
Abstract
According to the Learning Theory of Attachment, neuroendocrinological processes affect the association between parental support and change in attachment. The current study aimed to test this assumption for oxytocin (OT) given its role in social behavior. We conducted a three-wave longitudinal study in which 91 children (56% girls, M age = 9.55, SD age = 0.63) participated. Change in attachment was assessed from Wave 1 to Wave 3 and was indexed by measuring trust in maternal support and Secure Base Script (SBS) knowledge. Measures of salivary child OT and parental support (child and mother report) were obtained during respectively the first and last wave. Results indicated that child-reported parental support was positively related to change in trust and more so for children with high OT levels. No (moderation) effects were found for SBS knowledge. Overall, these findings illustrate the importance of considering biological factors along with experienced parenting to explain differences in attachment.
Introduction
According to Bowlby (1969) and Ainsworth’s (1974) attachment theory, the extent to which parents interpret signals of a child’s distress accurately and respond to these appropriately (i.e., parental sensitivity) predicts the quality of children’s attachment to their parents. Specifically, when parents respond consistently supportive to signals of distress of their child, attachment theory predicts that children’s trust in parents’ availability during future distress will increase and a secure attachment relationship will develop. In contrast, a child will have less trust in parents’ availability during distress and develop an insecure attachment relationship when parents are not available or do not provide support during distress. Main (1990) further described insecure patterns of attachment as secondary strategies to cope with insensitive care by maximizing (i.e., insecure-ambivalent or anxious attachment) or minimizing support-seeking behavior (i.e., insecure-avoidant attachment). Both strategies would result from a lack of trust in parental support during distress (Main, 1990). Although research found evidence for the assumption that parental sensitivity and secure attachment are associated, the strength of this association indicates that parental sensitivity explains only part of the variability in attachment quality (De Wolff & van IJzendoorn, 1997; Madigan et al., 2024).
To explain this discrepancy, Bosmans et al. (2020) formulated a Learning Theory of Attachment (LTA) that considers each parent-child interaction after children’s exposure to distress as a learning event (Figure 1). During each learning event, if the parent provides support, stress will be alleviated which is thought to provide the child with a sense of relief and comfort (McQuaid et al., 2016; Sroufe & Waters, 1977). These feelings are accompanied by changes on a neuroendocrinological level such as a decrease in cortisol and an increase in oxytocin (OT; Feldman & Bakermans-Kranenburg, 2017; Hostinar et al., 2015). Across learning events, feelings of relief and comfort are associated with the parent which in turn will lead to increased trust in parental support and eventually to the development of what has been called a Secure Base Script (SBS; Bosmans et al., 2020). Overview of the classical component of the Learning Theory of Attachment.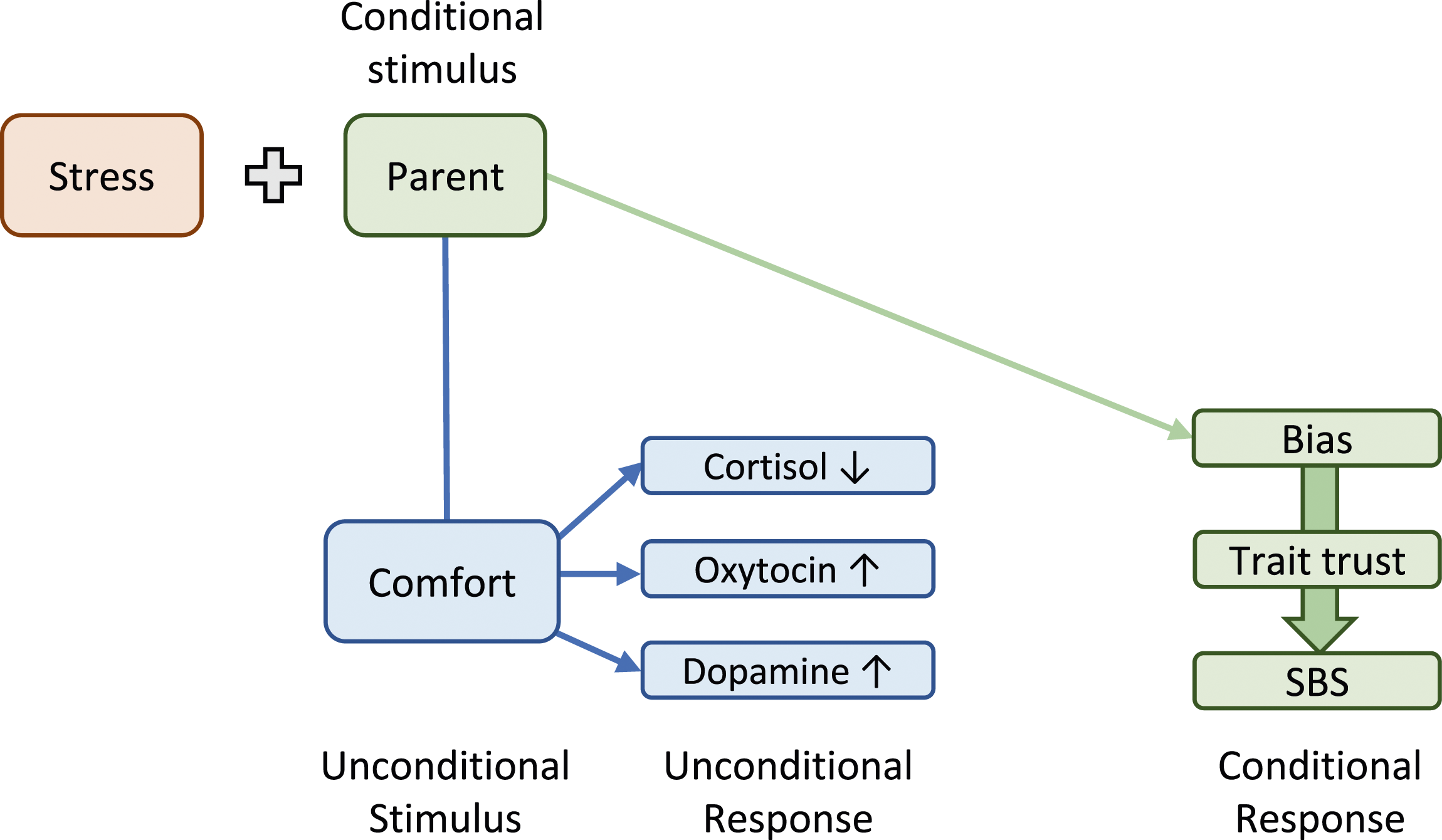
The SBS concept was introduced by Waters and Waters (2006) and refers to a script-like mental representation of children’s history of experiences with a parent’s support during distress (a secure base; Bowlby, 1969). Children with experiences of consistent secure base support develop a SBS which reflects the expectation of receiving support during future distress. Consequently, more securely attached children have more consolidated and easily accessible (implicit) knowledge about their SBS. In contrast, the SBS of children who did not receive consistent secure base support will be less well developed and thus less accessible which results in less (implicit) knowledge about secure base scripts (Waters & Waters, 2006).
