
Abstract
While independent preclinical studies have reported beneficial effects of glutamate-oxaloacetate transaminase (GOT) in models of ischemic stroke, these findings remain dispersed across the literature. This PRISMA-compliant systematic review and meta-analysis aims to combine data from these studies to determine GOT’s therapeutic potential in ischemic stroke, focusing on the effects on lesion size and neurofunctional deficit. After screening results from searches in PubMed and Web of Science, and citation chasing, 12 eligible studies were included. Range of evidence met nine out of 13 STAIR criteria. Median (Q1, Q3) quality score was 8.5 (6, 11.25) on the CAMARADES 15-item checklist. Both endogenous GOT up-regulation and exogenous GOT administration reduced infarct size, with SMD = 1.14 (95% CI 0.61–1.67; p < 0.0001), to a higher extent in mice than in rats. GOT interventions also improved edema, neuronal death, somatosensory evoked responses and neurofunctional score. The findings support the therapeutic potential of GOT for acute stroke. However, effect sizes were substantially reduced after publication bias correction (28% reduction for infarct size, with some functional outcomes losing significance), and the complete absence of female, aged, and comorbid animals limits clinical translation. High-quality, pre-registered studies in clinically relevant populations are essential before clinical trials.
• The therapeutic potential of glutamateoxaloacetate transaminase (GOT) in ischemic stroke was systematically reviewed and meta-analyzed.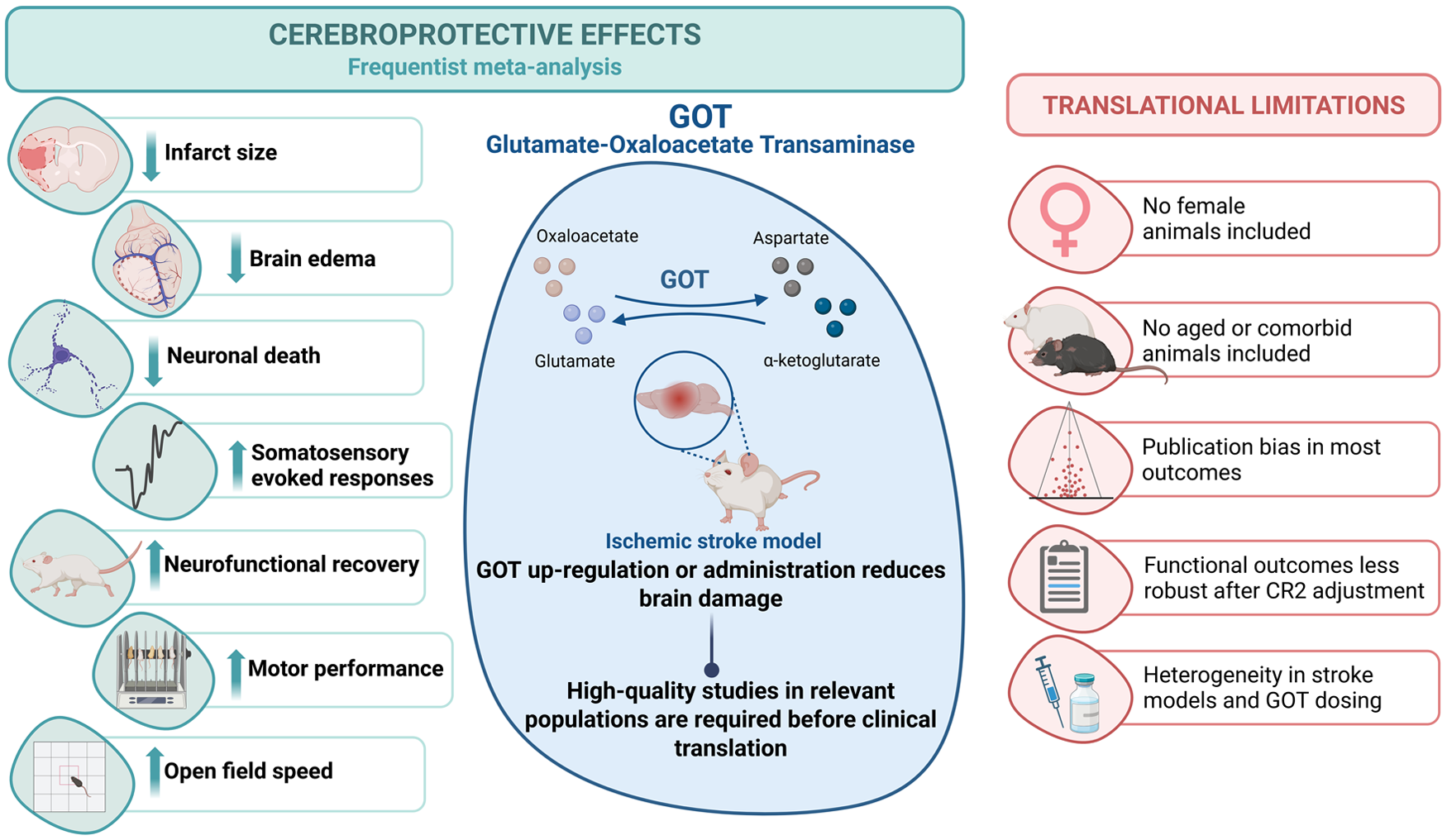
Introduction
The most recent Global Burden of Disease (GBD) 2021 stroke burden estimates showed that among non-communicable disorders, stroke remains the second leading cause of death (about seven million) and the third leading cause of death and disability combined (as expressed by disability-adjusted life-years lost—DALYs; over 160 million DALYs) in the world. In 2021, there were 93.8 million prevalent and 11.9 million incident strokes. The number of people who suffer a stroke, die from, or live with a disability after a stroke has risen substantially worldwide between 1990 and 2021. Although overall global age-standardized stroke incidence, prevalence, death, and DALY rates have reduced around the world, an aging population and population growth together with unfavorable trends of some major risk factors (mainly vascular and metabolic comorbidities) have continued to push the total burden in terms of absolute numbers ever higher, with ischemic stroke accounting for 65.3% of all stroke cases. 1 Despite decades of efforts, the thrombolytic agents alteplase (or the new variants, tenecteplase and reteplase) remain the only recommended drugs for the treatment of ischemic stroke, alone or combined with mechanical thrombectomy. 2 However, the drawbacks of this fibrinolytic therapy, including the limited proportion of eligible patients (roughly 10%–20% in well-organized health systems), mainly due to delays between onset and admission to hospital and the risk of hemorrhagic transformation,3,4 underscore the urgent need for new neuroprotective therapies, either for patients who cannot benefit from thrombolysis or as combination treatments alongside thrombolytic agents.
One of the major causes of stroke-induced brain damage is the vast increase in extracellular glutamate, leading to an influx of calcium and sodium, depolarization of the cell membrane and, ultimately, neuronal death. 5 Glutamate–oxaloacetate transaminase (GOT), also known as aspartate aminotransferase (AST), is an enzyme highly involved in glutamate metabolism and homeostasis. GOT is a pyridoxal phosphate-dependent enzyme with cytosolic (GOT1) and mitochondrial (GOT2) isozymes, which are both responsible for catalyzing the reversible transamination of oxaloacetate and glutamate into aspartate and α-ketoglutarate. This protein plays an essential role in a wide variety of cellular and metabolic processes, such as the malate-aspartate shuttle 6 or the urea and tricarboxylic acid cycles,7,8 as well as other metabolic pathways.9–12
GOT’s potential to control glutamate levels and reduce excitotoxicity has made it an attractive candidate for ameliorating neuronal damage caused by glutamate dysregulation. Several studies have shown promising results in preclinical models, suggesting that the modulation or administration of GOT could reduce neuronal injury and improve recovery outcomes in different pathologies. Some studies involving GOT in nervous system disorders include traumatic brain injury, 13 organophosphate intoxication, 14 amyotrophic lateral sclerosis, 15 glioma, 16 Alzheimer’s disease, 17 and notably, ischemic stroke.18–20
Regarding ischemic stroke, different hypotheses have been proposed in order to explain the beneficial effect of GOT, such as its ability to metabolize and reduce blood glutamate, further increasing the brain-blood gradient and reducing glutamate levels in brain parenchyma. 21 Other authors studied the ability of GOT to use glutamate as metabolic fuel in conditions of anaerobia, such as ischemia.22,23 This is supported by the capacity of GOT to reduce glutamate and attenuate ATP depletion during ischemia. 24 Another study has demonstrated the ability of mitochondrial GOT to protect against energy failure after an ischemic event. 25 Importantly, a more recent study by Pérez-Mato et al. 26 demonstrated that administration of human recombinant GOT in experimental models of cerebral ischemia not only confers robust cerebroprotection, but also shows the capacity of the enzyme to reach brain tissue, where it reduces apoptotic cell death and promotes autophagy-related protective mechanisms.
