
Abstract
This cohort study was conducted using prospective and retrospective data to investigate whether indirect encephaloduroarteriosynangiosis (EDAS) revascularization can reduce the risk of rebleeding in adult patients with hemorrhagic moyamoya disease (hMMD). We enrolled adult patients diagnosed with hMMD prospectively and retrospectively. All patients voluntarily chose to undergo EDAS or conservative treatment. The clinical features, angiographic findings, and follow-up outcomes were investigated and analyzed using the Kaplan–Meier survival analysis and Cox proportional hazards regression models to estimate rebleeding risks post-EDAS. Among the 186 patients with hMMD, 123 patients (66.1%) underwent EDAS, and 63 patients (33.9%) received conservative treatment. In the EDAS group, one (0.8%) patient suffered postoperative infarction, 16 patients (13.0%) experienced recurrent cerebral hemorrhage, and three patients (2.4%) died from rebleeding events. In the conservative treatment group, 18 patients (28.6%, p = 0.015) experienced cerebral rebleeding events and seven (11.1%, p = 0.033) died from rebleeding events. According to the Kaplan–Meier analysis, the annual rebleeding incidence rate was 1.4%/year in the EDAS group and 3.6%/year in the conservative treatment group (p = 0.005, Log-Rank test). Multivariate Cox regression analysis revealed that EDAS surgery was a protective predictor for rebleeding events, while age and the dilation of posterior choroidal artery were positive factors influencing recurrent hemorrhage events. Long-term follow-up results show that, compared to conservative treatment, EDAS revascularization can effectively reduce the rate of recurrent cerebral hemorrhage in adult patients with hMMD.
Introduction
Moyamoya disease (MMD) is a rare, chronic, and progressive cerebrovascular disorder characterized by stenosis and occlusion of the distal carotid, proximal middle, and anterior cerebral arteries and accompanied by the development of a fine collateral vascular network (moyamoya vessels) at the base of the brain.1,2
According to its different initial clinical symptoms, MMD can be roughly divided into two types: ischemic and hemorrhagic. For ischemic MMD patients, cerebrovascular reconstruction can form new collateral circulation, improve cerebral blood flow reserve, and reduce the occurrence of secondary stroke, which has become the consensus of many neurosurgeons. 3 However, no treatment policy for the prevention of rebleeding has been established. Revascularization can be considered for patients with hemorrhagic MMD (hMMD), but adequate scientific evidence is still lacking. 3 The Japanese Adult Moyamoya trial, a multicenter prospective study conducted at 22 high-volume centers across Japan, revealed that direct bypass surgery for adult patients with hMMD reduces the rebleeding rate and improves a patient’s prognosis during the 5 years after study enrollment. 4 However, the study investigators also pointed out that the result was statistically marginal and the number of patients enrolled was more seriously insufficient than expected in this study. Moreover, this trial did not explore the role of indirect revascularization in reducing rebleeding rates.
Our center is the largest specialized center for MMD in Chinese PLA General Hospital. We have treated >6000 MMD patients and performed >10,000 indirect revascularization surgeries since 2002. Some previous retrospective studies have shown that encephaloduroarteriosynangiosis (EDAS), a commonly used indirect revascularization procedure, can effectively prevent rebleeding in MMD patients.5,6 We therefore carried out a prospective observational study that assessed patients with hMMD since 2008 to explore whether EDAS can reduce the risk of recurrent cerebral hemorrhage. Patient enrollment was completed in April 2018, and final follow-up assessments were completed in June 2023.
Methods
Study design
This study was designed to investigate the effectiveness of an indirect revascularization—EDAS in preventing recurrent cerebral hemorrhage in patients with hMMD compared to the conservative group including both prospective and retrospective cases. This research was designed as an ambidirectional cohort study. The retrospective collection of baseline clinical data for patients treated between 2008 and 2018, along with the subsequent prospective follow-up phase, were approved by the Research Ethics Board of the Chinese PLA General Hospital (ky-2018-3-13). To rigorously monitor long-term outcomes, the prospective tracking phase of this established cohort was formally registered at ClinicalTrials.gov (NCT03627975) in July 2018. Informed consent for study participation was obtained from all patients or their immediate family members through written materials, letters, or telephone contact. The study was conducted in accordance with the principles set forth in the Declaration of Helsinki (2013) for studies involving human participants and according to the STROCSS guidelines. 7
Patient selection
We enrolled patients diagnosed with hMMD between July 2008 and April 2018 at the Department of Neurosurgery at the Chinese PLA General Hospital. Our inclusion was as follows: (a) all enrolled hMMD patients were diagnosed according to the criteria of the Research Committee on MMD of Japan 3 ; (b) patients aged ⩾18 years; (c) patients had experienced at least one digital subtraction angiography (DSA) examination; and (d) lesions showed bilateral changes. The exclusion was: (a) patients with moyamoya syndrome secondary to systemic diseases such as arteriosclerosis, sickle cell anemia, radiation therapy, etc.; (b) patients with severe mental disorders, liver and kidney insufficiency, severe depression, drug abuse, low IQ; (c) loss to clinical follow-up; and (d) failure to provide informed consent.
Treatment strategy
We explained to all of the recruited patients that there is no clear evidence on whether revascularization can reduce the rebleeding rate and informed them about the risks that may arise from the surgery. Each patient voluntarily chose whether to accept surgical treatment and signed an informed consent form after fully understanding our research program. EDAS was used in all surgical procedures. The specific perioperative management and EDAS methods used were described in Supplementary Methods.
Conservative treatment aims to manage symptoms and alleviate or eliminate episodes experienced by the patient mainly includes control of stroke risk factors (hypertension, diabetes mellitus, hyperlipidemia), prevention of secondary epilepsy, control of intracranial hypertension (including the application of mannitol and glycerol fructose), and neurotrophic therapy.
Thus, all enrolled hMMD patients were divided into an EDAS surgery group and a conservative treatment group, and their basic clinical data were collected. The follow-up protocol for the study was as follows. All surgically and conservatively managed patients were enrolled in a standardized longitudinal follow-up program documented in the hospital’s electronic medical record system. Assessments were conducted via in-person visits for hospitalized patients or annual remote video/telephone interactions for the others. Evaluations consisted of a neurological examination by a trained study physician, with administration of the mRS score to grade disability, as well as documentation of any recurrent stroke events (ischemic or hemorrhagic stroke).
Clinical data and angiographic features of the patients
The clinical data covered in this study included gender, onset age, hypertension, hyperlipidemia, diabetes mellitus, tobacco and alcohol use, type of cerebral hemorrhage, neurological status, and posterior circulation involvement (PCI). The types of cerebral hemorrhage included intracranial hemorrhage (ICH), intraventricular hemorrhage (IVH), subarachnoid hemorrhage (SAH), and IVH with ICH. Neurological status was evaluated with the modified Rankin scale (mRS) on admission and during follow-up periods.