In contrast to traditional attachment theory’s canonical view on parenting being the main factor explaining individual differences in attachment development, the LTA proposes that interindividual differences in neuroendocrinological processes involved in attachment development affect the strength of the association between parental support and attachment development over time (Bosmans et al., 2020). These differences stem from inherent genetic variability or from experience-induced alterations in children’s genetic material (e.g., methylation). For instance, single nucleotide polymorphisms (SNPs) in the CD38 gene, which mediates OT secretion, or the OT receptor (OTR) gene have been related to plasma OT levels (Feldman et al., 2012; Jin et al., 2007). In turn, plasma OT levels have been positively related to perceived parental sensitivity (Feldman et al., 2012). Thus, through their genetic makeup, children might be more or less susceptible to developing a secure attachment relationship with their caregiver. Supporting the LTA, Cuyvers et al. (2024) found that change in the oxytocinergic system over time, operationalized by change in OTR methylation, moderated the association between (changes in) parental support and attachment development in middle childhood.
On the neuroendocrinological level, Houbrechts et al. (2021) tested in middle childhood whether children’s cortisol response showed similar moderating effects in the association between supportive parenting and attachment. Specifically, using a two-wave longitudinal design, the researchers assessed whether children’s cortisol stress response moderated the association between parental support and change in attachment over a year. Attachment was operationalized using the Experience in Close Relationships Scale – Revised Child Version (ECR-RC) allowing for simultaneous assessment of anxious and avoidant attachment (Brenning et al., 2011). Children reported on parental support as well as attachment. Results showed that parental support was negatively associated with change in anxious attachment but more so for children with a weaker cortisol stress response even though no association between baseline attachment (at Wave 1) and child cortisol stress levels were found. In light of the LTA, a possible interpretation of this finding is that children with a strong cortisol response during distress remain stressed even after parental support, which would affect their ability to learn from this interaction (Houbrechts et al., 2021). This raises the question whether other neuroendocrinological processes relevant for attachment development show similar moderating effects in the relationship between parental support and secure attachment development.
Next to the cortisol system (Houbrechts et al., 2021), other plausible candidates are the dopamine (Bosmans et al., 2020) and the OT system. Feldman (2017) proposed a central role for the OT system in the neurobiology of parent-child attachment, based on studies that found that OT is essential for the formation and maintenance of mammalian attachment bonds (Feldman & Bakermans-Kranenburg, 2017; Yamamoto et al., 2019). For instance, in non-human mammalian species, OT facilitates the onset of maternal behavior and in humans, higher OT levels have been related to more positive parenting behavior such as affectionate touch in mothers and stimulatory contact in fathers (Inada, 2024; Naber et al., 2010; Shorey et al., 2023). Importantly, OT also affects how parenting behavior is perceived in humans as evidenced by the positive association between OT levels and perceived parental sensitivity (Feldman et al., 2012). Together, these findings suggest that OT is an important component within the neuroendocrine milieu relevant for attachment development by affecting both the onset and the perception of caregiving. The current study focused on individual differences in children’s OT response by investigating whether it may moderate the association between supportive parenting and secure attachment.
OT is a hypothalamic neuropeptide that is involved in a plethora of physiological processes such as inducing labor and stimulating lactation (Shyken & Petrie, 1995; Uvnäs-Moberg et al., 2020). Next to its possible role in attachment development, it has also been shown to affect social functioning more broadly (Rigney et al., 2022; Walsh et al., 2023). Of relevance for the LTA is the release of OT during the experience of parental support (Feldman & Bakermans-Kranenburg, 2017) and its positive association with trust (for review see van IJzendoorn & Bakermans-Kranenburg, 2012). Additionally, OT has also been shown to enhance the experience of secure attachment (Bernaerts et al., 2017; Buchheim et al., 2009). Furthermore, research shows that OT is released during stress (Dief et al., 2018; Love, 2018). According to Tops et al. (2013), increased endogenous levels of OT during (anticipatory) stress (i.e., in their study, arrival at experimental setting) reflect an active coping response to promote familiarization and accommodate to stress. This is consistent with research that found that OT motivated social support seeking specifically when participants reported distress (Cardoso et al., 2013).
Next to OT’s ameliorative effects on anxiogenic aspects of social behavior, research showed that OT can also increase antisocial behavior such as non-cooperation and aggression (for meta-analysis see Bakermans-Kranenburg & van IJzendoorn, 2013). To explain these contradictory findings, Shamay-Tsoory and Abu-Akel (2016) formulated the social salience hypothesis of OT. This hypothesis states that OT increases the salience of social cues by orienting attention. As such, the social salience hypothesis of OT can explain why OT would increase trust in a supportive context (because OT would orient attention towards safety) and non-cooperation in a threatening context (because OT would orient attention towards threat). Regarding attachment development, these findings could indicate that variations in the OT response during stressful situations could reflect children’s ability to cope with stress by variance in the motivation to seek parental support. Additionally, by increasing the salience of parental support, OT could make children more susceptible to benefit from it. This in turn would have implications for the development of secure attachment.
In the current study, we therefore investigated whether the OT response to anticipatory stress in the presence of the mother moderated the relationship between parental support and change in secure attachment in middle childhood. Although middle childhood is typically regarded as a period of stability in children’s psychosocial development including attachment development, results of research on attachment stability in middle childhood challenge this idea (Kerns & Brumariu, 2016; Waters, Facompré, Van de Walle, et al., 2019). Specifically, changes in attachment in middle childhood can be the result of major disruptions in children’s caregiving environment (i.e., lawful discontinuity; Bowlby, 1969) but can also occur due to the continued exposure of children to attachment learning events resulting in the development of more elaborate knowledge about the SBS (Kerns & Brumariu, 2016; Waters, Facompré, Van de Walle, et al., 2019). Together, these results suggest that middle childhood is a very relevant developmental phase to study changes in attachment.
Extending the work of Houbrechts et al. (2021), we used a multi-informant design with both children and their mothers reporting on parental support while attachment was operationalized with self-reported trust in maternal support (referred to as Trust below) and a narrative procedure to assess SBS knowledge. We assessed the quality of children’s attachment relationship with their mother because research shows that mothers remain the primary attachment figures in middle childhood, even though children’s social world starts to expand through the development of relationships with, for example, peers (Bosmans & Kerns, 2015; Seibert & Kerns, 2009).
We used a three-wave longitudinal design spanning one year to measure change in Trust and SBS knowledge from Wave 1 (W1) to Wave 3 (W3) to ensure sufficient time for development of attachment to occur (Houbrechts et al., 2021). At W1, similarly to Tops et al. (2013), we obtained a measure of the OT response to anticipatory stress in the presence of the mother by collecting saliva samples upon arrival of the participating children and their mothers at the experimental setting. At W3, we also measured parental support. We hypothesized that parental support at W3 would be positively associated with change in both Trust and SBS knowledge but more so for children with a stronger OT response to anticipatory stress in the presence of the mother since these children might benefit more from parental support than children with a weaker OT response to anticipatory stress in the presence of the mother.
