausted mother to come in and like have to sit down on the session? Or do I just take this as an opportunity for this child to basically kind of be like tutored for an hour? Because it’s like what is, what is the better? What is, what is worse? I almost feel like, again, it’s meeting child, the client and child where they’re at, especially on that day and trying to best serve them. (EI educator, Interview)
When participants discussed working with other professionals as a support to their use of best practices, they described engaging in mentorship, co-treatment sessions, and discussion. Participant 111 explained the importance of mentorship in the following quote: I like the pay it forward model. Like someone helped me get started in EI. [I] had a great mentor for EI, had a great clinic mentor, so I like to pay it forward as well. So some of the newer practitioners that I’ve met that have been going into it, we meet for coffee and kind of go through some different things or set up . . . talking the 60 minutes that we’re doing every month and kind of set up talking about certain kids that they may be struggling with to help increase their knowledge in that area. (PT, Interview)
Participant 72 explained the importance of co-treatment for her learning when she shared, “I have learned a lot co-treating with people I consider, really, really good in their fields, so PTs, OTs, and [SLPs], and I still continue to learn a lot from them” (EI educator, Interview). Social media groups were also used for collaborative learning. Participant 21 explained, There’s different Facebook pages and social media pages, that are providers that put, put it out there, and it’s like a Pinterest board, you’re like oh that’s—and I love that, and so I know it’s not necessarily, personally collaborating with them, but I have gotten a lot of good information and stuff from those as well. (EI educator, Interview)
In contrast, issues with collaboration included differences in service delivery and others’ lack of knowledge. Participant 72 explained that a challenge she experiences is when other EI providers do not align themselves with practices she believes are best. She shared, “Other therapists sometimes get frustrated with some of the guidelines that I would consider best practices and they say, ‘Why do they keep telling us to do this or that or the other thing?’” (EI educator, Interview). Two practices that seemed to be a point of conflict among EI providers were implementing caregiver coaching and bagless intervention. Some participants felt like they should be able to use these practices based on their own professional judgment, while others felt like they should be used consistently and without exceptions. Participant 132 explained that she encouraged other EI providers to use recommended practices that benefit the family.
There’s different interpretations of best practices or most people don’t want to – what’s a good word? Either they’ve been doing it this way for so long they’re not going to change, you know, therapists have been in here. I look at it more of, again, kind of from the parents’ point of view, what is going to be helpful for this family? And I’d say probably in the last few years too when we’ve been so encouraged to do the coaching model, I definitely am more parent focused about, “Okay, you try it.” Like say if I’m cotreating with a PT, they’re doing the activities with the child, I’ll kind of suggest, “Hey why don’t you let mom try it and make sure she’s doing it correctly?” So kind of pushing so the family is doing more than just the therapist doing more. (EI educator, Interview)
Participants also discussed issues around other EI providers lacking important knowledge, such as certain aspects of child development, intervention strategies, or how to use assistive technology. For example, Participant 111 spoke about her experience with some EI providers making mistakes that harmed children and resulted in her having to fix the problem.
I know quite a bit about assistive [technology], so I’ve gotten calls from orthotics gone wrong or you know, this child has like a blistery, bloody foot because they made the wrong selection, so some of that is a little frustrating to me just getting that correct education before, you know, sending the other practitioners out to complete evaluations or to work with more medically complex children on their own. (PT, Interview)
This theme demonstrates that collaborating with others can be a support or hinderance to EI providers’ implementation of what they consider best practice. When working with others, participants believed they benefit when there is a match in priorities and styles and when they can learn from the other person. In contrast, when they are working with a family or EI provider who has different priorities or knowledge, this is perceived as a barrier. The following theme addresses the types of experiences EI providers found beneficial in facilitating best practices.
Theme 3. Key Experiences That Support Best Practice
Participants believed a variety of experiences were useful in helping EI providers learn about and enact best practices. They reported that they drew on their personal experiences, self-directed learning, and formal education and training to guide how they delivered services. Personal experience, such as how long they have been in the field and their background experiences also contributed to their understanding and use of best practices. Participant 110 described using her other work experiences to guide her work in EI.