Each hemisphere was assessed for the association of the angiographic changes of the anterior choroidal and posterior communicating arteries (AChA–PCoAs) with hemorrhagic ictus. Moyamoya vessels were graded using the Suzuki angiographic stages: none, mild, and flourishing. 2 AChA–PCoAs findings were graded according to previously published methods: (0) normal without dilation or extension; (1) slight-moderate dilation and extension; (2) extremely dilated and presented abnormal branches; and (3) disappeared due to ICA occlusion.8,9 The PChA was defined as 0, no extension and dilatation or 1, extension and dilatation to the level of the lateral ventricle. All angiography images were reviewed by two experienced readers (Q-N-W and X-YB) independently and both of them were blinded to recurrent hemorrhage. Any differences in their observations were resolved by consensus.
Clinical and angiographic follow-up
Clinical follow-ups were performed through clinical visits, telephone calls, or letter interviews annually. The secondly DSA was performed 6–12 months postoperatively to assess EDAS efficacy and guide subsequent management. The development of neovascularization through bypass was graded according to the system described by Matsushima: 3, the collateral network of neovascularization accounted for two-thirds or more of the middle cerebral artery (MCA) distribution; 2, between one and two-thirds of the MCA distribution; and 1, less than one-third of the MCA distribution or none. 10
Follow-up events included recurrent cerebral hemorrhage, cerebral infarction, and death, and cerebral hemorrhage and cerebral infarction were confirmed by CT or MRI.
Statistical analysis
All clinical characteristic data are presented as mean ± SD for continuous variables and frequencies for categorical variables. Baseline variables were analyzed using the chi-square test or Fischer’s exact test, and continuous variables were compared using the paired t-test or Wilcoxon signed-rank test.
Time-to-event hazard ratio (HR) estimates (relative risk) for outcomes were calculated using Cox proportional hazard regression analysis to control for the effects of potential confounders while considering the varying lengths of follow-up. Time 0 refers to the point at which patients with hMMD undergo EDAS or conservative treatment at admission. The follow-up period was defined as the interval from the time 0 to the endpoint of recurrent hemorrhagic stroke events or the date of the last known clinical follow-up without hemorrhagic stroke events. The incidence of primary outcomes may be attributed to the clinical baseline characteristics (sex, age, mRS score, type of hemorrhage) and risk factors of stroke (hypertension, hyperlipidemia, diabetes mellitus, cigarette use, alcohol use). Therefore, model I was adjusted for clinical baseline characteristics as the minimally adjusted model. Given the degree of arterial lesion has been found associated with recurrent stroke events, model II was adjusted for the degree of moyamoya vessels, PCI, AChA–PCoAs grade, Suzuki stage as the fully adjusted model. The Durbin–Watson test assessed autocorrelation, and collinearity diagnostics were performed by evaluating the variance inflation factor (VIF) values. To mitigate potential selection bias arising from the observational nature of treatment allocation, a propensity score matching (PSM) analysis was conducted. A 1:1 nearest-neighbor matching algorithm was employed, and propensity scores were estimated using a multivariable logistic regression model. This model incorporated comprehensive baseline covariates, including age, sex, hemorrhage type, posterior circulation involvement, AChA–PCoAs dilation, PChA dilation, hypertension, hyperlipidemia, smoking, drinking, and Suzuki stage. Subsequent survival analyses were re-performed on this matched, pseudo-randomized cohort to verify the robustness of the treatment effect. To further address potential attrition bias, baseline characteristics were compared between the final included cohort and patients who were excluded or lost to follow-up. Moreover, to evaluate the stability of the treatment effect against this attrition rate, a worst-case scenario sensitivity analysis was performed. In this model, we adjusted for comprehensive baseline covariates while assuming the most unfavorable clinical outcomes for the surgical group among the lost-to-follow-up population. Finally, a post-hoc power analysis was conducted based on the final sample sizes and observed event rates. This was performed to objectively evaluate the statistical power of our cohort for detecting differences in the primary endpoint (rebleeding-free survival) between the two treatment modalities. All statistical analyses were performed using SPSS (version 27.0; IBM, Armonk, NY, USA). Differences were considered statistically significant when two-tailed p < 0.05.
Results
Patient characteristics
A total of 346 patients with hMMD were enrolled in this study between July 2008 and April 2018 at our center. Moreover, 160 patients were excluded based on the exclusion criteria: 96 patients were lost to follow up, 48 were without complete clinical or radiological data, nine were suspected to have trauma/tumor-causing bleeding, and seven were without any form of informed consent. Finally, 186 patients (43 prospectively and 143 retrospectively) were included in the analysis and the flow diagram of the study is shown in Figure 1. Among all patients with hMMD, 103 were women and 83 were men and the average age at symptom onset was 39.6 ± 8.9 (range, 18–65) years. Twenty-six patients (14.0%) had hypertension, four (2.2%) had diabetes, 18 (9.7%) had hyperlipidemia, and 31 (16.7%) had a history of previous tobacco or alcohol use. Sixty (32.3%) presented with PCI. CT imaging revealed the presence of pure ICH in 82 patients (44.1%), pure IVH in 74 patients (39.8%), SAH in 18 patients (9.7%), and ICH with IVH in 12 patients (6.5%). Furthermore, 123 (66.1%) underwent EDAS, and 63 (33.9%) received conservative treatment. The clinical characteristics are summarized in Table 1. The firstly DSA examination at admission was required for all patients. Angiographic characteristics were investigated in the hemorrhagic hemisphere and there were no significant differences in general and angiographic conditions at admission between the conservative and EDAS groups (Table 2).
