
Abstract
The effectiveness and safety of human urinary kallidinogenase (HUK) in acute ischemic stroke (AIS) patients undergoing endovascular therapy (EVT) due to large vessel occlusion (LVO) was unclear. A pooled analysis was performed using individual data from the DEVT and RESCUE BT trials. Patients were divided into two groups based on HUK treatment. The primary outcome was the 90-day modified Rankin Scale (mRS) score. Safety outcomes included 90-day mortality and symptomatic intracranial hemorrhage (sICH) within 48 hours. A total of 1174 patients were included in the study. Of these, 150 (12.8%) patients received HUK. The adjusted common odds ratio (OR) of the mRS score was 1.458 (95% confidence interval [CI] = 1.072–1.983; p = 0.016) favoring HUK. The incidence of sICH (2.0% vs. 8.6%; adjusted OR: 0.198; 95% CI: 0.061–0.638; p = 0.007) and mortality (11.3% vs.18.5%; adjusted OR: 0.496; 95% CI: 0.286–0.862; p = 0.013) was lower in HUK group than non-HUK group. This association was consistent with propensity score-matching and the inverse probability of treatment weighting analysis. In conclusion, HUK was safe and associated with a preferable prognosis in AIS patients due to LVO in the anterior circulation.
Introduction
Acute ischemic stroke (AIS) is a major cause of morbidity and death worldwide, thus considerably increasing the global economic burden annually. 1 Endovascular therapy (EVT) has become a standard treatment for AIS patients caused by large vessel occlusion (LVO). EVT can restore cerebral blood flow perfusion early and salvage ischemic penumbra, thereby reducing mortality and improving prognosis. 2 However, severe functional damage is still observed in some patients despite active reperfusion, which might be caused by different pathological processes, such as excitotoxicity reduction, oxidative stress, inflammation, and cellular apoptosis. 3 Because of these pathological processes, the application of neuroprotection therapy after successful reperfusion has gained significant attention.
Research suggests that the kallikrein-kinin system might be associated the key pathological hallmarks of ischemic and traumatic brain injury (e.g. edema formation, inflammation, and thrombosis). 4 Kallikrein is distributed in various tissues of the body and human urinary kallidinogenase (HUK) is a tissue kallikrein (TK) that is extracted from male urine. The literature indicates that HUK can regulate blood pressure, smooth muscle contraction and diastole, vascular cell growth, vascular permeability, inflammatory cascade response, electrolyte homeostasis, and pain stimulation by cleaving kininogen to release vasoactive kinins, which activates bradykinin B1 and B2 receptors in a rat model with middle cerebral artery occlusion. 5 Furthermore, exogenous HUK improves cerebral blood flow (CBF) and ameliorated neurological deficits in the mice model. 6 Moreover, in AIS patients, HUK expression is negatively associtaed with the incident and recurrent stroke and positively correlated with the favorable outcomes.7,8 A systematic review comprising 24 trials and 2,433 participants reveals that individualized intravenous administration of exogenous HUK was substantially beneficial for AIS patients. 9 However, the effectiveness and safety of HUK in AIS patients undergoing EVT remains undertermined. This study aims to investigate the effectiveness and safety of exogenous HUK therapy in LVO patients who underwent EVT.
Method
Patient selection
The AIS patients who underwent EVT treatment for anterior circulation LVO were selected from two randomized controlled trials, including the DEVT trial 10 and the RESCUE BT trial. 11 The DEVT, was a multicenter, randomized, open-label clinical trial conducted at 33 stroke centers in China (http://www.chictr.org.cn, ChiCTR-IOR-17013568), while the RESCUE BT was an investigator-initiated, multi-center, randomized, double-blind, placebo-controlled trial conducted at 50 stroke centers in China (http://www.chictr.org.cn, ChiCTR-IOR-17014167). The DEVT trial and the RESCUE BT trial followed the ethical principles of the Helsinki Declaration and were approved by the ethics committees of the Xinqiao Hospital, Army Medical University, and all participating centers. Written informed consent was taken from all the patients or their legal representatives before enrolled in these trials.10,11 Main inclusion criteria included: (1) Aged 18 years or older; (2) Occlusion of the intracranial internal carotid artery (ICA), M1 or M2 segment of the middle cerebral artery (MCA) confirmed by computer tomography angiography (CTA), magnetic resonance angiography (MRA) or digital subtraction angiography (DSA); (3) Acute ischemic stroke occurred within 24 hours of time last known well and then received EVTs. Main exclusion criteria included: (1) Pre-morbidity with a modified Rankin scale (mRS) score of ≥2; (2) Incomplete data on follow-up and non-detailed HUK treatment data; (3) Severe heart/liver/renal/lung/hemopoietic system dysfunction; (4) CTA or MRA evidence of hemorrhage.
HUK treatment
Patients received EVT, including mechanical thrombectomy, thromboaspiration, balloon dilation, stenting, intra-arterial thrombolysis, or various combinations of these approaches, as well as the best medical care according to the guidelines provided by modern acute stroke care. The HUK treatment data was obtained by reviewing patients’ electronic medical records. Based on whether received HUK therapy, patients were divided into two groups: HUK and non-HUK. The HUK therapy was applied at the discretion of the physician as needed. The drug instructions were 0.15 PNA unit HUK (Trade name: Kailikang, Guangdong Techpool Bio-pharma Co., Ltd) was diluted in 100 mL of 0.9% saline solution before infusion. The actual duration of HUK varied depending on the of the hospitalization length. HUK was recomenmended to be administered once a day as a single intravenous dose for 21 maximum consecutive days according to the recommended instructions.
