
Abstract
Cardiovascular–kidney–metabolic (CKM) syndrome has increasingly affected the middle-aged and elderly population. The relationship between CKM risk factors and stroke at metabolomic level and underlying genetic alterations remains unknown. Elastic net regression was utilized to establish a metabolic signature indicative of CKM risk factors in 108,305 participants in UK Biobank. Multivariable COX proportional hazard models were utilized to determine the association between CKM plasma metabolic signature and incident stroke. Causal relationships between metabolites and stroke were explored through Mendelian randomization (MR) analysis and colocalization analysis. During a follow up of 13.94 years (interquartile range (IQR), 13.00–14.43), 3881 incident stroke events were documented. Forty-eight metabolites were identified to represent the metabolic process of CKM risk factors. After adjustment of demographic factors and CKM risk factors, the elevated metabolic signature was correlated with higher stroke incidence risks with hazard ratio of 1.075 (95% confidential intervals (CI), 1.001–1.154). MR analysis identified 38 potential causal metabolites. In addition, colocalization analysis revealed LDLR and CELSR2 as two genetic targets. In general, this study identified a metabolic signature reflecting CKM risk factors is positively associated with stroke, while LDLR and CELSR2 might impact the metabolic process in CKM population at genetic level.
Introduction
At the end of 2023, the American Heart Association (AHA) formally integrate cardiovascular disease, metabolic disorders, and kidney dysfunction as cardiovascular-kidney-metabolic (CKM) syndrome. 1 This concept considered metabolic disorders or subhealth, kidney dysfunction, and conventional cardiovascular risks (e.g. hypertension and hypertriglyceridemia) as predictors for cardiovascular organic lesions including heart failure, coronary heart disease, stroke, myocardial infarction, and atrial fibrillation. 2 According to the latest epidemiological report, the global burden of key components in CKM, including high body mass index (BMI), diabetes, and chronic kidney disease (CKD) continuously burst in the last decades.3,4 As the series of diseases dominantly lead to irreversible damage in the cardiovascular system, secondary prevention is of great importance.
Stroke, as one of the most common end-stage diseases of CKM syndrome, is the fourth-leading cause of disability adjusted life years (DALYs) in 2021 and long-term disables in most survivors.5,6 In recent years, the absolute burden of stroke is continuously aggregating due to population growth, bringing challenges for worldwide healthcare.5,6 Owing to the exceedingly high requirement for oxygen supply for brain, a lack of prompt medical intervention following the onset of a stroke frequently results in significant neurological deficits or disabilities. Therefore, early prevention and in-time management of strokes are pivotal strategies in mitigating the overall disease burden. Till now, previous studies have proved the causality between early-stage CKM risk factors and onset of stroke.7–9 Beyond this, previous studies have demonstrated some circulating metabolites, such as lipoproteins10,11 and triglycerides,12,13 significantly involve in pathogenesis of stroke, making the control of blood metabolites as a feasible way to alleviate stoke occurrence.
However, the majority of current evidence focused on independent associations between individual risk factors (e.g. hypertension) and stroke, overlooking the influences of comorbidities in CKM syndrome. Till 2020, approximately 89.4% U.S. citizens met the criteria for CKM syndrome, with more than 50% for stage 2 or above. 14 The concept of CKM syndrome highlights the importance of comorbidities in stroke, which are increasingly prevalent in the general population, the underlying mechanisms between multiple risk factors and stroke, as well as synergistic effect of plasma metabolites. Beyond these, relatively small sample sizes of current studies also restricted universalities of the conclusions.
To bridge these gaps, we recognized existence of obesity, hypertension, chronic kidney disease, hyperlipidemia, and hyperglycemia as CKM risk factors. Based on associations between metabolites and CKM risk factors, we identified a metabolic signature in response to adherence to CKM risk factors and investigated the relationship between CKM-associated metabolic signature and onset of stroke via available nuclear magnetic resonance (NMR) data in UK Biobank. Furthermore, Mendelian randomization (MR) plus colocalization analysis were employed to explore the causal relationships and possible therapeutic targets for stroke in CKM syndrome.
Methods
Study population and metabolite profiles
The UK Biobank study is a longitudinal cohort study recruiting ~500,000 participants aged 40–69 years from 2006 to 2010 from various locations across England, Scotland, and Wales, which was conducted in full compliance with the Declaration of Helsinki. These participants underwent the first assessment in 22 tertiary centers and submitted the written informed consent. Detail information of this cohort has been published in a previous report. 15 Before participance, all participants provided a written informed consent, and the North West Multicenter Research Ethics Committee (REC reference: 16/NW/0274) approved conducting UK Biobank study. BMI, waist circumference, serum creatinine, urine albumin, blood pressure, blood lipids, medical histories including prior diagnosis of hypertension, CKD and obesity, and glycated hemoglobulin in UK Biobank were utilized for assessments of CKM risk factors. In our study, we included stroke-free participants and excluded those with coronary heart disease, heart failure, and atrial fibrillation (Figure 1). Additionally, participants without assessments of CKM risk factors were excluded as well, leaving 108,385 individuals for ultimate data analysis.
