
Abstract
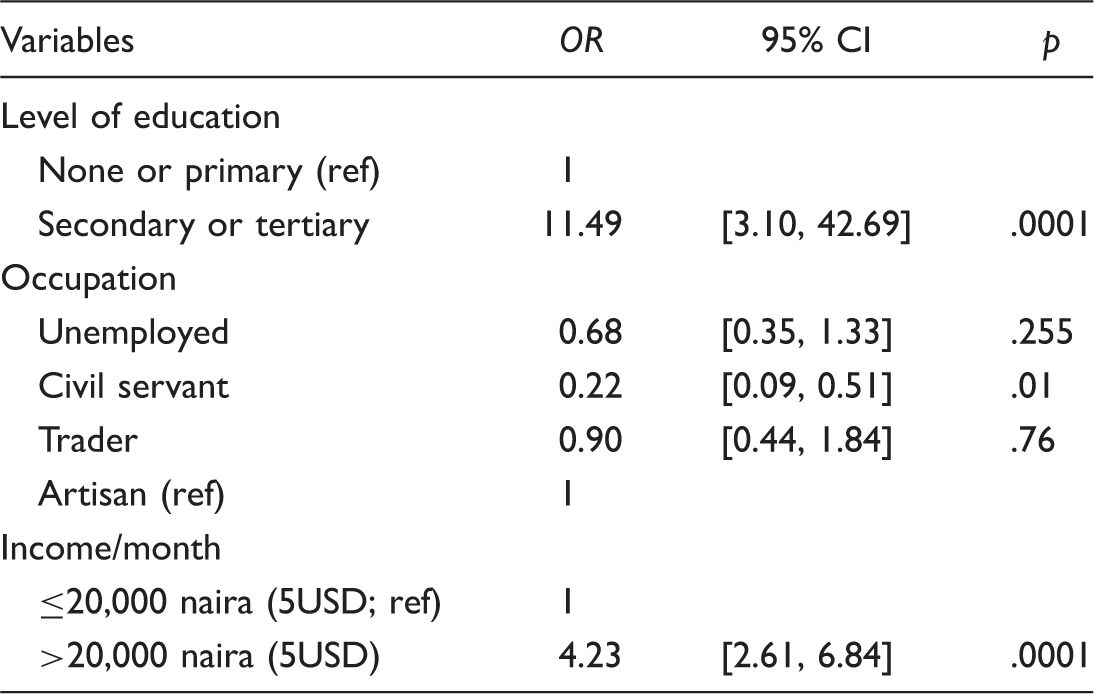
Lassa fever had been reported as a cause of death especially in endemic parts of Nigeria. This study assessed the knowledge, attitude, and practices toward Lassa fever control and prevention among residents of Ile-Ife, southwest Nigeria. Descriptive cross-sectional study was conducted among consenting randomly selected adults using an interviewer administered questionnaire. Data were analyzed using descriptive and inferential statistics. A total of 400 questionnaires with completed data were analyzed (response rate 96%). Majority, 207 (51.8%), were males while 193 (48.2%) were females. Most, 234 (58.5%), had tertiary education while 148 (37%) had secondary education. Fifty-nine percent had heard of Lassa fever with radio as their major source of information. About 76% had inadequate knowledge, 54% had negative attitude while 51% had poor practice toward Lassa fever. Determinants of knowledge of Lassa fever include having higher education (Adjusted Odd Ratio (AOR) = 11.49, 95% CI [3.10, 42.69], p = .0001), being in civil service (AOR = 0.22, 95% CI [0.09, 0.51], p = .01), and earning higher income (AOR = 4.23, 95% CI [2.61, 6.84], p = .0001). In conclusion, the knowledge, attitude, as well as preventive practices to Lassa fever were poor. It is necessary to increase public education and improve hygienic practices.
