
Abstract
HIV prevalence and transmission is still of public health concern in low-resource climes like Nigeria. Transactional sex is a well-known risk factor for HIV transmission. This study therefore assessed the prevalence of transactional sex and associated factors among women attending the antiretroviral clinic in Sagamu, Nigeria. A cross-sectional study was carried out among 204 women attending antiretroviral treatment center in Sagamu, Ogun State, Nigeria, selected via total population recruitment. Data were collected using a validated, semistructured questionnaire. Respondents’ written informed consent was obtained. The mean age of respondents was 38.3 ± 9.0 years. Two thirds (66%) were in monogamous marriages. About two thirds (64.2%) had at least secondary education. Almost 50% spent more than half of their income on food. About 90% had commenced antiretroviral therapy. The prevalence of transactional sex was 7.4%. Household size (p = .031), marital status (p = .015), reduction of food ration (p = .010), skipping of medication (p = .001), and starving for a whole day (p = .044) were associated with transactional sex. Food assistance programs, socioeconomic empowerment schemes, and targeted counseling should be given to people living with HIV to halt HIV transmission.
Introduction
Globally, it is estimated that close to 37 million people are living with HIV or AIDS and sub-Saharan Africa bears 70% of this burden. About three and a half million people are living with HIV in Nigeria according to 2014 estimates with women aged 15 years and older numbering about 1.9 million. One tenth of the global total of new infections occur in Nigeria; hence, Nigeria remains at the frontier of the spread of HIV.1,2
The pattern of HIV transmission in Nigeria is mainly through the heterosexual route and this accounts for more than 80% of the means by which the virus is spread in the country. Intravenous drug users, female sex workers, and men who have sex with men consist of a group with an increasingly significant role in HIV transmission in Nigeria and are estimated to contribute about 40% to the burden of new infections. 3 The AIDS narrative in the country is said to have been feminized, as women are disproportionally more infected and at risk across most age categories and demography. Some of the factors put forward to account for this disparity include the patriarchal nature of the society, anatomical influences, harmful traditional practices, and norms with the resultant imbalance in the distribution of power and wealth among the sexes. 2
The coinage of the term transactional sex might be relatively new; 4 however, the exchange of sex for material gain has been from time immemorial with documented evidence of such exchanges in early Mesopotamian societies. 5 It involves the transfer of sexual favors in exchange for gifts, money, drugs, or otherwise, out of the formal arrangement of commercial sex work.6–9 Hence, the operational definition of transactional sex was conceptualized as “non-commercial, non-marital sexual relationships motivated by the implicit assumption that sex will be exchanged for material support or other benefits.” 6 Although differentiating transactional sex from commercial sex work can be sometimes blurry, it has been documented that transactional sex involves an implicit notion of the likelihood of sex with benefits, while commercial sex involves an explicit, negotiated, and instant remuneration of a sexual activity. 6
The underlying reasons why women engage in transactional sex exist in a spectrum with “survival sex” at one end and “ostentatious motives” at the other. This therefore implies the involvement of a heterogeneous group of individuals across the social ladder who may be trying to meet basic physiological needs or secure a means to sustain a lifestyle of drugs and affluence.10,11 However, among people living with HIV (PLWH), this form of exchange is usually at the lower end of the range. Survival sex occurs in the setting of desperation and poverty, thereby comprising women’s ability to negotiate safer sex and exposes them to riskier sexual practices with their attendant dangers. 12 It has been documented that women were more likely to have sex for money or food on the days when they or a household member is ill with increased likelihood of engaging in risky sexual activities such as poor assertiveness of condom use, incorrect and inconsistent condom use, and sexual exploitation. 13
PLWH and AIDS represent a vulnerable group in society, just as much as they are at the forefront of the prevention and transmission of HIV.9,13 They face emotional, societal, and financial hardships which are known motivations for women to engage in transactional sex, in addition to issues of gender inequality, lack of financial empowerment, lack of education of the girl child, and deep-rooted cultural practices that stack the odds against women in general and PLWH in particular. 9