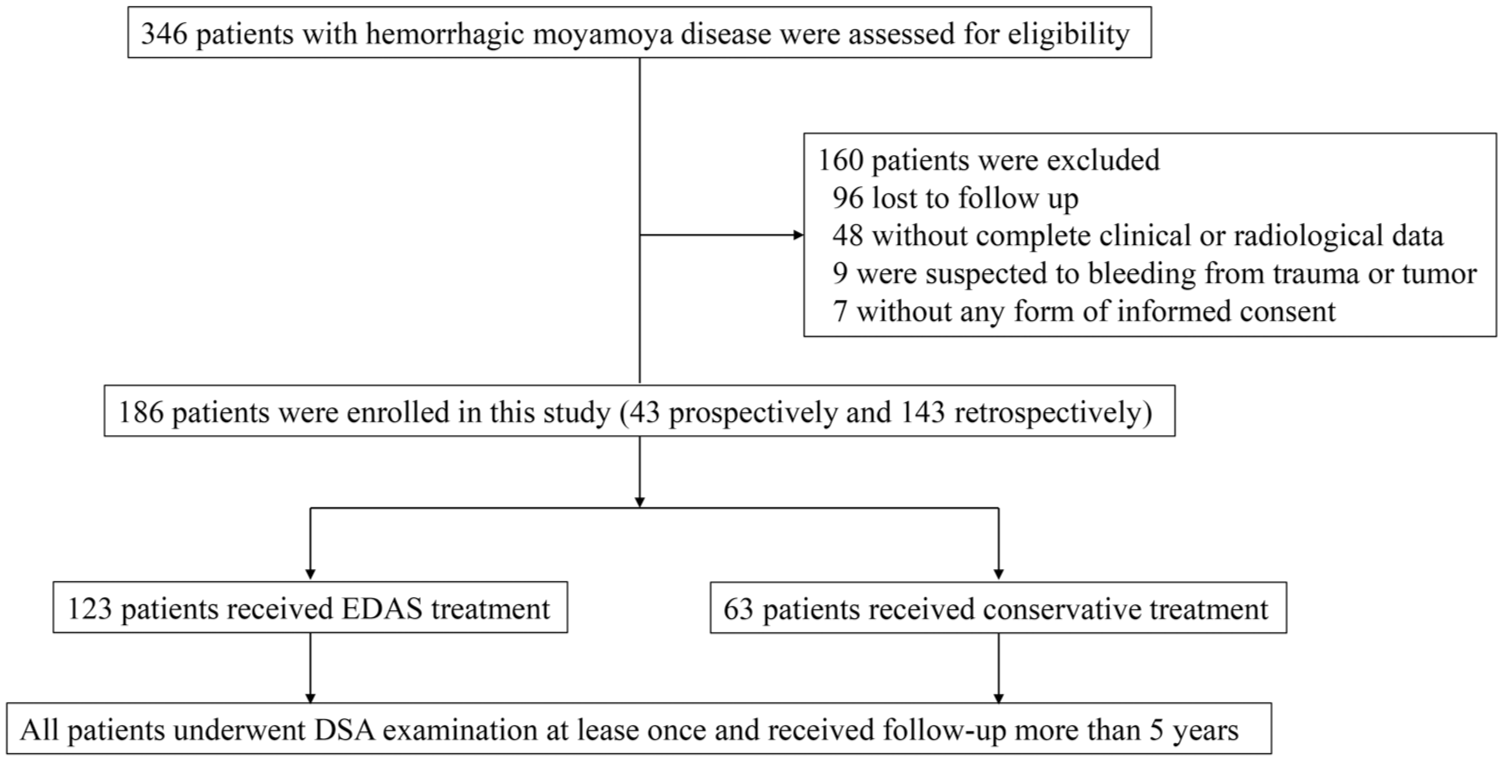
Flow diagram of the study.
Baseline characteristics of patients.
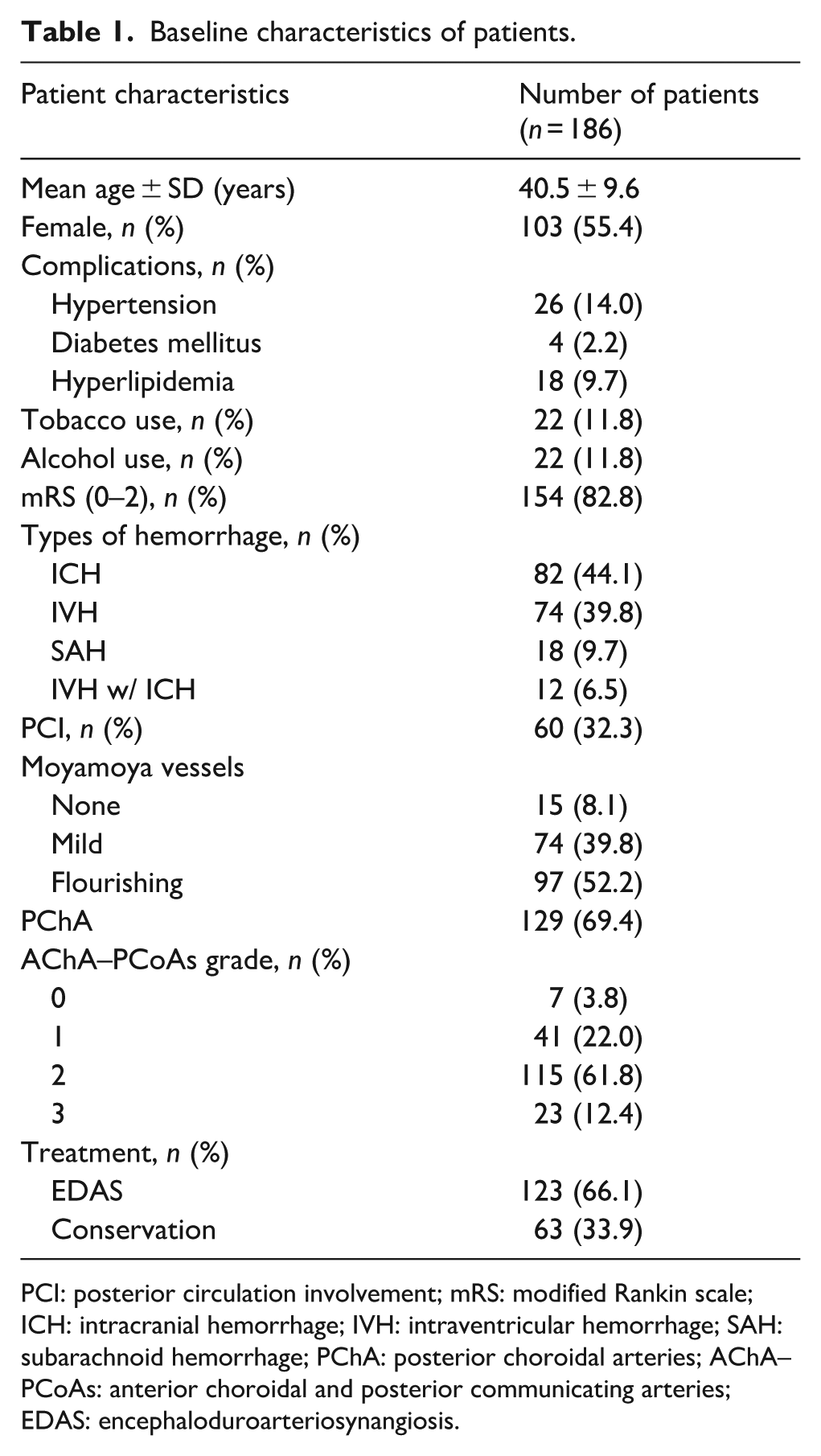
PCI: posterior circulation involvement; mRS: modified Rankin scale; ICH: intracranial hemorrhage; IVH: intraventricular hemorrhage; SAH: subarachnoid hemorrhage; PChA: posterior choroidal arteries; AChA–PCoAs: anterior choroidal and posterior communicating arteries; EDAS: encephaloduroarteriosynangiosis.