I’m also a special education teacher so like using all of those like skills that I’ve learned from being a teacher over the years. I do teach students that are non-verbal, so parent communication has always been something that I’ve done . . . so I really have brought that into the EI setting. (EI educator and behavior, Interview)
Some participants said that their experience as a parent of a child in EI was a support. Participant 60 combined her professional and parental experience. She said, I’ve been a provider for 22 years. So experience, lived experience. My son . . . was in [EI] in 2003, probably until 2005 or so. So not only was I a provider, I was also a parent of a child who was in [EI]. (EI educator, Interview)
Participant 100 emphasized the importance of experience to develop EI providers’ skills. She said, “I always talk about tools in your belt, you know, the longer you work with kids, the more classes you take, the more people you learn from, you have more tools” (PT, Interview). Similarly, participants also noted that changes in the field over the course of their career also influenced how they deliver services. Participant 48 said, When I started in EI, getting away from that clinical method, of like you just take the kid to another room and sit down with them, and play with them and return them to their parent. That was starting to go away, and now it’s like flipped to the opposite where it’s like, this whole coaching model where you’re like talking to the parent and not spending as much time with the child . . . and I’m sure in another 5 to 10 years there’s going to be a whole other method that’s like supposed to be like best practice. (EI educator, Interview)
Participants believed that their formal pre-service and in-service training experiences were useful in helping them learn about best practices. For example, when asked how she learned about best practices, Participant 77 said, I took an [EI] elective in grad school and that opened me to the world of [EI] and of what kind of best practices there are. And then I think when I got my [EI] credential the training involved a lot of information about best practices and what’s expected when you actually start going in the field, going into homes. (SLP, Interview)
While nearly all the participants discussed education and training as influencing their understanding and use of best practices, many of them mentioned that they learned more from their hands-on experience. For example, Participant 122 explained, You learn about child development and you learn about typical development versus atypical development, things like that, but I think it’s really through experience where you learn about how to implement these things and how best to relate with families and how best to teach families. (EI educator, Interview)
Participants also believed that they learned by engaging in self-study, which helped them stay up-to-date on changes in the field. Participant 54 explained, “Child development is such a wide thing and there’s always changing. So, for me, it’s just keeping up with the research and knowing that there’s many ways to learn and then there’s new findings” (EI educator, Interview). Relatedly, a few participants said they had delivered PD to others to share their expertise, such as presenting at conferences and hosting reflective practice sessions.
In sum, participants drew on a number of experiences to guide their practices including their personal experiences, self-directed learning, and formal education and training. Notably, participants believed that the less formal experiences were more influential to their practices. The next theme addresses the EI providers’ perceived needs in the area of professional development.
Theme 4. Meaningful PD Is Needed to Support Best Practice
As noted in the previous section, many participants believed that their education and training were insufficient in helping them implement best practices. However, they also reported what made a training “quality” from their perspective, such as its usefulness, its alignment to state requirements, having practice opportunities, and their ability to access and get EI continuing education credits for the training. For example, Participant 103 described why a training focused on play was meaningful to her when she said, “You want to take that class more, because you know you’ll get the credit for it, but you also know it’s something that will be useful in carrying over to your therapy sessions” (SLP, Interview). In addition to a training being useful, Participant 122 wanted it to be delivered by someone who is working in the field.
I would rather learn some of these things from people who are doing it on a regular basis as opposed to someone who isn’t hands on, you know, who may be phenomenal at research but has never had to implement the strategies on a regular basis or doesn’t work regularly with families . . . just kind of think on their feet and teach real life examples on the best way to implement those strategies (EI educator, Interview)
Some participants noted that the increase in remote trainings available has been positive. For example, Participant 48 explained, “I feel like being like able to do the trainings like remotely is awesome. So, you have access to more stuff” (EI educator, Interview). Some specific trainings were named by participants as high quality, such as the PLAY Project workshop, the Facilitating Attuned Interactions Approach (FAN) training, Rush and Shelden’s coaching trainings, as well as those offered by Illinois’ Developmental Therapy Association, Early Intervention Training Program, and Erikson Institute.
