
Abstract
Background
Supporting a child’s healthy development is determined, in part, by a parent’s ability to seek, access, interpret and effectively utilize health information. This aspect of parenting draws on a set of skills referred to as health literacy.
Objective
To assess the level of health literacy among parents/carers in a regional South Australian community.
Methods
Parents/carers of primary school-aged children, residing in Whyalla, South Australia, were invited to complete the 13-item All Aspects of Health Literacy Survey.
Results
155 parents/carers completed the survey (79% mothers). Most participants were English-speaking (97%), employed (62%) and had 2–3 children (62%), with 52% completing tertiary education. Median total health literacy scores were mostly in the moderate-high range (median 27, IQR 26,27), as were critical health literacy scores (median 7, IQR 6,8). Higher scores were reported for functional health literacy (median 8, IQR 7,9), communicative health literacy (median 9, IQR 8,9) and empowerment health literacy (median 4, IQR 3,5).
Conclusions
Our findings reveal modest levels of health literacy among a sample of parents/carers of primary school-aged children in a regional South Australian community. Further work is needed to understand the differential effect of parental health literacy on child health outcomes, and the types of strategies that may mitigate the impact of these barriers on a child’s healthy development.
Health literacy – a multidimensional construct covering a number of domains of behaviour and competence - is increasingly being recognized as a social determinant of health. This is because health literacy impacts how people “access, understand, appraise and use information and services to make decisions about health.” 1 There is also a strong association between health literacy and other health determinants, such as income, employment, education and social status.2,3
The relationship between health literacy and health outcomes has been the focus of many studies to date. A review of 98 cross-sectional and cohort studies found a consistent association between low health literacy and poorer health outcomes (including higher mortality rates), poorer health status, increased utilization of emergency services and more hospitalizations. 4 This review, in addition to other studies, have also revealed a link between low health literacy and adverse health behaviors, including smoking, physical inactivity, lower diet quality, reduced health screening and difficulty managing medications.4–7 Accordingly, low health literacy may have negative health implications for individuals, as well as those dependent on these individuals, such as children.
Parental behaviors are an important determinant of a child’s health, wellbeing and development, with parent actions shown to predict child behaviors, such as physical activity, diet quality and screen time. 8 Given that health literacy impacts health behavior,4–7 it would be reasonable to assume that low health literacy in a parent would contribute to adverse health behaviors/outcomes in a child. Indeed, a number of studies have demonstrated a significant association between low health literacy in parents and undesirable health behaviors/outcomes in their children, including poorer asthma control,9,10 worse oral health11,12 and shorter sleep duration.13,14 Parents with lower levels of health literacy also report difficulties with communication in pediatric consultations. 15
Various factors have been shown to be associated with lower health literacy, including increasing age, male gender, lower levels of education, lesser income and ethnicity minority status.16–18 However, it is not entirely clear if these factors apply to parents due to the paucity of studies examining the determinants of health literacy in this population. Also poorly understood is the influence of geographical location on health literacy, with studies to date reporting conflicting findings with regards to the health literacy of regional versus urban populations.19–21 In light of these knowledge gaps and uncertainties, we set out to examine the level of health literacy among parents/carers of primary school-aged children living in a regional city in South Australia.
Methods
Study Design
Cross-sectional survey.
Objectives
The objectives of this study were to: (a) determine the level of health literacy (including total, functional, communicative, critical and empowerment health literacy) among parents of primary school-aged children living in Whyalla, South Australia, and (b) identify the sociodemographic factors associated with parent health literacy.
Participants
Parents/carers of primary school-aged children (i.e. aged 5–15 years), residing in Whyalla, South Australia, were eligible to participate. Whyalla is the largest industrial city in regional South Australia, housing a population of 21,828 people. 22 The city has a high level of socioeconomic disadvantage, with a high unemployment rate, large Aboriginal population and low proportion of people with university degrees relative to the state average. 22 Based on a target population of 5,410 parents, 22 we needed to survey at least 147 parents/carers in order to achieve a margin of error of 8% and a confidence interval of 95% for any individual item in the questionnaire.