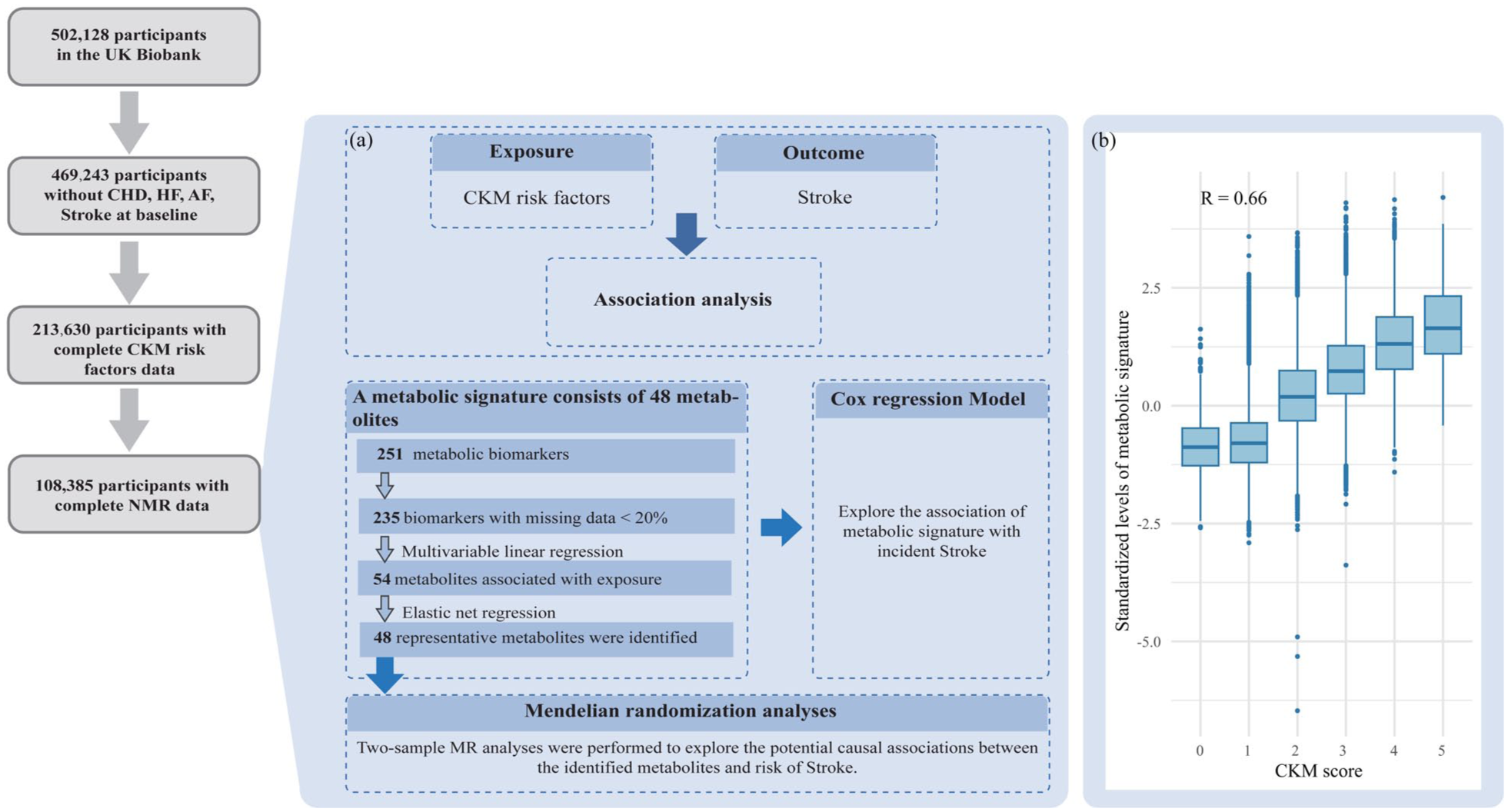
The metabolic signature for adherence to CKM risk factors: study design and participant inclusion flow chart: (a) the training procedure and study design for development of metabolic signature and (b) correlation between CKM risk factor score and metabolic signature using the baseline data.
We obtained NMR metabolic profiling data used for analysis from Nightingale Health. Currently, these data are available only in phase 1 and phase 2 across the study. A total of 251 metabolic biomarkers were measured from EDTA plasma samples of over 280,000 participants. One hundred seventy of them were measured at absolute level while the other 81 were measured by composite ratio indexes. The biomarkers include a wide range of metabolic activities including low-molecular agents (animo acids, ketone metabolism as well as carbohydrates), lipoprotein lipids, fatty acids composites. Biomarkers with missing data >20% were excluded from final analysis (Figure 1(a)), and 235 biomarkers were profiled for constructing the metabolic signature. This work is reported obeying guidance of STROBE checklist for cohort studies.
Assessment of CKM score
Based on stage 0–3 for CKM syndrome, we identified obesity, hyperglycemia, CKD, hypertension, and hyperlipidemia as five key risks following the previous studies.1,3,16–18 In this newly constructed score, a score of 1 point was allocated to the presence of each risk factor and the overall CKM score, ranging from 0 to 5 points, was based on the accumulative sum of CKM risk factors. The data required for evaluation of these factors was acquired from the baseline laboratory examination and questionnaires with comprehensive definitions. Specifically, CKM risk factors were determined as follows: (1) obesity was identified if either high BMI (⩾30 kg/m2) or high waist circumference (⩾88/102 cm in women/men), (2) hyperglycemia was determined once HbA1c ⩾6.5%, diagnosed diabetes or previous usage of glucose-lowing agents were reported, (3) CKD was assessed as estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 or albuminuria ⩾30 mg/g following the guideline of KDIGO 2024, 19 (4) hypertension was recognized for history of diagnosed hypertension, regular use of anti-hypertension drugs, average systolic blood pressure ⩾130 mmHg or diastolic blood pressure ⩾80 mmHg, and (5) hyperlipidemia was defined predominantly on triglycerides higher than 150 mg/dL.
Follow-up and ascertainment of stroke
In the UK Biobank, follow-up was performed for each participant after the initial recruitment. In our study, follow-up assessment stretched from the initial examination until the very first occurrence of the initial diagnosis of stroke, date of death or date of attrition, or the end of the study (October 31, 2022). The onset of all-cause stroke, ischemic stroke, intracranial hemorrhage, and subarachnoid hemorrhage were obtained by records from hospital inpatients department of Health Episode Statistics in England and Wales, along with the Scottish Morbidity Records in Scotland. National Health Service Digital for England and Wales and the Information Services Division for Scotland identified the additional cases. All the stroke events were documented by using International Classification of Disease (ICD) coding system with details of ICD-10 in Table S1.
Assessment of covariates
Medical histories and sociodemographic factors were further considered as underlying confounders in COX regression models. Sociodemographic factors were mostly evaluated through questionnaires. These factors included baseline age, sex (male or female), race (White, Black, Asian, or Mixed), alcohol status (never, previous, or current), smoking status (never, previous, or current), and Townson deprivation index. The Townson deprivation index estimates the substantial well-being of participants and general household economic levels via factors like income, employment, and accessibilities to services with scores from 0 to 1. Higher scores indicate severe deprivation. Physical intensities were evaluated by Metabolic Equivalent Task (MET) scores from the International Activities Questionnaire (IPAQ). This questionnaire classified physical activities into low, moderate, and high levels 20 and MET scores were calculated by summed MET minutes per week for all activity. Sleep duration was obtained by touch-screen questionnaire that assessed their sleep health in seven important dimensions.
Statistical analysis
Construction of metabolic signature reflecting CKM risk factors
For development of the metabolic signature, we utilized baseline metabolomics data to identify metabolites adhering to CKM risk factors. Prior to formal analysis, 16 metabolites with missing value >20% were excluded and the remaining 235 metabolites were log-transformed and standardized to the same scale. Correlations between metabolites and CKM risk factors were performed through Pearson correlation coefficient. The relationship between each metabolite and CKM risk factor was accomplished by multivariable linear regression with significance set as p < Bonferroni corrected 0.05 (Figure 1(a)). Subsequently, an elastic net regression model was used to examine metabolites and reflect the metabolic signature for CKM risk factors. This classification algorithm integrated the merits of Lasso and Ridge methods, which cope with multicollinearity and overfitting for selection of relevant characteristics. 21 We regressed CKM risk factor scores and 235 standardized metabolites with a 10-fold cross-validation method. Furthermore, the total metabolic signature was calculated through the weighted sum of the selected metabolites (coefficient ≠ 0). In all, the metabolic signature could reflect the combined effect of the weighted sum of selected metabolites (Supplementary Methods).
