
Abstract
Background
The individual knowledge of the effects of tobacco usage on health plays an important role in its uptake. Tobacco consumption usually starts during adolescence, and lack of knowledge about the oral problems of tobacco usage probably plays a role in it.
Aim
To determine the knowledge of adolescents about the effect of tobacco usage on oral health.
Methods
A cross-sectional study was conducted among 1,465 adolescents aged 12 to 20 years who attended senior secondary schools in a major city in Nigeria. Data were obtained through a semistructured questionnaire. Data obtained were analyzed with SPSS.
Results
The mean age of respondents was 15.2 (±1.4) years. Only 40 (2.7%) of them used tobacco at the time of study and 992 (67.7%) said that tobacco usage has effect(s) on oral health. The main effects mentioned were mouth odor: 338 (34.1%); teeth discoloration: 297 (29.9%); tooth decay: 138 (13.9%); damage to teeth: 72 (7.3%); lip discoloration: 39 (3.9%); and oral cancer: 11 (1.1%). It was found that female respondents (72.1%, odds ratio = 1.4, confidence interval = 1.1–1.7, p = .005); those aged 12 to 15 years (73.6%, odds ratio = 2.0, confidence interval = 1.6–2.5, p < .001); and children of skilled workers (73.4%, odds ratio = 1.9, confidence interval = 1.2–3.0, p = .008) were more likely to mention that tobacco has adverse effect(s) on oral health.
Conclusion
Although two thirds of the students knew that tobacco usage has effects on oral health, there were gross inadequacies in the knowledge and misconceptions about those effects.
Introduction
Tobacco usage is a leading public health problem worldwide, and it is responsible for the death of more than 7 million people a year. 1 Tobacco usage is on the rise with the incidence being sustained by initiation of adolescents to the population of users. 2 More than 2,800 adolescents are initiated daily into the population of tobacco users. 1 Tobacco usage usually starts in adolescent years as evidenced by the finding that most adult smokers initiated their smoking habit during adolescence.3–5 Surveys conducted among adolescents showed a wide variation in current smoking rates: 8.6% in the United States, 6 10.2% in India, 7 20.2% in Saudi Arabia, 8 8.5% in Zimbabwe, 9 19.3% in Madagascar, 10 12.6% in a study carried out among some selected African countries, 11 and 3.3% to 5.7% in Nigeria.4,12,13
Interventions have been instituted in different countries with the aim of curbing tobacco usage and to discourage it among adolescents.14,15 The interventions have not resulted in a significant downward trend in the rate of cigarette smoking globally. 15 The persistence of tobacco usage among adolescents may be due to lack of appropriate interventions or, probably, deficiencies in the interventions made.15,16 Among several methods of discouraging tobacco usage and encouraging those already using it in quitting, health warnings about its adverse effects on personal health has been one of the most effective. 17 Knowledge about the effects of tobacco usage on health had been documented to result in the reduction of the prevalence of adolescents who had initiated smoking.1,16–18 Likewise, the knowledge has also increased the number of tobacco users who have quitted the habit.1,17
Unfortunately, studies have also shown that comparatively few people understand the specific risks of tobacco usage on general health and probably much less have the knowledge about the oral health problems associated with it. 1 Surprisingly, relatively sparse information exists about the knowledge of oral problems associated with tobacco usage among adolescents. More so, the mouth remains the most frequent route of tobacco usage. These coupled with the fact that individual knowledge of adverse health effects of tobacco plays an important role in its uptake and usage 19 offered a research avenue on the knowledge of adolescents about the oral effects of tobacco usage. This will provide baseline information that is important in planning further interventions on dissuading adolescents from initiating, or persuading them in quitting, tobacco usage. The study thus aims to find out the knowledge of adolescents about the effect of tobacco usage on oral health in Ibadan, Southwest Nigeria.
