
Abstract
This community-based study examined differences in parenting quality and parent symptoms for youth in four categories: anxious (elevated anxiety symptoms), depressed (elevated depressive symptoms), comorbid (elevated anxiety and depressive symptoms), and nonelevated (elevations of neither type). Respondents were 976 young adolescents (mean age = 11.3) and their parents (912 mothers, 647 fathers) randomly selected from 28 rural/small town communities. Results indicated that depressed and comorbid groups were associated with significantly lower parenting quality and higher parent psychopathology compared to the nonelevated and anxious groups. This pattern was generally consistent across reporters (youth, mother, and father) and four domains of or related to parenting (support/warmth, conflict/anger, general child management (GCM), and parent psychopathology). Results highlight the importance of accounting for comorbidity when examining relationships between psychopathology symptoms and related variables such as parenting. Implications include the need to address relationships with parents when intervening with youth at risk for or experiencing elevated depressive symptoms.
Epidemiological research indicates that as many as 21% of children and adolescents experience an anxiety disorder (Kashani & Orvaschel, 1990) and that up to 20% to 25% of adolescents experience a depressive disorder by the time they finish high school (Lewinsohn, Hops, Roberts, Seeley, & Andrews, 1993). In addition to youth who meet diagnostic criteria for these disorders, a substantial proportion of individuals may experience significant distress from subsyndromal symptoms (Hammen & Rudolph, 2003). Thus, adolescent anxiety and depression are substantial public health issues. Research also suggests that rates of depression in childhood and adolescence have increased in recent decades (Kessler, Avenevoli, & Merikangas, 2001), which is particularly important given that adult depression is often considered to have its roots in adolescence (Hammen & Rudolph, 2003). Increasing evidence indicates that adolescents with both an anxiety disorder and major depression have a high risk of attempting suicide (Pawlak, Pascual-Sanchez, Rae, Fischer, & Ladame, 1999), highlighting the serious implications of these disorders for today’s youth (Albano, Chorpita, & Barlow, 2003). Furthermore, anxiety and depressive symptoms may interfere with key adolescent developmental processes which include identity development, increasing friendship intimacy, adjustment to physical and social changes, changing relationships with parents, and school transitions. Thus, anxiety and depression have the potential to negatively impact academic, social, and family functioning at a time marked by much transition (Albano et al., 2003; Crocetti, Klimstra, Keijsers, Hale, & Meeus, 2009; Hammen & Rudolph, 2003). Additionally, because symptoms increase notably beginning in early adolescence, it is important to study the experiences of youth in this life phase separately from children and older adolescents.
Measures of anxiety and depression are highly correlated. About 10% to 15% of youth with an anxiety disorder also have a depressive disorder, and 25% to 50% of youth with a depressive disorder also have an anxiety disorder (Axelson & Birmaher, 2001; Cole, Truglio, & Peeke, 1997). Compared to youth with only anxiety or depression, comorbid youth tend to be older and more symptomatic (Brady & Kendall, 1992). A meta-analysis of community studies of comorbidity of youth psychiatric disorders also revealed a high degree of association between depression and anxiety (Angold, Costello, & Erkanli, 1999). Because of the relatively common co-occurrence of anxiety and depression, it can be challenging for researchers to identify differential correlates of these disorders and symptom syndromes. The primary goal of the current study is to examine differences in parenting characteristics, as reported by youth, mothers, and fathers, among early adolescents categorized as nonelevated, anxious, depressed, or comorbid. By separating the sample into these four groups we are attempting to identify correlates that may distinguish symptoms of depression from those of anxiety.
Unique aspects of this study include, (a) it is drawn from a large community sample of youth, (b) it analyzes data from multiple family members, including fathers, and (c) it examines youth with elevated symptoms of anxiety and depression (comorbidity) in comparison to youth who are only high on either anxious or depressive symptoms. Regarding this last point, it is important to tease apart the correlates of depressive symptoms from those of other types of symptoms in order to better understand the development of different types of disorders (Hammen & Compas, 1994). However, most studies that have examined the relation between parenting and adolescent internalizing have assessed internalizing symptoms generally, without making a distinction between anxiety and depressive symptoms (see Hughes & Gullone, 2008), or they assessed one or both types of symptoms without accounting for comorbidity (i.e., without comparing those with both types of symptoms to those with only one type). Whereas some have argued that anxiety and depression cannot be distinguished in youth, research suggests that while they may represent one construct in young children, these are distinct constructs in adolescence (Anderson & Hope, 2008).
The tripartite model of anxiety and depression conceptualizes the roles of positive and negative affect on the development of anxiety and depression (Clark & Watson, 1991). It posits that negative affect (NA) is associated with internalizing symptoms generally, whereas low positive affect (PA) is unique to depression and is not characteristic of anxiety (Clark & Watson, 1991; Lonigan, Phillips, & Hooe, 2003). While tests of this conceptualization have yielded mixed results (for reviews see Anderson & Hope, 2008; De Bolle & De Fruyt, 2010), research in support of this theory has found that among clinical and community samples of youth, NA is strongly associated with both anxiety and depression, yet (low) PA is more strongly related to depressive symptoms only (Fox, Halpern, Ryan, & Lowe, 2010; Lonigan, Carey, & Finch, 1994; Lonigan et al., 2003). Other research has differentiated correlates of anxiety versus depression in youth. For example, Starr and Davila (2008) found that social anxiety among early adolescent girls was more strongly related to peer rather than family variables and that depressive symptoms were more strongly related to family rather than peer variables.
A central goal of the current study is to further elucidate the distinction between anxiety and depression in adolescence by examining their relations to parenting quality. Here we focus on several parenting factors pertinent to youth anxiety and depressive symptoms: (a) support/warmth, (b) conflict/anger, (c) general child management (GCM), and (d) parent anxiety and depressive symptoms.
Parental Support and Warmth
The parenting dimension of support/warmth includes affection, expression of positive affect and positive regard, and parent involvement (Ginsburg, Siqueland, Masia-Warner, & Hedtke, 2004). Parental support is theorized to help protect youth from the effects of life stress and negative mood by fostering feelings of efficacy and self-esteem (Bearman & Stice, 2008). Lamborn and colleagues posit that this dimension of parenting is critical to the formation of positive self-concept and psychological well-being in youth (Lamborn, Mounts, Steinberg, & Dornbusch, 1991). It follows, then, that youth lacking such support are at increased risk for psychological distress.
