
Abstract
Excluding communities in planning and implementing research maximizes internal risks that are otherwise visible and avoidable when there is adequate community consultation. Communities might not meaningfully use research results if majority of the researched people have minimal or no participation in information generation and dissemination. However, effective participation of researched communities in research is key to transferring knowledge to action. Using a qualitative approach, the study identified barriers to, and relevant strategies for improving health research uptake, particularly for schistosomiasis (commonly known as bilharzia) in the Ingwavuma area, uMkhanyakude District of KwaZulu-Natal. Data was collected through modified ethnography using participant observation, focus group discussions, unstructured in-depth interviews, and ethnographic conversational interviews. Results reveal that research uptake is inhibited by reduced opportunities for habitual interaction between residents, a paucity of innovative and inclusive health education activities and unsafe recreational facilities. The community’s strategies on strengthening social capital for disease control include using existing social systems and power hierarchies to mobilise and organise and using the performing arts to facilitate habitual interaction and knowledge sharing. The study recommends a community consultation flow which facilitates openness about the benefits and the community’s role in research, a pre-condition for community wide efforts in local disease prevention and control.
Keywords
Globally there is consensus that citizen participation in health research can lead to improved health outcomes.1–4 However, research uptake processes are complex and fraught with fraught with challenges, including citizen apathy. Consequently, there are increased efforts encouraging people to use research findings. 5 Brownson et al. 6 suggest that dissemination and implementation science should be cross disciplinary, drawing on multiple fields. Research uptake ought to be approached with community experimentation, 7 empathy and systems thinking. 8 Mindu 9 in turn argue that the most effective methods for research uptake leverage community participation, interpersonal communication and respect for cultural context and indigenous knowledge systems. Clearly, determining the best approach for research uptake remains a critical question. It appears the process of translating research into meaningful actions that positively impact people’s lives involves actions that go beyond those traditionally associated with knowledge creation. 10
This paper reports on a case study investigating the prospects and challenges of implementing health research uptake predicated on social relationships and accessible communication. The objective of this study was two pronged. Firstly, the study identified the contextual barriers to health research uptake, particularly for schistosomiasis (commonly known as bilharzia) in Ingwavuma community. Relatedly, the second focus was to outline research uptake strategies based on the links between social relationships and medium of communication in the same community. To achieve this, the study engaged selected community members in a consultative process on planning and implementing strategies with an understanding that effective community participation in health research processes in which communities are subjects is key to understanding of study findings and subsequent translation of knowledge to action. Ultimately, the key ethos of the study was to amplify the voices the researched community and increase its participation in research uptake, hence the consultative process.
Excluding communities in planning and conducting research maximizes the risks of hitting blind spots presented by internal risks that are otherwise visible and avoidable when there is adequate community consultation. 11 In addition, communities might not use the research results meaningfully if majority of the researched people have minimal or no participation in information generation and dissemination (p. 24). 12 However, addressing community interests and representation can strengthen individual and communal consent and acceptance of research. 13 Community participation and by extension community engagement is highly relevant in our setting, a busy multidisciplinary Ecohealth research project, set in a poor community in rural KwaZulu-Natal.
In South Africa community participation has now become an established orthodoxy in research as it “promotes community empowerment, health promotion and disease prevention, access to services and community accountability”. 14 There is a realisation that relegating local people, their lived and existential realities, poses challenges to public health. For public health researchers to effectively understand and tackle disease there is need to conduct studies with affected people.12,15 It is also important to ensure that research findings are accessible, and they systematically influence cultural and individual change. 16 As a result, the value of community participation and interest in place-based approaches has gained currency in South Africa as it helps to inform understanding of the local context.17,18 The South African government considers effective coverage of community engagement and participation as guiding and strategic pillars of policy on the elimination and control of neglected tropical diseases. 19
One of the ways to promote successful community participation in the research process and use of research findings particularly in research naïve communities is through community engagement. 20 Community engagement is defined by the Centres for Disease Control and Prevention (CDC) as, “The process of working collaboratively with and through groups of people affiliated by geographic proximity, special interest, or similar situations to address issues affecting the well-being of those people”. 21 Researchers, communities, regulatory agencies and funders have also advocated for the involvement of the community in research with the aim to reinforce subjects’ protection and improving research efficiency. 22 Although a model for community engagement and its key ethical principles are clearly pronounced by Musesengwa et al., 23 the urge for multidisciplinary research is to contextualise and apply these principles.