Association between CKM risk factors, metabolic signature, and stroke
Secondly, the COX proportional regression models were employed to explore the hazard ratios (HR) and 95% confidence intervals (CI) for the correlations between CKM risk factor scores and metabolic signature with stroke risks. A total of three models were conducted following a sequence of covariates accounting for potential confounding factors. Model 1 only adjusted age and sex, while model 2 expanded to include race, Townsend deprivation index, smoking, alcohol, MET, and sleep time. In model 3, a mutual adjustment of both CKM risk factor scores and metabolic signature was performed simultaneously to figure out their independent effect. Furthermore, restricted cubic spline analysis was conducted for investigation of non-linear relationships between CKM risk factor scores, metabolic signature, and stroke risks.
Subgroup analysis and sensitivity analysis
In order to investigate the roles of demographic factors, we conducted subgroup analysis in terms of age, sex, smoking history, and alcohol consumption. Additionally, several sensitivity analyses based on COX proportion models were performed to test the robustness of findings: (1) exclusion of stroke occurring within the first 3 years of follow-up; (2) further adjustment for usage of anti-coagulants; (3) considering all-cause mortality as completing event; and (4) constructing new metabolic profile within 251 metabolites without exclusion of biomarkers with missing data >20%.
Mendelian randomization and colocalization analysis
The two-sample Mendelian randomization (MR) analysis was used to demonstrate the causal relationships between metabolites and risks of stroke.
From published genome-wide association study statistics, genetic instrumental variables were obtained for MR analysis of each metabolite. These datasets involved 115,078 participants from the UK Biobank. Another summary statistics of stroke constitute 18,661 European stroke patients and 162,201 controls (the FinnGen dataset). For selection of independent single nucleotides polymorphism, a stringent linkage disequilibrium (LD) with 10,000 kb clumping window and r2 threshold = 0.1 was conducted. An inverse variance weighted method was regarded as the initial MR analytical method to conclude the overall estimate. As a part of sensitivity analysis, alternative methods including the weighted median, MR-Egger regression and simple and weighted mode-based estimation were employed to test the robustness of primary inverse variance weighted estimates.
A further analysis of colocalization was conducted to identify possible linkage disequilibrium driving the association between the metabolites and stroke. The Bayesian method was used to assess whether each gene locus supports the following assumptions (1) no association with either trait; (2) only associate with trait 1; (3) only associate with trait 2; (4) associations present in both traits but distinct causal variants were for two traits; and (5) both traits have correlations and the same shares causal variants. 22 We set prior probabilities of the SNP being corelated to trait 1 only at 1 × 10−4; trait 2 at only 1 × 10−4 and both trait 1 and trait 2 at 1 × 10−5. When the possibility of shared casual variants (pH4) was ⩾0.8, strong evidence of colocalization was considered. For 0.5 < pH4 < 0.8, medium colocalization was suggested.
Two-sided p < 0.05 was regarded as statistically significant. For multiple testing, Bonferroni corrections were applied to avoid potential mistakes. R packages of “glmnet” for net elastic regression and “survival” for COX regression analysis was used for data analysis.
Results
Baseline characteristics of participants
As Table 1 shown, a total of 108,305 participants free of stroke was included in analysis with average age (standard deviation (SD)) of 58.76 (7.47), of whom 48.9% were female. During the median 13.94 years (interquartile range (IQR), 13.00–14.43) of follow-up, 3881 incident stroke patients were recorded, with 2678 ischemic stroke cases (69.0%), 634 intracerebral hemorrhage (16.3%), and 315 subarachnoid hemorrhage (8.1%) cases (The remaining 254 were unspecified). At baseline, individuals with incident stroke were prone to be older male while with higher smoking rate, educational level, and lower alcohol consumption. In comparison with participants without stroke, strokes cases had higher systolic blood pressure, glycated hemoglobin, lower diastolic blood pressure, and Townsend deprivation index, with more likelihood of hypertension, diabetes, hyperlipidemia, and CKD (all p < 0.05). Furthermore, the metabolic signature of stroke participants was observed to be higher than non-stroke ones (Figures S1 and S2).
Baseline characteristics of participants stratified by stroke incidence.
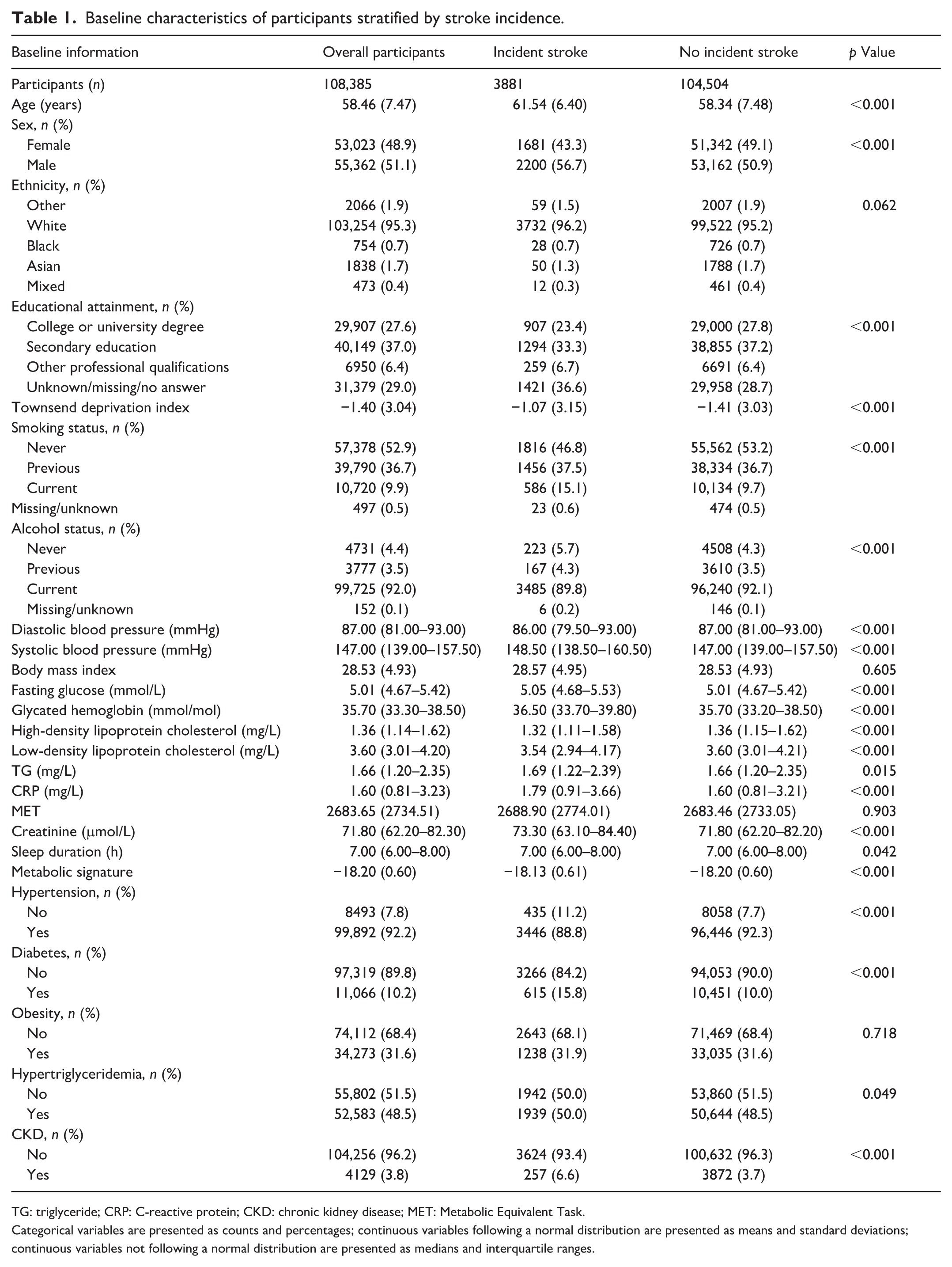
TG: triglyceride; CRP: C-reactive protein; CKD: chronic kidney disease; MET: Metabolic Equivalent Task.
