
Abstract
As the opioid crisis escalates across North America, photographers are highlighting the gravity of the situation. However, many of their images of people who use drugs are problematic and stigmatizing. This study looks at how digital storytelling (DST) was used in order to assist long-term heroin users taking part in North America’s first heroin-assisted treatment program in Vancouver, BC, in amplifying and sharing their personal experiences. DST is a participatory and collaborative process designed to help people share narrative accounts of life events. A total of 10 participants took part in a 3-day DST workshop and eight individuals completed 2 to 3-minute digital stories. Participants demonstrated increased agency in terms of how they represented themselves. Their digital stories disrupt hegemonic representations of heroin users and can help educate the public and decision makers about compassionate and science-based treatments for chronic addiction. Theory, methodology, practical applications, and ethics are discussed.
Introduction
A growing opioid crisis is spreading across North America. In Canada, it is estimated that over 4,000 people died from opioid-related overdoses in 2017. A year earlier, officials reported 2,681 overdose deaths, according to Dr. Theresa Tam, the country’s chief public health officer. 1
British Columbia (BC) is facing the most critical situation in the country. From 2000 to 2010, approximately 200 people died every year in the province from drug-related overdoses. 2 By 2017, the number of people who experienced fatal overdoses in BC had climbed to more than 1,422. 3 The figure marks a 43% increase from 2016 and authorities say the number of overdose deaths will continue to rise.
BC has asked the federal government to declare a national health emergency in order to address the situation. Meanwhile, the Liberal government led by Prime Minister Justin Trudeau has ruled out implementing the Emergency Act, claiming it is doing all it can to respond what it calls the “greatest public-health crisis we face in Canada.” 4
The number of fatal drug-related deaths has significantly escalated because of the widespread availability of synthetic opioids, including fentanyl and carfentanil, on the market. BC’s Coroners Service indicated that fentanyl was found to be exclusively or partially connected to more than 80% of fatal overdoses in the province in 2017. 3 Five years ago, fentanyl was reported to be linked to only 4% of drug-related deaths. 5 Fentanyl and carfentanil are part of the same class of drugs as morphine and oxycodone. 6 Fentanyl is as much as 100 times more potent than morphine. 7 It is sold on the street and amounts as small as a grain of sand can be powerful enough to kill someone if consumed. 6 Carfentanil, also widely available on the streets, is used as an elephant tranquilizer and is 100 times stronger than fentanyl. People who ingest less than 20 µg, amounts smaller than a grain of salt, can die. 8
Conventional therapies such as methadone maintenance are widely available in Canada, but not all drug users respond to them. There is a growing recognition that opioid substitution and maintenance treatment could play a greater role in curbing the number of deaths related to synthetic opioid consumption. However, there have been few attempts to examine whether other opioids aside from oral methadone can be effective in treating people who are dependent on opioids, including heroin. 9
In 2011, the University of British Columbia and Providence Health Care (PHC) launched a 4-year study in Vancouver’s Downtown Eastside (DTES) aimed at determining if diacetylmorphine, the active ingredient of heroin, could be effective in treating chronic and vulnerable drug users. 10 The study was known as the Study to Assess Long-Term Opioid Maintenance Effectiveness (SALOME), and 202 drug users took part. Heroin-assisted treatment has been available across Europe through national health-care programs for decades, but this was only the second time it had been offered in North America. Previously, the North American Opiate Medication Initiative (2005–2008) tested the effectiveness of prescription heroin in treating chronic addiction in Vancouver and Montreal.
SALOME was based in Vancouver’s DTES at the Crosstown Clinic which is run by PHC. The neighborhood has long been known for its open and illicit drug scene. 11 Journalists have frequently focused on drug use, poverty, and homelessness in the DTES, while rarely exploring root causes of these issues. Many journalism organizations have also long ignored a long tradition of social activism in the community. 12 Reporters often refer to the DTES as “the poorest postal code in Canada,” even though that is inaccurate. Many First Nations communities in Canada experience worse social and economic conditions than many residents of the DTES, 13 which is one of the ongoing impacts of colonialism. 14
The impetus for this study was that Canada’s federal Conservative party, in power from 2006 to 2015, had forced SALOME to shut its doors. In October 2013, former Health Minister Rona Ambrose declared that diacetylmorphine was a restricted substance through the Food and Drug Act. She stated: “We do not support giving heroin to those who are struggling to recover from addiction.” 15 The decision meant that physicians working with SALOME were no longer able to prescribe diacetylmorphine. In response, on November 2013, five SALOME participants took their case to BC’s Supreme Court demanding the right to continue to access their treatment. In May 2014, the court ruled in favor of the participants and granted SALOME physicians the right to continue treating all 202 drug users who had entered the study with diacetylmorphine.
In spite of the court’s ruling, the Conservative party continued to communicate inflammatory rhetoric about SALOME and injection drug users. The party launched an online petition calling on Canadians to “act to ensure this never happens again”. It was referring to other potential clinical studies and heroin-assisted treatment programs such as SALOME. The petition added: “We will continue to fight to protect our streets and our communities, but we need your support. Are you with us?” 16
A number of people began posting negative messages in online comment sections connected to journalism articles about SALOME. These are just two of many statements published online: “What a joke. I am a taxpayer and I do not want to supply bums with free heroin!”; 17 and, “Let’s give the gamblers tax payer money to go and gamble even more. That way they can still have their habit and hopefully cure themselves.” 18
Some readers posted supportive comments about SALOME such as: This is a smart program. It disappoints people who believe the only acceptable outcome is complete abstinence from drug use. But a doctor would still treat a broken knee even if it will always be a little stiff. And a doctor would still treat diabetes even if the person will always be an insulin-user. This is hardly a cure. These people are still addicts. But it is still worth a try.
19
This program will not lead to addiction because the patients are already addicted Heroin does not lead to “brain death.” Addicts can use heroin for decades and it doesn’t kill them. Crack cocaine is highly damaging but heroin just isn’t. Giving addicts clean drugs and a clean environment to use it can only help them in the long run, and also help society by reducing the damage that illicit drug use causes like rampant theft.
20
Virtually any story produced for the Internet can be considered a digital story. In the context of this study, DST refers to a community-based participatory research method first developed by Joe Lambert, 24 founder of the Story Center (formerly the Center for DST) in Berkeley, CA. Story Center workshops are typically 3 days long. Participants share and receive feedback on their story ideas in a collaborative and supportive setting. They write scripts and create their stories with a mix of still photographs, video, voiceover recordings, music, and text. The stories are almost always written and produced from the storyteller’s point of view and often reveal personal insights about social issues.
My interest in DST grew out of my long-standing work as a researcher, journalist, and documentary maker specializing in social and humanitarian issues. I have consistently strived to highlight how individuals and communities have experienced conflict, disaster, and human rights abuses. I reached a point though when I wanted to develop the skills to support people in telling their own stories. That led me to the Story Center and the University of Colorado-Denver where I completed a 2-year certificate in DST from 2012 to 2014. I then founded an organization known as StoryTurns (www.storyturns.org), and have facilitated a number of DST workshops with community organizations. The methodology that I adopt in these workshops is inspired by the Story Center’s practices along with others that I developed in my journalism and documentary work and that other facilitators have shared with me.
