
Abstract
In addition to amyloid and tau pathology, elevated systemic vascular risk, white matter injury, and reduced cerebral blood flow contribute to late-life cognitive decline. Given the strong collinearity among these parameters, we proposed a framework to extract the independent latent features underlying cognitive decline using the Harvard Aging Brain Study (N = 166 cognitively unimpaired older adults at baseline). We used the following measures from the baseline visit: cortical amyloid, inferior temporal cortex tau, relative cerebral blood flow, white matter hyperintensities, peak width of skeletonized mean diffusivity, and Framingham Heart Study cardiovascular disease risk. We used exploratory factor analysis to extract orthogonal factors from these variables and their interactions. These factors were used in a regression model to explain longitudinal Preclinical Alzheimer Cognitive Composite-5 (PACC) decline (follow-up = 8.5 ±2.7 years). We next examined whether gray matter volume atrophy acts as a mediator of factors and PACC decline. Latent factors of systemic vascular risk, white matter injury, and relative cerebral blood flow independently explain cognitive decline beyond amyloid and tau. Gray matter volume atrophy mediates these associations with the strongest effect on white matter injury. These results suggest that systemic vascular risk contributes to cognitive decline beyond current markers of cerebrovascular injury, amyloid, and tau.
Keywords
Introduction
Emerging research strongly suggests that while a great deal of cognitive decline is seen in older adults with elevated amyloid,1 –3 many individuals with elevated amyloid do not show clear cognitive decline during longitudinal follow-up. This underscores that important factors other than amyloid likely influence neurodegeneration and the emergence of cognitive decline, alone or in combination with canonical AD pathology. Vascular contributions to cognitive and neurodegenerative trajectories are well-established and important factors in this context 4 which can be identified using systemic and/or brain injury measures.
Notably, data from Harvard Aging Brain Study (HABS) demonstrate a large impact of systemic vascular risk factors (including hypertension, obesity, and smoking) on cognitive decline and tau accumulation.5,6 In addition, other studies show that tau PET levels predict cognitive decline7,8 and neurodegeneration. 9 Moreover, white matter injury10,11 and reduced cerebral blood flow12,13 are associated with cognitive impairment and increased risk of dementia. Apart from the individual effects, these measures interact with one another to accelerate cognitive decline. For example, amyloid burden interacts with systemic vascular risk to accelerate cognitive decline and brain atrophy in preclinical Alzheimer’s disease (AD),6,14 and the effect on cognitive decline is mediated by tau accumulation. 15
Given the collinearity among these variables and the potential for complex interactions, we proposed a framework to extract latent factors that isolate maximally orthogonal domain-specific variance to explain cognitive decline. We hypothesized that there are latent sources of variance that exist across measures and across interactions between measures that will streamline the interpretation of contributing factors to late-life cognitive decline.
Material and methods
Participants
One hundred and sixty-six older adults who were cognitively unimpaired at baseline were selected from HABS based on the availability of included measures. At study entry, all participants had a global Clinical Dementia Rating of 0 and an education-adjusted Mini-Mental State Examination score of 27 or greater. Exclusion criteria included a modified Hachinski ischemic score greater than 4, and a history of stroke or evidence of infarcts with persistent neurological deficits. Our study included all HABS participants who had neuroimaging – including amyloid PET, tau PET, and MRI – as well as cognitive assessments, and sufficient baseline medical information to calculate an algorithmic vascular risk score. Data were collected from April 2010 through August 2021. The Mass General Brigham Institutional Review Board approved the HABS protocol and procedures (Helsinki Declaration of 1975 (and as revised in 1983)), and all participants signed a written informed consent prior to the completion of any study procedures.
Magnetic resonance imaging (MRI)
Participants underwent MRI on a Siemens Trio-TIM 3T scanner equipped with a 12-channel phased-array whole-head coil. 16 The following MR images were used: 1) High-resolution 3D T1-weighted multi-echo magnetization-prepared, rapid acquisition gradient echo anatomical images were collected with the following parameters: TR = 2200 ms; multi-echo TEs = 1.54 ms, 3.36 ms, 5.18 ms, and 7 ms, dimensions = 1.2 × 1.2 × 1.2 mm3; 2) 3 D fluid-attenuated inversion recovery (FLAIR): TR/TE/TI = 6000/454/2100 ms, dimensions =1 × 1 × 1.5 mm3; 3) 2 D EPI diffusion-weighted imaging: TR/TE = 8040/84 ms, dimensions = 2 × 2 × 2 mm3, number of directions = 30, b-value = 700 s/mm2.
We segmented white matter hyperintensities (WMH) on FLAIR images using the HyperMapp3r algorithm. 17 HyperMapp3r is a convolutional neural network-based segmentation algorithm that uses T1-weighted, FLAIR, and brain mask images to generate WMH predictions in the subject space. We estimated the peak width of skeletonized mean diffusivity (PSMD) from DTI using a publicly available script (http://www.psmd-marker.com). 18 This pipeline preprocessed diffusion MRI (eddy current and motion correction) followed by tensor fitting, skeletonization of the data, and histogram analysis using FSL6.0.1 tools including Tract-Based Spatial Statistics procedure (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/TBSS) and fractional anisotropy template (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Atlases). Total gray matter (GM) volume was extracted from the longitudinal FreeSurfer segmentation 19 and served as a global index of neurodegeneration after correction for intracranial volume.
