
Abstract
Research on stroke recovery has shifted from acute survival to the restoration of function and quality of life. Although many rehabilitative and restorative interventions have shown promising benefits, trial outcomes remain inconsistent. A major limitation is the misalignment between intervention mechanisms and outcome measures, along with an underuse of minimal clinically important difference thresholds that define meaningful changes. This opinion focuses on motor recovery trials after ischemic stroke and highlights how inappropriate reliance on global disability scales, short-term endpoints, or mismatched impairment and activity measures can obscure true therapeutic effects. Ultimately, aligning intervention mechanisms with appropriate outcome domains represents a fundamental principle in the design of interpretable and clinically meaningful stroke recovery trials.
Introduction
Stroke remains a leading cause of long-term disability worldwide, despite remarkable advances in acute reperfusion therapy. Intravenous thrombolysis and endovascular thrombectomy achieve high rates of angiographic reperfusion; however, functional independence at 90 days remains substantially lower, even in patients with successful recanalization.1,2 This persistent gap highlights the urgent need for adjunctive interventions that promote recovery beyond the acute phase.
Recovery following stroke is heterogeneous and influenced by biological factors, such as corticospinal tract integrity, as assessed via biomarkers such as motor-evoked potentials (MEP) and fractional anisotropy (FA). 3 These provide mechanistic insights but address only impairment. Stroke recovery, however, is multidimensional and encompasses activity and participation domains that directly impact quality of life (QOL).
The World Health Organization’s International Classification of Functioning, Disability and Health (ICF) provides a useful framework for conceptualizing recovery across three levels: (1) body functions and structures (impairment) (e.g., muscle strength), (2) activities (e.g., reaching, walking speed), and (3) participation (e.g., independence in activities of daily living (ADL), returning to the community) (Figure 1). This framework highlights the need to align