Stigmatizing Narratives and Shaming Strategies
Although photojournalists are helping to raise awareness about the opioid crisis, many of the images they are producing are stigmatizing. People who use drugs are often portrayed as social outcasts. For example, CBC News published a who lack agency. photograph about the opioid crisis on its website on January 18, 2017. 29 The image features a man stretched on his back in what looks like an alley in Vancouver’s DTES. His belly and chest are exposed, and rescue workers huddle over him. The firefighters’ first and last names are listed in the image’s caption. Meanwhile, the man on his back is identified as “an addict.” Dr. Scott MacDonald, lead physician at PHC’s Crosstown Clinic, and others argue the word “addict” is a pejorative and are calling on journalism organizations and the public to stop using it. MacDonald suggests it is less stigmatizing to use language such as people with “substance use disorder[s].” “They’re just people with a medical problem, a chronic disease that’s manageable with treatment,” McDonald has said. 30 It would be unethical to publish images or text that could identify people who are experiencing overdoses. Doing so could potentially create a number of social and legal risks for these individuals. At the same time, images such as the one described earlier published by CBC and others31,32 perpetuate a practice of denigrating photography focused on injection drug users that has existed for decades.
Larry Clark 33 , Eugene Richards, 34 and Lincoln Clarkes 35 are among the most influential documentary photographers in North America who have represented heroin users in problematic ways. Their iconic, graphic, and unsettling images of people consuming injection drugs have contributed to dominant and negative public attitudes about substance users. Their work has fueled the notion that people who use drugs deserve to remain in the margins of society. (For a more detailed analysis of their photographs, see the study by Goodman 36 ). These photographers and others have consistently cast substance users as residents of “dark, seedy, secret worlds.” This can “Other the subject, or make them appear different through eroticizing or exoticizing them.” 37 Photographers who create and publish work like this engage in “symbolic violence” and “ritualized expulsion” in the way that they “mark, assign and classify subjects.” 38
From 1997 to 2001, former fashion photographer Lincoln Clarkes took portraits of more than 300 female heroin users in Vancouver’s DTES. His images were published in a book titled Heroines: Photographs. 35 The images helped raise awareness about the fact that dozens of women from the neighborhood had gone missing or had been murdered. Although Clarkes claims to have befriended many of the women he photographed, scholars such as Paul Ugo consider his methods exploitative. 39
Several of the women in Clarkes’ series are photographed in model-like poses. They stand with hands on their hips in graffiti-laced alleys and streets of the DTES. The images reveal the women’s emaciated figures and scabs caused by long-term drug use. In one of Clarkes’ photographs, a woman purses her lips as she self-injects drugs into her neck (Figure 1). Capturing images of people using illicit substances in this way has been repeated countless times over decades. Clarkes’ image may be visually compelling, but like all of the photos in his series, it fails to communicate anything about the woman other than the fact that she uses drugs. Her backstory is more important to communicate than her drug use in my view.
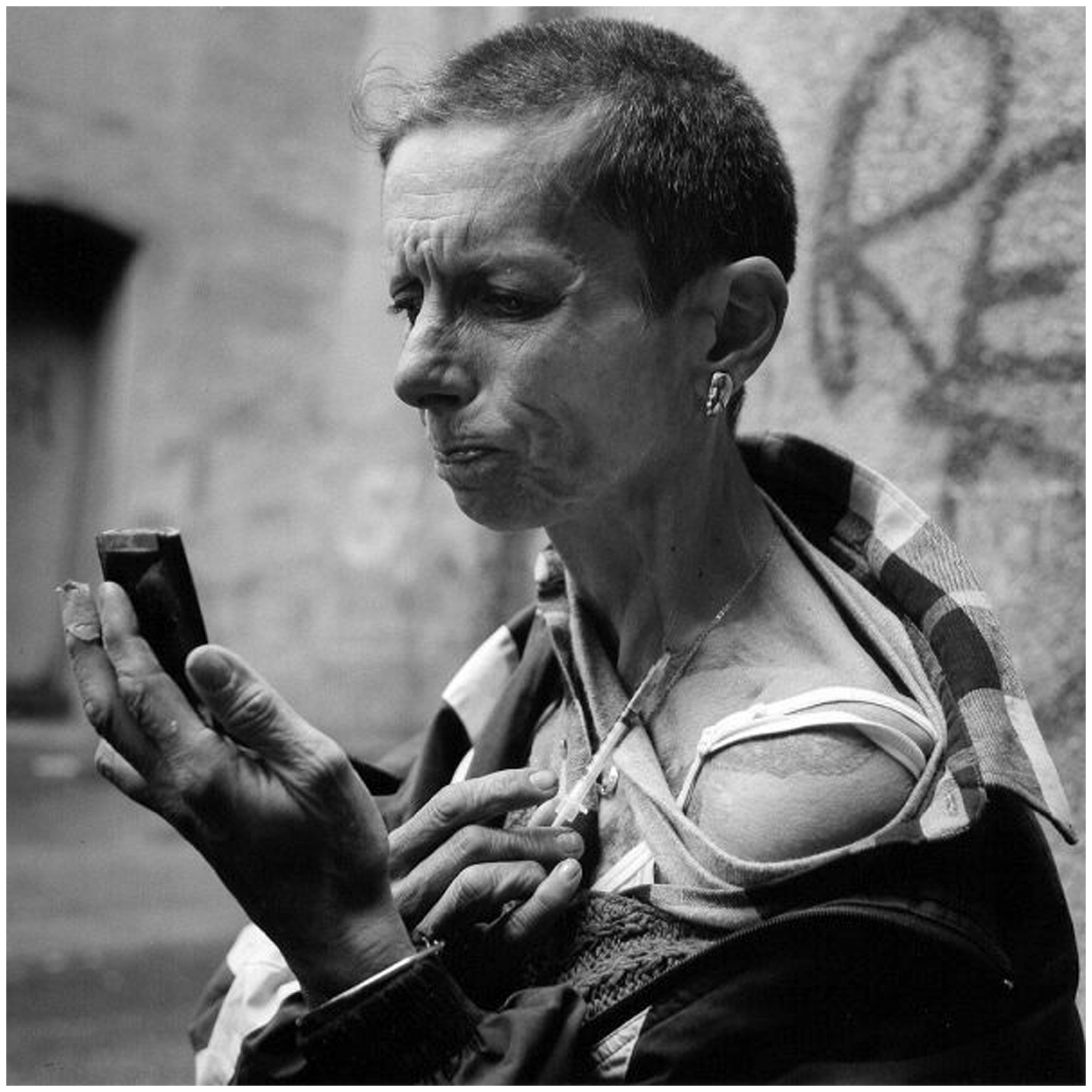
Woman injecting into her neck. Chinatown, 127 East Pender Street (1998) by Lincoln Clarkes. © 1971 Lincoln Clarkes; Courtesy of Anvil Press.