Questionnaire
The study questionnaire was a 32-item composite instrument comprising measures of health numeracy, health information seeking and health literacy. To maintain alignment with the study objectives, this section focuses only on the development and validation of the health literacy component of the questionnaire. Other components of the questionnaire will be described in more detail in future publications arising from this research.
The research team scoped the published literature for measures of health literacy. Measures were required to be brief, easy to understand and administer, pertinent to the study population and objectives, and suitable for self-administration. Four measures of health literacy were identified, of which two were rated most suitable for the study. Feedback on the two outcome measures was sought from six parents, including two fathers and four mothers (one of whom was Aboriginal and one for whom English was a second language). All parents indicated a preference for the All Aspects of Health Literacy Survey (AAHLS) due to its brevity and simplicity. The AAHLS has also been shown to have good internal consistency. 23
The AAHLS comprises 13 statements. Eleven statements use a 3–4 point frequency Likert scale, and two statements use a dichotomous response format. The AAHLS is able to generate a total health literacy score (i.e. sum of all 13 items, with scores ranging between 10 and 36), and subscale scores for four constructs of health literacy:
24
Functional health literacy score: defined as an ability to read and/or understand health information (based on the sum of 3 items; score range: 3–9) Communicative health literacy score: defined as an ability to communicate with health professionals (based on the sum of 3 items; score range: 3–9) Critical health literacy score: defined as an ability to manage health information (based on the sum of 4 items; score range: 4–12) Empowerment health literacy score: defined as capacity to take action for one’s health (based on the sum of 3 items; score range: 0–6).
Higher AAHLS scores indicate a higher level of health literacy. To address the second objective of the study, the survey also included eight demographic questions, including parent/carer role (i.e. mother, father, other carer), highest level of education, employment status, main language spoken at home, Aboriginal/Torres Strait Islander (ATSI) status, number of children and child(ren) with a disability/chronic disease. The estimated completion time of the survey was 10 minutes.
Data Collection
As people who live in rural areas are under-represented in health research and reportedly difficult to recruit, we were aware of the need to intensify efforts to reach this population. 25 As such, the survey was promoted using myriad strategies, including printed flyers (posted in public locations, such as libraries and shopping center/community/university notice boards), community radio (i.e. radio interview with study investigators), primary school newsletters, and a display table in the main local shopping center. Printed copies of the questionnaire were also distributed to parents attending local primary schools and placed in school front offices. Eligible participants were directed to complete the survey either: (a) online (via the LimeSurvey platform), (b) in print copy (and lodge this in the collection box provided), or (c) with the assistance of a member of the research team (particularly if individuals were not proficient in the English language). All participants were required to provide informed written consent prior to participation. Data collection was undertaken between September and November, 2018.
Data Analysis
Data were imported into IBM® SPSS® Statistics 25.0 for coding and data analysis. AAHLS scores/subscores were reported as medians and IQRs as data were not normally distributed. Associations between AAHLS scores/subscores (i.e. total score, functional health literacy score, communicative health literacy score, critical health literacy score, empowerment health literacy score) and nominal sociodemographic characteristics (i.e. Aboriginal/Torres Strait Islander status, parent/carer role, child(ren) with a disability/chronic disease, main language spoken at home, employment status) were assessed using Cramer’s V. Relationships between AAHLS scores/subscores and ordinal sociodemographic characteristics (i.e. number of children, highest level of education) were tested using Kendall’s tau (τ). Coefficients ranging between 0.10–0.29 represented a weak association, 0.30–0.49 a moderate association, and 0.50 and above a strong correlation. The level of significance was set at p < .05.
Ethics
The study was approved by the University of South Australia Human Research Ethics Committee.
Results
The survey was undertaken by 155 parents/carers, of which 140 (90.3%) surveys were fully completed. Participants who did not persist with the survey until completion still answered a sufficient number of items for their responses to be included in the analysis. The survey response rate could not be determined as the population reach was uncertain.
Demographic Characteristics
Participants were predominantly mothers (79.4%), non-Aboriginal/Torres Strait Islander (92.3%), and spoke English as the main language at home (97.4%) (Table 1). More than one-half of participants were employed (61.9%) and had completed tertiary (Technical and Further Education [TAFE] institute or University) education (52.3%). Most participants had 2–3 children (62%), of which 42.6% reported a child(ren) with a disability or chronic illness.