interventions with outcome measures that are sensitive to the targeted level of recovery. For instance, impairment-focused interventions should be evaluated using the Fugl–Meyer Assessment (FMA); activity-focused programs with the Action Research Arm Test (ARAT), gait measures, or the Functional Independence Measure (FIM). Global disability scales including the modified Rankin Scale (mRS) and Barthel Index (BI) encompass both activity and participation domains rather than representing pure participation outcomes. Conceptually, the BI primarily reflects activity performance in basic ADL, while the mRS leans more toward participation by capturing overall social and functional independence. Patient-reported measures such as the EuroQol 5-Dimensions 5-Levels (EQ-5D-5L) are essential complements to fully assess participation and QOL. The failure to match intervention goals with outcome measures has contributed to negative and inconclusive rehabilitation trials. 4 Aligning post-intervention assessments with mechanistic targets is essential to ensure that restorative trials achieve true translational and clinically meaningful impact.
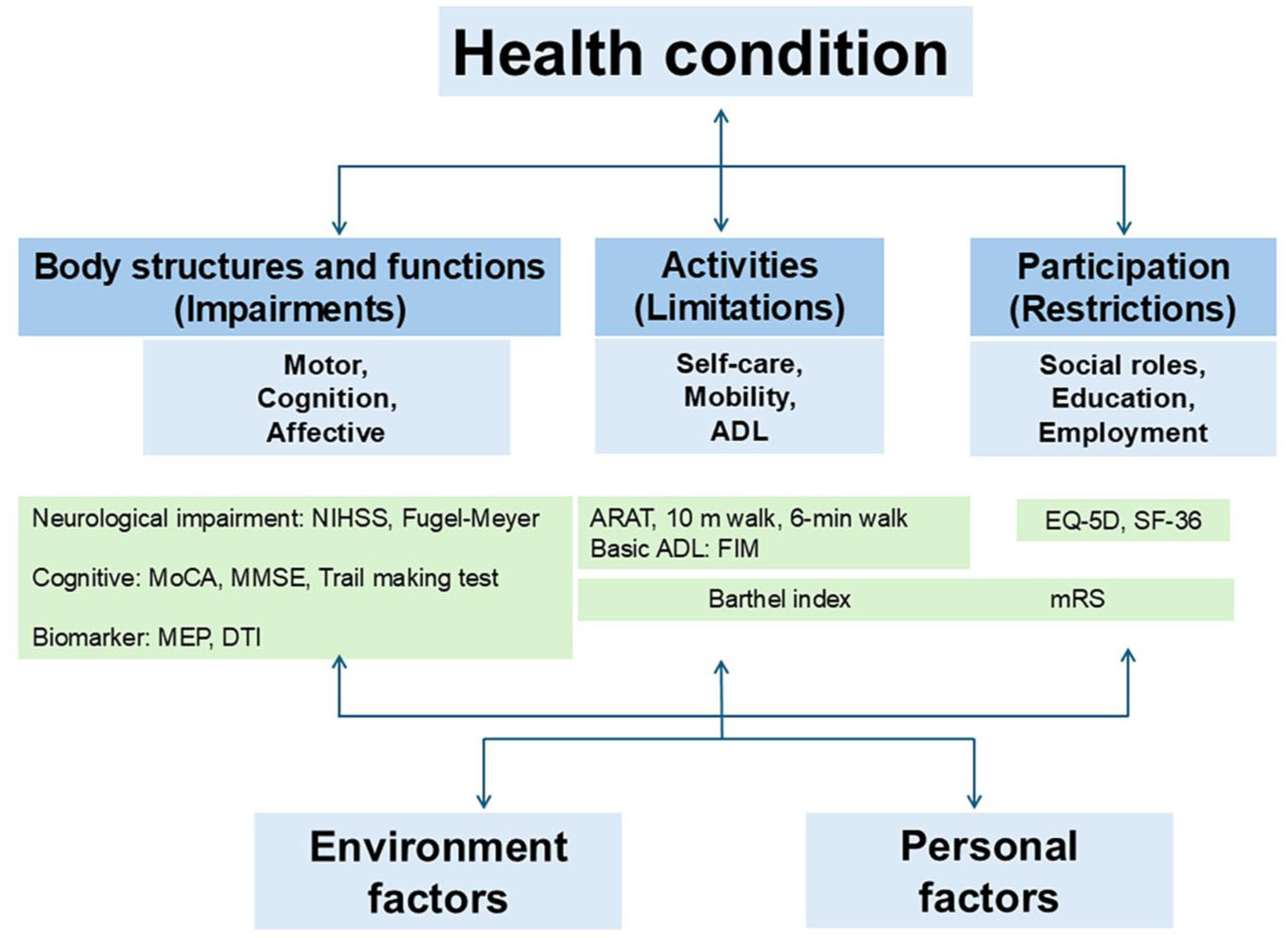
The ICF model of functioning and disability.
This opinion summarizes the evidence for restorative interventions and their outcome measures, focusing primarily on motor recovery trials after ischemic stroke and emphasizing how alignment between intervention mechanisms and outcome domains determines interpretability. We also discuss the role of minimal clinically important differences (MCID) in defining clinically meaningful change. Our purpose is not to re-rank therapies by efficacy, but rather to clarify how recovery should be measured in future clinical trials-thereby enabling rigorous, translational, and patient-centered research.
Interventions after stroke
The diversity of interventions for post-stroke recovery reflects the multifaceted nature of impairment, activity, and participation outcomes. In reviewing each approach, it is critical to consider not only signals of efficacy but also the alignment between intervention targets and the outcomes chosen to evaluate them (Table 1).
Interventions for post-stroke recovery, outcome measures, and level of evidence.
