
Abstract
Developmental shifts during early adolescence relate to type 1 diabetes (T1D) self-management, increased risk of emotional distress, and worsening health status. Less is known about positive experiences related to T1D. This study evaluated associations of positive well-being (PWB) with diabetes burden, self-management, and glycemic control. Youth (N = 55, age = 12-13 years;
Early adolescence is a period during which physiological, emotional, and social changes occur, including puberty, increasing independence, changes in family relationships, and growing risk of internalizing symptoms (Steinberg & Morris, 2001). Given the multiple changes and transitions in early adolescence, this is a vulnerable developmental period. Thus, traditionally, research has focused on identifying risk factors for poor outcomes. Yet, many youth do well, and recently there has been a surge in research focused on resilience and related processes (Masten & Monn, 2015). Resilience is commonly defined as achieving “good outcomes in spite of serious threats to adaptation or development” (Masten, 2001, p. 228). This increased focus on resilience extends to work with children and adolescents with chronic health conditions (Hilliard, McQuaid, Nabors, & Hood, 2015), who are noted to be at risk of poor behavioral, mental health, and health outcomes (Turkel & Pao, 2007).
Type 1 Diabetes (T1D)
T1D is a chronic health condition in which the pancreas produces little or no insulin, a vital hormone that allows glucose (sugar) to enter the cells and be used for energy (Chase & Maahs, 2012). T1D is the most common type of diabetes in youth, with an estimated 15,600 youth in the United States diagnosed each year (Haller, 2013). T1D requires constant self-management and adherence to a complex daily treatment regimen, including frequent monitoring of blood glucose levels, food intake, and insulin calculation and administration (Chase & Maahs, 2012; Haller, 2013). Blood glucose levels are unpredictable and can be difficult to manage, and there are risks of short-term adverse events as well as long-term health complications (Haller, 2013).
Roles and responsibilities for T1D management shift from childhood through adolescence, with caregivers typically managing T1D for infants and younger children, and youth gaining greater autonomy in later childhood through adolescence. During this time period, parents often adopt more of a monitoring role, as opposed to being the sole or primary diabetes managers as is more typical in earlier childhood (Markowitz, Garvey, & Laffel, 2015). T1D regimen adherence and glycemic control often begin to decline during early adolescence, due to a combination of factors including typical developmental changes (e.g., hormonal and body changes, increased academic responsibilities, desire for autonomy) and T1D-specific changes (e.g., increased insulin needs due to the onset of puberty and associated insulin resistance, greater difficulty managing blood glucose levels, weight and body image concerns, and decreased parental involvement in T1D management; Amiel, Sherwin, Simonson, Lauritano, & Tamborlane, 1986; Chiang, Kirkman, Laffel, & Peters, 2014). Youth may experience challenges related to diet and meal planning, as their school, activity, and social schedules often become more variable and they may have more responsibility for food choices away from home (Higgins & Zacharatos, 2013). Shifts in family T1D management responsibilities can co-occur with more diabetes-related conflict and difficulties in self-management (Hilliard et al., 2013a). Emotional changes also accompany early adolescence and can affect diabetes outcomes (Hood et al., 2014).
T1D is for the most part a self-managed condition and often caregivers assume youth are more capable of managing T1D than they are, based on ongoing development in cognitive functioning and self-management skills (Funnell & Siminerio, 2013). Throughout childhood and adolescence, positive T1D outcomes are more likely among those with parental involvement in tasks, low diabetes-specific family conflict, and less diabetes-related distress (Wysocki et al., 2009). Given the deteriorations in T1D management and outcomes that are common across adolescence, it is necessary to understand the period directly beforehand, early adolescence, as this may be an ideal time to identify and target factors that may set the stage for future outcomes.
“Diabetes resilience” has been defined as the achievement of good quality of life, high treatment adherence, and in-range glycemic control despite the challenges of living with T1D (Hilliard, Harris, Weissberg-Benchell, 2012). Behavioral research in T1D has begun to focus on resilience and protective processes that predict these positive outcomes (Hilliard et al., 2012; Yi-Frazier et al., 2015). For instance, Monaghan, Clary, Stern, Hilliard, and Streisand (2015) described associations between protective factors and T1D outcomes in young children (age 2-5 years), including better child quality of life, fewer parental depression symptoms, and less parenting stress. They reported similar levels of protective factors as in other samples of children without T1D, suggesting that despite having diabetes, young children with T1D may not inherently be at a disadvantage compared with peers without chronic illness. In school-age youth (age 10-16 years) with T1D, Van Allen and colleagues (2015) reported that hope and optimism were related to T1D clinical outcomes, and that the relation between hope and glycemic control was mediated by blood glucose monitoring frequency. Rohan and colleagues (2015) also sought to identify factors related to resilient T1D outcomes in youth (ages 9-11 years) over a period of 3 years. They found that more frequent blood glucose monitoring, better self-management, and lower levels of diabetes-related family distress were related to resilient health outcomes, defined in this study as glycemic control within the target range of the American Diabetes Association (ADA; A1c < 7.5%). These studies lay important groundwork for the study of resilience and protection in youth with T1D. As the prevalence of chronic health conditions among children grows (Van Cleave, Gortmaker, & Perrin, 2010), continued attention to the processes that promote good outcomes despite risk is increasingly relevant to promote well-being in youth with a variety of complex chronic conditions.