The relationship between warmth and anxiety is inconsistent (Gar, Hudson, & Rapee, 2005; Ginsburg et al., 2004; Wood, McLeod, Sigman, Hwang, & Chu, 2003). Most studies that have found a relationship between these variables have focused on clinically diagnosed youth and report that parents of children with anxiety disorders show less warmth and more control than parents of nonclinical children (Barrett, Fox, & Farrell, 2005; Suveg, Zeman, Flannery-Schroeder, & Cassano, 2005). Although some research has indicated a relationship between anxiety and parental support/warmth in community samples, analyses often have not controlled for the presence of depressive symptoms (e.g., Vazsonyi & Belliston, 2006). In contrast to findings on anxiety, clinical studies of depressed youth indicate that low parent support and warmth are consistently related to depression (Barrera & Garrison-Jones, 1992). Moreover, several community studies using adolescent self-report have found that lower parental support is related to greater depressive symptoms among European American (Lewinsohn et al., 1994; Windle, 1992), African American (Bean, Barber, & Crane, 2006), European (Vazsonyi & Belliston, 2006), Chinese (Lee, Wong, Chow, & McBride-Chang, 2006), and Canadian (McFarlane, Bellisimo, Norman, & Lange, 1994) adolescents. Studies that have included observation and/or self-report of parents have also found that parents of youth with higher depressive symptoms show lower levels of support or warmth (Dallaire et al., 2006; Ge, Best, Conger, & Simons, 1996; Oldehinkel, Veenstra, Ormel, de Winter, & Verhulst, 2006; Sheeber, Hops, Alpert, Davis, & Andrews, 1997). An exception to this is a study by Caples and Barrera (2006) in which youth report of lower maternal support was related to higher internalizing (anxiety and depressive symptoms combined), while mother report was not.
Parent-Youth Conflict, Negative Affect, and Parent Anger
There is a normative increase in mild to moderate conflict in early adolescence as youth express their growing autonomy and challenge parent authority; disagreements may be frequent and cover multiple topics (Allison & Schultz, 2004; Steinberg, 2001). Although conflict frequency tends to decline across adolescence, negative affect associated with conflict increases (Laursen, Coy, & Collins, 1998). Frequent intense conflict and the negative affect associated with it are not normative and impact youth by reducing the protective parental support described above, and by providing models of ineffective emotion regulation (Kim, Conger, Lorenz, & Elder, 2001; Laursen & Collins, 1994). Youth of parents who display frequent negative affect not only have fewer opportunities to learn how to regulate their own emotions, but also carry such patterns into other social relationships (Kim et al., 2001); poor social relationships, in turn, may further increase adolescents’ risk for negative outcomes like depression.
Garber (2005) noted that the relation between youth depression and family conflict has been supported in clinical and community samples. In community samples, youth self-report has demonstrated consistent relations between high conflict and depression from a diversity of samples, including African American (Constantine, 2006), Mexican American (Caples & Barrera, 2006), European/European American (Vazsonyi & Belliston, 2006), Chinese (Lee et al., 2006), and Australian (Bond, Toumbourou, Thomas, Catalano, & Patton, 2005) adolescents. Studies have also found that conflict and parent hostility/anger predict youth depressive symptoms longitudinally (Ge et al., 1996; Lewinsohn et al., 1994; Sheeber et al., 1997). A number of studies have also indicated an association between parent-youth conflict and youth anxiety (Burt, Cohen, & Bjorck, 1988; Caples & Barrera, 2006; Rueter, Scaramella, Wallace, & Conger, 1999; Vazsonyi & Belliston, 2006); however, these studies have either not controlled for depressive symptoms when assessing the association between conflict and anxiety, or they examined anxiety and depressive symptoms combined. Stark and colleagues (Stark, Humphrey, Crook, & Lewis, 1990) classified youth in fourth to seventh grades in four categories based on diagnostic interviews: anxious, depressed, comorbid, and control. Children in all diagnostic categories reported their families to be less supportive and to have higher levels of conflict in comparison to control youth. Furthermore, comorbid youth reported significantly more conflict than anxious children.
General Child Management (GCM)
GCM consists of three components: child monitoring, for example, how often the parent knows where the child is and who he or she is with; fair and consistent discipline, for example, discipline that does not depend on mood of parent; and democratic parenting, for example, giving youth reasons for parent decisions and asking for the child’s perspective in making important decisions (Redmond et al., 2009). This construct mirrors elements of authoritative parenting (firmness, consistency, and autonomy granting), which is related to lower levels of internalized distress and behavior problems compared to parenting styles lacking in these elements (Steinberg, Lamborn, Darling, Mounts, & Dornbusch, 1994). Relatedly, Stark et al. (1990) found that youth with both anxiety and depression diagnoses report their families as being significantly lower on “democratic family style” than youth who are anxious only. The structure and autonomy-granting provided by authoritative parenting are theorized to “work” because they encourage development of self-regulatory skills as well as cognitive and social competence; this competency, then, allows for adaptive functioning outside the family environment (Steinberg, 2001).
Parent Psychopathology
Parent psychopathology is a critical risk factor for anxiety and depression in youth, with research suggesting that children of anxious parents have two to seven times the risk for developing an anxiety disorder compared to children of nonanxious parents, with up to 60% of such children meeting criteria for an anxiety disorder (see review by Ginsburg, 2004). Similarly, children of depressed parents have rates of depression that are up to six times higher than children of nondepressed parents, and they also experience earlier ages of onset (see review by Essau, 2004). Potential methods of transmission of psychopathology from parents to youth include genetics, relationship factors (e.g., low support/warmth), marital conflict and the family stress associated with it, and modeling of maladaptive behaviors such as avoidance of feared situations and negatively biased interpretations of events (Essau, 2004; Garber, 2005; Gar et al., 2005).
Hypotheses
Given the findings reviewed above, it is expected that there will be significant relationships between anxiety and depressive symptoms and the parenting variables of (a) support/warmth, (b) conflict/anger, (c) GCM, and (d) parent psychopathology. It is hypothesized that,
Hypothesis 1: Youth with elevated anxiety and depressive symptoms (comorbid) will be associated with lower quality parenting (i.e., less warmth, more conflict, and poorer child management) as reported by youth, mother, and father compared to youth with no symptom elevations (nonelevated).
Hypothesis 2: Youth with elevated anxiety or depressive symptoms, but not both (the anxious and depressed groups), are expected to be associated with lower quality parenting than youth with no elevations (nonelevated), but are expected to be associated with higher quality parenting than those with elevations in both categories (comorbid).