Introduction
Lassa fever is an acute zoonotic illness caused by Lassa virus, an arenavirus, known to be responsible for severe hemorrhagic fever. Lassa virus was isolated in 1969 in Lassa town, Borno State, North East Nigeria. Lassa fever is endemic in West African countries including Nigeria, Liberia, Sierra Leone, Guinea, and Mali. 1 It accounts for 10% to 15% of all hospital admissions with case fatality rate of 50%. About 300,000 to 500,000 are infected yearly with 5,000 dying yearly.2,3 The natural host of Lassa fever is the multimammate rat, Mastomys natalensis, which is commonly found in human households and eaten as a delicacy in several African countries, including Nigeria. Other rodent hosts, such as M. erythroleucus and the Rattus and Mus genera, have been suggested.1,3,4 Recent evidence exists that Lassa virus is hosted by other rodent species such as the African wood mouse Hylomyscus pamfi in Nigeria and the Guinea multimammate mouse M. erythroleucus in both Nigeria and Guinea. 5
Lassa fever infection is acquired mostly through the excreta of the natural host in the food that is inappropriately stored or dried in the open. Also, infection has been reported from direct exposure of the infective agent to broken skin, mucous membrane while person-to-person transmission has occurred. Lo Iacono et al., 6 using an innovative modeling approach to analyze data from published outbreaks and the number of Lassa fever hospitalized patients at Kenema General Hospital in Sierra Leone to estimate the likely contribution of human-to-human transmission, showed that almost 20% of the cases at Kenema General Hospital were secondary cases arising from human-to-human transmission. Also, much of this human-to-human transmission is associated with a disproportionally large impact of a few individuals called super spreaders. This discrepancy between the size of reported Lassa fever outbreak and clinical perception that human-to-human transmission is low should be noted in future assessment of the risk of Lassa fever and infection control guidelines. 6
Lassa fever affects all age-groups and gender with a seasonal clustering around the late rainy season and dry season.4,7,8 It is endemic in Edo state, Nasarawa state, and Plateau state with sporadic cases reported in over 22 out of 36 states in Nigeria. 9 Also, outbreak of Lassa fever occurs with recorded fatalities much more than other hemorrhagic fevers including Ebola, but it receives much less attention. 10 Lassa infection is symptomatic in about 20% of cases when it causes an acute illness with fever and general weakness followed by nonspecific symptoms such as headache, chest pain, vomiting, diarrhea, cough, pleural effusion, bleeding from orifices, and in the late stages, sometimes disorientation and coma. The overall case fatality rate is usually 1%, increasing to 15% of hospitalized cases. 4
Despite the transmissibility of Lassa fever from animal to human, human to human, and possibly human to animal, meticulous adherence to appropriate infection control practices to prevent unprotected exposure to blood and other body fluids is essential for the safe management of suspected patients with Lassa fever and the prevention of onward transmission particularly given the nonspecific presentation of Lassa fever. 6 There is no vaccine to prevent Lassa fever while Ribavirin, the only known drug that cure cases, needs to be commenced early in the infection.9,10 It is therefore important for community members to be aware of the disease to ensure prevention and early diagnosis and treatment of cases. This study assessed the knowledge, attitude, and practices toward Lassa fever control and prevention among residents of Ile-Ife, southwest Nigeria.
Methods
This study was conducted in Ile-Ife, an urban town with an estimated population of 167,000. The people were mainly Yoruba living with other Nigerian tribes such as Hausa and Igbo. Ile-Ife is the cradle of the Yoruba people.
The study design was a descriptive cross-sectional community-based survey with residents of Ile-Ife as the study population. The sample size was determined using an appropriate statistical formula for estimating the minimum sample size in descriptive health studies (n = Z2pq/d2), 11 where n = sample size, Z = standard normal deviate corresponding to confidence level at 95% = 1.96, d = degree of accuracy desired = 0.05, p = 62% have good general knowledge of Lassa fever 6 while q = 1−p = 1−0.62 = 0.38; n = 1.962 × 0.62 × 0.38/(0.052) = 362. A sample size of 400 was used after nonresponders were taken into consideration.
A multistage sampling technique was employed in this study. Stage 1 involves selecting 5 wards out of 21 wards in Ile-Ife using simple random technique (balloting). Stage 2 involves selecting 8 streets out of an average of 24 streets per ward by simple random technique (balloting). A total of 40 streets were selected. Stage 3 involves listing the houses on each selected street and using systematic sampling technique to select every fourth house on each street. Stage 4 involves approaching all adults older than 18 years old to participate in the study till the sample size was reached.