Materials and Methods
Study Setting
A cross-sectional study was conducted among adolescents aged 12 to 20 years attending senior secondary schools in Ibadan, Nigeria. Ibadan is the capital of Oyo State in Southwest, Nigeria. It is the largest city in West Africa. The students who participated in the study were from randomly selected schools in Ibadan. A minimum sample size of 1,363 participants was calculated based on a power of 80%, confidence interval of 95%, nonresponse rate of 10%, and proportion of smokers of 3.3% from a previous study. 13
Ethical Approval
Ethical approval for the study was obtained from the Ethics Committee of the State Ministry of Health. Permission to conduct the study was obtained from the State Commissioner for Education. Permission was also obtained from the principal of each school that participated in the study before entering the school for data collection. In each school, the students recruited for the study were selected from the school registers using a table of random figures. All selected students were gathered in a classroom and the purpose of the study was explained to them and their questions concerning the study were entertained. Each student was then given an informed consent form to present to the parents irrespective of their age to conform to the regulation of the schools. The consent forms were available in both English and Yoruba, the local language, to ensure proper understanding of the purpose and process of the study as well as to facilitate understanding of the parents/guardians who were not fluent in English.
Sampling
The schools were selected using a multistage sampling technique. In the first stage, 4 local government areas (LGAs) were randomly selected from the 11 LGAs within the city. In the second stage, five schools from each LGA were selected using a table of random numbers with the list of schools obtained from the State Ministry of Education. The last stage involved recruiting 26 students from each of the three senior secondary school classes making 78 students in each school and a total of 1,560 students overall. Out of this number, 1,465 students consented to participate in the study, that is, a response rate of 93.9%.
Questionnaire
Data for the study were collected using a semistructured questionnaire, which elicited the sociodemographic characteristics of the respondents; the questions assessed the age of the respondents; educational qualification of the father or guardian, categorized into none, primary, secondary, and tertiary; and the occupation of the father or guardian. Occupation was further classified into classes, based on a modification of Office of Population Census and Surveys classification that has been used in the environment,20,21 as skilled job, unskilled job, and dependents. Other questions in the questionnaire assessed if the respondent consumed tobacco in any form, that is, if currently or actively smoking (defined by respondent smoking consistently in the last 6 months). The perceived effects of tobacco usage on oral health were presented as an open-ended question: “What are the perceived effects of tobacco usage on oral health?” The questions on the effects of tobacco use on oral tissues were also assessed with response on a Likert scale: Strongly agree, Agree, Don’t know, Disagree, and Strongly disagree. The students filled the questionnaires under the guidance of a dentist to minimize nonresponse. The questionnaire was pretested among 56 students in a senior secondary school in an LGA not selected for the study to ascertain the feasibility of the study, comprehensiveness of the questionnaire, and its validity.
Data Management and Analysis
Data obtained were analyzed using SPSS version 23 after content analysis was carried out. Similar responses to the open-ended questions were grouped together after two independent research assistants read them several times. Thereafter, codes were assigned and data were entered into SPSS. The frequency of the occurrence of the codes was presented using proportions. Numeric variables, such as age, were summarized using means and standard deviations. A test of the association between categorical variables—sociodemographic characteristics and response to the question on the effect of tobacco usage on oral health—was done using chi-square statistics. Variables significant at p < 5% at bivariate analysis were further subjected to multinomial regression and p value set at < 5%. Knowledge of oral effects of tobacco was taken as the dependent variable and positive knowledge (mentioning that tobacco usage has an oral effect) was taken as reference.
Results
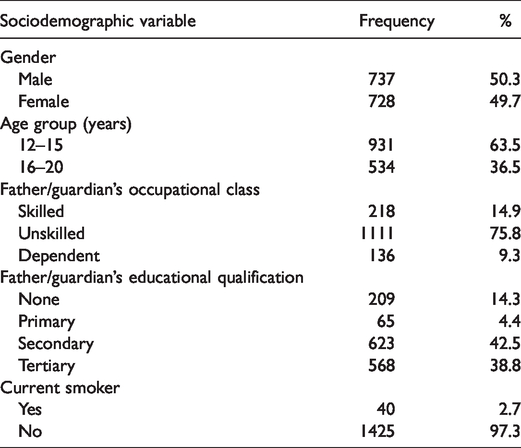
A total of 1,465 students participated in the study. The age of the respondents ranged from 12 to 20 years and the mean age was 15.2 (±1.4) years. There were 737 (50.3%) male students and 728 (49.7%) female students. Three quarters of the fathers or guardians (1111, 75.8%) were unskilled workers. Many fathers or guardians (623, 42.5%) had secondary school education, that is, had completed the 12th grade (Table 1).
