
Abstract
To determine the compliance, barriers, and effects of participation in a 4-week exercise intervention aimed at reducing risk factors for noncommunicable diseases among community-dwelling adults from a low-resourced area of South Africa. An exercise program and associated pre-posttest were performed by 76 participants (men, n = 26 and women, n = 50) aged 35 to 65 years. Baseline and end tests included height, weight, hip and waist circumference, heart rate, blood pressure, glucose, cholesterol, quality of life, and cardiorespiratory fitness measurements. The intervention consisted of 3 days/week combined aerobic and resistance exercise at an intensity of 70% heart rate reserved as determined at baseline. Compliance and barriers to participation were determined post-intervention by means of attendance registers and interviews. ANCOVA with adjustment for pretest was performed for all repeated variables. The Cronbach’s alpha coefficients for exercise benefits were 0.81 and for barriers 0.84. Of the 26 men (40.8 ± 5.45 years) and 50 women (43.6 ± 7.8 years) recruited, 54 completed the intervention (71% compliance). The 4-week aerobic exercise intervention significantly reduced body mass, rate of perceived exertion, and mental components summary in men, and body mass, body mass index, VO2max, rate of perceived exertion, glucose, physical components summary, and mental components summary in women. Participants reported that the exercise milieu as a major barrier to exercise compliance while the interviews reported lack of time. A 1-month exercise intervention elucidated positive changes in risk factors for noncommunicable diseases in a low-resource community. A drop-out rate of 29% in this study is consistent with other exercise intervention trials. Exploration of the reported barriers may be useful for planning to increase compliance with future programs.
Keywords
Introduction
The main goal of Healthy People 2020 is to achieve health equity, eliminate disparities, and improve overall health for all. 1 Consequently, the risk factors linked to noncommunicable diseases (NCDs) as a result of a detrimental lifestyle have been cited several times in literature. 1 The diseases most cited are increased risk of coronary heart disease, Type 2 diabetes, cancer, hypertension, dyslipidaemia, stroke, liver disease, gall-bladder disease, sleep apnoea, respiratory problems and osteoarthritis, low quality of life (QoL), and physical inactivity. 1 Regular physical activity (PA) and exercise is beneficial by improving the overall health and aerobic capacity and minimizing the aforementioned risks factor and chronic diseases of lifestyle.1,2 The World Health Organization (WHO) physical activity guidelines recommend that, adults should accumulate at least 150 minutes per week of moderate intensity PA or 75 minutes of vigorous intensity aerobic PA or a combination of the two. 3 The same guidelines are currently advocated for South Africa. 4 In spite of the guidelines, more than 50% of South Africans are not sufficiently physically active to elucidate health improvement. 5
In conjunction with the high levels of physical inactivity in South Africa, more than 28.5% of all deaths occur from chronic diseases of lifestyle in persons between the age of 35 and 64 years while more than 56% of the population between ages 15 and 64 has at least one modifiable risk factor for chronic disease of lifestyle. 4 South Africa is a country where many communities are still going through rapid epidemiological, nutrition, and demographic transition. 4 It was reported that the level of PA in the urban population mirrored the level of PA in developed nations because South Africa is seen as a sporting nation, 4 the changes in PA levels among the urban populace is not reflected in low-resourced communities due to a lack of facilities,6,7 a safe environment, 8 and poverty. 9 Therefore, based on these barriers, the proportion of the South African population that is participating in PA is decreasing in low-resource communities despite the known benefits of regular PA on health outcomes. However, Healthy People 2020 has specified that physical inactivity needs to be addressed as a matter of urgency in order to decrease the number of adults who do not participate in regular PA. 1
Regular PA at intensities presented by the guidelines improves cardiorespiratory fitness (CRF). 10 In addition, research indicated that PA and CRF are linked to a sound mental ability 11 and functional work capacity. 12 This improvement in mental ability and functional capacity could be linked to the two component summary (mental and physical) of the health-related quality of life (HRQoL) assessment. A known relationships exist between PA and risk factors for chronic diseases of lifestyle; therefore, aerobic PA interventions should be developed and implemented 13 to reduce risk factors for chronic diseases and improve the aerobic capacity and HRQoL of people. Additionally, a community-based physical exercise intervention that targets many individuals coupled with modern exercise recommendations for frequency, intensity, and duration are key to a solution. 13
In a study of Gordon et al., 14 a community-based aerobic exercise training on the functional status and health-related quality of chronic stroke survivors, a randomized controlled trial study involving 64 participants who exercised for 30 minutes, 3 times per week for 12 weeks showed that there was an improvement in the physical components of QoL and fitness levels of the participants. A high-quality systematic review to identify controlled community-based PA interventions published between 2001 and 2012 comprising 55 studies with 20,532 participants reveals that half of the studies reported a positive exercise intervention outcome. 15 Arslan studied the effect of 8-week step-aerobic dance exercise on body composition among 49 healthy sedentary women and found that there were significant improvements in body mass index (BMI), body weight, waist-hip ratio (WHR), waist circumference (WC), fat percentage, lean body mass (LBM), and basal metabolic rate (BMR) in the experimental group after 8 weeks. Regular PA can lead to a significant change by reducing many health risk factors. Ickes and Sharma 1 reviewed existing community-based PA intervention on Hispanic adults between 1988 and 2011 for which family-based and faith-based settings were represented. The report of the review shows that in relation to PA, each of the intervention was successful.
Another important situation which could threaten the recommendations stated earlier are those barriers which could negatively affect adults’ PA participation such as age, income, time, motivation, physique (in terms of obesity and overweight), and poor health perception. 1 These barriers stated earlier could cause a high rate of dropout during a structured aerobic exercise intervention. Nam et al. 17 reported 27% dropped out rate among the participants randomized into exercise intervention group and 10% dropped out rate in control group. It is, therefore, important to consider these challenges and barriers and minimize them. South Africa is a community regarded as a transitional process community for which a development of successful community-based PA interventions is related in parts to overcoming cultural, sociodemographic, physical, and financial barriers to participation. 4 There are thus very few community-based interventions for lifestyle and PA data, with the exception of one regional initiative aimed at increasing participation in PA. This was the Community Health Intervention Programmes (CHIPS) which was organized among privately funded and nonprofit academic institutions and a national insurance company. 4 The program aimed at promoting good health among both adults and children in communities by involving them in regular PA to improve general well-being. 4 Therefore, this study has been specifically designed to examine the compliance, barriers, and effect of a 4-week exercise intervention on risk factors for NCDs among Setswana speaking community-dwelling Potchefstroom adults from a low-resourced area. The findings from this study will form the basis of future PA interventions in other low-resourced communities in South Africa or the rest of Africa to improve PA adherence.