Categorical variables are presented as counts and percentages; continuous variables following a normal distribution are presented as means and standard deviations; continuous variables not following a normal distribution are presented as medians and interquartile ranges.
Identification of CKM risk factor-associated metabolic signature
After exclusion of 16 metabolites with missing value >20%, we have investigated 235 metabolites in this study, with most of them, including lipoprotein and fatty acid, identified to significantly associated with CKM risk factors at the baseline. Moreover, we detected the correlations between metabolites and CKM risk factors and discovered 54 significant metabolites, which presented strong clustering patterns among lipids and lipoproteins (Figure 1). Subsequently, elastic net regression analysis on 235 metabolites at baseline were performed to build metabolic signature for CKM risk factors. Ultimately, 48 metabolites were selected to represent total metabolic signature and displayed a significant association with CKM risk factors (r = 0.66, p < Bonferroni corrected 0.05; Figure 1(b)). These metabolites consisted of lipids, lipoprotein subclasses, fatty acid, triglycerides, ketone bodies, and inflammation-related metabolites (Table S2) and observed to have consistent associations with CKM risk factor scores its components (Figure 2). Among all the metabolites, phosphoglycerides, free cholesterol in very small very-low density lipoprotein (VLDL), and concentration of intermediate-density lipoprotein (IDL) particles contributed most positively. For functional categories, lipoprotein subclasses accounted for the highest proportion (41.7%), followed by relative lipoprotein lipid concentrations and fatty acid (both 12.5%; Figure S3). On the contrary, total choline and omega-3 fatty acids to total fatty acids percentage played the most profound role in influencing reverse coefficient of the metabolic signature.
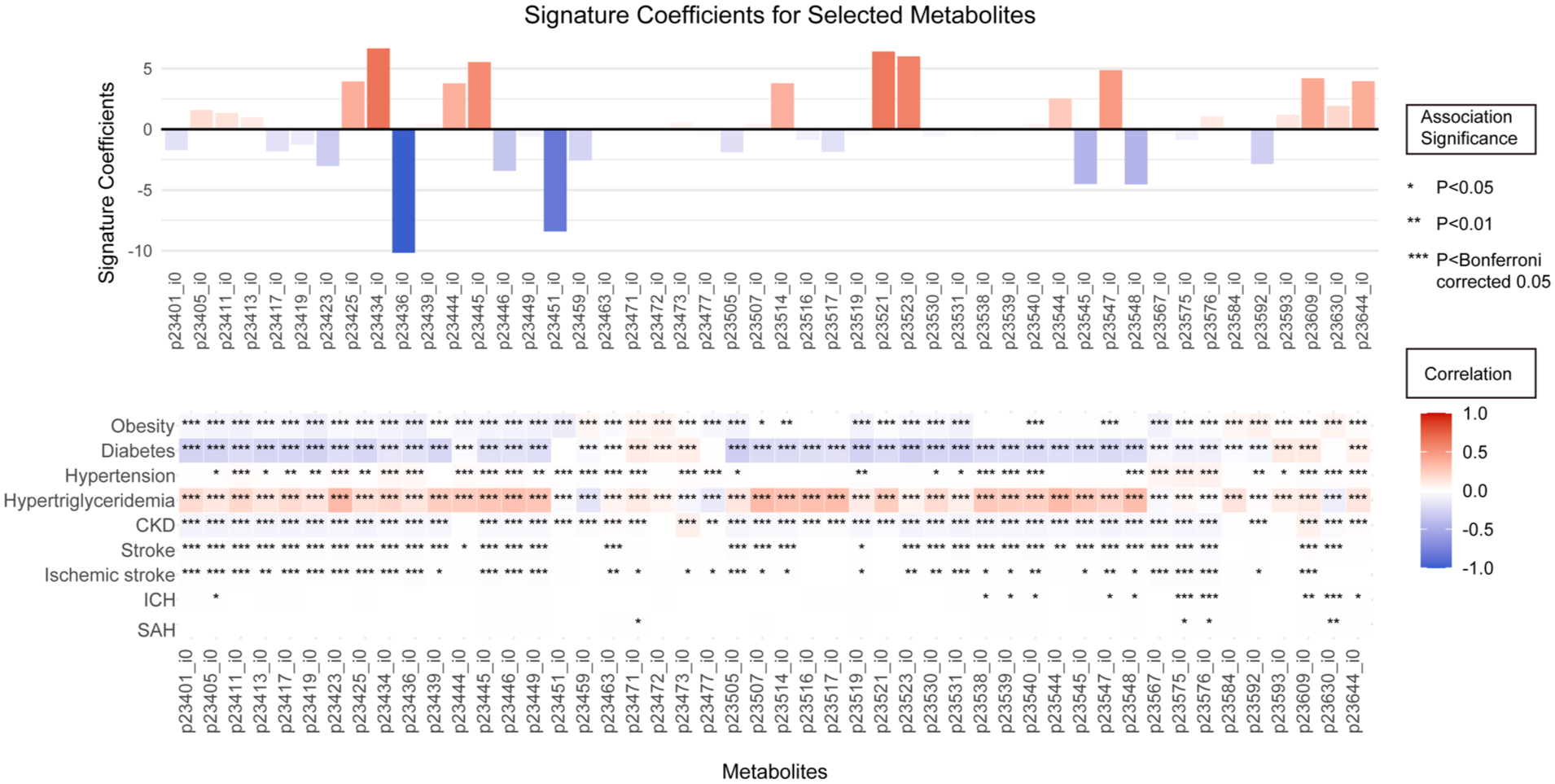
Associations between 48 metabolites and stroke and CKM risk factors. Presented form from top to bottom are coefficients and weights of metabolites in the metabolic signature and in association with CKM risk factors score, each CKM risk factor and subsequent stroke risks. Asterisks denote the significance of association levels.
