
Abstract
Girls are vulnerable to HIV in part because the social systems in which they live have failed to support and protect them. The goal of this research was to develop a viable supportive community index and test its association with intermediate variables associated with HIV risk across 16 communities in Botswana, Malawi, and Mozambique. This cross-sectional survey with separate samples randomly drawn in each country (2010) yielded a total sample of 1,418 adolescent girls (aged 11–18). Multilevel, multivariate logistic regression, while controlling for vulnerability, age, religion, and residence, found that an increase in supportive community index is positively associated with the odds of indicating improved community support for girls and with the confidence to refuse unwanted sex with a boyfriend across the three countries, as well as with self-efficacy to insist on condom use in Botswana and Mozambique. Program implementers and decision makers alike can use the supportive community index to identify and measure structural factors associated with girls’ vulnerability to HIV/AIDS; this will potentially contribute to judicious decision making regarding resource allocation to enhance community-level, protective factors for adolescent girls.
Background
Over the past decade, scholars and practitioners alike have come to recognize that social structures are instrumental in the transmission of HIV and, when appropriately brought into play, could become key to HIV prevention.1–4 In the field of HIV prevention, structural factors that influence the social determinants of HIV include policies, laws, and regulations as well as the social, economic, and environmental conditions that affect human agency, or the ability to take action to protect oneself or others from transmission. Examples of structural interventions in the HIV prevention arena include efforts to bring about policy or legal changes, enable community mobilization, or increase access to essential resources such as income, employment, education, or housing. Although attention to the key role of social structures in the incidence of HIV is not new, 5 it was only with the call for HIV combination prevention, which includes not only biomedical and behavioral interventions but also structural approaches, that more explicit calls for research regarding the role of structures and support for structural interventions to address those factors became widespread.4,6,7
A review of the literature revealed a range of structural factors that have been linked to HIV prevention, and thus lower levels of vulnerability, including access to health-care services, 8 community cohesion and safety,9,10 economic opportunities,11,12 and school safety. 13 Factors associated with exacerbating girls’ vulnerability include weak alcohol regulation with easy access for adolescents 14 and sexual abuse. 15 These, then, are some of the structural areas that should be included in a vulnerable girls index (VGI). Indeed, even though the historical preponderance of biomedical and behavioral research in the HIV prevention arena 16 underlies the focus on individual-level factors,17,18 important inroads have been made in the assessment of structural factors and HIV vulnerability, such as a study of the effects of conditional cash transfers for girls in Malawi, 11 needle and syringe exchange programs, 19 or, more broadly, a study of the association between the accumulation of co-occurring structural vulnerabilities and HIV-risk behaviors. 20
As recognition of the importance of structural factors in HIV prevention evolves, the need for measures to assess such factors grows.1,21,22 To that end, the authors of this study developed the vulnerable girls supportive community index (VGSCI), a unique index designed to assess the level of community support for vulnerable girls as perceived by girls. The index is designed both to measure the extent to which structural factors mitigate or augment girls’ vulnerability to HIV prior to the development of interventions and to test intervention effects during and after implementation. This article elucidates the conceptual framework that guided the study, describes the development of the index, and examines the utility of the index across three countries.
Conceptual Framework
Social structure is of key importance because it is manifested in the life chances of individuals and groups. Indeed, Max Weber 23 contended that “[life] chance is socially determined and social structure is an arrangement of chances”; 24 thus, life chances are beyond individuals’ control. Still, according to Weber, individuals can and do make deliberate choices (human agency) based on their interpretation of any given situation but cautioned that those choices are constrained or enabled by chance or the social structure within which the individual lives. 24 This is not to suggest that individual action is structurally predetermined, but that social structure has a powerful influence on individuals’ thoughts, self-efficacy, decisions, and actions.
The supportive effects of community-level factors on individual actions has been explored and confirmed in other studies. For example, a study of community cohesion in Zambia found that community cohesion was positively associated with HIV testing at the individual level. 25 And more broadly, the effects of social and community-level factors on both the rate and the type of HIV transmission are elaborated by Campbell and Mzaidume. 26
In light of this theoretical understanding and evidence from the field, a confluence of extra-individual factors in tandem with individual choices is hypothesized to determine any given girls’ vulnerability to HIV. A social ecological perspective, 27 which views individuals as nested within a system of sociocultural relationships—families, social networks, communities, nations—that potentially influence, directly or indirectly, individuals’ ability or propensity to act, informed the development of the index. In short, individuals’ choices, decisions, and actions are theorized to depend not only on their own characteristics but also on group- or community-level attributes, thus implicating the larger social and environmental contexts within which they live. Thus, policies and laws, resource availability, community support for girls, social support from parents and other community members, and girls’ normative constructs all shape the degree to which girls are vulnerable to HIV are included in the VGSCI (see Measures section for a detailed explanation regarding index development).