Positron emission tomography (PET) imaging
Detailed amyloid and tau PET protocols have been previously described. 20 Briefly, brain amyloid burden was measured at baseline using 11C-Pittsburgh Compound-B (PiB) PET using the Siemens ECAT EXACT HR+ scanner. Amyloid PET (PiB) measurements were represented as a distribution volume ratio across a composite of frontal, lateral temporal, parietal, and retrosplenial regions, as defined using FreeSurfer (version 6.0). Flortaucipir (FTP) PET was introduced into HABS mid-study to measure tau burden, with participants undergoing their first FTP PET at 2.1 ± 1.5 years after the baseline visit. Tau PET measurements were computed as standardized uptake value ratios (cerebellar gray matter as the reference region) within the inferior temporal cortex, an early site of neocortical tau accumulation associated with clinical impairment.
Relative cerebral blood flow (R1) was extracted from dynamically-acquired PiB PET images. We performed kinetic modeling on PiB PET data using the multilinear reference tissue model (known as the MRTM method) to calculate regional R1, an index of PiB tracer delivery, 21 using FreeSurfer segmentation. We then calculated the average of R1 values within the cortical regions to serve as a global proxy of relative cerebral blood flow.
Clinical measures
Cognitive assessments: Cognition was assessed annually using the Preclinical Alzheimer Cognitive Composite-5 (PACC). 22 The PACC is a composite score that includes the Mini-Mental State Examination, Wechsler Adult Intelligence Scale–Revised Digit Symbol Coding, Wechsler Memory Scale–Revised Logical Memory delayed recall, the Free and Cued Selective Reminding Test (free recall plus total recall), and the category Fluency Test.
Cardiovascular Disease Risk: We calculated the office-based Framingham Heart Study cardiovascular disease risk score (CVD), 23 which represents a weighted sum of age, sex, antihypertensive treatment (dichotomous), systolic blood pressure (millimeters of mercury), body mass index, history of diabetes (dichotomous), and current cigarette smoking status (dichotomous). The CVD score provides a 10-year probability of future cardiovascular events, including coronary death, myocardial infarction, coronary insufficiency, angina, ischemic stroke, hemorrhagic stroke, transient ischemic attack, peripheral artery disease, and heart failure.
Statistical analyses
Imaging and clinical data were anonymized prior to analysis. We calculated PACC decline and GM volume atrophy using separate linear mixed-effect models on longitudinal data. The remaining neuroimaging and clinical data were obtained from baseline measurements. We calculated two-way interactions between age, CVD score, amyloid, tau, WMH, PSMD, and PiB-R1 to assess whether these interactions are related to PACC decline. We then used an exploratory factor analysis using varimax rotation as a dimensionality reduction technique from clinical and neuroimaging measures including two-way interactions. Varimax rotation involves adjusting the coordinates of data that result from a principal components analysis. The adjustment, i.e., rotation, is intended to maximize the variance shared among variables. By maximizing the shared variance, results more discretely represent how data correlate with each principal component. To maximize the variance generally means to increase the correlation of items related to one factor, while decreasing the correlation on any other factor. 24 These factors then were used as independent variables in a linear regression model to explain PACC decline. Notably, we did not include GM volume in the factor analysis. We further used GM volume atrophy as an additional independent variable to examine its role as a mediator in the relationship between factors and PACC decline. Finally, we examined the interactions between these orthogonal factors on PACC decline. All analyses were performed in R (v4.0.2).
Results
Table 1 summarizes participants’ demographics and neuroimaging measures at baseline as well as follow-up time for GM atrophy and cognitive decline. Figure 1 demonstrates a high degree of Pearson’s correlation among these measures. For example, we observed that older age is related to PACC decline, GM volume atrophy as well as elevated tau burden, WMH volume, PSMD, and lower R1. In addition, CVD score was correlated with PACC decline, GM volume atrophy, WMH, PSMD, and R1 but not PiB or FTP. The strongest correlations were observed between PSMD and WMH volume (r = 0.51) as well as PiB and FTP (r = 0.45). R1 was moderately correlated with WMH and PSMD (|r| > 0.2)
Participants demographics.
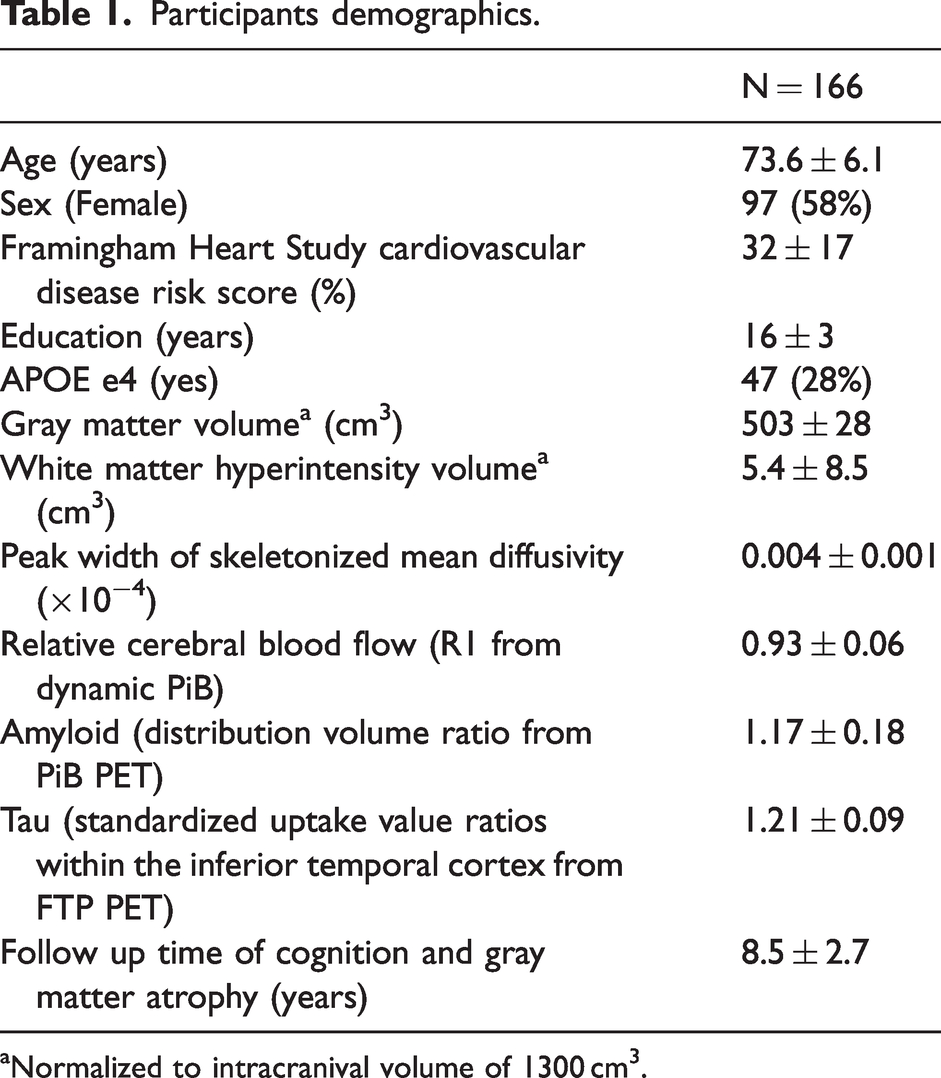
Normalized to intracranival volume of 1300 cm3.