Data collection
The following details of the patients were extracted from the combined database: sex, age, medical history, including hypertension, atrial fibrillation, smoking, diabetes mellitus, hyperlipidemia, ischemic stroke, and coronary heart disease. Furthermore, stroke etiology, the cerebral artery occlusion site, severity of ischemic injury upon admission, systolic and diastolic blood pressure upon admission, collateral vessel status, quality of reperfusion, time from stroke onset to groin puncture and randomization were all included. Two researchers independently collected the data and any discrepancies were resolved through consensus. If agreement could not be reached, a third researcher was consulted. The severity of ischemic injury was measured using the National Institutes of Health Stroke Scale (NIHSS) score 12 , whereas the stroke etiology was classified according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification. 13 The Alberta Stroke Program Early Computed Tomography Score (ASPECTS; range, 0 to 10) was used for quantifying the brain tissue alterations due to AIS. 14 The American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) collateral vessel grading system was utilized for assessing the collateral vessel status. 15 The time of stroke onset was the patient’s last known normal time. The quality of reperfusion was evaluated by the expended Thrombolysis in Cerebral Infarction (eTICI) score on the final angiogram. 16
Outcomes
The primary outcome was the mRS score at 90 days, which was used to evaluate neurological functional disability. The mRS score ranges from 0 (indicating no residual symptoms) to 6 (indicating death). 17 The secondary outcomes included the rate of favorable functionals, indicated by the mRS score of 0–3 (indicating an ability to walk unassisted), function independence, defined by the mRS score of 0–2 (indicating the ability to manage one’s affairs without assistance), and excellent outcomes depicted by the mRS score of 0–1 (indicating the ability to carry out all usual duties and activities) at 90 days. For safety outcomes, the mortality within three months and symptomatic intracranial hemorrhage were evaluated using follow-up CT or MRI based on the Heidelberg Bleeding Classification (HBC) within 48 hours. Follow-up examinations were conducted by local neurologists who were blind to treatment information and had received specialized training.
Statistical analysis
The variable’s statistics were computed based on their data type. The continuous variables were presented as median and interquartile range. The differences between the HUK and non-HUK groups were compared using the Mann-Whitney U test, χ2, or Fisher exact test, as appropriate. Categorical variables were reported as numbers and percentages sand and analyzed by the Chi-squared or Fisher exact test, as appropriate.
Furthermore, univariable analysis was performed, then using an ordinal logistic regression model, the shift toward mRS improvement by one score, while binary logistic regression was used for dichotomized outcomes such as sICH, 90-day mortality, mRS 0–1, 0–2, and 0–3. Potential confounding factors were selected based on clinical experience, their association with stroke outcomes, sociodemographics analysis results, and those associated with functional outcomes in the literature. To assess the adjusted odds ratios, the following variables were considered in the logistic regression model: age, NIHSS and ASPECTS score at admission, onset to randomization time, trail, and occlusion site. These variables were also used for balancing the covariates. Using the nearest-neighbor matching algorithm, the covariates were balanced through 1:1 propensity score matching (PSM) with a caliper width of 0.2.Furthermore, the treatment effect was estimated using the inverse probability of treatment weighting (IPTW) by utilizing the inverse propensity score to weigh each subject. The doubly robust estimation was used to reduce bias as it was less sensitive to misspecification. A p-value of <0.05 was considered to be statistically significant. For statistical assessment, IBM SPSS Statistics v.27 (SPSS Inc.) and R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria) were employed. Furthermore, all of the work has been reported following the STROCSS criteria. 18
Results
The characteristics of patients
Based on the inclusion and exclusion criteria, 1174 out of 1182 patients were included int this study (Supplementary Material Figure 1.). All patients completed 90 days of follow-up. Among them, 683 (58.2%) were men, and the average age was 68 (57–75) years old. At baseline, the NIHSS score was 16 (12–19), the ASPECTS score was 8 (7–9), and the systolic blood pressure (SBP)/diastolic blood pressure (DBP) was 145 (130–161)/84 (75–95) mmHg. A total of 150 (12.8%) received HUK treatment, while 1,024 (87.2%) did not. Overall, no statistically significant difference was observed in patient clinical characteristics between the two groups (Table 1).
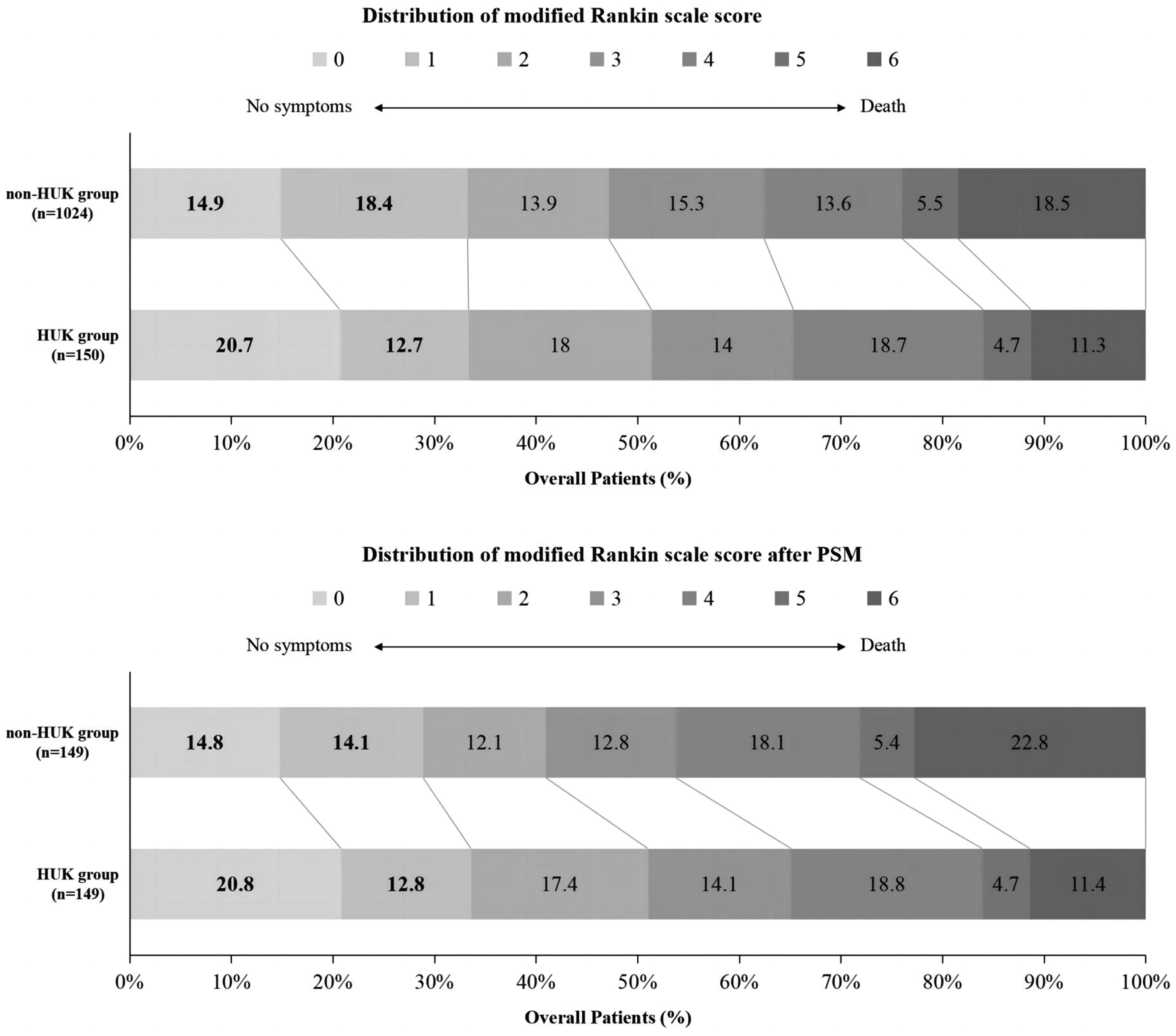
Distribution of the modified Rankin scale (mRS) score at 90 days in the HUK group and the non-HUK group. A, shown are scores on the mRS for patients of all patients treated by EVT. B, shown are scores on the mRS for patients treated by EVT after PSM. HUK: human urinary kallidinogenase; EVT: endovascular therapy; PSM: propensity score matching.
