
Abstract
Researchers have identified cancer, diabetes mellitus, cardiovascular, and respiratory diseases as being the principal pathologies of increased aged standardized death rates (ASDRs) among noncommunicable diseases (NCDs). The objective of this study was to compare the change in the ASDR of these principal NCDs between the years 2010 and 2016 in Botswana, Mozambique, Namibia, South Africa, and Zimbabwe. ASDR data were collected from the 2016 Global Health Estimate. Among the selected Southern African countries for both 2010 and 2016, the order of prevalence of NCDs linked to increased ASDR was cardiovascular diseases (both cardiac and stroke), cancer, diabetes mellitus, and chronic respiratory diseases. The percentage of the total number of NCDs linked to increased ASDR in relation to total deaths increased from 43.8% (in 2010) to 51.0% (in 2016) from (p < .0001). The percentage of principal NCDs in relation to total ASDR increased from 33.0% (in 2010) to 38.2% (in 2016; p < .0001).
The global health and wellness profile have undergone remarkable changes within the last 40 years 1 : the primary cause of disease and disability has moved from communicable diseases to noncommunicable diseases (NCDs). 2 Longevity has increased in many parts of the world, primarily due to improved communicable and NCD management (Dishman et al.), with the decline in NCD aged standardized death rates (ASDRs; mortality) in high-income countries primarily attributed to early identification, better medication, sound multidisciplinary medical counseling, improved nutrition, regular physical activity, and alcohol, sugar sweetening, and tobacco taxation.3,4 Africa remains, however, a predominantly low-income continent and is still struggling with effective management of communicable diseases as well as with the provision of quality neonatal and maternal care, where difficulties in surmounting nutritional deficiencies contribute to the problems faced. 1 This scenario is further compounded by the emergence of NCDs, which are expected to become the leading contributor to mortality by 2050. 5 The incidence of cardiovascular diseases (heart and stroke), chronic respiratory disease, and diabetes mellitus has been predicted to increase geometrically over the next three decades, becoming the primary causes of NCD mortality on the African continent. 5 Cardiovascular diseases have already been identified as the leading cause of NCD mortality, with ischemic heart disease being the primary pathology of cardiovascular NCD mortality.2,6 In a global survey, Owolabi et al. reported that cerebrovascular disease (stroke) is the second ranked cardiovascular disease contributor of NCD mortality with a mortality prevalence of 70.9%, and 77.7% disability-adjusted life years lost in low- and middle-income countries (many of which are countries on the African continent). 6 The NCD epidemic is thus a significant medical concern on the African continent.4,7
Strong et al. recommended that a goal of reducing premature death caused by non-communicable diseases (NCDs) by 2% annually be set, receiving unanimous consensus at the United Nations NCDS summit in 2011.4,8 The United Nations went further in adopting a very ambitious goal of decreasing the premature NCD mortality rate by 25% by the year 2025 (using a 2010 level baseline), targeting the following principal NCDs in particular (cardiovascular and cerebrovascular diseases, chronic respiratory diseases, diabetes mellitus, and cancer).9,10 The aim of this article was to review the NCD ASDR for the aforementioned principal NCDs in the interim period from 2010 to 2016 in the following southern African countries: South Africa, Namibia, Zimbabwe, Botswana, and Mozambique.
Methods
This study’s design was observational and descriptive: ASDRs were gathered from the Global Health Estimates (GHEs) 2016.
11
This method of gathering mortality rates has proven to be both successful and reliable having been used in previously published literature.4,11 Nojilana et al. used ASDR data gathered from the GHE 2010 in order to determine the developing configurations of NCD mortality in South Africa during the 1997 to 2010 period.
4
This study reviewed the ASDR of the following selected principal NCDs: cardiovascular (rheumatoid and ischemic heart disease, hypertension, cardiomyopathies and cerebrovascular—stroke), diabetes mellitus, chronic respiratory disease,s and cancer in countries in Southern Africa. In this study, cardiac NCD pathology related to rheumatoid and ischemic heart diseases, hypertension, and cardiomyopathies. The Southern African countries included in the study were Botswana, Mozambique, Namibia, South Africa, and Zimbabwe. The GHE is public domain data; therefore, the manuscript did not require ethical approval. A comparative review of 2010 and 2016 GHE ASDR data was conducted for the aforementioned NCDs.
11
Percentage change was determined by the following formula:

Descriptive (mean, standard deviation, percentages, and frequencies) and inferential statistics (t test and correlation) were used. Probability was set at p < .05.
