
Abstract
Purpose:
This paper examines community leaders’ and researchers’ recommendations for reaching rural communities in a southeastern U.S. state with cancer prevention and control programming.
Research Design:
A qualitative inquiry of a grant network’s research and community councils was conducted to explore members’ opinions on how to engage rural communities and obtain input on how to recruit rural organizations for a mini-grants program.
Study Sample and Data Collection:
Telephone/virtual interviews were conducted with all 13 council members. Responses were analyzed using thematic analysis and findings were examined within the context of system-centric and patient-centric dimensions.
Results:
Council members discussed limited education, lack of insurance, low socioeconomic status, health care avoidance, and transportation as barriers to cancer prevention and control. They recommended reaching rural populations by partnering with community and faith-based organizations, use of targeted multi-media, and tailored cancer education trainings.
Conclusions:
Findings are used for guiding outreach with rural communities and recruitment of rural organizations for a cancer-focused mini-grants initiative.
Keywords
Introduction
Rural communities in the United States (U.S.) face notable disadvantages compared with urban areas, including higher poverty rates, lower educational attainment, limited access to health services, and a lack of resources needed to support public health infrastructure.1–3 Consequently, rural communities often face elevated rates of disease incidence and mortality, including cancer.1,4 Despite an overall decrease in cancer death rates in the U.S. in recent decades, rural areas are experiencing a reduction in cancer death rates much more slowly than in urban regions. 3 Many of these rural counties are in states that have rejected Medicaid expansion, thus exacerbating existing trends.2,5,6
To reduce the burden of cancer, especially among those disproportionately affected, the CDC-funded Cancer Prevention and Control Research Network (CPCRN) works through a national network of academic, public health, and community partners to conduct partner-engaged cancer research. 7 In the state of South Carolina, this SC-CPCRN Collaborating Center has been funded continuously since 2009. Efforts are aimed at accelerating the adoption and implementation of evidence-based cancer prevention and control strategies in communities, enhancing large-scale efforts to reach rural and minority populations in order to reduce the burden of cancer, and developing the dissemination and implementation workforce in cancer prevention and control. 8 In South Carolina (SC), African Americans and rural residents make up ∼28% and ∼34% of the total population, respectively, 9 and SC has one of the largest rural minority populations (∼43.5%) in the U.S. 10 Programs such as the SC-CPCRN that aim to reduce disparities work most effectively if they address two dimensions for improving access to care: (1) the system-centric dimension which refers to the operationalization of available resources of health systems in communities using five dimensions of accessibility, and (2) the patient-centric dimension, which refers to the abilities of populations that serve as a means for engagement with accessible health resources.11,12
For the current 5-year grant cycle, both a Research Advisory Council (RAC) and Community Advisory Council (CAC) were established. The RAC consists of five scholar experts in rural cancer control, community-engaged research, and implementation science. Research Advisory Council members advise on research protocols and ensure that all partner-engaged research efforts align with the proposed aims of the grant. The CAC consists of eight community leaders who offer context-relevant information and recommend recruitment and outreach strategies within rural areas of the state. The councils were created to engage community and academic partners in planning, implementing, and evaluating cancer prevention and control efforts during the entire grant period.7,13 These types of partnerships allow for capacity building and facilitation of cancer prevention and control efforts through the reciprocal exchange between partners and academic researchers. 14 The SC-CPCRN also collaborates with the SC Primary Health Care Association and federally qualified health centers to achieve its intended goals. Through these established partnerships with target audiences and these stakeholders, the relevance of the efforts is strengthened leading to improved health outcomes.14,15
The SC-CPCRN utilizes mini grants to encourage and engage communities in utilizing evidence-based interventions (EBIs) to facilitate the dissemination and implementation of cancer prevention and control. 16 Evidence-based interventions are peer-reviewed practices or programs with documented empirical evidence of effectiveness that often can be adapted to fit specific community needs.16,17 While each council typically meets separately, they have interacted via email and in virtual meetings in the planning of the SC-CPCRN’s mini-grants program. They also have received joint updates and presentations from community grantees. Community Advisory Council members who were previous grantees also collaborated with investigators on an informational webinar for current mini-grant applicants. Community Advisory Council and RAC members shared their perspectives on how to effectively recruit applicants for the SC-CPCRN’s Community Health Intervention Program (CHIP) mini-grants initiative in rural areas of SC. 8 Currently, mini-grant funds are intended for program-specific expenses over a 12-month period. Each recipient organization receives technical assistance from the SC-CPCRN staff to help with implementing and evaluating the program aimed at improving health outcomes for their rural communities. Community Advisory Council and RAC members are offered the opportunity to review proposals and serve as liaisons and/or advisors in recruitment, implementation, and/or evaluation.