Characteristics of Participants (N = 1,465).
Forty (2.7%) respondents currently smoked and the same number used tobacco in its various forms. Two thirds of the respondents (992, 67.7%) mentioned that tobacco use has an effect on oral health. The effects of tobacco usage on oral health mentioned by those who reported that tobacco has oral effect included mouth odor (338, 34.1%), teeth discoloration (297, 29.9%), tooth decay (138, 13.9%), damage to the teeth (77, 7.8%), lip discoloration (39, 3.9%), oral cancer (11, 1.1%), and burning of the teeth (3, 0.3%). Only three respondents indicated that tobacco usage had a positive effect on oral health. About 236 (23.8%) could not mention how tobacco usage affects oral health (Table 2).
Effects of Tobacco Usage on Oral Health Reported by Participants (N = 992).
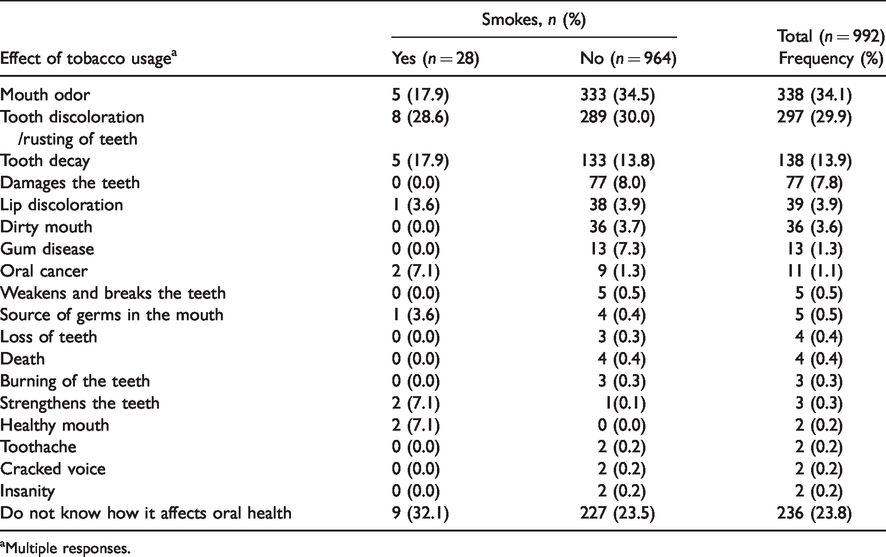
aMultiple responses.
Among all respondents, many (1,002, 68.4%) strongly agreed or agreed that tobacco use had harmful effects and 463 (31.6%) did not know that tobacco use had harmful effects on the oral tissues. Quite a number of students (1,226, 83.7%) strongly disagreed or disagreed that tobacco usage was beneficial to oral health; 3 (0.2%) agreed that tobacco usage was beneficial to oral health; and 236 (16.1%) did not know if tobacco usage was beneficial to oral health. Of the three who agreed that tobacco usage was beneficial to oral health, two (66.7%) were smokers.
Bivariate analysis of the sociodemographic characteristics of the respondents and their knowledge about oral effects of tobacco usage showed that the gender, age, and father’s or guardian’s occupational class were significantly associated with the knowledge that tobacco usage has an effect on oral health (Table 3). More female students than males (52.9% vs. 47.1%), students aged 12 to 15 years compared to 16 to 20 years (69.1% vs. 30.9%), and those students whose fathers or guardians were in the skilled worker class compared to others (16.1% vs. 76.1% vs. 7.9%) mentioned that tobacco has an effect on oral health (Table 3). There was no relationship between sociodemographic characteristics and respondents currently using tobacco.
Sociodemographic Variables and Knowledge of Oral Effects of Tobacco Usage (N = 1,465).