Participants and Methods
Research Design
This was a pretest posttest exercise intervention study primarily designed to determine the compliance, barriers, and effect of aerobic exercise intervention on NCD risk factors among adult Setswana speaking-community-dwellers aged 35 to 65 in a low-resourced community from Potchefstroom.
Participants
A total of 76 men (n = 26) and women (n = 50) aged between 35 and 65 were recruited from the Kenneth Kaunda district, a low-resourced area in Potchefstroom. All the participants gave voluntary, informed consent in writing before participating in the study. The study was approved by the Health Research Ethics Committee for Humans from the North-West University (NWU 00002-14-A1). The participants were asked to provide demographic information: date of birth, age, sex, marital status, current employment status, level of education, type of house in which they live, and household income. Apparently, healthy Setswana-speaking men and women, aged 35 to 65 years, with no orthopedic limitations were included in the study. Persons were considered apparently healthy if they were not taking any chronic medication or diagnosed with any known diseases. Potential participants who showed any signs of chronic disease 18 or answered “yes” to any question on the Physical Activity Readiness Questionnaire (PAR-Q) were asked to see their physician for a letter confirming suitability to participate. However, only participants with a low risk for exercise were included in the study. People with blood pressure higher than 160 mmHg (systolic) or 95 mmHg (diastolic), or had a temperature >37.5℃, as well as pregnant or lactating women, were excluded.
Anthropometric Measurements
Participants’ height, body weight, and body circumference of the waist and hip were measured according to the protocol of the International Society for the Advancement of Kin-anthropometry (ISAK). 19 WHRs were calculated by dividing the waist measurement by the circumference obtained for the hips. 20 BMI was calculated by dividing the weight in kilograms by the square of the height in meters (kg/m2). 21
Blood Pressure and Heart Rate
Resting blood pressure was measured after participants had rested for 10 minutes in a semi-recumbent position. Blood pressure (BP) was measured with a sphygmomanometer (Omron Xinxiang Golden Elephant Sci-Tech Co., Ltd., China) using the Riva-Rocci/Korotkoff method on the left arm. 22 Duplicate measures were taken with a 5-minute resting period between each measurement. The average of the two measurements was used in the statistical analyses. The pulse rate was measured with a stethoscope (3M™ Littmann® Stethoscope, USA) by counting the beats in a set period of 15 seconds and multiplying by 4 to arrive at the number of beats per minute. Maximal heart rate and blood pressure were also measured by the same method immediately at the end of the CRF step test while in a sitting position.
Fasting Peripheral Blood Measurements
Fasting peripheral blood measurements of glucose and total cholesterol were measured by puncturing a finger with a lancet and applying a drop of blood on a strip for automatic analyses with the Accutrend® Plus (Roche, Germany) according to the user’s manual. 23 The calibration of the Accutrend® machine was performed by inserting the code on the meter batch-related strip before taking the first measurement.
Questionnaires
HRQoL short form-8 survey (SF-8)
The South Africa Setswana version of the SF-8, a translated version of the original SF-8, is an eight-itemized questionnaire which measures the following broad domains: Physical Functioning (PF), Role-Physical (RP), Body Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role-Emotional (RE), and Mental Health (MH). The SF-8 has two component measurements, namely, the physical components summary (PCS) and the mental components summary (MCS). The scoring in Setswana version of SF-8 was based on this two-component summary (PCS and MCS) and was calculated by weighting each SF-8 item using a norm-based procedure in the instrument guidelines. The Setswana version of SF-8 was a 5-point and 6-point Likert scale questionnaire, respectively (i.e., the options are either 5 or 6 of which the participant can only select one). The participants were requested to complete the questionnaire during the pretest (baseline) and posttest. The posttest questionnaire was completed 4 weeks after the exercise intervention programme.
Perceived Exercise Benefits and Barriers Scale
Perceived benefit and barrier strengths to participation in exercise were evaluated by the perceived Exercise Benefits And Barriers Scale (EBBS) Questionnaire, which was categorized into two different components (as it reflected in the name above):
the benefits of exercise and the barriers of exercise.
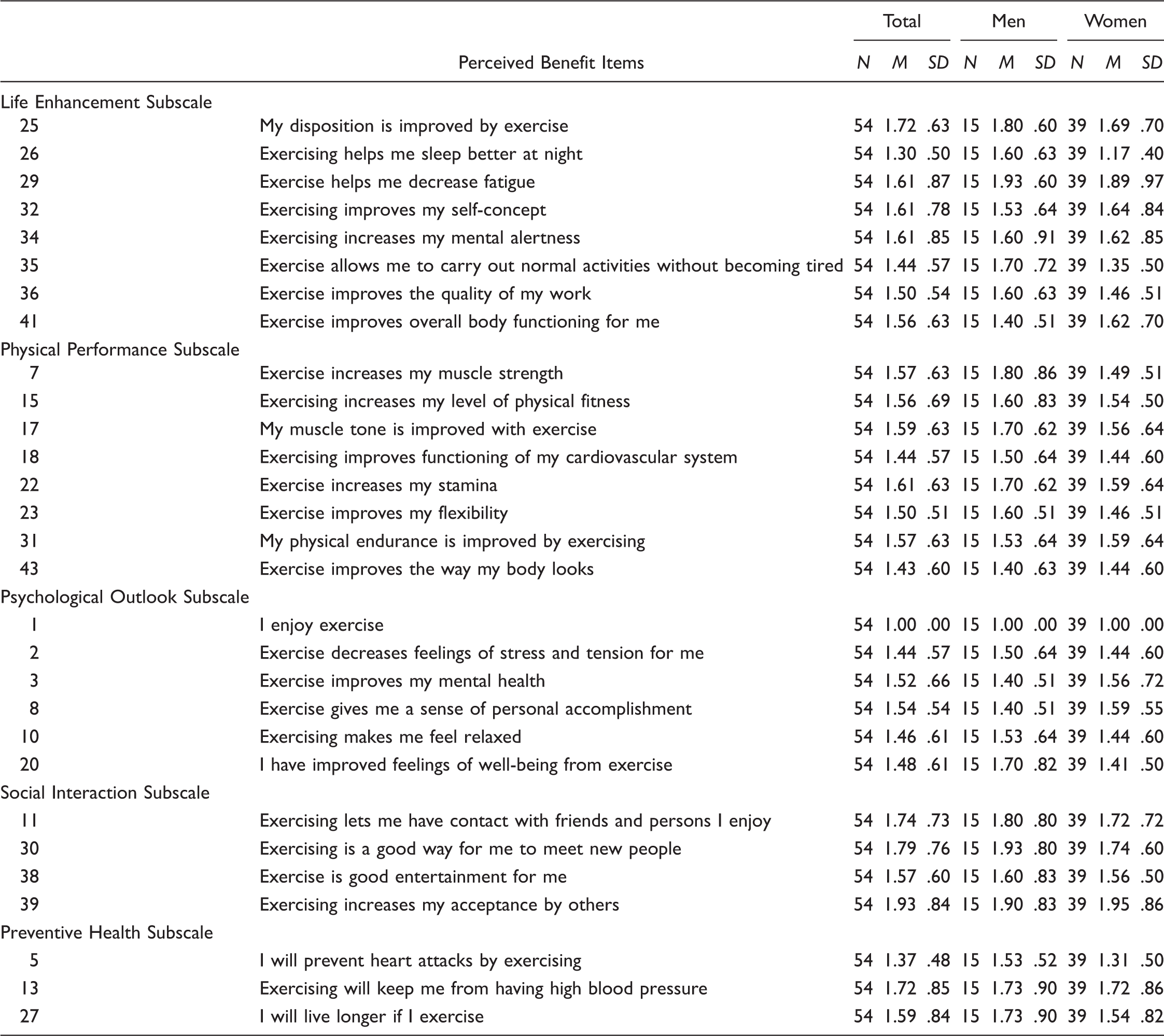
For the exercise benefit category, 29 items were categorized into five subscales which were the following:
life enhancement, physical performance, psychological outlook, social interaction, and preventative health.