The overall goal of this paper is to present CAC and RAC members’ opinions and ideas for reaching rural communities in SC with cancer prevention and control guidelines and programs. Specific objectives were to: (1) obtain RAC and CAC members’ ideas for effective outreach with rural communities; (2) examine RAC and CAC members’ opinions on how to recruit community-based organizations for the mini-grants initiative. Findings from the interviews conducted are used to guide outreach with rural communities and recruitment of rural organizations for a cancer-focused mini-grants initiative.
Methods
Interview Recruitment and Protocol
The lead author contacted council members by email and/or telephone to invite them to participate in interviews. This author also conducted the interviews. All 13 advisory council members were contacted, and all agreed to participate: i.e., 8 CAC members and 5 RAC members. Each RAC and CAC member was provided with a US$10 gift card for their participation. Separate, but related, open-ended interview questions were created for the RAC and CAC, and all protocols and interview questions were reviewed and approved by the University’s institutional review board (IRB).
Both the RAC and CAC interview guides underwent several revisions by team members prior to submission to the IRB. The CAC interview guide consisted of 17 open-ended questions within four categories: (1) the CAC members’ affiliated organization’s community outreach; (2) how their organization specifically addressed cancer-related information and resource needs within their communities; (3) the CAC members’ collaborations with the SC-CPCRN; and (4) CAC members’ ideas for recruitment of rural organization applicants for the CHIP program.
The RAC interview guide consisted of 18 open-ended questions within five overarching categories: (1) the focus and research areas of RAC members’ affiliated organization; (2) individual research interests; (3) collaborations with the SC-CPCRN; (4) perspectives and expertise pertaining to cancer prevention and control specifically in rural areas in alignment with the current focus of the SC-CPCRN; and (5) CHIP mini-grant applicant recruitment in rural areas.
Interviews lasted 30–45 min and were conducted remotely via telephone call, Zoom, and WebEx platforms.18,19 One CAC member and one RAC member provided responses via email correspondence. Each interview was recorded, and notes were taken for reference during data analysis and for verification of transcript accuracy. Original recordings were stored electronically, and password protected by the interviewer (AB). Interviews were transcribed verbatim by a professional transcription company and all transcripts were quality checked using the audio recordings by two of the authors (AB and CT). All personal identifiers were removed prior to coding and analysis.
Coding and Thematic Analysis
In order to develop the codebooks for analysis, two RAC and two CAC transcripts were selected randomly. These transcripts were reviewed independently by three of the authors (AB, CT, and DBF). The two interview guides were used as an initial framework for the two codebooks. Each codebook was then entered into NVivo® 12, and the transcripts were uploaded for line-by-line open coding within their respective codebook. 20 Each interview was then coded by two coders (AB and CT) using the established codebooks to identify high frequency themes and subthemes.21,22 New codes were added into the codebook as they were identified during this full coding process. Axial coding, used to identify thematic relationships between codes, followed.23,24 Coders also used a constant comparison process in which themes were compared and contrasted across groups (i.e., RAC and CAC members). 23 Coders maintained open channels of communication to maintain consensus and discussed any coding discrepancies throughout the coding process.
Responses also were categorized using system-centric and patient-centric dimensions to care. The system-centric dimensions utilized were: (1) Approachability: the organization’s ability to augment individuals’ understanding and identification of available resources, (2) Acceptability: the social and cultural perspectives that influence patients’ ability to seek and accept health services, (3) Availability and Accommodation: the ease of access and availability of care provided by organizations, (4) Affordability: the expenditure of resources and access to adequate funding and availability of resources of an organization, and (5) Appropriateness: the quality and adequate availability of services provided by organizations that support the continuity and quality of care.11,12 The corresponding abilities of populations to engage were analyzed through the five patient-centric dimensions: (1) Ability to Receive: the ability of individuals facing illness to identify and understand the accessibility of resources, (2) Ability to Seek: the cultural, autonomic, personal, and social values that influence an individual’s ability to seek and accept care, (3) Ability to Reach: the patient’s ability to access appropriate information and services, (4) Ability to Pay: the social, bureaucratic, and economic influences that impact the ability of patients to receive care, and (5) Ability to Engage: the patient’s ability to actively make decisions relating to their treatment as well as their level of engagement with providers.11,12 The patient-centric dimensions intersect with social determinants of health. According to the CDC, social determinants of health fall under five domains: economic stability, health care access and quality, social and community context, education access and quality, and neighborhood and built environment. 25 To ensure quality coding and interpretation of the data, including categorizing responses according to dimensions of care, coders met to discuss their independent review of the open-ended interview responses. Coders arrived at complete agreement on coding categories and main emergent themes. Unique quotes were selected to support themes and to help validate the authors’ coding and interpretation.
