
Abstract
Patient safety is influenced by a set of factors in various levels of the healthcare system. One of the factors affecting patient safety is safety competencies of the nursing students. The current study aimed to evaluate the effect of patient safety education on patient safety competencies of the nursing students. This quasi-experimental study was conducted with a pretest-posttest deign. The levels of patient safety competencies of 50 nursing students were investigated in a nursing school affiliated to large university of medical sciences in the south of Iran in 2019. Data were collected using Health Professional Education in Patient Safety Survey (H-PEPSS). The data were analyzed in SPSS 21 using descriptive statistics and repeated measures ANOVA. The three investigated intervals were significantly different in terms of the total H-PEPSS dimensions, while the lowest was attributed to the dimension “managing safety”. Mean scores of “how broader patient safety issues are addressed in health professional education” and “comfort speaking up about patient safety” significantly increased during the follow-up periods. The educational intervention was partially effective in improving patient safety competencies of the nursing students over long term.
Patient safety (PS) is an international issue since health professionals are ethically responsible to ensure PS within the healthcare system. 1 Patient safety is the absence of preventable harm to a patient during the process of health care. 2 PS can be achieved by reducing and mitigating unsafe measures, and using best practices that can lead to optimal patient outcomes. 3 Nurses can ensure PS through monitoring and supervision. Therefore, they should provide patient-centered care, work in interdisciplinary teams, use evidence-based practices, improve safety and quality, and meet needs of patients in the 21st century. 2 Nurses must be equipped with PS competencies either in their studentship or their working periods. 4 Despite the emphasis of international and national guidelines. 3 nursing education does not address PS deeply, and it is unable to bridge the gap between theory and practice without integrating PS into the nursing education. 5
In 2006, the Canadian Patient Safety Institute (CPSI) designed The Safety Competencies for health professionals. The Safety Competencies has six core domains: 1) contribute to a culture of patient safety, 2) work in teams for patient safety, 3) communicate effectively for patient safety, 4) manage safety risks; 5) optimize human and environmental factors, and 6) recognize, respond to, and disclose adverse events. 6 The fundamentals of PS and risk management skills should be trained to nurses to develop their PS competency. 3 Ginsburg et al. designed the Health Professional Education in Patient Safety Survey (H-PEPSS) for reflecting the six key domains of PS competency. 7 Educational innovations and PS competency evaluation have been recommended to enhance PS among nurses. 2 Although the importance of PS training has been acknowledged for over a decade, it is still underutilized and undervalued in most countries. 8
The PS curriculum focuses on clinical processes that are related directly and indirectly to the patient, and includes the structures, processes, tools, and activities used by hospital staff to identify, analyze, control, and manage risks during healthcare delivery. 9 Such a curriculum is suitable for both patients, and the health care team and organizations, and can minimize the risks to patients. 4 However, due to the wide range of patient safety aspects, it is not possible for all countries to include all the principles of PS competency in the curriculum of students. Students should be aware of the conditions, which predispose to medical errors, especially during their studentships, respect the patients’ safety principles, and receive the necessary training to obtain PS competencies. 10 Lee et al. emphasized on the need to revise the nursing curriculum and to use various teaching methods to deliver PS education more comprehensively and effectively. Furthermore, researchers reported a need to develop an integrated approach to ensure students’ PS competencies. 2 However, the process of enhancing PS competency and restructuring the nursing curriculum is very slow. 11 A number of studies examined trainees’ PS knowledge, skills, and attitudes, but most of them assessed either the impact of specific PS curriculum or training interventions.12,13 Tella et al. reported that only few studies investigated promotion of PS competencies among nursing students. 14 A systematic review found no surveys on the broad content reflected in PS competencies of healthcare professionals based on H-PEPSS. 15 In most of these studies, research instruments were designed and used to measure the impact of specific PS curriculum. However, such studies have not used H-PEPSS. In Iran, nursing schools have incorporated PS content into their curriculum, but to the best of our knowledge, little has been published so far about these efforts. Considering that assessment is central to all educational programs, curriculum designers should ensure that the registered nurses are safe and competent. To provide effective and safe care services, nursing graduates need to attain the vital competencies set by the CPSI. Furthermore, assessment of the students’ self-perceived competencies after an educational program can help adjust curricula to students’ needs. 16 Therefore, the current study aimed to investigate the effectiveness of PS education on PS competencies of the undergraduate nursing students in Iran.
Methods
Study Design and Setting
This quasi-experimental study was carried out among undergraduate nursing students with a pretest-posttest design, in which the students were followed up after one, three, and six months. The participants included 50 students selected from the nursing school of Kerman University of Medical Sciences in southeast of Iran. According to the academic law in Iran, the bachelor's degree includes four years of study and the curriculum is based on a semester system. Students have to pass theoretical and clinical units in university and educational hospitals, respectively. The students experience clinical learning opportunities, such as long-term care, family/community health, and critical care setting (e.g., medical-surgical, pediatrics, maternity, mental health).