Hypothesis 3: Youth with elevated anxiety and depressive symptoms (comorbid) will have parents with significantly higher anxiety and depressive symptoms compared to parents of youth with no symptom elevations (nonelevated).
Method
Procedure
Data for the current study were obtained as part of a large-scale effectiveness trial of youth substance abuse prevention (Spoth, Greenberg, Bierman, & Redmond, 2004). The project involved youth from two cohorts of sixth graders from 28 communities (seven intervention and seven control communities in each of two states). Students in each cohort completed in-school questionnaires, and families of students in the second cohort were randomly selected for participation in in-home assessments with their sixth-grade child. A total of 2,267 families were recruited for the in-home family assessments; of these, 975 (43%) completed the assessments at the pretest (prior to intervention). Targeted sample sizes ranged from 30 families in the smallest school district to 74 families in the largest district, and actual sample sizes ranged from 18 to 68 families across the 28 communities. Recruitment included mail and telephone contacts followed by an in-person recruitment visit. In-home assessments included written questionnaires completed independently by youth and their parents (mothers and fathers completed separate forms) and videotaped family interaction tasks. Data used in the current study were obtained from self-report measures administered at the pretest in-home family assessments.
To test for selection bias, youth in the in-home sample were compared to youth in the total sample assessed at school (n = 4,400) on demographic and behavioral outcomes.
1
Youth in the in-home sample were not different from the larger sample on receipt of free or reduced-cost lunch (33.6% vs. 33.0%, respectively), living with both biological parents (59.3% vs. 62.5%), race (88.6% White vs. 86.5% White), or gender. In addition, no differences were found between groups on stress management; assertiveness; youth-to-parent or parent-to-youth expressions of care, affection, and appreciation; or frequency of activities with parents. However, youth who participated in in-home assessments reported higher family cohesion (
Participants
The sample of 975 young adolescents (mean age = 11.3) and their parents (912 mothers, 647 fathers) were assessed in the fall of the youths’ sixth-grade year. The youth sample was predominantly White (88% White, 6% Hispanic, 2% African American, 4% Other) and 52% were female. Sixty-one percent were living in Iowa and the remainder (39%) was living in Pennsylvania, with the majority living in rural areas. This sample of families is primarily middle class, indicated by a mean household income of US $51,000 and an average parent education of some college. The average ages of mothers and fathers were 38.7 and 41.1, respectively. The majority of youth (80%) lived with a parent who is married, with 54% living with both biological parents. The average number of children in the family was three.
Measures
Adolescent Internalizing
Adolescent internalizing symptoms were assessed using 14 items from the Youth Self-Report (YSR), the youth-report version of the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001). Six items were selected to assess anxiety (e.g., “I am nervous or tense,” “I worry a lot,” “I am too fearful or anxious”) and eight were chosen to measure depression (e.g., “I cry a lot,” “I am unhappy, sad, or depressed,” “I think about killing myself”). Youth rated how true each item was for them “now or within the past 6 months” on a Likert-type scale ranging from 0 (not true) to 2 (very true or often true). Cronbach’s coefficient alphas were .75 (anxiety) and .78 (depressive).
Parenting Measures
The parenting scales were developed based on relevant literature and with the use of exploratory and confirmatory factor analyses (Spoth, Redmond, & Shin, 1998). Mothers, fathers, and youth reported on all three scales, with respondents completing separate forms. All items were rated on a 5- or 7-point Likert-type scale indicating how often the behavior in question was displayed.
Support/Warmth
This scale assessed parental support (6 items, e.g., “I show support when my child talks about what he or she wants to do when grown up”), positive affective quality (3 items, e.g., “Act loving and affectionate toward him or her”), and parental involvement (2 items, e.g., “I find ways to keep my child involved with fun activities in our family”). Mothers (α = .85) and fathers (α = .88) responded to all 11 items, whereas youth responded only to the positive affective quality items (α = .79 youth about mother, α = .88 youth about father).
Conflict/Anger
This scale measured recurring conflict between parents and youth (3 items, e.g., “During an average week, how often do you and this child have serious arguments?”) and negative affective quality (3 items, e.g., “During the past month . . . how often did you yell, insult or swear at your child when you disagreed?”). Alpha levels for all six items were as follows: .85 (mothers), .83 (fathers), .80 (youth about mothers), and .81 (youth about fathers).
General Child Management (GCM).
This scale assessed parental monitoring (5 items, e.g., “In the course of a day, how often do you know where this child is?”), consistent discipline (4 items, e.g., “Once a discipline has been decided, how often can he or she get out of it?”), and democratic parenting (4 items, e.g., “How often do you give reasons to this child for your decisions?”). Alpha levels for the 13 items were: .71 (mothers), .72 (fathers), .68 (youth about mothers), and .80 (youth about fathers).
Parent Internalizing
Parent symptoms of depression and anxiety were assessed using two subscales of the Symptom Checklist-90-R (SCL-90-R; Derogatis & Lazarus, 1994), a well-known 90-item self-report inventory of psychological symptoms. The Anxiety scale consists of 10 items such as, “During the past week how much were you distressed or bothered by nervousness or shakiness inside.” The Depression scale includes 13 items, for example, “During the past week how much were you distressed or bothered by feeling hopeless about the future.” Participants rated each item using a 5-point Likert-type scale. Reliability for the current study was strong: α = .89 and α = .91 for maternal anxiety and depressive symptoms, respectively, and α = .80 and α = .89 for paternal anxiety and depressive symptoms.
Results
Analytic Strategy
To examine parenting differences between groups of youth, youth were first categorized as elevated or not on anxious and depressive symptoms, separately, by dichotomizing the sample at greater than or equal to one standard deviation above the mean versus less than one standard deviation above the mean. (Established norms for the YSR were not used because not all YSR items were used.) As a result, 18% of youth reported elevated anxiety symptoms and 13% reported elevated depressive symptoms. These rates are comparable to those found in other community studies (Albano et al., 2003; Hammen & Rudolph, 2003). Second, in order to examine anticipated comorbidity of anxiety and depressive symptoms, youth were then categorized into four groups: anxious (11%, n = 103, elevated on anxiety symptoms only), depressed (6%, n = 59, elevated on depressive symptoms only), comorbid (7%, n = 72, elevated on both types of symptoms), and nonelevated (76%, n = 745, elevated on neither type of symptom). These numbers indicate that while the majority of youth did not have symptom elevations, approximately one in four adolescents in this community sample had elevated symptoms in one or both categories.