The success of community engagement in achieving transformation in communities is often dependent on collaborative partnerships as opposed to transactional partnerships.24,25 Musesengwa et al. 23 further argue that “Community engagement in health research ensures research is consistent with the socio-cultural, political and economic contexts where the research is conducted”. Suffice to say, community participation in the research processes facilitates diverse narrations of ideas and experiences important in nurturing the culture of research uptake
This study communicates results from a community consultation process detailing the community’s views on social and power dynamics of place, cultural and social capital that can be harnessed to facilitate accessible communication and use of research findings. Community participation in the Community Driven Change (CDC) project is stratified as follows: (1) consulting the community to outline what should be done; (2) planning on how the suggested activities should be done; (3) implementing the intervention activities together with the community; (4) assessing the process and efficacy of the intervention. 26 This article reports on the first two domains relating to consultation and strategic planning which are important in mobilising and organising community led social change. 27
Study Setting
The study was carried out in the Ingwavuma area in uMkhanyakude district of the KwaZulu-Natal province of South Africa where schistosomiasis is endemic.4,28 The Ingwavuma community is a predominantly Zulu speaking rural community, mostly governed by traditional authority in northern KwaZulu-Natal. 29 KwaZulu-Natal province has the third poorest human population in South Africa, 30 while uMkhanyakude is the 3rd poorest district in the province 31 and has relatively higher prevalence of neglected tropical diseases.” 19 Members of the uMkhanyakude district have limited access to basic services and the unemployment rate stands at 72%.1,31 The Ingwavuma area is underdeveloped, with people living on less than an estimated 1USD per day. 29
Research Approach
This study adopted a qualitative approach to pursue an engagement process that consulted selected members of the community on how to i) improve community wide participation, ii) build relationships and strengthen social capital useful for local disease control. The qualitative research approach was chosen for its ability to provide complex contextual descriptions of how people experience a given research issue. The study sought contextual meaning, not a generalisation, hence settling for a qualitative approach based on everyday activities and conversations. The vivid description of experience has potential to inspire community action as posited by Poovey 32 who argues that “there are limits to what the rationalizing knowledge epitomized by statistics can do. No matter how precise, quantification cannot inspire action, especially in a society whose bonds are forged by sympathy, not mere calculation”. The import of Poovey’s sentiments is that the choice of research is determined by what the study seeks to find out and why.
Study Design
The study was designed as an exploratory case study due to the uncertainty associated with assigning social practice placemaking to research uptake. 33 The design was necessary in order to identify challenges, opportunities and salient variables relevant to the area of research. However, the study is part of a larger project which adopts a participatory action research methodology. Therefore, it embraces an emancipatory paradigm in a bid to transform the Ingwavuma community through group efforts. 34
Selection of Participants
Study participants were selected using purposive sampling. We engaged 54 participants based on their diverse and in-depth knowledge of the Ingwavuma community, behaviour change communication and public health research. At this preliminary stage we targeted people through schools, community research assistants and local leaders. The participants were a diverse group of people who included lay citizens, Community Research Assistants (CRA) and the Community Advisory Board members who included the local area leader (Induna) who all have “…tacit knowledge of the rules, conventions and stocks of knowledge that they use and draw on in everyday life”. 35 We also included participants, mostly women who did not necessarily occupy any position of authority with an understanding that their experiences and knowledge is legitimate and should be captured in research. Kotzé et al. 36 posit that inclusion of marginalised voices has potential to raise creative alternative discourse which can transform dominance and power differentials and undesirable practices peddled as culture.
Data Collection
Data was collected through modified ethnography due to logistical challenges. The modified ethnography entailed living and interacting with the participants for two weeks in every month for 6 months. In order to establish and set up conditions necessary for collaborative community engagement at entry level stage, data was also gathered using ethnographic conversational interviews. Additionally, we used participant observation, focus group discussions, unstructured in-depth interviews.