Associations between stroke and CKM risk factors and metabolic signature
We confirmed that CKM risk factors were associated with stroke incidence and indicated a U-shape manner (Table 2 and Figures S4 and S5). In multivariable adjusted model 2, each increase of CKM risk factor score was associated with HRs of 1.049 (95% CI, 1.014–1.085) for stroke (Table 2) and 1.103 (95% CI, 1.060–1.148) for ischemic stroke (Table 2). Conversely, CKM risk factor score exhibited negative association with intracerebral hemorrhage (HR, 0.866; 95% CI, 0.794–0.945) and subarachnoid hemorrhage (HR, 0.710; 95% CI, 0.623–0.808; Table S2). After further adjustment of metabolic signature in model 3, CKM risk factor score only positively correlated with ischemic stroke (HR, 1.078; 95% CI, 1.022–1.0136), while the negative associations with intracerebral hemorrhage (HR, 0.821; 95% CI, 0.733–0.920) and subarachnoid hemorrhage (HR, 0.675; 95% CI, 0.572–0.798) were consistent.
Association between incident stroke risks and CKM risk factor scores and metabolic signature in UK Biobank.
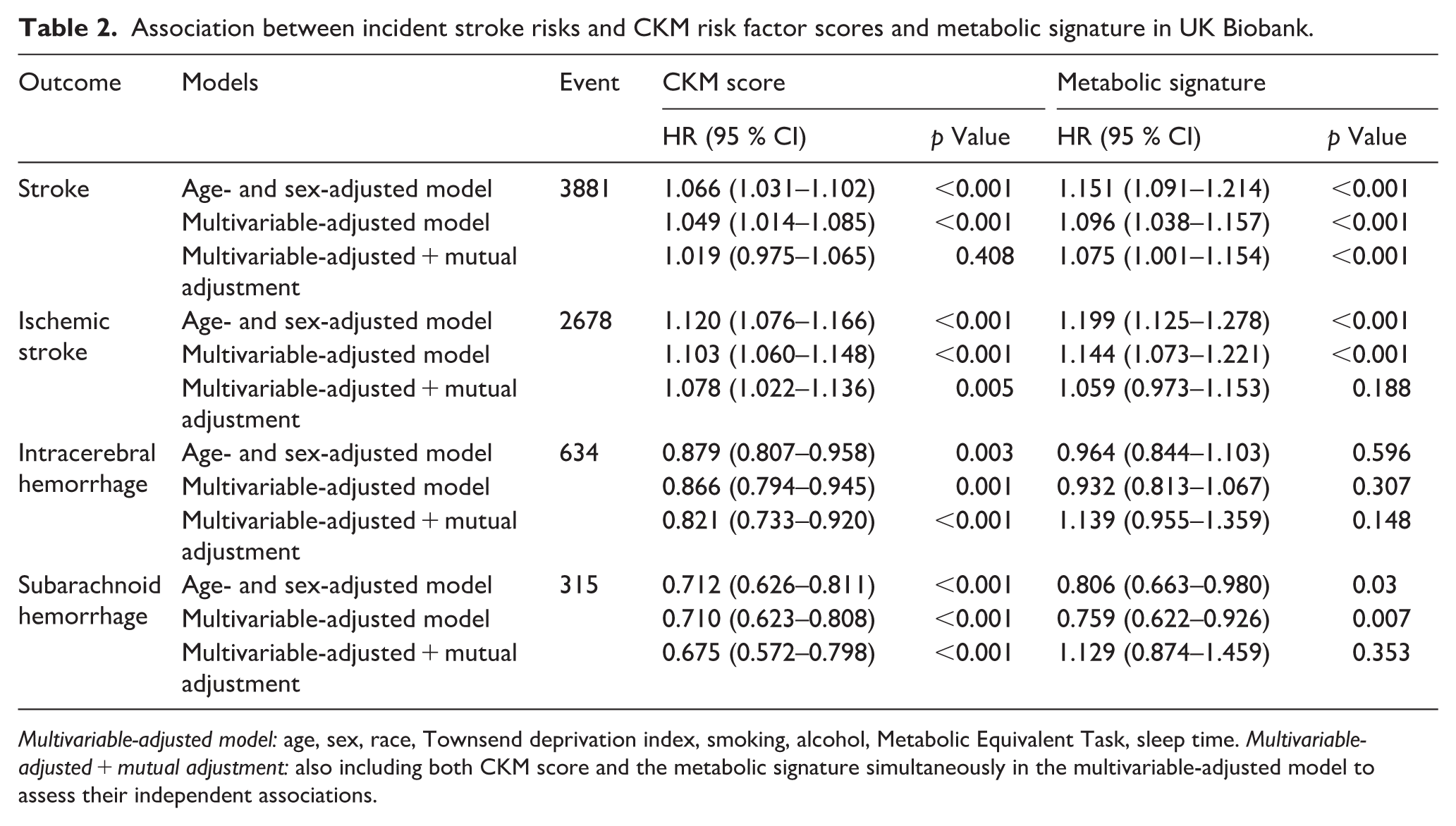
Multivariable-adjusted model: age, sex, race, Townsend deprivation index, smoking, alcohol, Metabolic Equivalent Task, sleep time. Multivariable-adjusted + mutual adjustment: also including both CKM score and the metabolic signature simultaneously in the multivariable-adjusted model to assess their independent associations.
Additionally, metabolic signature was found to impose positive effect on stroke incidence with significant dose–response manner (Table 2 and Figures S4 and S5). In model 2, metabolic signature associated with increased stroke risks (HR, 1.096; 95% CI, 1.038–1.157) and ischemic stroke risks (HR, 1.144; 95% CI, 1.073–1.221). Moreover, metabolic signature exhibited correlation with reduced subarachnoid hemorrhage risks (HR, 0.759; 95% CI, 0.622–0.926). However, the association between metabolic signature and intracerebral hemorrhage was not significant (Table 2). Notably, the association between metabolic signature and stroke remained significant even after further adjustment of CKM risk factor scores, with HRs of 1.075 (95% CI, 1.001–1.154). However, in terms of ischemic stroke, intracerebral hemorrhage and subarachnoid hemorrhage, these associations did not reach statistical significance.
Subgroup analysis and sensitivity analysis
Tables S3 and S4 summarized results of subgroup analysis. In terms of CKM score, age and sex significantly influenced the risks of incident intracerebral hemorrhage and subarachnoid hemorrhage (both p for interaction <0.05). Higher CKM score of elderly patients (HR, 0.838; 95% CI, 0.713–0.985) and female individuals (HR, 0.568; 95% CI, 0.457–0.705) had lower risks of incident intracerebral hemorrhage and subarachnoid hemorrhage, respectively. Age also has an interaction between metabolic signature of CKM score and intracerebral hemorrhage outcome (p for interaction = 0.003). Similarly, elderly individuals (age >60) of higher metabolic signature had lower risks of intracerebral hemorrhage. Additionally, the protective association of subarachnoid hemorrhage only available in non-smoking patients (HR, 0.528; 95% CI, 0.388–0.719).