The percentage of PLWH on antiretroviral therapy (ART) in Nigeria is abysmal at 20%.1,2 Data suggest that every 10% increase in the coverage of ART treatment causes a 1% decrease in the number of new infections. 1 The minimum recommended adherence to ART is set at 95%, and skipping meals may be associated with poor adherence. 14 The availability of the basic amount of nutrition is also an important aspect of the lives of PLWH as this influences their use of medication; as drugs might be skipped due to the unavailability of food and an overall increase in risky sexual practices.15,16 The vicious cycle of high HIV prevalence, poor treatment coverage, low drug adherence, slow decline in rates of new infections, and the perpetuation of risks factors for the transmission of HIV are firmly entrenched in Nigeria. Each of these factors needs to be addressed to achieve a significant control of HIV transmission in low-resource settings and poor treatment coverage regions. The benefits of ART cannot be overemphasized, as it reduces the rate of new infections, the risk of multidrug resistance, and viral loads while increasing CD4 counts, thereby causing an overall reduction in the burden of HIV.2,17,18
Transactional sex among PLWH is a potential threat to existing control measures against transmission of the infection. It is a documented risk factor for transmission of HIV and other sexually transmitted infections. 19 The factors that drive this high-risk behavior among an already vulnerable group put others at risk of infection and have to be clearly understood. Even though antiretroviral therapy is known to reduce the infectivity of HIV, other factors such as poor treatment adherence, inconsistent condom use, and the risk of acquiring resistant viral strains, often associated with inability to negotiate for safer sex, multiply the risks of transactional sex.7,20 Poor treatment adherence in people taking ART results in failure of preventing viral replication and this may increase viral load and infectivity. 20 In Ghana, 80% of transmission to men was acquired from sex workers. This occurred despite the recorded prevalence of HIV among sex workers being just 4.9%, put in contrast to the implied 100% prevalence of HIV among women attending retroviral clinics. 21 Hence, transactional sex probably stalls existing efforts in improving HIV morbidity and mortality indices among the general population. Adult females in the country still make up close to two thirds of the people living with AIDS, while young women are twice more likely to be living with HIV than their male counterparts. 3 A backdrop to this finding is the fact that women play a significant role both in the family unit but also on a larger economic scale accounting for more than half of the nation’s growth and development. 22
This study, therefore, assessed the prevalence of transactional sex and its associated factors among women attending antiretroviral clinics in Ogun State, Nigeria.
Methodology
Ogun State is one of the six states in Southwest Nigeria. It has a population of about 3.75 million according to the 2006 census. It has 20 local government areas and 2 publicly owned tertiary health facilities: Federal Medical Centre, Abeokuta and Olabisi Onabanjo University Teaching Hospital, Sagamu. These two centers have a large turnout of clients seeking comprehensive HIV treatment care and support services. Also, they serve as the port of call for specialized medical services, teaching, training, and research. Olabisi Onabanjo University Teaching Hospital is the only state-owned tertiary health-care facility and is located in Sagamu. Sagamu is a transit zone connecting Lagos and the rest of the country. Its proximity to Lagos State and Benin Republic largely explains its multiethnicity as well as the high level of commerce and industry within it.
A cross-sectional study was carried out among a representative sample of adult females attending the antiretroviral ARV clinic at Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State, Nigeria. Only returning clients, aged above 18 years and resident within Ogun State, were eligible for participation in the study.
The sample size was calculated using the statistical formula for descriptive studies (Z2pq/d2). Using a prevalence of 5.5% for transactional sex among adult Nigerian women from a previous study, 9 a sample size of 220 was arrived at, allowing for 20% nonresponse, incomplete questionnaires, and other unforeseen challenges with data collection.
All consenting adult females who met the eligibility criteria and accessed care during the study period (4 weeks) were recruited into the study.
Data were collected using a semistructured, interviewer-administered questionnaire. The questionnaire was designed after an extensive literature search and pretested among adult females accessing ARV services in a nearby tertiary health facility (Federal Medical Centre, Abeokuta) with similar characteristics as the study location. The questionnaire had three sections: (a) demographic variables, (b) respondents’ involvement in transactional sex, and (c) factors associated with transactional sex. Data were analyzed using the IBM Statistical Package for Social Sciences version 21.0. Only 204 properly filled questionnaires were included in the analysis. The prevalence of transactional sex was calculated by the proportion of respondents who exchanged sex for food, monetary benefits, or both as documented in a previous study. 9 Frequencies, means, and relevant inferential statistics were calculated. Chi-square test and Fisher exact test were used to determine associations between categorical variables with the level of significance (p) set at .05.