Methods
Participants
The sample in the current study was a community subsample of a broader longitudinal research project in which 118 children were recruited from various elementary schools (4th and 5th grade) in Flanders, Belgium. From this sample, we retained 91 participants with at least one valid OT measurement and one valid measurement in other variables of interest for the current study. We conducted a power analysis using G*Power to assess whether this sample size was sufficiently large to pick up increases in the amount of explained variance (R2) when adding an interaction to our models. Given that we planned to test four interactions effects, alpha was Bonferroni-adjusted (α = .0125). This analysis revealed that we could detect increases in R2 due to moderate to large effects (f2 ≥ .13) with a power of .80, based on field-specific benchmarks (Schuengel et al., 2021). Missing data was imputed and, apart from the calculation of sample characteristics and Cronbach’s α, all analyses were conducted on this imputed dataset (see details below).
In our sample, 51 children were girls (56%) and 34 children were boys (37.4%) while data on sex was missing for 6 children (6.6%). They were between 9 and 11 years old (M = 9.55, SD = 0.63). Regarding nationality, 76 children were Belgian (83.5%), 8 had other nationalities (8.8%) and data on nationality was missing for 7 (7.7%). Furthermore, 59 children lived in their original family (64.8%), 14 lived in newly composed families after divorce (15.4%), 9 lived in one-parent families (9.8%), 1 lived in yet another family structure without further specification (1.1%) while information was missing for 8 children (8.8%). Of the 23 children living in newly composed or one-parent families, 9 stayed with their mother alone or lived together with her in a newly composed family (34.8%) while the other 14 alternated between living with mother and father (65.2%). Mother was the primary caregiver during the first three years of life for 82 children (90.1%) while one child was primarily being raised by the father in this period (1.1%) and for 8 children information was missing (8.8%). Regarding maternal level of education, 21 mothers obtained a Master degree (23.1%), 38 mothers a Bachelor degree (41.7%), 23 mothers a high school degree (25.3%), and 2 mothers obtained a different level of education (2.2%) while information was missing for 7 mothers (7.7%).
Measures
Trust in Maternal Support
Trust in maternal support was measured with the Dutch version of the trust subscale of the People In My Life questionnaire (PIML; Ridenour et al., 2006). It consists of 10 statements related to the child’s relationship with mother (e.g., “My mother accepts me the way I am”) and is scored on a 4-point Likert scale ranging from 1, (almost) never true to 4, (almost) always true. Mean scores were calculated over all items with higher scores indicating more trust in maternal support. Ridenour et al. (2006) demonstrated adequate psychometric properties for this measure. Specifically, results revealed good internal consistency and predictive validity through negative correlations between children’s trust scores and measures of internalizing and externalizing problems. Moreover, internal consistency has also been demonstrated in samples of Flemish children (e.g., Bodner et al., 2019; Cuyvers et al., 2024) along with theory-consistent links between children’s trust scores and support-seeking behavior (Bosmans et al., 2015). In the current study, internal consistencies for the different waves indicated adequate reliability, with Cronbach’s alpha scores of .77 at Wave 1 (W1), .79 at Wave 2 (W2) and .68 at Wave 3 (W3).
Secure Base Script Knowledge
Prompt Words Scary Dog in the Yard.

Examples of a high, moderate and low scoring ‘Scary Dog in the Yard’ story.
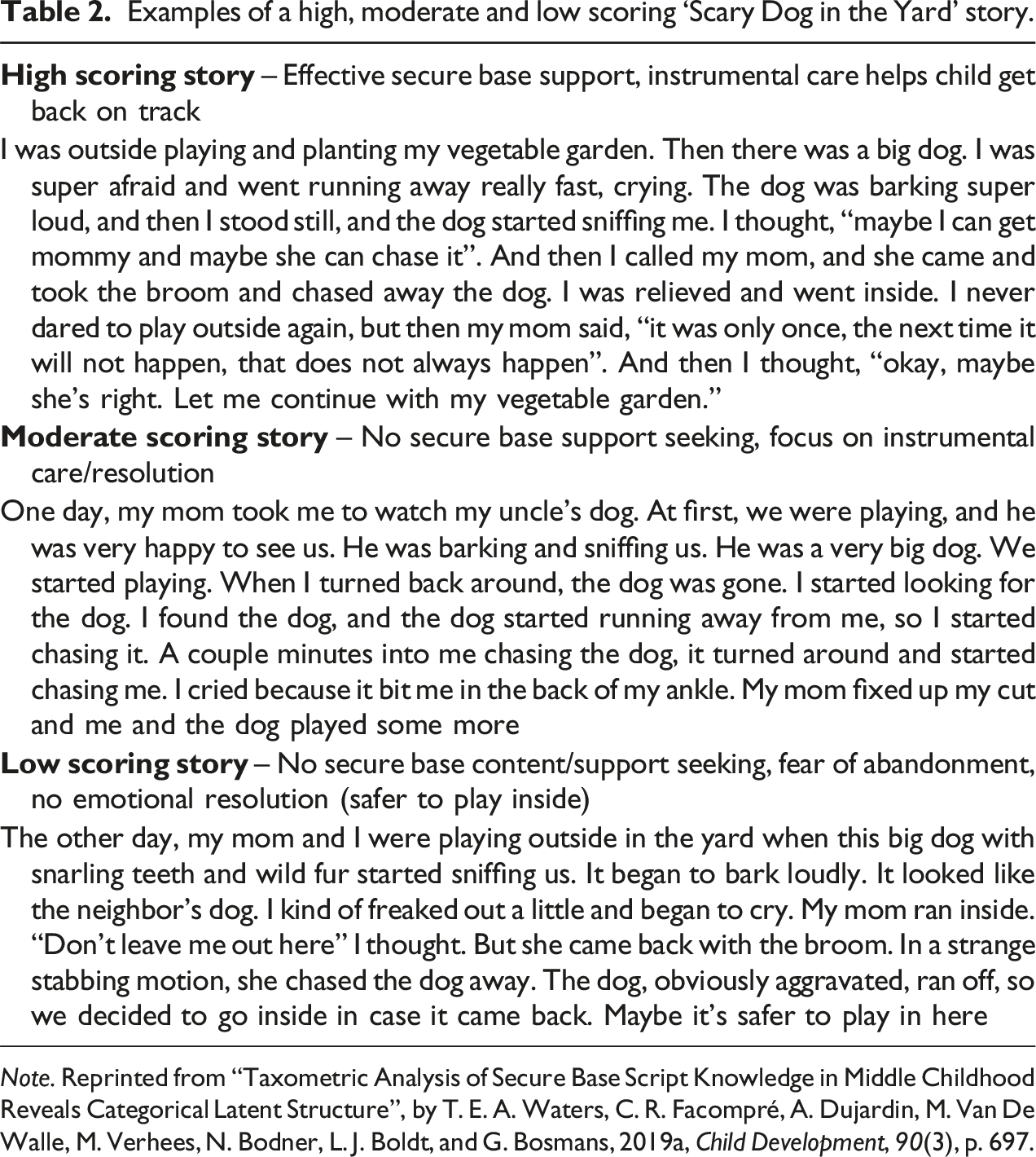
Note. Reprinted from “Taxometric Analysis of Secure Base Script Knowledge in Middle Childhood Reveals Categorical Latent Structure”, by T. E. A. Waters, C. R. Facompré, A. Dujardin, M. Van De Walle, M. Verhees, N. Bodner, L. J. Boldt, and G. Bosmans, 2019a, Child Development, 90(3), p. 697.