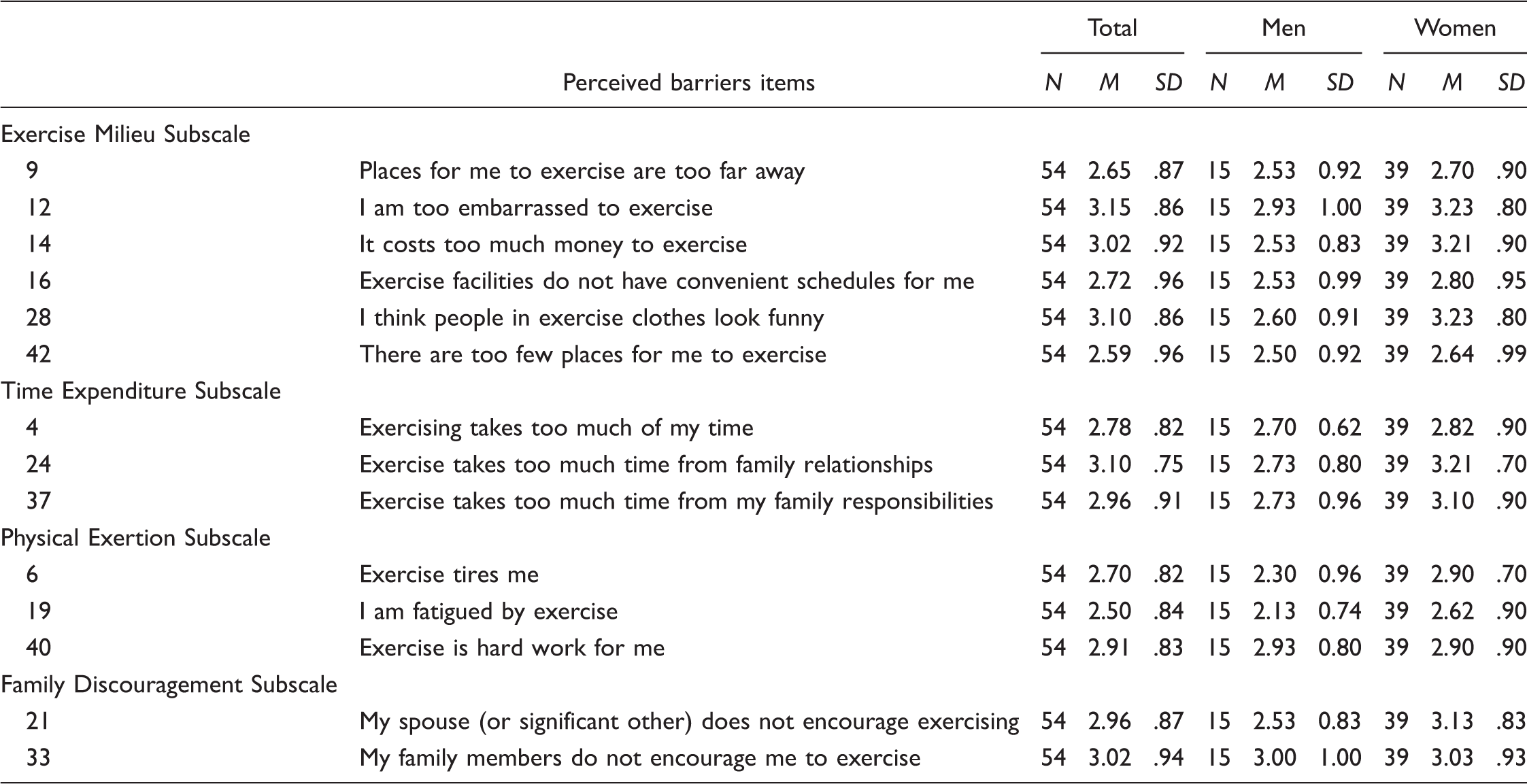
For the exercise barrier category, 14 items were categorized into four subscales which were the following:
exercise milieu, time expenditure, physical exertion, and family discouragement.
Scales and Subscales of the Exercise Benefits/Barriers Questionnaire.