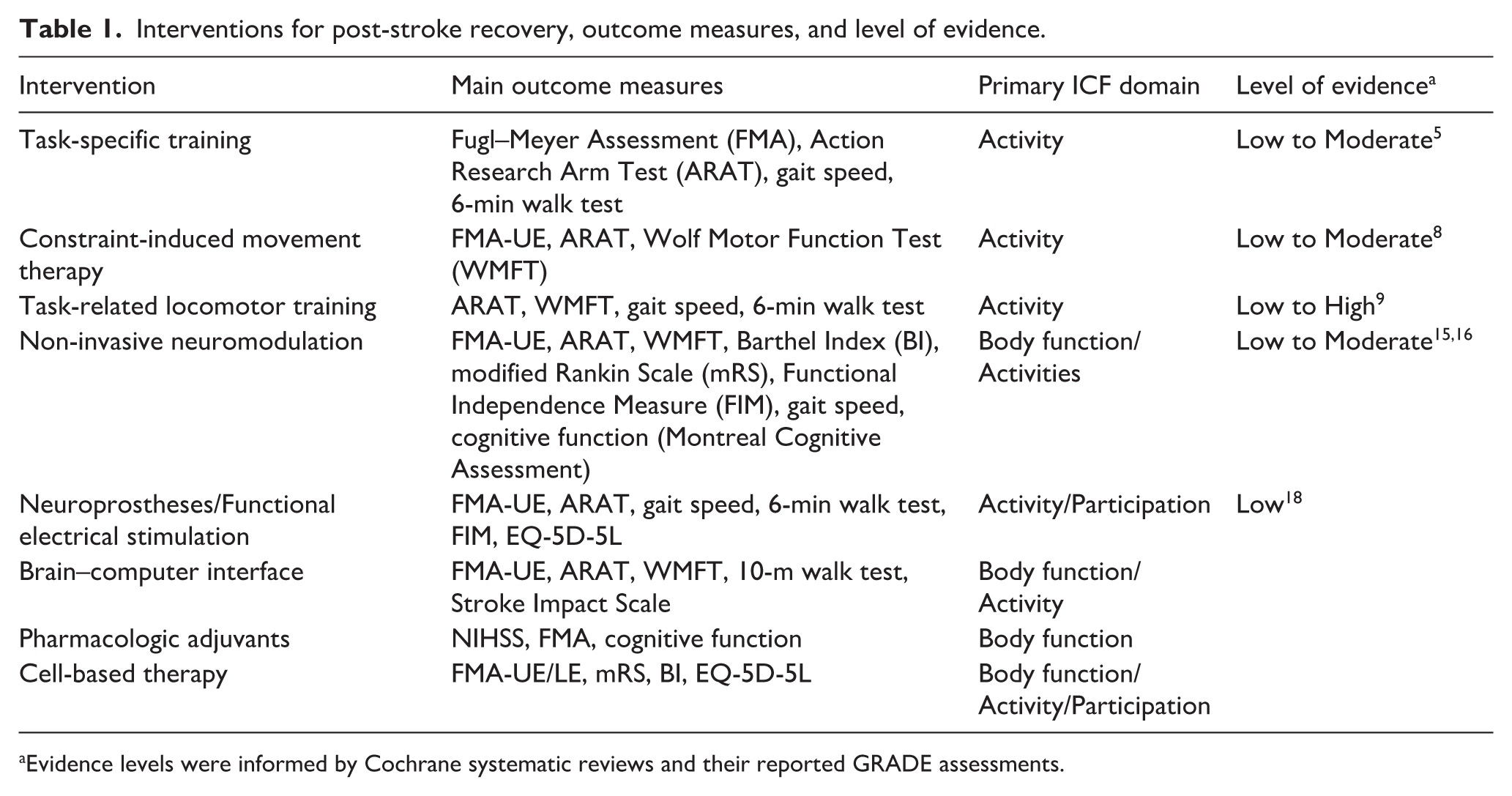
Evidence levels were informed by Cochrane systematic reviews and their reported GRADE assessments.