Ethical approval was obtained from the Health Research Ethics Committee of Olabisi Onabanjo University Teaching Hospital, Sagamu. Written, informed consent was obtained from each participant before starting the interview, confidentiality was guaranteed, and privacy was ensured. Respondents were free to withdraw from the study at a time they deemed fit and were assured their decision would not affect their quality of care.
Results
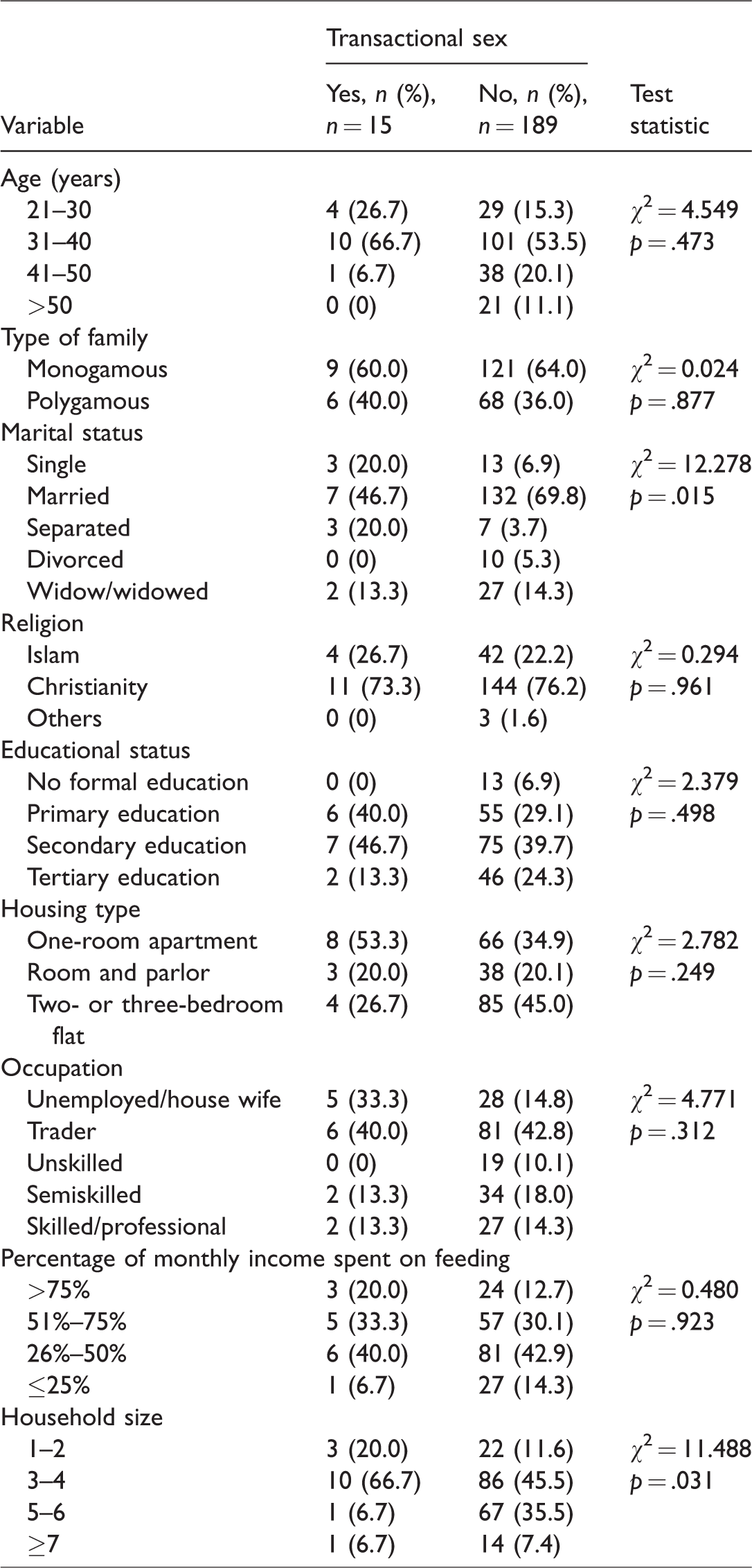
The mean age of respondents was 38.3 ± 9.0 years with the modal age-group being 31 to 40 years. Two thirds (66%) were in a monogamous marriage and majority (76%) were Christians. About two thirds (64.2%) had at least secondary education. About one third (36.3%) lived in a room apartment. Almost half (42.9%) spent more than 50% of their monthly income on food. Majority (87.7%) were not on any food assistance program and more than four fifths (85.8%) had commenced ART (see Table 1). The prevalence of transactional sex was 7.4%. Almost 5% (4.9%) had cause to exchange sex for food over the past 1 year, while 7.4% exchanged sex for economic or financial benefits.