Positive Well-Being (PWB) and T1D
PWB is one aspect of emotional functioning that has received limited attention in pediatric diabetes research, yet may be related to diabetes resilience. Increased focus on PWB is consistent with the recommendations of the Centers for Disease Control and Prevention’s (CDC, n.d.) Healthy People 2020, which emphasizes the importance of both quality of life and well-being. It states that well-being encompasses “positive emotions and moods (e.g., contentment, happiness), the absence of negative emotions (e.g., depression, anxiety), satisfaction with life, fulfillment and positive functioning.” Increased focus on PWB also aligns with the World Health Organization’s (WHO) definition of health as “a complete state of physical, mental and social well-being, and not merely the absence of disease or infirmity” (WHO, 1948, p. 100), and with their recent definition of mental health as one’s capacity to “cope with the normal stresses of life, . . . work productively and fruitfully, and . . . make a contribution to her or his community” (WHO, 2014, p. 12). In addition, the Diabetes Attitudes, Wishes, and Needs (DAWN) summit highlighted that psychological care in diabetes management was lacking and called for equal emphasis to be placed on “psychological, social and physical factors in diabetes management” (DAWN Summit, 2004). The DAWN study group suggested the use of the World Health Organization–Five Well-Being Index (WHO-5), a measure of PWB, as a standard questionnaire to assess such factors in diabetes care (DAWN Summit, 2004).
PWB has only begun to be researched in youth with diabetes. In research with older adolescents (ages 13-17) with T1D, de Wit and colleagues (2007) found that higher WHO-5 scores were associated with lower depressive symptoms, less diabetes-specific family conflict, and higher self-esteem, but not with glycemic control (a measure of overall diabetes-related health status). No significant relations were found with other demographic (i.e., sex, age, ethnicity, family structure) or medical (i.e., diabetes duration, treatment regimen, body mass index) characteristics. These findings suggest that PWB may be related to emotional experiences of adolescents with T1D and that this construct appears to be stable across various factors that are less directly related to behavioral functioning. Although this is informative about older adolescents, little is known about PWB in the vulnerable early adolescent years.
Although T1D has unique characteristics from other medical conditions, its chronicity, self-management demands, and relations with emotional health are relevant to other pediatric chronic health conditions (e.g., asthma). Moreover, although the specific treatment tasks differ, during early adolescence, youth with and without chronic conditions experience shifts in independence and are expected to take more responsibility for health care behaviors such as diet (Ensaff et al., 2015) and physical activity (Kumar, Robinson, & Till, 2015). Thus, lessons learned about PWB in relation to health among youth with T1D in early adolescence may be helpful for all youth, and could inform assessment and intervention efforts in primary and specialty care to promote optimal health and well-being during this important period of developmental transition.
Study Aim and Hypotheses
The aim of this study was to characterize PWB and its relations to psychological (i.e., depressive symptoms, diabetes-specific burden) and clinical (i.e., T1D adherence, glycemic control) characteristics among early adolescent youth with T1D. It was hypothesized as follows:
Method
Participants
Participants were youth and their caregivers recruited for a prospective study of diabetes strengths and resilience in late childhood and early adolescence. Participants were recruited from the diabetes care center of a large tertiary medical center serving the southern United States. Eligibility criteria for the larger study included youth ages 9 to 13 years, youth and parent fluency in English, diagnosis of T1D (according to ADA criteria) for at least 6 months prior to enrollment, and receiving T1D care at the diabetes clinic where recruitment took place. Participants were excluded from the study if they had a major medical condition, developmental delay, or cognitive impairment, which would affect study participation, or if they had participated in any intervention research within 3 months prior to enrolling in the current study. Informational letters were mailed to 232 families of potential participants; 36 were unable to be contacted due to inaccurate mailing addresses, canceled/missed clinic appointments, or transferring care to a different hospital location. Of the 196 families approached in person for participation in the study, six (3.1%) were deemed ineligible due to comorbid medical/cognitive condition, six (3.1%) opted out of learning about the study, and nine (4.6%) declined to participate due to time or no interest in research. This resulted in 175 (89.3%) participants who consented, enrolled, and provided baseline data. Secondary data analysis for the current study included only individuals ages 12 to 13 years (N = 55) due to the validation age range of the measure of PWB and the emphasis on the point of transition from childhood to adolescence. Participants received a modest monetary sum in appreciation of their participation.