Comparison of baseline characteristics between the EDAS and conservative groups.
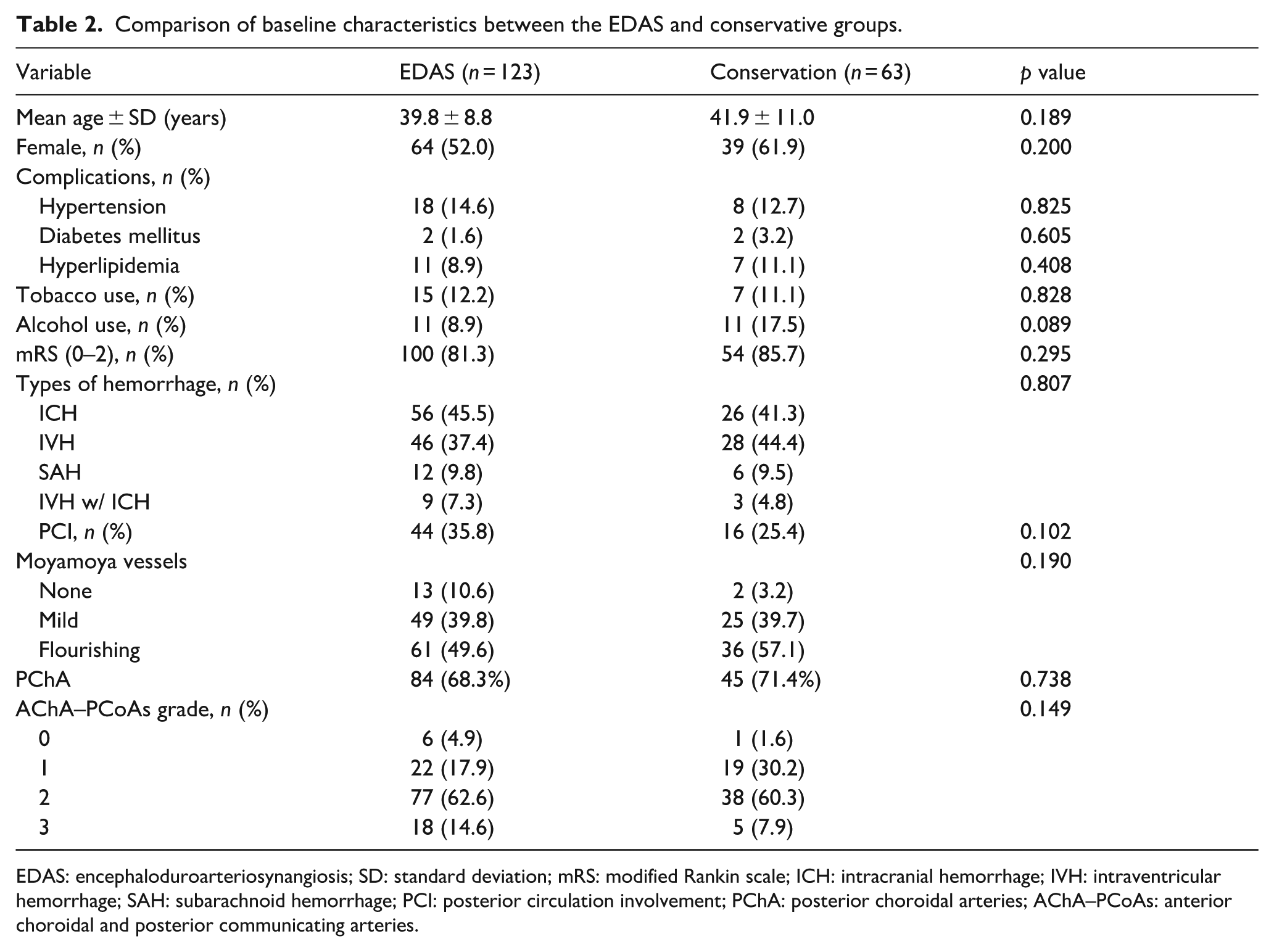
EDAS: encephaloduroarteriosynangiosis; SD: standard deviation; mRS: modified Rankin scale; ICH: intracranial hemorrhage; IVH: intraventricular hemorrhage; SAH: subarachnoid hemorrhage; PCI: posterior circulation involvement; PChA: posterior choroidal arteries; AChA–PCoAs: anterior choroidal and posterior communicating arteries.
Sensitivity analysis for attrition
A comparison of baseline characteristics revealed no statistically significant differences between the included patients and those lost to follow-up (all p > 0.05; Supplementary Table 1), indicating that the attrition was likely missing at random. Moreover, the worst-case scenario sensitivity analysis confirmed that the therapeutic benefit of EDAS remained highly significant even after adjusting for baseline covariates and assuming extreme attrition outcomes (adjusted OR = 0.27, 95% CI: 0.10–0.69, p < 0.01; Supplementary Table 2). This demonstrates that the observed protective effect is robust and not a byproduct of attrition bias.
Follow-up arteriographic findings
Although we recommended follow-up DSA at 6–12 months post-discharge for all patients, many declined the invasive procedure due to economic considerations or a lack of new clinical symptoms. Consequently, only 45 patients in the EDAS group and four in the conservative group underwent follow-up DSA. Due to this severe imbalance in imaging sample size, direct statistical comparisons of radiological outcomes between the two groups were not feasible. Therefore, our evaluation of angiographic changes in hemorrhage-risk vessels (moyamoya vessels, AChA–PCoAs, and PChA) was strictly confined to the EDAS cohort.
In the EDAS group, Matsushima grading for surgical neovascularization revealed that four (8.9%) of the 45 investigated hemispheres were classified as Grade A, 13 (28.9%) as Grade B, and 28 (62.2%) as Grade C. Compared to preoperative DSA, the regression of moyamoya vessels was observed in 13 (28.9%) cases, 29 (64.4%) remained unchanged, and three (6.7%) showed progression. Regarding the extension and dilation of AChA–PCoAs, 10 (22.2%) patients showed improvement, eight (17.8%) experienced complete regression, and 27 (60.0%) remained unchanged. Notably, PChA dilation improved in 11 (24.4%) patients, remained unchanged in 32 (71.1%), and deteriorated in two (4.4%). The overall angiographic changes in these vessels at the end of the follow-up are summarized in Supplementary Figure S1.