While multiple independent preclinical studies have consistently reported beneficial effects of GOT in experimental models of ischemic stroke, these findings remain dispersed across the literature. To date, there is no systematic review and meta-analysis that integrates and quantitatively evaluates the available evidence from these independent studies to comprehensively assess the therapeutic potential of GOT. On that account, the current meta-analysis aims to combine data from all the preclinical studies involving GOT-based interventions in order to determine their true therapeutic potential in ischemic stroke, focusing on its overall pooled effect on lesion size and other brain damage parameters, as well as on neurofunctional deficit. These results will further clarify the role and benefits of using GOT as a pharmacological tool or target to address the burden of stroke.
Methods
All methods were prespecified in a systematic review protocol for animal intervention studies (CRD420251048479, Version 1.0) that was registered and published online on the PROSPERO International prospective register of systematic reviews (National Institute for Health Research). Available from: https://www.crd.york.ac.uk/PROSPERO/view/CRD420251048479. The methodological approach followed specific guidelines for meta-analysis of data from animal studies, 27 as well as the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and recommendations (PRISMA 2020). 28
Literature search strategy
The search process was carried out according to the guidelines to systematically identify all relevant animal studies. 29 Two reviewers (AD-L and MAL-M) identified studies on GOT in animal models of ischemic stroke from electronic searches of Medline (using PubMed interface) and Web of Science, from inception to June 16, 2025. Search syntax was: (glutamate oxaloacetate transaminase OR glutamic-oxaloacetic transaminase OR GOT OR GOT1 OR aspartate aminotransferase OR AST) AND (stroke OR ischem* OR ischaem* OR MCAO OR pMCAO OR tMCAO) AND (rat OR rats OR mouse OR mice OR rodent* OR rabbit* OR dog OR dogs OR canine OR cat OR cats OR feline OR pig OR pigs OR porcine OR monkey*) AND (infarct* OR neurofunct* OR neurologic* OR edema OR oedema OR damage OR injury OR lesion OR neuroprotect*) AND (brain OR cerebral) NOT review. Search fields were (Title/Abstract) in PubMed and (Topic) in Web of Science. There were no language restrictions. References were added to a Mendeley Reference Manager library dedicated to this review’s topic and checked for duplicates. As a supplementary search method, R-package “citationchaser” was used for conducting forward and backward citation chasing from a starting set of eligible studies. 30 The search was not extended to unpublished studies or other sources of gray literature.
Study selection: Eligibility criteria and screening process
We included studies published as full-length original research articles in any language, provided that the English abstract was available. In cases of studies with duplicate or overlapping animal cohorts, only the publication with the most complete dataset was included. Protocol and review articles were excluded.
Regarding study design, primary experimental studies with control group (receiving no treatment, vehicle, or other sham intervention), regardless of randomization, were included. Preclinical studies in rats, mice, rabbits, or other laboratory animal species used in models of ischemic stroke, regardless of strain, age, weight, or sex, were included. GOT-based interventions were included: (1) administration of GOT (or analogs), either alone or in cotreatment with medications commonly used in stroke patients (i.e. fibrinolytics, statins, blood pressure-lowering medication, aspirin, etc.), regardless of dose, route, method and treatment schedule, (2) other interventions that modify endogenous GOT levels, or (3) a combination of the two. Finally, studies analyzing brain damage (i.e. infarct size, brain edema, neuronal injury, impairment in somatosensory evoked responses (SERs), and/or neurofunctional outcomes) were included.
Observational studies and experimental studies without control group were excluded. In vitro studies (i.e. cell cultures), ex vivo studies (i.e. brain slices), in silico studies, and studies in animal models of global cerebral ischemia, hemorrhagic stroke, traumatic brain injury, or spinal cord injury were excluded. Finally, studies reporting results without individual or aggregate data, or no statement of sample size, were excluded.
Search results were screened independently by title and abstract by two reviewers (AD-L and MCB), using the above predefined inclusion/exclusion criteria. Full reports were obtained for all titles that appeared to meet the inclusion criteria or where there was any uncertainty. Two reviewers (AD-L and MAL-M) then screened the full-text reports of potentially eligible studies and decided whether these met the inclusion criteria. Discrepancies were resolved through discussion and consensus with the supervisor (JBS).
Data extraction
Two reviewers (AD-L and MAL-M) independently extracted and tabulated study ID (first author, year, journal name, and DOI), study characteristics for the assessment of external validity, and study quality data for the assessment of internal validity.
Study characteristics included experimental groups and sample sizes, animal model (species, strain, gender, age, co-morbidities, type of ischemic stroke, duration of ischemia, and anesthetic used), intervention (type of intervention, GOT dosage, route, method and treatment schedule, and co-treatment), assessment of GOT biomarkers, outcome measures, time-points and methods of assessment (infarct size, brain edema, neuronal injury, impairment in SERs, and neurofunctional outcomes).
Range of evidence was assessed by using a 13-item checklist, 31 taken from the updated STAIR criteria 32 : (1) evidence from two or more laboratories, (2) from two or more species, (3) from animals with comorbidities, (4) from male and female animals, (5) from both permanent and temporary models of ischemia, (6) testing at least two doses of the drug, (7) with some doses given at least 1 h after vessel occlusion, (8) testing using a feasible route of drug delivery, (9) use of both histologic and behavioral outcomes, (10) outcome measured at least 4 weeks after vessel occlusion, (11) from species other than rodents, (12) interaction studies with medications commonly used in stroke patients, and (13) use of relevant biomarker endpoints.
Study quality was scored to assess risk of bias by using both the former 10-item CAMARADES’ checklist, 33 and an adapted checklist 31 that included up to 15 relevant items from the updated STAIR criteria 32 : (1) peer reviewed publication, (2) control of temperature, (3) randomization of group allocation, (4) blinded induction of ischemia, (5) blinded assessment of outcome, (6) avoidance of anesthetics with marked intrinsic neuroprotective properties, (7) use of animals with co-morbidities (e.g. hypertension, diabetes), (8) sample size calculation, (9) statement of compliance with animal welfare requirements, (10) statement of potential conflicts of interest, (11) physiological monitoring during stroke induction (in addition to control of temperature, e.g. blood pressure or gases), (12) prespecified inclusion and exclusion criteria, (13) reporting of animals excluded from analysis, (14) reporting of study funding, and (15) injury confirmed via laser Doppler or perfusion imaging.
Two unblinded reviewers (AD-L and MCB) independently collected data from outcome measures for all time points. Discrepancies were resolved through discussion and consensus with the supervisor (JBS). Infarct size (continuous variable, expressed in absolute or percent units) was considered as the primary outcome measure to stablish whether GOT might have cerebroprotective effects. Secondary outcome measures were brain edema, neuronal injury, impairment in SERs (continuous variables, expressed in absolute or percent units), and neurofunctional outcomes (continuous, expressed in absolute units, or ordinal, in absolute units within the score range). For each outcome measure, the number of animals in which this was assessed, the aggregate value of effect (i.e. mean or median) and a measure of group variance were extracted. Data were extracted from text and tables. When only graphic presentation was available, data were obtained by using WebPlotDigitizer 4.8 (https://apps.automeris.io/wpd4/) on highly magnified images. Information was also requested directly from authors for checking extracted data or if it was unavailable in the publication.