Observational data was collected mostly during community scoping. 37 The process entailed observing both the physical and social infrastructure of the community for the purposes of familiarising with the environment and to be ‘seen’ by the people. The observations were either diarised or captured using a digital camera.
For the focus group discussions, data was elicited data from 37 participants gathered in 5 groups. Of these 5 groups, 3 had 7 participants each while the remaining two had 8 and 9 participants each. The engagement process sought the community’s views on the ways to build relationships and strengthen social capital useful for local disease control. In addition, the engagements were also meant to involve the community in identifying and developing a relatable media for communicating research results.
Semi-structured interviews were used to collect data from key informants who included 1 representative of the pre-school boards, 1 traditional leader, 3 CRAs and 2 school principals. The interviewed participants were purposively kept at a small number in order to maintain the dignity and care for respondents through devoting more time to their responses. 38 Interviewees responded to questions which generally sought to determine barriers to social connectedness, what makes people work together in their community and lastly why those strategies mattered.
All the interviews and focus group discussions that were conducted with school principals, teachers, learners and parents were conducted on school premises to provide participants a sense of security and be in relaxed familiar environs. The interviews were held at times that did not disrupt school activities and with express authority of the school principals. The conversational interviews with Community Research Assistants and the Induna were conducted onboard the TibaSA field trip car as well as at lunch breaks. The idea was to maintain the conversations as collegial and natural as possible. We conducted the interviews in the local language, isiZulu. The decision to use the local language was in order to allow participants the full freedom to express themselves freely and comfortably.
Data Analysis
Data was analysed using inductive analysis and creative synthesis where patterns, themes, relationships and attitudes were searched through the spoken and non-verbal language material. This inductive analysis process follows 39 that “good research is not generated by rigorous data alone … (but by) ‘going beyond’ the data to develop idea” through detecting the typical within the general and the general within the particular. We identified themes and arranged them in thematic frames for presentation, interpretation and analysis. We also used still photographs to present findings.
Limitations
This case study results may not be generalised to apply to the whole of KwaZulu-Natal, but they can be transferrable to communities in similar contexts seeking to strengthen social capital for community disease control.
Validity and Reliability/Trustworthiness (Qualitative Research)
The validity of this study was ensured through juxtaposing findings from interviews, video recordings and observations and interpretations as participant observers. Additionally, the results were solidified by using purposive sampling to select respondents who had good knowledge of Ingwavuma community and were also in a strong position to champion research uptake. Validity was ensured through comparing and contrasting theoretical perspectives on the subject against the study’s field experiences. 40
Ethical Considerations
Ethical approval was obtained in the context of the bigger project from the University of KwaZulu-Natal. Participation in the study was voluntary and participants were told beforehand that they participated on their will and they can withdraw from the research at any stage. Participants were assured of anonymity and that their responses would not be traced back to them. The study maintained the confidentiality of all participants by not referring to any one of them by their names or any identifier. All the photos used were captured with a blurred lens or from a distance in order to make it difficult to identify individuals.