Baseline characteristics of all the patients.
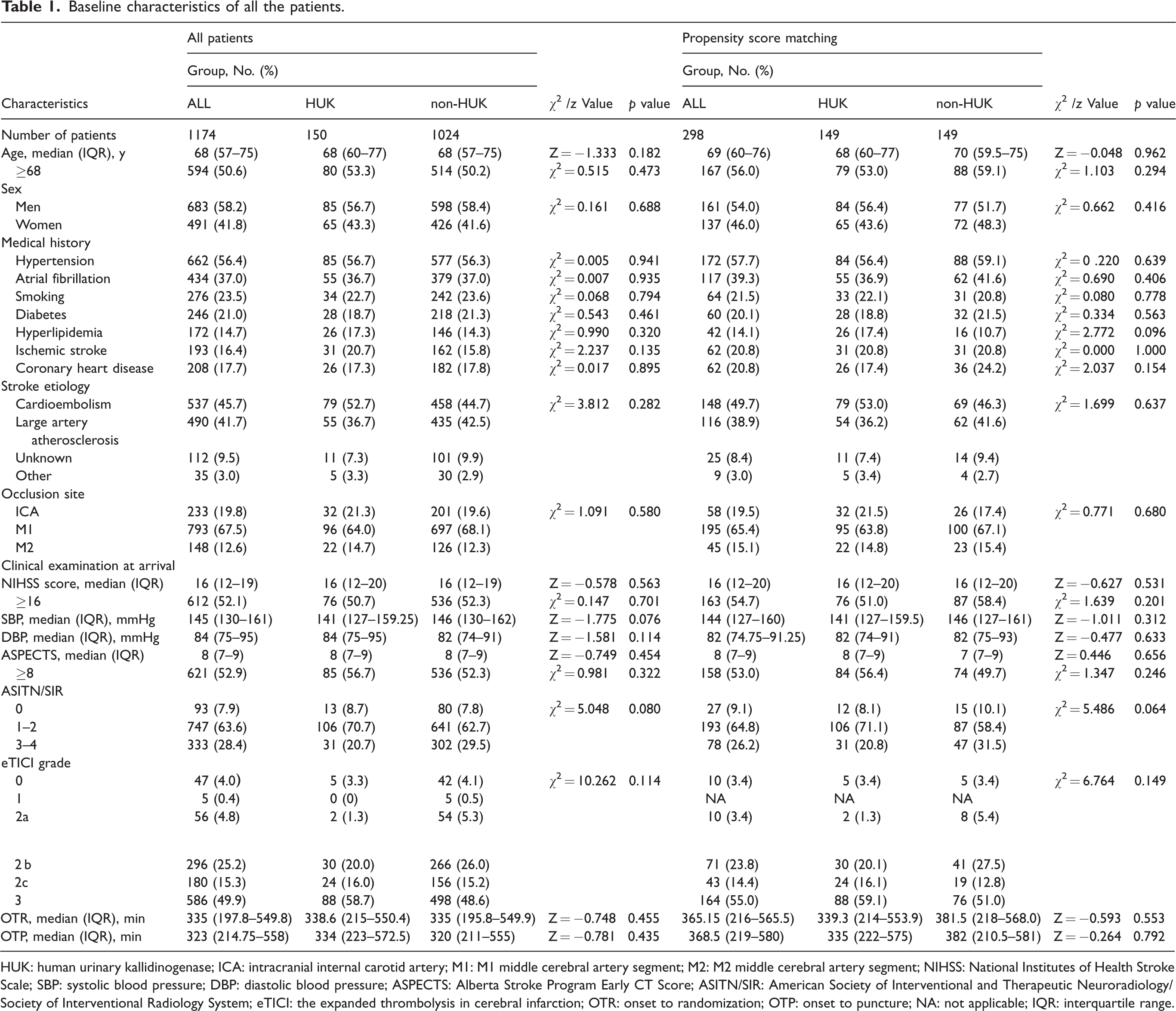
HUK: human urinary kallidinogenase; ICA: intracranial internal carotid artery; M1: M1 middle cerebral artery segment; M2: M2 middle cerebral artery segment; NIHSS: National Institutes of Health Stroke Scale; SBP: systolic blood pressure; DBP: diastolic blood pressure; ASPECTS: Alberta Stroke Program Early CT Score; ASITN/SIR: American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology System; eTICI: the expanded thrombolysis in cerebral infarction; OTR: onset to randomization; OTP: onset to puncture; NA: not applicable; IQR: interquartile range.