Our sensitivity analysis revealed that even after taking all-cause mortality as a completing event or reconstructing a metabolic signature without exclusion of 16 metabolites, the correlation between metabolic signature and stroke stayed robust (Tables S5 and S6 and Figure S6). Additionally, after further exclusion of stroke events occurred within the first 3 years of follow-up and additional adjustment for application of anti-coagulant agents, the overall associations remained consistent (Tables S7 and S8).
Mendelian randomization and colocalization analysis
Results from MR studies indicated consistent outcomes with the observational study (Figures 3 and S7). Genetic instruments confirmed that low density lipoprotein (LDL) and VLDL subclasses are predominantly associated with elevated stroke risks. For instance, genetically increased expression of free cholesterol to total lipids in very large VLDL percentage, cholesteryl esters in small LDL and concentration of small LDL particles were considered to increase stroke risks. However, high-density lipoprotein (HDL) subclass, such as concentration of small HDL particles and cholesteryl esters in small HDL, together with omega-6 fatty acids to omega-3 fatty acids ratio were linked with lower risks of stroke.
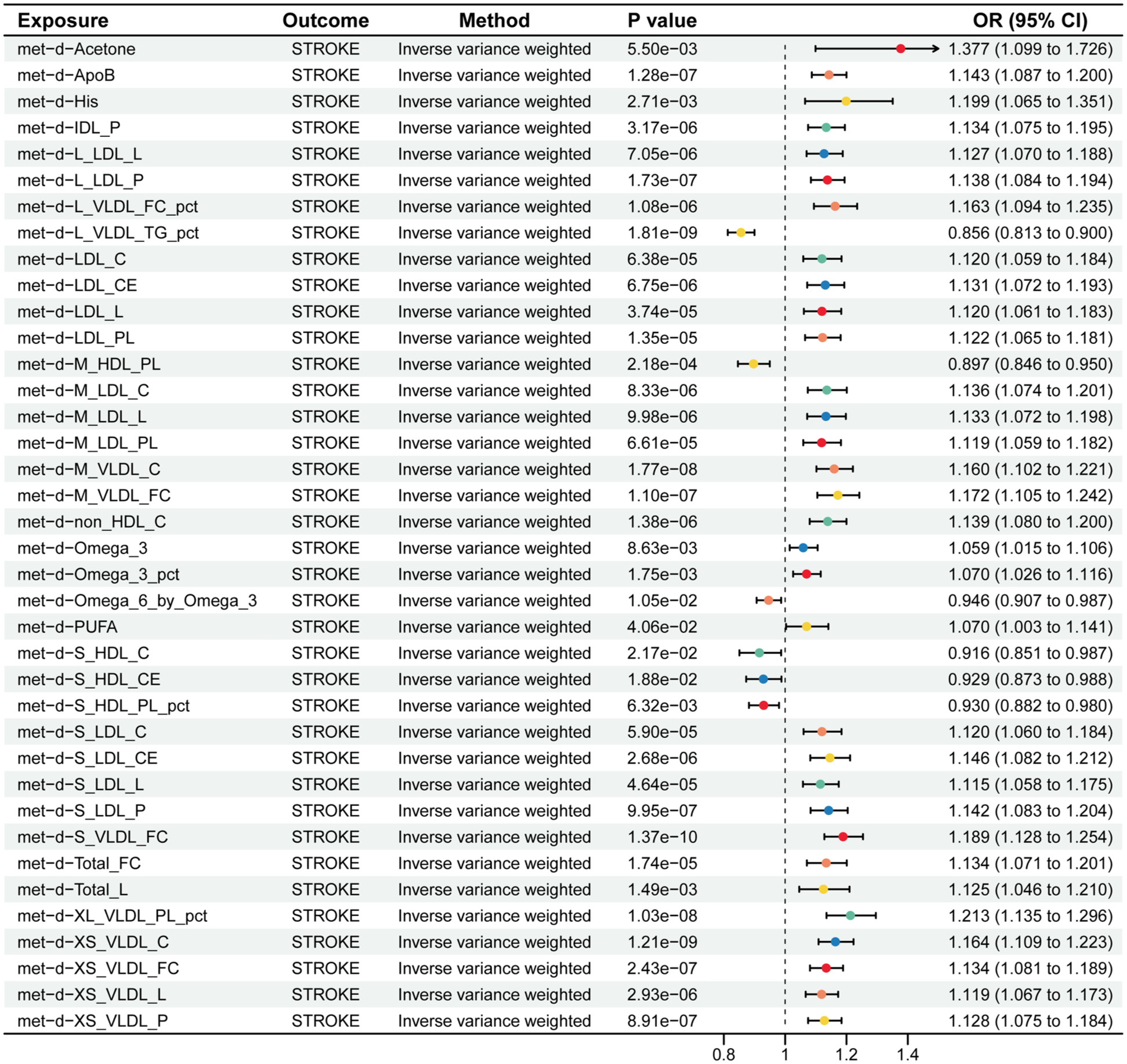
Mendelian randomization analysis of associations between genetically determined metabolites with stroke. p values are all corrected by Bonferroni method.