Procedure
Potential participants were mailed an informational letter, which invited families to arrive early to their upcoming scheduled diabetes clinic visit to learn about the study, and included instructions to opt out of being approached about the study if desired. They received a phone call reminder prior to the clinic visit, and then were approached in the waiting room prior to the clinic visit for informed consent, enrollment, and data collection. The study from which these data were drawn included two study visits, which occurred at the time of two consecutive diabetes clinic appointments approximately three months apart. The secondary data analysis reported here used only data from the baseline study visit of participants ages 12 to 13. The Institutional Review Board of Baylor College of Medicine approved this study.
Measures
Demographic information
Caregivers reported on youth race/ethnicity, number of caregivers in the home, and type of insurance (private, public, or none). Age and sex of the child, length of time since T1D diagnosis (T1D duration), and current insulin regimen were collected through electronic medical chart review. For the majority of participants, insulin regimens included either injections (n = 31) or a subcutaneous insulin pump (n = 21) in which a base level of insulin is administered throughout the day and boluses of insulin are administered as needed at mealtimes and to treat high blood glucose values.
PWB
Youth completed the WHO-5, the measure of PWB recommended by the DAWN study group (DAWN Summit, 2004). This measure was validated for youth in a study of adolescents with T1D (ages 13-17 years) and demonstrated good internal consistency, α = .82 (de Wit et al., 2007). The readability of the measure has been confirmed with a Flesch Reading Ease score of 90.0, at approximately a fifth-grade reading level (de Wit et al., 2007), thus it was deemed reasonable to administer to youth ages 12 to 13 years in this exploratory study designed to learn more about PWB in early adolescents. In this sample, the internal consistency was good, α = .80. Participants rated the frequency of positive emotional states experienced over the past 2 weeks on a 6-point Likert-type scale. Scores for all answered items were averaged and multiplied by five to calculate the raw total, which was then multiplied by four, resulting in a 0 to 100 scale for the adjusted total score (higher scores were indicative of greater levels of well-being; WHO, 1998). The WHO-5 was included as part of the Monitoring Individual Needs in Diabetes Youth Questionnaire (MY-Q; de Wit et al., 2012); if three or fewer MY-Q items were missing, mean replacement was used, and if four or more items were missing, the measure was not scored.
Depressive symptoms
Youth completed the Children’s Depression Inventory–Short Version (CDI-S), a 12-item self-report measure of depressive symptoms with strong psychometric properties based on a sample of youth ages 7 to 17 years (Kovacs, 2011). In this sample, the internal consistency was adequate, α = .73. Higher scores indicated a greater number of depressive symptoms over the past 2 weeks. Depressive symptoms were evaluated both as a continuous score, and categorized using a clinical cutoff t score of 60. T scores below 60 represented a typical or low number of concerns, and scores 60 or above were considered high average, elevated, or very elevated number of concerns. Scores were categorized into below cutoff and at/above cutoff (Kovacs, 2011). If one item was missing, an average of the answered items was calculated and multiplied by the total number of items. CDI-S scores were not calculated if more than one item response was missing.
Diabetes burden
Youth completed the Problem Areas in Diabetes Questionnaire–Teen Version (PAID-T), a 26-item measure of the intensity of distressing experiences related to living with and managing T1D over the past month, with strong psychometric properties based on a study of youth ages 11 to 19 years (Weissberg-Benchell & Antisdel-Lomaglio, 2011). In this sample, the internal consistency was excellent, α = .94. The measure is rated on a 6-point Likert-type scale (scores range from 26 to 156) with higher scores indicating greater levels of distress. If three or fewer responses were missing, mean replacement was used; if four or more items were missing, a total score was not calculated.