Primary outcome
Primary outcome analysis indicated that adjusted common odds ratio (OR) for a favorable shift to a lower mRS score at 90 days was 1.459 (95% CI = 1.073–1.985; p = 0.016), favoring HUK after adjusting for confounding factors. The median (interquartile range) mRS score at 90-day was 2 (1–4) in HUK group and 3 (1–4) in non-HUK group (Table 2). Figure 1 indicates the distribution of mRS score of the treated individuals. Using the IPTW method, analysis of the primary outcome indicated the adjusted common odds ratioOR for a favorable shift to a lower mRS score at 90 days was 1.325 (95% CI = 1.150–1.528; p < 0.001; Table 3), favoring HUK. The finding was consistent with the doubly robust analysis results (Table 3 and Figure 2).
Effectiveness outcomes and safety outcomes.
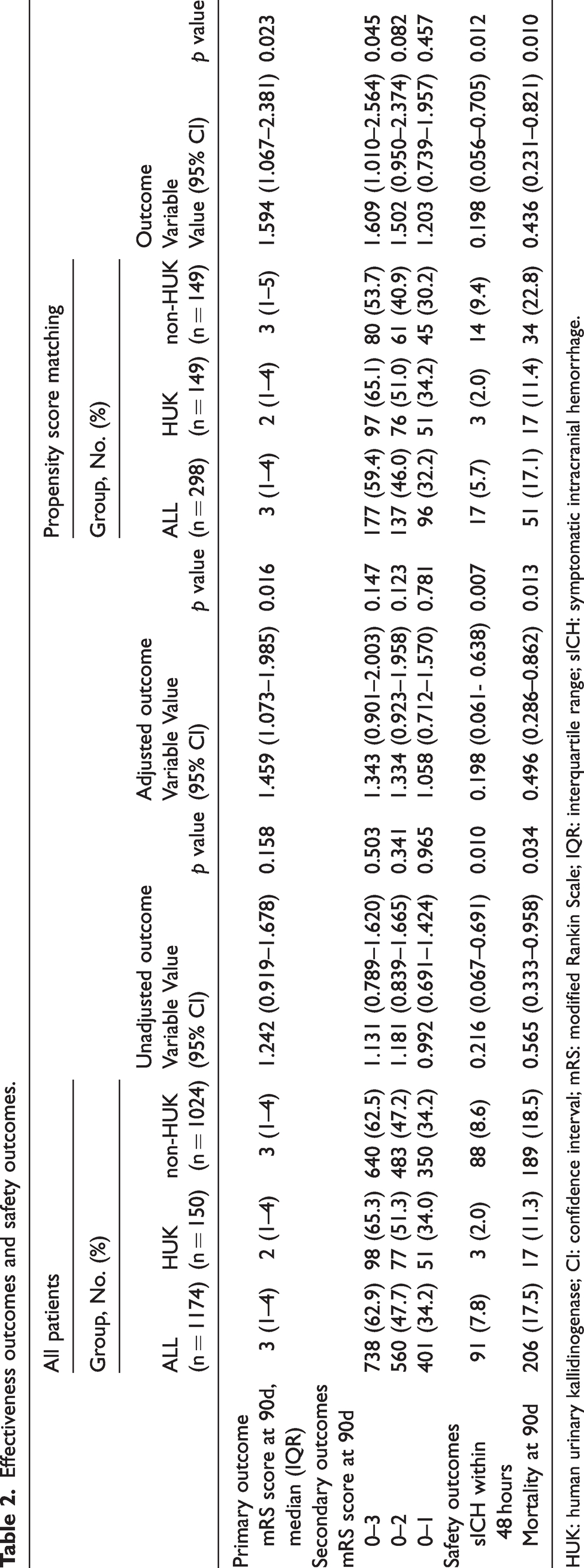
HUK: human urinary kallidinogenase; CI: confidence interval; mRS: modified Rankin Scale; IQR: interquartile range; sICH: symptomatic intracranial hemorrhage.
Effectiveness outcomes and safety outcomes in the inverse probability of treatment weight cohort.
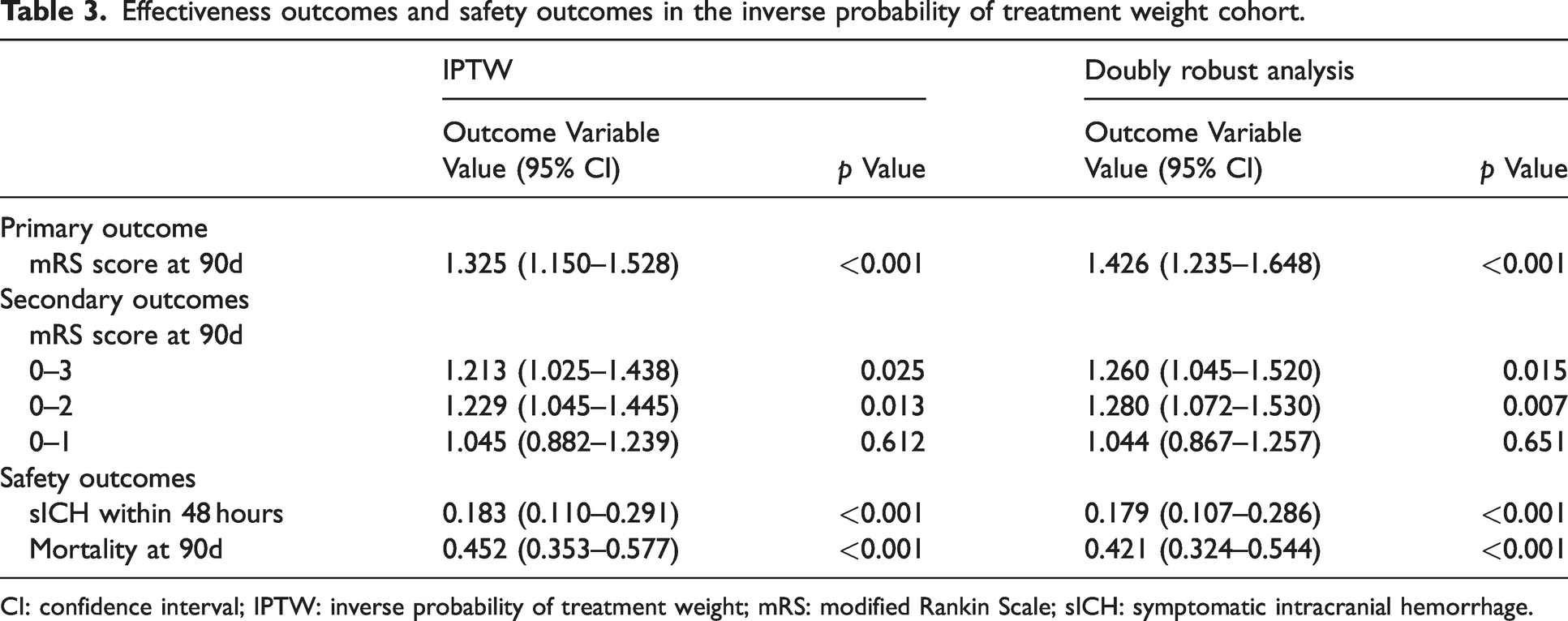
CI: confidence interval; IPTW: inverse probability of treatment weight; mRS: modified Rankin Scale; sICH: symptomatic intracranial hemorrhage.