The next analytic step involved conducting a multivariate analysis of variance (MANOVA) for each group of dependent variables: (a) youth report about maternal parenting, (b) youth report about paternal parenting, (c) maternal self report of parenting, (d) paternal self report of parenting, (e) maternal internalizing symptoms, and (f) paternal internalizing symptoms. MANOVA was chosen in order to control for the increased risk of family-wise Type I error associated with conducting only ANOVA for each dependent variable separately (Tabachnick & Fidell, 2007). Parent symptoms were analyzed separately from parenting behaviors because correlations between these constructs were small and MANOVA is most appropriate with moderately correlated dependent variables. Prior to conducting MANOVA the data were carefully examined with respect to relevant statistical assumptions (e.g., sample size, normality, outliers, multicollinearity). As a result, seven dependent variables were transformed according to procedures recommended by Tabachnick and Fidell (2007) for dealing with multivariate outliers: youth report of maternal and paternal support/warmth (reflect and logarithm transformations), youth report of paternal conflict/anger (logarithm transformation), and maternal and paternal anxiety and depressive symptoms (inverse transformations).
The Pillai’s Trace statistic, which is recommended for unequal group sizes, was used to determine whether there were statistically significant differences between the four groups of youth on the linear combination of each group of dependent variables. This test was significant for each MANOVA (details below), thus, we next examined the effect for each dependent variable to determine where groups differed. To control for Type I error at this step we used a Bonferroni correction by dividing the alpha of .05 by three where there were three dependent variables per MANOVA, resulting in a p value of .017; similarly, we divided .05 by two where there were two dependent variables per MANOVA, resulting in a p value of .025. Next, for each dependent variable with a significant effect, we then conducted a one-way ANOVA to determine the nature of the group differences. At this final step we controlled for Type I error by using the Scheffe test, the most conservative of the post hoc tests.
Descriptive Statistics
Means and standard deviations of youth-reported symptoms and percentages by sex are provided in Table 1. Comorbid youth reported higher symptoms, on average, than youth in the anxious and depressed groups. ANOVAs with Tukey’s pot hoc comparisons revealed that these differences were statistically significant, with comorbid youth reporting higher anxiety than anxious youth (p < .05) and higher depression than depressed youth (p < .05). Equal percentages of females and males were in the depressed group (6%); however, somewhat more females were in the anxious (12% vs. 9%) and comorbid groups (9% vs. 6%). Likewise, somewhat fewer females were in the nonelevated group (73% vs. 79%). T tests indicated that anxiety symptoms were higher among females (
Descriptive Statistics for Youth Internalizing Symptoms by Youth Symptom Group.
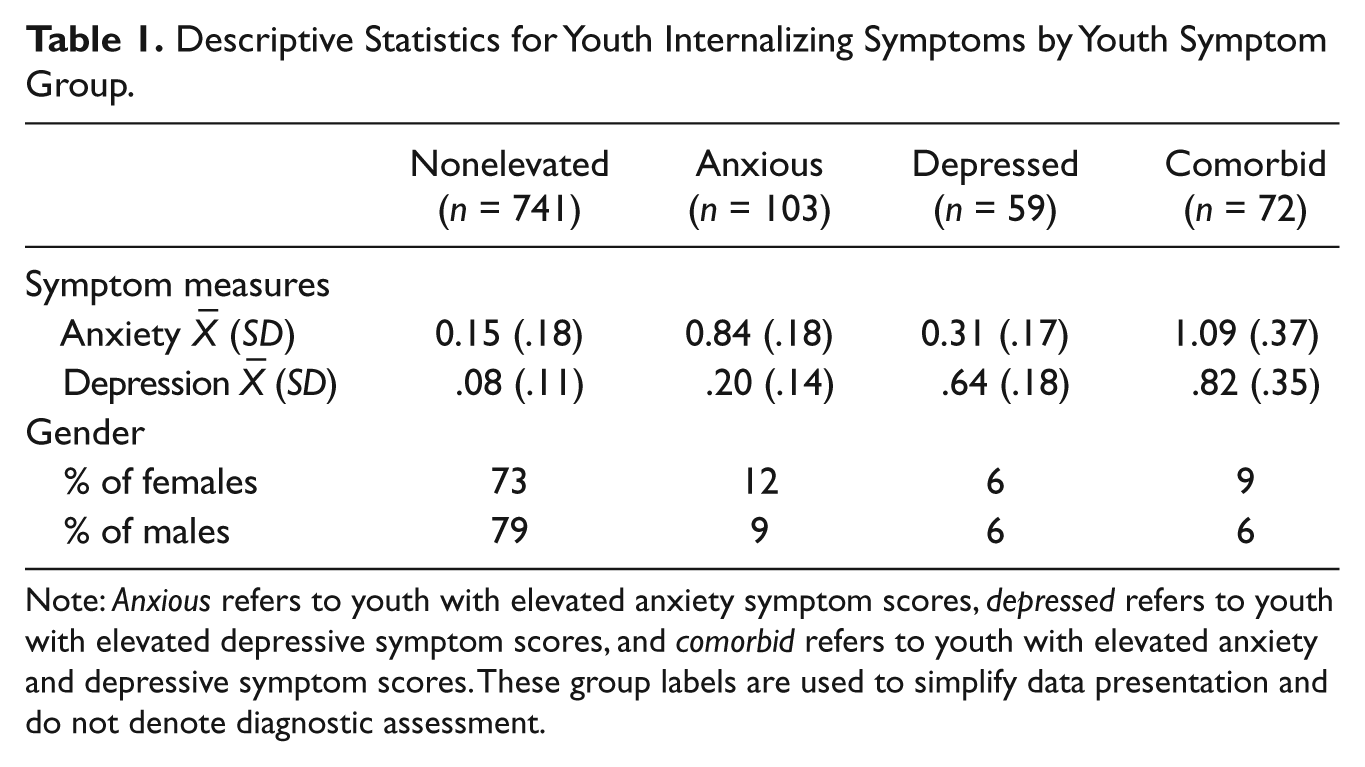
Note: Anxious refers to youth with elevated anxiety symptom scores, depressed refers to youth with elevated depressive symptom scores, and comorbid refers to youth with elevated anxiety and depressive symptom scores. These group labels are used to simplify data presentation and do not denote diagnostic assessment.
Means and Standard Deviations on Youth-Reported Parenting by Youth Symptom Group.