Diabetes treatment adherence
Diabetes treatment adherence was assessed via objective and subjective measures. Adherence to one key T1D management behavior (blood glucose monitoring) was assessed objectively via mean daily blood glucose monitoring frequency. The youth’s blood glucose meters were downloaded in clinic. Due to between-person variability on how many days of data were available, readings were averaged across number of days available (up to 14;
Although objective measures are considered ideal for assessing adherence to specific self-management behaviors, subjective measures are also important to measure adherence to the numerous other behaviors in the T1D treatment regimen that cannot be captured through physiological or electronic monitoring data (Gandhi, Bach-Mai, Eshtehardi, Wasserman, & Hilliard, 2015). Thus, caregivers completed the Diabetes Self-Management Questionnaire (DSMQ-P), a nine-item measure of completion of various T1D management tasks, with adequate psychometric properties from a sample of youth ages 9 to 15 years (Markowitz et al., 2011). In this sample, the internal consistency was adequate, α = .65 (consistent with the low number of items of the scale). Scores range from 0 to 35, with higher scores indicative of greater adherence to key diabetes self-management behaviors (Markowitz et al., 2011). The mean score of all answered items was reported.
Glycemic control
Hemoglobin A1c is the standard biomarker of overall glycemic control. It represents the average blood glucose level over the past two to three months, and is a strong predictor of diabetes complications (ADA, 2015). A1c is measured routinely at diabetes clinic visits via a fingerstick blood sample and is documented in the electronic medical record. A1c values from the day of baseline data collection were used in this study. For youth with T1D, the ADA recommends an A1c goal of less than 7.5% (ADA, 2015). Thus, A1c data were analyzed both continuously and categorized as within target range versus above target range.
Data Analyses
Data from the WHO-5, CDI-S, and PAID-T measures in this study were not normally distributed (WHO-5, negatively skewed; CDI-S and PAID-T, positively skewed), thus nonparametric statistical tests (Spearman correlations, Mann–Whitney U tests) were performed. Two separate hierarchical linear regression analyses were conducted to evaluate the relative associations of PWB with the (a) psychological (i.e., depressive symptoms, diabetes burden) and (b) clinical (i.e., adherence, A1c) constructs of interest, respectively, controlling for related covariates in each model. The dependent variable in each regression model was WHO-5 scores. The first step included as independent variables any demographic or medical variables that had significant (p < .05) bivariate associations with PWB, and the second step added as independent variables either