The ASA has shown adequate psychometric qualities with high intercoder reliability, acceptable internal consistency and theory-consistent associations with maternal caregiving quality and children’s behavioral problems (e.g., Waters et al., 2015; Waters et al., 2017). Associations with children’s behavioral problems, early maladaptive schema’s and indirect associations with psychopathology have also been found in middle childhood samples including Flemish children (e.g., Li et al., 2024; Scott et al., 2021; Waters et al., 2015). In the current study, internal consistencies for the different waves were .68 at W1, .71 at W2, and .53 at W3. Given the low internal consistency for W3, we examined whether the internal consistency would increase by dropping any of the items. However, results indicated no substantial improvements. We then calculated correlations between the items at W3 as well as the average inter-item correlation. All 3 stories were positively correlated (.16 < r < .46) with an average inter-item correlation of .29 falling within the recommended range (.15 < r < .50; Clark & Watson, 1995). Based on these results and the use of the ASA with similar internal consistencies in previous research (e.g., Houbrechts et al., 2023), we decided to retain all items in analyses.
To ensure reliable scoring, we calculated the Intraclass Correlation Coefficient (ICC) for intercoder reliability. To this end, two independent coders scored 10 transcripts from each story. For At the beach and Soccer game, we reached an ICC of respectively 0.80 and 0.90 which indicates good reliability (Koo & Li, 2016). For Scary dog in the yard, this criterium was not reached so we scored 10 extra transcripts and obtained an ICC of .93, which indicates excellent reliability. Agreement scores were assigned to the first 10 Scary dog in the yard transcripts. All subsequent transcripts were scored by one coder.
Parental Support
Parental support was measured with the support subscale of the parental support questionnaire part A (APAR) and B (BPAR; both mother-reported and child-reported), which were both constructed by combining items of various existing questionnaires (Janssens et al., 2015), including the Louvain Adolescent Perceived Parenting Scale (LAPPS; Delhaye et al., 2012), the Parental Behavior Scale (PBS-S; Van Leeuwen et al., 2013), the Perceptions of Parents Scale (POPS; Grolnick et al., 1991) and the Research assessment Package for Schools (RAPS; Research and Reform in Education, 1998). Janssens et al. (2015) assessed the validity of these parental support measures in a sample of Flemish middle childhood children. Results supported a five-factor parenting model including a parental support dimension that showed discriminant and criterion validity along with excellent internal consistency.
The BPAR consists of 8 statements (e.g., “When my child has a problem, I discuss with him/her what exactly is going on”) while the support subscale of the APAR consists of 15 (14 in the child version) statements (e.g., “I encourage my child to find his/her own direction”). Both the BPAR and the APAR are scored on a 5-point Likert scale ranging from 1, (almost) never to 5, (almost) always. Statements in the child-versions were adjusted to their perspective (e.g., “When I have a problem, my mom discusses with me what exactly is going on” and “My mom encourages me to find my own direction”). Mean scores were calculated over all items for both BPAR and the support subscale of APAR with higher scores indicating more parental support.
Given the similarity in descriptive statistics between BPAR (Mmother = 4.44, SDmother = 0.36; Mchild = 4.29, SDchild = 0.45) and APAR (Mmother = 4.50, SDmother = 0.24; Mchild = 4.39, SDchild = 0.33) and the high correlations between the two measures (rmother = .69; rchild = .65), we calculated an average mother-reported and child-reported parental support score over both measures. These scores were used in all analyses. Internal consistencies for this parental support score reported by mother and child were respectively .87 and .85.
OT
Endogenous OT levels were measured in participants’ saliva. To this end, we asked participants to chew for 2 minutes on a salivette (Sarstedt ®) which was subsequently stored at −20°C to preserve the biological integrity of the sample. Upon completion of data collection, salivary OT levels (pg/mL) were determined with Oxytocin Enzyme Immunoassay Kits (Arbor Assays®). To minimize circadian variation in OT levels as much as possible, saliva samples were collected in the morning (between 8:00 AM and 12:00 PM).
In the broader project, we obtained 8 saliva samples per participant but only the first was of relevance to investigate the research questions in the current work. This sample was collected upon participants’ arrival at the experimental setting to obtain a measure of children’s OT response to anticipatory stress (as in Tops et al., 2013). However, immunoassay analysis revealed extreme OT levels in some saliva samples (>Q3 + 3 x IQR), possibly due to measurement error. Since we had other valid OT measurements for each participant, we decided to exclude these extreme OT levels (rather than exclude the participant) and subsequently impute missing values (see below) taking into account the remaining valid OT measurements to retain our sample size.
Covariates
Covariates included in moderation analyses were children’s gender (0 = girl, 1 = boy), engagement in intensive physical activity prior to participation (0 = no, 1 = yes) and the consumption of high sugar food or beverages prior to participation (0 = no, 1 = yes) since these variables have been related to differences in OT levels in previous research (Marazziti et al., 2019; Mitra et al., 2010; Yüksel et al., 2019).
Procedure
Flyers with information about the study were distributed in primary schools throughout Flanders, Belgium. Interested families could contact the researcher by mail after which a moment for data collection was scheduled in at the school of the child or at our research center. The study comprised three equally-spaced waves with 6-month intervals. In all three waves, informed consent was obtained from both mother and child before any experimental procedures were started. Data collection at each wave involved the assessment of secure attachment (PIML and SBS knowledge) and administration of questionnaires relevant for the broader project.
During the first wave, we also collected 8 saliva samples to determine children’s OT response to various stages of experimentally-induced stress. To induce stress, children were subjected to a modified version of the Trier Social Stress Test (TSST-M; Yim et al., 2010). The TSST-M is a 15-min, laboratory stressor test. After a 2-min introduction to the test, children had to perform a speech task in which they were instructed to prepare a text (3 minutes) as if they were to introduce themselves to a new classroom (6 minutes). This was followed by a mental arithmetic task (subtract 5 consecutively from 1027; 4 minutes) that children had to perform as fast and accurate as possible. After each mistake, children were corrected and had to start over. Throughout, a video camera was placed in front of the children to further increase stress as they were told that the videotapes would be shown to experts to analyze their behavior. The TSST-M has been shown to reliably induce stress in children with similar ages as in our sample (Gunnar et al., 2009; Yim et al., 2010). As noted above, only the first saliva sample was of relevance for the current work. This sample was collected upon children’s arrival in the experimental setting in the presence of the mother. Since they were informed in advance about the stressful procedure they would take part in, this sample reflects children’s OT response to anticipatory stress similar to Tops et al. (2013).
Additionally, at the third wave, we obtained measures of both mother-reported and child-reported parental support (APAR and BPAR). We measured parental support only in the third wave to alleviate the burden on children who were already subjected to several procedures and questionnaires relevant to the broader project in all waves. This decision was further based on observations that parental support is a relatively stable phenomenon, as illustrated by previous longitudinal studies spanning even more than a year (e.g., Cuyvers et al., 2024; Dallaire & Weinraub, 2005).