Results
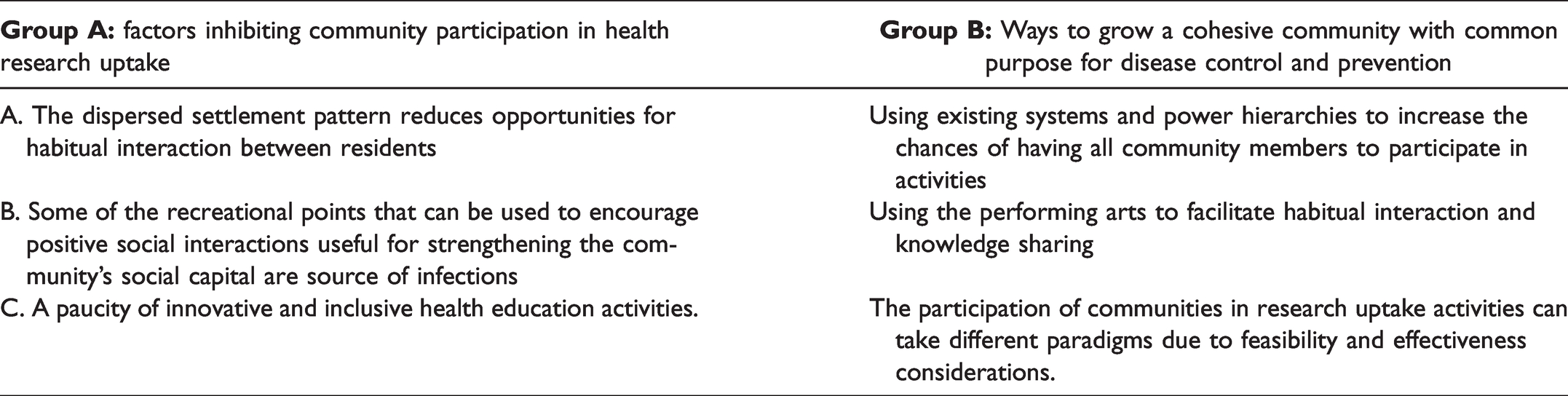
Data analysis classified the data into two broad categories;1) factors inhibiting community participation in research uptake and 2) ways that can be used to promote community efforts in working together in disease prevention and control. Table 1 presents the challenges and opportunities for two groups.
Challenges and Opportunities for Improving Health Research Uptake in Ingwavuma Area.
Factors Inhibiting Community Participation in Research Uptake
Settlement Pattern Reducing Habitual Interaction
We noticed, during community scoping, that homesteads in Ingwavuma had a dispersed settlement pattern which potentially limited neighbour interactions. The interviewees confirmed our observations. This sentiment was echoed by teachers we engaged, most of whom predictively said the dispersed settlement pattern was a possible threat to collective community actions. One of the Indunas who is also a member of the CAB said that conversations between neighbours were limited due to the distance between the family compounds. The Induna had the following to say;
…as you can see, some of the homesteads are built a distance from each other. It is possible for neighbours not to see each other or speak on a daily basis.
This community has large compounds. Meetings between neighbours are therefore reduced. However, for those with pre-school going children they meet every weekday when they drop their children at school.
However, this does not imply people in the study area lead isolated lives. When asked about the presence of activities and resources that could be used to facilitate interaction between residents, some of the participants informed us that people meet in their everyday lives, however community activities are coordinated by the local leadership. These participants also informed us that dams (water source) are definite sites for chance meetings.
Transmission Hotspots Are Recreational Facilities
The consultation exercise revealed that the community’s efforts to achieve a common agenda on schistosomiasis prevention and control can fail if solutions are not mindful of the community’s lived realities. Research participants pointed out that efforts aimed at community led schistosomiasis control might be scampered by the non-availability of recreational facilities that can substitute the role of natural water bodies as a source for water for domestic use and recreation for children. Community women who participated in a focus group discussion said that their roles as mothers demanded that they be in contact with water. One of the participants shared that: “We do not have access to piped water. We get water for all the domestic purposes from the dam”.

Community Members Doing Their Laundry at Local Pond (photo by First Author).
Part of the larger project involves community sensitisation and scooping in water bodies to look for snails that transmit schistosomiasis. As a result, we scooped near the schools where we did sensitisation. We found young children aged between 8 and 10 swimming at one of these ponds as shown on the photo below (Figure 2). The exposure of children to schistosomiasis infection was also raised by women during focus group discussion. One of the participants mentioned, with others nodding in agreement that:

Children Who Were Swimming Hid Behind Shrubs Upon Noticing Researchers (photo by first author).
It is a difficult task to watch over children’s play activities. Children go out to play on their own; that has always been the norm. When they go out, they swim just like we used to do when we were young.
The Induna also made a similar comment through the following rhetoric questions.
We are aware that the disease is transmitted in water. The whole community knows. But where we will get water if we avoid dams? Children swim in the river. I think our major worry is that they will drown. They learn to swim and create friendships at the river.