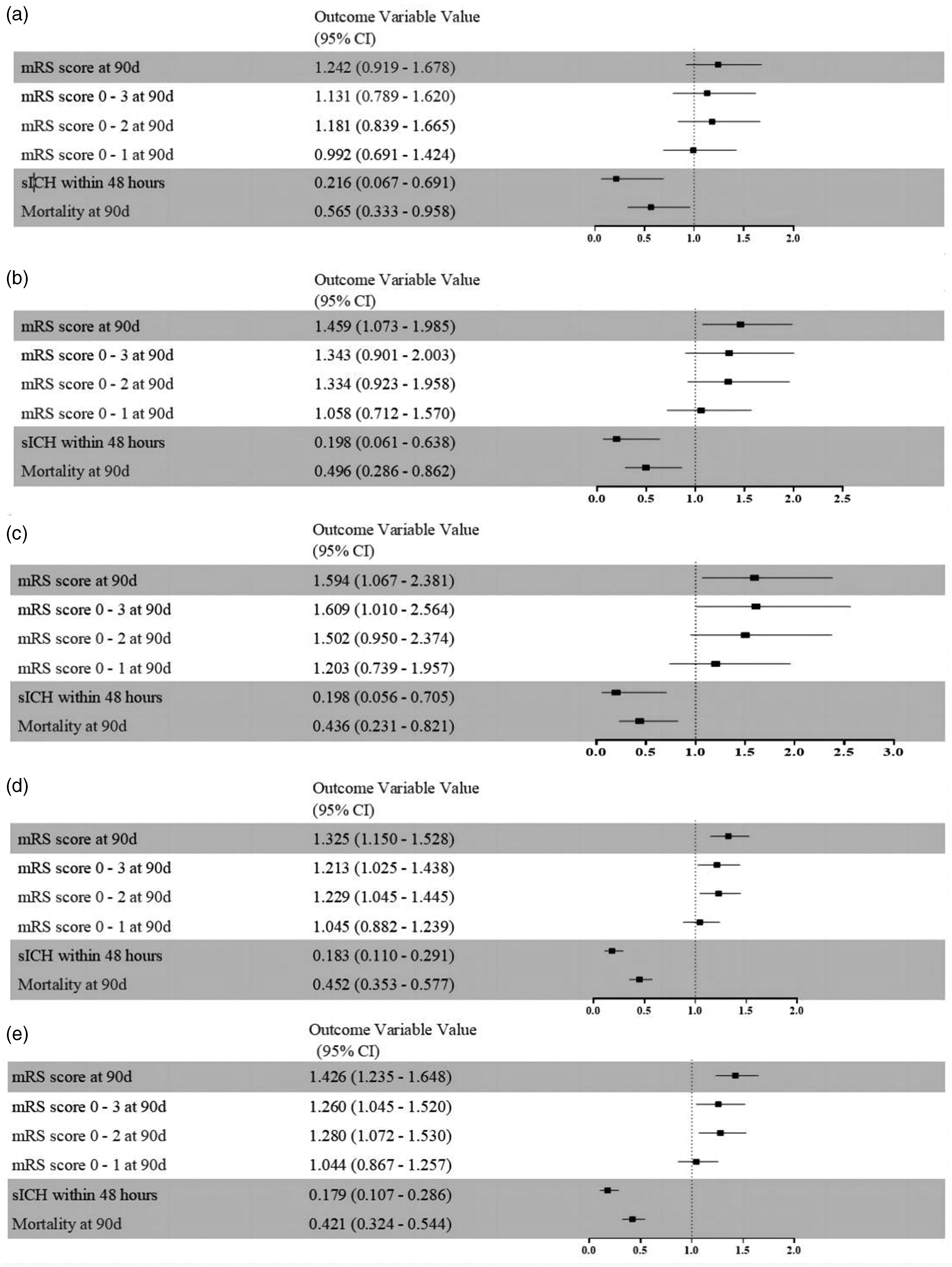
The effectiveness and safety outcomes. (a) Unadjusted outcomes. (b) Adjusted outcomes for confounding factors. (c) Propensity score matching analysis. (d) Inversed probability of treatment weighting and (e) Doubly robust analysis. sICH: symptomatic intracranial hemorrhage; mRS: modified Rankin Scale; CI: confidence interval.