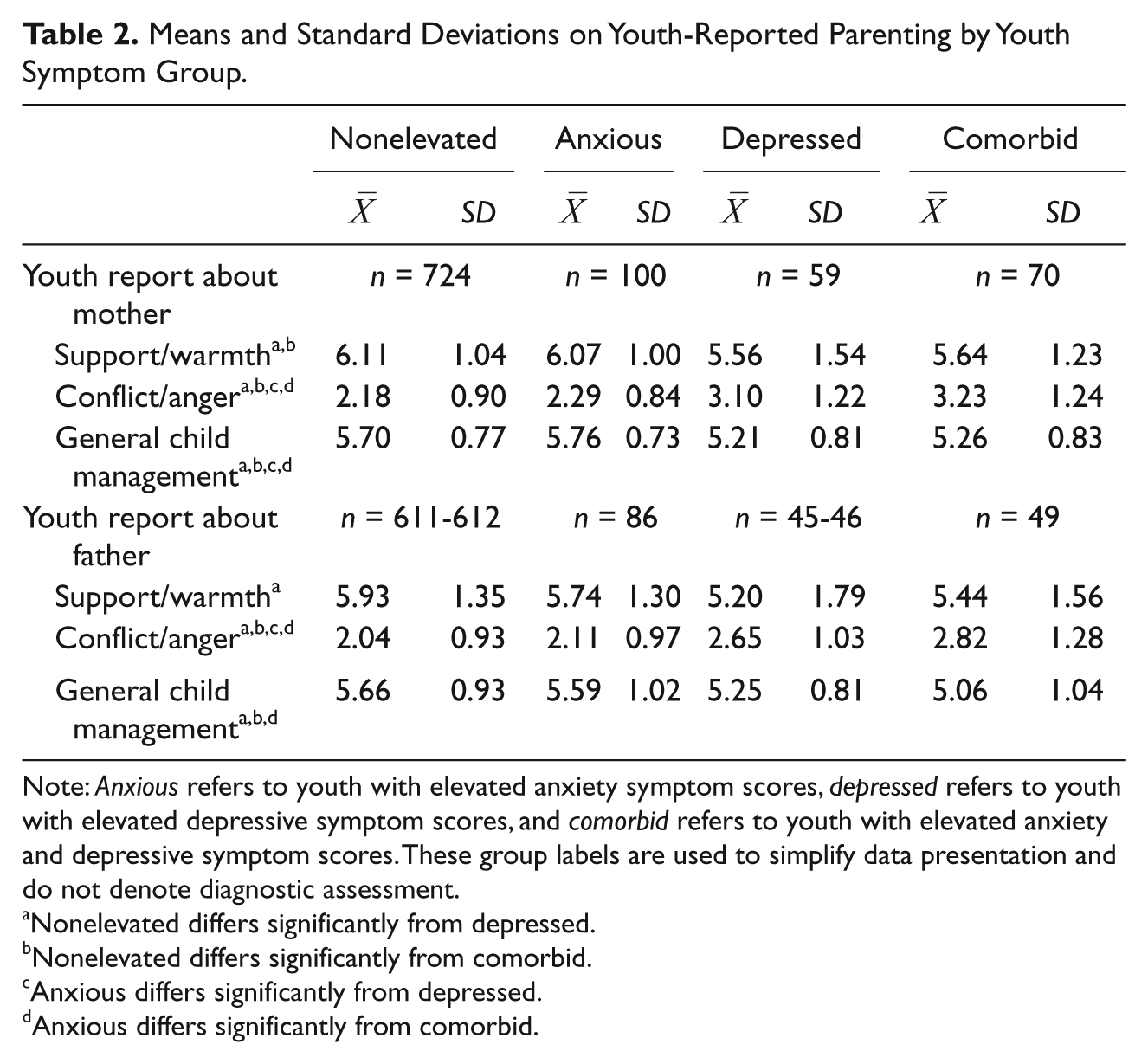
Note: Anxious refers to youth with elevated anxiety symptom scores, depressed refers to youth with elevated depressive symptom scores, and comorbid refers to youth with elevated anxiety and depressive symptom scores. These group labels are used to simplify data presentation and do not denote diagnostic assessment.
Nonelevated differs significantly from depressed.
Nonelevated differs significantly from comorbid.
Anxious differs significantly from depressed.
Anxious differs significantly from comorbid.
Means and Standard Deviations on Parent-Reported Parenting by Youth Symptom Group.
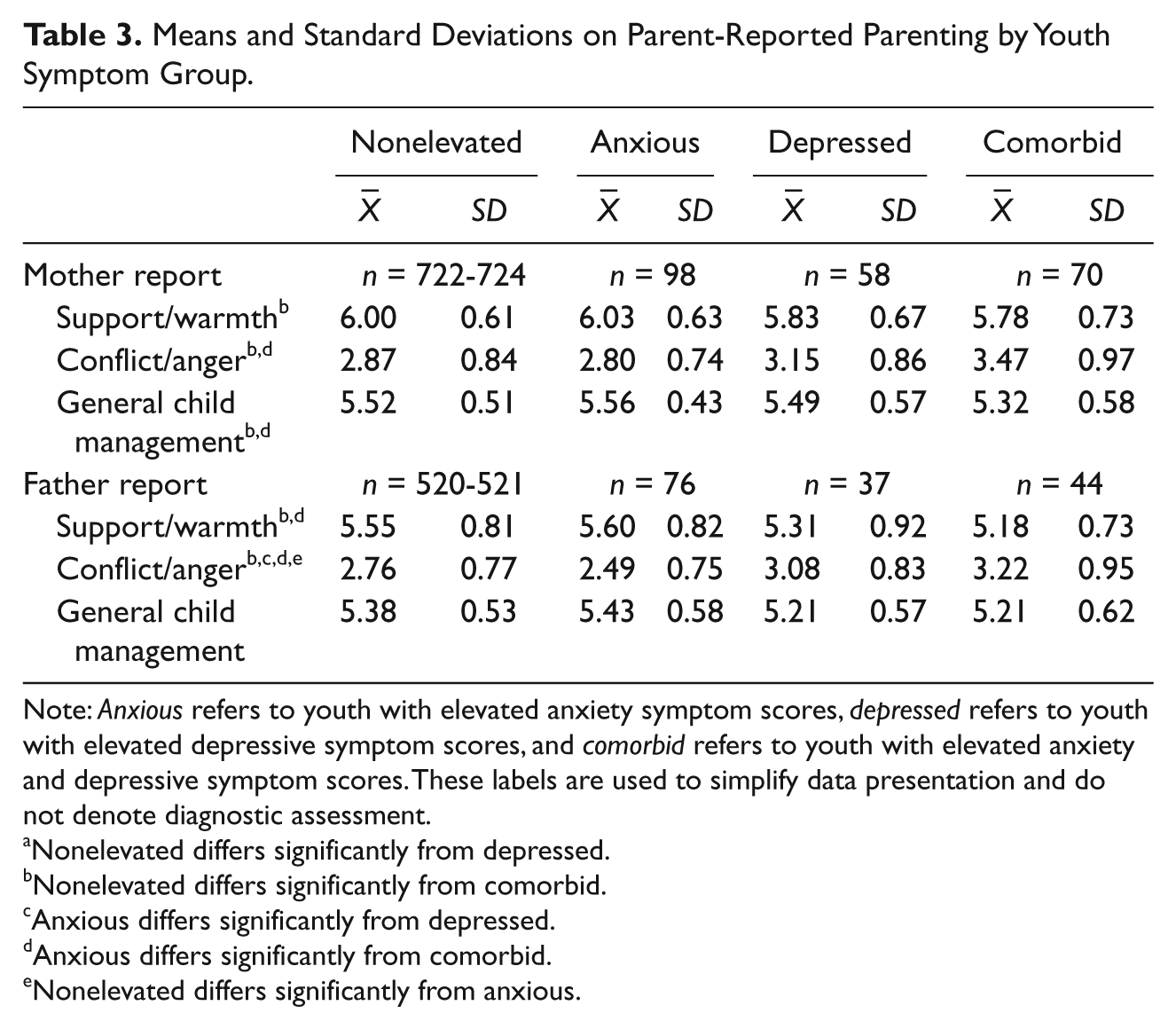
Note: Anxious refers to youth with elevated anxiety symptom scores, depressed refers to youth with elevated depressive symptom scores, and comorbid refers to youth with elevated anxiety and depressive symptom scores. These labels are used to simplify data presentation and do not denote diagnostic assessment.