After completion of each wave, children received a 30 euros voucher for a toy store as compensation for participating in the study. The procedure in the current study was approved by the local university’s ethical committee and the medical ethical committee of UZ Leuven (S63043) and in compliance with the Declaration of Helsinki.
Statistical Analysis
All data was analyzed using R (R Core Team, 2021) and IBM SPSS Statistics. To deal with missing data (16.9%), we used multiple imputation (MI). MI is a commonly used technique to handle missing data and typically assumes missingness to be random (MAR). However, this assumption cannot be formally tested. Nevertheless, MI has also been shown to be a valid approach when data is missing completely at random (MCAR) or missing not at random (MNAR; Baraldi & Enders, 2010; Pedersen et al., 2017; Schafer & Graham, 2002). Therefore, we imputed 50 datasets that were subsequently merged using the merge imputations function of the sjmisc package in R. This function selects for each missing value, the mean value calculated over all imputed datasets resulting in one dataset which was used for all subsequent analyses (Burns et al., 2011).
To investigate whether children’s OT levels upon arrival at the experimental setting moderated the effect of parental support (mother-reported and child-reported) on change in Trust and SBS knowledge, we conducted multiple hierarchical regression analyses. To examine change in Trust and SBS knowledge from W1 to W3, we regressed Trust and SBS knowledge at W3 on W3 parental support and child OT while controlling for respectively Trust and SBS knowledge at W1. Hereafter, we added the interaction between child OT and W3 parental support to the regression model. Significant interactions were followed up by simple slope analyses to test the slope of W3 parental support at low (mean – SD) and high (mean + SD) levels of child OT. Additionally, we assessed whether adding the interaction between mother-reported or child-reported parental support at W3 and child OT to the respective models significantly added to the amount of explained variance (ΔR2) by conducting the Wald test for nested models with Cohen’s f2 as indicator of effect size.
Before conducting the central analyses, assumptions for multiple linear regression were checked. When the homoscedasticity assumption was violated, we calculated robust standard errors (RSE) which were subsequently used in computing 95% confidence intervals (CI). Other assumptions indicated no major violations. To test interaction effects, we mean-centered children’s OT and mother- and child-reported parental support at W3. All analyses were repeated with the covariates. Given that we tested four different models, we controlled for multiple testing using the Bonferroni correction thus considering main and interaction effects significant at α = .0125.
Results
Preliminary Analyses
Means, Standard Deviations and Correlations Between Main Variables of the Current Study.
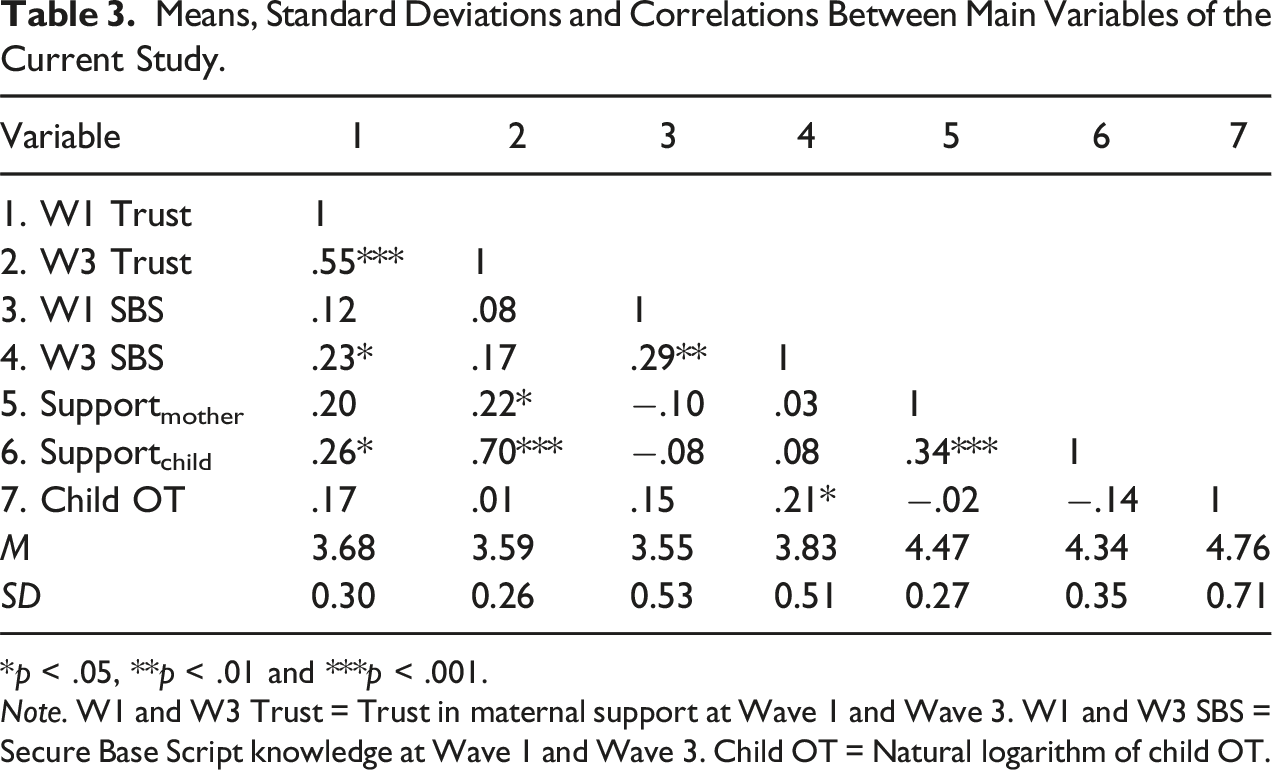
*p < .05, **p < .01 and ***p < .001.
Note. W1 and W3 Trust = Trust in maternal support at Wave 1 and Wave 3. W1 and W3 SBS = Secure Base Script knowledge at Wave 1 and Wave 3. Child OT = Natural logarithm of child OT.
The Association Between Parental Support and Change in Attachment
Change in Trust and SBS Knowledge From W1 to W3, Predicted by W3 Parental Support and Child OT.