Secondary outcome
Table 2 illustrated the secondary outcomes. The proportion of patients who achieved a favorable functional outcome (mRS 0–3) was 65.3% and 62.5% in HUK and non-HUK groups, respectively. The adjusted cOR was 1.343 (95% CI = 0.901–2.003). The function independent (mRS 0–2) was observed in 51.3% and 47.2% of patients in the HUK group and non-HUK groups, respectively, with an adjusted cOR of 1.344 (95% CI = 0.923–1.958). The rates of excellent outcome (mRS 0–1) were similar in both groups (34.0% vs. 34.2%; 1.058 [95% CI = 0.712–1.570]). Furthermore, using the IPTW method, the HUK group indicated a significantly higher frequency of favorable functional outcomes than the non-HUK group (OR = 1.213; 95% CI = 1.025–1.438; p = 0.025; Table 3) and the proportion of patients who achieved functional independence was higher in HUK group as compared to the non-HUK group (OR = 1.229; 95% CI = 1.045–1.445; p = 0.013; Table 3). These findings were consistent with the doubly robust analysis results (Table 3 and Figure 2).
Safety outcomes
The prevalence of sICH in the HUK group was 2.0%, which was significantly lower than the non-HUK group (8.6%) (p = 0.007). The investigation revealed the adjusted cOR was 0.198 (0.061–0.638; Table 2). Moreover, the mortality in the HUK group was significantly lower than that the non-HUK group at 90 days (11.3% vs. 18.5%; p = 0.013). However, the adjusted cOR was the same at 0.496 for both groups (95% CI = 0.286–0.862; Table 2). Using the IPTW method, the HUK group had significantly lower mortality within 90 days compared to the non-HUK group (OR = 0.452; 95% CI = 0.353–0.577; p < 0.001; Table 3), without increasing the incidence of sICH than the non-HUK group (OR = 0.183; 95% CI = 0.110–0.291; p < 0.001; Table 3). These findings were consistent with the doubly robust analysis results (Table 3 and Figure 2).
Propensity score matching analysis (PSM)
After 1:1 PSM, the baseline characteristics between the groups were well-balanced, resulting in 149 matched pairs (details in Table 1). The median mRS score at 90 days was 2 and 3 in HUK and non-HUK groups, respectively. According to the pairwise comparison, the mRS score at 90 days of HUK patients was significantly lower than non-HUK patients, with an OR of 1.594 (95% CI = 1.067–2.381; p = 0.023; Table 2). The rate of favorable functional outcome in the HUK group was notably better compared with the non-HUK group (97 of 149 patients [65.1%] vs. 80 of 149 patients [53.7%]; p = 0.045), with OR of 1.609 (95% CI = 1.010–2.564; Table 2). In the safety outcomes, sICH was observed in 3 of 149 (2.0%) HUK and 14 of 149 (9.4%) non-HUK patients after PSM (OR = 0.198; 95% CI = 0.056–0.705; p = 0.012; Table 2). The mortality in the HUK group was 11.4% (17/149 patients), whereas it was 22.8% (34/149 patients) in the non-HUK group (OR = 0.436; 95% CI = 0.231–0.821; p = 0.010; Table 2). The distribution of the mRS score for treated populations is shown in Figure 1.
Subgroup analysis
The functional outcome at 90 days remained consistent in the entire population of the following subgroups, including age ≥68, men, baseline NIHSS < 16, the onset of randomization ≥335 min occlusion site in M1 and M2, eTICI in 2 b–3, ASITN/SIR in 3–4, tirofiban treatment, hypertensive population and RBT database. According to the interaction analysis, there was heterogeneity in the effectiveness of HUK in ASITN/SIR (p for interaction = 0.016, Figure 3 and Supplementary Material Figure 2).
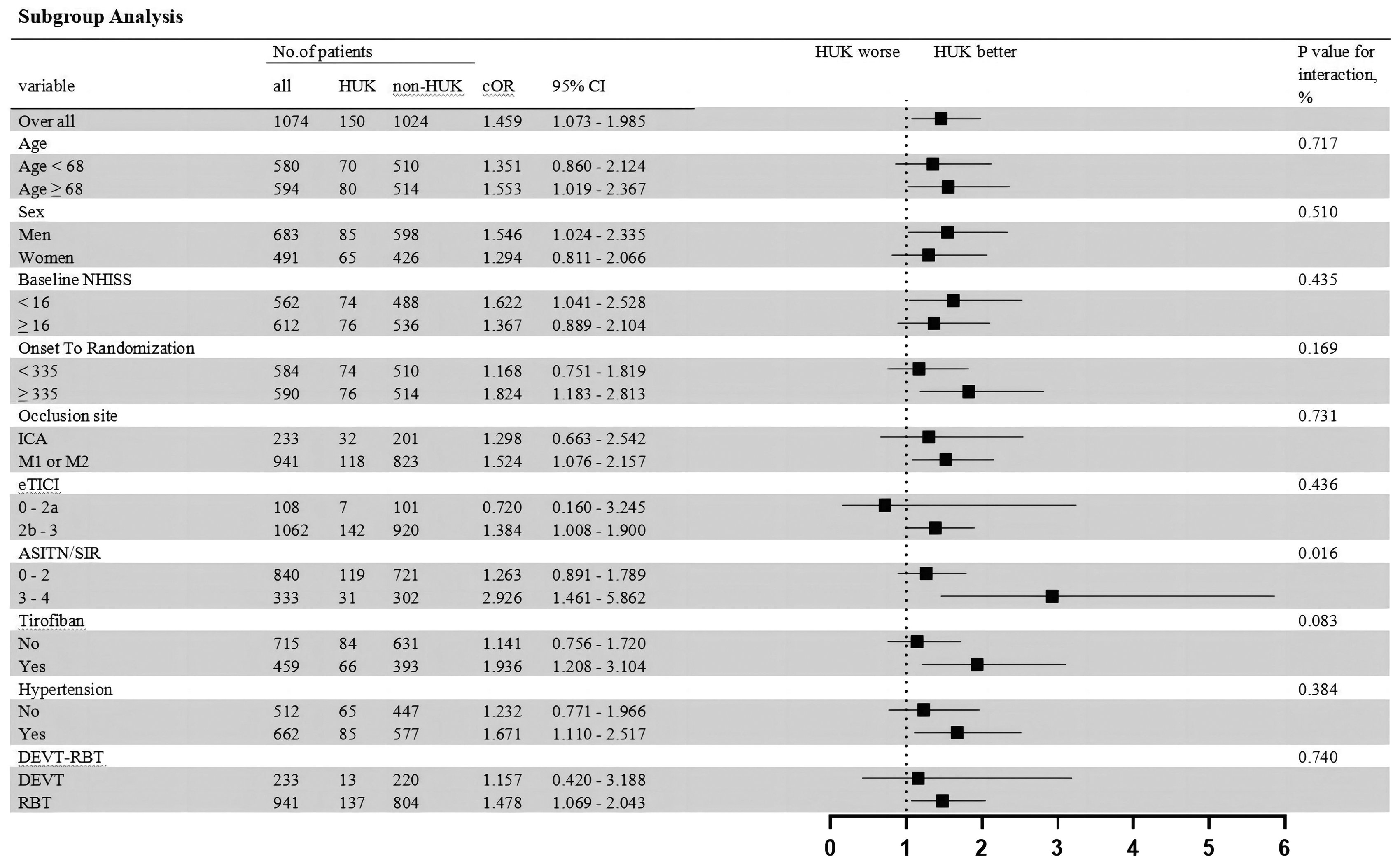
Subgroup analysis of modified Rankin Scale (mRS) score at 90 days in the HUK group and the non-HUK group. A forest plot shows the odds of improvement of one point on the modified Rankin scale at 90 days. The thresholds for age, NIHSS, eTICI, and onset to recanalization time were chosen at the median. HUK: human urinary kallidinogenase; eTICI: the expanded Thrombolysis in Cerebral Infarction; NIHSS: National Institute of Health Stroke Scale; ASITN/SIR: American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology System; ICA: intracranial internal carotid artery; M1: M1 middle cerebral artery segment; M2: M2 middle cerebral artery segment; CI: confidence interval; DEVT: the DEVT trial; RBT: the RESCUE BT trial.