Demographic Characteristics of Participants (n = 155).
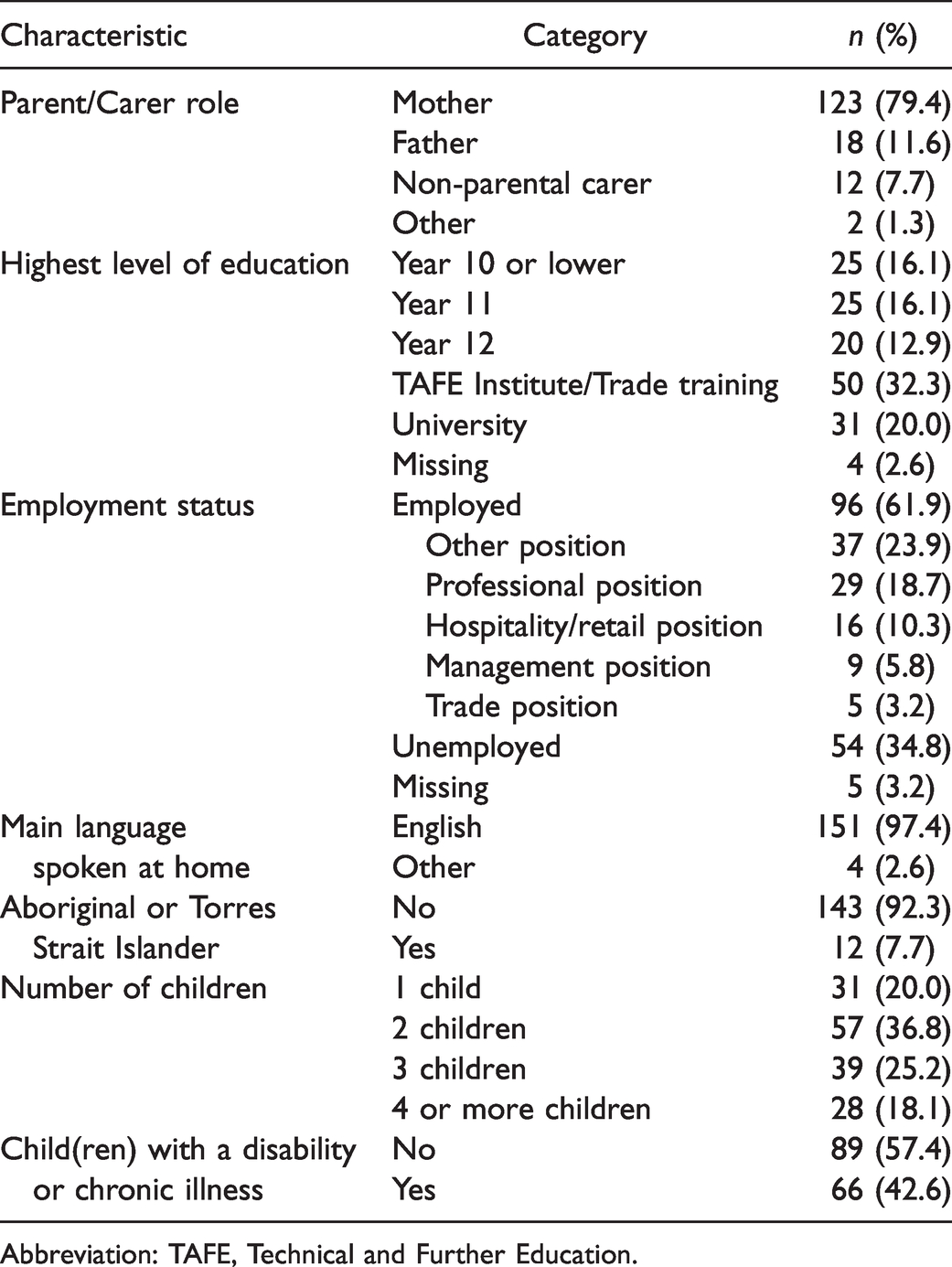
Abbreviation: TAFE, Technical and Further Education.