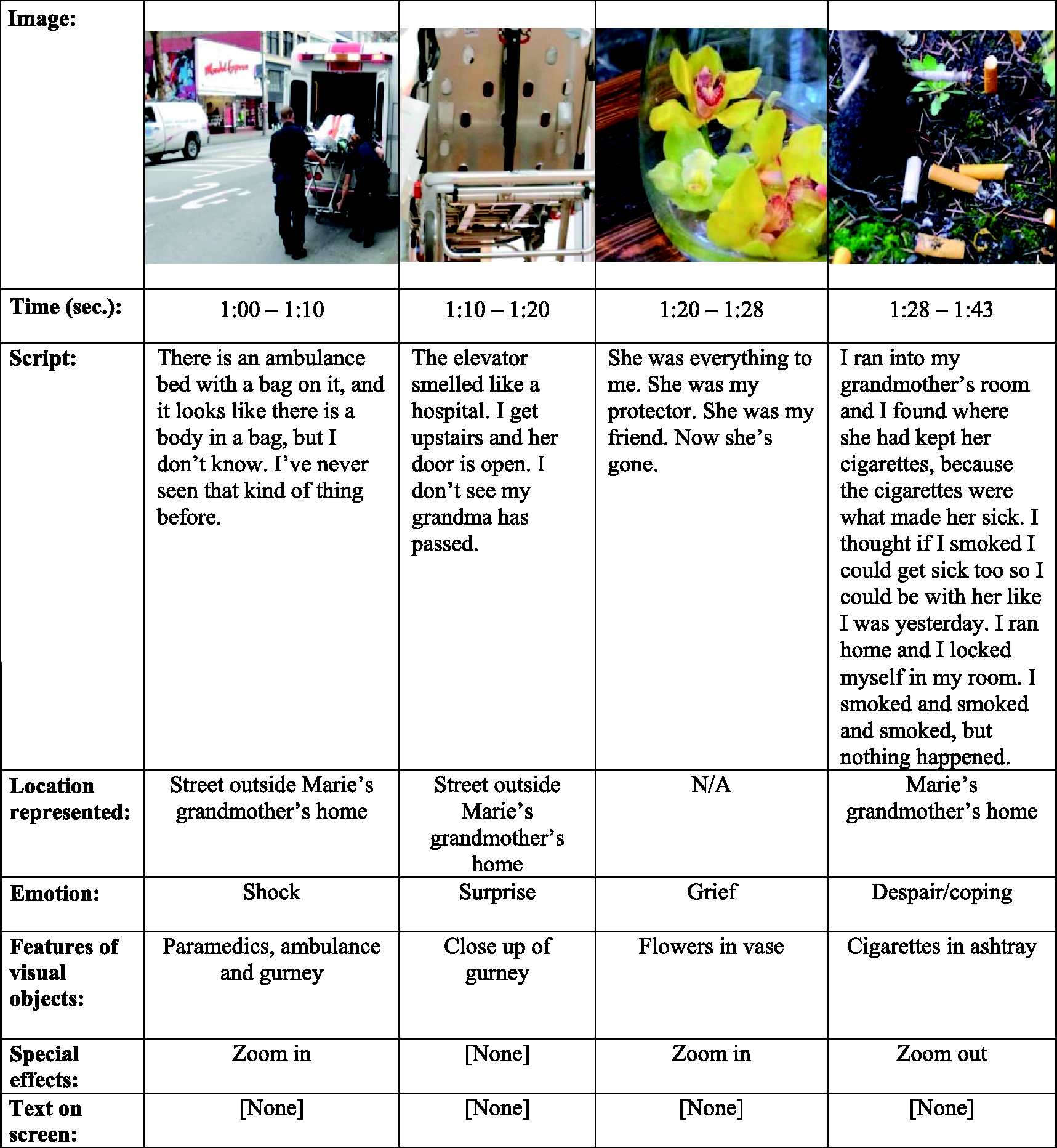
Multimodal media transcript Sample 1. Marie. A love of a grandma, StoryTurns, https://vimeo.com/94534895 (2004, accessed 24 October 2018).
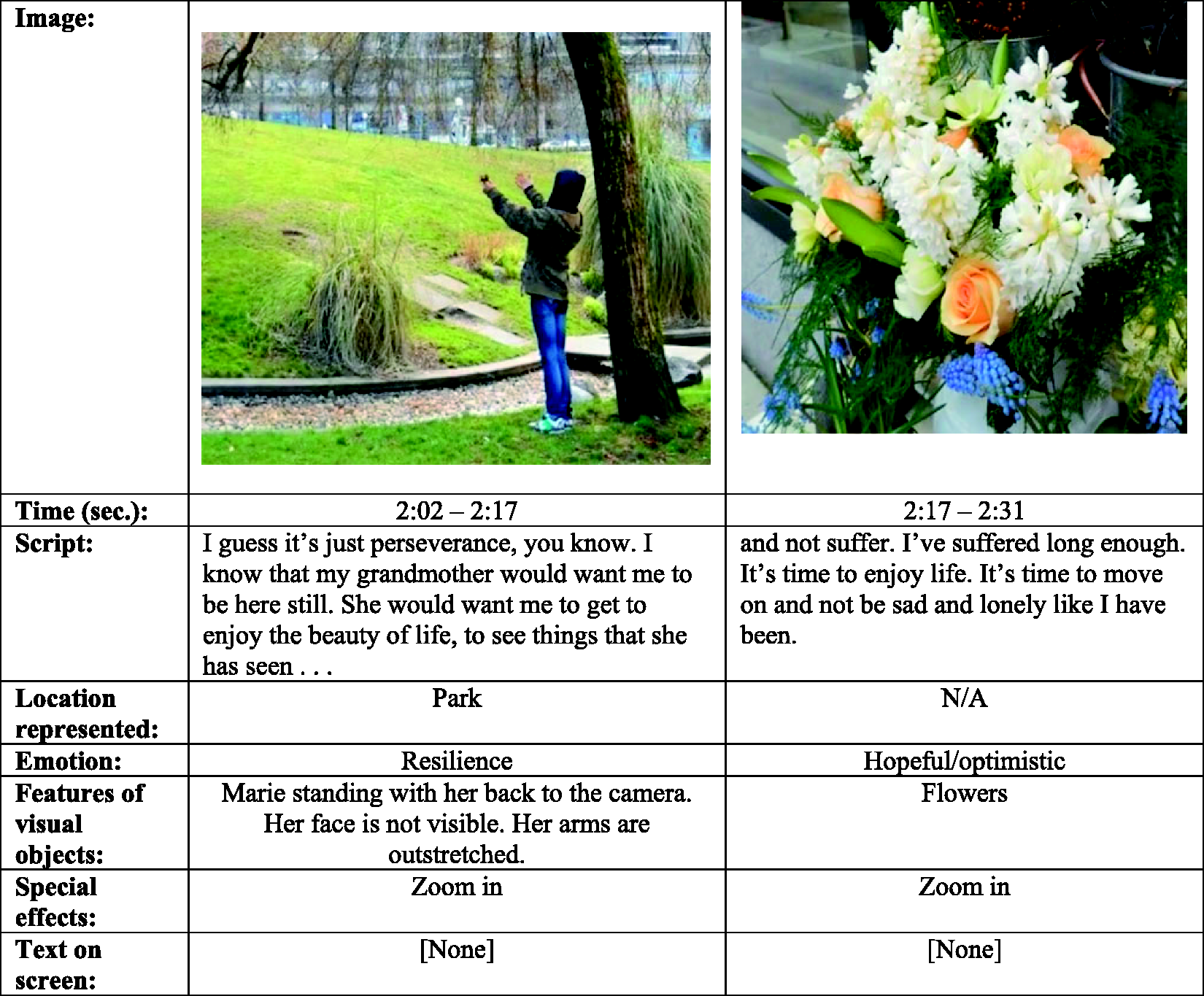
Multimodal media transcript Sample 2. Marie. A love of a grandma, StoryTurns, https://vimeo.com/94534895 (2004, accessed 24 October 2018).