Nonelevated differs significantly from depressed.
Nonelevated differs significantly from comorbid.
Anxious differs significantly from depressed.
Anxious differs significantly from comorbid.
Nonelevated differs significantly from anxious.
Parenting Characteristics for Nonelevated, Anxious, Depressed, and Comorbid Youth
Youth Report About Mothers
A one-way between-groups MANOVA was performed to examine group differences in youth report of maternal parenting on the dependent variables of support/warmth, conflict/anger, and GCM. There was a statistically significant difference between groups on the combined dependent variables, F(9, 2,847) = 12.90, p = .000; Pillai’s Trace = .12. Further, the results for each of the three dependent variables were significant using a Bonferroni-adjusted alpha level of .017: support/warmth, F(3, 949) = 6.47, p = .000; conflict/anger, F(3, 949) = 39.96, p = .000; and GCM, F(3,949) = 14.11, p = .000.
Scheffe post hoc tests generated using ANOVA revealed that the nonelevated group (
Youth Report About Fathers
MANOVA was used to examine group differences in youth report of paternal parenting on the same three dependent variables: support/warmth, conflict/anger, and GCM. There was a statistically significant difference between groups on the combined dependent variables, F(9, 2,361) = 5.26, p = .000; Pillai’s Trace = .06. Results for each of the dependent variables were significant using the Bonferroni-adjusted alpha level of .017: support/warmth, F(3, 787) = 5.06, p = .002; conflict/anger, F(3, 787) = 14.02, p = .000; and GCM, F(3, 787) = 8.27, p = .000.
Scheffe post hoc tests indicated that the nonelevated group (
Maternal Self-Report of Parenting
A MANOVA testing differences between the groups of youth in their mothers’ self-report of parenting revealed a significant difference on the combined dependent variables, F(9, 2,832) = 4.74, p = .000; Pillai’s Trace = .05. Results for each of the three dependent variables were significant using the Bonferonni-adjusted alpha of .017: support/warmth, F(3, 944) = 4.07, p = .007; conflict/anger, F(3, 944) = 13.10, p = .000; and GCM, F(3, 944) = 3.47, p = .016.
Scheffe post hoc comparisons revealed that mothers of youth in the nonelevated group (
Paternal Self-Report of Parenting
The MANOVA analysis on paternal self-report of parenting also revealed a significant difference on the combined dependent variables, F(9, 2,019) = 3.67, p = .000; Pillai’s Trace = .05. Effects were significant for two of the three dependent variables: support/warmth, F(3, 673) = 3.86, p = .009; and conflict/anger, F(3, 673) = 10.05, p = .000. The F value for GCM did not reach significance per the Bonferonni-adjusted alpha of .017.
Scheffe tests indicated that fathers of youth in the nonelevated (
Internalizing Symptoms of Parents of Nonelevated, Anxious, Depressed, and Comorbid Youth
Means and standard deviations of self-reported maternal and paternal internalizing symptoms, organized by youth symptom group, are provided in Table 4.
Descriptive Statistics for Parent Internalizing Symptoms by Youth Symptom Group.