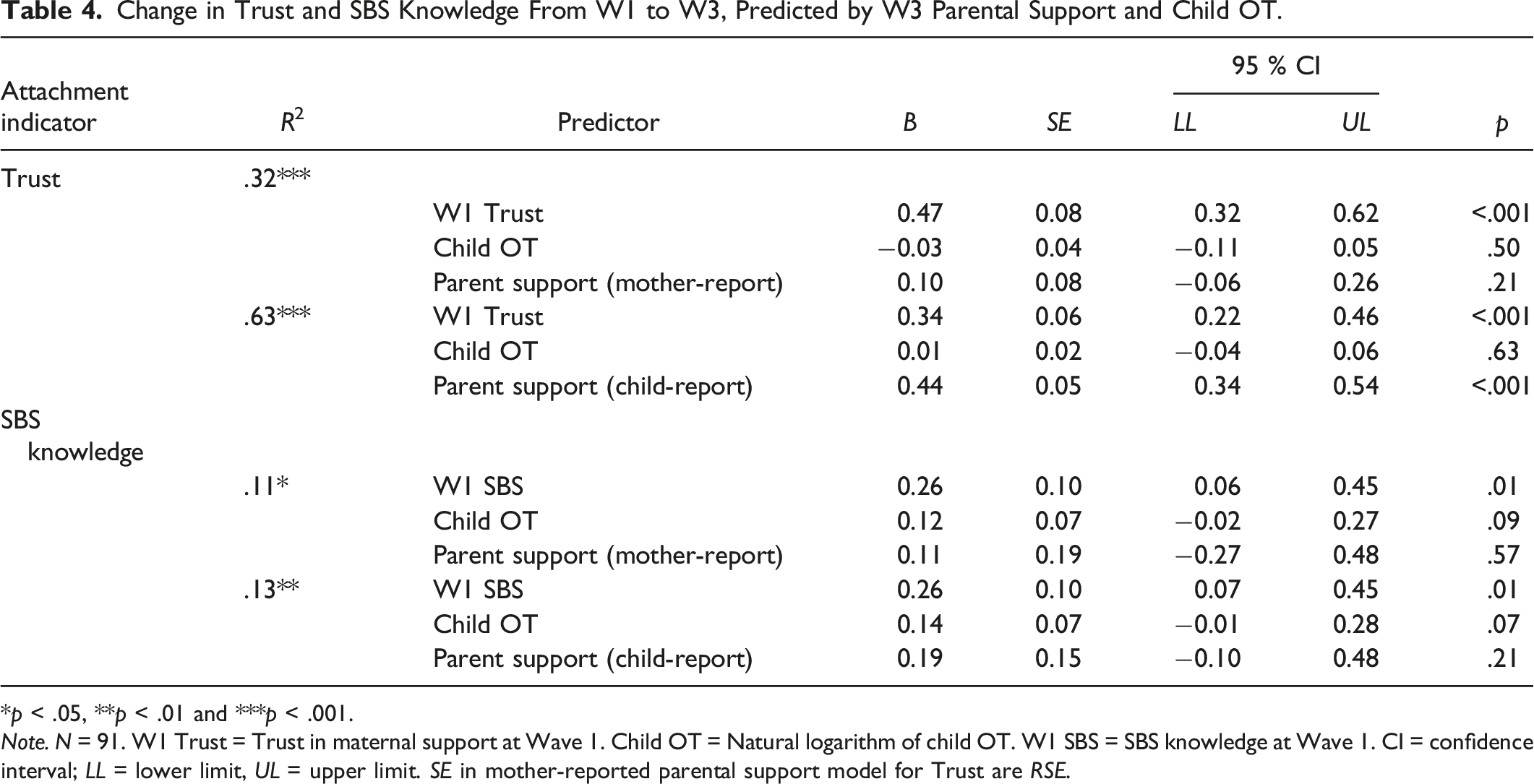
*p < .05, **p < .01 and ***p < .001.
Note. N = 91. W1 Trust = Trust in maternal support at Wave 1. Child OT = Natural logarithm of child OT. W1 SBS = SBS knowledge at Wave 1. CI = confidence interval; LL = lower limit, UL = upper limit. SE in mother-reported parental support model for Trust are RSE.
OT as Moderator of the Association Between Parental Support and Change in Attachment
Change in Trust and SBS Knowledge From W1 to W3, Predicted by W3 Parental Support x Child OT.
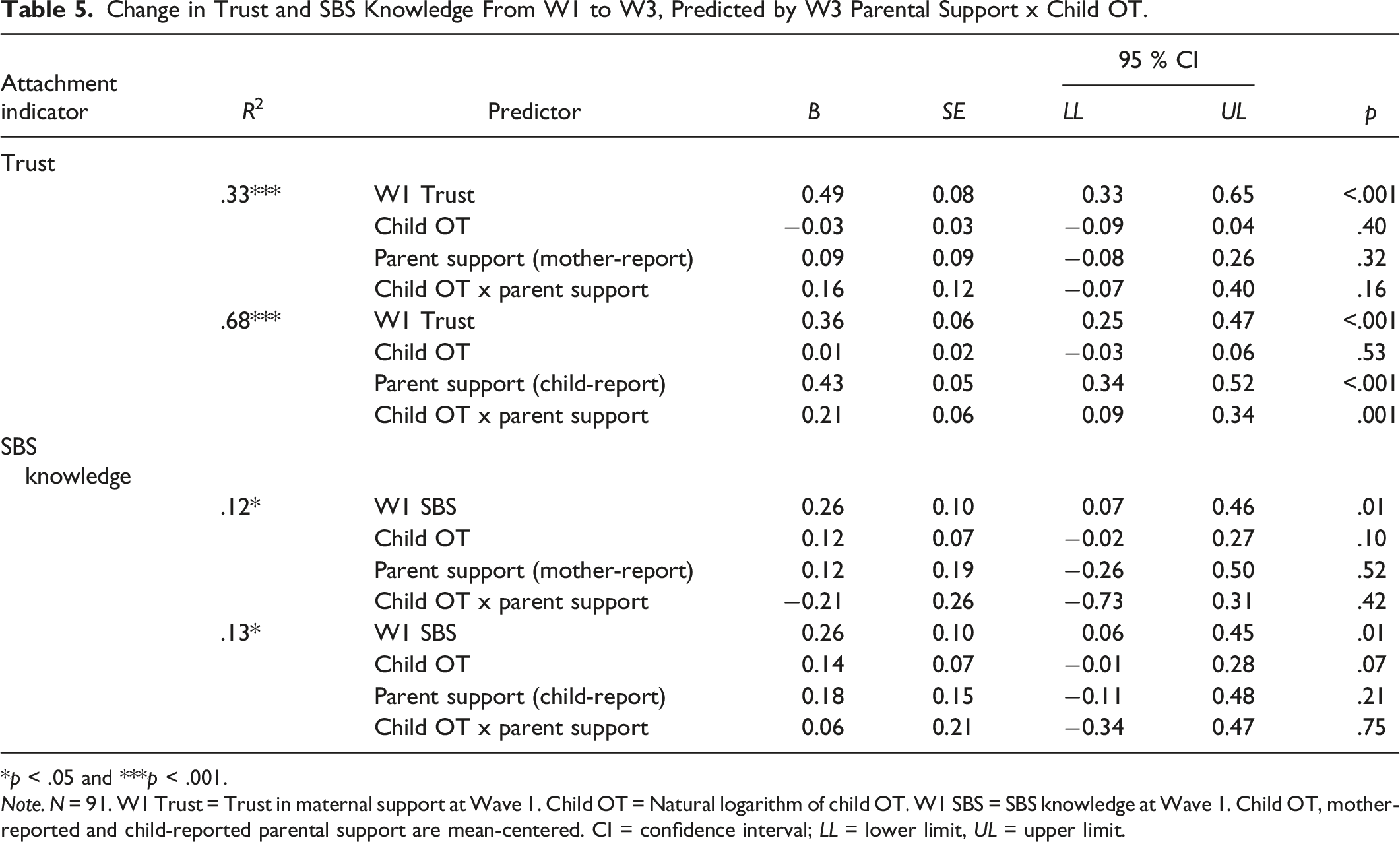
*p < .05 and ***p < .001.