the CDI-S and PAID-T scores (Model 1: emotional functioning) or DSMQ-P, blood glucose monitoring frequency, and A1c values (Model 2: diabetes constructs). There were limited missing data in the study (1.8% of data, n = 1, were missing for A1c, type of insulin regimen, and PAID-T; 5.5% of data, n = 3, were missing for blood glucose monitoring frequency), thus mean replacement was used to address missing continuous data, and for the categorical variable, the most frequent response was used (Cheema, 2014). All analyses were performed using SPSS version 22.
Results
Participant Characteristics
Participants were 55 youth (
Associations With the WHO-5—Bivariate Analyses.
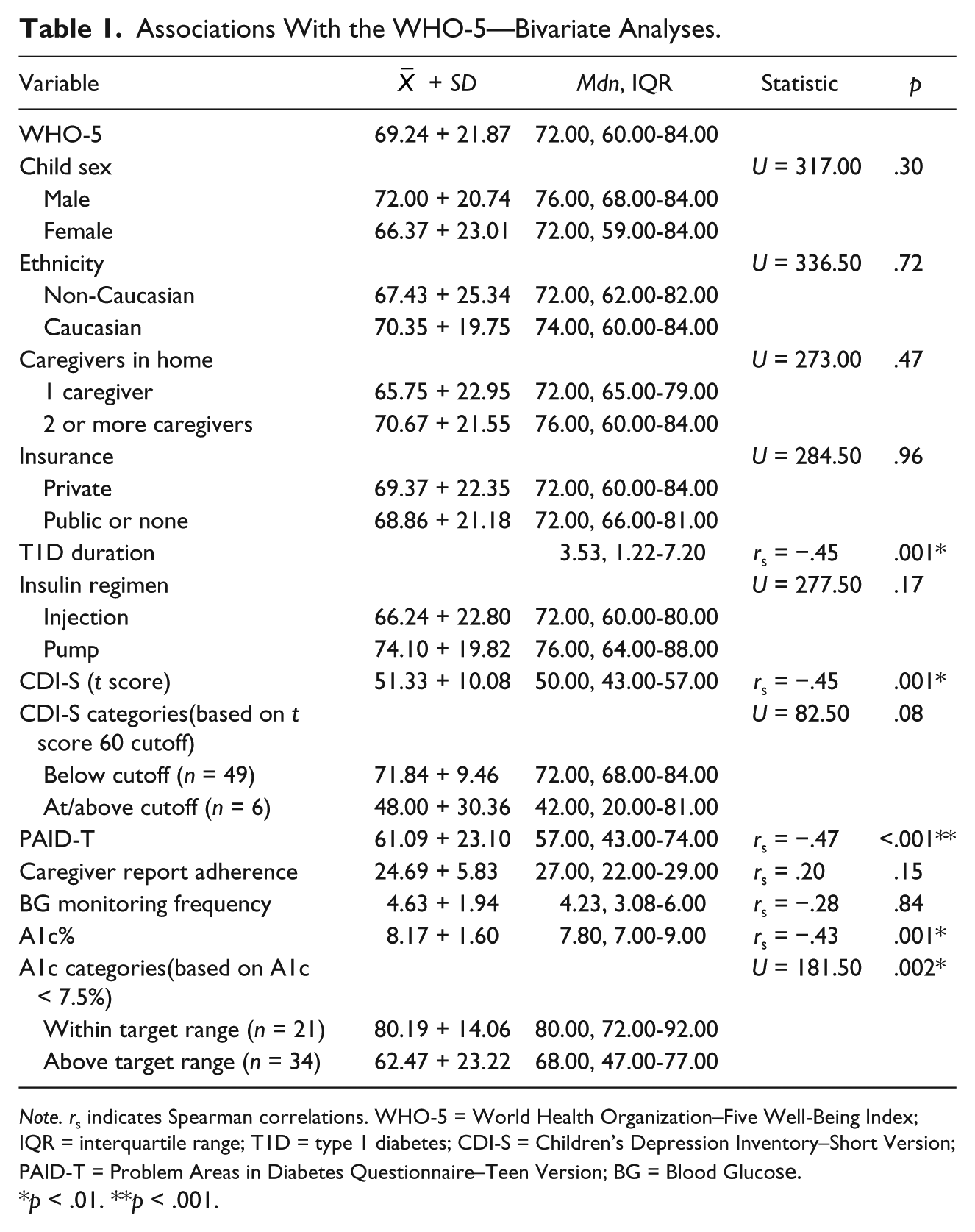
Note. rs indicates Spearman correlations. WHO-5 = World Health Organization–Five Well-Being Index; IQR = interquartile range; T1D = type 1 diabetes; CDI-S = Children’s Depression Inventory–Short Version; PAID-T = Problem Areas in Diabetes Questionnaire–Teen Version; BG = Blood Glucose.
p < .01. **p < .001.
WHO-5 and Participant Characteristics
Youth reported WHO-5 scores ranged from 20 to 100 with a mean score of 69.24 + 21.87 and a median score of 72.00 (interquartile range [IQR] = 60.00-84.00). The only participant characteristic with a significant correlation (p = .001) with higher WHO-5 scores was shorter T1D duration (Table 1), indicating that this variable should be entered as a covariate in subsequent multivariate analyses.
WHO-5 and Emotional Functioning
The mean and median t scores on the CDI-S were within the average range and below the clinical cutoff for elevated scores. There was a significant (p = .001) correlation between higher WHO-5 scores and lower CDI-S scores; however, WHO-5 scores did not significantly differ between youth in the below cutoff group versus those in the at/above cutoff group (Table 1). The mean score on the PAID-T measure of T1D burden was consistent with levels previously reported in adolescents ages 11 to 19 years (Weissberg-Benchell & Antisdel-Lomaglio, 2011). There was a significant relation (p < .001) between higher WHO-5 sores and lower PAID-T. There is no published clinical cutoff for this measure; thus, no categorical comparisons were conducted (Table 1).
A hierarchical linear regression with WHO-5 as the dependent variable and CDI-S and PAID-T as independent variables, controlling for diabetes duration, was significant, F(3, 51) = 11.51, p < .001. In addition to diabetes duration (β = −.39, p = .003), CDI-S scores were significantly associated with WHO-5 scores (β = −.55, p = .001), but PAID-T scores were not (β = .08, p = .64; Table 2). In the full model, CDI-S and PAID-T scores together explained a significant portion of the variance (25%, ΔR2 = .25) in WHO-5 scores, beyond the 15% accounted for by T1D duration, ΔF(2, 51) = 10.84, p < .001 (Table 2).
Hierarchical Linear Regressions With WHO-5 Scores.
