
Abstract
Somatic symptoms are common in adolescence and can predict later emotional distress, academic challenges, and chronic health problems. Their developmental origins, particularly before menarche, remain poorly understood. This cross-sectional study examined associations between psychological distress, parental modeling of pain behavior, pain sensitivity, and somatic symptom burden in premenarchal adolescents. A community sample of 228 adolescents (Age M = 11.3, SD = 0.9) completed standardized measures of anxiety, depression, stress, somatic symptoms, and parent-reported pain modeling. Participants also underwent laboratory-based bladder and pressure pain threshold testing. In multivariable regression, Tanner stage (β = .11), anxiety (.31), depression (.23), parental pain modeling (.15), and visceral pain sensitivity (.13) were independently associated with greater somatic symptoms. Results highlight a constellation of psychological, familial, and physiological factors related to somatic symptoms in early adolescence, suggesting that early identification of these risks could inform prevention strategies before puberty, when more persistent symptom patterns may emerge.
Introduction
Somatic symptoms, defined as non-specific bodily symptoms without identifiable disease, including palpitations, fatigue, and pain are common during adolescence and can interfere with emotional, social, and academic development (Beck, 2007). They are also among the leading causes of increased medical health utilization and important precursors to chronic pain in adulthood (Boerner et al., 2017; Heathcote, 2019; Latthe et al., 2006; McBeth et al., 2001; Smith, 1994). Early adolescence, particularly the years before menarche, is a sensitive developmental period when biopsychosocial processes interact to shape long-term health trajectories. From a developmental perspective, the pubertal transition brings rapid biological, cognitive, and social changes, making this a period of heightened vulnerability for the emergence of somatic symptoms. In fact, female adolescents experience an increase in somatic symptoms across the pubertal transition with a higher symptom burden than males (Garber et al., 1991).
There is also a rise in anxiety and depression in a sex-dependent manner during the pubertal transition, making it difficult to establish causality of somatic symptoms during this developmental period (Garber et al., 1991; Knight et al., 2021; Patton et al., 1996; Viner et al., 2017). Somatic symptoms are positively associated with psychological symptoms, such as depression, anxiety, and stress, in adolescents (Garber et al., 1991; Meesters et al., 2003; Vila et al., 2009). Depression symptoms and disorders commonly co-occur with anxiety and somatic symptoms (Lallukka et al., 2019), with a common onset of depressive disorders between the ages of 11 and 14, with a 15.9% prevalence rate for female adolescents (ages 13–18) (Merikangas et al., 2010). One potential explanation for the association between somatic symptoms and psychological factors is the generalized hypervigilance hypothesis, which proposes that heightened anxiety enhances attentional bias toward both external stimuli and interoceptive pain signals, resulting in amplified perception of somatic symptoms (McDermid et al., 1996).
Somatic symptoms are also associated with cutaneous pressure pain sensitivity (Cornelissen et al., 2014; Ramalho et al., 2015) as well as visceral pain sensitivity (Whitehead & Palsson, 1998). Sensory sensitivity, a neurobiological sensitizing mechanism that increases afferent activity, might underlie enhanced interoception, resulting in increased somatic symptoms (Bourke et al., 2015; Harshaw, 2015). However, a key limitation of most prior studies on somatic symptoms is a lack of consideration of potential contributing covariates, such as sensory sensitivity, which could be a primary mechanism responsible for increased somatic symptom sensitivity. Quantitative sensory testing allows for experimental measurement of sensory sensitivity, and this method can be used to evaluate the association between sensory sensitivity and somatic symptoms. To study visceral pain sensitivity, a noninvasive bladder filling task that correlates with somatic symptoms in adult women was used. A prior study has shown an association between somatic symptoms and visceral pain sensitivity, as measured by the bladder filling task (Tu et al., 2022). This earlier study also identified associations between visceral pain sensitivity, anxiety, and depression symptoms, indicating that psychological factors need to be accounted for along with visceral pain sensitivity when examining somatic symptoms.
Somatic symptoms in adolescence may also be influenced by observing parental pain behavior, such as moving stiffly or calling out for help (Stone & Walker, 2017). The potential psychological mechanism for this association is rooted in social learning theory, which proposes that children learn certain behaviors by observing others model that particular behavior and through operant reinforcement by others (Bandura & Walters, 1977; Stone et al., 2018). Regarding pain-specific social learning, one study found that when parents were instructed to exaggerate their pain response, their children (ages 6–8 years old) reported increased anxiety levels compared to those in the minimized pain response condition (Boerner et al., 2017). Additionally, somatic symptoms in parents were associated with somatic symptoms in adolescents with functional abdominal pain (Walker et al., 1991). Thus, adolescents’ observation of parental pain behavior appears to be a critical contributor to somatic symptoms.
Given the prior evidence of these different mechanisms which may contribute to somatic symptoms, the present study harnesses a biopsychosocial developmental framework (McKillop & Banez, 2016; Palermo et al., 2014), focusing on a sensitive premenarchal window before major pubertal and hormonal changes. Development is operationalized by age, Tanner stage, and premenarchal status, allowing for the examination of cross-sectional associations among psychological symptoms, somatic symptoms, parental modeling of pain behavior, and physiological pain sensitivity prior to the onset of menstrual pain and related pubertal processes.