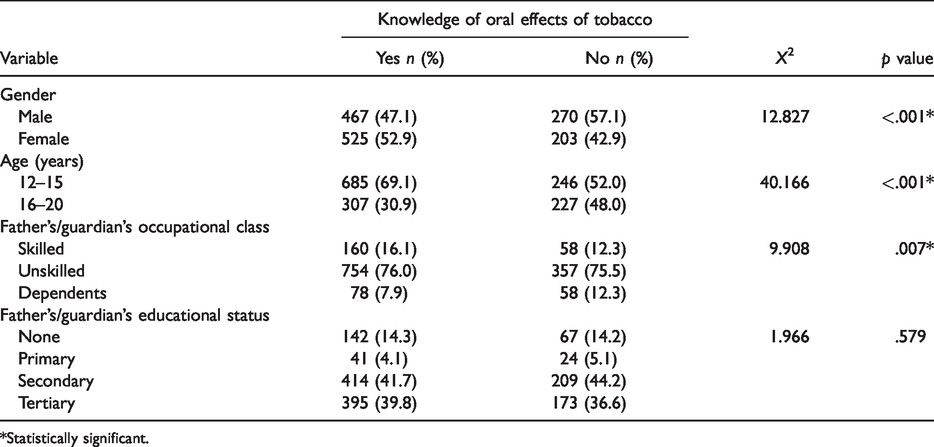
*Statistically significant.
On multivariate analysis (Table 4), it was found that female students, students aged 12 to 15 years, or students whose fathers or guardians were skilled workers had higher odds (odds ratio = 1.4, 2.0, and 1.9, respectively) of perceiving that tobacco usage had negative effect on oral health when compared to others.
Multivariate Analysis of Sociodemographic Variables and Knowledge of Oral Effect of Tobacco Usage Among Participants.
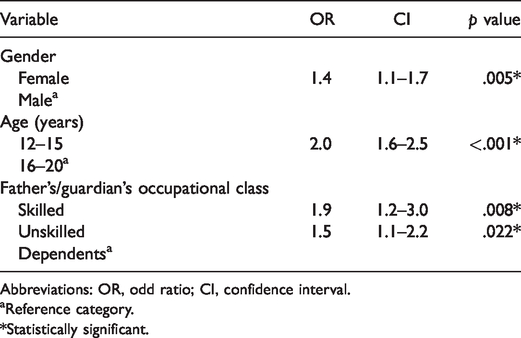
Abbreviations: OR, odd ratio; CI, confidence interval.
aReference category.
*Statistically significant.
Discussion
This study showed that there is a gross lack in knowledge about the oral effects of tobacco usage among the adolescents studied here. It was observed that about one in three adolescents did not know that tobacco usage has an effect on oral health; one out of every four that had this knowledge could not mention a single oral effect of tobacco usage. Overall, almost half (48.4%) of the adolescents either did not know that tobacco usage has an effect on oral health or could not mention any one effect from its usage. This is quite worrisome; more so that studies have identified the importance of perceived negative health effects of tobacco usage as a major factor in the decision against uptake of tobacco usage or for the intention to quit it.1,17,18 Importantly, tobacco control advocates need to make urgent intervention to educate adolescents about the ill-health effects of tobacco usage.
About 3% of adolescents in this study smoked at the time of study. This finding is similar to that of a previous study conducted in Port-Harcourt where a prevalence of smoking of 3.3% had been reported among adolescents. 13 The prevalence is, however, lower than that reported in Ilorin in another study, which reported a prevalence of 5.7%. 12 The differences in the prevalence rate of tobacco use noted in these studies may be attributed to the ages of the respondents, which was similar between this study and that conducted in Port-Harcourt. Conversely, the respondents in this study were much younger, with a mean age of 15 years, than those recruited in Ilorin with a mean age of 21 years. 12 It is probable that the proportion of tobacco users will rise with increasing age. 15 The proportion of adolescents using tobacco in any form in this study as well as in other previous studies from Nigeria12,13 appeared to be lower than the figures obtained from other settings where prevalence ranging from 8.5% to 20.6% had been reported.6–11 The reasons for the lower prevalence of tobacco usage among Nigerian adolescents compared to their counterparts may be multifactorial but not limited to cultural reasons, socioeconomic considerations, and access to tobacco products.4,6–13,15,17
The results showed that a higher proportion of nonsmokers agreed that tobacco usage has specific oral effects. This finding is similar to that of a study conducted among public school-going adolescents aged 15 to 19 years in Saudi Arabia where the odds of smoking were reported to be 22% to 47% less among those who were aware of the harmful effect of smoking on oral health compared to their colleagues who were less aware. 18 This further strengthens the idea that if adolescents are equipped with better knowledge about the health effects of tobacco usage, the prevalence of uptake and use of tobacco is likely to reduce among them. Also, this study showed that the majority of the few respondents who knew that tobacco usage has positive effects on oral health were all current smokers. Thus, having a perception that tobacco usage has positive benefits on oral health may be a factor associated with its use as well as future uptake as opined in previous studies.16–18
Very few students could correctly mention the oral effects of tobacco usage. Oral cancer is one of the most widely researched and reported causally linked oral effect of tobacco usage, and several studies19,22–24 have documented higher knowledge of oral cancer as one of the effects of tobacco amidst other effects on oral health. This is, however, not the case in this study, as only 11 (0.8% of the total participants and 1.1% of those who mentioned that tobacco had effect on oral health) mentioned oral cancer as one of the possible effects of tobacco usage. One of the possible reasons for this very poor knowledge about oral cancer being one of the oral effects of tobacco usage could be attributed to the general low level of oral health awareness among adolescents 25 and the general populace in Nigeria. 26 Misconceptions about the oral effects of tobacco such as brittle teeth and burning of the teeth reported by some students further confirm gross deficiencies in the knowledge base about oral effects of tobacco usage among adolescents.