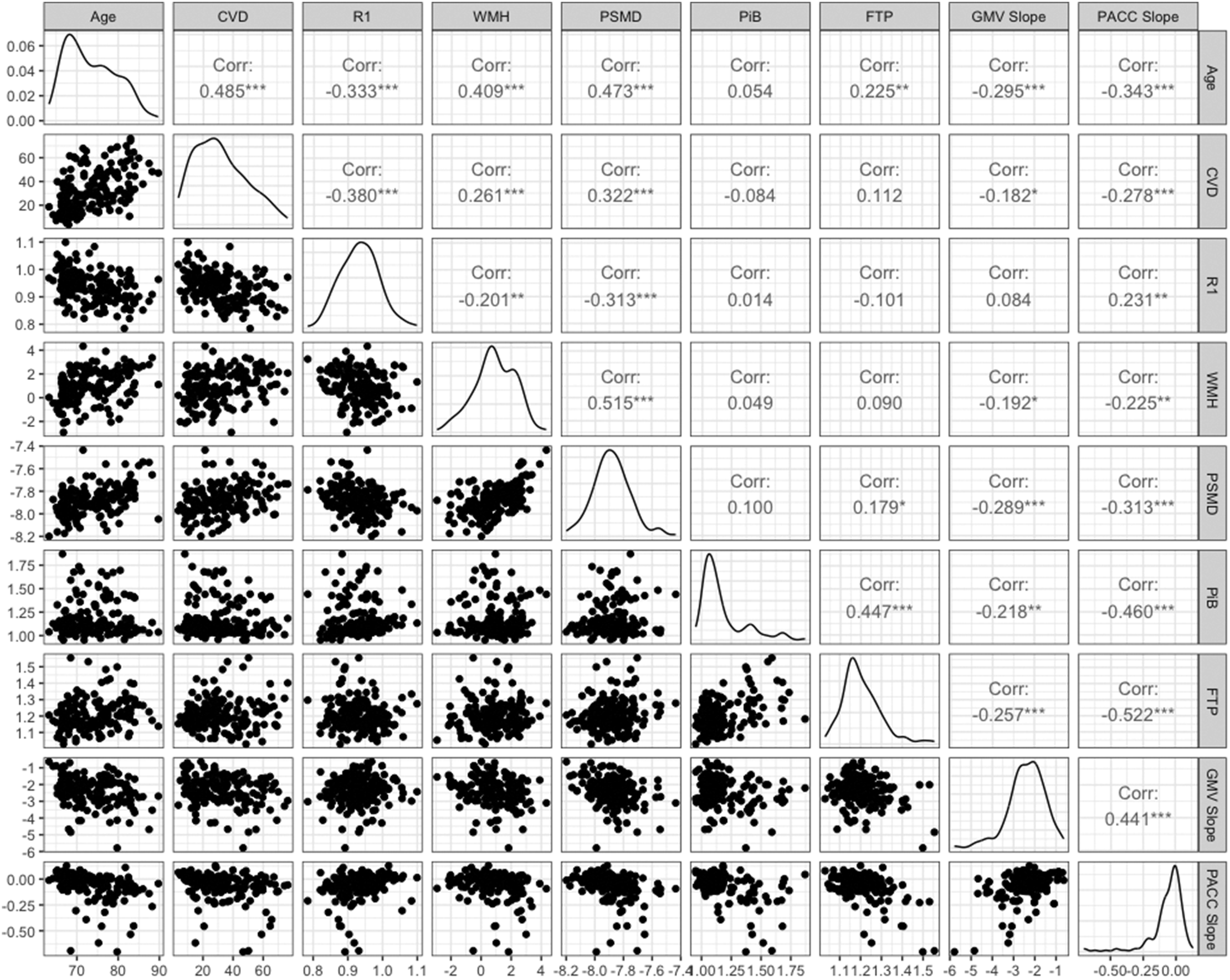
The relationship between cognitive decline, neuroimaging measures, age, and systemic vascular risk in the HABS cohort. Scatter plot, and Pearson’s correlation values between summary measures of white matter injury (
We then calculated two-way interactions between all these measures and examined their relationship with PACC decline. Figure 2 shows the R-squared values from linear regression models of individual and interactive terms with PACC decline. Here we observed that not only individual terms (as shown in Figure 1) related to PACC decline, but also their two-way interactions were highly related to PACC decline. We performed factor analysis using the 28 variables (including individual and two-way interaction terms shown in Figure 2) to extract orthogonal factors. Scree test showed that 6 factors were sufficient. The extracted 6 factors cumulatively explained 96% of the variance in the 28 variables. Figure 3 illustrates the factor loadings on each variable. As an exploratory analysis, we investigated the relationship between individual components of CVD risk score with the systemic vascular risk factor (factor 2). We observed a significant association between all the components and factor 2 (p < 0.001) with the highest effect size of diabetes in categorical components and systolic blood pressure among continuous variables (Supplementary Table 1).