Note. N = 91. W1 Trust = Trust in maternal support at Wave 1. Child OT = Natural logarithm of child OT. W1 SBS = SBS knowledge at Wave 1. Child OT, mother-reported and child-reported parental support are mean-centered. CI = confidence interval; LL = lower limit, UL = upper limit.
Adding the interaction between child-reported parental support at W3 and child OT significantly increased explained variance in Trust (ΔR
2
= .04; F1,86 = 10.76, p = .001, f2 = 0.13) but not in SBS knowledge (ΔR
2
= .001; F1,86 = 0.10, p = .75, f2 = 0.001). Furthermore, the interaction between child-reported parental support at W3 and child OT showed a significant association with change in Trust (B = 0.21, SE = 0.06, p = .001; Figure 2) but not with change in SBS knowledge (B = 0.06, SE = 0.21, p = .75). Simple slope analyses indicated that the slope was significant but moderate for children with low OT (B = 0.28, SE = 0.07, p < .001), and stronger for children with high OT (B = 0.58, SE = 0.06, p < .001). When controlling for the covariates, results were unchanged, with the interaction between child-reported parental support at W3 and child OT remaining significantly associated with change in Trust (B = 0.21, SE = 0.07, p = .002). Illustration of the significant interaction between W3 child-reported parental support and child OT to predict change in Trust.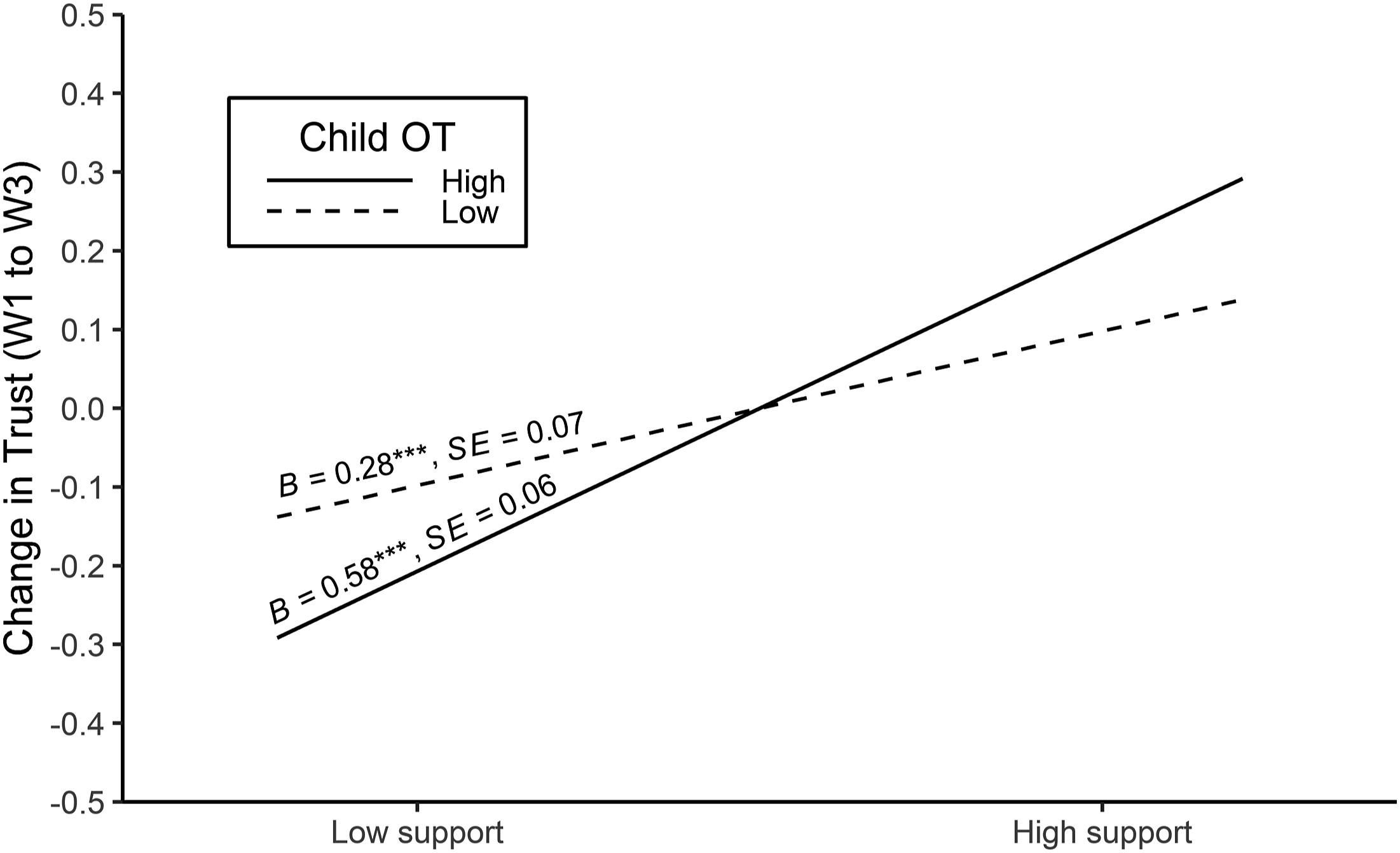
Discussion
The aim of the current study was to investigate whether the association between experienced parental support and change in secure attachment in middle childhood is dependent on children’s OT response to anticipatory stress in the presence of the mother. We expected that children with a stronger OT response to anticipatory stress in the presence of the mother would benefit more from parental support. In line with our prediction, we found that child-reported parental support at W3 was positively related to change in trust and more so for children with higher OT levels. Additionally, considering children’s OT response along with child-reported parental support at W3 explained additional variance within change in trust compared to considering only child-reported parental support at W3. In contrast, we found no evidence for such association when mothers reported on parental support. That is, both mother-reported parental support at W3 as well as its interaction with child OT were not related to change in trust. Neither mother-reported nor child-reported parental support at W3 or their interaction with child OT was associated with change in SBS knowledge.
With regard to the significant increase in explained variance in trust when considering children’s OT response along with child-reported parental support at W3, this finding is consistent with predictions of the LTA and provides further support for the involvement of neuroendocrinological processes in attachment development. In other words, our results add to literature that indicates that variance in the development of secure attachment might not be uniquely attributed to parental sensitivity (De Wolff & van IJzendoorn, 1997; Madigan et al., 2024). While Houbrechts et al. (2021) previously found that the cortisol system affected the association between parental support and change in attachment, the current work adds to this literature by demonstrating, in a different sample, a moderating role for the OT system as well.
It should be noted that children’s OT response to anticipatory stress explained a modest amount of variance in children’s trust scores. This might be the result of focusing on one hormone and not simultaneously taking into account multiple neuroendocrine systems relevant for attachment development. It remains at the moment unclear how different neuroendocrine systems interact when children seek and receive parental support during times of distress and how this could impact attachment development. For example, future studies may assess whether children who are highly motivated to seek parental support (high OT) would benefit more from this support independent of how strong they react to distress (e.g., high vs. low cortisol). The LTA provides a framework to investigate how any interplay of neuroendocrine processes might explain variance in the development of attachment at similar levels of parental support.