Long-term clinical outcome
Thirty-four of 186 patients (18.3%) suffered cerebral rebleeding during a median follow-up period of 8.7 ± 2.6 years and the average rebleeding interval was 6.0 ± 2.4 years. The mean follow-up time was 8.0 ± 2.4 years for the EDAS group and 9.1 ± 2.6 years for the conservative group. The mean follow-up times for the EDAS and conservative groups were 8.9 ± 2.9 and 7.4 ± 2.8 years for rebleeding, and 9.0 ± 2.7 and 7.7 ± 2.6 years for mortality, respectively.
In the EDAS group, one (0.8%) patient suffered postoperative infarction, 16 (13.0%) patients experienced recurrent cerebral hemorrhage and three (2.4%) patients died from rebleeding events. In the conservative treatment group, no patients suffered postoperative infarction, whereas 18 (28.6%, p = 0.015) experienced cerebral rebleeding events and seven (11.1%, p = 0.033) died from rebleeding events (Table 3). According to the Kaplan–Meier analysis (Figure 2), the annual rebleeding incidence rate was 1.4%/year in the EDAS group and 3.6%/year in the conservative treatment group, and this difference was statistically significant (p = 0.005, log-rank test). During the long-term follow-up, a total of 10 deaths were recorded, comprising three cases in the EDAS group and seven cases in the conservative group. Following a meticulous review of medical records, death certificates, and family interview logs, all 10 mortalities were confirmed to be directly caused by fatal recurrent hemorrhage.
Comparison of follow-up and outcomes between the EDAS and conservation groups.
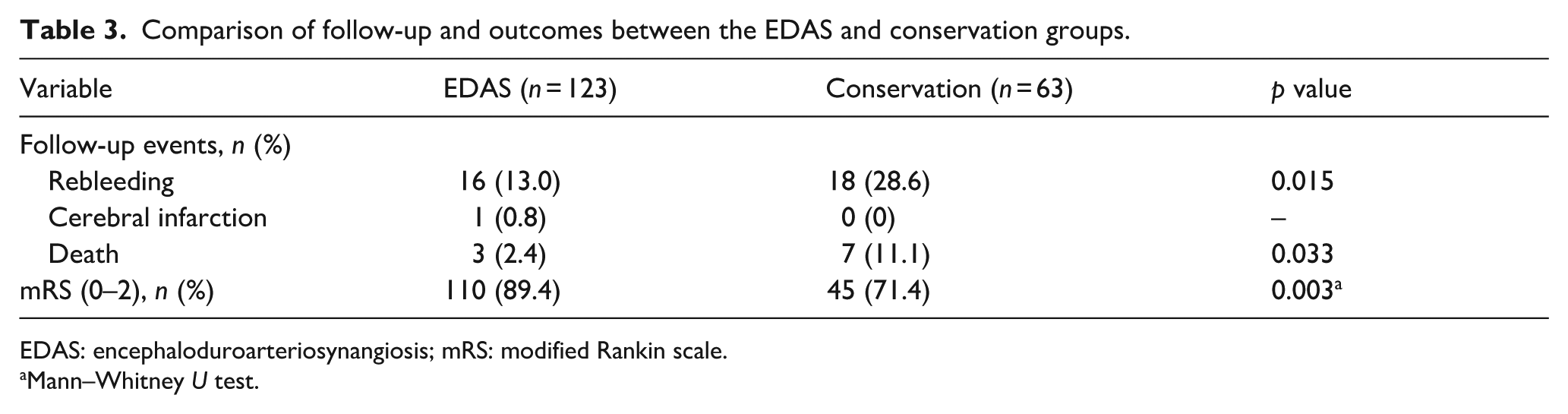
EDAS: encephaloduroarteriosynangiosis; mRS: modified Rankin scale.
Mann–Whitney U test.
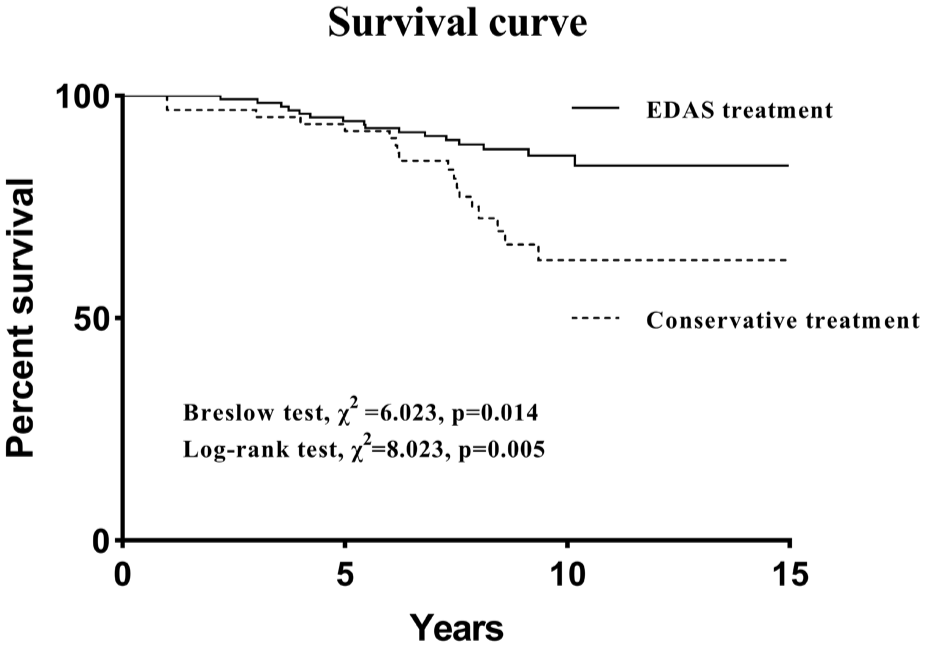
Kaplan–Meier estimates of rebleeding incidence rates.
The neurological status defined by mRS scores in the EDAS group was improved in 65 (52.8%) patients, unchanged in 49 (39.8%), and deteriorated in nine (7.3%, p < 0.001); in contrast, 17 patients (27.0%) improved, 32 (50.8%) remained unchanged, and 14 (22.2%) deteriorated in the conservative treatment group (p < 0.001). The changes of the mRS scores are shown in Supplementary Figure S2.
Multivariate Cox regression analysis of preoperative clinical variables revealed that EDAS surgery is a protective predictor of rebleeding, while age (HR, 1.043; 95% CI, 1.001−1.087; p = 0.042) and the dilation of PChA (HR, 4.589; 95% CI, 1.382−15.240; p = 0.013) were positive influencers of recurrent hemorrhage events (Table 4). The values of the Durbin–Watson (1.910) and VIF (range: 1.038–1.549) indicated good data independence within the model and no collinearity issues between variables.