Data were collected using a pretested interviewer administered questionnaire that captured information on sociodemographic variables, knowledge, attitudes, and practices regarding Lassa fever.
Data were analyzed using SPSS version 16. The data were summarized using mean and standard deviation for continuous variables, frequencies, and percentages for categorical variables. Knowledge, attitude, and practice scores were computed with “+1” assigned for correct response and “0” assigned for incorrect response. These scores were graded as appropriate or inappropriate knowledge, positive or negative attitude, and good or poor practice using their mean score as the cut-off point. Bivariate chi-square test and multivariate logistic analyses were performed on respondents’ characteristics and knowledge of Lassa fever. Variables in the bivariate test with p value of <.2 were included in the multivariate model. A p value < .05 was accepted as significant.
Ethical Consideration
The Ethics and Research Committee of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria approved the study. Written consent was taken from each participant after ensuring their privacy and confidentiality. Data collected were kept in a passworded computer.
Results
Sociodemographic Characteristics of Respondents.
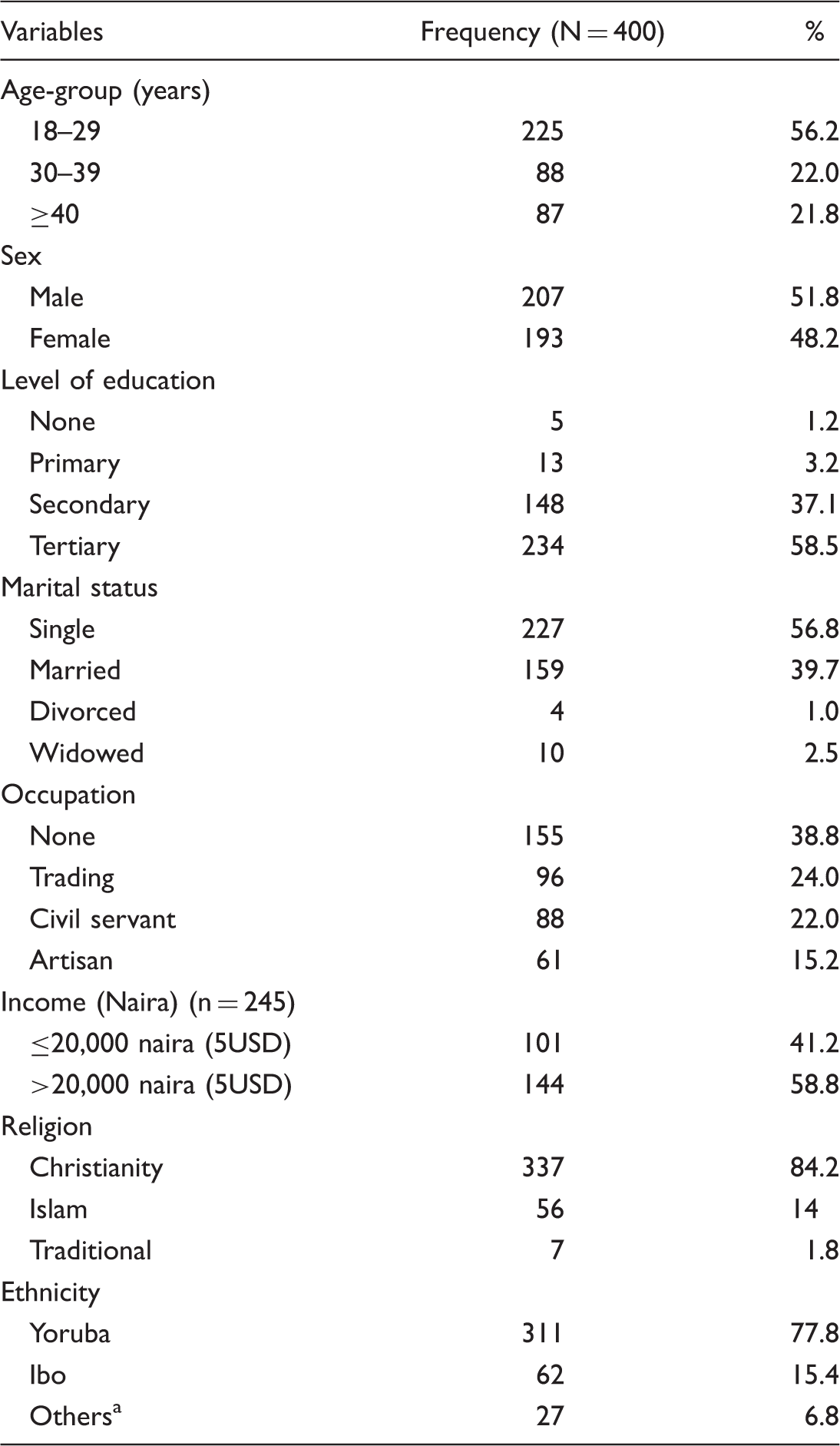
Hausa, Edo, and Ishan.