Poor Public Health Education
Our findings suggest that the community had limited spaces where they share knowledge and access to information on schistosomiasis. According to the teachers and parents they had very few opportunities where they can acquire knowledge on schistosomiasis from an expert. In the absence of conclusive results from an ongoing KAP study, we got the impression that the teachers and learners from the community had very low knowledge and understanding of schistosomiasis. Studies on the community’s knowledge, attitudes and practices showed that the community had low levels of knowledge on bilharzia snail cycle of leading them into risk behaviours.28,43 One of our team members who introduced our team and its purpose asked students in vernacular what they knew about schistosomiasis. The question was often met by either silence and visibly blank faces or sporadic responses that whispered, “we do not know”. In addition, the parents or guardians are likely research averse/naïve as suggested by the small numbers of parents who signed consent forms for parasitology. While methods used to come to a suggestion that the community lacks public health education are not robust and conclusive, the team’s prolonged presence in uMkhanyakude puts us in a position to know communities that have been directly reached in the recent past. The lack of spaces and opportunities to regularly access and share knowledge might be reason for poor knowledge as both the MABISA and TIBA projects engaged with the community.
Ways to Grow a Cohesive Community With Common Purpose for Disease Control and Prevention
We have presented above the community views on possible hindrances to community disease control and prevention The following section focuses first, on the participants suggested shared social space facility and secondly on the participants’ insights on how mobilisation and organisation should happen.
The results reveal that for effective mobilisation and organisation to subsist there is a need to invest in the following three interrelated processes; a.) making use of established social structures and power hierarchies; b.) facilitating habitual interaction through performing arts; c.) mobilisation, paradigms of participation and organisation.
Making Use of Established Social Structures and Power Hierarchies
Participants pointed out that the social systems and hierarchies in their community are important in mobilising a critical mass. Carapetis and Brown
45
also emphasise on the importance of community leadership in community diseases control, arguing that local leadership can influence communities to participate. In this study it was suggested that Indunas and school principals play a critical role in mobilising the community due to their cultural roles and social status respectively. A focus group discussant said the following.
My suggestion is that if you want to do anything with learners and their parents you should involve the principal and the teachers. Most parents respect the school head.
I am the chairperson of the pre-school boards of this area. I can communicate with my colleagues on your behalf to ensure that there is cooperation. You only need to tell me the full details of your project and you must attend the board meeting so that they can see you and ask questions.
I can assist you in calling a meeting for parents whose children are learners at my school. However, it is better you get the message through the Induna. He can summon everyone to attend the meeting and they will come. If we just call parents from my school, what happens to others whose children are still in ECD?
In addition, participants noted that the Induna should be notified and sanctions all communal public gathering events. The participants also said that for effective mobilisation to subsist there is need to carefully tread on the power relations between the community and university actors.
Facilitating Habitual Interaction Through Performing Arts
The engagements also sought the participating ideas on which activities to do to increase research uptake among school going children and how those activities can lead to organising context friendly and community led disease prevention and control.
The use of performing arts to attract people into habitual interaction was a popular opinion. The performing arts were preferred because they are an accessible medium for communicating health research results. While participants did not prescribe content of the performances, they emphasised that the production should be both problem posing and problem solving, effectively communicating the dangers posed by schistosomiasis infection as well as how the community can prevent infections and access treatment. Participants also pointed out that the community is particularly interested in the use of traditional African music and dance, drama, and games to communicate schistosomiasis research findings. Barber
49
argues African popular culture is relatable and communities can manipulate it to achieve desired ends, which in this instance is improving community research uptake. Contributions from the participants also suggested that content of the drama and music should suggest ways that the community can organise itself to work together on schistosomiasis prevention and control. Additionally, they suggested that cooperation can be triggered through introducing drama competitions where teachers, parents, and learners work together to create and present a performance themed on schistosomiasis relating to their context. One of the teachers suggested that: Introduce drama competitions where teachers, parents, and learners work together to create and present a themed performance.