Our findings further support the role of OT as an important component within this neuroendocrine milieu affecting the likelihood of children seeking parental support as well as enhancing the experience of parental support (Bernaerts et al., 2017; Buchheim et al., 2009; van IJzendoorn & Bakermans-Kranenburg, 2012). Together, over distinct learning events, this might make children with a high OT response during stress more susceptible to benefit from parental support and ultimately lead to increased levels of secure attachment compared to children with a lower OT response during stress. OT thus seems to facilitate secure attachment development in supportive caregiving contexts.
Since the current study used a continuous measure of secure attachment, this raises the question whether OT’s effects would generalize over different (insecure) attachment classifications. We may speculate that, in a context where parental support is low, children with low or high motivation (low vs. high OT) to seek parental support might be more likely to minimize or maximize support-seeking behavior, respectively contributing to the development of insecure-avoidant or insecure-ambivalent (or anxious) attachment. In light of this speculation, it is interesting to note that Houbrechts et al. (2021) found a moderating effect for children’s cortisol stress response only when predicting change in anxious but not avoidant attachment. This might indicate that children’s neuroendocrine responses not only contribute to secure versus insecure attachment development but also affect the strategies children employ to cope with high or low parental support, ultimately contributing to the development of different attachment strategies. Future research is needed to investigate these hypotheses. At the moment, the most parsimonious interpretation of our findings is that OT acts as facilitator of secure attachment development in supportive caregiving environments.
Mother-reported parental support at W3 and its interaction with child OT were not related to change in trust. A first explanation for this discrepancy refers to possible biases related to self-report in the current study. On the one hand, mothers might have reported less accurately on the support they provide compared to child-reported support due to social desirability bias (Krumpal, 2013). Consequently, some mother-reported parental support scores at W3 might be positively biased while this might be less the case for child-reported trust scores. This in turn could have suppressed a significant association. On the other hand, it is possible that the effect for child-reported parental support at W3 was stronger because of within-reporter bias. Children reported both on experienced support and trust which might have resulted in a stronger association between these variables, and hence contributed to the discrepancy in predictive power of mother-reported versus child-reported parental support at W3. Alternatively, assuming that mother report and child report were both accurate, our results are in line with literature that shows that subjective experiences (i.e., child-reported parental support at W3) are stronger predictors of developmental outcomes compared to other-reported measures of these experiences (e.g., Danese & Widom, 2020; Shields et al., 2023; Solomon et al., 1987). At the moment, it is unclear which or whether any of these explanations contributed to the discrepancy observed in the current study.
Change in SBS knowledge was not associated with either mother-reported or child-reported parental support at W3, nor by their interaction with child OT. These results indicate that our findings are not similar for different attachment indicators. According to Bosmans and Kerns (2015), different attachment measures are not necessarily identical operationalizations of attachment, but reflect various components of the attachment construct. Specifically, they distinguished between components that children can reflect upon and report explicitly (e.g., self-reported Trust), versus more automatic components, beyond children’s awareness (e.g., narrative measures such as the Attachment Script Assessment).
Although more automatic components of attachment are thought to stabilize earlier than more explicit components (Waters et al., 2021; Waters & Facompré, 2021), which would provide an explanation for the greater stability of SBS knowledge, research shows that in middle childhood more automatic components are still susceptible to change (Waters, Facompré, Van de Walle, et al., 2019). This idea is further supported by the lower correlation we found between SBS knowledge at W1 and W3 (r = .29) compared to the correlation between Trust at W1 and W3 (r = .55) indicating less stability.
To ensure the reliability of our findings regarding child OT, we determined OT levels in participants’ saliva while controlling for potential confounders in our analyses. Although previous research revealed no association between central and peripheral OT levels under baseline conditions (Martins et al., 2020; Valstad et al., 2017), a positive association was found after experimentally-induced stress (Valstad et al., 2017). Additionally, Martin et al. (2018) showed that salivary OT levels correlate higher with central OT levels (i.e., in cerebrospinal fluid) than plasma OT levels. Together, these findings indicate that in the context of the current study, the use of salivary OT was the most optimal method currently available to index central OT in non-clinical samples, adding to the reliability of our results.
Despite the strengths of this study in terms of the multi-method assessment of attachment, the use of multi-informant data, salivary OT measures, and the longitudinal design of the study, reliable interpretation of the results cannot be done without taking into account some limitations.
First, with regard to the possible biases in mother report and child report of parental support at W3, future research should apply observation of parental support in addition to questionnaires as well as multi-informant data for all measures to eliminate potential confounding factors.
Second, parental support was only measured in the third wave. Although parental support is a relatively stable phenomenon (e.g., Cuyvers et al., 2024; Dallaire & Weinraub, 2005), which suggests that parental support scores may not have changed substantially over time, future research should obtain parental support scores in multiple waves and before measuring change in attachment.
Third, we collected saliva samples upon children’s arrival at the experimental setting in the presence of their mother. Similar to Tops et al. (2013), this sample was assumed to reflect children’s OT response to anticipatory stress. However, since we did not assess children’s stress response directly, one could question whether they really experienced anticipatory stress. Although our procedure was sufficiently comparable to Tops et al. (2013) to assume anticipatory stress, future research can address this issue by obtaining additional parameters of stress, such as children’s electrodermal response, cortisol levels or self-reported stress levels.
Fourth, children in our sample lived in various family configurations which could have affected the amount of time they spent with their mother. Since we did not measure time spent with mother explicitly, we could not control for this potential confounder in our analyses. Nevertheless, at least 73.6% of our sample lived together with their mother, reducing the likelihood that our results would substantially change when including time spent with mother in our analyses.
Lastly, the average levels of parental support at W3 reported by mother and child in our sample were high with low variance which raises concerns about the generalizability of our findings. However, this restriction of range makes it not unlikely that the effects found in the current study are underestimations of the true effects. Specifically, receiving insufficient parental support during distress might be particularly upsetting for children that are highly motivated to seek social support (high OT) compared to children with lower motivation to seek social support (low OT; Cardoso et al., 2013). It could be that children with high OT levels will be more negatively impacted under these circumstances. This in turn could lead to a more negative change in trust compared to children with low OT levels. Thus, in a sample with greater variability in parental support, the interaction with OT may be stronger than observed in the current study. Future research is needed to investigate this hypothesis.
In sum, in line with predictions of the LTA, the current study's findings provide further support for the association between experienced parental support and change in trust and for the moderating role of neuroendocrinological processes in this association. Given the previously discussed limitations of the current study and the novelty of our hypotheses, these findings should be considered tentative until replicated in future studies. Nevertheless, our results do support the relevance of taking into account biological factors in addition to parenting behavior to explain differences in attachment development. Given that this is one of the core predictions of the LTA, the current study’s findings provide further support for the LTA as a promising theoretical framework for future research to elucidate processes and mechanisms underlying attachment development. Ultimately, this could have important clinical implications given that insecure attachment is a transdiagnostic risk factor (Ein-dor et al., 2016; Herstell et al., 2021) for a wide range of psychiatric disorders.
Footnotes
Acknowledgements
We thank Dr. Bien Cuyvers for her help in setting up the study as well as during the data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financed by Fonds Wetenschappelijk Onderzoek (FWO) Flanders grant numbers [G075718N, G0D6721N and G0I2422N].