To validate the index, it was necessary to demonstrate that the VGSCI predicts the hypothesized outcomes. We assess the relationship between girls’ perceptions that community support for them had increased over the past year, girls’ confidence to ask a partner to use condom, and girls’ confidence to refuse sexual intercourse with a boyfriend and the VGSCI, while controlling for socioeconomic status (SES) variables.
This is the first study to test the correlation between contextual domains (represented in the VGSCI), individual perceptions, and self-efficacy in an attempt to measure structural change theorized to be related to HIV prevention. There are analogous precedents, however, in the family planning and HIV prevention literature, which has found that ideational factors, including family planning knowledge, attitudes, and social norms predict family planning behavior, holding SES variables constant, 28 and that ideation related to condom use predicts self-reported condom use. 29 Even as ideation forms a type of intrapersonal context for individual behavior, perceptions about the community’s concerns, access to services, opportunities, and regulations constitute the context for community action. While the two notions are not equivalent, they are analogous.
The guiding hypothesis of this study is that the VGSCI will be (a) significantly associated with girls’ perceptions that the community in which they live is supportive; and a significant predictor of (b) adolescent girls’ perceptions regarding their self-efficacy to take protective action by insisting on condom use and (c) refusing unwanted sex. We rely on Bandura’s 30 definition of self-efficacy: “judgments of how well one can execute courses of action required to deal with prospective situations.” Self-efficacy to use condoms 31 and to refuse sex, 32 both strong predictors of the associated outcomes are used as dependent variables because of the low levels of sexual debut in Botswana and Malawi.
Data and Methods
Design and Participants
The data for this article are from a quasi-experimental, separate-sample posttest design. The communities for this study were purposively selected. Communities were selected based on a set of predetermined criteria, including 15% to 25% HIV prevalence, population size of approximately 5,000, geographic accessibility, and availability of relevant nongovernmental organizations to implement the program components. Half of the 16 communities included were peri-urban and half were rural: four communities in the Thyolo district in Malawi, four communities in the Francistown district of Botswana, and eight in Mozambique (four in Zambezia and four in Nampula province). None of the communities served as control communities in the program or the study.
This quantitative, interviewer-administered survey-based study was conducted between September and December 2010. In each study community, complete household (HH) listings were conducted prior to sample selection. In the next stage, HHs were randomly selected from the HH lists and, lastly, an adolescent girl was sampled from each HH using the Kish grid for random selection. Female interviewers conducted the interviews, which lasted 45 to 60 minutes, in the local language of each community and in a location selected by each girl for comfort and privacy. Separate samples were drawn for each country resulting in a total sample of 1,418 adolescent girls aged 11 to 18: 401 in Botswana, 414 in Malawi, and 603 in Mozambique (the sample share is larger in Mozambique due to the larger number of communities sampled in that country).
Measures
Independent variables
Vulnerable girls supportive community index
The main independent variable in this analysis is the VGSCI. To create the VGSCI, the research team turned to the previously cited literature regarding structural factors that are implicated in girls’ susceptibility to HIV together with the literature on community capacity and community support.33,34 From these references, domains integral to safeguarding girls’ health and reducing their vulnerability to HIV were identified. Broadly speaking, the VGSCI domains include community concerns for the well-being of its members, access to key services, and the existence and enforcement of regulations—or what could be described as “contextual” domains. For each domain, two or more indicators were developed, and question(s) for each were included in the questionnaires.
Girls Supportive Community Index (SCI) Domains, Questions, and Response Options.

Each domain within the VGSCI was standardized. The purpose of standardization was to make each domain equivalent since the number of variables per domain varied. For purposes of making one overall VGSCI score, each standardized domain score was dichotomized—either at the midpoint if the domain was normally distributed or at the median if it was not normally distributed. The respondent was then assigned a 0 if the domain score was below the cutoff and a 1 if above the cutoff. The domain scores were then summed to create the overall VGSCI. Parenthetically, it is worth noting that the component parts of indices, unlike scales, are not necessarily correlated. 39 Therefore, we do not report the correlation among the items.