Participants’ PD needs included specific topics, such as trauma/mental health, identifying community resources, applied behavior analysis, and teaming/co-treating. They also wanted opportunities to reflect and collaborate during PD. For example, Participant 132 shared, I wish there was more of a reflective practice system kind of already built in, because I know – I mean, we’re out here by ourselves a lot . . . I wish we would – in order to reduce burnout, we really should have more of a reflective practice. (EI educator, Interview)
Similarly, Participant 77 said, “It’d be awesome to get like one-on-one mentorship or like someone observing my sessions and giving me feedback” (SLP, Interview).
Overall, participants believed that quality PD was needed to enhance their practice. They wanted PD to be useful, accessible/affordable, delivered by someone immersed in EI, and include ongoing opportunities for reflection and collaboration.
Discussion
We aimed to understand what supports and barriers EI providers perceived as impacting their service delivery. We analyzed open-ended survey data from 95 participants and qualitative interview data from a subset of 19 participants. We developed four themes that represent participants’ responses: (1) systemic barriers in service delivery, (2) collaboration as a support and barrier, (3) key experiences that support best practices, and (4) the need for meaningful PD. Next, we discuss key findings, limitations, implications, and directions for future research.
One finding from this study is related to the systemic barriers facing EI providers. The financial strain of being an EI provider was prevalent among these participants, consistent with findings from other studies (Campbell & Halbert, 2002; Little et al., 2015; Vail et al., 2018). Similar to Campbell and Halbert’s results, we found that the financial burden was not only related to low salaries in EI, but also the lack of reimbursement for specific costs, such as traveling to families’ homes, canceled sessions, ongoing PD, collaboration time, and buying assessment tools. These costs are especially burdensome for providers who work independently for the state rather than a private EI program, who represented more than half of our sample. Each state determines who they contract with (e.g., independent providers, public agencies, private agencies; IDEA, 2004); thus, this issue may vary by state. However, even providers who work for an EI program may experience the effects related to the lack of funding, such as increased pressure to keep a high caseload. Relatedly, when EI providers discussed their PD needs, they wanted access to affordable or free high-quality trainings without having to lose pay.
Another finding related to financial concerns is that several EI educators in this study felt undervalued compared to providers in other disciplines as their reimbursement rate was lower, even when they had an advanced degree and/or more years of experience. One potential reason for undervaluing EI educators is that there are no required national preparation standards for the role. Instead, each state determines the requirements to be an EI educator, which tends to be less rigorous than the other main disciplines (i.e., OT, PT, SLP). Another potential reason is that EI educators may not be seen as specialists, as they do not focus on a specific developmental domain. DEC’s (2024) position statement on the role of special instruction advocates for EI educators, noting they are specialized and valuable team members.
Given the lack of financial security, participants in the current study described providers leaving the field, which ultimately results in families waiting for services for longer. Participants explained that the state has long waitlists for many EI services such as speech and physical therapy, which leads to several issues. One of these issues is that EI providers feel overworked because they need to provide services to so many families. Another issue is that the provision of services to families is inequitable, such that families who are racial minorities, from lower socioeconomic backgrounds, and/or live in rural areas receive services later than those with more advantaged backgrounds. This disparity in service provision is well documented in the literature (Barton et al., 2016; Gillispie, 2021; McManus et al., 2020; Raspa et al., 2010). Additionally, participants in this study believed they were referred to families inequitably, with some EI providers receiving more referrals than others. Participants in the present study seemed to believe that service coordinators were at fault for these inequitable referrals. It is important to recognize that service coordinators also face significant barriers in EI service delivery (Childress et al., 2019) and we caution readers not to blame any single role for these systemic challenges.