Results
Community Advisory Council members were affiliated with local government (n = 2), faith/community-based organizations (n = 3), medical associations (n = 2), or were retired (n = 1). Members’ organizations mainly focused on improving consumer and patient health literacy and access to health and cancer care in SC. All RAC members were affiliated with research/academic organizations and were focused mainly on research designed to improve health outcomes; for example, conducting health interventions and disseminating health-related information.
Council Members’ Recommendations Aligned with Patient Centric and System Centric Dimensions.
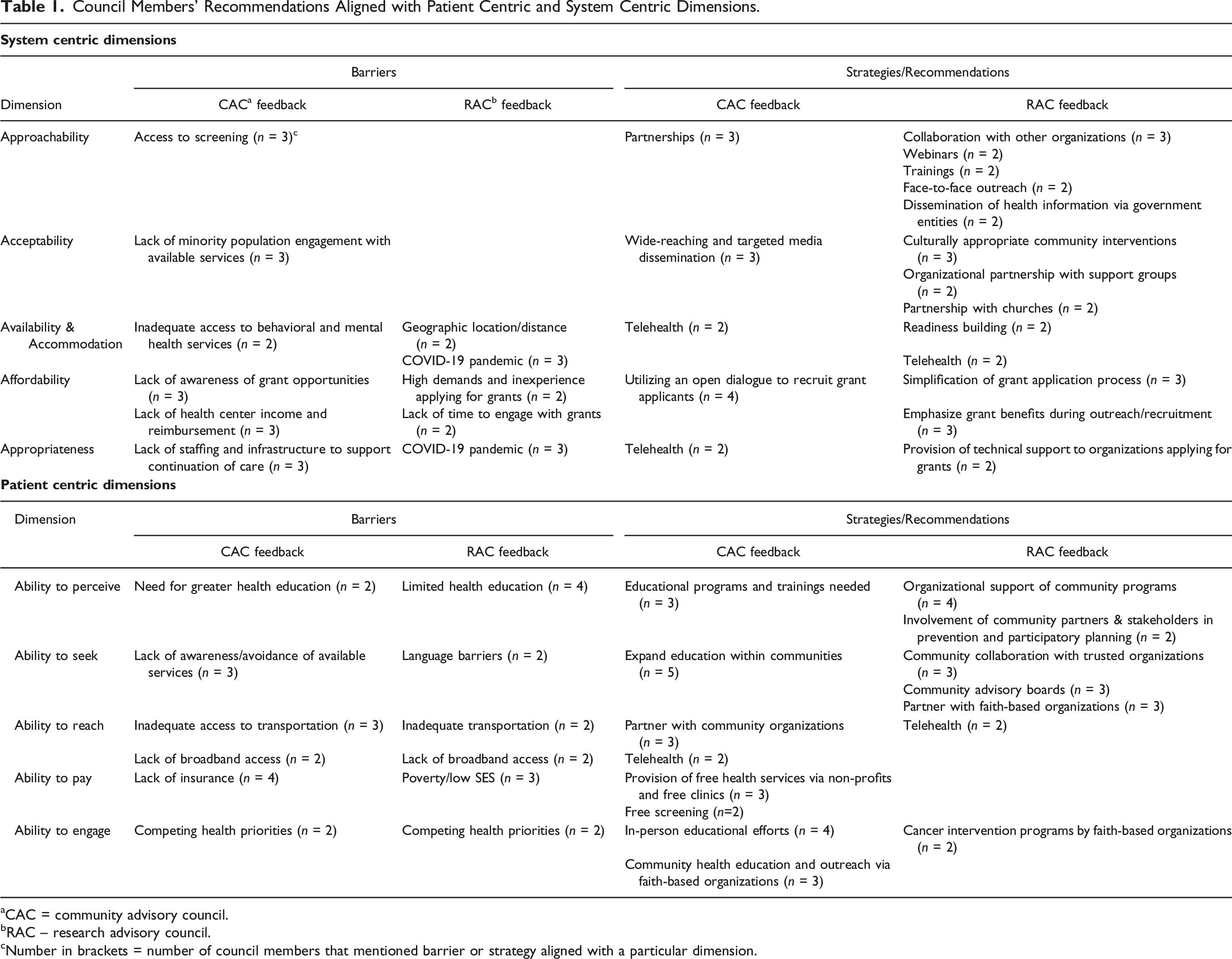
aCAC = community advisory council.