Sociodemographic Characteristics.
Factors Associated With Transactional Sex.
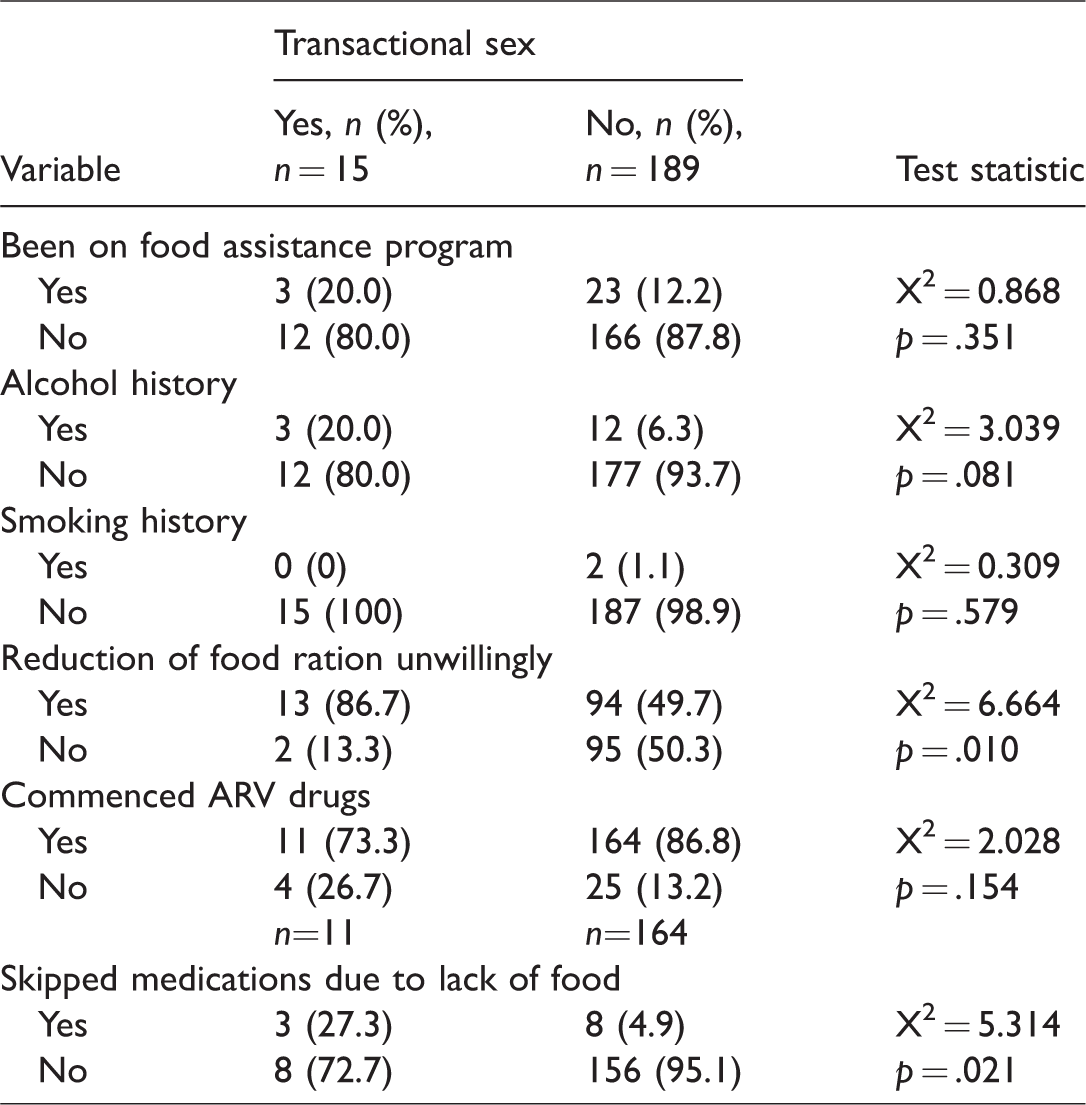
Household size (p = .031), marital status (p = .015), reduction of food ration unwillingly (p = .010), skipping of medications due to lack of food (p = .021), and starving for a whole day (p = .044) were significantly associated with transactional sex. Transactional sex had no significant association with age (p = .473), educational status (p = .498), family type (p = .877), occupation (p = .312), housing type (p = .249), percentage of income spent on feeding (p = .923), and commencement of antiretroviral drugs (p = .154). Being on a food assistance program was not associated with transactional sex (p = .351) even though a higher proportion (20.0%) engaged in transactional sex were on food assistance than those (12.2%) who did not (See Table 2). The monthly income of women who reported engaging in transactional sex was 35,433 ± 3,100 naira (NGN), while it was 31,592 ± 3,200 naira (NGN) among women who did not engage in transactional sex (p = .667).