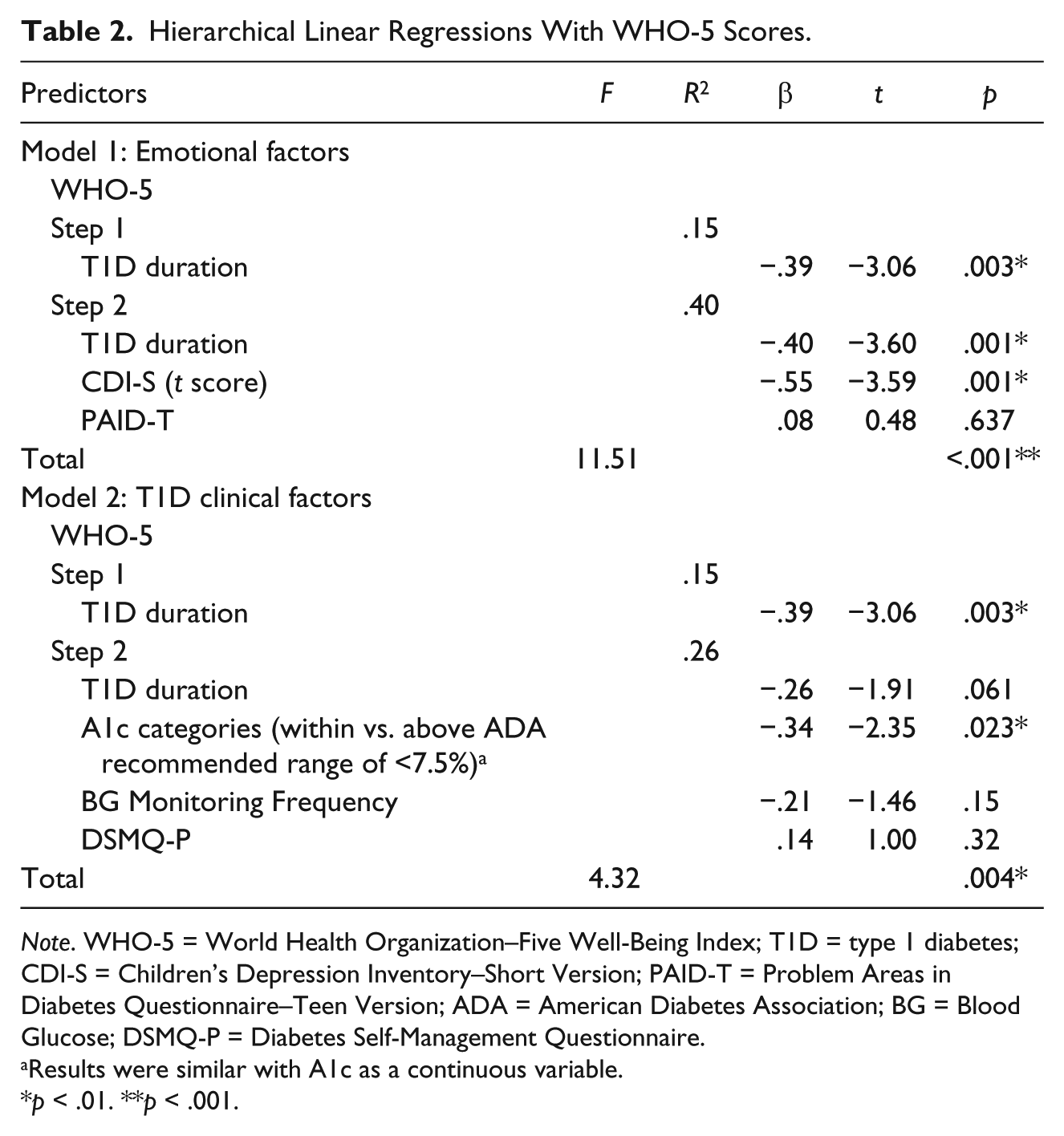
Note. WHO-5 = World Health Organization–Five Well-Being Index; T1D = type 1 diabetes; CDI-S = Children’s Depression Inventory–Short Version; PAID-T = Problem Areas in Diabetes Questionnaire–Teen Version; ADA = American Diabetes Association; BG = Blood Glucose; DSMQ-P = Diabetes Self-Management Questionnaire.
Results were similar with A1c as a continuous variable.
p < .01. **p < .001.
WHO-5, Adherence, and Glycemic Control
WHO-5 scores were not significantly correlated with mean daily blood glucose monitoring frequency (Table 1). However, higher WHO-5 scores were correlated with lower A1c values (p = .001) indicating better glycemic control, and were significantly (p = .002) higher among youth with A1c values within target range compared with those with A1c values above target range (Table 1).
A hierarchical linear regression with WHO-5 scores as the dependent variable and A1c (categorical), blood glucose monitoring frequency, and DSMQ-P as independent variables, controlling for diabetes duration, was significant, F(4, 50) = 4.32, p = .004. In addition to diabetes duration (β = −.39, p = .003), categorical A1c (within vs. above target range) was significantly associated with WHO-5 scores (β = −.34, p = .023), but blood glucose monitoring frequency (β = −.21, p = .15) and DSMQ-P scores were not (β = .14, p = .32; Table 2). In the full model, A1c, blood glucose monitoring frequency, and DSMQ-P scores together did not explain significantly more of the variance (10.7%, ΔR2 = .107) in WHO-5, beyond the 15% accounted for by T1D duration, ΔF(3, 50) = 2.39, p = .80 (Table 2). A regression model using continuous A1c values had nearly identical results.