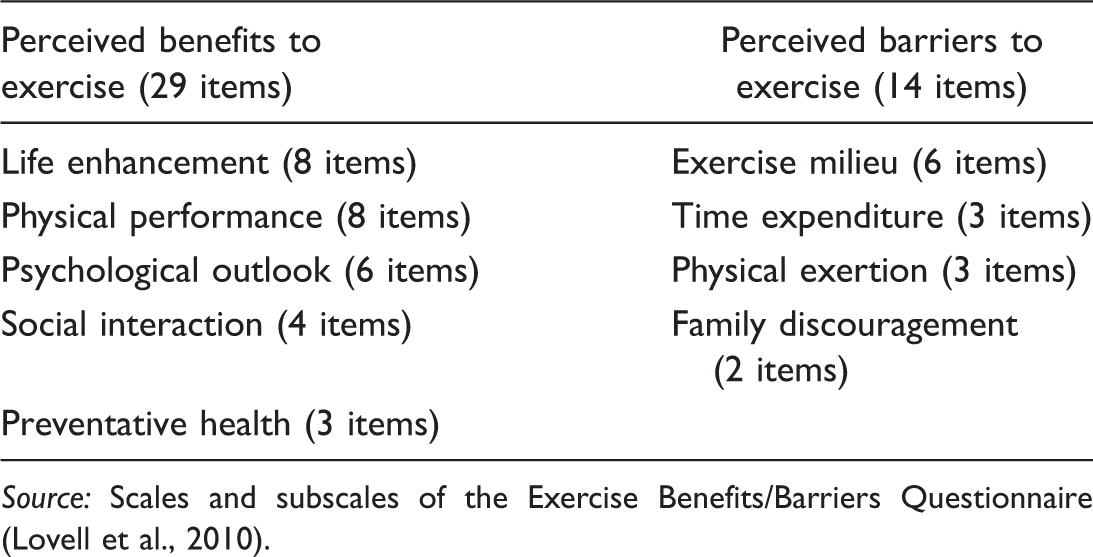
Source: Scales and subscales of the Exercise Benefits/Barriers Questionnaire (Lovell et al., 2010).
Cardio-respiratory fitness measurements
Cardio-respiratory fitness (CRF) by means of an 8-minute step test assisted with a combined heart rate and accelerometry device (Actiheart®, CamNTech, UK) that calculate a predicted CRF in the format of a relative VO2max. 25 The 8-minute step test was performed by stepping on a 21.5 cm box with a speed that ramps linearly from 15 step cycles (one step cycle is “up-up, down-down’’) per minute to 33 step cycles per minute by the end of the test. The stepping speed of the software was dictated by a metronome beat testing each person individually. After the 8-minute step test, the participant was requested to stay seated for 2 minutes without talking in order to determine the recovery heart rate. CRF was estimated relative VO2max in ml/min/kg.
Exercise Intervention
Planning for the exercise intervention programme was based on the findings of the Preferred PA questionnaires, and set at 3 days a week for a period of 4 weeks. The intervention was aimed at obtaining 70% of peak VO2 maximum heart rate during the exercise for a period of 45 minutes. The intervention consisted of 5-minute warm-up, 20 minutes of aerobic exercises, 15 minutes of muscle strength and endurance by means of body weight, and 5 minutes flexibility for cool down. Pulse rate was monitored by counting the pulse at the wrist for 10 seconds during the aerobic exercise intervention and multiplying by six to determine the intensity of the exercise. The Modified Borg scale for rate of perceived exertion (RPE) was used to assess participants’ perceptions of exertion during the aerobic exercise on the 1 to 10 scale. 26 Participants’ compliance to the exercise intervention was determined by means of an attendance register. All the participants raised their heart rates adequately to obtaining VO2max aimed at during the aerobic exercise intervention. Compliance was calculated as a percentage of sessions attended out of the maximum 12 training sessions.
Semi-Structured Interviews
To understand the reasons why people participated or dropped out of the exercise intervention, semi-structured individual interviews were undertaken. Two major interview questions were developed from a brief literature review of the main construct of benefits and barriers for exercise. Questions posed during the interviews were the following:
What is the reason that you attended the programme? What is the reason why you did not participate in the programme?
The interviews (N = 15) were audio recorded with permission. Nine (men = 3, women = 6) participants who completed the exercise intervention and six (men = 2, women = 4) participants who did not complete the exercise intervention were interviewed. The information obtained from the interviews was to obtain an in depth understanding of the perceived benefits and barriers for participation in exercise for which the responses were audio recorded.
Data analyses
Data analyses were carried out using the Statistical Package for Social Science (SPSS) software Version 22.0. 27 All statistical tests were two-tailed, and p ≤ .05 was considered statistically significant. Descriptive statistics, such as mean, SD, and percentages were used to examine the baseline characteristics of the participants. Independent sample t tests were performed to determine the significant difference of the baseline variables between men and women. A normality test for all variables was assessed using the Shapiro-Wilk test. Variables which were not normally distributed were analyzed by Wilcoxon matched-pairs signed-rank test. Variable which were normally distributed (a) were analyzed by a paired sample t test. For the pre- and post-QoL measure, two QoL indicators were used, namely, PCS and MCS, to assess the changes in the QoL components due to the PA intervention. Analysis of covariance (ANCOVA) was performed to determine if the changes from baseline to end were significant, adjusting for baseline (pretest). Internal consistency of the EBBS was assessed using the Cronbach’s alpha coefficient calculated for the scale. A coefficient alpha of 0.70 or greater is generally considered to be acceptable. Furthermore, mean and SD were computed for each subscale of EBBS to allow straight forward comparisons between each subscale. The recordings of the response from the interview were transcribed verbatim to support the real data and trustworthiness and used as a quote using code manager and code family manager and analyzed for major themes using AtlasTi7 (ATLAS.ti Scientific Software Development GmbH, Berlin).
Results
Participants
Of the 76 (100%) participants who enrolled and participated in the first assessment (baseline), only 54 (71%) completed the 4-week aerobic exercise intervention programme (See Figure 1); 22 participants (29%) dropped-out from baseline to end. Their reasons were due to work-related commitments (n = 10), family responsibilities (n = 3), medical problems (n = 3), lack of time and distance to exercise venue (n = 2), and domestic-related injuries (n = 4). Meanwhile, the internal consistencies based on the samples of this current study for benefits scale was 0.81 and barriers scale was 0.84.