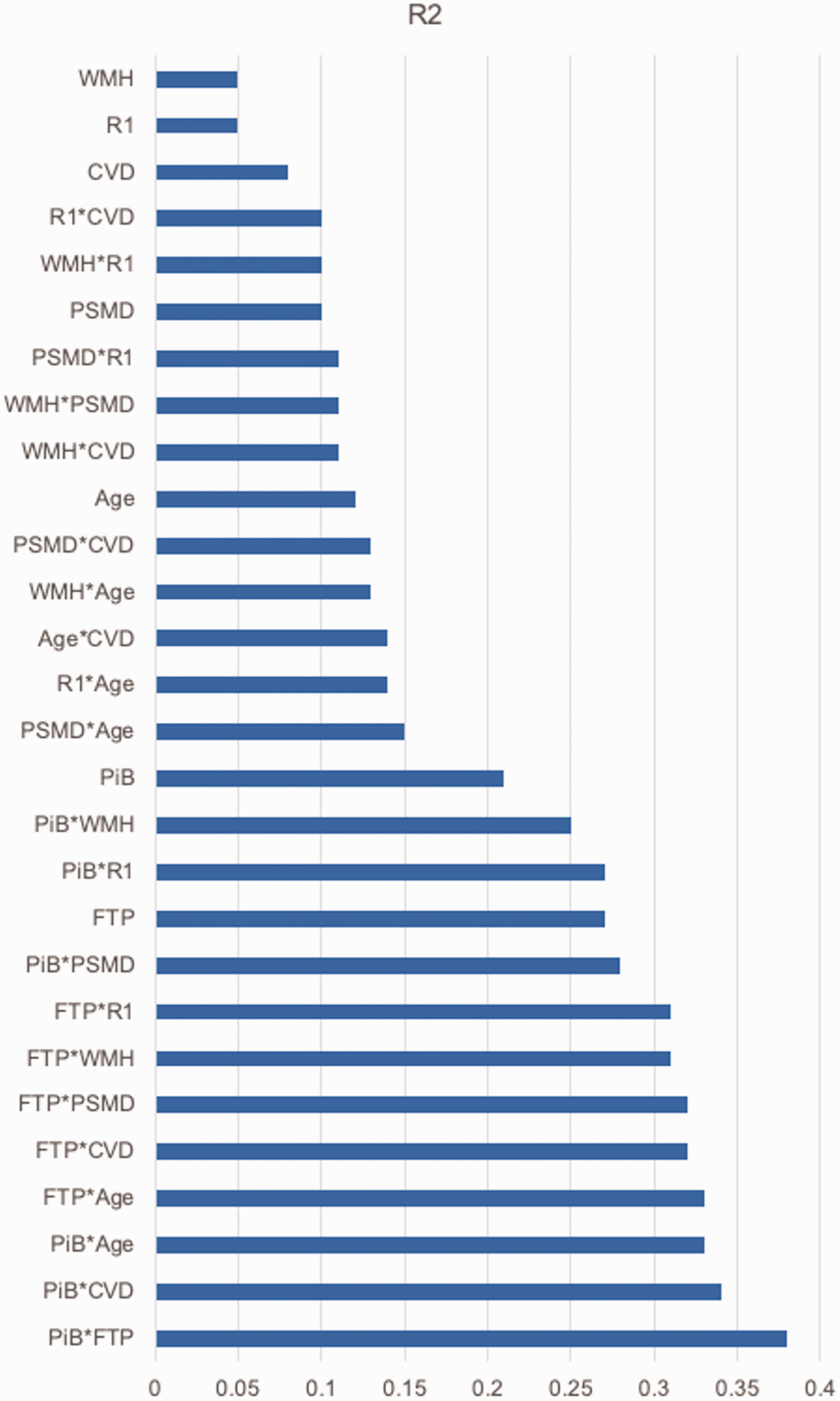
Sorted R-squared values from linear regression models for individual measures as well as their two-way interactions (indicated by “*”) with PACC decline. Summary measures of white matter injury (
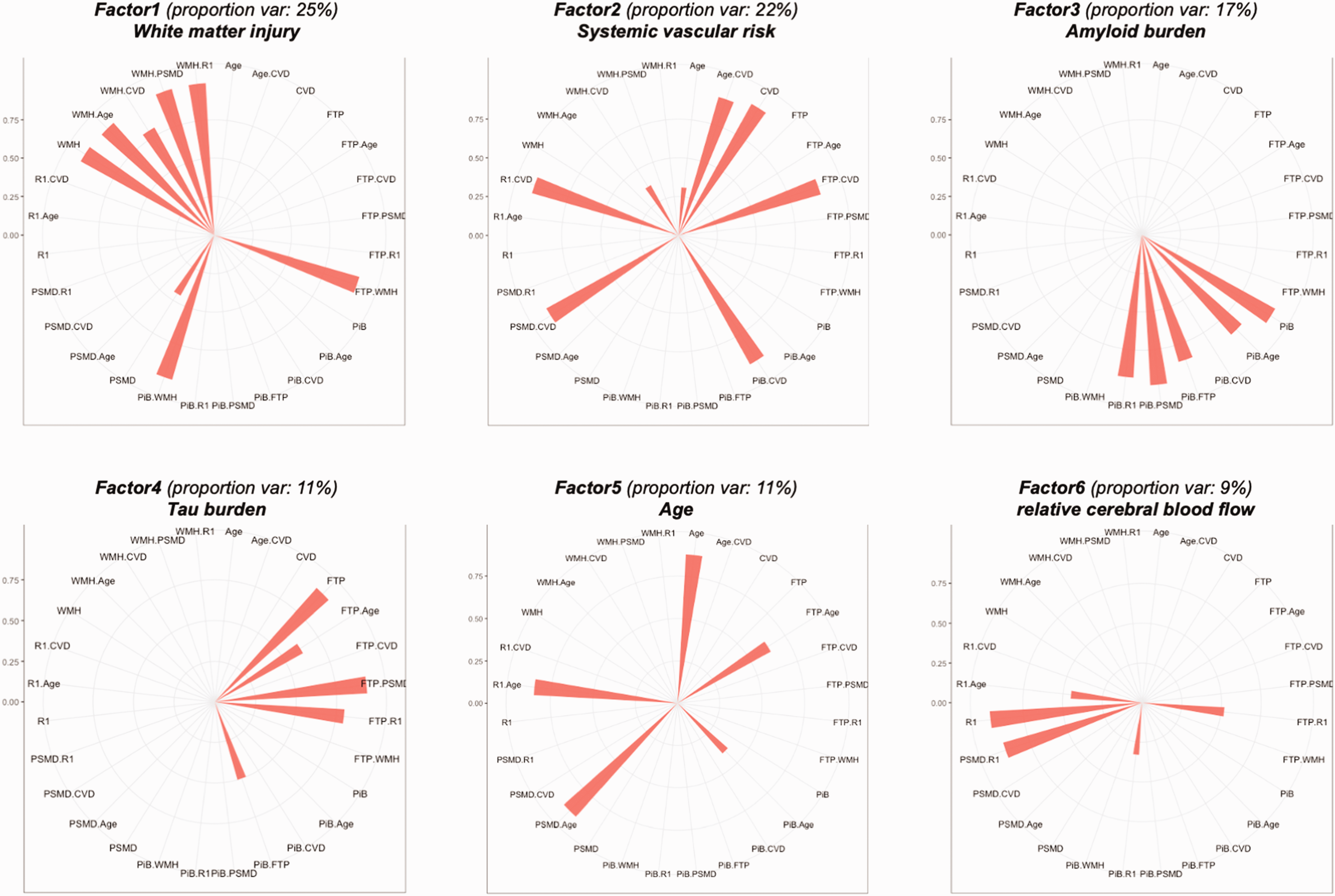
Polar plots of factor loadings (distance from the center) for factors 1 to 6. Only loadings> = 0.3 were shown. Note that 28 variables were used in the factor analysis including the original variables and interactions.
Next, we used these six orthogonal factors as independent variables in a linear regression model to explain PACC decline adjusting for sex and years of education. We observed that latent factors of white matter injury, systemic vascular risk, amyloid, tau, and cerebral blood flow explained the PACC decline while the age factor did not. Including GM volume atrophy in this model removed the effect of white matter injury and reduced the effects of systemic vascular risk and amyloid (Figure 4 and Table 2). Lastly, we included two-way interactions between the amyloid factor and other factors in this model to examine their potentially synergic effects on PACC decline. Note that we did not include other interactions since we did not have the statistical power in this sample. We observed significant interactions between white matter injury and amyloid as well as amyloid and tau factors (Figure 5 and Table 2). For comparison, we also performed a linear regression model with PACC decline as the dependent variable and the major components of the obtained factors, namely, WMH, CVD, amyloid, tau, age, and cerebral blood flow as independent variables (model 0 in Figure 4 and Table 2). We observed that the total explained variance when we use the ‘raw’ variables is approximately equal to the model that utilizes the factors (only 3% less), however, the proportion of the explained variance attributable to the ‘raw' measures vs. factors is quite different with the factors uniformly showing stronger and more statistically significant effects than the raw variables. This difference is due to the complex covariance structure of the raw variables and reinforces the choice to use factors to gain a clearer understanding of the relative contributions of the different measurement domains to PACC decline.