Analysis
For each outcome measure (infarct, brain edema, neuronal injury, impairment in SERs, and neurofunctional outcomes), we calculated a standardized mean difference (SMD) as effect size for each comparison. The primary effect size was corrected for small sample size (Hedges’ g), calculated using the control–treatment sign convention, such that positive values indicated a beneficial effect. Then, estimates from the different comparisons were pooled using frequentist random effects models. When studies reported multiple comparison experiments, with a control group serving more than one treatment group, the number of control animals was divided by the number of treatment groups served. First, a classic model was fitted treating each comparison as independent (i.e. naïve model), and results displayed in forest plots. Subsequently, for outcomes with more than three studies, a multilevel model with an intercept per study was fitted to capture the dependence among comparisons from the same study. Given the potential for residual intra-study correlation and the limited number of independent studies, frequentist inference was supplemented with robust cluster standard errors (CR2 adjustment) at the study level. Heterogeneity was described using τ in the naïve model and σ in the per study multilevel model. When the number of studies and the distribution of data allowed, multilevel meta-regressions were performed to explore study characteristics (stroke model parameters) as possible relevant moderators and sources of heterogeneity. A subgroup analysis was performed to assess the impact of study quality, comparing high and low risk of bias (RoB) studies. We tested the naïve models for the presence and extent of publication bias using funnel plots. Adjusted effect sizes were then estimated by incorporating theoretically missing comparisons using the trim-and-fill approach.
For infarct size, the primary outcome measure, a Bayesian approach was used as sensibility analysis. First, a normal–normal Bayesian random effects model was fitted, assuming independence between comparisons. Subsequently, a multilevel Bayesian model with a random intercept per study was fitted to capture intra-study dependence. To explore possible sources of variability, multilevel Bayesian meta-regressions were adjusted. Weakly-informative priors were used for overall effect (μ ~ (0, 1)), regression coefficient (β ~ (0, 0.5)), and heterogeneity (τ ~ (0, 0.5)). Model convergence was assessed using the Gelman–Rubin statistic (R̂ ) and effective sample size; all monitored parameters showed R̂ = 1.00 and effective sample sizes >2000.
Statistical analyses were performed using R (version 4.5.0) and R packages: metafor (version 4.8-0), meta (version 8.2-1), bayesmeta (version 3.5), brms (version 2.22.0), and clubSandwich (version 0.6.0).
All frequentist estimates included a 95% confidence interval (CI) and p < 0.05 were considered statistically significant. The Bayesian inference was based on posterior means, 95% credibility intervals (CI), and posterior probabilities of relevant directions.
Results
Literature search
A detailed study selection flow chart is shown in Figure 1. Briefly, a total of 702 records were identified in Medline and Web of Science databases. After removing duplicate, retracted, and not relevant records, 12 full-text articles were assessed for eligibility. Reasoned exclusion of one study and identification of one study via “citationchaser” rendered 12 studies included in the qualitative synthesis and subjected to meta-analysis of nine stroke outcomes.18,22,24,26,34–41
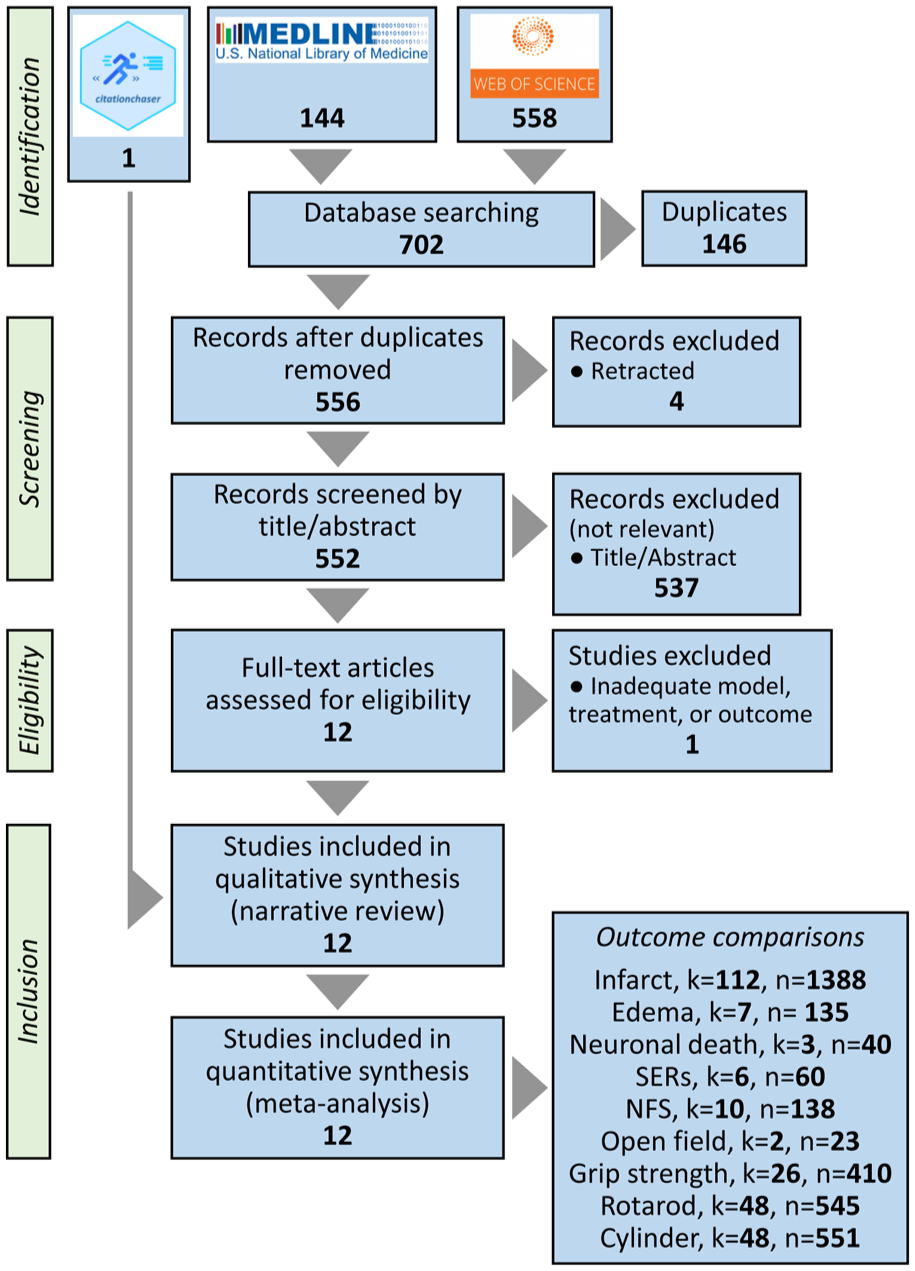
PRISMA flow diagram to depict the processes for literature search in two databases and subsequent study selection for qualitative and quantitative synthesis.
Study characteristics
A summary of the study characteristics is shown in Table 1. Briefly, studies were conducted in rats (58%), especially Sprague–Dawley strain, and mice (42%), especially C57BL/6 strain. All studies used young adult male animals without comorbidities. Intraluminal filament transient middle cerebral artery occlusion (MCAO) of different durations (45–120 min) was the most used (83%) ischemia method. Only one study avoided the use of intrinsically neuroprotective anesthetics. The GOT intervention was carried out through endogenous GOT modulation (83%), exogenous GOT administration (25%), or a combination of the two (17%). Median (Q1, Q3) exogenous GOT dose was 1 (0.6, 4) mg/kg. Most interventions were acute (92%), post-ischemic, i.v. injections (58%). All but one of the studies reported the primary outcome, infarct size. Other outcomes directly measured in the brain were edema, neuronal death, and SERs. Neurofunctional impairment was assessed by means of neurofunctional scores (NFSs), open field test, grip strength, rotarod test, cylinder test, or corner test. Most studies (83%) measured GOT or GOT-related metabolites. Key characteristics of each study are detailed in Table S1.
Study characteristics summary.