Figure 1 shows the knowledge, attitude, and practice toward Lassa fever. About 76% had inadequate knowledge, 54% had negative attitude while 51% had poor practice toward Lassa fever.
Knowledge, attitude, and practice toward Lassa fever.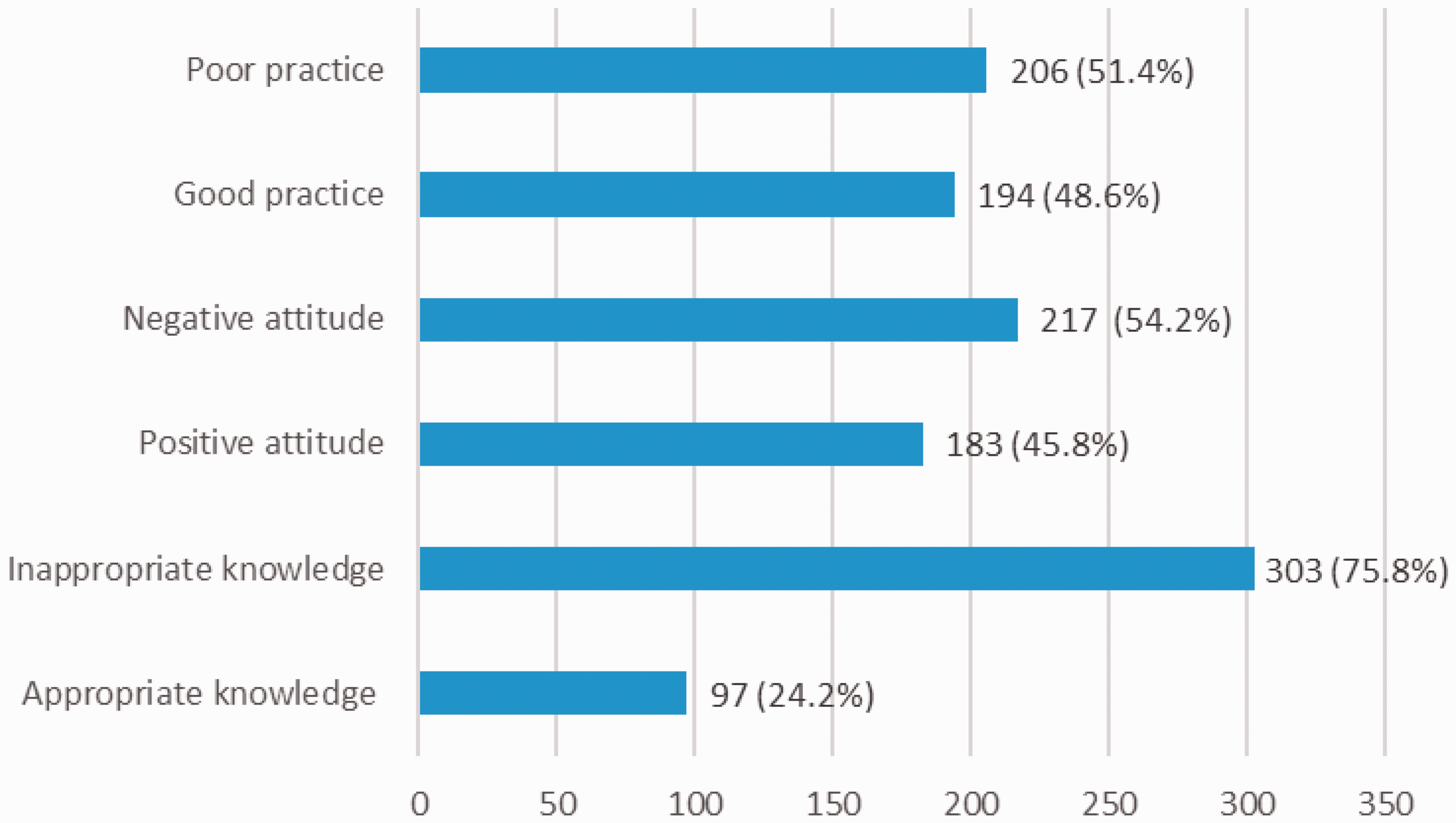
Knowledge About Lassa Fever Among Respondents.