Sensitivity analysis
A sensitivity analysis was performed. By univariate and multivariate analysis, there were several variables that affect the mRS score including: age, diabetes, coronary heart disease, occlusion site, NIHSS score on admission, ASPECTS score on admission, ASITN/SIR and eTICI grade. (Supplementary Material Table 1) After IPTW analysis, the adjusted common OR for a favorable shift to a lower mRS score at 90 days was 1.221 (95% CI = 1.059–1.408; p < 0.001; Supplementary Material Table 2), favoring HUK. The mortality within 90 days in HUK group was lower than the non-HUK group (OR = 0.635; 95% CI = 0.505–0.797; p < 0.001; Supplementary Material Table 2), without increasing the incidence of sICH than the non-HUK group (OR = 0.189; 95% CI = 0.115–0.297; p < 0.001; Supplementary Material Table 2). Via sensiticity analysis, the result was still robust with the primary analysis.
Discussion
This research aims to elucidate the effectiveness and safety of HUK in AIS patients treated by EVT due to LVO in the anterior circulation. Based on the DEVT and RESCUE BT databases, a large sample size was selected, and baseline and outcome data were analyzed. The findings revealed that HUK was safe and associated with a preferable prognosis within 90 days.
The endogenous HUK is a biomarker for better prognosis of stroke patients. The HUK is one of the TKs that has been found in human urine, and is widely distributed in different organ tissues, such as kidneys, blood vessels, the central nervous system, etc. It has been observed that high plasma TK levels can alleviate ischemic stroke in animal models and in vitro studies.19 –21 Research proposed that the higher plasma TK levels could be a biomarker to predict a lower risk of stroke recurrence and a longer stroke-free interval.6,7 Additionally, a singal center research found that higher baseline TK level in serum was independently associated with a favorable 90-day outcome in AIS patients with acute reperfusion therapy and the positive predictive value was 84.2%, the negative predictive value is 56.8%. 8 In this study, exogenous HUK was associated with a preferable prognosis in AIS patients treated by EVT, Therefore, further multi-center studies are required for its confirmation.
With the gradual maturation of EVT technology and equipment, EVT can significantly benefit patients with LVO by restoring blood flow reperfusion. Unfortunately, positive vascular reperfusion has not been fully translated for good patient prognoses, with <50% good prognoses cases. 22 Strategies to improve the recanalization rate alone were insufficient in achieving clinical benefits in AIS patients. The concept of futile recanalization, first identified in canine experiments, has become a major hindrance, limiting patient benefit. 23 However, various thrombectomy techniques have gradually stabilized the recanalization rates at >80%. 24 A meta-analysis revealed that the futile recanalization rate after successful reperfusion was >50%. 25 Several factors contribute to this phenomenon. On the one hand, during EVT, guidewires’ entry and mechanical expansion of balloons and stents can rupture atherosclerotic plaques, leading to the plaque fragments to fly downstream and promoting microcirculatory disorders. On the other hand, the inflammatory cells cause swelling of microvascular endothelial cells after ischemia and hypoxia, which narrows and even occludes the microvascular lumen. In addition, endothelial cells also become dysfunctional, causing brain tissue with infiltration with inflammatory cells and deteriorating neurological function. On the base of recanalization of large vessels, the treatments aiming at mechanisms for futile recanalization have gained importance. Neuroprotective treatments have been considered effective for these mechanisms and have attracted attention. Additionally, before recanalization caused by EVT, the neuroprotection pharmacodynamic effects were inadequate for the poor vascular conditions. In the current EVT era, the conjunction of recanalization with neuroprotective agents helps deliver neuroprotective agents to target brain regions. After recanalization, implementing neuroprotective treatments during the initial phase could maximize the effectiveness of both the neuroprotector and EVT, offering new possibilities for AIS patients. Current status-based, bridging neuroprotective agents are gaining substantial attention.
Preclinical trials have demonstrated that intravenous infusion of HUK could markedly reduce cerebral infarction caused by the occlusion of a middle cerebral artery in rats and improve neurological dysfunction. 26 Currently, as a state category I new drug approved by China’s State Food and Drug Administration (SFDA), HUK has been widely used for AIS patients to improve their neurological deficit as a neuroprotective agent. The RESK study was a multicenter phase IV study that enrolled 1206 eligible patients and confirmed that intravenous HUK infusion significantly improved the functions and neurological activities improvements in AIS patients. 27 Clinical researches showed that HUK could effectively and safely improve the neurological deficits of AIS patients with the use of rt-PA intravenous thrombolysis. 28 Unfortunately, the effectiveness and safety of HUK in AIS patients treated by EVT were previously uncertain.