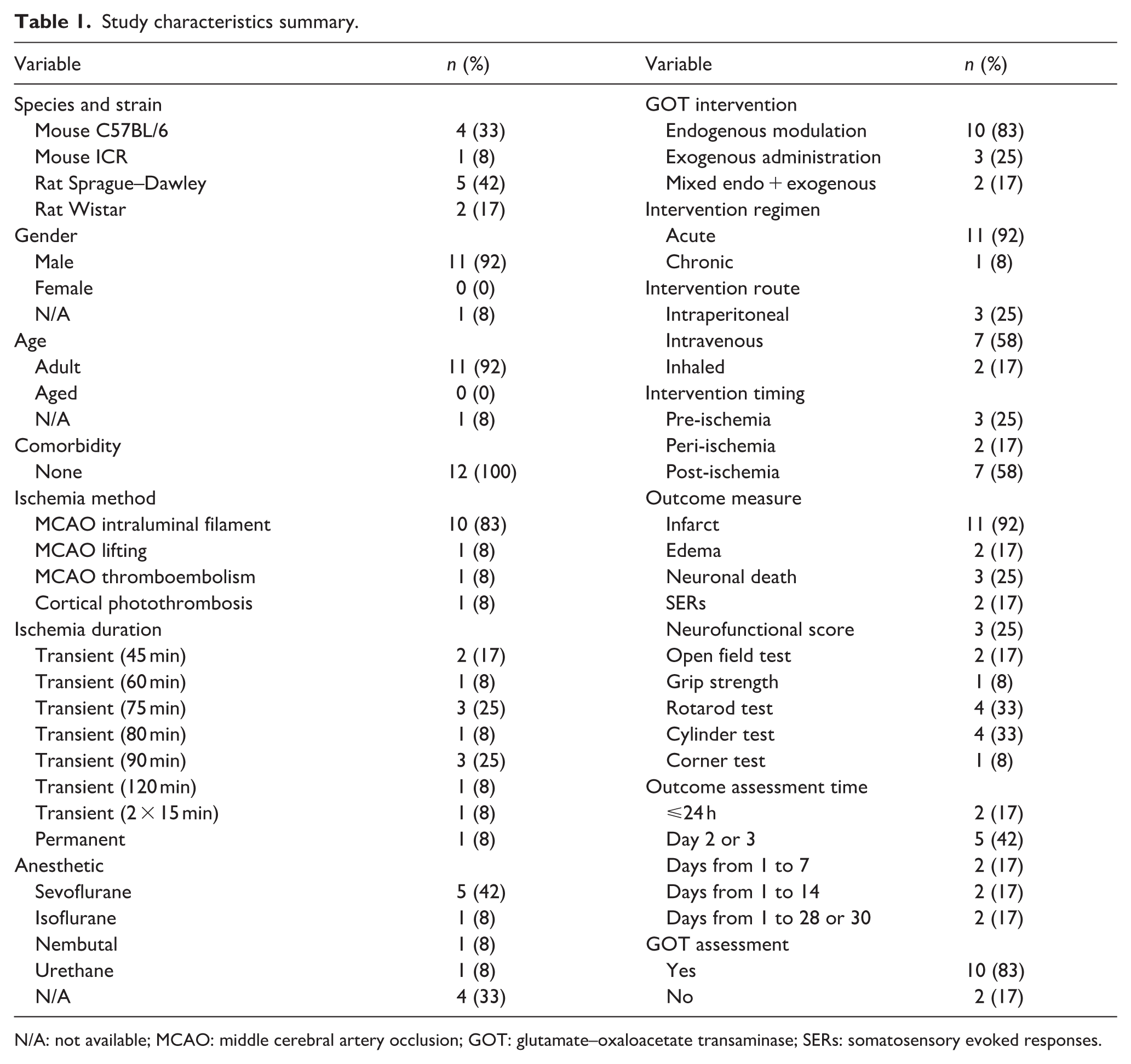
N/A: not available; MCAO: middle cerebral artery occlusion; GOT: glutamate–oxaloacetate transaminase; SERs: somatosensory evoked responses.
Range of evidence
The range of evidence met nine of the 13 updated STAIR criteria assessed. Twelve studies subjected to meta-analysis came from laboratories in four countries: Spain (5), USA (3), China (2), and Hungary (2). They used two rodent species: rats (7) and mice (5). The studies did not include animals with comorbidities or female subjects. GOT-based interventions were mostly tested in temporary models of ischemia, mainly intraluminal filament MCAO. Only one study used photothrombosis-induced permanent cortical ischemia. A wide range of doses of exogenous GOT or endogenous GOT modulating drugs were tested, given up to 10.75 h after ischemia onset (10 h after reperfusion), and using feasible, minimally invasive routes of drug delivery like i.p or i.v. injection. Ten outcome measures (structural and functional) were assessed, in some cases up to 30 days after the ischemia. The studies did not include species other than rodents (i.e. gyrencephalic species). Although one study included interaction with alteplase, these experiments were excluded because there was no control group. 26 Levels of clinically relevant blood biomarkers (i.e. GOT and glutamate) were measured.
Study quality
Table 2 shows methodological quality for each of the 12 studies included in the meta-analysis. Overall, the median (Q1, Q3) quality score (QS) was 4.5 (4, 7) on the 10-item checklist, and 8.5 (6, 11.25) on the extended 15-item checklist. Of note, all the studies were published in peer-reviewed journals, complied with animal welfare regulations, and reported sources of funding. By contrast, no study used animals with comorbidities, only one study avoided intrinsically neuroprotective anesthetics, 39 and two studies reported power and sample size calculation.26,36
Study quality report.
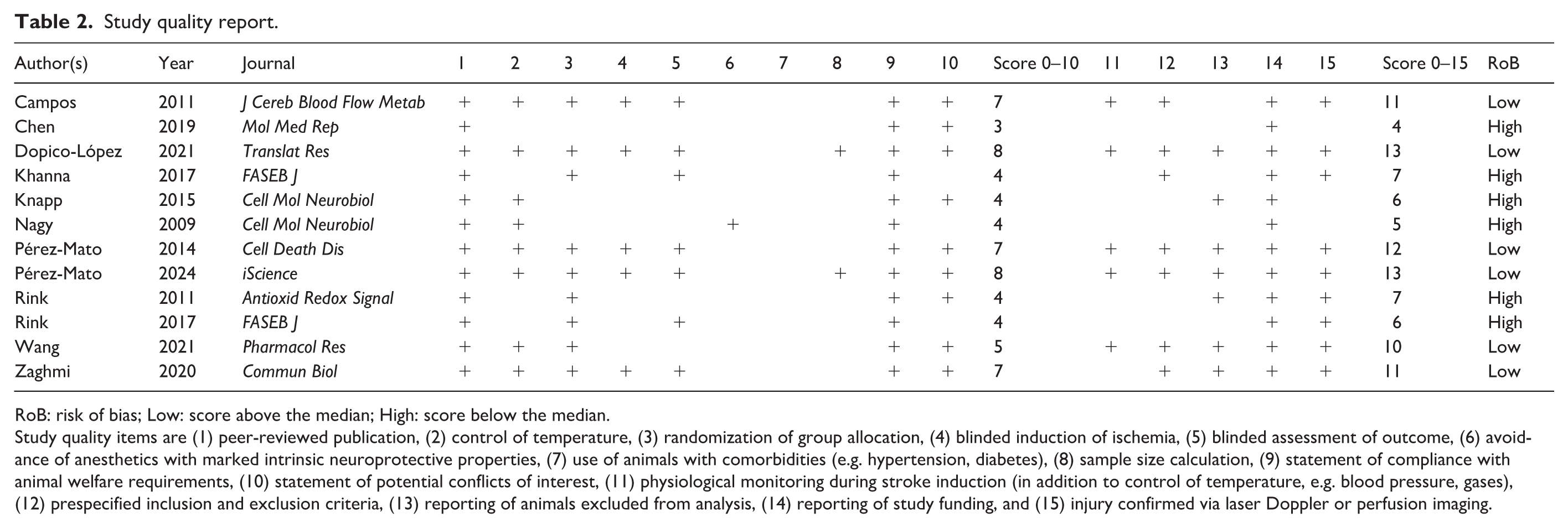
RoB: risk of bias; Low: score above the median; High: score below the median.
Study quality items are (1) peer-reviewed publication, (2) control of temperature, (3) randomization of group allocation, (4) blinded induction of ischemia, (5) blinded assessment of outcome, (6) avoidance of anesthetics with marked intrinsic neuroprotective properties, (7) use of animals with comorbidities (e.g. hypertension, diabetes), (8) sample size calculation, (9) statement of compliance with animal welfare requirements, (10) statement of potential conflicts of interest, (11) physiological monitoring during stroke induction (in addition to control of temperature, e.g. blood pressure, gases), (12) prespecified inclusion and exclusion criteria, (13) reporting of animals excluded from analysis, (14) reporting of study funding, and (15) injury confirmed via laser Doppler or perfusion imaging.