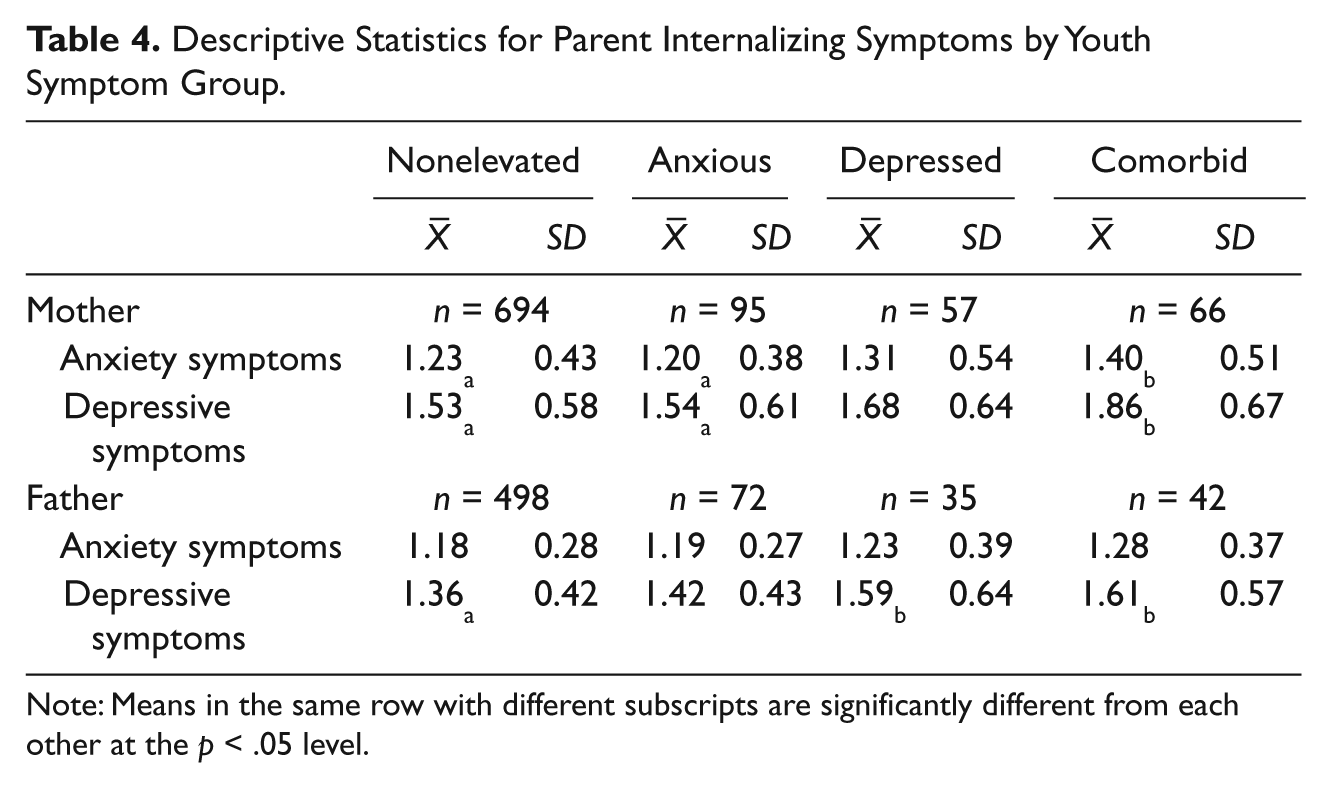
Note: Means in the same row with different subscripts are significantly different from each other at the p < .05 level.
Maternal Internalizing Symptoms
The MANOVA analysis on maternal self-reported internalizing symptoms indicated a significant difference on the combined dependent variables (anxiety and depressive symptoms), F(6, 1,816) = 5.12, p = .000; Pillai’s Trace = .03. Results were significant for both types of symptoms using the Bonferonni-adjusted alpha of .025: anxiety, F(3, 908) = 6.66, p = .000; and depressive symptoms, F(3, 908) = 9.60, p = .000.
According to Scheffe post hoc comparisons, mothers of youth in the nonelevated (
Paternal Internalizing Symptoms
The MANOVA analysis of paternal self-reported internalizing symptoms also indicated a significant difference on the combined dependent variables (anxiety and depressive symptoms), F(6, 1,286) = 4.24, p = .000; Pillai’s Trace = .04. Further examination revealed that results were significant for depressive but not anxiety symptoms using the Bonferonni-adjusted alpha of .025: F(3, 643) = 7.26, p = .000. Scheffe post hoc tests revealed that fathers of youth in the nonelevated group (
Discussion
The overall picture emerging from this community-based study of randomly selected early adolescents is that the depressed and comorbid groups were associated with significantly lower parenting quality and higher parent psychopathology compared to the nonelevated and anxious groups. Generally speaking, this picture is corroborated both by reports from youth about both parents, as well as by independent reports by mothers and fathers.
This study is unique from previous reports as it combines the following characteristics: (a) inclusion of youth, mother, and father reports; (b) a sample of young adolescents only; (c) a community rather than a clinical sample; and (d) examination of anxious- and depressed-only symptom profiles in comparison to a comorbid symptom profile. Many studies have included youth report only, with few assessing fathers’ perspectives even if mother report is included. Further, some studies have aggregated children and adolescents in analyses; given the distinctive nature of the early adolescent developmental period (e.g., the physical, emotional, and social changes related to puberty; increasing complexity of relationships) and the established finding that internalizing symptoms increase during this time, it is important to assess youth experiencing this developmental stage apart from younger and older youth (Hughes & Gullone, 2008; Rudolph, Flynn, & Abaied, 2008). As mentioned previously, most studies of adolescent internalizing and parenting involved assessment of only depressive or anxiety symptoms, the combination of these symptoms, or separate assessment of both types of symptoms without accounting for comorbidity (i.e., without comparing youth with only one type of symptom to those with both types). However, by separating youth with only anxiety or only depressive symptoms from those with both, we found that elevated depressive symptoms, whether in the presence of elevated anxiety or not, are significantly related to certain parenting variables. Conversely, anxiety symptoms were only significantly related to these parenting variables when in the presence of elevated depressive symptoms. Therefore, depressive symptoms appear to be the driving force in the association between internalizing and parenting for this sample of adolescents.
The one study reviewed that used the same four symptom categories as those in the present study (Stark et al., 1990) involved a small sample (n = 51) of youth across four grades that were selected as a result of diagnostic interviews. Whereas Stark et al. (1990) found that youth in the three diagnostic categories reported more conflict and less support than control youth, they also found some differences between comorbid and anxious youth; namely, comorbid youth reported more conflict and lower “democratic family style” compared to anxious youth. Thus, while that study’s findings do not mirror those of the current study, there appears to have been some evidence for poorer parenting quality among youth with depressive symptoms compared to those with anxiety symptoms only. The differences between the Stark et al. (1990) study and the present study may be attributable to differences between youth with clinical diagnoses versus youth categorized on the basis of elevated symptoms.
This study’s results are consistent with previous findings that adolescent depressive symptoms are associated with lower parent support, warmth, and GCM; to higher conflict with and negative affect displayed by parents; and to parent internalizing symptoms. It is theorized that parent support, warmth, and GCM (fair and consistent discipline, monitoring, and use of democratic parenting) help to protect youth by bolstering their self-efficacy, self-esteem, self-regulatory skills, and cognitive and social competence (e.g., Bearman & Stice, 2008; Steinberg, 2001). Without these protective parenting factors, youth are more vulnerable to distress, particularly in the context of frequent or high-intensity conflict and parent negative affect which can harm relationship bonds and leave youth lacking models for effective emotion regulation (Kim et al., 2001; Laursen & Collins, 1994). Results of this study differ from those that show significant relationships between these parenting factors and adolescent anxiety. These findings suggest that depressive symptoms may account for such relationships if both types of symptoms are not assessed or if comorbidity between them is not considered.