Method
Participants
Participant Demographics and Medical History
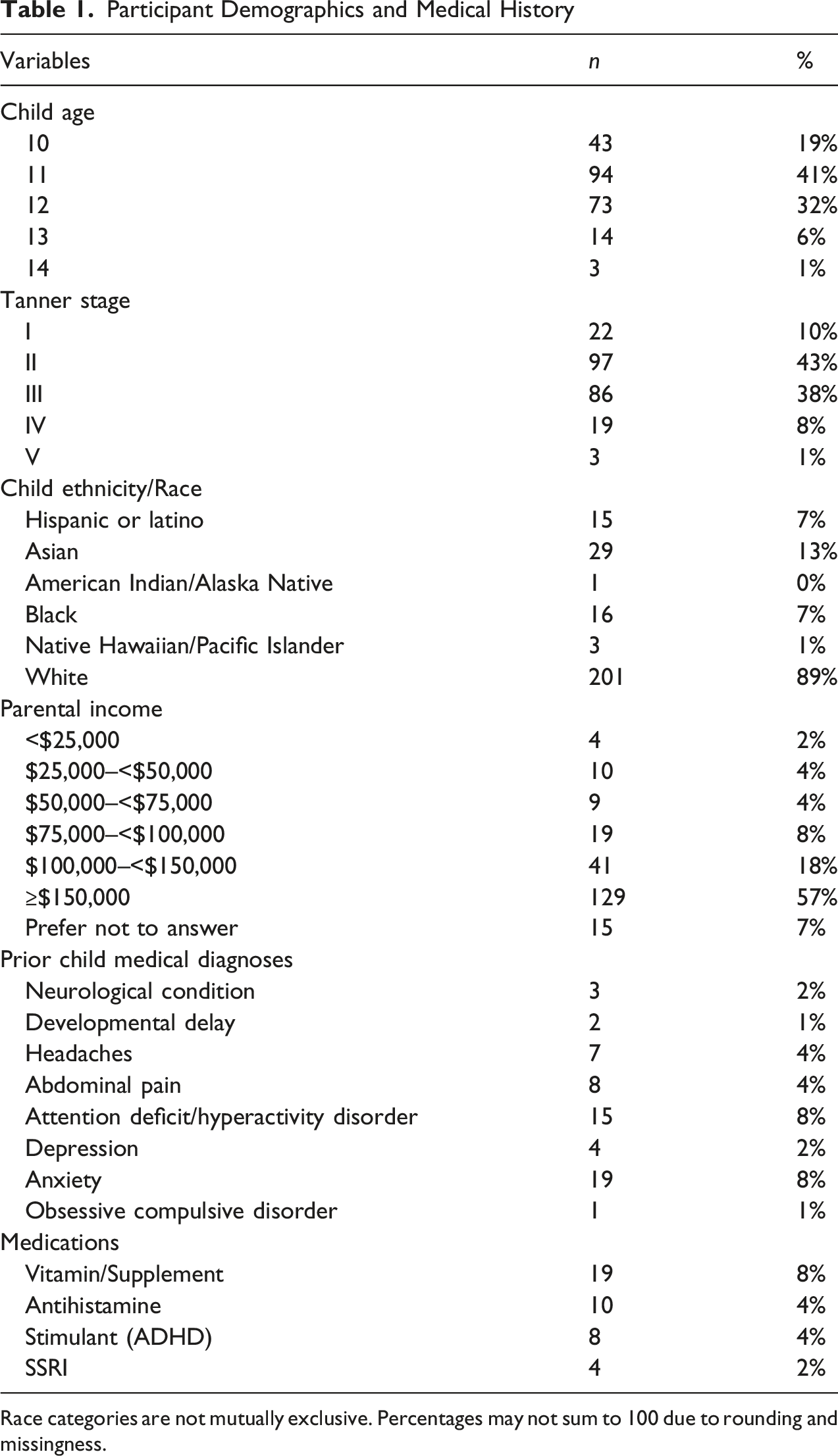
Race categories are not mutually exclusive. Percentages may not sum to 100 due to rounding and missingness.
Measures
Parents/guardians of adolescent participants completed a demographic questionnaire that asked about the child’s age, race, ethnicity, and the adult’s age, education level, marital status, and income level. Youth participants also completed measures evaluating current levels of somatic symptoms, anxiety, stress, and observations of parental pain behavior.
Children’s Somatic Symptom Inventory (CSSI)
The CSSI is a 24-item measure that assesses common nonspecific bodily symptoms (e.g., headache, upset stomach, weakness, hot or cold spells) over the past two weeks on a 5-point Likert scale (0 = “Never”, 4 = “Always”). The measure is scored by summing the 24 items; scores can range from 0 to 96, with higher scores indicating an elevated report of somatic symptoms (Walker et al., 2009). The CSSI has been validated in both clinical (Walker et al., 1991) and community samples (Garber et al., 1991), supporting its use as a clinical and research tool. In the present sample, this measure showed acceptable internal consistency (α = .88). Of the 24 CSSI items, 15 primarily reflect visceral, interoceptive, or autonomic symptoms (e.g., abdominal pain, nausea, bowel symptoms, dizziness, palpitations, fatigue), whereas only 4 items assess localized musculoskeletal pain (e.g., joint or limb pain), with the remaining 5 items reflecting more generalized neurological or diffuse somatic complaints.
PROMIS Pediatric Profile
The PROMIS Pediatric Profile includes questions about general psychosocial functioning, including physical function, anxiety, depression, fatigue, peer relationships, and pain interference; however, this paper only reports the results of the 8-item anxiety and 8-item depression scales. These measures have been well-validated in community samples (Irwin et al., 2010) as well as pediatric pain populations (Kashikar-Zuck et al., 2016). These scales ask the participant about their feelings of anxiety or depression over the past week (e.g., “I felt like something awful might happen”, “I felt worried”) using a 5-point Likert scale (1 = “Never”, 5 = “Almost Always”). This scale is scored by summing the items and converting the raw score to a T-score using the PROMIS manual; higher scores indicate increased feelings of anxiety or depression. In the present sample, this measure showed acceptable internal consistency (anxiety α = .90, depression α = .92).