Multivariable Cox regression analysis of predictive factors for recurrent hemorrhage events.
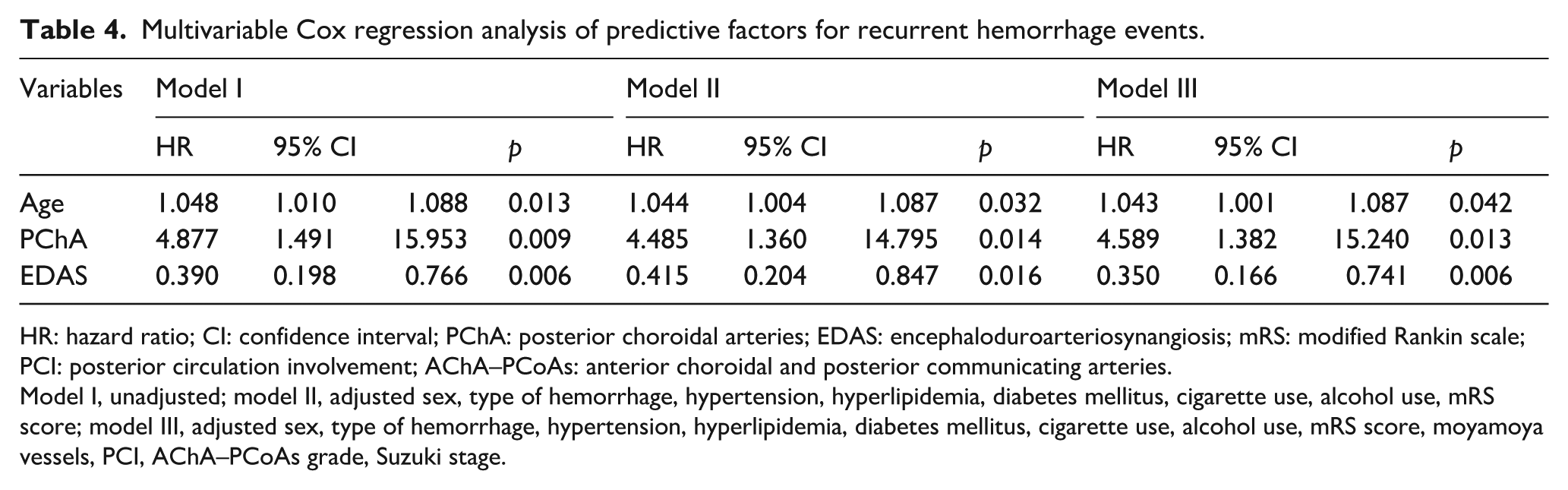
HR: hazard ratio; CI: confidence interval; PChA: posterior choroidal arteries; EDAS: encephaloduroarteriosynangiosis; mRS: modified Rankin scale; PCI: posterior circulation involvement; AChA–PCoAs: anterior choroidal and posterior communicating arteries.
Model I, unadjusted; model II, adjusted sex, type of hemorrhage, hypertension, hyperlipidemia, diabetes mellitus, cigarette use, alcohol use, mRS score; model III, adjusted sex, type of hemorrhage, hypertension, hyperlipidemia, diabetes mellitus, cigarette use, alcohol use, mRS score, moyamoya vessels, PCI, AChA–PCoAs grade, Suzuki stage.
Propensity score matching analysis
Following the 1:1 PSM, the baseline characteristics between the EDAS and conservative groups were successfully balanced, with no significant differences observed across all matched covariates (all p > 0.05; Supplementary Table 3). Crucially, survival analysis on this matched cohort directly corroborated our primary findings. The updated Kaplan-Meier curves demonstrated a consistently superior hemorrhage-free survival rate in the EDAS group (Supplementary Figure 3). Furthermore, the matched Cox proportional hazards regression model confirmed that EDAS remained a highly significant protective factor, reducing the risk of rebleeding by 72.4% compared to conservative treatment (HR = 0.276, 95% CI: 0.101–0.752, p = 0.012). This indicates that the clinical benefit of surgical revascularization is robust and independent of baseline confounding disparities.
Discussion
A key consideration in the treatment of hMMD is how to prevent recurrent cerebral hemorrhage. However, the choice of treatment for the disease remains controversial. There is insufficient evidence to suggest revascularization, either directly or indirectly, is effective in reducing the rate of recurrent cerebral hemorrhage. Only Japan has carried out a multicenter prospective randomized controlled trial of hMMD patients since 2001, and the sample size of enrolled cases was seriously reduced compared to what is expected with the experimental design, and only the direct revascularization method is selected as the surgical method. 4
EDAS has been a widely established treatment strategy for patients with MMD, especially ischemic-type MMD, because of its excellent postoperative results, which facilitate extensive collateral formation and minimal complications.11–15 However, whether EDAS can effectively reduce the rebleeding rate in patients with hMMD has not yet been reported by any center with a large sample size. We designed this prospective observational study with an average follow-up of up to 8.7 ± 2.6 years to provide a clinical basis for whether EDAS can prevent recurrent intracerebral hemorrhage.
The final results of this study showed that 16 (13.0%) patients experienced recurrent cerebral hemorrhage in the EDAS group and 18 (28.6%) patients experienced recurrent cerebral hemorrhage in the conservative treatment group. The annual rebleeding incidence rate was 1.4%/year in the EDAS group and 3.6%/year in the conservative treatment group, and this difference was statistically significant. The results of this study confirmed the important role of EDAS surgery in preventing recurrent cerebral hemorrhage, which undoubtedly offers great encouragement for the surgical treatment of hMMD.