The participants of this study were students who received no PS education.
According to the curriculum, a 4-hour mandatory workshop on PS is held at the beginning of the third semester in Razi School of Nursing and Midwifery. However, we conducted an eight-hour program with more comprehensive contents, and explained it in details in the data collection procedure and intervention section.
Sample
The target population of this study included all undergraduate nursing students in the third semester of the second year. Sixty-three participants were recruited from January to June 2019. Given the small size of target population, all students were selected as the study participants using census sampling method. Finally, 50 students completed the questionnaires (response rate = 79.36%).
Inclusion and Exclusion Criteria
Inclusion criteria were the nursing students who had not passed any PS training courses, those who passed the credit of “Fundamentals of Nursing”, those who started learning in the clinical setting, and those who were not employed. The exclusion criteria included failing to complete the questionnaires and being absent in one or more sessions.
Instrument
Data were collected using two questionnaires: a demographic questionnaire containing the participants' age and gender, observation of medical and nursing errors in clinical practices, reporting errors to clinical educators, hospital staff, and peer students, as well as PS quality in the university education, and a modified version of the Health Professional Education in Patient Safety Survey (H-PEPSS) . The latter is a self-reporting tool on PS competency. H-PEPSS can be used by health professional educators, the students and new graduates as a self-evaluation tool.7,17
The H-PEPSS is composed of 38 items divided into three sections. The first section deals with “Learning about specific PS domains” (27 items). These items begin with the stem ‘I feel confident in what I learned about and are categorized under seven dimensions: Clinical safety issues such as safe medication practices, hand hygiene, etc. (four items). These items are included in the H-PEPSS to help respondents distinguish between clinical and socio-cultural aspects of PS. The six sociocultural domains of PS competencies such as “Working in teams” (six items). Effective communication (three items). Safety risks' management (three items). Human and environmental factors (three items). Recognition of and response to adverse events (four items). Culture of safety (four items).
In the first section, participants were asked to respond each item regarding contents learned in the classroom and during their clinical experience. According to the purpose of this study, we asked the participants to respond each item regarding contents learned in the classroom (workshop). All 27 items of the first section were scored on the scale value of one (strongly disagree) to five (strongly agree), and the option of “no idea”. The mean and standard deviation of items in all seven domains was calculated on a Five-point Likert scale.
The second section of the H-PEPSS containing seven items considered “How broader PS issues are addressed in health professional education”.
The third section of the H-PEPSS included “Comfort speaking up about PS” and had four items. The second and third sections were scored on the scale value of one (strongly disagree) to five (strongly agree).
The H-PEPSS was developed to assess the levels of clinical safety and six core domains of CPSI Competency framework in newly graduated students. Three PS experts involved with the training of health professionals in medicine and nursing were asked to give feedback on the draft questionnaire. Its construct validity was confirmed through factor analysis (CFA). The internal consistency was calculated using Cronbach’s alpha coefficient; Cronbach’s alpha was between .81 and .85 indicating a good reliability.7,17
In this study, the H-PEPSS was used with the developers’ permission. The cross-cultural adaptation and translation of the questionnaire involved forward accurate translation of the original H-PEPSS into Persian. Later, a proficient English translator conducted the backward translation of the Persian version into English. Next, the translated version was matched with the original version. Face validity of the instrument was also examined and confirmed by students’ perception and understanding of the items. For a pilot study on the Persian version of the H-PEPSS to be conducted, 30 students not involved in the study process were asked to complete the questionnaire.
Furthermore, 10 nursing faculty members confirmed the content validity of Persian version of the H-PEPSS, and the Content Validity Index (CVI) was 90% for the entire instrument and more than 86% for all the items. Furthermore, the reliability of the questionnaire was calculated through internal consistency method, in which Cronbach’s alpha coefficient ranged from 0.73 (clinical safety) to 0.86 (effective communication and safety risks management) the whole instrument was 0.89.
Data Collection Procedure and Intervention
The participants were followed up from the second year of study (January 2019) to the next six months (June 2019). The co-researchers collected data from defined groups of students in the classroom. The participants were asked to complete the questionnaires that took = 15–20 min. The participants completed the questionnaire one week before the educational intervention (pretest), one month (posttest), three months (follow-up), and finally six months after the educational intervention (follow-up). Changes in the PS competencies were compared at pretest posttest, three-month follow-up, and six-month follow-up using the H-PEPSS.