PROMIS Psychological Stress Experiences
The PROMIS Psychological Stress Experiences survey is an 8-item measure which asks the participant to rate how often they experienced feelings of stress (e.g., “I felt that my problems kept piling up”, “I felt under pressure”) over the last seven days using a 5-point Likert scale (1 = “Never”, 5 = “Always”) (Bevans et al., 2018). The measure is scored by summing the items and converting the raw score to a T-score using the PROMIS manual; higher scores indicate elevated stress levels. In the present sample, this measure showed acceptable internal consistency (α = .91).
PROMIS Parent Pain Behavior Proxy (PPB-Proxy)
The PPB-Proxy is a 7-item self-report questionnaire that measures how often a child observes their primary caregiver engage in various pain behaviors (e.g., “When my caretaker was in pain, she/he moved extremely slow.”) over the last seven days using a 5-point Likert scale (1 = “Never”, 5 = “Always”) (Stone & Walker, 2017). We administered a modified version of the PPB-Proxy with our study cohort. This version of the questionnaire did not ask the initial branching logic question: “In the past 7 days, did your caretaker have pain?” The measure was scored by summing the item responses; higher scores indicated more frequent observations of parental pain behavior. In the present sample, this measure showed acceptable internal consistency (α = .78).
Tanner Stage
To identify participants’ pubertal stage, adolescents completed the Tanner Stage Development Questionnaire, which includes standardized images depicting stages of breast and genital development (Marshall & Tanner, 1969; Rasmussen et al., 2015). Participants self-assessed their pubertal stage by selecting the image that best reflected their current development.
Parental Pain Body Map
Parents of participants indicated on a paper 7-site body map chart (head, torso, 4 limbs, back) which sites they felt pain in the past week (Schrepf et al., 2018). The pain body map is a marker for the severity of centralized or nociplastic pain (Clauw, 2024).
Noninvasive Bladder Filling Task
Participants completed a validated, noninvasive bladder filling task to assess visceral pain sensitivity (Tu et al., 2013, 2022). At the beginning of the task, participants voided to empty their bladder. Then, a research assistant gave the participant 20 oz of water and instructed them to drink as much water as possible within 5 minutes. Participants were told to notify the research assistant when they reached three levels of bladder urgency: first sensation, first urge, and maximum tolerance. Given our early adolescent population, we modified these terms for comprehension purposes to green, yellow, and red zones, respectively. Green zone is defined as, “you are aware that there is some urine in your bladder.” Yellow zone is defined as, “you could go to the bathroom to pee, but you do not have to rush off to do this.” Red zone is defined as, “you would leave in the middle of your favorite movie to go to the bathroom even if you were missing the best part.”
After reviewing the bladder testing instructions, a research assistant assessed the participant’s comprehension with a brief multiple-choice quiz. If participants did not answer the questions correctly, the research assistant reviewed the correct answers and the task instructions to ensure the participants’ comprehension before moving forward with the task. Participants completed bladder urgency and bladder pain rankings using a 0–100 visual analog scale (0 = no urgency/pain, 100 = worst urgency/pain imaginable) at multiple time points: after the initial void, at each bladder urgency zone, and every 15 minutes. After the initial void and when participants reached each bladder urgency zone, their bladder volume was measured using a 3D ultrasound abdominal transducer (GE Voluson 750, Wauwatosa, WI) or a bladder scanner (Verathon Bladder Scan Prime, North Creek Parkway, Bothell, WA), which took approximately 15–30 s to complete. If participants did not reach the red zone (“maximum tolerance”) by 45 or 60 minutes into the task, they were given an additional 10 oz of water to drink and instructed to drink as much as possible within 5 minutes. The task was concluded if the participant did not reach the red zone by 75 minutes. Final bladder urgency, pain, and bladder measurements were obtained, and the participant was instructed to void into a graded toilet hat. The urine sample was collected to confirm ultrasound measurements. Based on prior research in adults that has found associations between experimental bladder pain at first urge, somatic symptoms, and menstrual pain (Tu et al., 2013), the bladder pain score reported at first urge (i.e., the “yellow zone”) was used as a measure of visceral pain sensitivity in analyses.
Pressure Pain Thresholds (PPTs)
After completing the bladder filling task, participants also completed external pressure pain threshold (PPT) testing on their left knee and left shoulder to assess cutaneous pain sensitivity using a digital pressure algometer with a 1 cm2 rubber tip (Wagner Instruments, Greenwich, CT). These sites were chosen because they correspond to American College of Rheumatology guidelines for fibromyalgia tender point sites (Wolfe et al., 1990). Software was used to guide pressure at a consistent rate of 4 Newtons/second up to a maximum of 70 Newtons. A research assistant reviewed the instructions for the task and assessed the participant’s baseline pain at each site using a 0–10 NRS. To ensure comprehension of the task, the research assistant conducted a practice test on the participant’s right knee. Participants were instructed to press a handheld button the moment the sensation from the algometer turned from pressure to pain (the moment the pain reached a 1 on a 0-10 NRS) and verbally rate their pain on a 0–10 NRS the moment they pressed the button for each site. When the participant pressed the button, the amount of applied pressure was automatically recorded on the computer program. If the participant reported pain greater than 1, the assistant reviewed the instructions and conducted a repeat practice test to ensure understanding. A research assistant performed the first trial at each site, took a 2-min break, and then repeated the trial at each site. PPT measurements were highly reliable and consistent across sites (α = .86). Staff conducting PPT testing performed reliability testing in practice sessions to achieve consistent results (<10% variance in thresholds). Based on prior research using this paradigm (Hellman et al., 2020) the mean pressure pain threshold was calculated by averaging the two knee and shoulder trials. A higher average score on the PPT task indicated a higher sensory threshold.