Another systemic barrier identified in this study was the lack of sufficient procedures in the state related to team collaboration. EI providers described feeling isolated from one another and did not feel like that they had enough time to engage in collaboration with other members of a child’s team. Similar issues were reported by Corr et al. (2023) who studied EI providers’ experiences with ethical dilemmas. They found that EI providers felt like they did not have sufficient supervision and did not know who to turn to with questions. Some policies in the state aim to support team collaboration in EI, such as requiring that EI providers engage in monthly consultation with other EI providers (Illinois Department of Human Services, 2022). Another policy is that EI providers can be reimbursed for time consulting with other EI providers on a child’s team, though the amount of consultation allowed is limited (e.g., 15 minutes per month per service) and required to occur using certain avenues (e.g., over a phone call or in-person is allowed but email or text message is not allowed). Ultimately, however, some EI providers in this study believed these avenues were not sufficient and wanted improved procedures for team collaboration to better support families.
Because EI providers in this study did not believe there were sufficient procedures for promoting team collaboration, it is not surprising that participants reported challenges related to collaborating with others. Participants noted it was difficult to navigate differences in approaches and knowledge between providers, which has been reported in previous research (Able et al., 2017; Corr et al., 2023). This is likely directly related to the systemic barriers outlined in the previous paragraphs (e.g., limited time to collaborate). Another potential reason is that EI providers in the state are not required to engage in ongoing PD related to teaming; therefore, the opportunities they have to learn from and with other professionals is self-directed, open-ended, and may not reflect what high-quality teaming looks like in EI. When participants discussed their PD needs, one of the topics they specifically wanted more training on was teaming and collaboration. Participants appreciated and desired more opportunities to learn from other professionals through discussion, reflective practice, formal mentorship, and co-treatment. EI providers in other studies reported that similar collaboration opportunities were helpful for implementing capacity-building with families and resolving ethical issues (Able et al., 2017; Williams & Ostrosky, 2023). Participants in the current study wanted these opportunities to be more formalized, rather than something they did on their own.
Our findings related to how EI providers view collaboration with families as both a facilitator and barrier connects to previous literature. Researchers found that EI providers believe that their ability and/or inability to implement recommended practices is dependent on family factors (Douglas et al., 2020; Fleming et al., 2011; Meadan et al., 2018, 2020; Spence et al., 2022, 2023; Stewart & Applequist, 2019; Tomczuk et al., 2022). When EI providers attribute their practices to family characteristics, they ignore their own professional responsibility to be responsive to all families. Though it is a common refrain that EI providers essentially “give up” or “blame” certain families for their lack of using recommended practices, it is important to recognize that some participants in this study did not align with this characterization. Some believed it was their responsibility to learn from each individual family or challenge themselves to figure out how to help a family become engaged. These reframed perspectives that put the responsibility on the professional, rather than the family, are important and align with priorities in the field. Some participants mentioned a lack of systemic procedures for addressing families’ needs. Further, participants wanted PD on topics such as trauma/mental health and identifying resources, indicating that participants considered it a priority to address diverse family needs, even though it was a gap in their knowledge/skills. These findings indicate that it may not be the EI providers, but rather, the system itself that is not responsive to diverse family factors.
Limitations
This study has two main limitations. First, the study was conducted in one U.S. state. Because EI services vary across states, the results of this study may not be applicable beyond this context. For example, providers in some states do not have the option to co-treat with other professionals. Given our qualitative design, our goal was not necessarily to generalize to a larger population, but rather, to provide enough details so that readers can determine how much the information in this study applies to their own experiences and settings. The second limitation is related to the participant sample. We only included providers from four main disciplines (EI educators, OT, SLP, PT), thereby limiting our findings to the perspectives of these providers. It is possible that if we included other disciplines (e.g., behavior analysts, social workers), our data may have been different. For example, social workers may be more equipped to support families’ needs, which was an identified barrier for providers in this study. Also, our participants were mainly white women, and we did not collect data on disability status or language. A more intentionally diverse participant sample would have allowed us to understand the full scope of supports and barriers facing EI providers with a range of backgrounds.
Implications
The implications of this study are three-fold, including implications for policy, personnel development, and practitioners. Each of these is important for helping align EI providers’ practices with recommended practices and addressing the barriers identified in this study.