Flow of participants during the 4-week exercise intervention.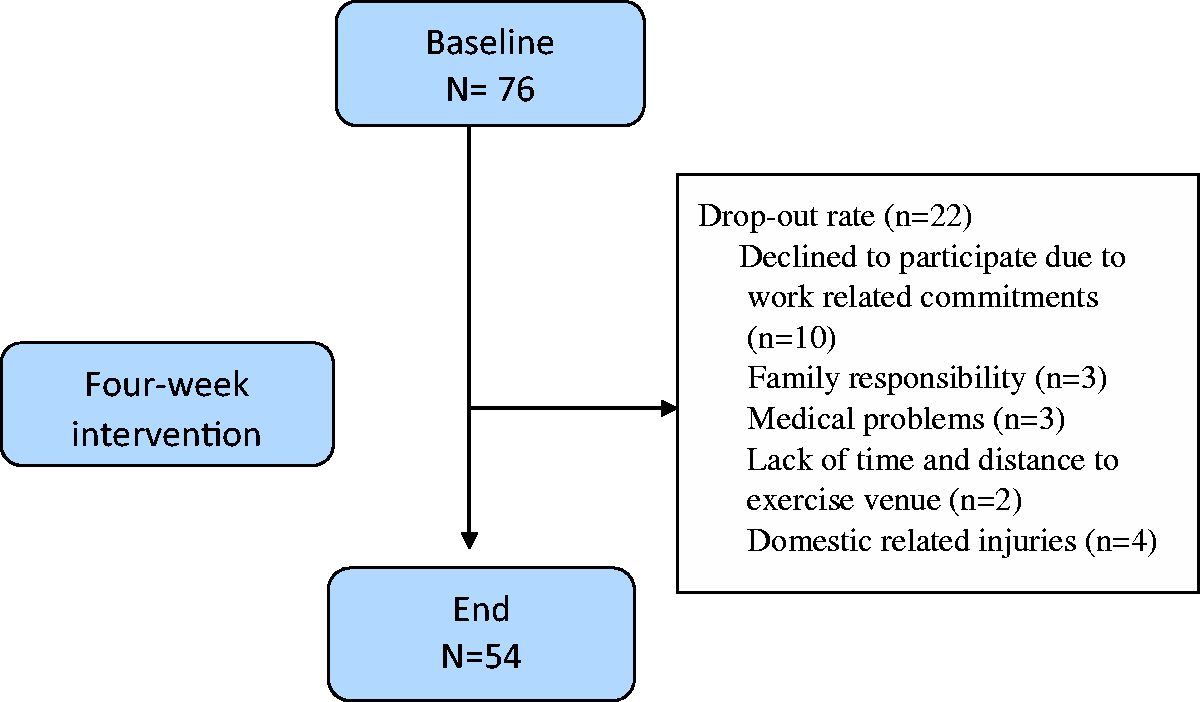
Baseline Characteristics
Baseline Characteristics of the Total Group and Per Gender (M ± SD).
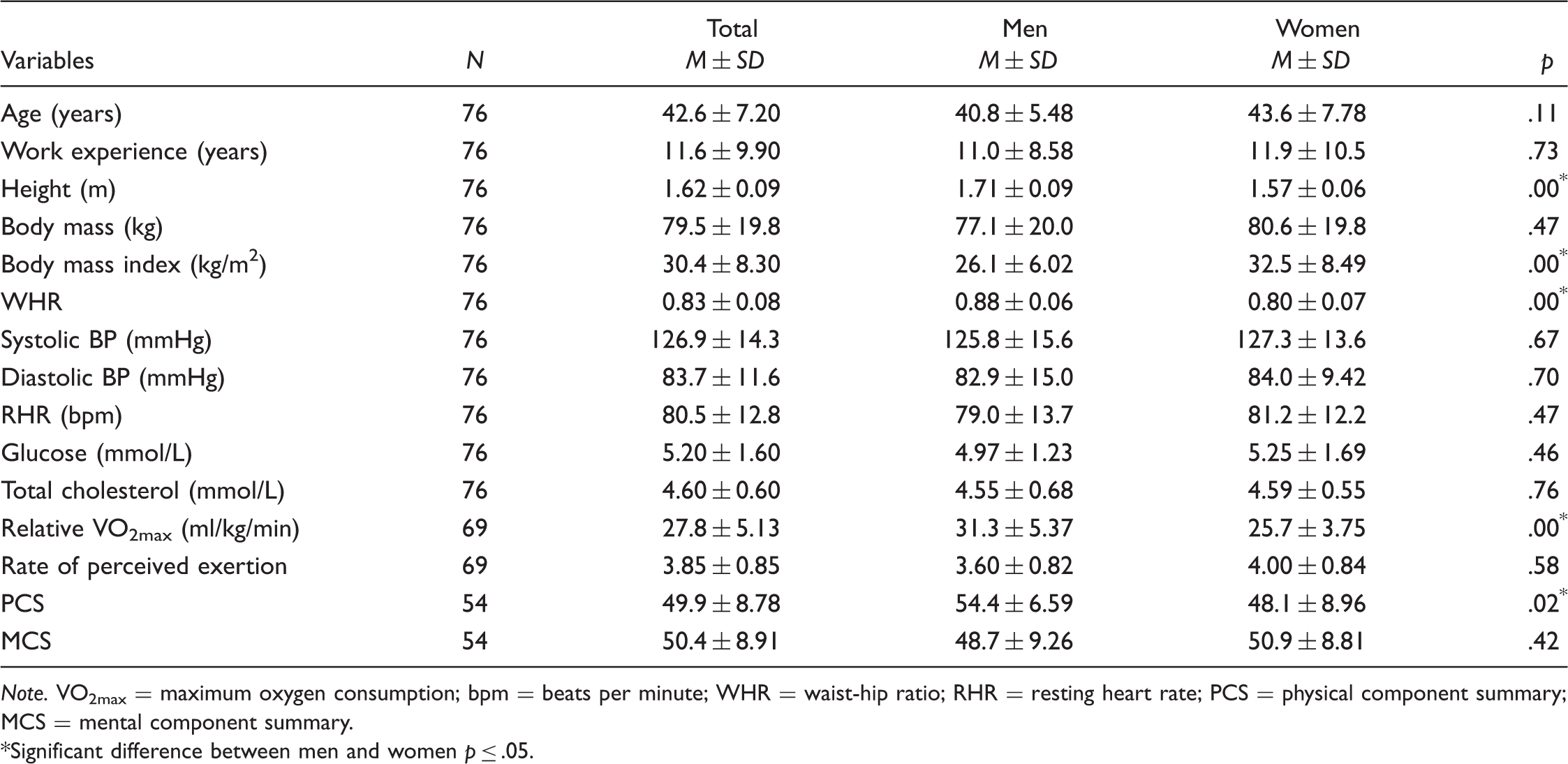
Note. VO2max = maximum oxygen consumption; bpm = beats per minute; WHR = waist-hip ratio; RHR = resting heart rate; PCS = physical component summary; MCS = mental component summary.
Significant difference between men and women p ≤ .05.
The Descriptive Statistics of Changes in Variables From Baseline to End for Men and Women Who Started and Completed the Aerobic Exercise Intervention.