Procedure
Parents/guardians of interested participants completed an initial phone screen with a trained research assistant to assess eligibility. Eligible participants were scheduled for an initial visit, and parents/guardians were sent consent/assent forms to review beforehand. At the initial study visit, a parent/guardian signed a consent form, and their child signed an assent form before participation. After obtaining consent, parents were asked to wait in an adjacent exam room. Parents completed demographic and medical history questionnaires on behalf of their children. Adolescents completed several questionnaires in REDCap (Harris et al., 2009) to assess key study constructs. They completed a noninvasive bladder filling task to measure visceral pain sensitivity and pressure pain thresholds (PPT) to measure cutaneous pain sensitivity. Approval for this study was obtained from the Institutional Review Board.
Analytic Plan
RStudio (4.1.0) was used for all data analyses. Participants who were missing data for bladder pain at first urge or had incomplete data (n = 27) were omitted from the dataset, resulting in a sample size of n = 228 for this study. Bladder pain at first urge (i.e., “yellow zone”) was missing for some participants due to participants sometimes “skipping” the first urge zone. The data were assessed for skewness (as defined by skewness value > +/− 1.0). The data were skewed. Therefore, Spearman’s correlations were run to examine associations among somatic symptoms, age, Tanner stage, parental pain bodymap, anxiety, depression, stress, observation of parental pain behavior, PPTs, and experimental bladder pain. Effect sizes based on correlations were categorized as small (.2), medium (.5), or large (.8) based on effect size guidelines (Ferguson, 2009). To control for multiple comparisons, p-values were adjusted using the Benjamini–Hochberg false discovery rate (FDR) procedure (Benjamini & Hochberg, 1995).
Our goal was to build a model explaining somatic symptoms before menarche, accounting for experimental sensitivity, psychological factors, and observed parental pain behavior. Therefore, a hierarchical regression with somatic symptoms as the outcome variable was run to examine (1) effects of development (Tanner Stage, Age) and parental pain (2) the variance accounted for by sensory sensitivity (PPTs and experimental bladder pain), (3) psychological factors (depression, anxiety and stress) and (4) observations of parental pain behavior. Semi-partial r2 describes the variance in the outcome variable that is explained by an independent variable after accounting for the variance associated with other independent variables (Fritz et al., 2012). Effect sizes were categorized as small (.04), medium (.25), or large (.64) following guidelines on η2 (Ferguson, 2009). Multicollinearity was assessed by variance inflation factor (VIF) and determined to be low (VIF <2).
Power analyses were conducted in R assuming a two-sided α = .05. Based on the observed sample size, the study was adequately powered to detect moderate associations, with approximately 86% power to detect correlations of r = 0.25. For hierarchical regression analyses, power calculations suggested 83% power to detect an incremental contribution of ΔR2 ≥ .018 in a four-step model including nine predictors.
The data supporting this study are available at Open Science Framework: https://doi.org/10.17605/OSF.IO/PBVHQ.
Results
Somatic Symptoms Were Correlated With Anxiety, Depression, Stress, Observations of Parental Pain Behavior, Cutaneous Pain Sensitivity, and Visceral Pain Sensitivity
Intercorrelations Between Participant-reported Outcomes and Pain Sensitivity Assay
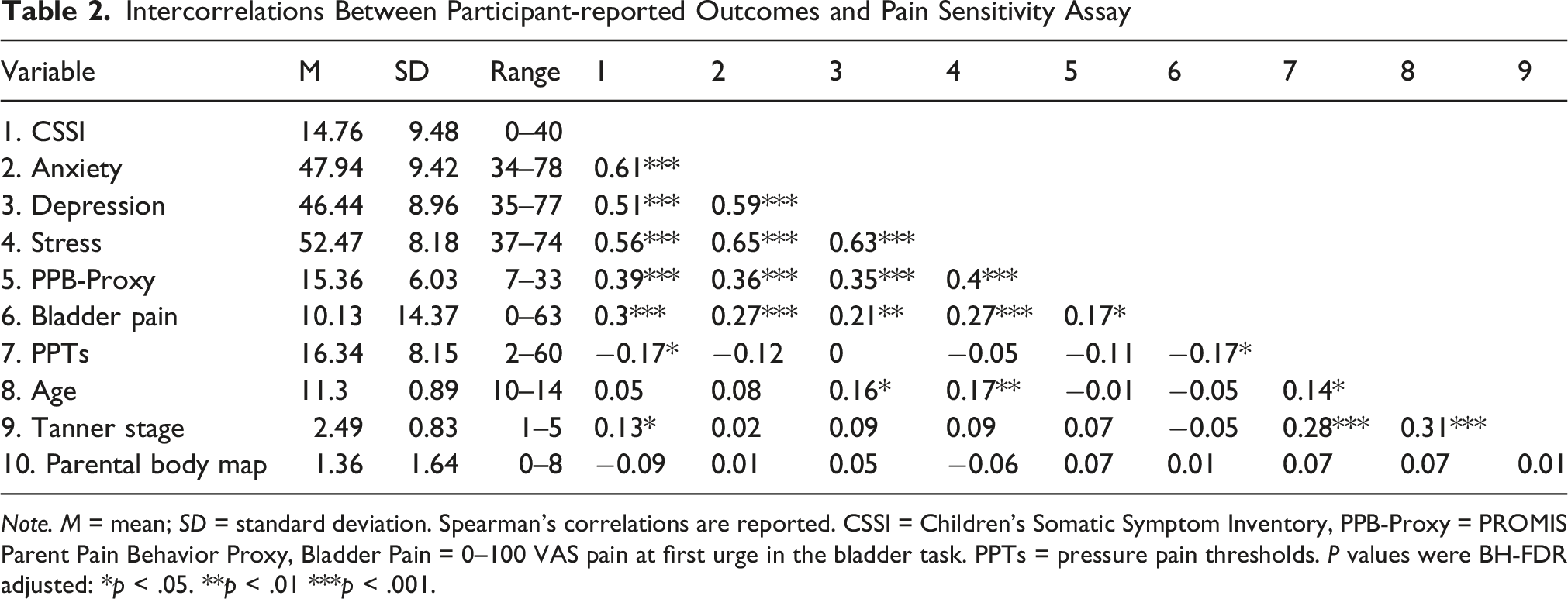
Note. M = mean; SD = standard deviation. Spearman’s correlations are reported. CSSI = Children’s Somatic Symptom Inventory, PPB-Proxy = PROMIS Parent Pain Behavior Proxy, Bladder Pain = 0–100 VAS pain at first urge in the bladder task. PPTs = pressure pain thresholds. P values were BH-FDR adjusted: *p < .05. **p < .01 ***p < .001.