Effects of GOT on the primary ischemic stroke outcome: Infarct size
The metrics of the effects of GOT-based interventions on infarct size after ischemic stroke are summarized in Table 3. The effects of GOT on infarct size were reported in 11 articles describing 112 comparisons. Figure S1 shows individual effect sizes for each of the 112 comparisons. Overall, the frequentist naïve model with independent comparisons showed that GOT significantly reduced infarct, with a pooled SMD estimate of 0.43 (95% CI 0.28–0.57; p < 0.0001), and with no heterogeneity (τ = 0.00; 95% CI 0.00–0.24). In the multilevel model per study, GOT significantly reduced infarct, with SMD estimate of 1.14 (95% CI 0.61–1.67; p < 0.0001), and heterogeneity σ = 0.70 (95% CI 0.37–1.38). The Bayesian sensibility analysis confirmed the beneficial effect of GOT-based interventions. The naïve model showed a positive effect of GOT with µ = 0.43 (95% CI 0.28–0.58) and low heterogeneity (τ = 0.13; 95% CI 0.00–0.31). In the multilevel model per study, GOT reduced infarct with µ = 1.03 (95% CI 0.56–1.54), heterogeneity σ = 0.65 (95% CI 0.35–1.06), and estimated benefit probability p (μ > 0) = 1.00.
Effects of GOT-based interventions on ischemic stroke outcomes.
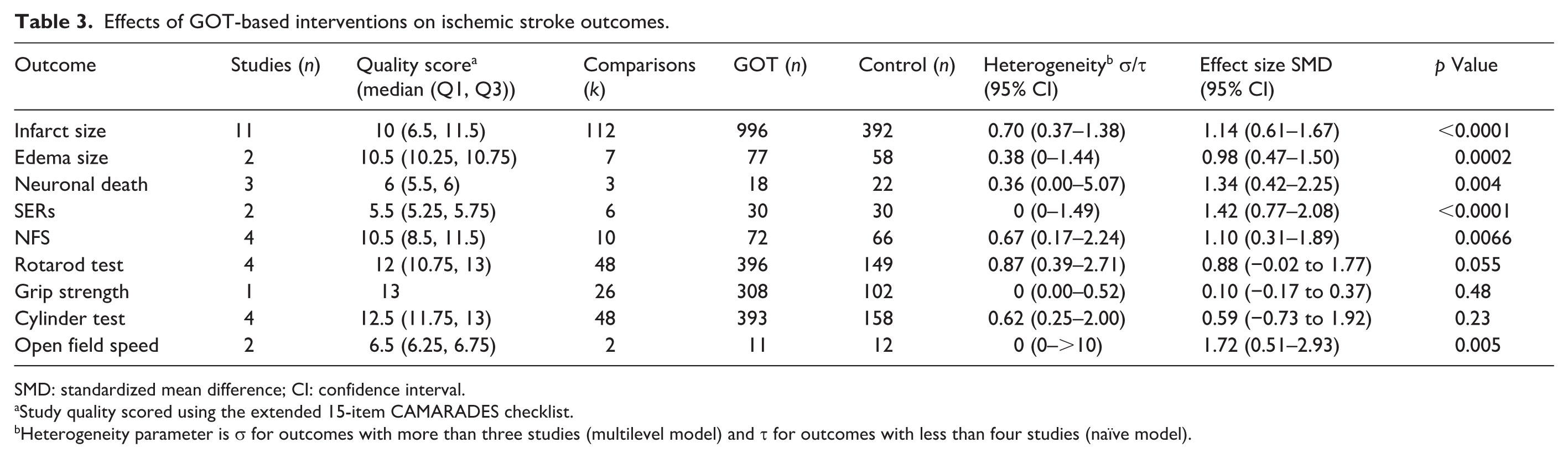
SMD: standardized mean difference; CI: confidence interval.
Study quality scored using the extended 15-item CAMARADES checklist.
Heterogeneity parameter is σ for outcomes with more than three studies (multilevel model) and τ for outcomes with less than four studies (naïve model).
The impact of study characteristics on the effect of GOT-based interventions is summarized in Table 4. Study-level meta-regression showed that the animal species was the only relevant modulator. GOT significantly reduced infarct in rats with SMD = 0.71 (95% CI 0.29–1.13; p = 0.0008). GOT effect was significantly higher in mice, with a coefficient β = 1.46 (95% CI 0.55–2.36; p = 0.0016). Introducing the species as a covariate reduced the heterogeneity to σ = 0.41 (95% CI 0.16–0.96). This was confirmed by Bayesian meta-regression. The effect in rats (µ = 0.83; 95% CI 0.39–1.33) was exceeded by the effect in mice, with β = 0.75 (95% CI −0.01 to 1.48; p (β > 0) = 0.97), and the heterogeneity was reduced to σ = 0.51 (95% CI 0.22–0.92). Regarding GOT source, exogenous GOT significantly reduced infarct, with SMD = 0.97 (95% CI 0.14–1.80; p = 0.02), which was not significantly different to the effect of endogenous GOT (β = 0.29 (95% CI −0.68 to 1.26); p = 0.56) or a combination of the two (β = −0.24 (95% CI −0.76 to 0.28); p = 0.37). Consistently, considering GOT source as a covariate did not reduce between-study variance (σ = 0.70; 95% CI 0.34–1.42). GOT effects on infarct were not significantly impacted by other study characteristics as ischemia duration (p = 0.89), GOT dose (p = 0.71), and time for outcome assessment (p = 0.79).
Effect of study characteristics as moderators of the effect of GOT-based interventions on infarct outcome after ischemic stroke.
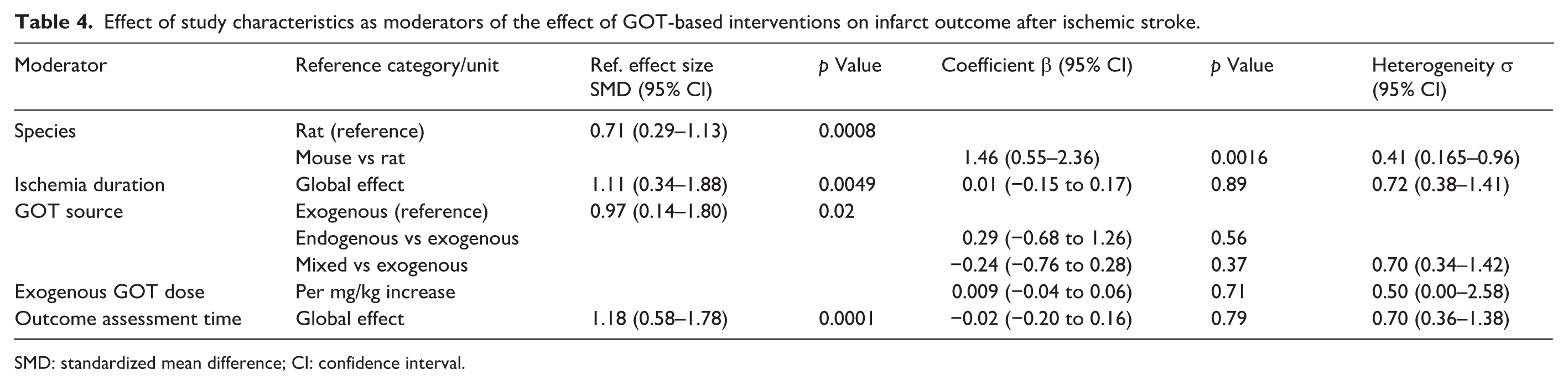
SMD: standardized mean difference; CI: confidence interval.
The impact of study quality on the effect of GOT-based interventions was assessed with a subgroup analysis comparing five high RoB and six low RoB studies. The multilevel model per study showed that GOT significantly reduced infarct in low RoB studies with SMD = 1.06 (95% CI 0.41–1.71; p = 0.001). Although GOT effect increased in high RoB studies, the difference was not statistically significant, with ΔSMD = 0.33 (95% CI −0.90 to 1.56; p = 0.60).
A naïve analysis of the publication bias revealed funnel plot asymmetry (Figure 2(a)), and the Egger test found this to be significant (p = 0.017). The trim-and-fill method imputed 15 potentially missing comparisons, reducing the overall SMD from 0.43 (95% CI 0.28–0.57) to 0.31 (95% CI 0.15–0.47); p = 0.0001. Since animal species was a modulator of GOT effect, publication bias was separately analyzed for rat and mouse studies. In rats, the Egger test did not reach statistical significance (p = 0.12). The trim-and-fill method imputed 10 potentially missing comparisons, reducing SMD from 0.33 (95% CI 0.18–0.48) to 0.29 (95% CI 0.14–0.43). In mice, the Egger test did not show statistical significance (p = 0.23). The trim-and-fill method imputed only two potentially missing comparisons, reducing SMD from 2.39 (95% CI 1.42–3.35) to 2.21 (95% CI 1.29–3.13).