We reviewed previous reports on the efficacy of direct revascularization in preventing rebleeding and found that the therapeutic effect reported earlier was similar to the rebleeding rate of patients in the EDAS group in our study. A multicenter, prospective, randomized controlled study on the efficacy of adult hMMD in Japan determined that the rebleeding rate was 14.3% in the direct revascularization group and 34.2% in the conservative group. 4 Amin-Hanjani et al. previously reported that direct revascularization could reduce the risk of rebleeding in hMMD from 30%–65% to 12.5%–20%. 16 Xu et al. followed 38 patients with hMMD in North America for about 60.8 ± 65.7 months. 17 The rebleeding rate was 14.3% in the operation group and 47.1% in the conservative treatment group. In our study, the rebleeding rate was 13.0% in the EADS group and 28.6% in the conservative treatment group, which also confirmed that EDAS can play a sufficient role in preventing rebleeding compared to direct revascularization. Of course, there is still no standard with respect to the ideal revascularization surgery for hMMD. Kawaguchi et al. reported that, compared to EDAS, direct bypass led to greater efficacy in the prevention of rebleeding in patients with hMMD. 18 Some scholars have recently compared the effects of combined revascularization and EDAS alone in adult hMMD. 19 It has been suggested that both combined revascularization and EDAS alone can reduce the risk of rebleeding in hMMD, and combined revascularization was found to be superior to EDAS alone in terms of preventing rebleeding events. However, recent multicenter studies found no difference in the incidence of recurrent hemorrhagic strokes between direct and indirect revascularization techniques.20,21 Therefore, the optimal treatment for hMMD remains controversial. It is worth noting that, in this study, compared to the seven patients (11.1%) in the conservative treatment group who died of rebleeding, only three (2.4%) in the EDAS group died of rebleeding; thus, even if patients undergoing EDAS surgery experience cerebral hemorrhage again, their severity of brain damage can be reduced to some extent compared to the damage in those receiving conservative treatment. A major methodological strength of this study in addressing these clinical controversies is the integration of extended longitudinal tracking and propensity score matching. While trials like the JAM study established the efficacy of direct bypass, skepticism has remained regarding indirect bypass in adults due to presumed inferior neoangiogenesis. Consequently, some previous short-term studies reported limited benefits of indirect bypass in preventing rebleeding. We hypothesize that the protective effect of EDAS requires a longer temporal window for collateral maturation and hemodynamic remodeling. By rigorously balancing comprehensive baseline confounders through PSM to minimize selection bias, our long-term data effectively counteracts previous skepticism. It demonstrates that once the temporal threshold is crossed, EDAS offers a durable and highly significant reduction in rebleeding risk (HR = 0.276 in our matched cohort), proving its robust efficacy independent of baseline disparities.
The specific mechanism of EDAS to prevent recurrent cerebral hemorrhage is still unclear. There are three reasons for cerebral hemorrhage in patients with MMD, including rupture of the choroidal arteries, moyamoya vessels, and arterial aneurysms.8,22 According to Morioka et al., rupture of dilated anterior choroidal arteries and perforating arteries of the thalamus, rather than the paraplastic small moyamoya vessels, is the main cause of hemorrhages in patients with MMD. 9 A supplementary analysis of the Japan Adult Moyamoya Trial conducted by Funaki et al. reported that the choroidal anastomosis was the leading cause in resulting the posterior rebleeding in hMMD. 23 In hMMD, collaterals are prone to arise more frequently from the choroidal arteries. 24 The hemodynamic overload of choroidal arteries enlarges these vessels and makes them more fragile, and the resulting development of “weak spots,” which arise more often at intraventricular rather than cisternal segments, explains anatomically why these patients present primarily with IVH. 25 A rupture of the anterior choroidal artery leads to lateral ventricular hemorrhage, while a rupture of the branch of the posterior communicating artery easily causes thalamic hemorrhage. 26 In this study, patients who underwent EDAS had less AChA–PCoAs dilatation postoperatively than before revascularization. Figure 3 depicts a representative case in the EDAS group, demonstrating a decreased possibility of rebleeding in the superior lateral compensatory hemisphere. We speculate that the new collateral circulation established by EDAS surgery can relieve the blood pressure of the AChA–PCoAs and PChA, which theoretically would allow gradual reduction of the hemodynamic stress on deep collaterals and regression of its associated weak points within 6–12 months after surgery, thereby reducing the recurrence rate of the patient.27,28 However, a notable finding in our angiographic follow-up was that despite the significant clinical reduction in rebleeding, macroscopic regression of these risk vessels was not universally observed. For instance, PChA dilation remained unchanged in 71.1% of the evaluated EDAS cohort. This apparent paradox further supports that the protective mechanism of EDAS relies more heavily on regional hemodynamic remodeling rather than mere anatomical shrinkage. Even modest surgical neovascularization can function as a collateral pressure release valve. By redirecting a fraction of the cerebral perfusion demand to the external carotid system, EDAS alleviates the peak wall shear stress and turbulent flow concentrated on the fragile, dilated PChA. Thus, the risk of subsequent rupture is mitigated despite persistent luminal dilation on macroscopic DSA. Importantly, conventional DSA is limited to luminal visualization and cannot assess microstructural changes within the vessel wall itself. Therefore, future prospective studies utilizing advanced neuroimaging modalities, particularly high-resolution magnetic resonance imaging (HRMRI) for vessel wall imaging, are warranted. HRMRI could provide crucial in vivo evidence to validate this hypothesis by directly visualizing microstructural changes in the PChA wall, such as the attenuation of wall enhancement, stabilization of micro-aneurysms, or positive remodeling, following EDAS, perfectly bridging the gap between macroscopic angiography and micro-hemodynamic relief.
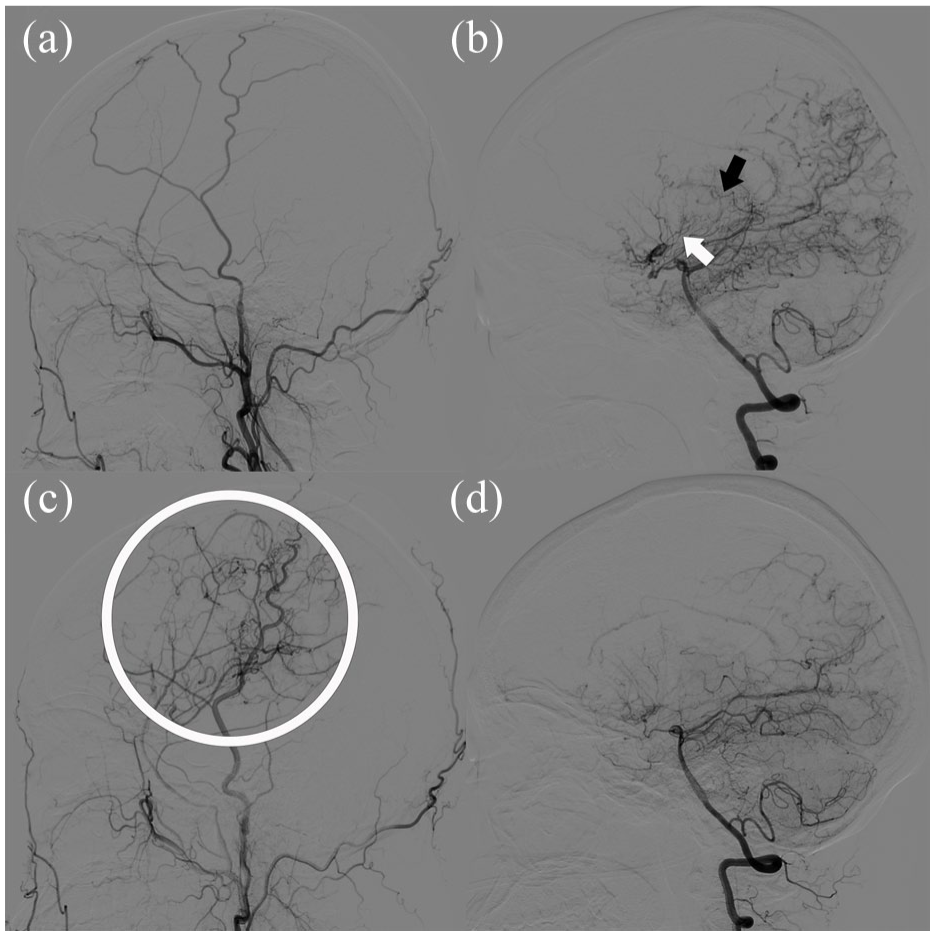
Lateral cerebral angiography at admission (a, b) and follow up (c, d): (a) angiography of the right external carotid artery, (b) angiography of the posterior cerebral artery showed dilated PChA (black arrow) and AChA–PCoAs (white arrow), (c) follow up angiography showed excellent surgical neovascularization (Matsushima grade A) from the right external carotid artery (white circle), and (d) follow up angiography of the posterior cerebral artery showed amelioration of AChA–PCoAs and PChA extension and dilation after encephaloduroarteriosynangiosis revascularization.