Task-specific, high-repetition training
Repetitive task-specific training is considered the foundation of motor rehabilitation. Cochrane reviews have demonstrated that high-intensity, task-oriented practice improves outcomes relative to usual care, especially within the first 6 months post-stroke. The effect size was modest but clinically relevant and was sustained for months in some studies. 5
Virtual Reality (VR)–based training enables high-repetition, goal-directed movement with small-to-moderate improvements in upper limb function (FMA, ARAT) and motivation when VR is combined with conventional therapy. 6
Constraint-Induced Movement Therapy
The Constraint-Induced Movement Therapy (CIMT) promotes the use of the paretic limb by restraining the unaffected arm. A randomized controlled trial (RCT) demonstrated durable improvements in upper-limb function between 3 and 9 months after stroke, primarily assessed using activity-level and patient-reported outcome measures. 7 Cochrane reviews have confirmed benefits on upper-limb activity outcomes, such as the ARAT, whereas effects on broader functional measures (e.g., WMFT, FIM) have been less consistent. 8 Notably, most large CIMT trials, including the EXCITE trial, 7 did not include impairment-based measures, such as the FMA, thereby limiting conclusions regarding impairment-level recovery. Although residual voluntary hand extension has frequently been used as an inclusion criterion, it likely reflects trial design and outcome selection rather than a definitive boundary of CIMT efficacy, underscoring an ICF-level mismatch between intervention targets and outcome measures.
Task-related locomotor training and electromechanical gait devices—lower limb
High-intensity locomotor training, treadmill-based therapy, and robot-assisted gait devices increase the likelihood of independent walking, particularly when applied in the subacute phase. Cochrane reviews report high-certainty evidence for gains in walking independence, although improvements in walking endurance (6-min walk test) are more modest. 9 However, because these interventions specifically target locomotor function, their effects may be underestimated when evaluated using global disability scales rather than task-specific walking outcomes.
Non-invasive neuromodulation
Repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) modulate cortical excitability and promote activity-dependent plasticity within motor networks. Mechanistically, these approaches are thought to influence interhemispheric inhibition and facilitate reorganization of residual corticospinal pathways, thereby supporting motor control recovery. Early experimental and clinical studies have demonstrated that non-invasive brain stimulation can enhance motor learning and improve upper-limb performance after stroke, particularly when combined with task-specific training.10 –12 However, more recent large multicenter RCTs, despite differences in stimulation intensity and study design, have consistently reported neutral results with respect to functional motor recovery.13,14 These neutral findings indicate that tDCS does not produce a large effect size at the population level in post-stroke motor recovery. Several factors, including methodological heterogeneity, variability in stimulation parameters, patient selection, and outcome sensitivity, have been proposed as potential explanations for these findings (discussed below). Consequently, the certainty of the evidence remains low to moderate, primarily owing to substantial heterogeneity in stimulation protocols, timing relative to stroke onset, patient selection, and outcome measures across studies. 15 Importantly, neuromodulation approaches are designed to modulate specific neural circuits that are involved in motor control. Consequently, their effects may be more readily detected in domain-specific motor outcomes than in global disability scales. When domain-targeted interventions are evaluated using broad global measures, such as mRS or BI, treatment effects may be diluted or obscured. 16 Similar challenges arise in other domain-specific interventions, such as aphasia rehabilitation. This mismatch between intervention targets and outcome measures may partly explain why some large RCTs have produced neutral findings despite biologically plausible mechanisms of action.