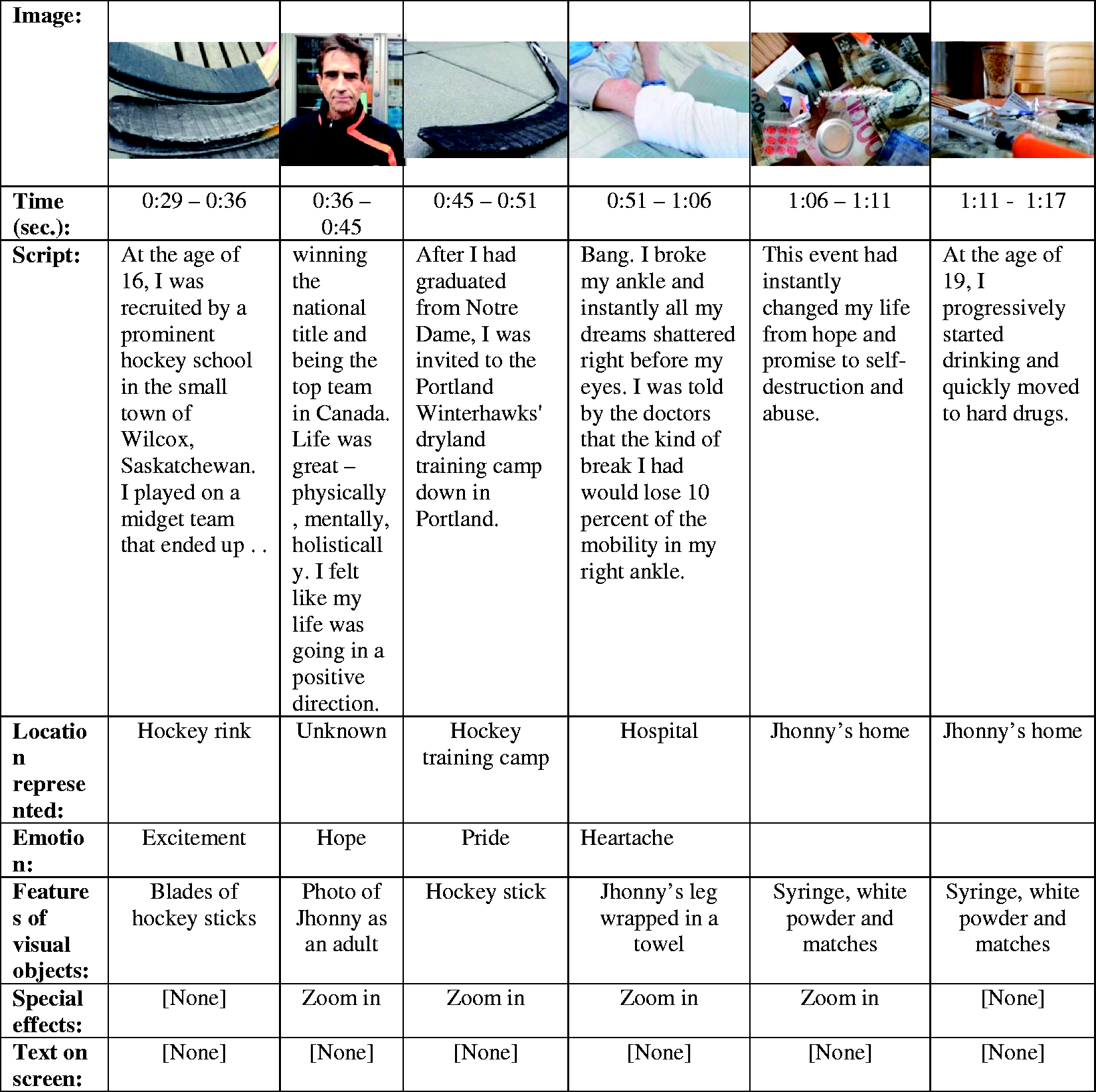
Multimodal media transcript Sample 3. Johnny. A new beginning. StoryTurns, https://vimeo.com/94532540 (2014, accessed 24 October 2018).
As a medium, photography is inherently limited in terms of the amount of information it can convey. Neil Postman claims photographs cannot accurately represent or inform the viewer about a subject’s inner world. 40 Susan Sontag argues that additional narratives can be helpful in allowing photographers to communicate details about their subjects. 41
Without narratives to help the viewer understand drug users’ backstories, photographers risk stereotyping their subjects. What is missing in Clarkes’ and many other photographers’ work is information that communicates the fact that substance users have often experienced significant challenges in their lives. Dr. Gabor Maté, a physician who has worked with drug users in the DTES for decades, writes: “Not all addictions are rooted in abuse or trauma, but I do believe they can all be traced to painful experience. A hurt is at the center of all addictive behaviors.” 42 Cultural and medical anthropologist Philippe Bourgois and photographer Jeffrey Schonberg documented the lives of homeless drug users in San Francisco for 10 years. In their book, Righteous Dopefiend, 43 they present excerpts of lengthy discussions with their subjects in order to share some elements of their backstories.
Photographers have not acted alone in producing stigmatizing narratives about drug users and other vulnerable populations. Government health agencies and lobby groups in the United States and beyond have often disseminated controversial images and messages intended to shame people, including substance users and cigarette smokers into adopting healthier behaviors. Leading politicians and government organizations have also attempted to shame welfare recipients. Highlighting some examples of the trend and the consequences of these actions helps to emphasize the risks of producing photography that stereotypes and villifies people. It also highlights the importance of representing marginalized people, including injection drug users, with dignity and respect.