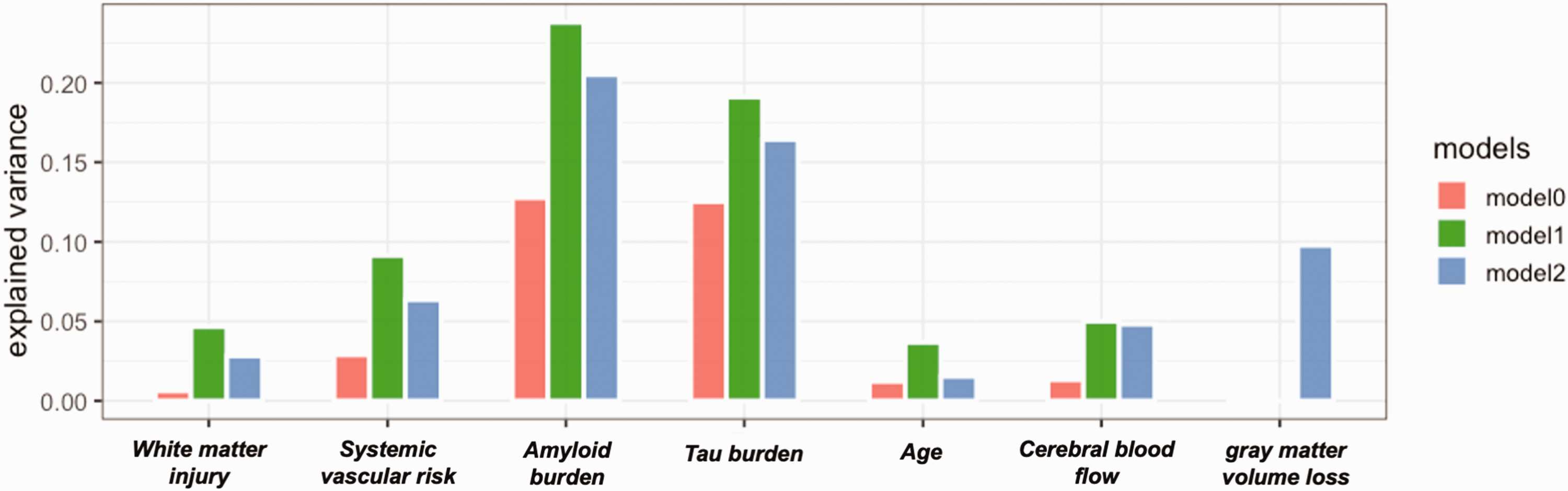
Comparison of explained variance in PACC decline for each variable in model 0 (independent variables: WMH, CVD, amyloid, tau, age, R1, sex, and years of education), model 1 (independent variables: factors 1 to 6, sex, and years of education), and model 2 (independent variables: factors 1 to 6, gray matter volume atrophy, sex, and years of education). White matter injury was no longer associated with PACC decline once gray matter volume atrophy was considered.
Results of linear regression models.
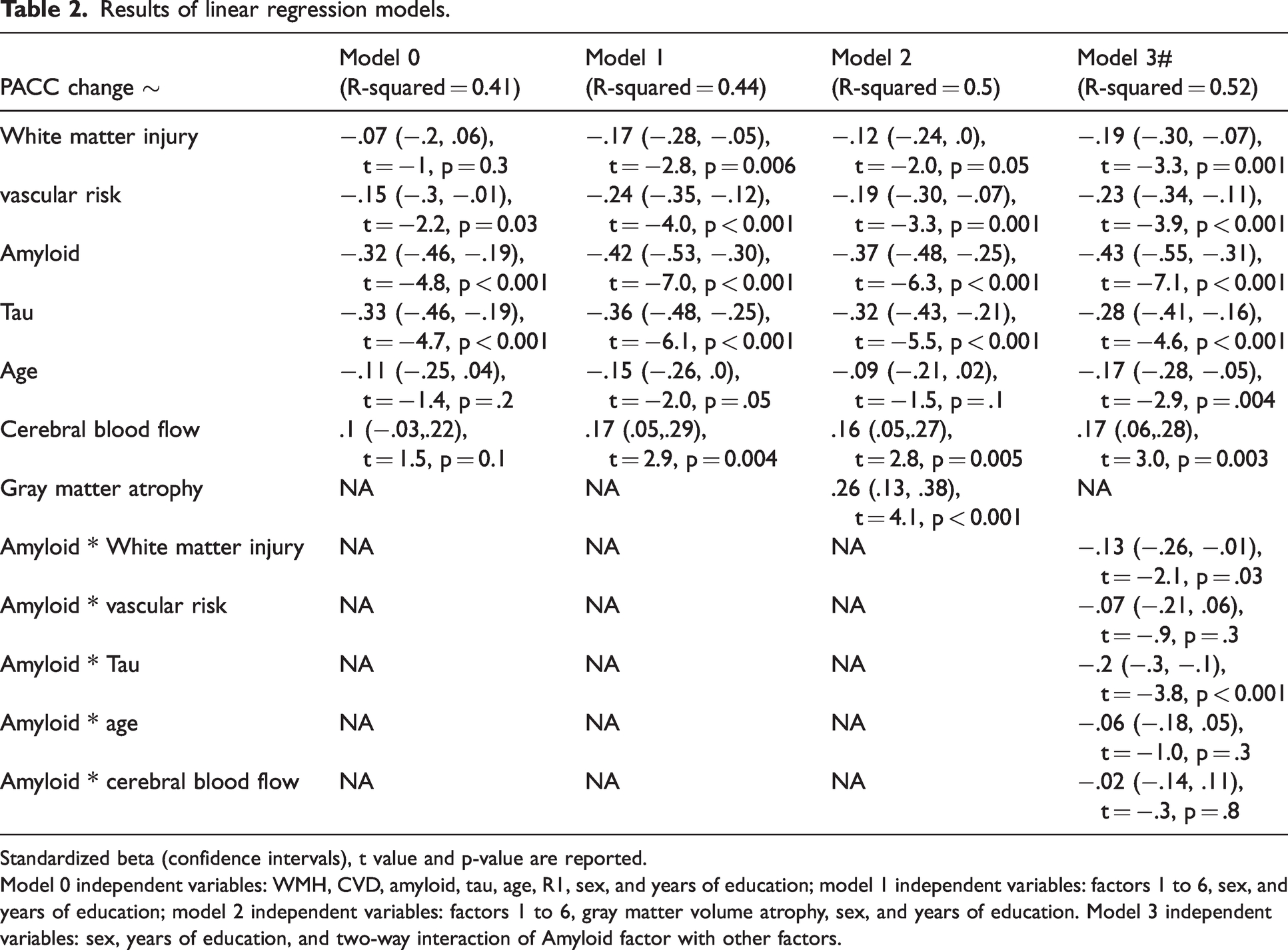
Standardized beta (confidence intervals), t value and p-value are reported.