Discussion
This study examined the relations between PWB and other emotional and clinical diabetes constructs. These initial findings suggest that positive emotional experiences are associated with other key psychological experiences and overall diabetes-related health status during the critical and vulnerable transition from childhood to adolescence. Reported levels of early adolescents’ PWB in this study were consistent with levels reported in the general population (Bech, 2012) and older adolescents with T1D (de Wit et al., 2007). The relatively high PWB reported in this study was also consistent with the 59% of adults with T1D who reported high levels of PWB in the DAWN study (Peyrot et al., 2005). There were no significant associations between PWB and demographic or diabetes-specific clinical characteristics, with the exception of length of time since T1D diagnosis. This is noteworthy, given the challenges of adjustment to a new diagnosis that youth with T1D often experience (Frank, 2005). It may suggest that closer to diagnosis, before diabetes burnout might develop, might be an opportune time to assess PWB, as capitalizing on positive emotions early could foster resilient outcomes later (Hilliard et al., 2012). Given the chronicity of T1D and lower PWB among youth with longer disease duration, this highlights the importance of continued attention to enhancing well-being in the years following diagnosis. Lack of association between other participant characteristics and PWB is consistent with the findings of de Wit and colleagues (2007), and suggests PWB might be consistent across diverse groups. Therefore, any observed differences in PWB are likely not attributable to these demographic or diabetes care characteristics and may reflect meaningful differences based on other factors of interest.
Higher levels of PWB may be advantageous in early adolescence, particularly in terms of other aspects of general emotional health. Youth who reported higher PWB reported lower levels of depressive symptoms, even after controlling for T1D duration, consistent with the reported links with depressive and other mental health symptoms in older adolescents with T1D (de Wit et al., 2007). These findings are further supported by the work of Allgaier and colleagues (2012) who reported on the diagnostic accuracy of the WHO-5 in relation to depression among youth ages 9 to 16 years recruited from pediatric hospitals. Although the WHO-5 is often used in the literature as a proxy measure of depression, there was only a moderate relation between the WHO-5 scores and CDI-S scores in this sample. This significant, yet modest, association suggests that the two constructs (PWB and depressive symptoms) overlap but that the WHO-5 and CDI-S instruments may capture distinct experiences. Further study of these instruments is needed to evaluate whether the WHO-5 may be appropriate for use in clinical practice in this age range, for example, as an initial, universal index of PWB followed if necessary by a more precise measure of depressive symptoms to identify whether depression-oriented intervention is needed. The lack of significant association between PWB and CDI-S scores when analyzed as a dichotomous variable (below cutoff vs. at/above cutoff) may be due to lack of power because of the small number of individuals (n = 6) whose scores were at/above cutoff.
Bivariate associations between higher PWB and lower diabetes burden did not persist when considered in the context of depressive symptoms and T1D duration. This suggests that the initial relation seen may be driven by other, more similar constructs. Specifically, PWB in individuals may be more influenced by general depressive symptoms than feelings of distress or burden specifically related to diabetes. de Wit and colleagues (2007) also found relations between aspects of diabetes distress and PWB, specifically lower PWB was associated with higher diabetes-specific family conflict, another aspect of diabetes distress.
The lack of significant relations between PWB and measures of adherence (subjective and objective measures of specific behaviors and the overall T1D regimen) was surprising, given other evidence linking emotional functioning with adherence in adolescents with T1D (McGrady et al., 2009). This study attempted to decrease the risk of single-rater bias across these constructs by including both subjective (i.e., parent report) and objective (i.e., blood glucose monitoring frequency via meter data) measures of adherence, yet neither revealed significant associations between adherence and PWB. In contrast to previous findings in older adolescents, the null finding in the current sample may reflect that caregivers continue to play a significant role in T1D management during early adolescence (Markowitz et al., 2015). That is, parental oversight of T1D self-management may supersede the impact of youth’s emotional states on adherence and buffer any association between youth’s emotional status and their health behaviors.
Typically, adherence and glycemic control are closely related (Hood et al., 2009); yet, in this study, despite the lack of a significant relation between adherence and PWB, there was a significant relation between PWB and glycemic control, even when controlling for T1D duration. Due to the cross-sectional nature of the data, the directionality or reason for this relation cannot be determined; perhaps better glycemic control leads to individuals feeling better overall, thus reporting higher levels of PWB, or perhaps lower stress in people with higher PWB influences A1c positively. These findings are distinct from those of de Wit and colleagues (2007), who did not find a significant bivariate relation between PWB and glycemic control in older adolescents. This may be due to the many social and behavioral factors that strongly influence glycemic control during the later adolescent years, beyond PWB (Markowitz et al., 2015).