The Partnership for Drug-Free Kids has used guilt as a central strategy in an attempt to reduce the number of people who use drugs and alcohol in the United States. Researchers have documented how the organization, first known as the Partnership for a Drug-Free America and later on as the Partnership at DrugFree.org, promoted the negative effects of consuming drugs in order to lead people to develop feelings of guilt. 44 This particular emotion is known to prompt people to modify their actions and adhere to laws and regulations.45–48
Anti-smoking activists have repeatedly attempted to shame smokers, which include some of the most economically disadvantaged people. 49 Their campaigns have frequently represented smokers as “deviant” and “pariah[s].” 50 Ronald Bayer 51 argues that tactics such as this could potentially limit the occurrence of illnesses and deaths connected to smoking. He writes that as a result it is appropriate for public health agencies to adopt strategies of this nature. Responding to Bayer, Scott Burris claims it can never be ethical or acceptable to employ stigma as a tactic. He insists that shaming strategies are an “arbitrary and cruel form of social control.” 52 Sholars claim that people who are less well-off account for the highest percentage of smokers.54–57 Researchers argue that health agencies should avoid using stigmatizing strategies in order to avoid contributing to further marginalization vulnerable populations.53,58 Bell et al. add that shaming smokers will not lead to a reduction in smoking rates in economically disadvantaged communities. 53 Instead, they argue this type of campaign could be counterproductive and make it harder for people who smoke to obtain health care and access to programs that could potentially help them stop smoking.
A national campaign coordinated by the American Legacy Foundation that originally began in Florida in 1998 and ran until 2003 known at the Truth Initiative highlighted the negative health effects of smoking and tobacco companies’ specious practices. Its organizers rallied young people in creating counteradvertisements with the intention of shaming these corporations. Their efforts reflect how in certain instances, shaming can be an appropriate strategy. 59
Beginning in 1976 during his presidential campaign, Ronald Reagan claimed he would tackle “the broken welfare system.” 60 He perpetuated the notion that women across the country who were receiving welfare were taking advantage of the system. He focused on a specific woman in Chicago, Linda Taylor, who was alleged to have received $150,000 in welfare payments. 60 Reagan’s rhetoric about the “welfare queen” led government agencies to curtail social security payments to the public and future administrations to restructure the way economically disadvantaged people applied for and received financial support. Under the Clinton presidency, the government discriminated against single women and promoted the idea that marriage was an effective way out of poverty. In doing so, the government failed to take domestic violence into account and the fact that women have the potential to provide for themselves and their families. 61 Scholars have also examined how media organizations engaged in racialized reporting that perpetuated the notion of the “welfare queen” and that visual journalism influenced public opinion about the welfare system. 62 Some of the consequences of stigmatization included an escalation in rates of criminalization and incarceration of people who had received welfare. 63
When it comes to drug users and drug policy in Canada, the former Conservative government frequently communicated inflammatory messages about opioid users and SALOME. According to Merrill Singer and Bryan Page, “mass media and culture industries” as well governments and courts frequently cast drug users as: worthless slackers, evil doers and lurking threats to the quality of life if not to the very survival of civil society—in short, as outcast Social Others with no positive value or useful contribution to society, the human rubbish of contemporary life.
64
I hoped the workshop could help “amplify marginalized voices by bring[ing] people made vulnerable by issues in the center,” as Luna and Luker write. 65 However, my expectations for creating positive change were not very large. I viewed the project as experimental and recognized that participants’ digital stories would likely be viewed by a much smaller segment of the population than that which is exposed to images of the opioid crisis published by mainstream journalism organizations. Nevertheless, by supporting a group of drug users to produce digital stories, my intention was to help create greater awareness about the potential for humanizing drug users through alternative and participatory media practices.
Methods
In what follows, I present details about participant recruitment, efforts to maximize their retention, and the approach that was adopted while facilitating the workshop. I then present an analysis of three participants’ digital stories and how I view them as counternarratives.
Recruitment and Retention
To recruit 10 participants, I created a one-page document outlining the purpose of the study, the activities that storytellers would engage in during the workshop, and that each participant would ideally complete a short film by the end of the process. Social workers at the Crosstown Clinic then circulated the script among SALOME participants. They also spoke directly about the project to some participants.
Several staff members at the Crosstown Clinic had cautioned me that they did not think any SALOME participants would be able to complete the 3-day workshop because what they described as their short attention spans and ongoing challenges in their lives. I proceeded to meet with approximately 20 SALOME participants who expressed interest in taking part in the workshop at the Crosstown Clinic. I spoke about how the workshop would be structured and emphasized that everyone who joined would need to attend the entire workshop in order to complete their digital stories.
I wanted to encourage people who had stories in mind that they were enthusiastic about telling to join the workshop. Many SALOME participants have experienced significant personal challenges, including sexual and physical abuse, poverty, homelessness, and more. People can sometimes benefit in significant ways by telling stories about issues such as these. However, if people are still processing their pain, it can sometimes be premature or unwise to tell these painful stories. I recognized it would be helpful if participants were able to come to the workshop with access to digital or printed photos that they wanted to use in their stories, although this was not a requirement for participation. I also wanted to ensure that participants were fully capable of providing consent to participate. I did not consider drug use to be a barrier to giving consent.
Finally, in consultation with social workers at the Crosstown Clinic, I identified 10 participants and invited them to attend the workshop. All of these individuals arrived at the workshop on the first day. Many expressed excitement and some appeared to be anxious about the process that they were about to embark on. All of the participants were between the age of 25 and 45 years and nearly all lived in the DTES. They had all used heroin for many years, had tried conventional treatments, and had been unable to stop. An equal number of women and men took part.
The workshop was held a half-block from the Crosstown Clinic in a spacious common room on the 10th floor of a residential tower known as Woodwards Community Housing. The building is home to many low-income people, including long-time residents of the DTES. It was not possible to run the workshop at the Crosstown Clinic because of a lack of space in the building. It was also helpful to facilitate the workshop outside of the clinic because this heightened participants’ abilities to focus on producing their stories with relatively few distractions. The workshop space was close enough to the Crosstown Clinic, so participants were able to walk there to receive their treatments 3 times a day and return relatively quickly to the workshop.
I was mindful that staff at the Crosstown Clinic had told me they thought the participants would not be able to complete the workshop. To maximize each person’s ability to produce a story, I invited a number of volunteers to support them. I recruited five students whom I had taught in my role as a faculty member in the Journalism and Communication Studies Department at Kwantlen Polytechnic University in Surrey, BC. They were tasked with assisting workshop participants as they brainstormed story ideas, responded to writing prompts, wrote scripts, took photographs, recorded voiceovers, and edited their stories using digital editing software on tablet computers. I also recruited an equal number of volunteers from PHC who had experience engaging with SALOME participants. A former pastoral care resident at St. Paul’s Hospital volunteered to be present throughout the workshop and played a key role in supporting participants. Together with other volunteers, she planned and led a number of breakout activities that involved physical movement, games, music-making, and drumming. The volunteers’ presence did not overwhelm the participants. I recalled producing a digital story at the Story Center during my training there and how grateful I was to have the support of qualified trainers and technical experts who were on hand.
Prior to the workshop, I spoke with staff members at the Crosstown Clinic about whether it was appropriate or ethical to provide the storytellers with financial compensation. We decided to offer each participant $100 because we thought that along with providing meals and snacks, it could encourage them to commit to the entire storytelling process. We felt that $100, while not too great an amount, could help those who had jobs make up for the financial losses they would experience by taking part in the 3-day workshop. One of the participants collected bottles and another worked at a harm reduction clinic in the DTES.