Discussion
The prevalence of transactional sex in this study was high. Feeding concerns and skipping of medications were significantly associated with transactional sex. These may imply that transactional sex was a survival strategy for those engaged in it. Poor adherence to antiretroviral medication has been shown in the literature, to be a predictor of poor treatment outcome. 23
The mean age of respondents in this study was 38.3 ± 9.0 years with the modal age-group being 31 to 40 years. This was similar to findings in Ibadan (southwest, Nigeria), Port Harcourt (south–south, Nigeria), and Sokoto (north-western, Nigeria) with the mean age of women attending ARV clinic being 33.8 ± 8.9, 34.34 ± 0.66, and 31.4 ± 0.4 years, respectively.24–26
The proportion of respondents engaged in transactional sex in this study was higher than the national prevalence from the demographic health report across some West African countries such as Mali (6.5%), Nigeria (5.5%), Benin (3.7%), Guinea (3.7%), and Togo (2.4%). 9 This might be attributed to the fact that our study population was among PLWH who have been found to be more vulnerable than the general population. 12 In Uganda, a lower prevalence compared with our study was reported at 3.7% which may be due to the younger demography of that study. 12 However, a study in South Africa reported a higher prevalence of 21.1% and this can be attributable to the documented evidence of the high burden of HIV and risky sexual practices among that study population. 8
Fifty-three percent of those who engaged in transactional sex were not presently in any spousal relationship and as such were single, separated, or divorced; this was found to be statistically significant. A similar finding was reported in Uganda where 60% of the women who engaged in transactional sex were not in a spousal relationship. This might be due to the fact they lack financial support from their spouse, for example, in a study in Connecticut, the majority of households below the poverty line that were food insecure were headed by a single parent, and single parenthood was associated with having a low income.12,26 This also compares to a study where married women in all the study countries were significantly less likely to engage in transactional sex than single women. 9 This may be explained by the fact that while marriage offers financial security in HIV negative families as well as deter transactional sex for consumerism in an HIV-positive family, the financial burden of the disease may be high and such families tend to be dysfunctional with reduced earning potential due to decreased productivity.26–29 This was corroborated in a study where those who received money or gifts for sexual favors were less likely to be married. 12 There was no significant difference in how the family setting affected the distribution of those who engaged in transactional sex, and both monogamous and polygamous family settings had nearly equal distribution with respect to transactional sex engagement.
Close to three quarters of those who engaged in transactional sex were Christians in our study compared with 90% in the study in Uganda. This may represent the religious affiliation of the study populations.9,12 In our study, religion did not play a significant role as those who partook in either transactional sex or not fell under roughly the same religious line. This may be due to the fact that all represented religions preach sexual chastity and conservativeness. Hence, the decision to engage in transactional sex could be based more on individual will than the tenets of one’s faith.
Educational status had no significant association with transactional sex in this study. There were higher percentages of people who had primary and secondary education in the group who engaged in transactional sex but a higher percentage of respondents with no formal education did not engage in transactional sex. This was contrasted by the fact that more people with a tertiary level of education did not engage in transactional sex. It has been reported in the literature that individuals who received money or favors for sex were more likely to have the equivalent or lower than primary school education. 12 The discrepancy in the distribution of educational status might be related to the motive for which people engaged in transactional sex; among people with HIV and AIDS, the assumption would be that they engage in transactional sex for desperate reasons. To further put this in perspective, our study found that one third of respondents who engaged in transactional sex were unemployed and about half resided in smaller residential apartments which reflected economic status. However, these associations were not significant.