As shown in Table 2, somatic symptoms were moderately to strongly correlated with anxiety, depression, and stress (Spearman’s ρ′s = 0.51–0.61, p’s < .001), and showed smaller but significant associations with observations of parental pain behavior, experimental bladder pain, Tanner stage, and PPTs (p’s < .05). Experimental bladder pain was modestly correlated with somatic symptoms, psychological distress, and parental pain behavior, whereas PPTs were inversely related to somatic symptoms and bladder pain but not to anxiety or stress. Developmental effects were modest: age was weakly associated with depression, stress, and PPTs, but not with somatic symptoms or bladder pain. In contrast, Tanner stage showed stronger associations with PPTs and age, and a small but significant correlation with somatic symptoms, suggesting that pubertal maturation—more than chronological age—relates to pain sensitivity. Parent body map scores were not significantly correlated with child somatic symptoms, pain sensitivity, or developmental variables.
Psychological Symptoms Demonstrate Stronger Associations With Somatic Symptoms Relative to Observations of Parental Pain Behavior and Visceral Pain Sensitivity
Hierarchical Regression Results for Somatic Symptoms
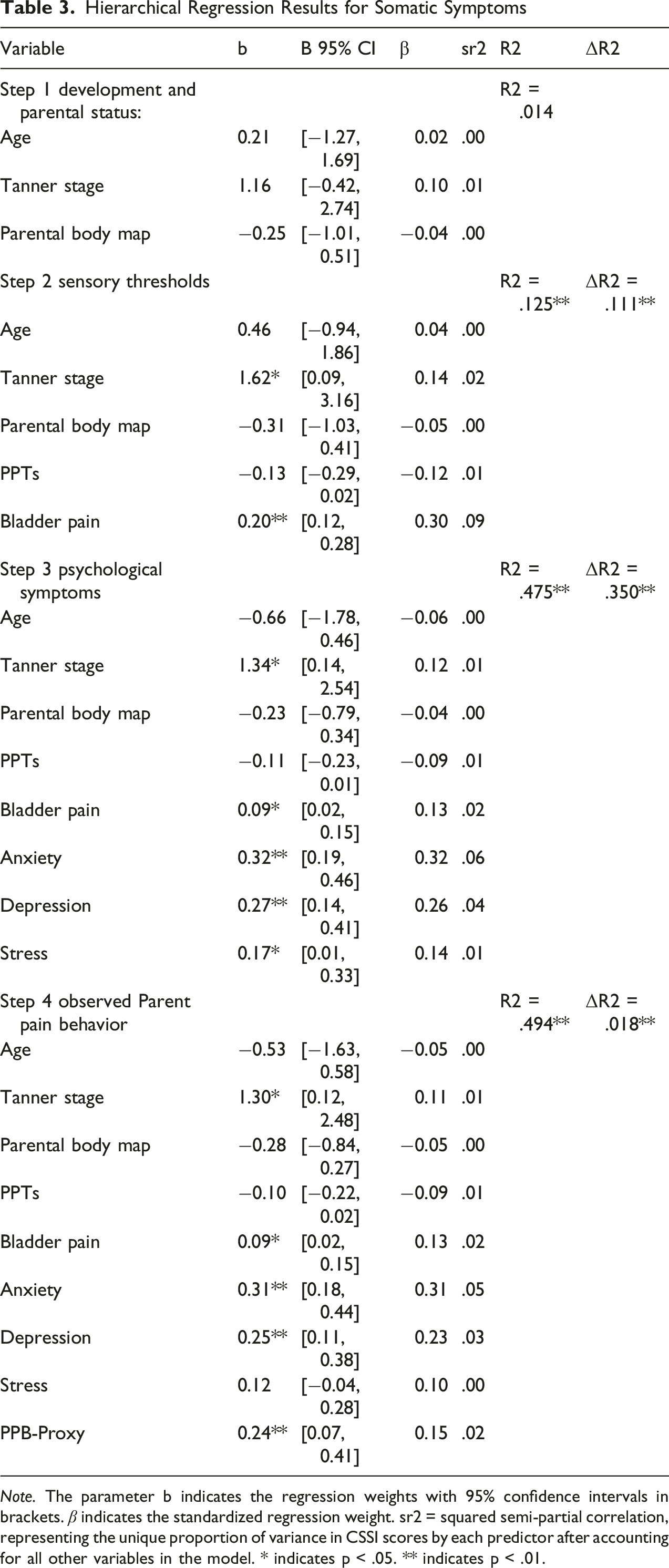
Note. The parameter b indicates the regression weights with 95% confidence intervals in brackets. β indicates the standardized regression weight. sr2 = squared semi-partial correlation, representing the unique proportion of variance in CSSI scores by each predictor after accounting for all other variables in the model. * indicates p < .05. ** indicates p < .01.