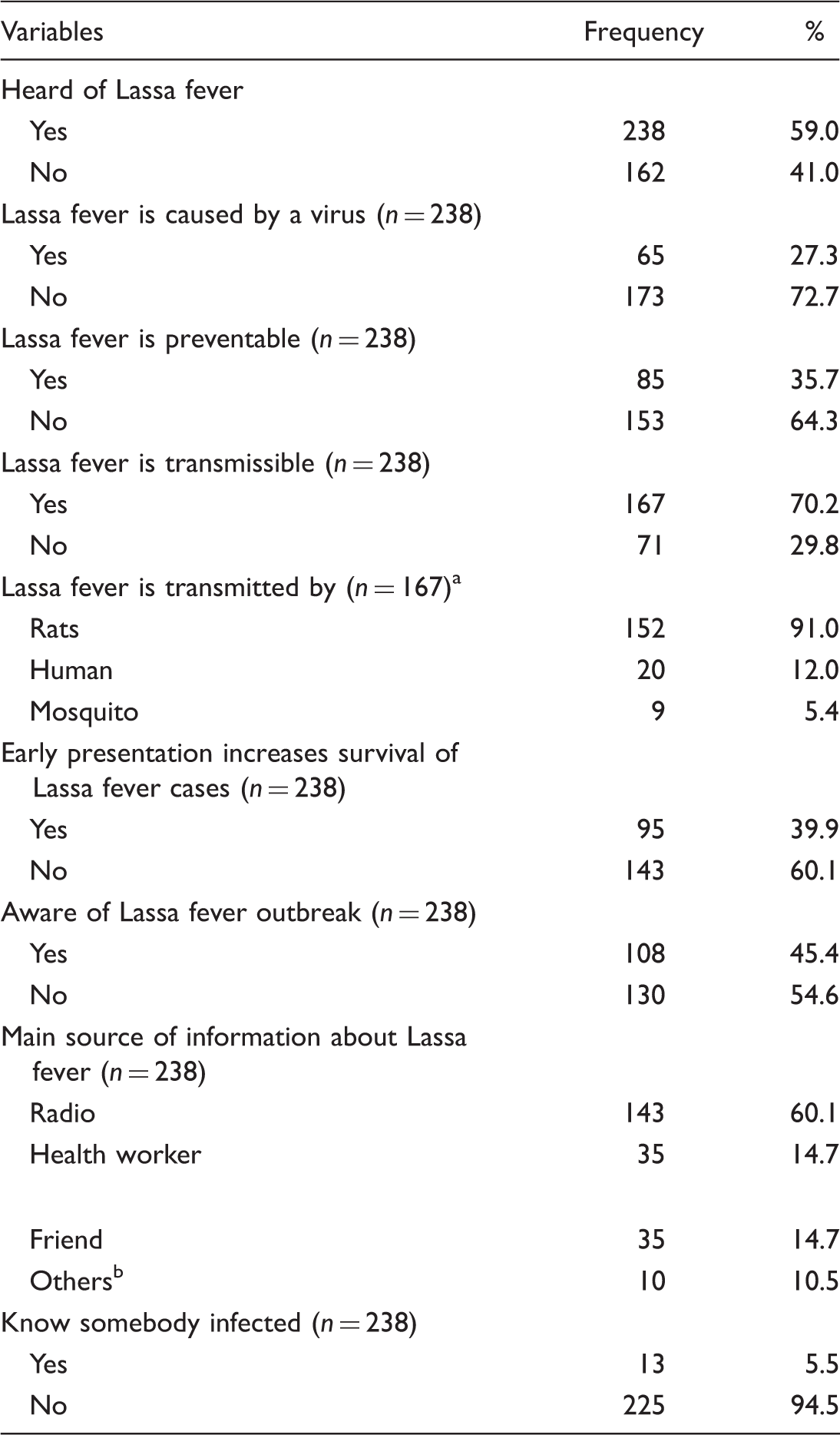
Multiple response.