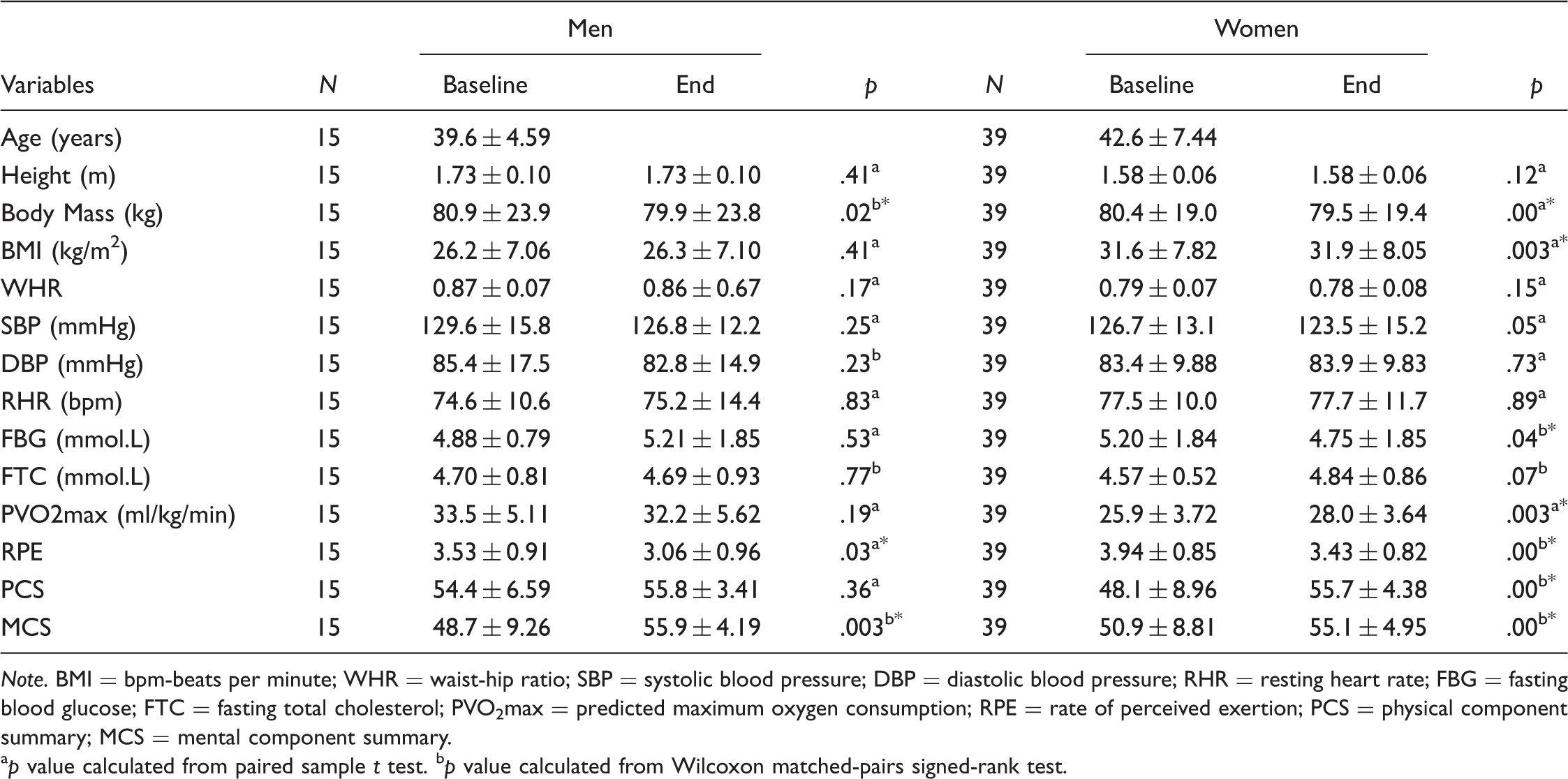
Note. BMI = bpm-beats per minute; WHR = waist-hip ratio; SBP = systolic blood pressure; DBP = diastolic blood pressure; RHR = resting heart rate; FBG = fasting blood glucose; FTC = fasting total cholesterol; PVO2max = predicted maximum oxygen consumption; RPE = rate of perceived exertion; PCS = physical component summary; MCS = mental component summary.
p value calculated from paired sample t test. bp value calculated from Wilcoxon matched-pairs signed-rank test.
The Descriptive Statistics of Changes in HRQoL Variables for Baseline and End for Men and Women who Started and Completed the Aerobic Exercise Intervention.
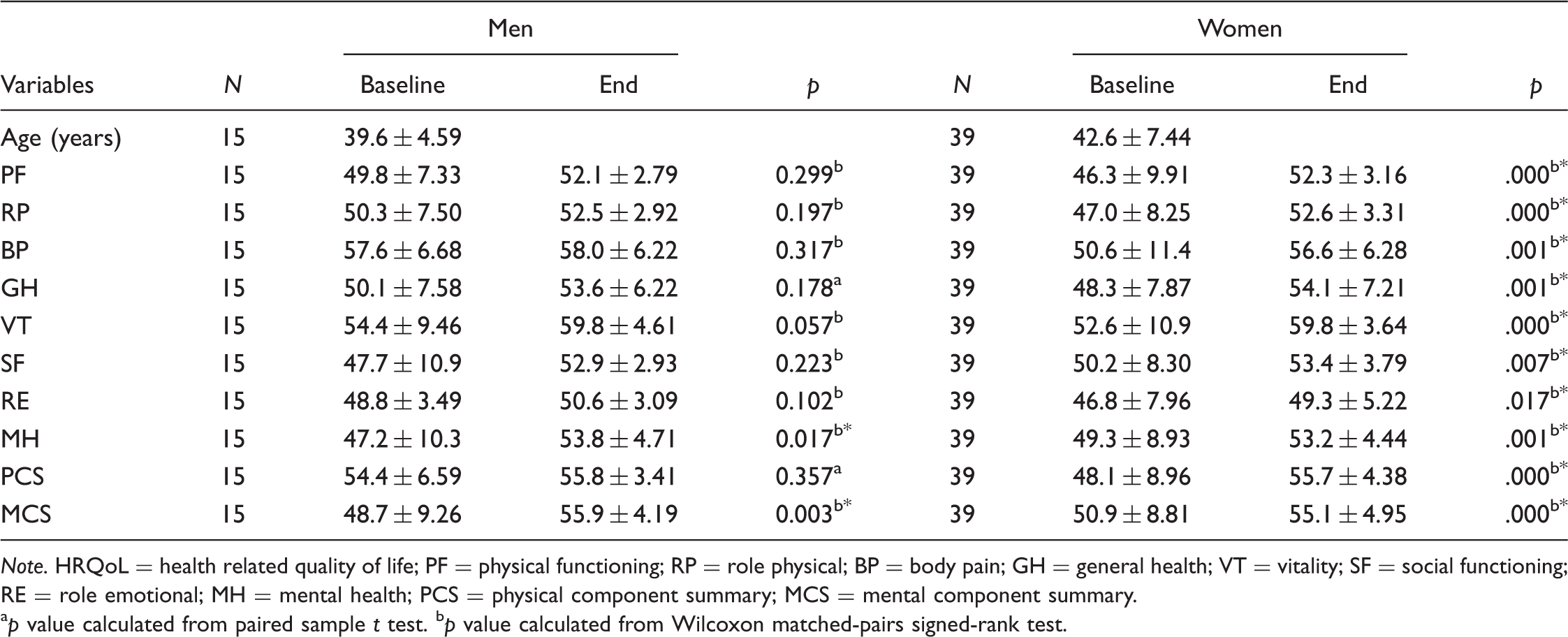
Note. HRQoL = health related quality of life; PF = physical functioning; RP = role physical; BP = body pain; GH = general health; VT = vitality; SF = social functioning; RE = role emotional; MH = mental health; PCS = physical component summary; MCS = mental component summary.