Health Literacy
Total Health Literacy
The median total health literacy score was 27 (IQR 26,29; range 19–32), from a possible range of scores between 10 and 36; indicating that the participant’s total health literacy scores were mostly in the mid-high range (upper end of the second tertile) (Figure 1). There was no significant association between total health literacy score and any sociodemographic factor (Table 2).
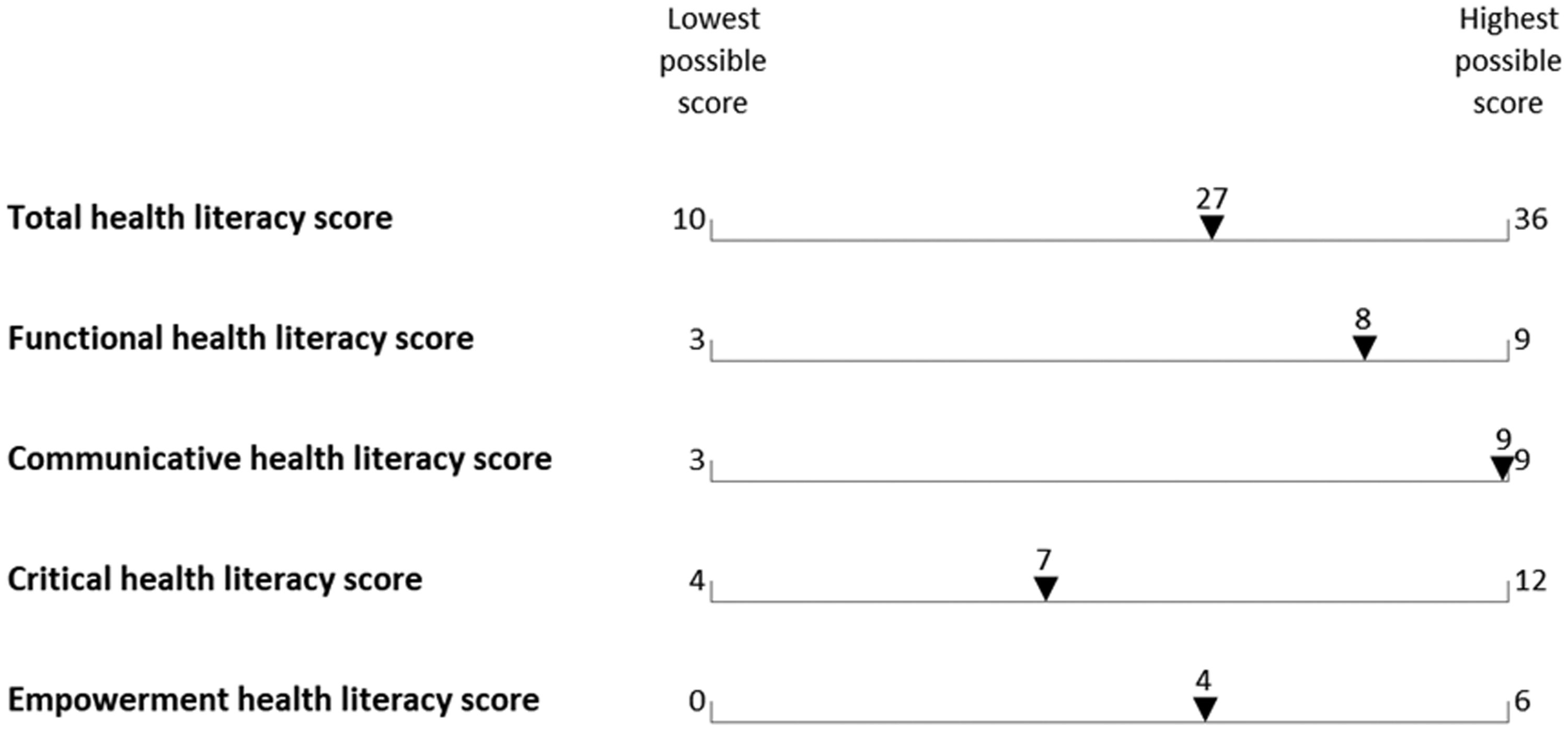
Median All Aspects of Health Literacy Survey (AAHLS) Total and Subscale Scores for All Participants (n = 155).