The study also found that younger adolescents compared to older adolescents had a higher odd of perceiving tobacco to have negative effects on oral health. This is significant because while it would ordinarily be expected that as adolescents get older, they should be better informed, as noted in a previous study where older adolescents had better oral health knowledge. 25 The opposite is the case among this study population. This would suggest that further studies are required to elucidate the seeming reversal of what is expected as well as investigating the possible reasons for such finding. Gender was another factor in the perception that tobacco usage had negative effects on oral health. That females have a better attitude toward oral health 22 may be a possible reason for this finding. Students whose parents had skilled jobs were also more likely to mention that tobacco had negative oral effects. The association between high socioeconomic status and positive oral health has also been documented. 27
Limitation
A limitation of this study is that only public schools were included in the study. Stratifying the LGAs into rural or urban and schools into public or private would have ensured better representativeness and hence generalizability. In addition, this study focused solely on students, excluding out of school adolescents in whom prevalence of tobacco use is worse. However, the study is aimed at providing baseline information on the need for inclusion of educational programs on tobacco usage as part of school oral health program in Ibadan and Southwest Nigeria at large. In terms of strength, this study investigated a very important aspect of tobacco usage—negative oral health effects of tobacco consumption, which has hitherto been sparsely studied, especially among adolescents.
Conclusion
This study showed that although two thirds of the students knew that tobacco usage has effects on oral health, there were gross inadequacies in the knowledge as well as misconceptions about those effects. An active intervention to improve the knowledge and perception of adolescents in schools on effects of tobacco usage on oral and general health is, therefore, important.
Supplemental Material
QCH896730 Supplemental Material - Supplemental material for Knowledge of School-Going Adolescents About the Oral Effects of Tobacco Usage in Ibadan, Southwest Nigeria
Supplemental material, QCH896730 Supplemental Material for Knowledge of School-Going Adolescents About the Oral Effects of Tobacco Usage in Ibadan, Southwest Nigeria by Folake B. Lawal and Omotayo F. Fagbule in International Quarterly of Community Health Education
Footnotes
Acknowledgments
The authors acknowledge Dr. Taiwo Lawal for the statistical inputs and proof reading of the manuscript. The authors also acknowledge all the school teachers, heads of schools, and the officials of the Oyo State Ministry of Education for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Consortium for Advanced Research Training in Africa (CARTA). CARTA is jointly led by the African Population and Health Research Center and the University of the Witwatersrand and funded by the Carnegie Corporation of New York (Grant No.: B 8606.R02), Sida (Grant No.: 54100113), the DELTAS Africa Initiative (Grant No.: 107768/Z/15/Z), and Deutscher Akademischer Austauschdienst (DAAD). The DELTAS Africa Initiative is an independent funding scheme of the African Academy of Sciences (AAS)’s Alliance for Accelerating Excellence in Science in Africa (AESA) and supported by the New Partnership for Africa’s Development Planning and Coordinating Agency (NEPAD Agency) with funding from the Wellcome Trust (UK) and the UK government. The statements made and views expressed are solely the responsibility of the Fellow. The funding body did not play any direct role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author Biographies
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.