The second step of the model was conducted to determine whether sensory thresholds were associated with elevated somatic symptoms. Experimental bladder pain was positively associated with somatic symptoms (β = 0.30, p < .01) and had a small effect size. However, PPTs were not associated with somatic symptoms (β = −0.12, p > .05). The model revealed a significant impact of sensory thresholds accounting for the variance associated with developmental and parental pain (ΔR 2 = .111, p < .01).
The third step evaluated whether psychological factors (anxiety, depression, and stress) were significantly associated with somatic symptoms beyond the variance associated with variables entered in the previous two steps. Indeed, anxiety (β = .32, p < .01), depression (β = .25, p < .01), and stress (β = .14, p < .05) were positively associated with somatic symptoms, accounting for a significant increase in variance, compared to the second step (ΔR 2 = .350, p < .01).
A fourth step examined the association between observations of parental pain behavior and somatic symptoms (see Table 3). This step demonstrated that observations of parental pain behavior had a small, but significant positive association with somatic symptoms (β = 0.15, p < .01) suggesting that adolescents who report more frequent observations of their parents in pain indicate higher levels of somatic symptoms (ΔR
2
= .018, p < .01). In this final model, Tanner stage (β = .11), anxiety (.31), depression (.23), parental pain modeling (.15), and visceral pain sensitivity (.13) were independently associated with greater somatic symptoms (Figure 1). Experimental bladder pain and observation of parental pain behavior displayed smaller effects relative to other variables in this model. Thus, adolescents’ observation of parental pain behavior was significantly associated with somatic symptoms even after accounting for the variance associated with development, sensory sensitivity and psychological symptoms. Marginal Effects of Psychosocial, Sensory, Developmental, and Parental Factors on Somatic Symptoms. Panels display the marginal effects of each predictor on the Children’s Somatic Symptom Inventory (CSSI) derived from the multivariable regression model. Solid lines represent model-estimated marginal effects, with shaded bands indicating 95% confidence intervals. All other covariates were held constant at their sample means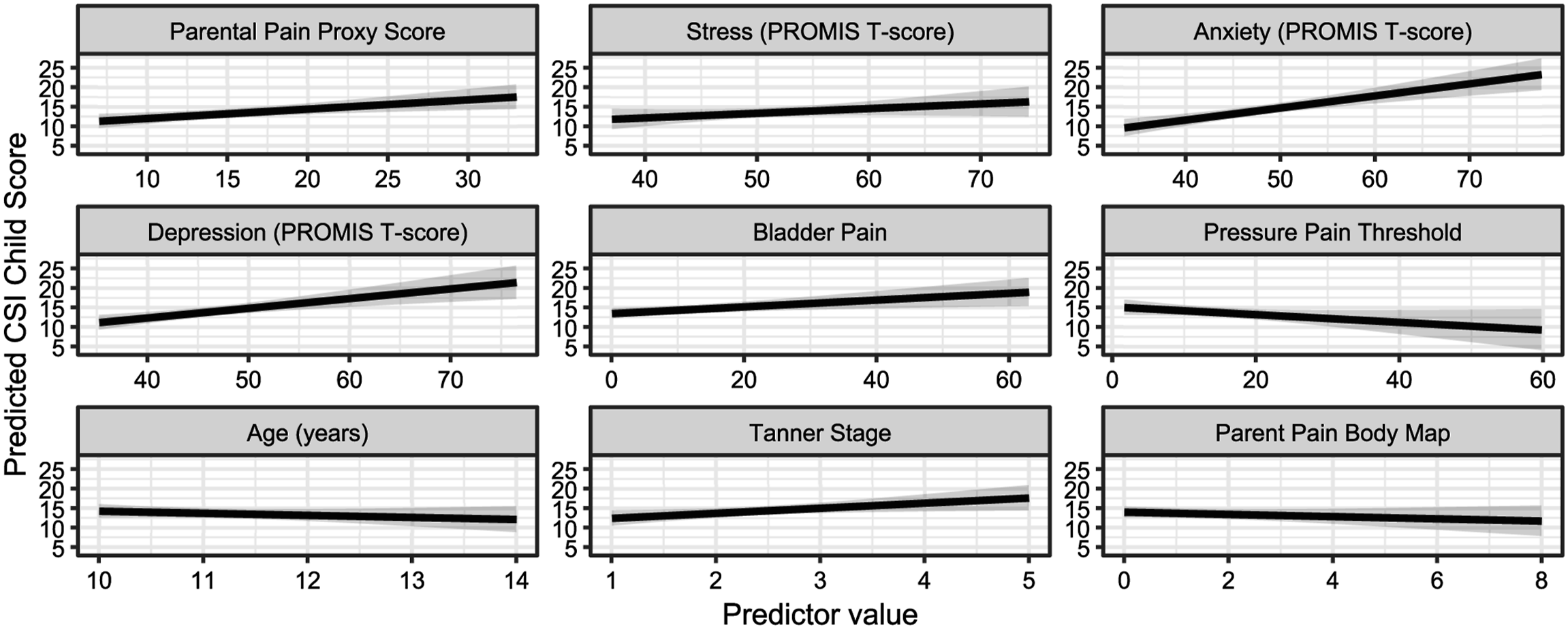
Discussion
The present findings indicate that anxiety and depression were the strongest correlates of somatic symptoms in early adolescence, followed by parental pain modeling and visceral pain sensitivity. Although the present analyses are cross-sectional, they demonstrate that these associations are detectable prior to menarche, a developmental stage that precedes the emergence of menstrual pain and established sex differences in somatic symptom burden. Chronological age showed minimal associations with somatic symptoms or pain measures, whereas pubertal maturation (Tanner stage) was weakly associated with somatic symptoms and more strongly related to pain sensitivity. This pattern suggests that pubertal development, rather than age per se, may be more relevant for emerging differences in pain processing during early adolescence. These results align with developmental theories emphasizing the interplay of emotional regulation, social learning, and physiological reactivity during this formative stage (Latham et al., 2017; McLaughlin et al., 2015). Although similar associations have been found in menstruating adults (Tu et al., 2017; Westling et al., 2013), the present cross-sectional study suggests that these relations are also present prior to menarche. Adolescents’ observation of parental pain behavior was positively associated with somatic symptoms after accounting for psychological and sensory sensitivity. These findings imply that adolescents might adopt pain beliefs and behaviors from their parents via observational learning. Although lower PPTs were associated with more somatic symptoms, they were not significantly predictive of somatic symptoms after accounting for experimental bladder pain. This suggests that visceral pain sensitivity may have a dominant, albeit overlapping effect on somatic symptoms compared to cutaneous sensitivity. While longitudinal and experimental studies are needed to establish causality, this study demonstrates that depression, anxiety, visceral pain sensitivity, and observation of parental pain behavior are key factors associated with somatic symptoms in this critical premenarchal window.