The other background variables adjusted for in this analysis include vulnerability (VGI score), age, religion, and residence.
Vulnerable girls index
In addition to the VGSCI, which focuses on the community and structural levels, the research team developed an index to measure family- or HH-level factors over which adolescent girls have limited or no control but that are statistically associated in the literature with HIV infection, or for purposes of this study, with vulnerability to HIV. These factors include orphanhood and HH composition,12,40 migration,41,42 social isolation,43,44 school attendance,42,45 SES,12,46 and poor communication with parents. 12 Based on the aforementioned factors, the VGI was designed to assess girls’ vulnerability to HIV. The index comprises 13 indicators: maternal orphan, paternal orphan, never attended school, not currently in school, lives in an impoverished HH (falls within the two lowest, country-specific wealth quintiles), lives in a child-headed HH, often goes to bed hungry, has often slept without an adult in the HH in the past 12 months, recent migrant, has no close female friends, identified no caring adult, poor relationship with mom or female guardian, and poor relationship with dad or male guardian. The VGI is an unweighted sum of the component items; it was created by assigning respondents one point for each of the indicators mentioned above. Thus, the higher the score, the more vulnerable the girl is.
Wealth quintiles
To create the wealth variable for each country, principal components analysis on ownership of 10 HH assets (electricity, radio, television, telephone, refrigerator, bicycle, motorcycle, car or truck, agricultural land, and livestock), three types of housing material (floor, roof, and wall), and the types of toilet and drinking water were utilized to categorize wealth into quintiles: low, second, middle, fourth, and high. Wealth was further delineated into poor, the two lowest wealth quintiles, and not poor, the upper three wealth quintiles, for inclusion in the VGI.
Dependent variables
To validate the VGSCI, it was necessary to demonstrate that the VGSCI predicts the hypothesized outcomes while controlling for socioeconomic variables. The hypothesized outcomes are the perception that the “situation of girls has improved over the past year” (response options are improved, stayed the same, worsened, or don’t know; coded improved as yes and all other responses as no), whether they were confident (self-efficacy) that they could “ask a sexual partner to use a condom” (response options are no, yes, or don’t know; coded as yes and all other responses as no), and “refuse unwanted sex with a boyfriend” (response options are no, yes, or don’t know; dichotomized as yes and all other responses as no).
Data Analysis
To determine statistical significance in bivariate analyses, chi-square tests of differences in proportions and Student’s t-tests for the difference in means were utilized. Bivariate logistic regression analyses were conducted to assess the relationship between the dependent variable and each independent variable. Multivariate logistic regression analyses were conducted to determine whether confounding accounted for significant differences in the bivariate analyses. The bivariate and multivariate regression analyses was also multilevel, to account for unobserved differences at the community level within each of the three countries. All variables included in the analysis are measured at the individual level except for the community residence variable used in the multilevel modeling. Stata/SE 12.1 was utilized for the analysis.
First, the prevalence of each indicator in the VGSCI, and overall, across the countries was assessed. Next, the multilevel, bivariate association between the dependent and independent variables were assessed. Finally, the multilevel, multivariate association between the dependent and independent variables were assessed, controlling for the potential confounders: vulnerability, age, religion, and residence.
Ethical Procedures
Ethical approval to conduct the two studies was obtained from the institutional review board at the Bloomberg School of Public Health, Johns Hopkins University, the Health Research Unit in the Ministry of Health in Botswana, the National Health Science Research Committee in Malawi, and the National Bioethics Committee, Ministry of Health in Mozambique. The support of community leaders was also obtained at the local level.
Informed parental consent for study participation was obtained from parents or guardians of adolescent girls aged 11 to 17 at their home. The adolescent girls aged 11 to 17 assented to study participation. Adolescent girls aged 18 consented to study participation. Both the adult consent and adolescent assent or consent were oral as opposed to written. Survey instruments were developed in English, translated into Batswana (Botswana), Chichewa (Malawi), and Portuguese (Mozambique) and back-translated for accuracy. Pretests were conducted first in Malawi for purposes of question flow; changes were made as necessary and conveyed to research teams in the other countries. Pretests were then conducted in Botswana and Mozambique for purposes of language clarity; changes were made after conferring with the teams across the three countries to ensure that the meanings had not changed.