bRAC – research advisory council.
cNumber in brackets = number of council members that mentioned barrier or strategy aligned with a particular dimension.
Council Members’ Engagement with Communities
Community Demographics and Health Care Needs
When asked to define the communities with whom they partnered or served, most CAC members described community in terms of geographic location. These specific target communities were defined as rural or statewide. Community Advisory Council members also described their community demographics in terms of ethnicity and age. Hospitals were identified as the target community for few CAC members. When asked what health care needs were present in their communities, all CAC members identified access to care as a critical need. They specified that access to cancer screenings, mental and behavioral health services, transportation to care, and health and cancer education were needs within their communities.
Community Advisory Council members shared strategies they used to share health- and cancer-related information with their communities including: partnering with community- and faith-based organizations, use of wide-reaching, targeted, multi-media, and offering educational programs and trainings. One CAC member suggested that their strategies differed depending on the needs and demographics of the group they are trying to reach, as reflected in these quotes: “We have health events where we partner with other churches in the area, and we have met at other churches in terms of health disparities and health issues ... we have different programs, we have different events, we’ve had plays, we just have different educational forums where we also invite the community.” (CAC Member 5) “A variety of different ways.... specific initiatives, where that could be actually real-time in person. It’s also through regular communication channels, newsletters, e-mail communications, social media, press releases, working through the media, also in different forms, depending on the group.” (CAC Member 1)
Research Advisory Council members also were asked to identify dissemination strategies. Strategies mentioned most often were collaborating with other organizations and conducting webinars and trainings. One representative quote was: “We’re engaged in the partnership, but we also provide resources and technical assistance related to health... We’re involved and partner with groups … and share information that way. And then I would say faith communities would be a strong group that we do share trainings and information lists.” (RAC Member 3)
Tailoring Cancer Research and Education for Different Communities
Research Advisory Council members identified involvement of community partners and stakeholders to be critical for encouraging cancer prevention. They also used organizational capacity to build readiness to gauge how they needed to tailor research and education to communities. Representative quotes included: “We have some projects that, from the very beginning, the communities at the table with us, and developing the intervention or program, and providing guidance on logistics and feasibility for evaluation. And so, they’re involved in every aspect.” (RAC Member 2) “Our readiness building system depends on what the readiness of that organization or community is and that we move forward with strategies to build readiness depending on the assessment... we’re developing readiness assessments in relation to colorectal cancer screening and child obesity prevention programs.” (RAC Member 4)
Research Advisory Council members also discussed the strategies they use to tailor cancer research to communities. Culturally appropriate, community-based interventions were most commonly mentioned, as reflected in this quote: “All types of cultural level adaptations of making sure the interventions have a look and feel that’s culturally appropriate or language appropriate ... everything I do is adapted to the group that I am working with.” (RAC Member 3)
Research Advisory Council members also stated that their organizations have had to adapt their strategies for disseminating cancer information in response to COVID. For example: “Before COVID lots of face-to-face interaction with community outreach activities like health fairs, speakers' bureaus, and participating on community advisory boards, forming community advisory boards, being in the community doing interventions and programs, and then now we do some of that stuff virtually, too.” (RAC Member 3)
Cancer Prevention and Control Initiatives
Community Advisory Council members stated that their organizations focus on a variety of cancer types with the most one being breast cancer. They also focused mainly on primary and secondary cancer prevention. Research Advisory Council members were also asked to discuss the focus of their cancer- related research. Research Advisory Council members discussed their work in implementation and evaluation, intervention development, health disparities, primary prevention, and community research. The most commonly mentioned topic area was obesity prevention.