The present findings regarding the relationship between somatic symptoms, PPTs and bladder pain sensitivity are consistent with studies in adults (Hellman et al., 2020; Tu et al., 2017). However, because menstrual pain often co-occurs with somatic symptoms and increased pain sensitivity in adults, it is difficult to determine whether increased pain sensitivity is a result of menstrual pain or increased somatic symptoms. Similar effect sizes of correlation coefficients have been observed between somatic symptoms and provoked bladder or rectal pain (Tu et al., 2017; Whitehead et al., 1997), suggesting that increased visceral sensitivity is related to increased somatic symptoms in both premenarchal and post-menarchal individuals. Previous brainstem research suggests that pain modulation of visceral pain sensitivity involves different neurons and more neurons than those involved in cutaneous pain sensitivity (Brink et al., 2006). Identifying the exact mechanisms underlying these distinctions remains an important direction for future research. One plausible explanation for the stronger association between the CSSI and bladder pain sensitivity, relative to PPTs, lies in the content of the somatic symptom measure itself. The majority of items on the CSSI align with symptom domains that may be more closely aligned with bladder pain sensitivity than localized cutaneous pressure pain thresholds. As a result, bladder pain sensitivity may be more closely aligned with the symptom domains captured by the CSSI than are localized cutaneous pressure pain thresholds.
In the present study, anxiety and depression were positively related to somatic symptoms after accounting for variance associated with experimental bladder pain and PPTs, suggesting the importance of incorporating anxiety and depression into conceptual models of somatic symptoms in youth. A study examining associations between pelvic pain and psychological factors in adult females found a slightly larger effect size between somatic symptoms and anxiety (ρ = .72) or depression (ρ = 0.66) than our results (Westling et al., 2013). One possible explanation for this difference in effect size magnitude between premenarche and postmenarche is that increases in psychological distress during the post-menarchal period might make individuals more vulnerable to somatic symptoms (Garber et al., 1991). While multiple studies have found consistent associations among psychological factors and somatic symptoms (Haug et al., 2004; Tu et al., 2022; Westling et al., 2013; Zuckerman et al., 2018), the present study examined these factors in a multivariable model that accounted for shared variance associated with all variables. Our analytical design advances earlier research on somatic symptoms that was limited in scope by an imbalanced reliance on a biomedical framework (Masi et al., 2002; Wade & Halligan, 2004), and typically excluded consideration of psychological distress factors. Results from the present study support the need to frame somatic symptoms in a more holistic context (Masi et al., 2002).
Adolescents’ observation of parental pain behavior in the present study was lower than in clinical samples in previous research (Stone & Walker, 2017), which is to be expected in a non-selected community sample of adolescents. Results also showed that frequent observation of parental pain behavior was associated with increased somatic symptoms, even after adjusting for sensory sensitivity and psychological factors. The relation between observation of parental pain behavior and somatic symptoms was indicative of a small to medium effect size and is supported by previous research linking pain-specific social learning and pain symptoms (Boerner et al., 2017; Stone & Walker, 2017). For example, adolescents’ perception of their parents’ pain behavior significantly predicted adolescents’ pain intensity, pain-related distress, and number of daily pain locations over seven days after accounting for variance related to parental pain, though these effect sizes were small (Stone & Walker, 2017). In another study that involved experimental manipulation of the parents’ pain behavior during a cold pressor task, parents’ exaggeration of pain behavior resulted in increased child report of anxiety symptoms (Boerner et al., 2017). Combining insights from observational learning and the generalized hypervigilance hypothesis (McDermid et al., 1996), these findings suggest that adolescents who witness parental pain behavior and parents’ expressed beliefs about pain might become more attentive to their bodily sensations, including pain and somatic symptoms, and develop attentional biases towards pain threats (Beck et al., 2011; Stone & Walker, 2017; Williams et al., 2011). As a result, they might likely report many somatic symptoms and adopt similar pain behaviors and beliefs to their parents via observational learning.
An important strength of this study is examining how often adolescents noticed parental pain behavior and how this related to their own somatic symptoms. Prior research has identified parental pain behavior and parent pain beliefs as critical factors in adolescent pain and somatic symptom report (Palermo et al., 2014; Rousseau et al., 2014; Walker et al., 2006); however, the majority of this research only examined the parents’ self-report of their pain behavior and did not assess whether children observed their parents’ pain behavior. The extent to which adolescents notice and interpret parents’ pain behaviors is not well understood, as measures to study adolescents’ observation of parental pain behavior have only recently been developed, leaving room for further investigation (Stone & Walker, 2017).