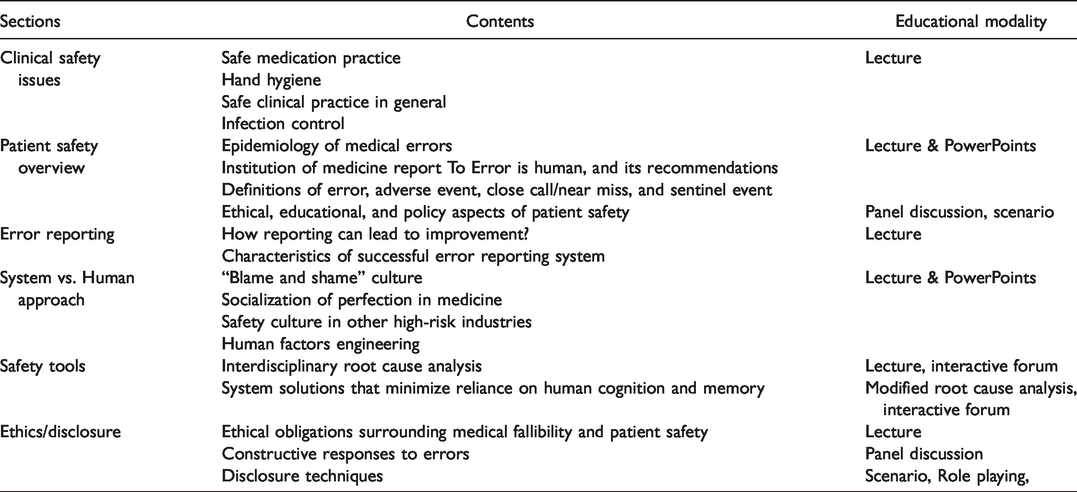
At the beginning of the third semester, a safety-training workshop was performed for 4 hours. The intervention group was divided into two groups to increase the opportunity for participation in the workshop, and an eight-hour workshop was held in two days. Contents of these training sessions and several educational videos and PowerPoints were then uploaded on the Nursing School website, so that students can continue their education virtually. The authors and a PS expert conducted the training program. The educational content of the sessions and modality are presented in Table 1. 18
Patient Safety Curriculum Content and Educational Modality.
Statistical Analysis
The data were analyzed in SPSS 20 using descriptive statistics (frequency, percentage, mean and standard deviation) and inferential statistics (repeated measures ANOVA). The Kolmogorov Smirnov test showed that the data followed a normal distribution. The significance level was set at ≤0.05.
Results
Demographic Information
Thirteen eligible nursing students did not complete the questionnaires in the three follow-ups. Our results showed that the mean age of participants was 20 years; 50% were women. About 96% of the participants reported medical errors, 80% reported errors to their clinical instructors, 42% reported them to hospital staff, and 84% reported them to peer students. Furthermore, 50% of the participants believed that the nursing curriculum covered PS issues.
Patient Safety Competency
As Table 2 represents, PS competency, and its domains were evaluated at four time points. Results showed that the participants' PS competency and its domains significantly increased after the training program (p < 0.001). With regard to the first part of the questionnaire, the highest mean score difference was related to “working in teams”, while the lowest one was attributed to “managing safety”.
Comparison of the Mean Scores of PS Competency and Its Dimensions at Pretest, Posttest, and Follow-Ups.
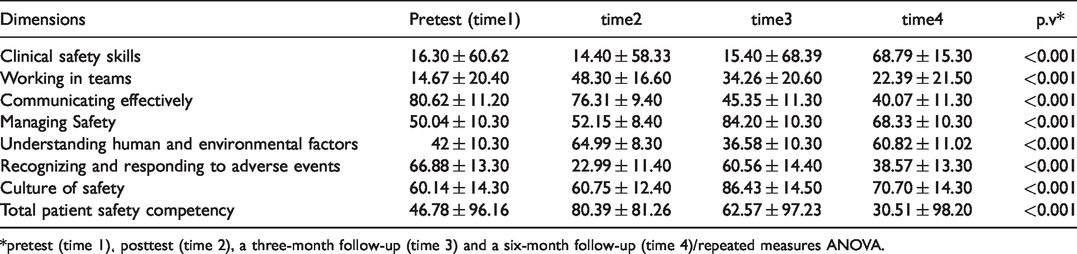
*pretest (time 1)، posttest (time 2), a three-month follow-up (time 3) and a six-month follow-up (time 4)/repeated measures ANOVA.
In the second and third parts of the questionnaire, “how broader PS issues are addressed in health professional education”, and “comfort speaking up about PS” were examined at different time intervals. The results showed a significant increase in the participants' knowledge of these domains (p < 0.001) (Table 3).
Comparison of the Mean Scores of PS Education and Comfort in Speaking About PS at Pretest, Posttest, and Follow-Ups.