Neuroprostheses/functional electrical stimulation
Neuroprosthetic interventions directly target the peripheral nervous and musculoskeletal systems by providing electrical stimulation to induce functional movements. Functional electrical stimulation (FES) produces functional movements such as hand opening or correction of foot drop. Integrated rehabilitation enhances task-specific practice and supports neuroplasticity. Small RCTs show that peroneal-nerve FES improves gait speed, endurance (6-min walk test), and efficiency compared with no stimulation or orthosis. 17 Meta-analyses report small-to-moderate gains in impairment and activity outcomes (FMA-UE, ARAT, gait speed), but effects on participation (BI, EQ-5D-5L) remain inconsistent. 9 Evidence for repetitive peripheral magnetic stimulation is insufficient. 18
Brain-computer interface
Brain-computer interfaces (BCIs) decode neural activity (electroencephalography, electrocorticography, or functional near-infrared spectroscopy) related to motor intention and translate it into robotic or FES-assisted movements. RCTs have shown promising improvements in chronic stroke where conventional gains typically plateau. 19 Meta-analyses suggest moderate effect sizes; however, small sample sizes and protocol heterogeneity reduce certainty. 20 Future trials should aim to standardize protocols, expand sample sizes, and incorporate long-term follow-up.
Pharmacologic adjuvants
Selective serotonin reuptake inhibitors (SSRIs), particularly fluoxetine, were once thought to enhance recovery (FLAME trial), but a systematic analysis showed that SSRIs improve mood and anxiety but do not consistently enhance motor recovery (National Institutes of Health Stroke Scale [NIHSS] and FMA) or reduce functional dependence after stroke. 21 Levodopa combined with therapy showed no significant motor benefit. 22 Pharmacologic augmentation remains experimental.
Cell therapies
Mesenchymal stem cells, bone marrow mononuclear cells, and multi-lineage differentiating stress-enduring (Muse) cells were evaluated. Meta-analyses suggest the potential benefits of impairment (NIHSS, FMA) and ADL (mRS, BI) but with substantial heterogeneity in cell source, timing, and delivery.23,24
In terms of risk of bias, the overall assessment revealed that five studies had a low risk. 25 These studies primarily used the NIHSS, mRS, and BI as evaluation methods (Supplemental Table 1). Some of these studies showed that activities such as mRS and BI may improve after cell administration, although the cell sources, timing, and targets were different. A trial of Muse cells reported improvements in FMA-UE exceeding MCID thresholds (⩾5 points in chronic stroke), with additional benefits in EQ-5D-5L at 12 weeks. 26 However, lower limb scores demonstrated ceiling effects, limiting sensitivity. Systematic reviews have concluded that overall certainty remains low, with safety more consistently demonstrated than efficacy. 25
Outcome measures: Statistical versus clinical significance
Statistical significance is often interpreted as therapeutic efficacy. Moreover, clinically meaningful changes that matter to patients, caregivers, and the healthcare system are not merely reflected in p-values. Primary and key secondary outcome measures should align with the ICF levels.
Impairment measures
The FMA is the gold standard for assessing motor impairment. It is responsive, internationally validated, and includes the FMA-UE and FMA-LE subscales. However, the lower limb subscales may exhibit ceiling effects, necessitating complementary measures such as the 10-m walk or 6-min walk test. 27
Other measures include neurophysiological (MEP) and imaging biomarkers (FA), which provide mechanistic insights3,28 but are not always directly applicable to functional recovery. The NIHSS, while widely used in the acute phase, is insensitive to distal deficits, cognition, and fatigue, and suffers from floor effects in chronic stroke. 29
Activity measures
Activity outcomes bridge the gap between impairments and daily function. The ARAT and WMFT capture task-specific upper limb function, while gait speed (10-m walk test) and endurance (6-min walk test) reflect lower-limb activity. The FIM is widely used to measure functional status—capturing self-care, transfers, and cognition—but it requires trained raters and may exhibit ceiling or floor effects, 30 and involves licensing and training requirements. Therefore, task-specific measures, such as the ARAT and gait speed, are frequently used as complementary or alternative outcomes in stroke trials. These outcomes are consistent with those observed in common recovery trial interventions, including behavioral rehabilitation, non-invasive neuromodulation, pharmacological agents, and invasive or device-based approaches.31 –33
Participation measures
The mRS and BI are global measures covering both activity and participation—BI mainly reflects basic ADL (activity), while mRS captures overall independence (participation). The Stroke Impact Scale (SIS) and EQ-5D-5L provide valuable patient-centered perspectives.5,34 The ceiling and floor effects and cultural variability in health state valuation remain potential limitations. 35 Moreover, the BI is generally not suitable as the sole primary endpoint due to pronounced ceiling and floor effects. 34
MCID
Statistical significance does not always equate to clinical importance. The MCID defines the smallest change that is perceived as meaningful by patients (Supplemental Table 2). Established MCIDs include 5–12 points for FMA-UE in subacute stroke (4–7 points in chronic stroke), approximately 6 points for ARAT, ⩾0.16 m/s for gait speed, and 0.07–0.10 for EQ-5D-5L index scores. 36 Incorporating MCIDs ensures that trial outcomes represent tangible patient benefit.