Barriers to Effective Cancer Prevention and Control among Rural Populations
Both RAC and CAC members discussed barriers to effective cancer prevention and control among rural populations. The financial barriers to effective cancer prevention and control were highlighted by the RAC and CAC member from both patient and system perspectives. From a patient-centric perspective, RAC members suggested that patient demographics were important to consider, especially limited health education and poverty/low socioeconomic status; similarly, CAC members identified lack of insurance as a barrier for patients. “Medical costs, if they don’t have insurance is pretty high... when we have the free health fairs where they offer free testing...of course, you have to get there early.” (CAC Member 5)
Community Advisory Council members further highlighted potential coding issues and/or lack of reimbursement that serve as a barrier on the provider side, as reflected in this quote: “I would say another barrier would be the ability for providers to utilize certain chronic care codes, either in their practice or in health centers – maybe not having enough sales to do that, maybe not having an understanding of what those codes are, but that could certainly increase reimbursement for providers, which could go back to perhaps seeing more patients in that community.” (CAC Member 1)
Both CAC and RAC members identified inadequate access to transportation; however, both councils suggested telehealth as a strategy to improve patients’ access to medical services. Research Advisory Council and CAC members identified lack of access to broadband as a further barrier in rural areas. “I think telehealth holds promise for follow-up ... allowing them to stay closer to home and removing or reducing the transportation barrier via telehealth for follow-up I think makes a lot of sense.” (CAC Member 7) “There’s a lot of variability in rural settings ... we’re seeing a slower uptake on the technology for telehealth within the organizations but also on the part of patients. Patients tend to be older, lower education levels, poorer, and so they may not have access to high-speed Internet or some other things... in transportation/access to screening services ...” (RAC Member 1)
Furthermore, CAC members identified lack of awareness and avoidance of available services as an additional barrier that influences patients’ ability to seek resources. Additionally, CAC members identified limited minority population engagement with available services as a further barrier as reflected in these quotes: “I don’t think we could ever get enough education and just being educated enough to go to the doctor. I don’t know if it’s a fear or what – but just to be more aware of their own health issues that they may have.” (CAC Member 5) “Well, it’s the religious-based, African-American community … we focus on primarily because they have a higher propensity of getting colon cancer ... that portion of our population does not get colonoscopies as frequently or as per the guidelines from medical authorities with respect to the colonoscopies and the prevention of colon cancer.” (CAC Member 2)
From a system centric perspective, RAC and CAC members identified further barriers that influence established health systems’ ability to provide appropriate and accessible care to communities. The most frequently identified by CAC members was lack of staffing and infrastructure to support the continuation of care. Research Advisory Council members primarily mentioned the COVID-19 pandemic as a barrier to the provision of appropriate and adequate health services: “It may be capacity with staffing because their staff works in various areas and are already carrying a heavy load. Sometimes it may be some financial impact as it relates to making adjustments to the actual organizational or operational infrastructure and the utilization of some of the technology.” (CAC Member 6)
Effective Cancer Prevention and Control Strategies
In terms of improving ability to seek resources, CAC members described the importance of expanding cancer education to different groups of people as an effective strategy for cancer prevention and control. Research Advisory Council members mentioned several specific strategies, including community collaboration with trusted organizations, partnership with faith-based organizations, and establishing community advisory boards, as reflected here: “I think involvement with local communities, be it churches or community centers, can also work.” (RAC Member 1) “We have found that in rural communities, trying to look at organizations, or entities, that already exist in those settings, that people trust is a great way to get information out to people ... places where people come to naturally would be the big ones.” (RAC Member #2) “The most successful has been the personal intervention with the church leadership or community leaders to lay out the programs that are available to detect colon cancer ...” (CAC Member #2)
Both councils recommended strategies that could improve patients’ ability to understand their medical situation and actively engage in health-related decision making. Some CAC members specifically cited in-person educational efforts and community health educational outreach via faith-based organizations. Similarly, RAC members suggested organizational partnership with churches and support groups as well as face-to-face outreach, for example: “Mainly...by doing educational presentations to let the people know about prostate cancer, talking about statistics, risk factors, treatment options ... The main thing {is that} when men come to our meeting initially, they are normally newly diagnosed ... They are looking for information on treatment options and other information that we might have.” (CAC Member 4)
Finally, CAC members suggested strategies to address financial and economic barriers that influence patients’ ability to pay. The most commonly mentioned was the provision of free health services via non-profits and free clinics followed by the provision of free cancer screening. “I think the strategy of ...{making} sure that we get the educational word out to everyone ... We partner with the free clinic in X County. We provide education sometimes in their waiting rooms.” (CAC Member 3)
Recruitment of Mini-Grant Applicants
Both CAC and RAC members discussed barriers to and strategies for effective recruitment of mini-grants applicants for conducting cancer prevention and control efforts in rural communities. The council members provided suggestions for partnerships to promote the program.