*pretest (time 1), posttest (time 2), a three month- follow-up (time 3), and a six month- follow-up (time 4)/repeated measurement ANOVA.
Discussion
The current study examined the long-term effects of an educational intervention on the improvement of PS competencies in nursing students. The educational intervention had a significant effect on the overall PS competencies of nursing students, which was similar to other studies.5,13,19 The overall PS competencies scores of the students increased after the education compared to the baseline. In other words, significant positive changes were reported in PS competencies scores over time after the intervention. However, such an improvement may be resulted from education, maturity, and experience in working conditions. 20
Tom showed that staff’s perceptions of safety after PS training were significantly different from those before the intervention. In addition, the fall of patients has decreased by 54%. They believe that the training of PS competencies is necessary to clarify the roles, tasks, functions and responsibilities of staff. It is also an economical and cost-effective way to prevent the complications caused by non-compliance with PS. 21 Ignoring PS competencies of the students seems to weaken the quality of care and does not solve patients’ health-threatening problems. The results will be the waste of economic capitals, decreased level of health and social achievements in the long term. 22 Nie et al. in China studied the PS training to undergraduate medical students and found that PS competencies were one of the important issues that should be included in the student curriculum. 23 In addition, another study in the UK found no effective education on PS in universities, and healthcare professionals trained nursing graduates some safe care behaviors in the clinical settings. 24 The PS training is effective because PS competency is a set of integrated capabilities in relation to knowledge, attitude and skill that is a prerequisite for better performance and problem solving in clinical settings.
With regard to “learning about specific PS domains”, the results showed that the highest mean score was related to the dimension “working in teams”; whereas, the lowest mean score was attributed to the dimension “managing safety”. Ginsburg et al. assessed safety competency of the nursing and pharmacy students. Their results showed that “working in teams” gained the highest score after the dimension “effective communication with other members of the healthcare team”. 16 This result may be due to the mediating role of nurses in health care system; nurses learn and experience teamwork skills from the outset. Gaupp et al. added that the students' participation increased after PS education. Therefore, they hypothesized that this training activated students' systemic thinking and enhanced their engagement and teamwork. 5
In the present study, the lowest mean score difference was related to “managing safety” because our participants included first-year nursing students with no clinical experiences and could not manage safety competencies effectively.16,18 As a result, students need to acquire theoretical and practical safety management skills to manage other positions. 19 VanDenKerkh of et al. demonstrated that the score of “managing safety” was higher among the clinically educated nurses than the theoretically-educated nurses. 6 It should be noted that this study compared the newly graduated nurses in clinical settings and those who were studying nursing in theory; students will experience safety management skills until they finish their education.
Results of the second and third parts of the questionnaire (how broader PS issues are addressed in health professional education, and comfort speaking up about PS) showed a significant increase in the participants' scores in different time intervals. Lee et al. also indicated that PS education had a positive impact on nursing students' attitudes toward PS 2 because students involve in the clinical setting over time and their experience of PS increases gradually. 20 Furthermore, students' attitudes towards PS changed after the educational interventions, so that they considered it an important issue for patients.5,21 Ginsburg et al. also showed that students’ attitudes toward safety education were significant in the clinical setting. 16 Moreover, safety education becomes institutionalized in students in the clinical settings. 25 Therefore, PS education should be involved in the students' curriculum, and nursing school administrators and faculty members are recommended to continue safety training to enhance the students' PS competencies.
Limitations
The present study has some limitations. The number of participants recruited in this study was limited; so, we could not have any control groups to compare the results between the intervention and control groups. Therefore, the pretest-posttest design was used for the participants selected using the convenience sampling method. Furthermore, we did not have access to patients, and the results were specific to the study population. The results would have been more comprehensive in the case that patients who received care from the studied nurses had completed the questionnaire before and after the intervention. Therefore, the results should be generalized with caution.
Conclusions
The current study aimed to evaluate the effectiveness of PS education on nursing students' PS competencies. The results showed a positive and significant effect of safety education on all dimensions of students' PS competencies. Therefore, it seems necessary to consider PS training courses in nursing schools after applying appropriate needs assessment. Managing safety should be emphasized in the academic education of PS formally and informally, so that students can master safety management skills in the clinical settings.
Footnotes
Acknowledgements
The authors would thank all nursing students participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Ethics Committee of Kerman University of Medical Sciences with the code of ethics of IR.KMU.REC.1398. 053. In an open meeting, the first author invited the students to participate in the study and informed them about the study goals and methods. The researcher emphasized that participation was voluntary and students could withdraw at any time. The participants were reassured that their responses would be confidential and their identities would not be disclosed. Later, the participants were asked to sign written informed consent forms. Data were maintained anonymous using unidentifiable student numbers.