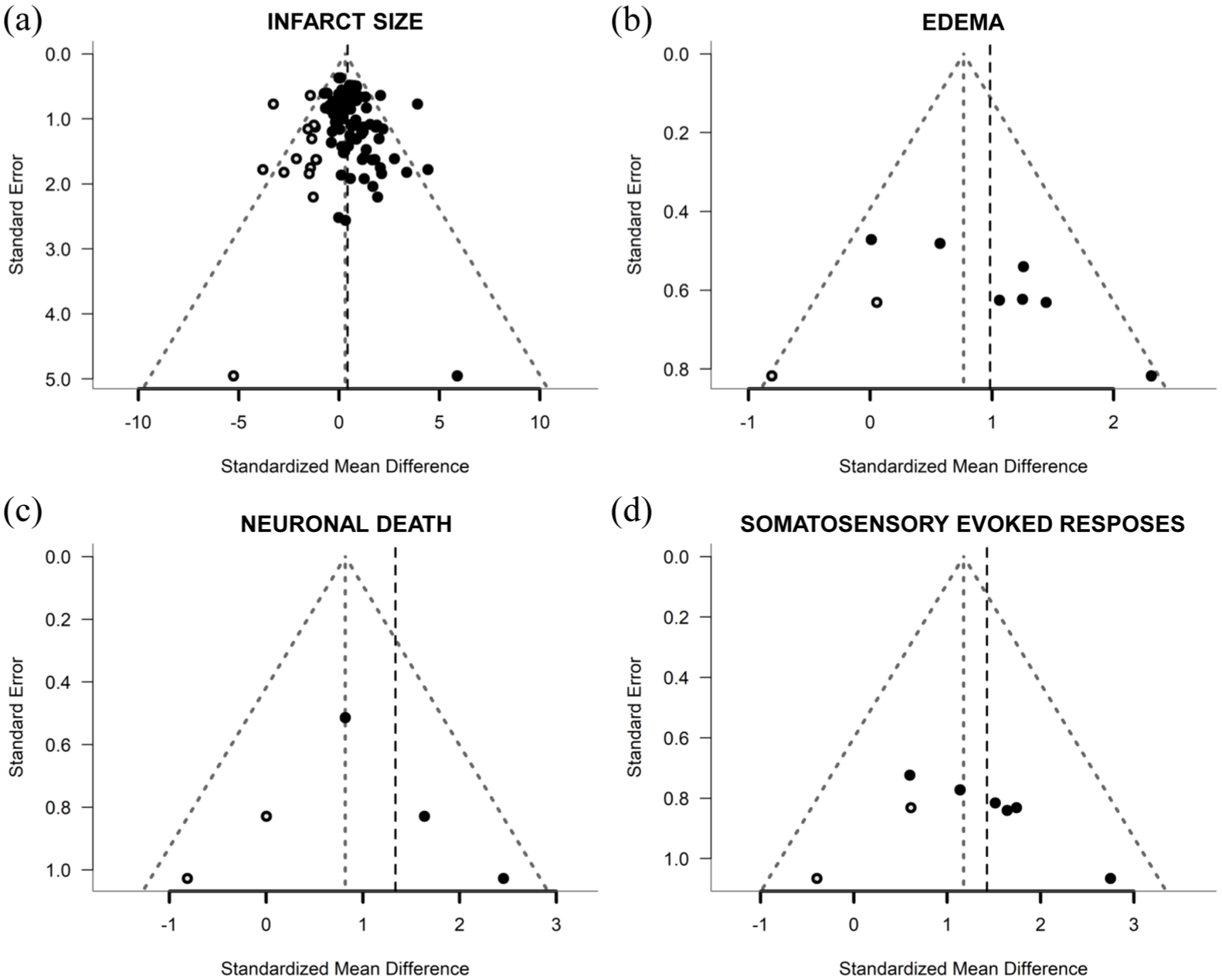
Funnel plots showing published studies (filled circles), trim-and-fill assigned studies (open circles), and the pooled estimate of efficacy before adjusting for publication bias (dashed vertical line): (a) infarct size, (b) edema, (c) neuronal death, and (d) somatosensory evoked responses.
Effects of GOT on secondary ischemic stroke outcomes
Table 3 summarizes the effects of GOT-based interventions on secondary ischemic stroke outcomes. The meta-analysis excluded corner test performance because there was only one study reporting a single experiment.
Regarding outcomes directly measured in the brain, the effects of GOT on edema were reported only in two articles describing seven comparisons. Figure S2 shows individual effect sizes for each of the seven comparisons. Overall, the frequentist naïve model with independent comparisons showed that GOT significantly reduced edema, with a pooled SMD estimate of 0.98 (95% CI 0.47–1.50; p < 0.0002), and with moderate heterogeneity although with considerable uncertainty in the estimate (τ = 0.38; 95% CI 0.00–1.44). The analysis of the publication bias revealed funnel plot asymmetry (Figure 2(b)), and the Egger test found this to be significant (p = 0.009). The trim-and-fill method imputed two potentially missing comparisons, reducing the overall SMD to 0.77 (95% CI 0.26–1.28; p = 0.0030). Just three studies, each one making one comparison, reported neuronal death. Figure S3 shows individual effect sizes for each of the three comparisons. Overall, GOT significantly reduced neuronal death, with a pooled SMD estimate of 1.34 (95% CI 0.42–2.25; p = 0.004), and with low-to-moderate heterogeneity although with considerable uncertainty in the estimate (τ = 0.36; 95% CI 0.00–5.07). The analysis of the publication bias revealed funnel plot asymmetry (Figure 2(c)), although the Egger test found this not significant (p = 0.13). The trim-and-fill method imputed two potentially missing comparisons, reducing the overall SMD to 0.82 (95% CI −0.08 to 1.71; p = 0.0726). Finally, the effects of GOT on SERs were reported only in two articles with a total of six comparisons. Figure S4 shows individual effect sizes for each of the six comparisons. Overall, GOT significantly reduced the impairment of SERs, with SMD = 1.42 (95% CI 0.77–2.08; p < 0.0001), and with no heterogeneity although with considerable uncertainty in the estimate (τ = 0,00; 95% CI 0.00–1.49). The analysis of the publication bias revealed a tendency to funnel plot asymmetry (Figure 2(d)), although the Egger test found this not significant (p = 0.086). The trim-and-fill method imputed two potentially missing comparisons, which corrected the SMD down to 1.18 (95% CI 0.59–1.76; p < 0.0001).