Implications for policy
The participants in this study mentioned several systemic barriers in the EI system that can be addressed through policy. One of the major implications is that all EI providers need to be compensated adequately and for all of the associated expenses of the job. While this study was conducted in one state, this is a national issue that needs addressed through increased funding for Part C programs (Vail et al., 2018). With additional funding, states could offer higher reimbursement rates for services, affordable PD options, and compensation for specific costs (e.g., cancelations, travel, assessment tools). Notably, each state determines the compensation rates for EI providers, with some states providing higher compensation than others. Therefore, there is a need for policies that address consistency in EI across states and disciplines and a need to identify model EI programs that can be replicated in other states. Another suggestion that would promote consistency is for statewide EI programs to align their CSPD supports with the cross-disciplinary early childhood intervention standards to ensure that EI providers receive initial and ongoing PD in four critical areas: (a) coordination and collaboration, (b) family-centered practice, (c) evidence-based practice, and (d) professionalism (Bruder et al., 2019). Policymakers could also require that states implement a specific collaboration framework, such as the transdisciplinary model (Boyer & Thompson, 2014).
Another area of needed policy change is related to equity in service provision. One potential solution is for statewide EI programs to collect more data on the families who receive EI services; currently, collecting data about income level or dual language status of EI recipients is not federally required (Gillispie, 2021). Also, states are not required to collect data (e.g., race, income, language) on the EI providers who deliver services, which also could shed light on equity issues. Finally, there is a need for procedures that systemically and consistently address families’ needs, such as delineating when to refer families to social work and external services.
Implications for personnel preparation
Implications for personnel preparation relate to both pre-service and in-service preparation. Related to pre-service preparation, it is important that pre-service EI providers representing multiple disciplines are given opportunities to learn about and with other disciplines. Institutions of higher education and personnel preparation faculty can accomplish this by having interdisciplinary courses, mandating field placements in interdisciplinary EI programs, explicitly teaching the roles of various EI providers, embedding the cross-disciplinary early childhood intervention standards into courses (Bruder et al., 2019), and emphasizing teaming in their instruction (e.g., Shelden & Rush, 2022). There is also a dire need to prepare the EI workforce to be responsive to families’ unique circumstances and characteristics (Campbell & Sawyer, 2009), such as by emphasizing family-centered, culturally responsive, and trauma-informed practices across all EI disciplines. Ideally, providers would receive pre- and in-service instruction on these topics. If it is only provided in a piecemeal fashion or after providers enter EI, there is a risk that the training will not be sufficient for supporting providers to feel confident in their practices. Without widespread, sustained, and meaningful PD offerings on these topics, providers are less likely to acquire needed expertise (Campbell & Sawyer, 2009).
Implications for practitioners
EI providers can take several steps to address the barriers identified in this study and intentionally align their practices with recommended practices. To address systemic issues, EI providers might benefit from engaging in advocacy in EI, such as attending town hall events related to EI, writing letters to policy-makers about funding Part C services, or seeking advocacy opportunities through professional organizations such as DEC (e.g., https://www.dec-sped.org/policy-and-advocacy). More practically, EI providers can take advantage of the opportunities that participants in this study deemed as helpful to their practice, such as collaborating with other EI providers, attending specific trainings (e.g., FAN, PLAY project), and engaging in self-study. Finally, it is important that EI providers continually engage in self-care and reflection to help them navigate the challenges they perceive as impacting their work, such as responding to providers and families with different backgrounds and beliefs.
Direction for Future Research
There is a need to continue to learn more about EI providers’ perspectives. Researchers could gather information about providers’ perspectives on salient debates (e.g., bagless therapy) through interviews or focus groups. Additionally, more research is needed about systemic barriers that EI providers experience, especially those related to inequities for providers and families. While this study provided some perspective on these inequities, future research should explicitly focus on EI providers and families from marginalized backgrounds to understand their unique perspectives. Regarding the inequities and inconsistencies related to referrals, it may be useful to examine the referral procedures within and across geographical regions to identify promising procedures that can be adopted broadly across U.S. states. Similarly, more exploration of teaming approaches is needed to identify and adopt model approaches. Finally, future research should address providers’ understanding and capacity to support diverse families in EI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.