Median All Aspects of Health Literacy Survey (AAHLS) Total and Subscale Scores by Demographic Characteristic (n = 155).
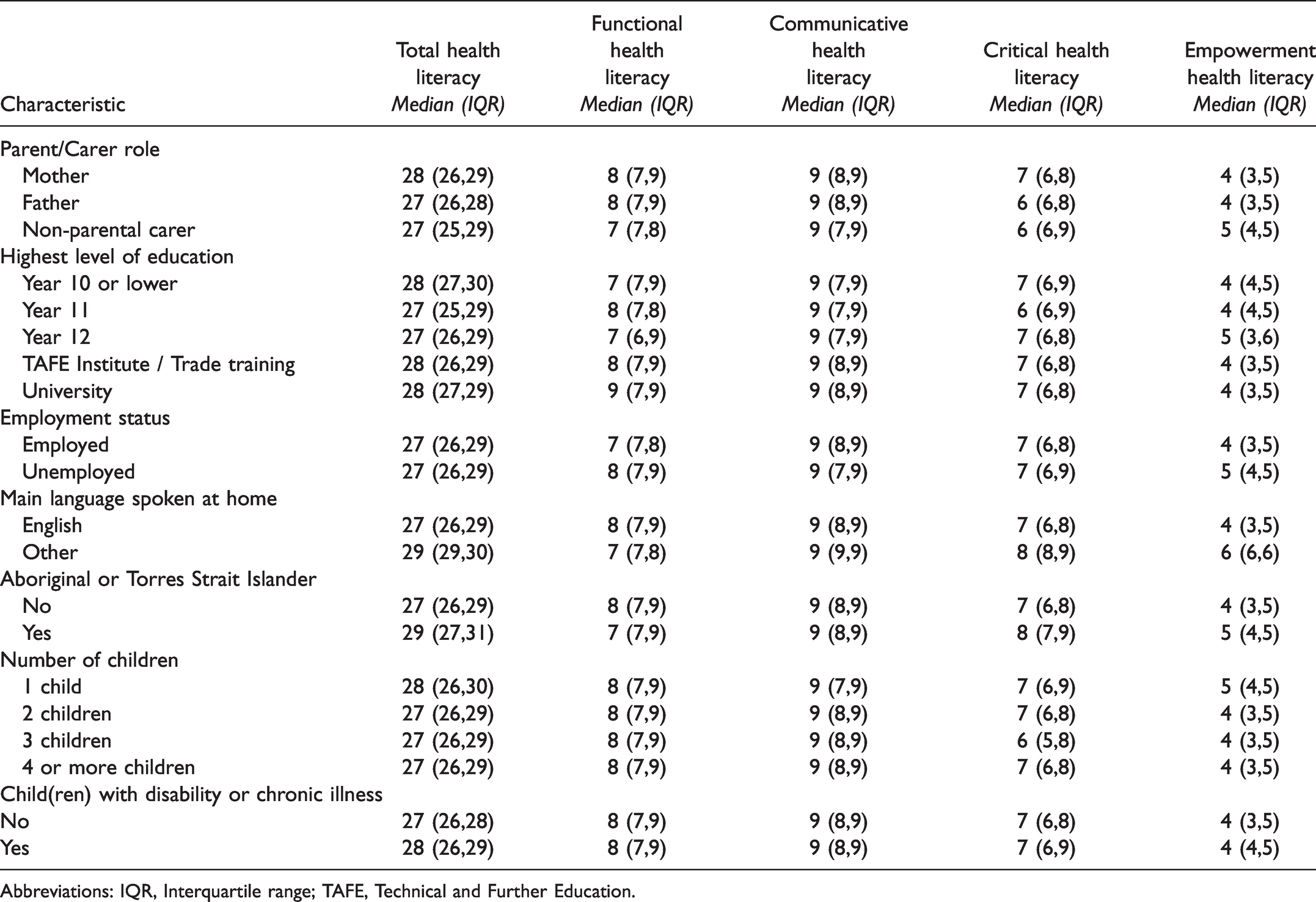
Abbreviations: IQR, Interquartile range; TAFE, Technical and Further Education.