Results
VGSCI Domains
Vulnerable Girls Supportive Community Index Prevalence Above the Mean by Domain and Overall Mean in Program Areas of Botswana, Malawi, and Mozambique, 2010.
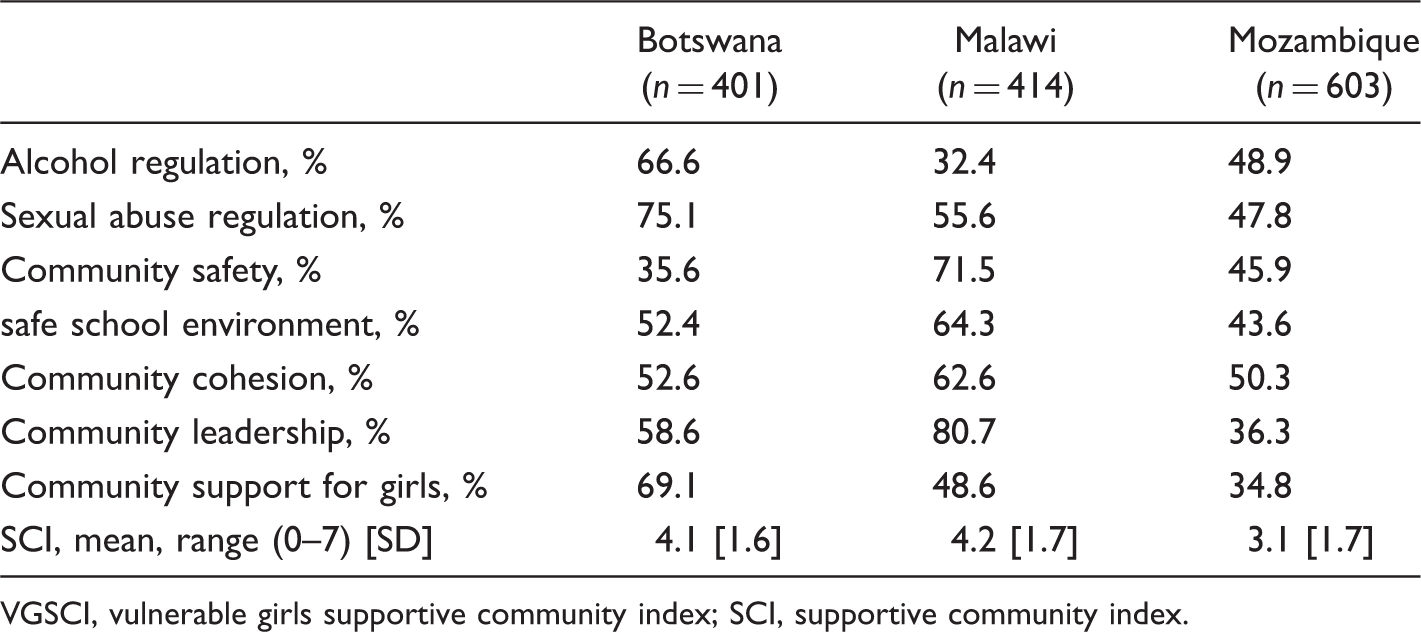
VGSCI, vulnerable girls supportive community index; SCI, supportive community index.
The Situation of Girls Has Improved
In the bivariate analysis, the VGSCI is significantly associated with indicating the situation of girls has improved over the past year in all three countries—the higher the VGSCI score the more likely to indicate the positive outcome. A lower VGI score and younger age were also associated with indicating the situation of girls had improved in the past year (data not shown).
Multilevel, Bivariate and Multivariate Logistic Regression Assessing the Relationship Between Sociodemographic Characteristics, the Vulnerable Girls Supportive Community Index, Vulnerable Girls Index, and Indicating the Situation of Girls Has Improved in the Community Among Girls in Selected Areas of Botswana, Malawi, and Mozambique, 2010.