Results
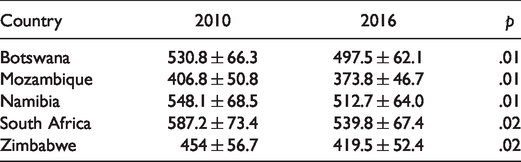
Table 1 displays the ASDR for all deaths, all NCD deaths, the selected principal NCD deaths for 2010, and percentage change for selected principal NCD deaths/total death rates. Similarly, Table 2 displays the comparative overall mortality rates, all NCD mortality, and selected NCD mortality rates for 2016. Table 3 shows the comparative percentage of ASDR between 2010 and 2016. There was a significant upsurge in the percentage of total NCD ASDR from 2010 to 2016 within each country and among countries (p < .01; Table 4). Tables 1 and 2 provide a more accurate picture of the percentage growth of NCD mortality rates between 2010 and 2016. There was a positive correlation between ASDR data reflecting hypertension and stroke as the cause of death (r = .67).
Comparative Overview of Total Number of Deaths, Total NCDs Deaths, Selected NCDs ASRD in 2010 Within the Selected Countries.
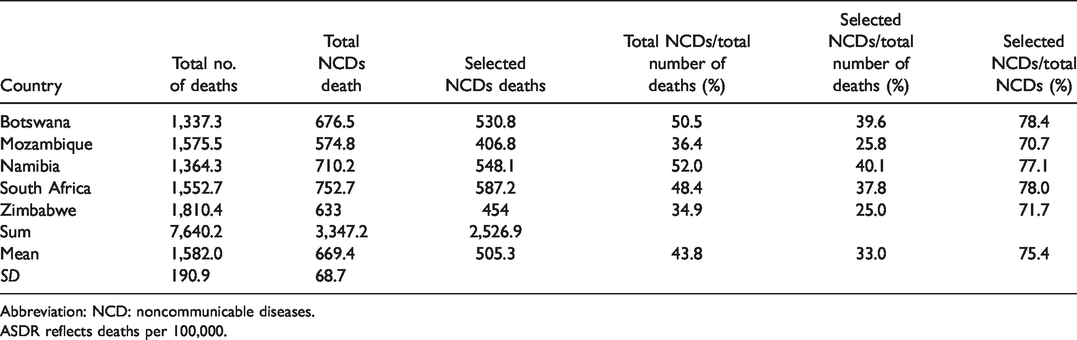
Abbreviation: NCD: noncommunicable diseases.
ASDR reflects deaths per 100,000.
Comparative Overview of Total Number of Deaths, Total NCDs Deaths, Selected NCDs ASRD in 2016 Within the Selected Countries.
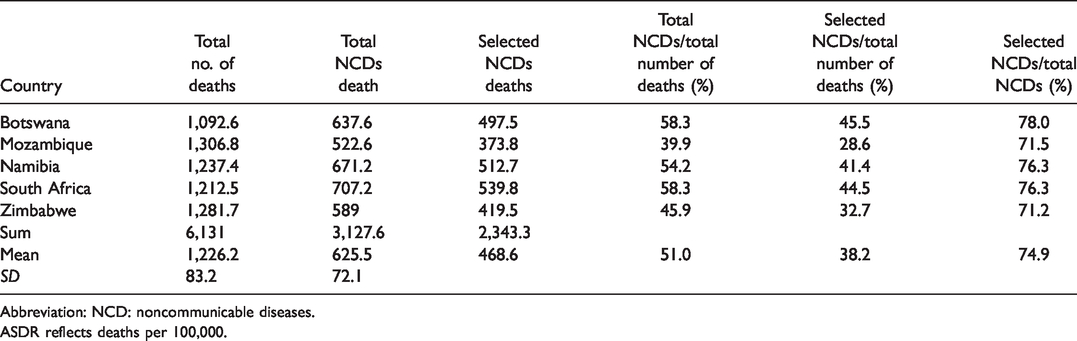
Abbreviation: NCD: noncommunicable diseases.
ASDR reflects deaths per 100,000.
Comparative Review of the Selected NCDs ASDR Between 2010 and 2016.
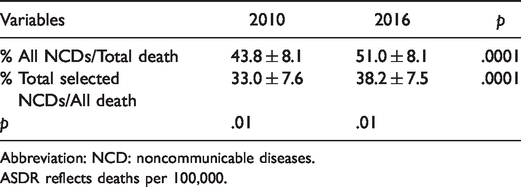
Abbreviation: NCD: noncommunicable diseases.