p value calculated from paired sample t test. bp value calculated from Wilcoxon matched-pairs signed-rank test.
Interviews
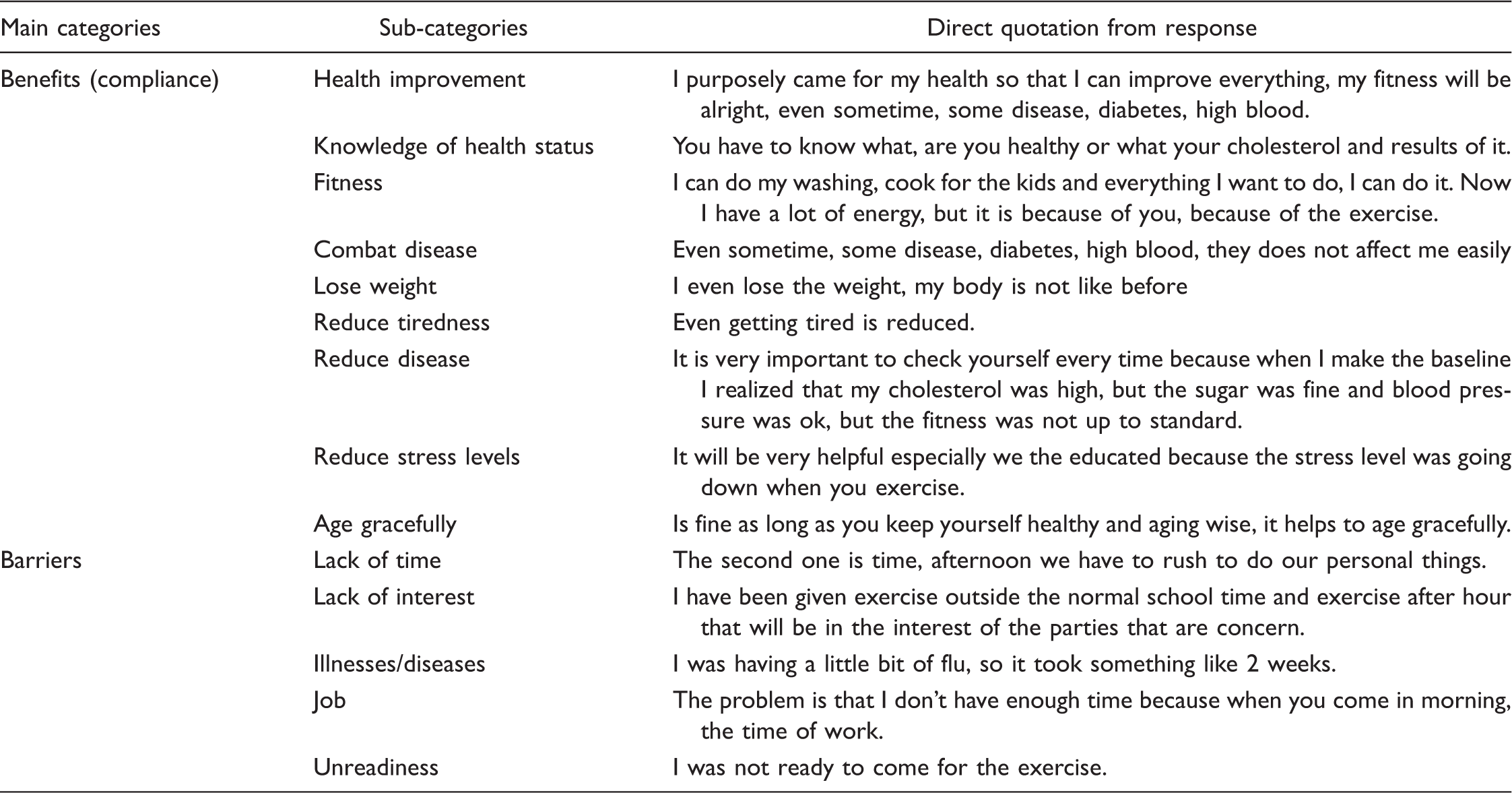
The results of the interview highlighted the participants’ “reasons for being part of the aerobic exercise intervention programme” and nonparticipants “reasons for not being part of the aerobic exercise intervention program.” Participants’ perceptions are presented in Table 7.
Discussion
In this study, we explore the effects of a 4-week exercise intervention on risk factors for NCDs among Setswana speaking community-dwelling Potchefstroom adults from a low-resource area of the Kenneth Kaunda district, Potchefstroom, North West Province of South Africa. This intervention followed a pragmatic approach in order to determine the acceptability of such an intervention in low-resourced communities by probing perceptions of benefit from exercise, and reasons for noncompliance in people who commenced the program but discontinued it. Resourced-poor community-dwelling adults are somewhat ignored in exercise research, perhaps because many of the barriers explored in this research have also prevented their representation in other studies. For example, people without their own vehicles, who are reliant on public transport, reported some difficulties in participation in this study. Transport limitations may be so substantial that they consider themselves unable to attend exercise trials undertaken in universities and thus do not even volunteer for them.