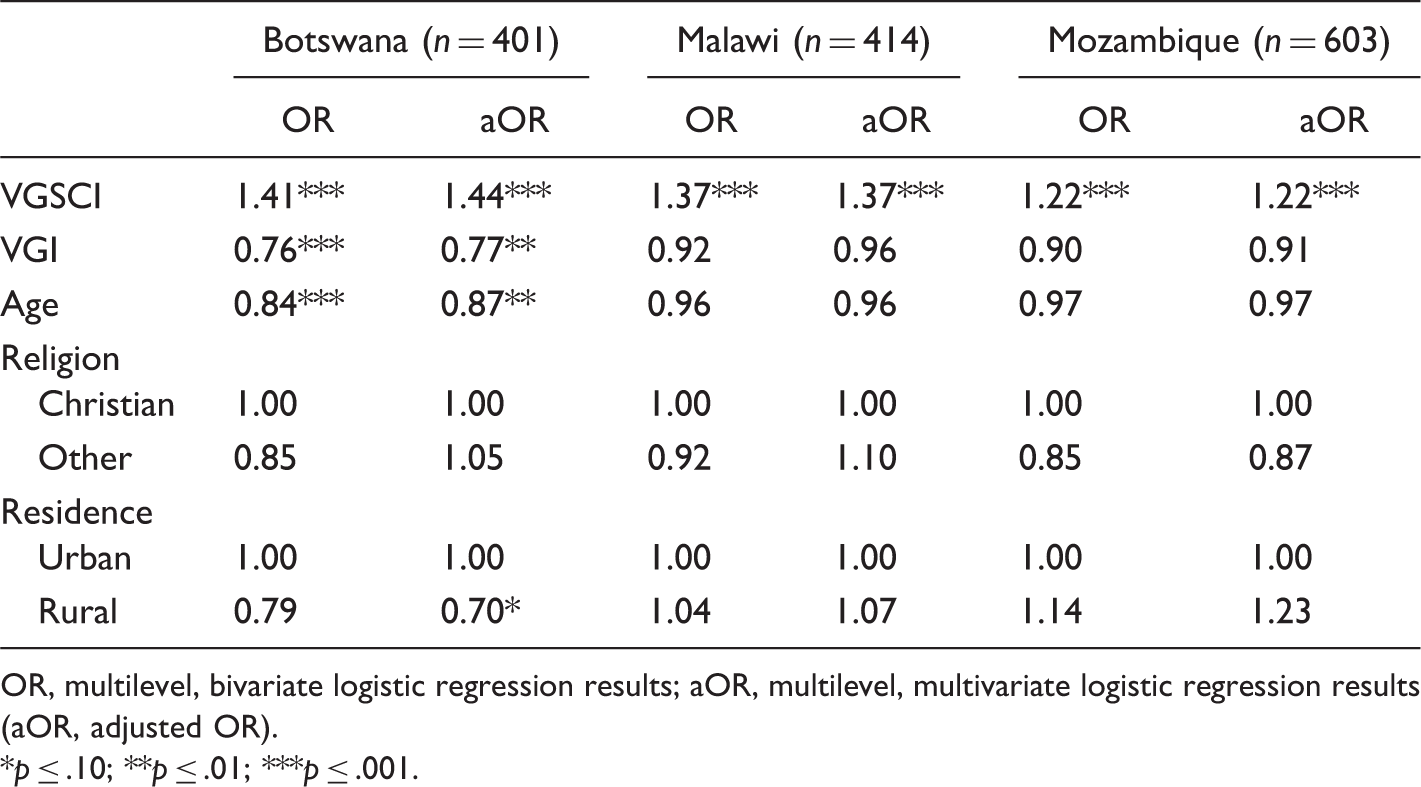
OR, multilevel, bivariate logistic regression results; aOR, multilevel, multivariate logistic regression results (aOR, adjusted OR).
p ≤ .10; **p ≤ .01; ***p ≤ .001.
Self-Efficacy to Ask a Partner to Use a Condom
In the bivariate analysis, the VGSCI is significantly associated with indicating the self-efficacy to ask a partner to use a condom in Mozambique. A lower VGI score in Botswana and Mozambique, and older age in all three countries were also associated with the self-efficacy to ask a partner to use a condom in the bivariate analysis (data not shown).
Multilevel, Bivariate and Multivariate Logistic Regression Assessing the Relationship Between the Vulnerable Girls Supportive Community Index, Vulnerable Girls Index, Sociodemographic Characteristics, and Indicating the Confidence to Ask a Sexual Partner to Use a Condom Among Girls in Selected Areas of Botswana, Malawi, and Mozambique, 2010.