Workshop Approach
A few of the participants came to the workshop with clear ideas about the stories they wanted to produce. To help stimulate others’ ideas, they were offered the five following prompts and given time to respond to these in writing: What is the story you have always wanted to tell?; What is your greatest inner strength, personality trait or gift that helped you at a critical moment?; Is there someone who helped you during a difficult time?; What has been your greatest challenge? What is your greatest personal accomplishment?
Inviting the participants to focus on their own positive attributes and experiences created the potential for their stories to be biased. In the end, none of the participants told completely positive stories. Virtually all of the storytellers focused on significant obstacles they have experienced and shared details of how they persevered and managed to improve their lives. The writing prompts did not specifically encourage participants to explore their experiences as drug users. In spite of this, all of the participants, either directly or indirectly, communicated personal experiences connected to substance use, including heroin. The purpose of the workshop was not to assess the impacts of SALOME, and participants were never prompted to address the program in their stories. In spite of this, several participants shared details about how they had benefited by taking part in SALOME.
Before participants voice recorded their scripts, the journalism students and I asked their permission to read them. In some cases, we offered suggestions when we thought elements of their stories could be clearer or more detailed. None of the stories required major changes. We were also looking out for stories about difficult experiences that could potentially be too raw or triggering for the storytellers. While facilitating a DST workshop in South Africa focused on gender-based violence and HIV or AIDS prevention, long-time DST facilitator Amy Hill encountered this type of situation. Many of the participants she collaborated with told stories about highly sensitive and personal issues, including abuse. Rather than insisting that storytellers edit the content of their stories, Hill chose not to release the stories on a DVD containing a number of other digital stories. Her decision stemmed from the fact that there is a lack of legal support or counseling services for survivors of domestic violence in the area where the workshop was held. 67 When it came to this workshop, although many participants explored personal and painful experiences in their stories, they were all eager to share them publicly. I did not think it was appropriate or necessary censor them or interfere in this process.
During the workshop, I explained out loud and in consent forms that participants could potentially experience elevated levels of psychological or emotional distress. These risks could come about by recalling and telling troubling or traumatic experiences. Participants were informed they could meet with social workers from the Crosstown Clinic during or after the workshop. None the individuals who took part in the study experienced elevated levels of distress.
To ensure participants’ stories were as unique and personal to them as possible, they were asked to only use original photographs that they or people they know had taken. Just a few participants came to the workshop with images they wanted to use in their stories. I anticipated this and planned a photography session during the workshop in order to allow participants to take photos they could use. I discussed the idea of creating an image bank with the participants and they all agreed that anyone taking part in the workshop could use the photos that they created.
Following a brief session focused on the basics of using digital cameras, participants spent roughly an hour taking photographs in the neighborhood. They were given a list of 10 words, including “beautiful,” “light,” “blue,” “friend,” and “hope.” Participants were invited to photograph objects that that corresponded in their minds with these words. I came up with the list of words, but in the future I will invite participants to do so. I am certain they would have easily come up with words, but early on in the workshop when the photography session was held, I was thinking of Crosstown staff members’ warnings that few participants would likely complete the workshop. This led me to try to be as efficient as possible. I recognize it would have been beneficial for participants to have more opportunities to conceptualize all parts of the workshop.
A student volunteer worked with participants in a separate quiet room to help them voice-record their scripts. Another student edited the voice recordings in order to reduce utterances, repeated phrases, coughs, sneezes, or sounds of sirens, for example, that would be disruptive in the stories.
By the end of the third day of the workshop, 8 of the 10 participants had completed their stories. I considered this a success given the apprehensions that some Crosstown Clinic staff had expressed to me prior to the workshop about people’s abilities to finish the process. The two individuals who did not complete their stories had difficulty focusing during the workshop in spite of the considerable support that was provided. I spoke with them and they did not seem overly disappointed. They told me they were preoccupied with personal issues and that made it difficult for them to concentrate.
At the end of the workshop, the completed stories were screened on a large projector and the participants seemed keen to watch each others’ work. There was a festive and joyful atmosphere in the space. Lambert writes that shared screenings as a way to conclude workshops are helpful to celebrate the participants’ collective accomplishments. 68 I invite you to watch some of their stories as well and listen to the participants in their own words: http://www.storyturns.org/#stories-harm-reduction
Several weeks after the workshop, I conducted individual interviews that lasted approximately 20 minutes with the participants. I wanted to hear directly from them about what motivated them to focus on particular themes in their stories. I asked them if they thought DST was an effective way for them to communicate their story and if they believed their digital story was different than dominant representations of heroin users. I was also interested in learning what they found helpful or challenging about the workshop, skills they learned, and how they felt after completing their stories.
Examining the Digital Stories Produced in the Workshop
In this section, I highlight elements of three participants’ digital stories and examine what makes them counternarratives. I provide intertextual transcriptions and multimodal presentations of key parts of digital stories produced by two workshop participants, Marie and Johnny, in order to demonstrate how these individuals chose and combined different media in order to emphasize particular messages.
“A Love of a Grandma” by Marie
Marie was in her mid-30s and like all of the workshop participants had used heroin for years. She had tried methadone and other treatments several times and has been unable to stop. In one-on-one discussions with Marie, she recalled that when she was a girl she dreamed of becoming a professional dancer and auditioned for the National Ballet School of Canada. Although she was ambitious and talented, the challenges brought on by her mother’s alcoholism and abusive partner made it impossible for Marie to realize her dreams. As a teenager, she started experimenting with drugs and eventually developed an addiction to heroin.
Marie’s 2-minute and 40-second digital story, “The Love of a Grandma,” is a compelling counternarrative told from the personal perspective of a chronic and vulnerable heroin user. In contrast to all of the other workshop participants, Marie chose not to mention heroin or drug use in her story.
Marie begins her story by describing a day when she was younger and at school. She remembers suddenly feeling overcome with emotion and having a premonition that something terrible had happened. She says: I am overwhelmed with some strong, strange feeling that I don’t know. I am shaking like a leaf and it feels like my chest is being crushed and I have a lump in my throat. And all of a sudden, tears are just pouring out of my eyes. I know something is wrong . . . . And for some reason that I don’t know, I get this vision of my grandma in my head. She was my protector, she was my friend, and now she is gone. I ran into my grandmother’s room and I found where she had kept her cigarettes, because the cigarettes were what made her sick. I thought if I smoked I could get sick too so I could be with her like I was yesterday. I ran home and I locked myself in my room. I smoked and smoked and smoked, but nothing happened.
69
Digital stories such as Marie’s could also inform the public and policy makers about some of the positive qualities of chronic and vulnerable heroin users. Dominant media narratives about heroin users rarely if ever portray these individuals in a positive light. We are used to seeing images of drug users pushing needles into their bodies, overdosing and sprawled on the ground, and being revived by first responders. In most of these photos, heroin users are presented as sick, diseased, and as threats to society. Marie’s digital story is unique in the way that she highlights her sense of self-worth, inner strengths, and determination to carry on.