Neighbor, teacher, textbook, and place of worship.
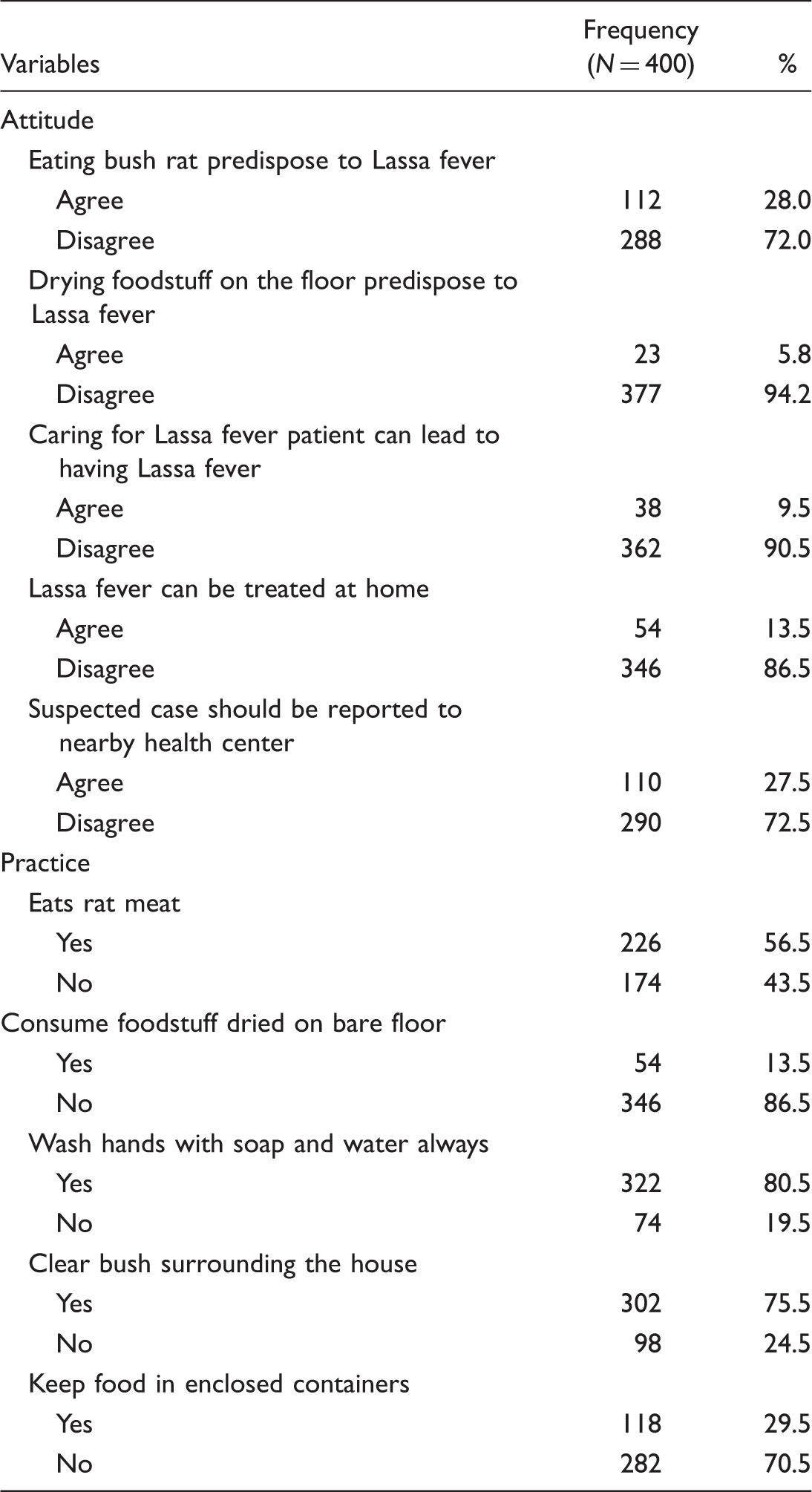
Attitude and Practices of Respondents to Lassa Fever Control and Prevention.