Cox survival analysis showed that, in addition to EDAS surgery being a protective factor to prevent recurrent cerebral hemorrhage, recurrent cerebral hemorrhage is closely related to dilated PChA. As mentioned earlier, the rupture of moyamoya vessels is currently considered one of the causes of bleeding. With the development of MMD, the large vessels at the ends of the bilateral internal carotid arteries gradually narrow, and chronic ischemia and hypoxia in brain tissue promote the formation of abnormal neovascularization, thus forming a dilated PChA network to compensate for blood supply to anterior ischemic brain territory. The new PChA collateral circulations lack normal vascular structure; are extremely distorted and dilated; and may even be associated with microaneurysms, which easily rupture and bleed. Therefore, patients with MMD who spontaneously form better posterior collateral circulation tend to have milder ischemic symptoms but are more prone to rupture and bleeding due to the unstable lumen structure of the newly formed collateral vessels. Another risk factor for rebleeding was older age, which is consistent with prior evidence. Morioka et al. 29 reported that the rate of rebleeding increases significantly when patients reach 46–55 years of age. Wang et al. 6 also demonstrated that the age at symptom onset is a positive predictor of rebleeding in patients with MMD and that the risk increases with age. The universal potential mechanism for this phenomenon may be the high prevalence of amyloid angiopathy and hypertension and the use of antithrombotic drugs in this age group.
The greatest difficulty in the implementation of this study was patient loss to follow-up. We followed our patients for an average of 8.7 ± 2.6 years, which is rare in the real world. However, at present, the effectiveness of the treatment of hMMD can only be evaluated by long-term follow-up. Many patients are at high risk of recurrent cerebral hemorrhage but lose the opportunity for timely clinical intervention due to a lack of safe and effective assessments, resulting in serious adverse events such as stroke and even death. We hope to find some more sensitive and specific parameters to evaluate and predict the risk of recurrent cerebral hemorrhage. The research experience of aneurysms suggests that cerebral vascular rupture and hemorrhage should be closely related to hemodynamic indexes, including wall shear stress and pressure drop, as well as the changes of vascular wall structure, so the hemodynamic parameters and the employment of 7 T MRI in patients with hMMD will be the focus of our team’s next research work.
Limitations
This study was originally designed as a prospective randomized controlled study. However, due to several reasons, such as medical ethics and patient compliance, the trial was difficult to implement as designed. Finally, the trial was changed into a prospective observational study with the approval of the ethics committee. Consequently, the level of evidence for the findings of the study has been downgraded. In addition, compared to the size of the EDAS group, the conservative treatment group in this study was smaller, which inevitably led to statistical bias. Another limitation of this study is the sample size and unavoidable attrition associated with a 9-year long-term follow-up. HMMD is a rare cerebrovascular condition, which inherently restricts cohort expansion. Our post-hoc power analysis revealed that the current cohort achieved a statistical power of 70.8% (α = 0.05) for the primary endpoint of hemorrhage-free survival. While slightly below the conventional 80% threshold, this study still provides moderate-to-high statistical power, successfully detecting the substantial clinical benefit provided by surgical revascularization without yielding a type II error. Furthermore, the extreme discrepancy in follow-up DSA rates between the surgical and conservative arms is a notable limitation. Because an invasive and costly angiographic evaluation was neither clinically indicated nor ethically justifiable for stable conservative patients without new neurological symptoms, our study lacks adequate radiological data to evaluate the natural angiographic progression of the conservative cohort.
Conclusion
In this study, long-term follow-up results demonstrated that indirect EDAS revascularization effectively reduced the rate of recurrent cerebral hemorrhage in adult patients with hMMD compared to conservative treatment. This may serve as a useful reference for clinical practice.
Supplemental Material
sj-docx-1-jcb-10.1177_0271678X261455499 – Supplemental material for Encephaloduroarteriosynangiosis effectively reduces rebleeding risk in adults with hemorrhagic moyamoya disease: A long-term ambidirectional cohort study
Supplemental material, sj-docx-1-jcb-10.1177_0271678X261455499 for Encephaloduroarteriosynangiosis effectively reduces rebleeding risk in adults with hemorrhagic moyamoya disease: A long-term ambidirectional cohort study by Qian-Nan Wang, Xiao-Peng Wang, Xiao-Mei Li, Jing-Jie Li, Zheng-Xing Zou, Xiang-Yang Bao, Zhi-Chao Li and Lian Duan in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Acknowledgements
The authors sincerely thank the Department of Statistics, Medical School of Chinese PLA, and the Outpatient Clinic of Statistics, Chinese PLA General Hospital for their invaluable statistical guidance on this study.
Author contributions
Qian-Nan Wang: concept and design, methodology, data curation, writing—original draft, writing—review and editing. Xiao-Peng Wang: concept and design, formal analysis, writing—original draft, writing—review and editing. Zhi-Chao Li: investigation, writing—original draft. Xiang-Yang Bao: concept and design, writing—review and editing. Xiao-Mei Li: data curation, investigation. Jing-Jie Li:fFormal analysis, visualization, and review the manuscript. Zheng-Xing Zou: data curation. Lian Duan: concept and design, investigation, supervision, writing—original draft, writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Natural Science Foundation of China (grant nos. 82571458, 82171280 and 82201451) and the Beijing Municipal Science & Technology Commission (no. Z171100001017144).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registration
This study has been registered in the ClinicalTrials.gov (NCT03627975).
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.