The AIS secondary to LVO was considered the most devastating subtype. This study targeted AIS patients undergoing EVT for LVO and found the HUK treatment was linked to restoring the function of neurological deficits within 3 months. After the recanalization of large blood vessels, HUK can reach the ischemic lesion and enhance blood supply to both ischemic areas and microcirculation in the distal region, thereby restoring blood perfusion to the brain tissue in the ischemic semidark zone.9,26,29 Besides, prolonged vascular wall mechanical operations damaged endothelial and aggravated the inflammatory response. Moreover, reperfusion injury was accompanied by a severe inflammatory response. 30 According to animals research, HUK essentially inhibited inflammatory response, thus avoiding complications such as cerebral edema, hemorrhage, and even death.31 –33 Additionally, animal research has also demonstrated that HUK could enhance glial cell survival and ischemic core migration, as well as enhance cerebral glucose metabolism, exerting a neuroprotective effect on ischemic brain tissue damage.19,34
Our article demonstrated that HUK was safe after recanalization. The ReMEDy trial conducted in Australia indicated that the use of Recombinant Human Tissue Kallikrein (DM199) resulted in a 12% reduction in 90-day mortality, consistent with this study.
After conducting the subgroup analysis, it was apparent that certain subgroups of the population had a higher likelihood of achieving a better mRS score within 90 days. These factors and HUK were independent influencers on the 90-day functional prognosis with no statistically significant interaction, except for ASITN/SIR. The effectiveness of HUK was attributed to the adequate collateral flow. Furthermore, better collateral flow was linked with a higher probability of successful recanalization and better clinical outcomes. 35 These findings provide a theoretical basis for selection of population for clinical HUK treatment, which is highly encouraging.
The innovative feature of this study was as follows. Firstly, the data were sourced from two large-scale, multi-center databases in China which has significantly increased the credibility of the research. Secondly, previous neuroprotection trials did not consider patients who undergo successful recanalization, whereas this analysis was focused on AIS patients who received EVT, facilitating the effectiveness of neuroprotectants, including HUK. Our analysis found that the HUK was more effective in patients who achiceved successful recanalziation, which is conisistent to the notion of retesting the effect of neuro protective agents in the reperfusion era. (Supplementary Material Table 3 and Table 4) It may be beneficial to combine reperfusion with neuroprotective therapy and this pairing could facilitate the evolution of between time and stroke intervention, extending it from initial emergency response to delayed interventions. After rapid and effective endovascular recanalization, HUK is able to reach the ischemic lesion along the vascular route and make effect on inhibiting inflammatory response and enhancing blood supply. 36 Thirdly, HUK influenced multiple targets to produce its effects, validating it as a neuroprotective agent according to the Stroke Treatment Academic Industry Roundtable (STAIR) criteria that neuroprotective agents must be drugs with multi-target therapeutic effects. 37 Besides, various statistical methods were performed to evaluate the effectiveness and safety of HUK including the multivariable logistic analyses, PSM, IPTW and doubly robust estimation in this study.
There were still some non-negligible limitations in this study. First of all, this study was based on individual patient pool analysis, there were some drawbacks of own conditions, and there was inevitable selection bias for not randomized trials. However, the effectiveness and safety of HUK remained robust even after the multivariable logistic analyses, PSM, IPTW, doubly robust estimation and sensitivity analysis. Secondly, we obversed that HUK treatment was associated with the lower incidence of sICH. As a observational design, only association can be revealed in this study, and we cannot drew causal relationship. However, we do think this study have provided new insight with the use of HUK in AIS patients with an evidence level of class IIb. And large sample randomized control trials are needed for further confirmation. Thirdly the study lacks biochemical indicators before and after HUK treatment, which are required to confirm the mechanism of HUK. Meanwhile, the hospitalization time for AIS patients was recommended within 7–14 days since 2016, according to the clinical practice. In this study, the median duration of HUK usage is 7 days (IQR: 4 to 10 days), with a maximum of 21 day. Even though the duration of HUK in most patients is shorter than the maximum duration, HUK is still associated with the better prognosis in AIS patients treated by EVT in this study, which is in line with the findings of animal studies. 38 Last but not least, this study was based on patients with LVO in the anterior circulation. It should not be generalized to patients with small vessel occlusion or posterior circulation.
Conclusion
In summary, HUK is safe and associated with a better prognosis, in AIS patients treated by EVT due to LVO in the anterior circulation. In the future, randomized control trials should be performed to confirm the data of this study.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X241238033 - Supplemental material for The effectiveness and safety of human urinary kallidinogenase in acute ischemic stroke patients undergoing endovascular therapy
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X241238033 for The effectiveness and safety of human urinary kallidinogenase in acute ischemic stroke patients undergoing endovascular therapy by Mengmeng Wang, Changwei Guo, Jie Yang, Jing Li, Jinrong Hu, Zhouzhou Peng, Meng Guo, Lingyu Zhang, Fengli Li, Qingwu Yang, Wenjie Zi and Pengfei Wang in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chongqing Natural Science Foundation (cstc2020jcyj-msxmX0926) and Weihai Municipal Hospital Subject Climbing Plan General Project (FH-2021-XY01).
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
PW and WZ take responsibility for the conception, design and revising draft critically for important intellectual content and final approval of the version to be published; MW and CG were involved in the design of the study, analysis and interpretation of data, drafting the article, and contributed equally to this paper. JY worked on drafting the article and the analysis and interpretation of data. JL worked on the conception and design and revise the article. JH worked on acquisition and analysis of data. ZP and MG worked on acquisition and analysis of data. LZ worked on drafting the article. FL worked on drafting the article and revising it critically for important intellectual content; and QY worked on revising the draft critically for important intellectual content. The corresponding author attests that all listed authors meet the authorship criteria. All authors read and approved the final manuscript.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.