Importantly, MCID values are context-dependent and should not be interpreted as fixed thresholds. They vary with baseline impairment severity, stroke chronicity, and the method of estimation (anchor-based vs distribution-based), and may not translate directly across different trial designs, intervention doses, or co-interventions. Moreover, the validity of MCID estimates is influenced by methodological factors, such as assessor blinding, outcome adjudication, and measurement rigor, which remain inconsistent across studies. Accordingly, MCID values should be interpreted in conjunction with intervention targets and outcome domains when evaluating recovery after stroke.
Beyond mean group differences, MCID-based responder analyses provide critical complementary information. Group mean changes may obscure clinically meaningful improvements in patient subsets, particularly in heterogeneous stroke populations. By contrast, responder analyses quantify the proportion of individuals who achieve a clinically meaningful threshold, thereby improving interpretability and translational relevance. This approach is especially important when biological recovery is constrained or variable, as mean changes alone may underestimate intervention-specific benefits.
Timing and follow-up
Outcome endpoints should be aligned with these mechanisms. Plasticity-oriented interventions should focus on outcomes at 3 months, whereas regenerative approaches require both early (6–12 weeks) and long-term (6–12 months) follow-up (Supplemental Table 1). Repeated measures and responder analyses, rather than mean changes alone, improve interpretability.
Integrating interventions and outcomes
A persistent question in stroke recovery research is why many clinical trials have yielded neutral results despite strong mechanistic rationale and encouraging early-phase findings. While lack of biological efficacy is one possible explanation, trial design factors are likely to play an equally important role. Stroke recovery interventions often target specific neural circuits or functional domains; however, their effects are frequently evaluated using broad global disability scales. Such mismatches between an intervention’s biological target and the outcome measures used to assess its effects may substantially reduce a trial’s ability to detect clinically meaningful improvements. In addition, biological heterogeneity in recovery potential, including variability in corticospinal tract integrity, lesion location, and baseline impairment, can further dilute treatment effects in heterogeneous trial populations. Prior work on stroke recovery has emphasized that inadequate patient stratification, insensitive outcome measures, and limited alignment between intervention mechanisms and outcome domains are major barriers to successful clinical translation. Moreover, heterogeneity in patient selection, stage of recovery, and treatment dosing further complicates interpretation. 37 Importantly, even recent high-quality multicenter trials such as NETS and TRANSPORT2,13,14 which employed rigorous designs and appropriate controls, yielded neutral results. The effective “dose” of neuromodulation—encompassing stimulation intensity, duration, repetition, and coupling with task-specific training—remains incompletely optimized across studies. 13 Moreover, the neutral findings of TRANSPORT2 may partly reflect a ceiling effect driven by highly intensive CIMT rather than a lack of biological effect. 14 Importantly, these findings further underscore how misalignment between intervention mechanisms and outcome measures can obscure biologically plausible effects. Consequently, negative trial results should not necessarily be interpreted as definitive evidence of inefficacy but may instead reflect limitations in trial design and outcome selection.