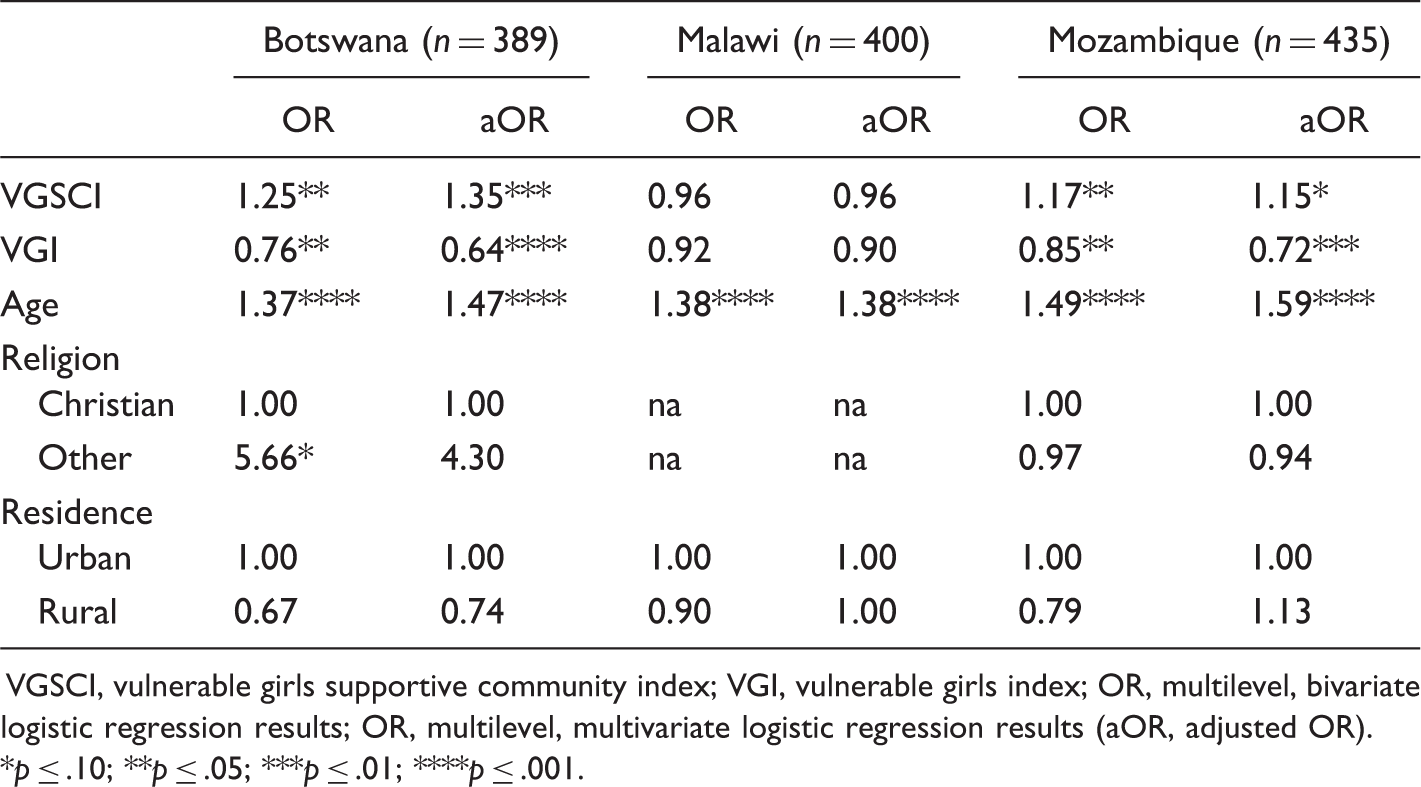
VGSCI, vulnerable girls supportive community index; VGI, vulnerable girls index; OR, multilevel, bivariate logistic regression results; OR, multilevel, multivariate logistic regression results (aOR, adjusted OR).
p ≤ .10; **p ≤ .05; ***p ≤ .01; ****p ≤ .001.
Self-Efficacy to Refuse Sex With a Boyfriend
In the bivariate analysis, a higher VGSCI was significantly associated with indicating the self-efficacy to refuse sex with a boyfriend in all three countries. A lower VGI score in all three countries, younger age in Malawi, and identifying as Christian in Mozambique, were also associated with the self-efficacy to refuse sex with a boyfriend in the bivariate analysis (data not shown).
Multilevel, Bivariate and Multivariate Logistic Regression Assessing the Relationship Between the Vulnerable Girls Supportive Community Index, Vulnerable Girls Index, Sociodemographic Characteristics, and Indicating the Confidence to Refuse Sexual Intercourse With a Boyfriend Among Girls in Intervention Areas of Botswana, Malawi, and Mozambique, 2010.