Learners can sing about the disease. Our community likes isicathamiya (traditional choral music)
Mobilisation, Paradigms of Participation and Organisation
It was suggested that community leaders such as Indunas and school principals should participate and make decisions on behalf of all residents. For instance, planning activities that lead to the community interacting in shared social spaces. Participants argued that the structure of the society and the subsisting power relations suggest that it is impractical to consult every community member prior to making decisions that affect community participation in research uptake. For instance, principals made decisions on behalf of the community in cases where the proposed activities to strengthen social capital involved use of school premises and interruption on class activities. On the other hand, it was also argued that ensuring that parents, teachers and children work together in making decisions has the potential to increase ownership and belonging to the projects. The argument was that participating in decision making and planning processes conscientizes every individual on the importance of sole contribution in the broader context community efforts.
Teachers and parents also suggested that the performing arts intervention should be inclusive. It was recommended that for community disease control to become a reality all community members should participate in activities, whether they had school going children or not. For instance, participants recommended that parents, teachers and learners should be targeted at once in order to unify the efforts to control and prevent new infections among school going children. We interviewed two school principals who told us that the success of related previous programmes rested on the consent and involvement of parents and guardians. A principal at one of the targeted schools said the following
The primary school children in uMkhanyakude spend only half of their day in school. As a result, teachers and parents or guardians share the duty to watch over their health behaviours, playing patterns and activities.
It is not always that you must call every parent to school. We have the school governing body that we can work with if it is not possible or important to have everyone.
Discussion
The currency of participation is widely recognised, however participatory approaches are either seldomly practiced or inaccurately followed Marston et al. 53 For community participation in research processes to proceed there is need to consult about the participation process itself demonstrated by this study which afforded the community a platform to outline what should be done and planning on how the suggested activities should be carried out. Barriers to participation are inherent in communities and best known by local people. Research uptake interventions can fail due to poor or no consultation; and poor design and implementation which not owned by the researched communities. Results from this and other studies have shown that communities might seem as if they are rebelling against biomedical evidence suggested if contextual considerations are not fully considered. 44
As such, effective models of participation should prioritise the community and their context. For example, this study revealed that to build awareness and collective action on local schistosomiasis control, attention should be paid on how power is structured in the community to determine who participates and why, the types of media that can be used for accessible communication, whether meetings are held at convenient times and venues. Our findings demonstrate the importance of teachers and school principals to take a leading role in mobilising and organising community efforts in controlling schistosomiasis as they spend more time with children and are respected by parents. Conversely, Indunas play an integral role as traditional leaders in getting the community engaged on schistosomiasis control. It is therefore important to involve community leaders in mobilising and organising the community as they have authority to give instructions or to call for meetings.
The consultation process revealed that improving community participation in schistosomiasis research uptake should be done following either through representative or transformative participation. In this study representative participation is essentially a form of power held and organised by an intersection of leaders with community members. Representative participation is more effective when there is a broader inclusion of different stakeholders and interest groups. 54 School principals and teachers, in their dual roles as leaders and residents had the authority to represent learners and parents providing suggestions on where and how to effectively improve research uptake among students and by extension the community. “Power is always at play in social relations and thus must be thoughtfully utilized to promote social justice, including in participatory initiatives.” 55 The community leaders, teachers, representative of parents and children participated in initial stages through representative participation.
However, since everyone can be infected by schistosomiasis and they can potentially transmit, transformative participation becomes crucial. The suggestion that parents, teachers and learners should work together on a creative project which speaks to both strengthening the community social capital and raising awareness on schistosomiasis prevention, treatment and control is indicative of transformational participation.
The use of arts-based methodologies and languages that the community prefers and is familiar with improves the quality of health education, provided that entertainment is not the only primary goal, but correct information is also communicated. Entertainment can be used to package age and culturally appropriate messages that effectively communicate with children and parents on schistosomiasis infection, treatment, prevention and control. The problem posing performances that community preferred are important in that they help in bringing out the health challenges the community faces as a result of schistosomiasis, as well as the knowledge gaps, attitudes and practices regarding schistosomiasis disease control and prevention. Subsequently, these performances are followed by edutainment activities based on solution focused approach proposing and educating the community on how to prevent and control the disease.