The effects of GOT on neurofunctional impairment were assessed by meta-analyzing results from neurofunctional score (NFS), rotarod test, cylinder test, open field test, and grip strength. The effects of GOT on NFS were reported in four articles describing 10 comparisons. Figure S5 shows individual effect sizes for each of the 10 comparisons. Overall, the frequentist naïve model with independent comparisons showed that GOT significantly improved NFS, with a pooled SMD estimate of 1.19 (95% CI 0.60–1.79; p < 0.001), and with moderate heterogeneity (τ = 0.66; 95% CI 0.00–1.63). In the multilevel model per study, GOT significantly improved NFS, with SMD estimate of 1.10 (95% CI 0.31–1.89; p < 0.0066), and heterogeneity (σ = 0.67; 95% CI 0.17–2.24). However, applying cluster-robust inference (CR2) to the four studies widened the SMD (95% CI −0.26 to 2.46; p = 0.081). Study-level meta-regression showed that the animal species was a relevant modulator. Although GOT improved NFS in rats with SMD = 0.58 (95% CI −0.27 to 1.43; p = 0.18), the effect was higher in mice, with a coefficient β = 1.05 (95% CI −0.20 to 2.29); p = 0.099. Introducing the species as a covariate reduced the heterogeneity to σ = 0.45 (95% CI 0.00–2.60). However, applying CR2 reduced species differences to β = 1.05 (95% CI −1.48 to 3.57); p = 0.216. The analysis of the publication bias revealed funnel plot asymmetry (Figure 3(a)), and the Egger test found this to be significant (p < 0.001). The trim-and-fill method imputed three potentially missing comparisons, reducing the overall SMD to 0.84 (95% CI 0.22–1.47; p = 0.0081). The effects of GOT on rotarod performance were reported in four articles describing 48 comparisons. Figure S6 shows individual effect sizes for each of the 48 comparisons. Overall, the naïve model showed that GOT significantly improved rotarod performance, with SMD = 0.24 (95% CI 0.07–0.41; p = 0.006), and with low-to-moderate heterogeneity (τ = 0.25; 95% CI 0.24–0.88). In the multilevel model per study, GOT significantly improved rotarod performance, with SMD = 0.88 (95% CI −0.02 to 1.77; p = 0.055), and high heterogeneity σ = 0.87; 95% CI 0.39–2.71. However, applying CR2 to the four studies widened the SMD (95% CI −0.58 to 2.33; p = 0.151). The analysis of the publication bias revealed funnel plot asymmetry (Figure 3(b)), and the Egger test found this to be significant (p = 3.4 × 10−10). The trim-and-fill method imputed 13 potentially missing comparisons, reducing the overall SMD to 0.06 (95% CI −0.19 to 0.31; p = 0.6430). The effects of GOT on cylinder test performance were reported in four articles describing 48 comparisons. Figure S7 shows individual effect sizes for each of the 48 comparisons. Overall, the naïve model showed that GOT tended to improve cylinder test performance, with SMD = 0.19 (95% CI −0.01 to 0.39; p = 0.066), and with moderate heterogeneity (τ = 0.40; 95% CI 0.26–0.99). In the multilevel model per study, GOT improved cylinder test performance, with SMD = 0.59 (95% CI −0.12 to 1.30; p = 0.10), and heterogeneity σ = 0.62; 95% CI 0.25–2.00. However, applying CR2 to the four studies widened the SMD (95% CI −0.73 to 1.92; p = 0.23). The analysis of the publication bias revealed funnel plot asymmetry (Figure 3(c)), and the Egger test found this to be significant (p < 0.001). The trim-and-fill method imputed 17 potentially missing comparisons, changing the overall SMD to −0.05 (95% CI −0.27 to 0.17; p = 0.6837). The effects of GOT on open field speed were reported only in two articles each one making one comparison. Figure S8 shows individual effect sizes for each of the two comparisons. Overall, the naïve model showed that GOT significantly increased open field speed, with SMD = 1.72 (95% CI 0.51–2.93; p = 0.005), and with no heterogeneity (τ = 0,00; 95% CI 0–>10). Just one study, including 26 comparisons for different doses, reported grip strength. Figure S9 shows individual effect sizes for each of the 26 comparisons. Overall, GOT did not significantly modify grip strength, with SMD = 0.10 (95% CI −0.17 to 0.37; p = 0.48), and without heterogeneity (τ = 0,00; 95% CI 0.00–0.52). The analysis of the publication bias revealed no funnel plot asymmetry (Figure 3(d)), confirmed by the Egger test (p = 0.92). Accordingly, the trim-and-fill method did not impute potentially missing comparisons. Meta-regression with exogenous GOT dose as a moderator showed a significant positive relationship, indicating a dose-response pattern in the effects on grip strength, with β = 0.093/mg/kg (95% CI 0.018–0.168; p = 0.015) and no heterogeneity.
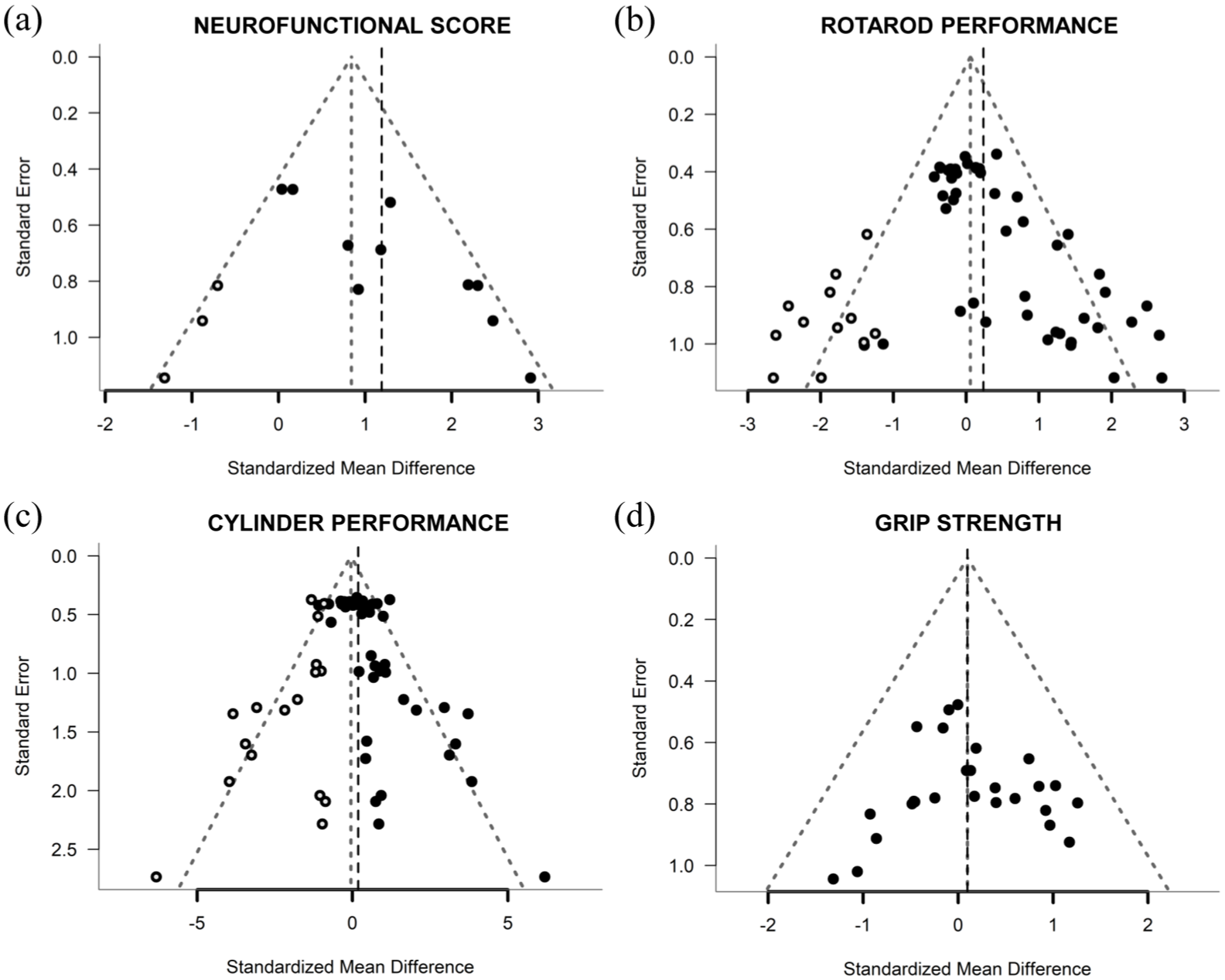
Funnel plots showing published studies (filled circles), trim-and-fill assigned studies (open circles), and the pooled estimate of efficacy before adjusting for publication bias (dashed vertical line): (a) neurofunctional score, (b) rotarod performance, (c) cylinder performance, and (d) grip strength.
Discussion
To our knowledge, this is the first systematic review and meta-analysis specifically evaluating the preclinical evidence supporting the neuroprotective potential of GOT in experimental ischemic stroke. Overall, the findings consistently demonstrate that GOT-based interventions exert a cerebroprotective effect across multiple structural and functional outcomes, reinforcing the potential therapeutic value of this biological strategy.
The primary outcome of this meta-analysis, infarct size, provides the most reliable indicator of protection in preclinical models of ischemic stroke. The results of the frequentist meta-analysis were confirmed by Bayesian models as sensitivity analysis. Our results show that GOT significantly reduces infarct size, with a large pooled effect size in multilevel analysis. Although moderate between-study heterogeneity was observed, a substantial proportion of this variability was explained by species differences. Indeed, the effect of GOT was significantly greater in mice compared to rats. This underscores the importance of testing the beneficial effects in different rodent species. The difference may be related to variations in species-specific features, such as cerebrovascular anatomy and metabolic rate, as well as stroke model severity. However, a recent meta-analysis showed higher cerebroprotective effects of resveratrol in rats compared to mice, using similar stroke models. 42 This points to species differences in the efficacy of the GOT mechanism of action. On the other hand, effect sizes in both rats and mice were slightly reduced by imputation of potentially missing studies when publication bias was separately analyzed. Importantly, other relevant experimental factors—including ischemia duration, GOT dose, and timing of outcome assessment—did not significantly influence treatment effects. This relative consistency across experimental conditions suggests that the protective effect of GOT is not restricted to a narrow therapeutic window or specific protocol, which strengthens its translational relevance.