Therefore, optimal trial design requires explicit alignment between intervention mechanisms and the outcome domains used to evaluate them. For example, impairment-targeting approaches such as cell therapy should be evaluated using impairment measures (FMA), whereas activity-oriented interventions such as CIMT and FES require activity-based outcomes (ARAT, gait speed). Participation outcomes, such as the SIS and EQ-5D-5L, are essential for capturing a broader impact on patients.
To enhance translational interpretability, outcome selection should be guided by a pragmatic framework. Specifically, investigators should consider the following:
(1) the mechanistic target of the intervention (impairment, activity, or participation) to define the primary outcome domain;
(2) the expected time course of therapeutic effects to determine appropriate assessment windows;
(3) the anticipated effect size and inter-individual heterogeneity, supporting the use of MCID-based responder analyses alongside mean group comparisons; and
(4) the risk of ceiling or floor effects, prompting prespecified secondary or backup measures.
Trials that incorporate multiple outcome domains, MCID-based responder analyses, mean group comparisons, standardized rater training, and rehabilitation protocols across centers are more likely to generate interpretable and clinically meaningful results.
Future directions
Future trials should address the structural factors that contribute to misalignment between intervention mechanisms and outcome selection. Although impairment-based measures and global disability scales remain widely used for practical and regulatory reasons, they are often insensitive to domain-specific therapeutic effects. This limitation is particularly evident when trial design and outcome selection remain misaligned with advances in intervention science.13,38 As demonstrated across neuromodulation, CIMT, locomotor training, and regenerative therapies, reliance on global scales such as the mRS or BI, short-term endpoints, or mismatched impairment/activity measures may obscure biologically plausible benefits. To improve interpretability, primary endpoints should be explicitly aligned to the ICF domain targeted by the intervention, with long-term follow-up for regenerative approaches and routine incorporation of MCID-based responder analyses. Participation-level outcomes should be included when broader functional independence is expected to change. A more mechanistically grounded and domain-specific approach to outcome selection will improve the interpretability and translational relevance of future stroke recovery trials.
Practical considerations
Functional assessments often require skilled raters; centralized training and video-based scoring can improve reliability. 39 Emerging digital tools (e.g., wearable sensors and accelerometers) may reduce bias but require further validation. Rehabilitation “dose” is rarely standardized yet strongly influences outcomes, emphasizing the need for structured documentation in multicenter trials.
Conclusion
The validity and clinical relevance of stroke trials are dependent on appropriate alignment between interventions and outcome selection. Previous studies have often overemphasized impairment while neglecting activity, participation, and patient-reported outcomes. Future trials should align interventions with ICF domains, integrate MCID-based responder analyses, and employ rigorous multicenter methodologies to achieve patient-centered recovery. Ultimately, aligning intervention mechanisms with appropriate outcome domains represents a fundamental principle in the design of interpretable and clinically meaningful stroke recovery trials.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X261454108 – Supplemental material for Interventions and outcome measures for motor recovery after ischemic stroke: The importance of intervention-outcome alignment
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X261454108 for Interventions and outcome measures for motor recovery after ischemic stroke: The importance of intervention-outcome alignment by Masato Kanazawa, Keigo Tamakoshi and Masahiro Hatakeyama in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Acknowledgements
We thank Prof. Masanori Fukushima (Foundation of Learning Health Society Institute, Japan) and Prof. Takayoshi Shimohata (Gifu University, Japan) for continuous guidance and encouragement.
Author contributions
M.K. analyzed the data, developed the concept, and wrote the manuscript. K.T. and M. H. supervised all aspects of this project. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Kanazawa is an academic advisor, OhGooD Inc. The authors declare no financial interests related to the materials in this manuscript. Dr. Tamakoshi and Dr. Hatakeyama declare no competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant-in-Aid for Scientific Research 22H03183, 23K24442), a grant from TERUMO LIFE SCIENCE FOUNDATION and Moriyama Award of Japan Brain Foundation (Prof. Kanazawa).
Required author forms
Disclosure forms provided by the authors are available with the online version of this article.
Availability of data and materials
All data and materials are available within the article file on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.