Functional health literacy: The median functional health literacy score was 8 (IQR 7,9; range 4–9), from a possible range of scores between 3 and 9 (Figure 1). This suggests the participant’s functional health literacy scores were mostly in the high-range (third tertile). There was a weak positive association between functional health literacy score and highest level of education (τ = 0.137, p = .048). There was no significant association between functional health literacy score and other sociodemographic factors (Table 2).
Communicative Health Literacy
The median communicative health literacy score was 9 (IQR 8,9; range 3–9), from a possible range of scores between 3 and 9 (Figure 1). This suggests the participant’s communicative health literacy scores were largely in the high-range (third tertile). There was a weak positive association between communicative health literacy score and carer status (V = 0.248, p = .012; with higher scores reported among fathers), meaning fathers had higher levels of communicative health literacy relative to mothers and non-parental carers. There was no significant association between communicative health literacy score and other sociodemographic factors (Table 2).
Critical Health Literacy
The median critical health literacy score was 7 (IQR 6,8; range 4–12), from a possible range of scores between 4 and 12 (Figure 1). This indicates the participant’s critical health literacy scores were predominantly in the mid-range (second tertile). There was a moderate positive association between critical health literacy score and ATSI status (V = 0.367, p = .010; with higher scores reported among people identifying as ATSI, meaning ATSI people had higher levels of critical health literacy than non-ATSI participants. There was no significant association between critical health literacy score and other sociodemographic factors (Table 2).
Empowerment Health Literacy
The median empowerment health literacy score was 4 (IQR 3,5; range 1–6), from a possible range of scores between 0 and 6 (Figure 1). This suggests the participant’s empowerment health literacy scores were largely in the high-range (third tertile). There was no significant association between empowerment health literacy score and any sociodemographic factor (Table 2).
Discussion
This is the first known study to examine the health literacy of parents living in a regional Australian community with a high level of socioeconomic disadvantage. The findings revealed a moderate-high level of health literacy amongst participating parents, including moderate critical health literacy, and high functional, communicative and empowerment health literacy. ATSI participants, fathers and those with a high level of formal education reported significantly higher levels of critical, communicative and functional health literacy, respectively.
Functional health literacy reflects a person’s ability to read and understand health information. Parents in this study largely reported a high level of functional health literacy, indicating that most did not require assistance with the interpretation and/or completion of health documents. This contrasts with other studies that have uncovered high rates of inadequate/marginal functional health literacy in regional populations.26,27 It is possible that the young age (i.e. parents of primary school children) and high education level (i.e. 52% holding a post-school qualification) of participants may have contributed to the high level of functional health literacy reported in this study.16–18 Regional stoicism (i.e. the reliance on self rather than others) and poor accessibility to health services/providers in the region (which may have induced parents to find alternative ways to obtain health information) are other potential explanations for the results that warrant further exploration. While comparisons between our findings and studies examining pertinent urban parent populations may have helped support this hypothesis, this was not possible given the current dearth of parent health literacy research in Australia. 28
Most participants rated their ability to manage health information (i.e. their critical health literacy) as moderate. In other words, the majority of parents sought out different information on their child’s health, questioned health provider advice, and/or explored the trustworthiness and sensibility of information obtained, only sometimes. Thus, parents were not consistently discerning of health information relating to their child. This may be problematic where access to qualified health providers is limited (i.e. regional communities), and online resources become the primary source of health information, as the quality of online information can be highly variable and in turn, misleading.29–31
An interesting finding of this study was the positive association between critical health literacy score and Aboriginal or Torres Strait Islander status. This is interesting because findings from other studies suggest people from ethnic minority groups have relatively lower levels of health literacy.16,32 Perhaps those elements considered important to Aboriginal or Torres Strait Islander people (i.e. social connection and collaboration) 33 – the same factors that contribute to critical health literacy in the general population 34 – fostered critical health literacy among participating Aboriginal or Torres Strait Islander parents. Though limited by a relatively small number of Aboriginal or Torres Strait Islander participants, this is an interesting hypothesis, which through further examination, may allude to new strategies to improve critical health literacy in parents.