Overall, the psychosocial findings are generally consistent with de Wit and colleagues’ (2007) analysis of PWB in older adolescents with T1D, suggesting this construct may develop in or before early adolescence and persist over the adolescent years. This highlights the potential benefits of early, regular PWB monitoring to build on initial positive experiences and possibly prevent general distress prior to the challenges of adolescence. However, the link with A1c differs in this current sample compared with older adolescents. In addition to the age and developmentally related distinctions described above, other differences (e.g., geographic/institution differences, cohort differences) between the two samples may explain these disparate findings. More research is needed to evaluate how trajectories of PWB relate to trajectories of self-management and health variables across the stages of adolescent development.
Considerations and Limitations
The relatively small convenience sample used in this secondary data analysis was not fully powered to detect associations with PWB. Yet, as the first study to examine the construct of PWB among youth with T1D during early adolescence, this sample size permitted exploratory analyses for hypothesis-generation purposes that can guide future, fully powered studies of this important topic. The demographic characteristics of this sample (61.8% Caucasian, 74.5% private insurance) are important to consider in terms of potential generalizability to other populations. Compared with other behavioral studies of youth with T1D (e.g., Hilliard et al., 2013b; Jaser, Patel, Rothman, Choi, & Whittemore, 2014; Yi-Frazier et al., 2015), this sample is more demographically diverse and, thus, may be more likely to generalize across populations. Due to its cross-sectional design, the directionality of the relations among PWB and psychological, behavioral, and clinical variables cannot be determined. In addition, data on the pubertal status of the participants (e.g., Tanner stage) were not available; in light of known increases in insulin resistance in puberty (Amiel et al., 1986), the potential influence of puberty on glycemic control was not accounted for in this study. It is possible that differences in PWB could have been influenced by whether or not individuals were experiencing difficulties that at times accompany puberty, both specially related to T1D (i.e., increases in insulin resistance) and apart from it (e.g., appearance changes, social changes). There is additionally the risk of recall and social desirability biases, although the study is strengthened by the use of both subjective measures from multiple raters (i.e., validated youth and parent-report instruments) and objective data (i.e., blood glucose meter downloads, glycemic control biomarker). Another limitation of this study is that the internal consistencies for the CDI-S and the DSMQ-P, which are validated measures, were somewhat low, likely due to the measures being abbreviated versions of longer instruments.
Implications for Clinical Practice
This study provides initial indication that PWB may be related to important psychological experiences and glycemic control among young adolescents with T1D. Ultimately, this line of research may support routine screening using the WHO-5 as a brief five-item measure of positive emotional functioning, in combination with targeted measures of psychosocial risks or symptoms. This may help diabetes care providers systematically monitor and discuss changes in emotional status before they elevate to clinically significant levels or affect diabetes outcomes. This aligns with the DAWN guidelines (2004), as well as national and international diabetes organization guidelines to systematically assess and intervene to support psychological and behavioral well-being in youth with T1D (ADA, 2015; Delamater et al., 2014).
The brevity, free access, and availability in many languages of the WHO-5 measure increases its feasibility as a brief screening tool (Topp, Østergaard, Søndergaard, & Bech, 2015). The emphasis on well-being rather than problems or pathology may make this measure a more palatable way to introduce mental health concepts into conversations with youth and their families. This may serve to strengthen the patient–provider relationship as it could communicate the interest of providers in not only medical outcomes but also other aspects of their patients’ lives. A strong patient–provider relationship could be important particularly as youth enter the more tumultuous period of adolescence and beyond (Monaghan, Hilliard, Sweenie, & Riekert, 2013).
The ADA (2015) emphasized the importance of individualizing diabetes treatment plans, and information about PWB could ideally be incorporated into these plans to promote both optimal health and optimal mental health. Integrating a focus on PWB into care for youth with T1D would align with increasing attention to using strengths-based approaches to care (Hilliard et al., 2012). Indeed, Jaser, Patel, Linsky, and Whittemore (2014); Jaser, Patel, Rothman, et al. (2014); Rosenberg and colleagues (2015); and Kichler and Kaugars (2015) have all described intervention strategies that emphasize positive aspects of diabetes management to promote resilient outcomes. The results of this study may help to guide ongoing research for strengths-based, resilience-oriented clinical research and practice to enhance health and well-being during vulnerable developmental periods such as early adolescence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Grant K12 DK097696 from the National Institutes of Health awarded to Barbara J. Anderson.