Model 0 independent variables: WMH, CVD, amyloid, tau, age, R1, sex, and years of education; model 1 independent variables: factors 1 to 6, sex, and years of education; model 2 independent variables: factors 1 to 6, gray matter volume atrophy, sex, and years of education. Model 3 independent variables: sex, years of education, and two-way interaction of Amyloid factor with other factors.
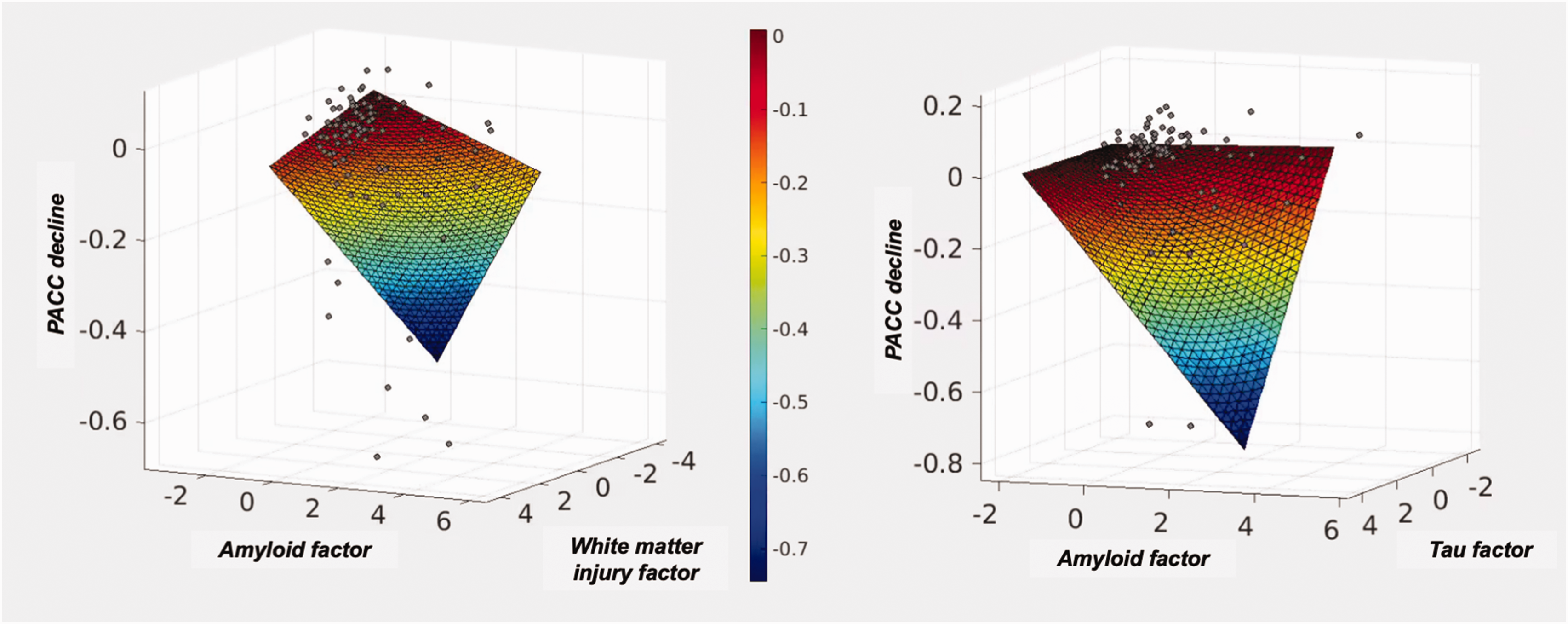
The interactive effects of Factor 3 (amyloid) with Factor 1 (white matter injury, left panel) and Factor 4 (tau, right panel).
Discussion
Late-life cognitive decline is not only associated with amyloid and tau but also related to systemic vascular risk, white matter injury, and cerebral blood flow. By including the variables and all the interactions, we extracted the latent independent features from the large pool of variance, thus for example, the tau and amyloid factors are independent rather than correlated. The rationale for factor analysis was two-fold: 1) use a data reduction technique to generate independent factors underlying cognitive decline and 2) generate a framework that simplifies the interpretation of different yet related contributors to cognitive decline. Our method was able to extract orthogonal components from highly correlated measures such as cortical amyloid and tau, and we were able to use this strength to further understand the complexity of cognitive decline and gray matter atrophy. Since we extracted orthogonal variables, we were able to examine interactions within an organized framework with no collinearity between main effects and interactions.
We observed 3 key findings that add to the growing literature on determinants of cognitive decline. First, latent factors extracted from the colinear brain and systemic measures as well as their interactions show independent factors for white matter injury, global cerebral blood flow, and systemic vascular risk suggesting that while these measures of ‘vascular injury’ are correlated with each other, they are distinct enough to represent different factors (unlike PSMD and WMH that shared a factor) and they independently contribute to cognitive decline. Second, gray matter volume atrophy removed the effect of white matter injury on cognitive decline suggesting a close link between white matter injury and neurodegeneration. Third, among all possible interactions between factors, the interaction of amyloid factor with tau and white matter injury contributed to cognitive decline.
Our findings reveal systemic vascular risk explains cognitive decline in older adults beyond white matter injury and relative cerebral blood flow – commonly used markers of cerebrovascular injury. These results suggest that the mechanism by which systemic vascular risk affects brain function in older adults requires further investigation. Importantly, after extracting these independent factors, it was the systemic vascular risk – and not age – that explained the cognitive decline in this cohort. Similar findings were reported previously about the interaction of systemic vascular risk – and not age and sex alone – with amyloid in the neurodegeneration. 14 The systemic vascular risk-loaded factor (i.e. factor 2) is associated strongly with individual components of the CVD risk score with the highest effect size of diabetes and systolic blood pressure. Notably, while age and the systemic vascular loaded factor are associated, as expected, the effect size of age is minimal compared to other components of the CVD risk score. These results are in line with our previous findings on individual components of CVD risk score in the HABS study 15 and emphasize the importance of vascular injury on brain function and cognition.