In her postworkshop interview, Marie stated her story is about “loss . . . grief, learning, and life.” She stated she wanted to make a connection between her suffering and her heroin use and communicate this information to the viewer. She said: “Because it [her grandmother’s death] . . . set me on my self-destructive path. It’s what caused that sense of loss and like I didn’t belong anywhere.” 70
When I asked Marie if she thought her story was different than dominant media representations of heroin users, she was concise but clear. She stated: “It’s real. It’s true. It’s to the point.” 70 She added that viewers are able to “see the story behind me” and not the “actual drug use.” Her response suggests that Marie deliberately tried to produce a counternarrative by focusing on her inner experiences and not on the act of consuming an illicit substance. Marie’s willingness to share these deeper and personal elements of her life seemed to allow her to bolster her self-confidence. In her postworkshop interview, she stated: “It kind of makes me want to feel better about myself. It makes me want to not be so hard on myself.”
The way that Marie and others who took part in the workshop combine still images with their own voiceover recordings allows their digital stories to inform the viewer in ways that still images are unable to. When it comes to photojournalism and documentary photography, if captions accompany images, they are able to provide the viewer with basic information and context. In cases when there are no captions or additional narrative, the viewer can be left uninformed about a range of important issues. As noted earlier, when it comes to images of drug users, subjects’ backstories are almost always not communicated to the viewer. DST breaks this convention and if storytellers are willing, they are able to share details about significant moments and events in their lives that help influence how their personal stories and images are understood by the viewer. In this way, DST can be an effective way of educating the public and decision makers about drug users and resist stereotypes and stigma perpetuated by dominant media organizations and others.
Marie matches her words with photographs that she took during the workshop of a puddle meant to symbolize her sadness and tears, an ambulance and stretcher, an ashtray full of cigarette butts, and more. She chose not to include photos of herself that could make her identifiable to viewers. The only image that she uses of herself is one that shows her standing in a park in the DTES, her back to the camera, with her arms outstretched. Paired with the following words, the image communicates how she is optimistic about her future in spite of the challenges she has endured. She says: I guess it’s just perseverance, you know. I know that my grandmother would want me to be here still. She would want me to get to enjoy the beauty of life, to see things that she has seen and not suffer. I’ve suffered long enough. It’s time to enjoy life. It’s time to move on and not be sad and lonely like I have been.
69
“A New Beginning” by Johnny
Johnny is in his mid-40s and has used heroin for decades. His digital story challenges dominant representations of opioid users. Like Marie, he explores parts of his past, his love of hockey, and how he struggled to deal with a devastating physical injury in his youth.
Johnny begins his story with a photo of himself taken in his apartment in the DTES. In the image, he has a wide smile and is holding a photograph of his favorite professional hockey star, Bobby Clarke, who played for the Philadelphia Flyers. In his story, Johnny recalls how he admired the player from an early age. He says: “I was captivated by Clarke’s style and his swagger. I had found an idol.” 71
Johnny describes how he started skating at age 11, “found a purpose in life,” and developed a deep love of his favorite sport. He says: “I trained year-round and caught on to the game of hockey.” 71 He matches his words with a pair of hockey skates and hockey sticks that he took during the workshop.
Johnny then reveals that as a teenager, he was recruited by a prestigious hockey school in the province of Saskatchewan. He describes how he trained intensively and that his team won first place in the country. He then states that his dream of becoming a professional hockey player was dashed after he broke his ankle during a training session. He says: Bang. I broke my ankle and instantly all my dreams shattered right before my eyes. I was told by the doctors that the kind of break I had would lose 10% of the mobility in my right ankle. This event had instantly changed my life from hope and promise to self-destruction and abuse.
71
The DST workshop process enabled Johnny to engage in a deep level of introspection and communicate details of his backstory to viewers. He makes a connection between the crushing disappointment he felt about his ankle injury and how he started to use drink alcohol and later began to use drugs. The way that Johnny pairs the words “self-destruction” and “abuse” 71 with images of drugs, a syringe and matches allows him to share critical background information that would not be easily conveyed through images alone on life.
Throughout his story, Johnny includes photos of his own face. In one of the images, he is lying on the floor of his apartment and playing with his pet cat. At this point in his story, Johnny says, “I’ve set some realistic goals that are attainable.” 71 In this photo, Johnny is beaming and looks healthy. He does not look anything like “the ‘suffering,” “monstrous, freakish, diseased Other[s]” 73 that are prevalent in so many photographers’ images of drug users. The fact that the viewer can hear Johnny’s voice and see photos of him allows Johnny to humanize himself in his story.
Johnny’s statements in his postworkshop interview suggest that his digital story, like others produced in the workshop, could play a role in educating the public and decision makers about the reasons why some people experience opioid addiction.
Johnny said he felt compelled to highlight in his story how he was determined to improve his quality of life without stopping using opioids. He said: I wanted to get across the point, being, you could have something detrimental happen to you, you can either take one or two roads, I took a road that was close to me dying but through people helping me and getting me the right support I managed to get my life on track . . . I think for myself it was an effective way in telling my story because a lot of people can relate to having something happen detrimental in their life.
74
“I Wanted to Clean Up My Life. I Wanted to Live Again” by Oralie Sagmoen
Oralie Sagmoen is a middle-aged woman who has used heroin for years. In her story, she describes how she struggled to build a healthy and positive life. She describes reaching a point where she wanted to get support, but she did not know where to turn. She says: “When you’re a drug addict and you’ve exhausted all your finances and friends and family, and you’re left standing alone. Yea, it’s a pretty dark place.” 75 Sagmoen matches these words with images of a DTES alley and spray-painted graffiti on brick walls and wooden boards. Her voiceover and images combine to create a bleak picture of the state she was in at that particular time.
Sagmoen recalls finding a women’s shelter in the DTES and was able to stay there. She calls herself “lucky” because there was only space for 12 women at the center, and she presents an image of a four-leaf clover that she created during the workshop. She says: “I wanted to clean up my life. I wanted to live again.” 75
As stated above, although the workshop was not designed to assess the impacts of SALOME, Sagmoen chose to explore how she personally benefited by taking part in the program. For her, “cleaning up” her life does not mean breaking her addiction to heroin. It implies enjoying an improved level of physical health, finding purpose, contributing to society, and taking responsibility for herself. She says: “I don’t get sick anymore. I’m working; I have a job and I just got more hours at work. I have a home. My bills are paid.” 75 She uses a photo of herself standing with a staff member at the Crosstown Clinic in which she is smiling. She also chose an image of a doorway to represent the home she has lived in since starting heroin-assisted treatment. The content of Sagmoen’s personal script that she wrote, the fact that viewers can hear her speaking in her own voice, and the images she uses make her story one that that could be used to educate the public and policy makers. Viewers could learn that there were few resources available to her when she needed them and that she has been able persevere while continuing to use drugs.