PA Intervention and Changes in NCDs Risks Factor
At the end of the 4-week aerobic exercise intervention, there were statistically significant reduction in body weight, and an improvement in the RPE and mental component HRQoL in men. Significant reduction in body mass, BMI, fasting blood glucose, improved predicted maximum oxygen, RPE, physical and mental component HRQoL were noticed in women who completed the aerobic exercise intervention program. This study also revealed an insignificant reduction in WHR and systolic blood pressure (SBP). There was also an insignificant reduction in diastolic blood pressure (DBP) and improved physical components in men.
The results showing a reduction in body weight and BMI are in agreement with the findings of Mujica et al. 28 who evaluate the effects of a structured intervention programme of PA and nutritional counseling in adults with metabolic syndrome for 18 weeks. The intervention group showed a significant reduction in body weight and BMI in both men and women. Another study was designed to examine the effects of light and moderate aerobic intensity on body composition and serum lipid profile in obese or overweight women aged 25 to 40. The participants were randomized into three groups of light exercise, moderate exercise, and a control group for a 10-week period, three times for 60 minutes each per week, and the results showed that both light and moderate aerobic exercise significantly reduced body weight, BMI, and WHR and also reduced fasting total cholesterol. 29 Based on the findings of this study, the increase in fasting total cholesterol in women was not so clear. Meanwhile, PA is somewhat liable for the increase in the production of numerous enzymes that may alter the transport system of cholesterol. 30 Therefore, this may have increase the level of cholesterol in the blood. 30
The reduction noticed in the SBP and DBP of the participants of the current study after the 4-week aerobic exercise intervention corroborates the findings of the review of Buttar et al. 31 in that regular aerobic exercise has a positive effect by reducing the blood pressure in hypertensive patients, considering the fact that the participants of this study were hypertensive, having blood pressure higher than normal of 120/80 mmHg. The reduction in BP could be clinically relevant in that a decrease of 10 to 12 mmHg SBP and 5 to 6 mmHg DBP have previously been indicated to reduce the risk of stroke by 38%, the risk of coronary disease by 16%, and the risk of premature death by 21%. 32 Furthermore, the significant improvement in the participants’ relative VO2max in this current study was in agreement with the study of Boileau et al. 33 who examined the effects of moderate aerobic exercise training on CRF in sedentary participants aged 60 to 75 for 40 minutes three times per week. The participants were randomly assigned to exercise and control groups and pre- and postmeasures were obtained. The result shows that both absolute and relative VO2max significantly improved in the exercise group while it was reduced moderately in the control group. There was a significant improvement in the perceived rate of exertion after the 4-week aerobic exercise intervention. This was supported by Grant et al. 34 who compared the physiological responses and ratings of perceived exertion to aerobic dance and walking sessions completed at a self-selected pace. The RPE was significantly improved for both aerobic dance and walking. The increase in resting heart rate after aerobic exercise intervention of both genders in this current study is supported by the findings of Almeida and Araujo 35 who stated that an individual who has a slow heart rate recovery in the first minute post-exercise is at increased risk of death.
PA Intervention and QoL
The changes in the overall HRQoL of participants in this study indicated a statistically significant change after a 4-week aerobic PA intervention. It has been reported that exercise intervention may have beneficial effects on overall HRQoL and its entire domain, 36 as PA levels have been linked to the improvement of one or more HRQoL domains. 37 The findings revealed statistically significant improvement after the 4-week aerobics exercise intervention in all domains of HRQoL (including PCS and MCS) in women compared with their men counterparts. Significant improvements were established in the women’s physical functioning, role physical, body pain, general health, vitality, social functioning, role emotional, mental health, and the two major components summary of physical and mental. Meanwhile, statistically significant improvements were seen in mental health and the MCS in men. Other HRQoL domains also gained improvement but were not statistically significant. The findings of this study corroborated the findings of some previous studies.38,39 PA, if well-structured and supervised, can improve many components of HRQoL, notwithstanding the mode of participation 39 because of its positive effect on overall health. Furthermore, the finding of this study shows that there is a possibility of improving all the domains and components summary of HRQoL, if a well-structured aerobic exercise intervention is in place.
Exercise Benefits and Barriers
Mean and Standard Deviation of Each Exercise Benefits Scale Questionnaire Item.
Mean and Standard Deviation of Each Exercise Barrier Scale Questionnaire Item.
Benefits (Compliance) and Barriers to Exercise Intervention.
Interviews: The Reasons for Participation and Nonparticipation
Participation in PA has been known to promote good health. 24 Considering that the participants from this study are from a low-resourced community, the participants still indicated during the interview that they understood the benefits of regular exercise. The most prominent barrier or reason for not participating in PA was lack of time due to the respondents’ job and personal reasons (Table 7). This finding was supported by Schutzer and Grave 41 who stated that lack of time due to office work is commonly cited by most adults. Lack of interest was another reason cited by the participants of this study, and this was corroborated by the findings of Moschny et al. 42 Other reasons such as un-readiness, illness, and disease, not able to exercise alone and work- or job-related matters were also cited. Furthermore, the most cited reason for taking part in the aerobic exercise intervention was mainly because of their health. This was supported by Schuler et al. 43 who identified and compared barriers and motivations to exercise associated with older African American (115) and European American (89) women with the mean age of 72 and found that the most cited reason for their participation was because of their health. The other reasons cited by the participants of this current study were to prevent diseases, reduce tiredness and fatigue, for relaxation, to reduce pain, increase fitness, age gracefully, feel good, lose weight, and improve their QoL.
Conclusion
A 4-week exercise intervention in community-dwelling persons of African descent indicated that a third of the participants were lost to the intervention. Those who participated, however, still indicated an improvement in the risk factor profile with this short intervention period in particular to the HR QoL. Exercise milieus on the subscale of perceived benefits and barriers and lack of time on the basis of interview were the major barriers to exercise participation. Furthermore, a higher drop-out rate is expected to occur during a long-term aerobic exercise intervention. Future studies on PA intervention will be required to be conducted for a longer period of time, while effort should be made during planning to consider and minimize those barriers of PA, most especially in adults.
Limitation
The main limitation of this study was the rate of drop-out of the participants. Some of the participants were unable to complete the study because of one engagement or the other, such as work-related commitments, family responsibility, medical problems, lack of time, distant exercise venue, and domestic-related injuries, which are seen as barriers to PA intervention. Furthermore, cold weather was seen as another limitation that restricted many people from taking part in the study.
Footnotes
Acknowledgments
The authors would like to thank all the participants in this study and would also like to thank Caroline Madise, Maluleke Ntiyiso, Mashudu Phiza, and Gudani Nelly for assisting with the data collection.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author declares that there was no conflict in interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the NOrth-West University and PhASRec research Focus Area for the financial support for this project.