Gray matter volume atrophy is strongly related to cognitive decline in this preclinical AD cohort (explained ∼10% of variance). The difference in the effect size of GM volume atrophy and other measures should be considered in the context that it is modeled longitudinally whereas other imaging and systemic measures are obtained from baseline in an attempt to predict the effect of brain injury on longitudinal cognitive decline. Importantly, the effect of white matter injury on PACC decline is removed by GM volume atrophy emphasizing the relationship between white matter injury and neurodegeneration as previously reported.25,26 The effects of amyloid and systemic vascular risk on PACC decline are reduced by GM volume atrophy indicating that while amyloid and vascular risk affect neurodegeneration, 14 they impact cognitive decline through other potentially independent mechanisms. The relatively small but independent effect of reduced cerebral blood flow in predicting cognitive decline is also in line with previous research in preclinical and clinical AD27,28 and it remained significant even after including other contributors including white matter injury, tau, and gray matter volume atrophy. These results are not only in line with recent findings about the reduced cerebral blood flow in the early and late stages of AD29 –31 but also reveal an independent role of cerebral blood flow beyond amyloid, tau, and white matter injury, and systemic vascular risk in cognitive decline which warrants further investigation.
The synergistic effect of the amyloid factor with tau factor and white matter injury factor further explains PACC decline. While intriguing, the effect size of these interaction terms is smaller compared to the main effects of amyloid, tau, and systemic vascular risk factors. The lack of interaction between CVD and amyloid factors on PACC decline can be explained by the inclusion of tau in our models. As shown in our recent study, tau mediates the interactive effects of amyloid and CVD on cognition. 15
This study has some limitations. Notably, these results should be interpreted in the context of the study population (older adults without cognitive impairment) and their level of vascular risk, amyloid, and cognitive impairment. Specifically, we excluded individuals with extensive vascular risk factors at baseline, and thus the results might not represent the full clinical spectrum. In addition, the sample size was relatively small thus we were not able to include all the possible interactions between the obtained factors. Further research is needed to examine the reproducibility of our findings in other cohorts. Moreover, apart from tau, other brain injury measures were summarized using global whole-brain measures, accordingly, we also used a global cognition measure that is sensitive to early cognitive changes in preclinical AD. Further research is needed to extend this work to specific cognitive domains and investigate the regional specificity of these markers. Lastly, R1 (obtained from dynamically acquired PET) is a measure of tracer delivery and relative cerebral blood flow and does not reflect absolute cerebral blood flow.
Our study proposes a new framework to investigate the complex interactions between brain injury and systemic measures and their impact on cognition. We found that independent factors reflecting white matter injury, relative cerebral blood flow, systemic vascular risk, and amyloid and tau accumulation contribute to late-life cognitive decline.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X241237624 - Supplemental material for Vascular contributions to cognitive decline: Beyond amyloid and tau in the Harvard aging brain study
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X241237624 for Vascular contributions to cognitive decline: Beyond amyloid and tau in the Harvard aging brain study by Zahra Shirzadi, Rory Boyle, Wai-Ying W Yau, Gillian Coughlan, Jessie Fanglu Fu, Michael J Properzi, Rachel F Buckley, Hyun-Sik Yang, Catherine E Scanlon, Stephanie Hsieh, Rebecca E Amariglio, Kathryn Papp, Dorene Rentz, Julie C Price, Keith A Johnson, Reisa A Sperling, Jasmeer P Chhatwal and Aaron P Schultz in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH; [grant numbers P01AG036694]; Drs. Chhatwal, Sperling, Johnson, Rentz, and Schultz). Zahra Shirzadi gratefully acknowledges fellowship awards from the Alzheimer’s Society of Canada, the Health Equity Scholars Program, and the Brighfocus Foundation that supported this work. This research was carried out in part at the Athinoula A. Martinos Center for Biomedical Imaging at the Massachusetts General Hospital, using resources provided by the Center for Functional Neuroimaging Technologies, P41EB015896, a P41 Biotechnology Resource Grant supported by the National Institute of Biomedical Imaging and Bioengineering (NIBIB), National Institutes of Health. This work also involved the use of instrumentation supported by the NIH Shared Instrumentation Grant Program and/or High-End Instrumentation Grant Program; specifically, grant numbers S10RR021110, S10RR023401, and S10RR023043.
Acknowledgements
The authors thank the participants of the Harvard Aging Brain Study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Zahra Shirzadi: conception and design of the study, analysis of data, drafting the text or preparing the figures
Rory Boyle: analysis of data, revising the text
Wai-Ying W. Yau: analysis and acquisition of data, revising the text
Gillian Coughlan: analysis of data
Jessie Fanglu Fu: analysis of data
Michael J Properzi: analysis of data
Rachel F. Buckley: analysis of data
Hyun-Sik Yang: analysis and acquisition of data, revising the text
Catherine E Scanlon: analysis and acquisition of data
Stephanie Hsieh: analysis and acquisition of data
Rebecca E. Amariglio: analysis and acquisition of data
Kathryn Papp: analysis and acquisition of data
Dorene Rentz: analysis and acquisition of data
Julie C. Price: analysis of data
Keith A. Johnson: conception and design of the study
Reisa A. Sperling: conception and design of the study, revising the text
Jasmeer P. Chhatwal: conception and design of the study, analysis of data
Aaron P. Schultz: conception and design of the study, analysis of data, drafting the text or preparing the figures
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.