Research processes and study results should be spoken in languages/activities accessible to the common people. 56 For instance, the community’s preference for indigenous arts-based methods of communication suggest a need to for context specific and culture specific means to influence social behavioural change for schistosomiasis control and prevention across the social strata. The study focused on understanding community preferences related to school going children because they engage in activities such as playing and bathing in water bodies that predispose them to the risk of contracting schistosomiasis. 28
The use of performing arts is however not only an effective way of communicating; it can be used as a ‘meeting place’, an experiential platform that can be used to overcome apathy and poor participation in research processes. The performing arts are central in rural communities; they provide a platform for dialogic interaction and stimulating collective action. Our findings show that performing arts can encourage community members to work together in the making and consumption of arts products that can enhance efforts to prevent and control schistosomiasis. Nicholson 57 notes that knowledge in performance is embodied, culturally located and socially distributed. This means that knowledge is produced through interaction with others, and that reciprocity between participants creates new forms of social and cultural capital. 57 In the context of this study the pull power of arts can increase opportunities for the community to dialogue and work together towards schistosomiasis control and prevention thereby potentially solving the problem created by dispersed settlements discussed earlier.
Findings show that some of the barriers to community led schistosomiasis control and prevention are linked to coming up with interventions that are not mindful of context. Therefore, consultative engagements are important to get leaders goodwill and community participation. Person et al. 45 also suggest that by encouraging local people to actively participate in the process of designing interventions, it is possible to draw upon socio-cultural norms and to develop locally tailored behaviour change messages, activities and structural interventions. Consultation provides an opportunity to know and understand the limitations as well as to find ways to counter the anticipated challenges. In this study consultation established the community preferences and priorities in designing mediums for improving research uptake among primary school. It is fair to assume that consulting the community on their participation has the potential to increase traction and buy-in from the community if the participants or beneficiaries personalise the benefits of bringing social change through research uptake activities.
The consultation process gave the community an opportunity to outline how proposed activities will be carried out in a manner that gives the community agency to contribute to the change process. Research engages with participants in ways that are related to the socio-cultural and political culture, feasibility and transformative potential. Hickey and Mohan 58 posit that efforts towards increasing participation of communities in projects should be mindful of underlying tensions and synergies supporting greater participation. As such, the community’s suggestion that existing power and decision-making structures should be used prevents a situation where the researchers fall into the trap of usurping power from primary stakeholders and in the process destabilising the community. Marston et al. 53 caution that there is need to consider issues of power and control in order to understand systems better and to ensure that participatory interventions do not reverse gains, unintentionally.
Implications and Weaknesses
The participants responses show that for positive social interactions to subsist in rural communities, there should be infrastructure that allows interaction and activities for people to do in those spaces. The consultation process also showed that social offerings, openness and aesthetics can contribute to motivating people to work together for community disease prevention and control. The study also highlights the importance of person and environment fit in communicating research findings or improving research uptake and vice versa. However, while the study has important implications on the use of social practice creative placemaking to improve research uptake, the consultation was done with a very small sample, therefore the findings are not transferrable to the rest of the KwaZulu-Natal province. Notwithstanding this, the non-transferability of findings emphasises the importance of context specificity in effective community engagement.
Conclusion
In summary, efforts to increase individual and group participation in research uptake should start with consulting communities on how the process should flow and why. Consultation facilitates openness about the benefits and the community’s role in research which is a condition precedent to community wide efforts in local disease prevention and control. The rebalancing of powers between researchers and communities should not be misconstrued as a leeway to temper with societal power relations especially in rural communities where tribal hierarchies are observed. Instead existing power structures and social and physical infrastructure should be harnessed to mobilise and organise communities into collective action.
Footnotes
Acknowledgments
We would like to acknowledge, Ms Thulisa for her support in collecting data for this study. Special thanks also go to the study participants, school principals, community leaders and mothers and the pupils at the schools where we collected data. We would like to acknowledge the support we received from; The National Research Foundation Community Engagement grant The College of Health Sciences, University of Kwazulu-Natal The National Institute for Health Research (NIHR) Global Health Research programme (16/136/33) using UK aid from the UK Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Research Foundation (NRF) This research was also funded by the National Institute for Health Research, using Official Development Assistance (ODA) funding 16/136/33. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health or the National Research Foundation (NRF). The funders had no role in the conception, study design, data collection and analysis, decision to publish or preparation of the manuscript.