Sagmoen also examines her personal relationships in her story. She created a colorful stick-figure drawing to represent four family members. In the picture, they are standing on grass surrounded by red flowers and the sun is shining. It is unmistakably optimistic. She says: “My family and I have had a rocky past, but I was able to rekindle a relationship with my mother and father, which I never thought would be possible.” 75 Her description of this part of her life allows her story to be a counternarrative. It could help inform the public and decision makers that people who use drugs are not always isolated, that many have families, and that loved ones are able to be in positive and healthy relationships with them.
At the end of Sagmoen’s story, she offers encouragement to others in the DTES who may still be struggling. She says: “A lot of people down here, they get in this rut, you know, and it just seems like there’s no way out. I want to say that there is a way out and it can be very rewarding.” 75 Sagmoen matches her words with a photo of herself taken during the workshop. In the image, she is wearing a black t-shirt with the insignia of Vancouver’s Insite Clinic, North America’s first legal safe injection site, where she works. She looks into the lens and appears genuinely content.
In her postworkshop interview, Sagmoen stated that people who use drugs should not be demonized. She underscored how her digital story is a counternarrative and this illustrates how it could be used as an educational resource. She said: People tend to think that drug addicts are all bad but we’re not, and I think that people need to know that, because I think they forget. When you’re in this life for so long, you forget how to feel good about yourself. And, I don’t know, I think people need to know that just because they’re using or if they fall off the wagon, you can still get back on it, and keep going and it’s all good.
76
My story is real and truthful. I think that sometimes the media doesn’t have a real story, you know? That they’re just putting it together from bits and bobs they’ve collected from different people . . . I told the real story. It came from my heart . . . . Real means to me just honesty, very matter of fact—all facts from my point of view. And I have experience. I’ve been down here for 30 years. You know I’ve seen a lot and did a lot. I don’t think that anyone can know what that is like until they actually go through it themselves. So it’s hard to put together a real story unless you’ve been there and done that.
76
Concluding Discussion
Most of the workshop participants agreed to allow me to publish their stories on my DST organization’s website. Although I am pleased to be able to share their stories with the public in this way, the website does not receive a considerable amount of traffic. Documentary filmmakers and DST facilitators have experimented with a range of innovative ways of disseminating stories. Some of these strategies include holding public screenings and discussion forums, creating virtual museums, 77 storing digital stories on USB drives, and handing them to conference attendees and more. UK-based Curiosity Creative uses a repurposed red British telephone booth fitted with a digital screen in order to share digital stories produced by Newcastle residents. 78 I was interested in exploring some of these possibilities and others with PHC. Although officials at PHC stated they were happy with the stories that were produced in the workshop, they did not respond to my invitations to explore opportunities to make the digital stories more accessible to the public, decision makers, educators, and students, and I did not feel it was appropriate to pursue these options without their support and collaboration. The fact that PHC has not been willing to disseminate the stories more widely has not been has not dampened my enthusiasm for DST and its outcomes. I believe the stories produced in the workshop reflect the potential to engage more people who use drugs in a similar process in order to produce further counternarratives at a critical time.
Toronto’s medical officer of health, Dr. Eileen de Villa, has called on authorities in Toronto, Canada’s largest city, to decriminalize possession of all drugs for person use. At the same time, she has urged decision makers to increase “prevention, harm reduction and treatment services.” 79
Many journalism organizations continue to publish problematic and stigmatizing images of drug users. Further digital stories produced by drug users could help educate the public and inform decision makers about the need for effective harm reduction as well as opioid substitution and maintenance programs. The digital stories produced by the participants in this digital workshop illustrate challenge dominant narratives about drug users and could help people understand the connection between addiction and painful experiences.
Facilitating the workshop, conducting this study, and the stories that the participants created inspired me to develop further projects about the opioid crisis.
Following the workshop, I conducted a yearlong study in which I tried to produce counternarratives and humanizing representations of three vulnerable heroin users in the DTES. Two of the project participants were Marie and Johnny, who also took part in the DST workshop and whose stories are examined in this article. The other participant, Cheryl, was also a SALOME participant and did not join the workshop. At the end of the year, I chose 10 photos that I had taken of each person and asked them for their feedback about the images in photo-elicitation interviews. I then combined the images with excerpts of the participants’ audio-recorded interview responses in an online and interactive initiative called as The Outcasts Project (www.outcastsproject.com) (for more details, see Goodman 36 ).
The DST workshop also led me to conduct a further scholarly project aimed at creating counternarratives about the opioid crisis and its victims. For a year, I engaged in semiregular conversations with three individuals. They were personally and intimately connected to Michael Stone, an internationally recognized yoga and meditation instructor, writer, and activist who died from an opioid overdose in July 2017. The purpose of the project was to support the participants in recording nuanced audio testimonies about Mr. Stone and their experiences with grief. Together we have created a digital memorial about him (for more details, see www.losingmichael.com).
I will soon facilitate a DST workshop with opioid users who have experienced nonfatal overdoses and have been revived with Naloxone, an opioid antidote. The purpose of the Naloxone workshop is to help amplify the voices of drug users, resist dominant narratives, and help educate first responders about different approaches to overdose treatment. The partner organization is Vermont Cares, a harm reduction provider in Vermont Theresa Vezina is the organization's associate director and insists that DST could help insists it is important to “open the hearts of the public [about] safety and public health.” 81 It could also be beneficial to hold DST workshops with first responders and paramedics in order to develop an understanding of their impressions of the people they are treating and to assist them in communicating their experiences. I am also interested in facilitating DST workshops with harm reduction researchers and advocates in order to amplify their voices and create further counternarratives about the situation.
In future projects, I am interested in collaborating with partners to increase the visibility of participants’ stories in order to maximize the potential of educating the public, first responders, and decision makers. As noted above, there are many creative ways of disseminating stories produced in DST workshops and supporting public education. Some of the possibilities include hosting public screenings, discussion forums, and running workshops with journalists, including photojournalists and documentary photographers. Scholars and facilitators have used DST to share information and generate dialogue within communities about a range of issues, including challenges that young Native people in Alaska face, 82 obstacles experienced by single refugee women, 23 and sexual health of young and urban African Americans. 83 Together with partners and participants, we could encourage policy makers and educators to introduce digital stories in school-based education programs.
Photojournalists and documentary photographers will not collectively and suddenly alter the way they report on the opioid crisis and drug users. The ways that many continue to represent individuals affected by the situation reflect the aesthetic traditions that have been practiced for decades. It is essential though that photographers begin to question their methods and experiment with less harmful ways of covering the crisis.
In order for this happen, photographers need to become more aware of the impacts of their work that stigmatizes people who use drugs. They must be willing to refrain from producing sensational images and they must have the support of their editors and publishers to do so. Taking more time to develop a rapport with their subjects, learning about their backstories, and trying to communicate this information could help to humanize drug users. The digital stories produced in this workshop illustrate that there can be benefits from telling deeper, humanizing narratives, and providing opportunities for people who use drugs to tell their own stories.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 0.6% Faculty Professional Development Fund at Kwantlen Polytechnic University under grant number 2015–036.