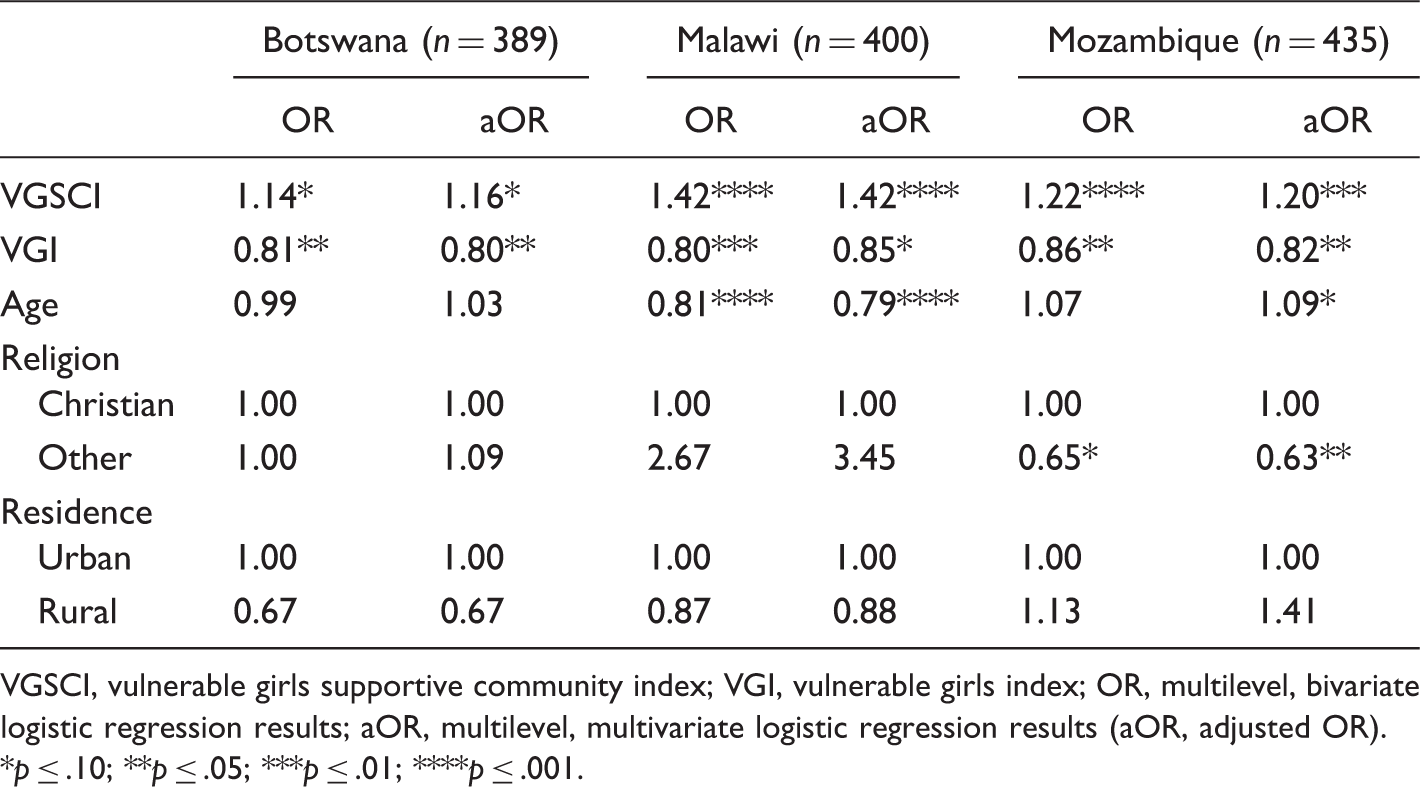
VGSCI, vulnerable girls supportive community index; VGI, vulnerable girls index; OR, multilevel, bivariate logistic regression results; aOR, multilevel, multivariate logistic regression results (aOR, adjusted OR).
p ≤ .10; **p ≤ .05; ***p ≤ .01; ****p ≤ .001.