Another key finding of this meta-analysis is that the reduction in infarct volume was consistently observed across different therapeutic approaches targeting GOT. Specifically, both exogenous administration of recombinant GOT and strategies aimed at modulating endogenous GOT activity resulted in significant neuroprotective effects. This convergence of findings suggests that the beneficial effect is primarily driven by the enzymatic activity of GOT itself. Altogether, these results reinforce the robustness and translational potential of GOT-based interventions in ischemic stroke.
Beyond infarct size, GOT also demonstrated significant benefits across other secondary endpoints, particularly those directly reflecting brain damage. The reduction in brain edema and neuronal death further supports the notion that GOT not only limits infarct expansion but also mitigates secondary injury processes, such as brain swelling and apoptotic cascades. Brain edema, of both cytotoxic and vasogenic origins, is a leading cause of death after stroke. 43 Vasogenic edema and eventual hemorrhagic transformation are particularly relevant as part of the post-ischemic reperfusion injury contributing to brain damage and stroke outcome. 44 Notably, the largest effect sizes were observed in somatosensory evoked responses (SERs), suggesting a strong preservation of neuronal function. This finding is particularly relevant, as SERs are considered a sensitive and clinically translatable biomarker of good functional recovery after stroke. 45 The consistency between structural and electrophysiological outcomes reinforces the biological coherence of GOT-mediated neuroprotection.
Neurofunctional outcomes present greater complexity and should be interpreted more cautiously. GOT significantly improved neurofunctional scores (NFS) and behavioral tests such as rotarod and cylinder performance. Of note, animal species was also a moderator of GOT effect on NFS. However, GOT’s effects on these functional outcomes lost statistical significance after applying CR2 cluster-robust adjustment. This suggests that part of the apparent statistical evidence in conventional multilevel models may have been influenced by within-study dependence and multiple correlated comparisons, reducing the effective amount of independent information contributing to these outcomes. These discrepancies highlight a common limitation in preclinical stroke research: functional outcomes are often more variable than structural measures. Furthermore, the presence of publication bias (evidenced by funnel plot asymmetry) and subsequent trim-and-fill adjustments suggest that the actual magnitude of the effects may be more modest than initially estimated.
Despite these limitations, the overall pattern of results indicates that GOT exerts a consistent and biologically meaningful cerebroprotective effect, particularly at the structural level. This distinction is important, as structural preservation is a prerequisite for functional recovery, but not always sufficient to guarantee it. The partial dissociation between structural and functional outcomes observed in this meta-analysis is consistent with previous literature and may reflect the complexity of post-stroke recovery, which involves not only neuroprotection but also neuroplasticity and network reorganization. 46
From a translational perspective, several aspects of the included studies regarding the range of evidence (external validity) warrant careful consideration. First, none of the studies incorporated clinically relevant comorbidities, such as hypertension, diabetes, obesity, or aging, despite these conditions being highly prevalent among stroke patients and known to markedly influence ischemic pathophysiology and treatment response. Likewise, all experiments were conducted exclusively in young male rodents, with a complete absence of female animals. This lack of representation of clinically relevant populations constitutes a major limitation for translational interpretation and reflects a persistent gap between current preclinical practice and STAIR recommendations. In this context, an ongoing multicentric preclinical trial (Preclinical Trials EU ID PCTE0000609) evaluating GOT administration in male and female rodents, as well as in aged and comorbid animals, represents an important step toward addressing these translational shortcomings and strengthening the clinical relevance of the available evidence. 47 Furthermore, evidence from gyrencephalic species is still unavailable, limiting the generalizability of the findings to the human condition. Finally, although some studies administered GOT several hours after ischemia onset, most interventions were performed during the acute phase, and the therapeutic window remains insufficiently characterized. Collectively, these limitations highlight the need for future high-quality preclinical studies incorporating clinically relevant populations and experimental conditions to better support the clinical development of GOT-based therapies in ischemic stroke.
Regarding internal validity of the studies, although the overall methodological quality was moderate, several important sources of bias were identified, including lack of randomization, blinding, and sample size calculation. The subgroup analysis comparing high and low risk of bias studies did not reveal significant differences in GOT effect size, but the relatively small number of studies limits the power of this analysis. Therefore, caution is warranted when interpreting the magnitude of the reported effects. The possible impact of overall quality score on estimated effect sizes of drugs/interventions is controversial. Quite interestingly, a higher power meta-analysis of meta-analyses, analyzing and pooling several different therapies instead of looking at only one single intervention, found no apparent difference in treatment efficacy between high- and low-quality studies. 48
Comparative analysis with other emerging neuroprotective agents, such as uric acid, further highlights the potential therapeutic efficacy of GOT. Uric acid has emerged as one of the most extensively studied candidate neuroprotective agents in ischemic stroke, consistently demonstrating beneficial effects in unicentric preclinical studies, largely attributed to its antioxidant properties and its ability to neutralize reactive oxygen and nitrogen species. 49 Moreover, its efficacy has been validated in a multicenter preclinical trial, conducted within the Stroke Preclinical Assessment Network (SPAN), where uric acid showed consistent benefit across different species, sexes, ages, and comorbidity conditions. 50
In the absence of a fully effective neuroprotective drug in clinical practice, uric acid may therefore be considered a reference or “gold standard” comparator for emerging therapies in ischemic stroke. In this context, the magnitude and consistency of the effects observed with GOT-based interventions in the present meta-analysis appear comparable to those reported for uric acid, 49 further supporting the potential of GOT interventions as a promising neuroprotective strategy.
Another important consideration is the integration of GOT-based therapies within the current clinical landscape of stroke treatment. Given that reperfusion therapies remain the standard of care but are applicable only to a limited proportion of patients, GOT could represent a valuable adjunctive or alternative strategy. In particular, its safety profile—given that GOT is an endogenous enzyme—makes it an attractive candidate for early administration, potentially even in prehospital settings. Furthermore, combining GOT with reperfusion therapies could provide synergistic effects by simultaneously restoring blood flow and inducing cerebroprotection. Importantly, recent preclinical evidence indicates that GOT is compatible with combined administration alongside chemical reperfusion strategies (i.e. thrombolysis), without compromising efficacy and potentially enhancing neuroprotective outcomes.26,51
It is important to summarize the limitations of the studies included in this meta-analysis. Clinically relevant populations are not represented: females, aged animals, or those with comorbidities (such as obesity or diabetes). Species differences deserve further research. Moreover, publication bias was detected in the majority of outcomes, and clustering-corrected confidence intervals revealed uncertainty in neurofunctional outcomes, which may limit the impact of the estimated effects. Finally, there is some heterogeneity both in the animal models used and in the therapeutic approach, which hinders data unification and interpretation, although it reinforces the idea that GOT is cerebroprotective regardless of methodological heterogeneity.
In conclusion, this meta-analysis provides strong preclinical evidence supporting the cerebroprotective effects of GOT in ischemic stroke, particularly in reducing infarct size and preserving neuronal integrity. Neurofunctional outcomes show more variability and are reported in a limited number of studies. Although the encouraging beneficial effects of GOT-intervention should be tempered by methodological quality in need of improvement and potential publication bias, the overall findings support the biological and therapeutic relevance of targeting glutamate homeostasis through enzymatic scavenging.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X261462771 – Supplemental material for Cerebroprotective effects of glutamate–oxaloacetate transaminase enzyme in ischemic stroke: Systematic review and meta-analysis of preclinical studies
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X261462771 for Cerebroprotective effects of glutamate–oxaloacetate transaminase enzyme in ischemic stroke: Systematic review and meta-analysis of preclinical studies by Antonio Dopico-López, Mikahela A López-Morales, María C Burguete, Esteban López-Arias, Clara Correa-Paz, María Pérez-Mato, Lluis Morales-Caba, Juan B Salom and Francisco Campos in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the RICORS-Ictus network of the Instituto de Salud Carlos III, Ministerio de Ciencia, Innovación y Universidades (RD24/0009/0003 and RD24/0009/0017, PI24/00652), and co-financed by the European Union through the European Regional Development Fund. Fundación Mutua Madrileña, and Xunta de Galicia (IGNICIA program of GAIN, no. 002_IN855A_2023). The funding source had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report and in the decision to submit the paper for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Raw extracted data, analytic R code, and any other material generated during the current study but not published within the article, including supplemental material, are available from the corresponding authors upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.