ASDR reflects deaths per 100,000.
Comparison Among the Sum of Selected Principal NCDs for 2010 and 2016.
In 2010, the estimated total ASDR for the aforementioned selected Southern African countries was 764,020,000 of which total NCD mortality contributed 43.8% (334,720,000; Table 2). Further statistical stratifications show that the principal NCDs accounted for 33.0% of overall deaths in these selected Southern African countries (Table 1). In 2016, the estimated total ASDR was 613,100,000 of which 51.0% were total NCDs deaths (312,760,000; Table 2) with the selected NCD mortality accounting for 38.2% of total NCD mortality (Table 3). Although the estimated total NCD mortality rate of 2010 (334,720,000) dropped in comparison to 2016 (312,760,000), this is a misleading statistic; consider rather that the percentage change of selected NCD mortality from 2010 to 2016 increased by 13.6% a statistic which offers a more realistic overview. Similarly, total NCD deaths increased by 14.1% from 2010 to 2016. The percentage change of selected NCD ASDR from 2010 to 2016 was calculated as follows:


The order of NCD ASDR prevalence among the selected southern African countries for both 2010 and 2016 is cardiovascular diseases (cardiac and stroke), cancer, diabetes mellitus, and chronic respiratory diseases. However, when stroke data for 2010 and 2016 are reviewed as an independent principal NCD, the order can be given as cardiac diseases, cancer, stroke, diabetes mellitus, and chronic respiratory diseases. The percentage ASDR of selected NCDs progressively increased from 2010 to 2016 (p < .0001).
Discussion
The discussion is organized as follows: a comparative review of total NCD mortality which is then amplified by a consideration of the impact of selected cardiovascular diseases, chronic respiratory diseases, diabetes mellitus, and cancer among the selected Southern African countries.
Total NCDs Mortality
Although total ASDR has dropped by 19.7% from 2010 to 2016, the total number of NCD ASDR increased by 14.1% and the selected principal NCDs increased by 13.6% in the given time period. 11 In 2010, total NCD mortality was responsible for 43.8% of all deaths in the selected Southern African countries, a figure that fell below the comparative global figure where 60% of all deaths were attributed to NCDs. 11 The unique findings of this study are that the selected principal NCD (cardiovascular and chronic respiratory diseases, diabetes mellitus, and cancer) ASDRs were responsible for 33% of total deaths in the aforementioned countries in 2010, confirming the hypothesis that the aforementioned NCDs are the major contributors to mortality. 11 In 2016, however, total NCD mortality accounted for 51% of the total mortality in the selected countries, showing steep growth in the prevalence of NCD mortality. 11 Further stratification shows that the selected principal NCDs account for 38.2% of all deaths in these countries. A further and more worrisome statistic is that the 2016 ASDR of the selected NCDs has increased by approximately 13.6% from the 2010 statistics, moving in the opposite direction of the strategic goals adopted by United Nations.4,10 These findings concur with Ojji et al. and Chetty who reported that NCDs are on the rise in Africa.1,2 The novelty of this study’s findings lie in the fact that they show an increase in premature NCD deaths, more specifically as concerns the selected principal NCDs for the interim period of 2010 and 2016. Furthermore, this article differs from the study undertaken by Nojilana et al. who reported on the NCD mortality rates, focusing only on data from South Africa between the periods of 1997 to 2010. 4 This study reviews the estimated NCD mortality rates of five southern African countries, thereby providing a more holistic view of the NCD epidemic in this region between 2010 and 2016. It is recommended that more sound strategic medical and clinical therapeutic interventions need to be adopted in the aforementioned countries in so far as NCD management is presently limited to early identification, prudent counseling, dietary changes, and pharmacological medication.2,4,12 There is a need for structured regular exercise therapy as Dishman et al. have shown that exercise therapy is successful in the management of NCDs, being particularly successful in the management of the principal NCDs that have been identified in this article. 3
Cardiovascular Diseases
The leading case of NCD ASDR in 2016 was heart disease following the trend identified in 2010. 4 Further stratification of the 2016 ASDR shows that ischemic heart diseases remain the greatest contributor to NCD mortality followed by cerebrovascular diseases (stroke) and hypertension, supporting the findings presented by Ojji et al. 2 Cerebrovascular diseases have been identified as an established strong contributor to NCD ASDR primarily stemming from hypertension and atherosclerosis. Owolabi et al. ranked cerebrovascular diseases as the second leading contributor to cardiovascular NCD mortality. 6 The figures reported by Owolabi et al. reflect a broader trend in African countries, a finding that concurs with those presented in this article. 6 In this study, when stroke data were reviewed as an independent pathology, it was identified as the third leading NCD mortality pathology after heart disease and cancer in the five selected Southern African countries. This study furthermore found a positive relationship between stroke and hypertension ASDR, concurring with the findings of Kengne and Mayosi. 7