Discussion
The VGSCI brings structure clearly to the forefront of girls’ vulnerability by demonstrating that community concerns, access, opportunities, and regulations are associated with intermediate predictors among vulnerable adolescent girls. Across the three countries, an increase in the VGSCI was associated with increased odds that adolescent girls perceived that the situation of girls had improved over the previous year and the efficacy to refuse unwanted sex with a boyfriend. In Botswana and Mozambique, one middle- and one low-income country, the odds indicating an efficacy to use condoms increased with each increase in VGSCI score. Yet, this finding did not hold in Malawi. The ability to insist on condom use would arguably require greater negotiating skills and greater self-efficacy than would the ability to refuse unwanted sex with a boyfriend. Further research is needed to develop a clearer understanding of which community-level factors need to be strengthened to enable greater self-efficacy during intimate relations.
The VGSCI responds directly to the recent call for tools to measure structural changes. 21 These findings point to and reconfirm the fact that social structure has a powerful influence on individuals’ agency, as Weber asseverated. 23 Thus, action must be taken not only at the individual level but also at the family and community levels to reduce social vulnerability (Piot, Larson, Zewdie, & Mane, 2008). 47 Doing so will comprehensively address the factors that hamper individuals’ ability to protect themselves and others from HIV infection. Application of the VGSCI can bring to light the central role of extra-individual factors in girls’ susceptibility to HIV. 48 Moreover, use of the VGSCI may help reorient policy makers and programmers alike to allocate resources for, or create interventions that address policy, economic, and social support factors—such as enforcement of alcohol regulation laws, community safety, and community cohesion—as integral to the mitigation of HIV.
While programmers recognize the need to address structural barriers, they feel ill equipped to measure those changes. The VGSCI is a tool that can be utilized to assess structural factors at baseline, change over time, and program-related changes.
Limitations
The communities represented in these findings were purposively selected for implementation purposes so are not necessarily representative of the provinces or countries in which they are located. The samples are cross-sectional; a longitudinal sample design would have been stronger, would have controlled for self-selection bias, and would help address the issues of directionality and causality, which are key weaknesses in correlational studies. Additionally, more nuanced measures of the various components of the indices would likely have strengthened the study. And, finally, community support, as defined and measured herein, is not exhaustive; it would be important to consider other aspects in future studies.
Conclusions
The evidence presented here suggests that the structural factors that constitute the VGSCI are associated with community actions that can be protective of vulnerable girls and are important in mitigating potential threats to their well-being. This is an important contribution to the literature given the acknowledged need for extra-individual measures2,21,26 The availability of this index may encourage broader consideration of community-level factors in research, program design, and policy decisions, as it provides ready indicators for purposes of measurement and intervention.
Existing programs can use the VGSCI as a starting point to measure current or posttest levels of community support and the association between community support and community actions to protect vulnerable girls. Future programs can use the VGSCI to measure the pretest levels of community support prior to program implementation, identify areas that need programmatic support, and measure the effect of interventions aimed at strengthening community and structural support. And governments can use the VGSCI as a starting point to assess community support for girls. Although not exhaustive, the information provided by the VGSCI could help governments identify areas in their respective countries to allocate additional resources for sustained community support for girls.
While these findings are important, the next step is to demonstrate that high VGSCI scores not only lead to protective perceptions and self-efficacy to take protective action, but that those perceptions are associated with decreases in the proximal determinants of girls’ vulnerability to HIV—or exposure to unprotected sex—in the sub-Saharan African context and beyond.
The VGSCI is unique and has been tested in this study, yet validation and refinement are required. This is likely to entail augmentation of the domains, expansion to other population groups, and application of the VGSCI to additional health fields. Even at this stage, however, researchers and programmers should feel equipped to measure important aspects of structural change using this index. Such applications will provide additional validation and, potentially, encourage funders to support structural-level interventions for improved and sustained health outcomes.
Footnotes
Acknowledgments
The funder did not influence the study design, data collection, data analysis, data interpretation, report writing, or the decision to submit the paper for publication. The contents are the responsibility of the authors and do not necessarily reflect the views of PEPFAR, the United States Government, or the Johns Hopkins University. The authors would like to thank Susan Krenn, Joanna Skinner, Jane Brown, Patricia Poppe, Enni Panizzo, Assana Magombo, and Tinaye Mmusi for their contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research findings elaborated in this article were part of the Go Girls! Initiative, which was funded by the President’s Emergency Plan for AIDS Relief (PEPFAR) and the United States Agency for International Development (USAID) under the terms of Contract No. GHH-I-00-07-00032-00, USAID | Project SEARCH, Task Order 01.