It was previously documented that the average amount spent on food in Nigeria was 40% of income; 30 this contrasted with the findings in our study where more than 50% of those who engaged in transactional sex spent more than 50% of their income on food. This might lend credence to the belief that transactional sex among people with HIV and AIDS might have a relationship with food security, as the highest percentage of respondents not engaging in transactional sex spent less than 50% of their income on food. The percentage of income spent on food had an inverse relationship with economic status. 30
The proportion of people who engaged in transactional sex who had been on any food assistance program was 20% which was slightly higher than the 12% of people who did not engage in transactional sex but had been on food assistance program. This low prevalence of food assistance among this vulnerable group might be due to paucity of funds, particularly in an era where donor fatigue seems to have set in; it may also be a consequence of the diversion of attention and ultimately funds to the plight of the internally displaced people in northern Nigeria where it is estimated that those in need of food assistance doubled in 6 months to 4.5 million during the peak of the insurgency. 31 In Kenya, where food assistance has been provided to PLWH and integrated into services for the treatment of HIV using a community-based approach, there was an increase in the number of people accessing these services, increased adherence, and better treatment outcomes. 32 The introduction of food assistance programs was shown to increase drug adherence to 98.3% in a Tanzanian study. Therefore, highlighting both the danger of food insecurity and the measures that can be taken to increase adherence, decrease morbidity and mortality, and increase the overall quality of life of PLWHA.33,34
In our study, the prevalence of alcohol consumption was found to be 6% among those who did not engage in transactional sex and 20% among those who did. This was similar to a study in Ibadan, Nigeria, where almost 20% of women in the general population consumed alcohol. 35 However, these findings were lower than the study in Columbus, USA, where 40% of women with HIV consumed alcohol. 36 Tobacco use among respondents was about 1% which was higher than the national prevalence among Nigerian women which stood at 0.4%. 37 This trend of a higher tobacco use in PLWH was also found in a study in New York where PLWH were 3 times more likely to use tobacco than the general population. 38 Substance use has also been associated with poor drug compliance as an indicator of poverty and increase in comorbidities. 39
Close to 90% of respondents who engaged in transactional sex reported an unwilling reduction in food rations as compared with 50% who did not engage in transactional sex, and this relationship was found to be statistically significant highlighting the role of food security and prevalence of transactional sex. This finding was substantiated by the study in Uganda which found that food insecurity increased sexual risk-taking behavior and gave a harrowing account of the challenges women, and in particular PLWHA, go through to provide sustenance for themselves and their families. 40 The consequence of this is reflected by the significant finding in our study that 27% of those who engaged in transactional sex reported skipping their medications as compared with almost 5% of those who skipped their medication in those who did not engage in transactional sex. The inverse relationship between food insecurity and adherence to medication was also described in Atlanta, USA. 41 Also, nonadherence has been attributed to fear of side effects and increase in hunger. 41 While more has to be done to increase the coverage of ART in low-resource settings, provision of ART alone would not efficiently curb the transmission of HIV. Factors encouraging transactional sex among PLWH have to be addressed with respect to providing food assistance programs which not only encourages compliance to ART use but also discourages engagement in risky sexual practices. 15
The study population represents a vulnerable demography in the society and is susceptible to harmful sexual practices which may contribute to the chain of transmission of HIV. Concerted efforts involving all stakeholders should include equitable distribution and availability of food assistance programs, socioeconomic empowerment schemes, and targeted counseling to people living positively with HIV. This will help halt and reverse HIV transmission and optimize HIV control in Nigeria.
Limitation and Strength
This study is a nonanalytical study and could not expressly depict a cause–effect relationship between variables. While we acknowledge the fact that women may deliberately underreport transactional sex due to social norms, concerted efforts were made to overcome every form of social desirability bias. The strictly confidential and private nature of the study encouraged respondents to be open and sincere about their sexual practices. A detailed qualitative study on the subject matter may explore some factors to a greater extent, providing more information on determinants of transactional sex within the social context of the respondents.
Conclusion
Transactional sex among respondents was higher than the national average and was mostly associated with existential challenges. A holistic approach is expedient in dealing with the situation, particularly as regards the potential risks it poses toward HIV control. The findings on transactional sex and its associated factors, from this study, may therefore require some modification to service delivery to consider the existential needs of women accessing those services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.