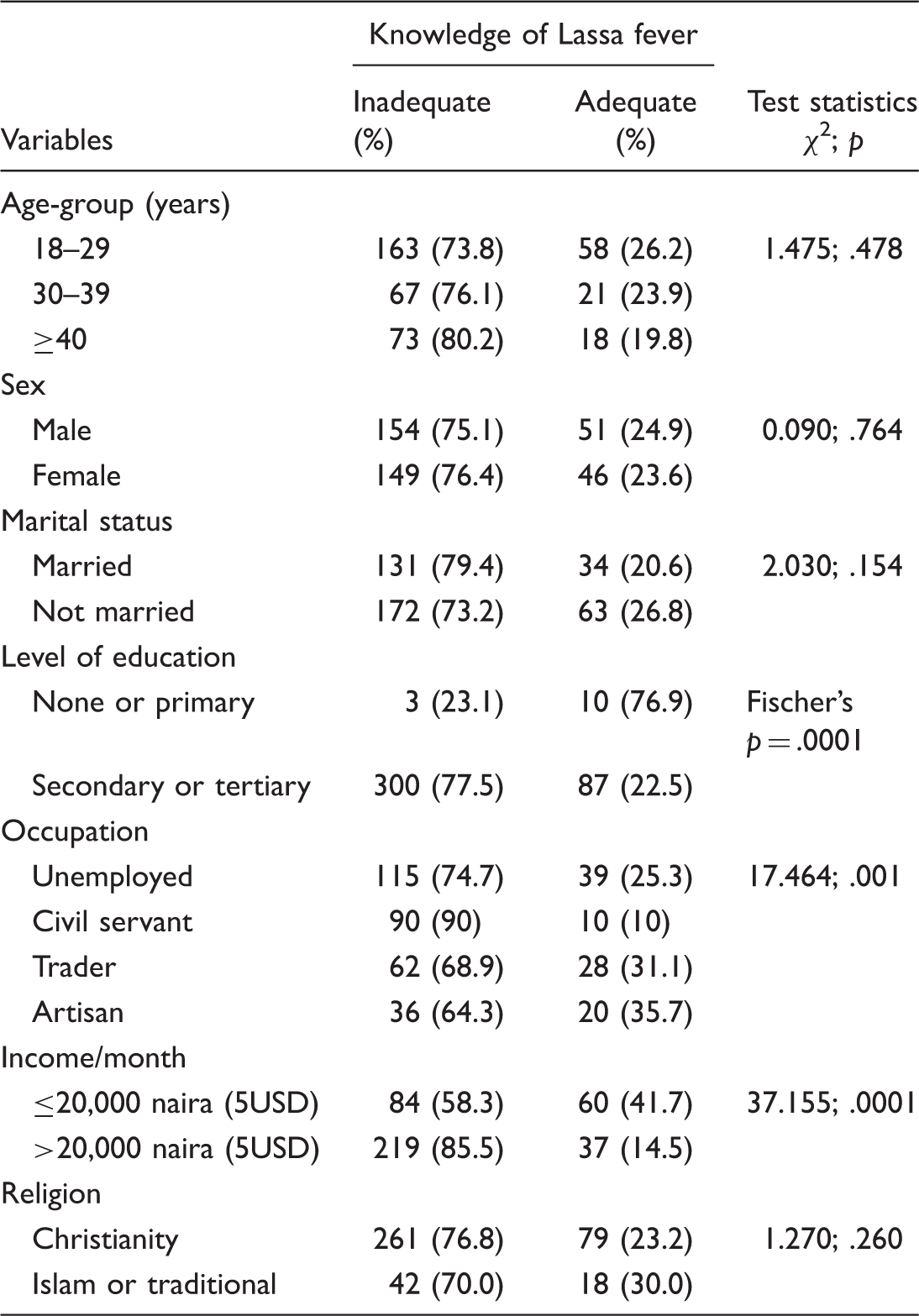
Association Between Sociodemographic Variables and Knowledge of Lassa Fever.