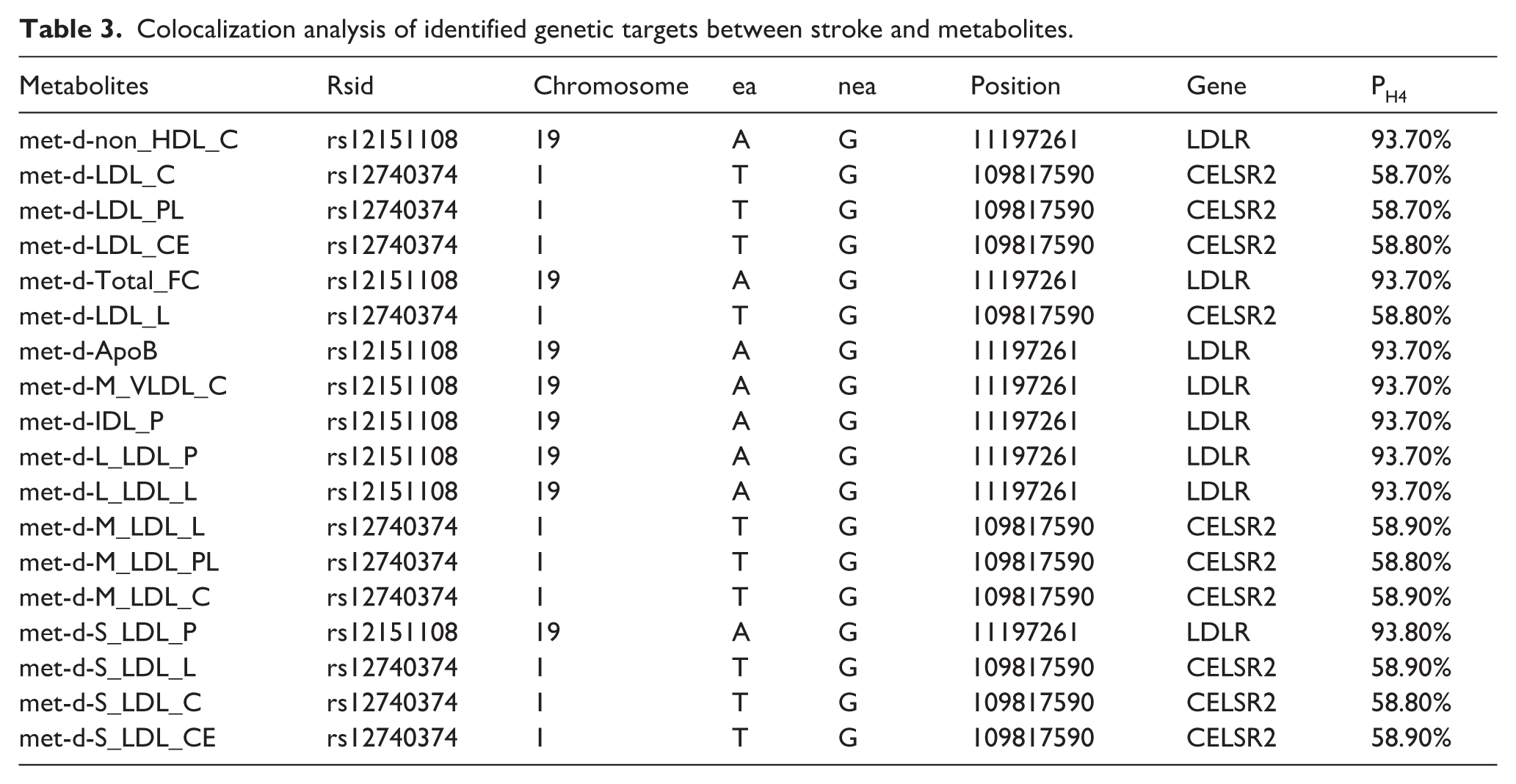
For further investigation of potential drug target genes, we performed colocalization analysis at the genome-wide significance level (Tables 3 and S7 and Figures S8 and S9). A compelling colocalization evidence was observed in one gene (LDLR) and stroke, which was identified as tier 1. In addition, cadherin EGF LAG seven-pass G-type receptor 2 (known as CELSR2) was considered as a medium colocalization between metabolites and stroke.
Colocalization analysis of identified genetic targets between stroke and metabolites.
Discussion
In this national investigation based on UK Biobank dataset, we developed a metabolic signature consisting of 48 metabolites in adherence to CKM risk factors. This metabolic signature was observed to associate with increased risks for incident stroke (mainly ischemic stroke). MR analysis conferred causal relationships between identified metabolites and stroke. To explore underlying mechanism, colocalization analysis identified LDLR and CELSR2 evidently supported associations between metabolites and stroke.
Previous studies had examined links between metabolomics and CKM risk factors, disclosing sophisticated networks between individual metabolism and risk factors, including hypertension, CKD, obesity, and diabetes.23–27 In the present study, we developed a metabolic signature constituting 48 metabolites, which established robust associations with CKM risk factors in response to early CKM syndrome and eventually demonstrated as a hazard factor for strokes. Our findings aligned with similar research that employed metabolic profiles to investigate correlation with various health outcomes. For example, Xie et al. 28 developed a SCORE2 algorithm by using 30 metabolites and observed the associations of cardiovascular disease and diabetes in general population. Additionally, another MR study at metabolome-wide level identified 46 metabolites which owned causal associations with type 1 diabetes. 27 Among these metabolites, lipoprotein family, such as apo-B containing lipoproteins, had been validated to arouse risks for cardiovascular damage, which was consistent with our findings. 29 However, no prior studies have ever emphasized metabolic characteristics in multidomain CKM risk factors, while simultaneously exploring links to long-term risks for stroke, a devastating end-stage disease in CKM syndrome. Some studies directly investigated the metabolic markers linked with stroke, which could be served as approaches to stratify stroke risks,30–32 while none of these studies incorporated key risk factors in CKM syndrome or launched a distinct metabolic signature. As stroke is a multidivisional disease triggered by dysfunction of a variety of metabolites, our findings considered diverse biological effects of metabolites and offered an integral insight into pathogenesis of stroke in early CKM syndrome.
Additionally, several lipidomic analysis highlighted the significance of lipoprotein and long-chain fatty acid metabolism in pathogenesis of stroke.30,33,34 In our study, a substantial body of lipid-related metabolites were identified, implying a vital role of lipids in neurovascular health. Furthermore, this identified metabolic signature was regarded as a comprehensive reflection of metabolic hemostasis under conditions of multidomain CKM risk factors. When considering patients in early CKM stages, it is more likely to trigger measurement and reporting bias without fully capturing the complexities of metabolic processes and how they contribute to stroke. By developing this metabolic signature, we obtain a more objective insight into metabolic change accompanying with multidomain CKM risk factors, which offers a precious tool for understanding how CKM risk factors influence individual metabolic health and decision-making in metabolic variations prior to stroke.
MR analysis and colocalization analysis shed the light on metabolic targets might play a vital role in pathogenesis of stroke. MR analysis indicates that within various dimensions of CKM risk factors, LDL subfractions of different molecular weights are major risk factors for future stroke events, while HDL and VLDL are potential protective factors. These findings are concordant with conclusions drawn from prior studies conducted within both the general population and groups exhibiting specific CKM risk factors.35–38 Moreover, Cox regression analysis reveals that in the mutually adjusted Model 3, the CKM risk factor score does not exert a significant influence on stroke outcomes. This suggests that traditional epidemiological risk factors for stroke are highly likely to impact its occurrence through alterations in metabolites. 39 Notably, CKM risk factor scores demonstrate a protective effect against intracerebral hemorrhage and subarachnoid hemorrhage, potentially attributable to increased awareness and improved medication adherence among individuals with comorbid multidimensional CKM risk factors. 40 As for intracerebral hemorrhage, previous studies have identified hypertension as the strongest risk factor for intracerebral hemorrhage. However, in our study, for the sake of clinical feasibility, blood pressure was included in the CKM score only as a binary variable. Patients with a high CKM score may receive earlier and more systematic antihypertensive treatment due to their metabolic disorders, thereby reducing the risk of incident intracerebral hemorrhage compared with those with a low CKM score. Simultaneously, subgroup analysis claimed that this protective effect solely appears in elderly patients (age >60), which might account for regular blood pressure control and awareness to seek in-time medical assistance. Beyond these, cholesterol and the LDL family played a major role in the metabolic signature constructed using elastic net regression in this study. A post hoc analysis of the SPARCL trial and a study from the Kailuan cohort in China indicated that low LDL-C levels or intensive statin therapy may be associated with a slightly increased risk of intracerebral hemorrhage, whereas higher LDL-C levels might exert a “protective” effect against the rupture of intracranial small vessels.41,42 These paradoxical epidemiological associations may be related to cell membrane stability, the integrity of the blood–brain barrier, and the role of apolipoproteins in transporting vitamin E.42,43 These findings help us explain the inverse correlations observed between the CKM score, the metabolic signature, and intracerebral hemorrhage. Obese paradox was also a possible reason for these inverse associations. Our findings are consistent with some previous studies suggesting a protective effect of higher BMI on intracerebral hemorrhage. 44 This obesity paradox is likely related to factors such as better nutritional reserves, modulation of inflammatory responses, or reduced blood pressure variability. Similarly, subarachnoid hemorrhage is most often caused by ruptured aneurysms and is only weakly associated with metabolic factors. The observed protective association with a higher CKM score is likely related to better blood pressure management in elderly population population. 45 Consequently, these inverse associations between CKM score, metabolic signature and hemorrhagic stroke should not be simply interpreted as protection effects. Long-term prospective cohort studies are needed, in which advanced causal inference methods, such as marginal structural models or instrumental variable approaches, can be employed to better account for time-varying confounding and unmeasured confounders, and thereby more robustly evaluate the causal relationship. For interventional strategy policy making, the public authorities could promote regular body examinations and in-time follow-up to build up awareness of blood pressure management in the younger generation.