Diabetes Mellitus
In this study, ASDRs attributed to diabetes mellitus have dropped in Botswana, Mozambique, and Namibia but not in South Africa and Zimbabwe. These findings partially support those of Hunter-Adams et al. who reported an increased prevalence of diabetes mellitus in Africa. 13 The incidence of diabetes mellitus is predicted to grow by 110% from the year 2013 to 2035 due to poor dietary choices. 13 A further concern is that many diabetic patients remain unidentified: vigilant monitoring and improved treatment are thus urgently needed. The new South African Sugar Sweetened Beverage Tax, which came into effect on the April 1, 2018, is estimated to reduce the incidence of obesity by 220,000 patients. 4 It is further postulated that this tax will help to reduce the incidence of diabetes mellitus due to the pathophysiological relationship between obesity and diabetes mellitus. In 2014, the Mexican government introduced a similar sugar sweetened beverage tax which resulted in a 12% drop in the sale of sugary drinks within the first year of its launch. 14 Many Mexicans altered their purchasing behavior, purchasing plain water instead of sugary beverages in an attempt to avoid the increased financial cost, which had the knock-on effect of improving their diet in so far as the consumption of sugary beverages was reduced. 14
Cancer
As concerns cancer, ASDRs have diminished by 4.6% from 2010 to 2016, a finding that concurs with those presented by Somdyala et al. who attributed the significant reduction in cancer mortality to urbanization, changes in socioeconomic status, and diet. 15 Many Africans have relocated from rural areas to towns and cities in search of employment, thereby increasing urbanization and improving their socioeconomic status. They now have the financial independence to secure better health care enabling early detection, prevention, and management of cancer-related diseases. Furthermore, urbanization has led to a change in diet, with a decrease in the consumption of home grown maize and a consequent increase in the consumption of industrially and commercially sourced products, thereby decreasing esophageal cancer mortality. 15 Unfortunately, urbanization has also negatively impacted many African diets, resulting in obesity and an increased incidence of diabetes mellitus due to the prevalence of and popularity of poor nutritional choices such as fast food. 15
Chronic Respiratory Diseases
The ASDR of chronic respiratory diseases has dropped by 11.3% in the period from 2010 to 2016. This finding supports those of Nojilana et al. 4 This can be accounted for by the fact that a number of African countries (including South Africa) have introduced Tobacco Taxes, which, similarly to the Sugar Sweetened Beverage Tax, deter consumers from purchasing tobacco products. 4 The Tobacco Tax has had a positive influence, curbing the number of people who smoke, thereby decreasing the incidence of chronic respiratory diseases (asthma, COPD, and lung cancer) and mortality. 4 It is also postulated that the South African Laws, which legislature where and when an individual may smoke, may also have an effect on COPD. South African Laws that restrict people to smoke outside in confirmed area may increase the risk of secondhand smoke and COPD.
Conclusion
A critical statistical review of the insurgence of total NCD mortality in relation to ASDR in the selected Southern African countries indicates that these countries comply neither with the recommendation put forward by Strong et al. of a 2% reduction in NCD mortality per annum nor with the World Health Organization goal of a 25% reduction of NCD deaths based on 2010 baseline figures. 8 Although there has been a decrease in the ASDR of cancer and chronic respiratory diseases in the five countries and given the lower prevalence of diabetes mellitus in three of the five countries, the increase in cardiac and cerebrovascular diseases increases collective NCD mortality. The findings demonstrate that the medical strategy adopted by the health-care systems of the aforementioned countries requires urgent revision in order to combat increased NCD mortality rates. The authors recommend the introduction of exercise therapists (biokineticists) in Botswana, Mozambique, Namibia, South Africa, and Zimbabwe as part of a National Strategic Public Healthcare Plan. Exercise therapy has been clinically shown to improve the management of cardiovascular and chronic respiratory diseases and diabetes mellitus as well as improve the quality of life of cancer survivors. 3 Whereas traditional strategies used to combat NCDs have predominantly been those of early detection, education (in order to promote healthy lifestyle choices), improved dietary choices, and pharmaceutical management, renewed emphasis should be place on public exercise therapy, which may turn the tide of the NCD epidemic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.