Limitations and Future Directions
Several limitations should be noted for this study. Because analyses were cross-sectional, causality and developmental trajectories cannot be inferred; however, the findings demonstrate that these associations are already present prior to menarche. Age- and puberty-related effects should be interpreted as concurrent associations rather than maturational change. Although a community sample was recruited, the composition of the study sample largely reflected the demographics of neighborhood surrounding the medical institution where data collection occurred, which included a high proportion of White individuals, affluent families, highly educated parents, and an English-speaking population. Though our community-based approach could have yielded better diversity than a clinical sample, the present study sample limits the generalization of this research beyond the sample’s privileged realm. Using a community sample may also explain the relatively small effect sizes in this study. Contrary to clinical samples, non-selected community samples of adolescents tend to have lower scores across psychological, sensory sensitivity, and somatic symptom variables.
Many aspects of the parent-child interactions and social learning around pain experiences warrant further investigation beyond the current study. Future research might explore the extent to which observations of parental pain behavior impact the self-reported experience of somatic symptoms. Additionally, although the impact of parental pain behavior scores is indicative of parental environmental influence, there may also be genetic mechanisms that contribute to pain risk (Mogil, 2021). In sum, future research should examine adolescents’ observation of parental pain behavior to understand the impact of observational learning on somatic symptoms rather than draw conclusions about adolescent pain and somatic symptoms solely based on a parental perspective.
Conclusion
Depression, anxiety, visceral sensitivity, and observations of parental pain behavior were significantly positively associated with somatic symptoms in premenarchal adolescents. While additional research is needed to further establish and extend the generalizability of the findings, the present study has identified possible avenues for intervention. These results suggest that early adolescence—before the onset of menarche—may be a sensitive period in which emotional distress, heightened interoceptive sensitivity, and family modeling processes converge to shape emerging symptom patterns. Because anxiety and depression showed the strongest associations with somatic symptoms, prevention and intervention efforts in this developmental window may benefit from targeting emotion regulation and stress management skills. Family-based approaches that address parental modeling of pain behavior may further reduce risk by interrupting social learning pathways that reinforce symptom attention. Given that psychological factors, including anxiety and depression, had the most robust relations to somatic symptoms, future studies developing therapeutic interventions should consider targeting psychological symptoms as an early point of intervention. Notably, functional abdominal pain patients who reported many somatic symptoms had better reductions in pain with cognitive behavioral therapy (CBT) than subgroups that reported fewer somatic symptoms (Walker et al., 2021). Family-based approaches may further reduce risk by addressing parental modeling of pain behavior, which was significantly related to somatic symptoms and demonstrated a stronger association than sensory sensitivity. In parallel, for adolescents exhibiting multimodal hypersensitivity, complementary intervention strategies targeting sensory processing may be warranted. Indeed, desensitization-based interventions and occupational therapy approaches have demonstrated efficacy in pediatric pain populations characterized by heightened multisensory sensitivity (Walia et al., 2024). In addition, adolescents’ observation of parental pain behavior was significantly positively related to somatic symptoms and had a more substantial effect relative to sensory sensitivity. Together, these findings underscore the importance of developmentally informed, phenotype-sensitive interventions that integrate psychological symptom management with family-contextual and sensory-targeted approaches.
Footnotes
Acknowledgements
The authors thank Dr. GF Gebhart for advice on study design, interpretation, and editorial assistance. They are also grateful to our laboratory staff for performing the sensory testing assessments and to the study participants for their contributions.
Ethical Considerations
Approval for this study was obtained from the NorthShore University HealthSystem’s (now Endeavor Health) Institutional Review Board (EH17-338, Sept 10, 2018).
Consent to Participate
At the initial study visit, a parent/guardian signed a consent form, and their child signed an assent form before participation.
Author contributions
We prepared this statement according to CRediT (Contributor Roles Taxonomy). Genevieve E. Roth: Conceptualization (equal), Data curation (equal), Formal Analysis (lead), Investigation (supporting), Methodology (equal), Project administration (supporting), Writing—original draft preparation (lead), Writing—review & editing (lead). Katherine M. Jabaay: Conceptualization (supporting), Writing—original draft (supporting), Writing—review & editing (supporting). Rebecca L. Silton: Conceptualization (supporting), Formal Analysis (supporting), Methodology (supporting), Supervision (supporting), Writing—original draft (supporting), Writing—review & editing (supporting). Frank F. Tu: Conceptualization (supporting), Funding acquisition (equal), Methodology (supporting), Supervision (equal), Resources (equal), Writing—review & editing (supporting). Lynn S. Walker: Conceptualization (supporting), Methodology (supporting), Writing—review & editing (supporting). Amy M. Bohnert: Conceptualization (supporting), Methodology (supporting), Writing—review & editing (supporting). Matthew J. Kmiecik: Conceptualization (supporting), Data curation (equal), Formal Analysis (equal), Writing—review & editing (supporting). Kevin M. Hellman: Conceptualization (equal), Data curation (equal), Formal Analysis (equal), Funding acquisition (equal), Methodology (equal), Supervision (equal), Resources (equal), Writing—original draft (equal), Writing—review & editing (equal).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) under grant number (R01 HD098193, R01 HD096332).
Declaration of conflicting interests
Frank F. Tu reports royalties from Wolters Kluwer and grant support from Dot Laboratories and Myovant outside the submitted work. The remaining authors have no conflicts of interest to declare.
Data Availability Statement
The data that support the findings of this study are openly available in OSF at https://doi.org/10.17605/OSF.IO/PBVHQ, reference number PBVHQ (Hellman, 2024).