Moreover, previous studies have rarely explored the potential associations between metabolites and stroke at the genetic level. This study employs colocalization analysis to exploratively establish the association between the LDLR and CELSR2 genes and stroke phenotypes. LDLR is a crucial membrane protein that regulates the uptake and clearance of LDL-C on the cell membrane. 46 Numerous studies have demonstrated that LDLR achieves vascular protection by modulating cholesterol clearance and maintaining LDL homeostasis, thereby controlling oxidative stress and counteracting apoptosis. 47 Existing research has shown that the biological function of LDLR in regulating circulating LDL and cholesterol levels is linked to downstream cascades involving proprotein convertase subtilisin/kexin type 9 (PCSK9), sorting nexins (SNXs), and Ras-associated binding proteins (Rabs).48,49 Changes in these signaling pathways can disrupt LDL metabolic homeostasis, resulting in vascular damage or thrombosis. Thus, targeting LDLR upstream to maintain LDL metabolic balance could be a promising therapeutic strategy. Meanwhile, CELSR2, served as an atypical cadherin, is highly expressed in motor neurons of both humans and mice and is involved in the biological processes of nerve repair through negative regulation. 50 Studies have suggested that this process is linked to sphingolipid metabolism, implying that CELSR2 could serve as a target influencing stroke by modulating lipid metabolism. 51
Our study has promising implications for clinical management and public health strategies. The discovery of 48 metabolites associated with specific CKM risk factors and the development of a metabolic signature provide novel biomarkers or screening tools for evaluating stroke risk. This could profoundly provide new approaches for early prevention and personalized medicine in the tremendous CKM population. Furthermore, our outcomes underscore the importance of monitoring key CKM risk factors, as depicted by metabolic signature, in intensifying stroke risks. This further emphasizes the critical role of managing metabolic markers in mitigating the burden of stroke at the population level. Moreover, this study conducts an exploratory analysis to elucidate the link between genetic factors and alterations in metabolic markers, thereby providing novel insights into the pathophysiological mechanisms underlying stroke in CKM populations and informing the development of broadly applicable therapeutic interventions. This knowledge contributes to targeted intervention design and sharpens clinical practice in brain health.
Admittedly, our study has some limitations. Firstly, metabolic signature development and examinations between metabolic signature and stroke were based on a same cohort, which may not fully eliminate potential bias and generalize people from different national backgrounds. Beyond this, the development of CKM score was an innovative exploratory attempt rather than a fully validated evaluation system. Based on these facts, future large cohort study within external population could validate reliability of CKM score and extrapolate present associations. Secondly, the evaluation of CKM risk factor populations, as well as the count of individual CKM risk factors, may be prone to inaccuracies due to potential early misdiagnosis or underdiagnosis in some participants. Meanwhile, metabolite measurements could not fully get rid of measurement errors or viability. Metabolomics data provided in a relatively narrow targeted panel in the UK Biobank restrict the enrichment investigation of upstream and downstream relationships of selected metabolites in metabolic signature. Further investigation using broader untargeted metabolomics data and experimental studies will be required to elucidate the underlying mechanisms. Third, despite our efforts to adjust various confounders, there are innate factors that may cause bias to our results. Fourth, although innovative genetic associations are observed in our analysis, the specific metabolic mechanisms underlying these associations and the exact roles of colocalized genes warrant further investigation.
Conclusion
In general, this study innovatively established a metabolic signature reflecting CKM risk factors, which was positively associated with stroke risks, while LDLR and CELSR2 might impact metabolic process in CKM population at genetic level. These findings have great potential to personalize preventive strategies and identify at-risk populations based on metabolic profiles, together with providing new insights into genetic metabolisms.
Supplemental Material
sj-docx-1-jcb-10.1177_0271678X261462718 – Supplemental material for Plasma metabolic signature of cardiovascular–kidney–metabolic syndrome and incident stroke: A nationwide prospective cohort study
Supplemental material, sj-docx-1-jcb-10.1177_0271678X261462718 for Plasma metabolic signature of cardiovascular–kidney–metabolic syndrome and incident stroke: A nationwide prospective cohort study by Kaixin Lei, Bojun Ma, Chenxi Lu, Lifan Xu, Chunxia Qiao, Yi Teng and Wen Guo in Journal of Cerebral Blood Flow & Metabolism
Supplemental Material
sj-docx-2-jcb-10.1177_0271678X261462718 – Supplemental material for Plasma metabolic signature of cardiovascular–kidney–metabolic syndrome and incident stroke: A nationwide prospective cohort study
Supplemental material, sj-docx-2-jcb-10.1177_0271678X261462718 for Plasma metabolic signature of cardiovascular–kidney–metabolic syndrome and incident stroke: A nationwide prospective cohort study by Kaixin Lei, Bojun Ma, Chenxi Lu, Lifan Xu, Chunxia Qiao, Yi Teng and Wen Guo in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Acknowledgements
The authors are grateful to the participants who dedicated their time to taking part in the UK Biobank study and contribute to the well-being of humanity, and the UK Biobank team who generously provide access for our study. This study project has been registered on UK Biobank platform with the application number of 717009.
Author contributions
Kaixin Lei analyzed the data and wrote the manuscript. Bojun Ma conceptualized the study and wrote the manuscript. Chenxi Lu provided guidance for statistical analysis. Lifan Xu and Chunxia Qiao supervised the manuscript. Yi Teng helped to visualize the figures and Wen Guo conceptualized this study, supervised the manuscript, and acquired the funding.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by Sichuan Science and Technology Program (no. 2025ZNSFSC1021) and National Science Foundation for Distinguished Young Scholars of China (grant no. 82501656) for Dr. Wen Guo.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.