These results provide partial support for the first two hypotheses, that parenting quality would be higher for nonelevated (N) compared to anxious only (A) and depressed only (D) groups, and that parenting quality for those with only one type of symptom elevation would be higher than for those in the comorbid (C) group (i.e., N > A, D > C). The general pattern was one of higher parenting quality associated with nonelevated and anxious youth compared to depressed and comorbid youth (i.e., N, A > D, C). So, the findings that nonelevated youth were associated with higher quality parenting than depressed and comorbid youth and that anxious youth were associated with higher quality parenting than comorbid youth are consistent with hypotheses. The findings that nonelevated youth did not differ from anxious youth and that depressed youth did not differ from comorbid youth were unexpected. Thus, while we predicted differences in parenting quality based on the amount of symptoms present (none vs. one type vs. two types), we found that it was the type of symptoms present that distinguished groups of youth on parenting quality (presence vs. absence of depressive symptoms).
As noted earlier, only one finding was inconsistent with the overall pattern: fathers of anxious youth reported significantly less conflict/anger with their adolescents than did fathers of nonelevated youth. It may be that anxious youth are sensitive to or fearful of conflict and make efforts to avoid it with their fathers to the extent that father-adolescent conflict is actually lower for this group compared to nonsymptomatic youth. Given the relative paucity of research including fathers’ perspectives, this finding warrants further investigation.
Although there was substantial concordance for parenting findings for mothers and fathers, a few differences were found. For youth report of parenting there were two more significant group contrasts for youth report about mothers (10 total) compared to youth report about fathers (8 total), with one in the domain of support/warmth and the other in GCM. This may indicate that maternal parenting is slightly more salient than paternal parenting with respect to youth depressive symptoms. With respect to parent-reported parenting, patterns of significance were similar for support/warmth and, although there were somewhat more significant contrasts for fathers vs. mothers on conflict/anger, the patterns of means were quite similar (see Table 3). Finally, there were two significant contrasts for mother-reported GCM and none for fathers. As women often are still the primary caregivers and managers of their adolescents’ everyday activities, it may be that maternal GCM is more relevant to youth outcomes. This interpretation is speculative and awaits further research on the differential impact of relationships with mothers and fathers.
The third hypothesis predicted that youth with symptoms would have parents who reported significantly more symptoms than the parents of youth with no symptoms. This prediction was supported by findings that mothers of comorbid youth reported higher anxiety and depressive symptoms than mothers of nonelevated and anxious youth and that fathers of depressed and comorbid youth reported higher depressive symptoms than fathers of nonelevated youth. As with parenting characteristics, these results follow the general pattern of nonelevated and anxious youth having more similar experiences with their parents compared to depressed and comorbid youth. As noted earlier, there are several potential mechanisms through which parent symptoms may contribute to youth symptoms: genetics; parenting behaviors; stressful conditions associated with parent symptoms, such as marital conflict; and modeling of maladaptive parent behaviors such as ineffective emotion regulation. The testing of such mechanisms is beyond the scope of the current study.
Distinctions Between Anxious and Depressed/Comorbid Youth
The pattern of results that anxious youth report similar parenting qualities as nonelevated youth is notable, especially considering that much previous work has found that parenting plays a role in youth anxiety. As noted above, previous reports usually have not accounted for the presence of depression when assessing the relationship between anxiety and parenting and thus such findings may be confounded by comorbidity. Further, much of the research on parenting and youth anxiety has been with children or with children and adolescents combined; it may be that parenting plays a more prominent role in childhood (i.e., earlier onset) anxiety, and that adolescent anxiety may be more influenced by factors outside the family, such as peer relationships and school transitions (Starr & Davila, 2008).
An explanation for the difference between anxious and depressed/comorbid youth may lie in the tripartite model of anxiety and depression (Anderson & Hope, 2008; Clark & Watson, 1991). As described earlier, this model specifies that while negative affect (NA) is a general risk factor for symptoms of internalizing disorders, (low) positive affect (PA) is a risk factor unique to depression and that generalized anxiety alone may not be related to low PA. It is possible that youth with low PA and high NA (more likely to be depressed), compared to youth with high NA only (more likely to be anxious), elicit more conflictual and less supportive behaviors from parents. Reciprocally, it is possible that parenting marked by low support/warmth and high conflict/anger contribute both to low youth PA and youth depression. Further longitudinal research is needed, however, to study the interactive nature of these pathways between youth characteristics and parenting.
Differential symptom presentations between anxious and depressed youth may also help explain why depressed and comorbid youth are associated with more negative parenting compared to anxious youth. For children and adolescents experiencing depressive symptoms the predominant mood disturbance may be irritability rather than sadness or anhedonia (American Psychiatric Association, 1994). Such irritability may negatively impact the parent-youth relationship such that the parent exhibits less warmth and interactions are more conflictual.
Finally, it cannot be ruled out that there is something unique to the sample assessed for this study that led to the findings; this possibility seems unlikely considering the large size of the sample, but future research could address this issue by conducting similar analyses with different samples. It is also possible that the current findings reflect limitations in the measure of anxiety used; however, the items have high face validity for generalized anxiety and an acceptable coefficient alpha.
Limitations
Limitations of the current study that speak to future directions include the cross-sectional nature of the data, the reliance on self-report (as opposed to observation or diagnostic interviews), and the predominantly White middle-class sample. Further, while participants were randomly selected, there was some evidence that families who participated were somewhat higher functioning than those who chose not to. Therefore, generalizability of these results is limited to similar populations of families. We acknowledge that self-report bias may influence results to the extent that youth with elevated symptoms perceive their relationships in a more negative light than youth without such elevations; however, the corroboration of findings by independent reports of parenting by mothers and fathers strengthens our confidence in the pattern of results that emerged.
Implications
Despite these limitations, this study presents several important implications for research and intervention with youth. First, it underscores the importance of controlling for comorbidity when examining relations between symptoms and parenting. In studies where comorbidity was not considered, it appeared as though anxiety and depression were both related to lower support and higher conflict. Findings here suggest that only depressive symptoms may be related to these variables for young adolescents. While it remains unclear why this is the case, results emphasize the need to isolate empirically the correlates of different types of symptoms. Second, regarding intervention, this study adds to the evidence indicating the importance of addressing relationships with parents when treating youth with depressive symptoms, specifically regarding dimensions of support, conflict, and GCM. Likewise, an emphasis on such factors may be useful in attempts to prevent depression in youth.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Jochebed Gayles for statistical consultation regarding analyses conducted for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute on Drug Abuse, 2 R01 DA13709-06A1.