Logistic Regression Analysis of Determinants of Adequate Knowledge of Lassa Fever.
Discussion
This study reported inadequate knowledge, negative attitude, and poor preventive practices toward Lassa fever among residents of an urban community in southwest Nigeria. This finding requires urgent response so as to curtail the yearly occurrence of this deadly infection in Nigeria. The study population who were mostly young, males, educated, and employed will require continuous education on Lassa fever control and prevention so as to enable early referral of suspected cases and for notification purposes. Early referral of these cases will improve survival and reduce disease transmission. It will also ensure that the population will not become infected or serve as a source of infection to family and other community members.
Although most respondents have heard of Lassa fever with some knowing somebody infected previously, they displayed inappropriate knowledge. This finding had been reported in previous studies in Nigeria and elsewhere.4,9,12 It is therefore essential that this population access accurate information on Lassa fever to reduce the occurrence of this disease and stamp out the nearly yearly outbreaks. Also, radio was identified as the major source of information about Lassa fever for most respondents. Previous studies have shown the importance of the media, especially the transistor radio, as source of necessary information for the general population, especially in resource-limited setting such as the study site.13,14 This further shows that the media should have more programmes on Lassa fever that target the general population, especially in the local dialects.
The fact that the information available to this population about this life-threatening infection is inadequate needs further enquiry so as to improve the knowledge content of information placed on the media. This could be the main reason behind the nearly yearly outbreak of this deadly disease in Africa despite the fact that it is treatable and preventable. Emphasis should therefore be on more community-based education on Lassa fever control and prevention. Although some respondents knew that Lassa fever is transmissible with rat as the natural host, majority still engage in practices that encourage rat breeding through poor personal and environmental hygiene with exposure of rat excreta to foodstuff during drying on bare floor and storing in open containers. This important link is yet to be realized by the study population despite their high formal education status. Also, the latest finding on human-to-human transmission needs to be added in community-based education and mode of preventing such exposure such as reducing contact with suspected cases through use of personal protective equipment. The negative attitude and behavior of this population encourages Lassa fever outbreak, hence the need for strengthening of environmental sanitation laws and changes in government and nongovernmental organizations approach to control and prevention of the spread of Lassa fever.
High education, income, and working in civil service were factors determining Lassa fever knowledge. Several studies had reported similar finding as this group of people have better personal hygiene and environmental sanitation practices.7,12–14 They also have access to information through various reliable sources. Therefore, it is necessary to focus on the less educated, those earning less income, such as traders and artisans, as they are likely to engage in behaviors that make them prone to Lassa fever infection. Motivating and training more environmental sanitation workers will help to prevent further spread of the deadly infection.
Furthermore, behavioral change in waste disposal, personal hygiene, and handwashing with universal precaution will curb the persistence of Lassa fever in the community.10–14 Also, health-care workers will benefit from continuous training on recent and accurate information on Lassa fever diagnosis, treatment, control, and prevention. Isolated wards, personal protective equipment, and necessary drugs including Ribavirin in appropriate doses and route should be provided in such designated wards so that there will be no delay in attending to suspected cases.15,16
We recognize that this study limitation includes its cross-sectional study design which relies on information from respondents, information bias such as recall bias may occur. Recall bias was reduced by asking questions to double-check the responses. Although the response rate was high compared with some community-based studies, a generalization of findings to other communities in this and other parts of the country will be limited. However, this study provides important information that will guide planning and implementing interventions targeted at controlling and preventing Lassa fever infection in the study area.
Conclusion
In conclusion, community members have inadequate knowledge, negative attitude, and poor preventive practice about Lassa fever. It is necessary to strengthen environmental sanitation laws, government, and nongovernmental organizations approach to control and prevention of the spread of Lassa fever. Also, community-based education will increase community knowledge, especially among the disadvantaged population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.