Despite the moderate level of critical health literacy reported by parents, most reported a high degree of communicative health literacy (i.e. the capability of communicating with health professionals). To elaborate, parents were generally confident in providing health providers with the information they need, asking health providers questions, and ensuring health providers explained anything that was not easily understood. This type of health literacy is particularly important in regional communities where communication between health providers/services represents a major barrier to health care access, and can in turn contribute to undesirable health outcomes.35,36
The higher level of communicative health literacy among male carers (i.e. fathers) was particularly noteworthy given that previous studies have reported lower levels of health literacy in males relative to females.18,37 While the reasons for this finding are not entirely clear, a significantly higher proportion of fathers (compared with mothers) did hold a post-school qualification (77.8% vs. 52.9%; V = 0.335, p < .001) – a known predictor of health literacy.17,38 Another possibility is that fathers engage in conversations with health care providers differently than mothers; although, there is currently limited evidence to support this claim.
Health literacy is not just about accessing, appraising and interpreting health information (WHO, 2015); it is also about using health information to inform and change behavior. The ability to take action to address a health issue is referred to as empowerment health literacy. In this study, parents reported a high degree of empowerment health literacy. This result has positive implications for parents and their children, with findings from previous research of maternal-child dyads in a home visiting program indicating that empowerment health literacy can assist parents to better manage their own, as well as their child’s, health and healthcare. 39
The relevance of these findings to the Whyalla context is supported by the fact that the study sample closely approximated the demographic characteristics of this regional city. In terms of indigeneity (5% of the Whyalla population), highest qualification (years 10 [13%], year 11 [13%], year 12 [13%] and TAFE [28%]), and proportion of persons employed in a professional (15%), managerial (8%) or retail/hospitality (9%) position, the sample was similar to the distribution observed in the general Whyalla population. 22 However, males (50%) and trade workers (18%) were somewhat under-represented, and persons reporting university (6%) as their highest qualification were somewhat over-represented in the study sample. 22 Notwithstanding, this gender and education profile is characteristic of parent studies more generally.9,11,14
While the study sample may be broadly representative of the Whyalla population in terms of sociodemographic characteristics, there are some limitations worth noting. As the study used non-probability sampling, the study is susceptible to self-selection bias. This, together with the fact that the survey was self-administered, might mean that the survey could have attracted people with higher levels of literacy and health literacy. This risk was tempered to some degree by directly recruiting parents from schools with diverse levels of socioeconomic disadvantage, as well as public venues (e.g. shopping centers and libraries), and by offering participants the opportunity to complete the survey with the assistance of a member of the research team. Another limitation of the study is that the findings reflect the health literacy of participating parents within the city of Whyalla; as such, the results may not be generalizable to parents living in other regional communities in South Australia or nationally.
Conclusion
Supporting a child’s healthy development is a societal priority. Yet, parents face a challenging task when navigating the landscape of health information to support their children’s healthy development. Furthermore, until now, comparatively little has been known about the health literacy of parents, beyond infancy. In addressing this knowledge gap, this study has revealed new insights into the health literacy of parents/carers of primary school-aged children living in a regional community context. Notwithstanding, further work is still required. For instance, there is a need to explore the differential effect of parental health literacy on child health outcomes. Following this, it will be necessary to examine the types of strategies that may be effectively employed by parents, clinicians and relevant stakeholders to mitigate the impact of these barriers on a child’s healthy development.
Footnotes
Acknowledgments
The authors would like to thank the participants and the Whyalla community for supporting this project.
Author Contributions
M. J. L. and S. N. conceived the project. M. J. L. performed the analysis and drafted the results. S. N. and S. T. drafted the introduction, methods and discussion. All authors reviewed, edited and approved the manuscript prior to submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by funding from the Research Themes Incentive Scheme, University of South Australia.
Availability of Data and Material
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Consent to Participate
Written informed consent was obtained from all participants.
Consent for Publication
Written informed consent was obtained from all participants.
Ethics Approval
The study was reviewed and approved by the University of South Australia Human Research Ethics Committee.