Recruitment Barriers
The most commonly mentioned barrier by CAC members was limited awareness. Two RAC members cited inexperience with the grant process as well as lack of time to engage with grants: “I think there’s a point of making folks aware that the grants are available, and how do you make them aware of it is based on how well you can reach out to community leaders and telling community leaders what’s available out there.” (CAC Member 2) “Probably lack of time and right now might be a particularly challenging time ... if they think there’s going to be a lot of reporting, or paperwork, or things like that, that could be a barrier for them initiating something like that.” (RAC Member 2)
Recruitment Strategies
Strategies for recruiting rural applicants mentioned most frequently by the RAC members were to emphasize the benefits, simplify the application process, and offer technical support. Several CAC members suggested the importance of open dialogue as a recruitment strategy. “… make the application process pretty easy, so that people aren’t, that the provider is not turned away from it … and trying to promote that in the materials, like why they should do this, or why they’d want to do this, or how it would help them or their practice, or that sort of thing.” (RAC Member 2) “The key...is just finding methods of getting the information to the leaders ... I’ve found that personal intervention is probably the most effective way of making it happen ... it just takes time ... but it’s the most effective because you have an opportunity then to sit with the person and talk to – there’s dialogue, and that’s probably – whenever you have dialogue, it’s probably the most effective means of getting someone to buy in.” (CAC Member 2)
Partnerships
Ideas for partnerships to pursue to promote the mini-grants program were recommended by both councils. Community Advisory Council members most frequently mentioned community groups, federally funded clinics, churches, and health ministries. For example, “I think there should be a linkage between the health ministries and CPCRN to lay out the mini-grant opportunities for them because, again, my – we’ve already worked with colon cancer, but with the grant, the grant is really about awareness about all cancers ... Some of the churches don’t have health ministries, but I think one of the methods that would surely help would be to identify those with health ministries, maybe look up the health ministries, for opportunities, and then let them take off.” (CAC Member #2)
Similar to the feedback from the CAC members, RAC members mentioned faith-based organizations and community organizations. “This will differ by area … for us, we use a combination of advocacy groups, faith and education-based groups, patient advocates, health care associations, and health councils.” (RAC Member #5)
Discussion
Identifying the health care needs of communities is essential for tailoring cancer prevention and control efforts for rural communities. 8 Understanding community needs from the perspective of community leaders and champions and research gaps and strategies from research advisors is critical for effective outreach to and cancer prevention and control with underserved rural communities. The CAC serves as a conduit for information exchange between communities across SC and the SC-CPCRN. As such, it allows for increased visibility of contemporary health needs. All CAC members stated that access to care is a need within rural communities. South Carolina is a rural state (e.g., Charleston and Columbia, with populations of 156,600 and 139,600, respectively, are the largest cities in the state) with a high rate of unmet need. Of South Carolina’s 46 counties, 29 are considered fully medically underserved by the CDC, with 14 other counties being partially medically underserved.26,27 Disparities exist in both rural and urban settings, including those that impact the elderly, Hispanics, and African Americans; however, these disparities exist to a greater extent in rural areas. 28 Understanding how these disparities manifest requires a robust understanding of how barriers in care access can be overcome by tailoring efforts to the specific needs of communities.
Relating to ability to perceive the need for cancer prevention and control, CAC members suggested that limited education serves as a barrier to effective dissemination of cancer-related information and services and serves to maintain a lack of awareness in terms of being able to access, understand and apply relevant information. 11 Inadequate health literacy has been associated with increased rates of hospitalizations, increased mortality, and poorer health outcomes. 29 Community Advisory Council members referenced partnerships with other organizations and educational trainings as effective strategies for reaching rural communities. This included implementing cancer education programs in a faith-based setting which can serve as a culturally appropriate outlet for effective dissemination and can help facilitate a dialogue between providers and individuals living in rural communities. 30 A theatrical production focused on colorectal cancer screening created and presented by a health and wellness ministry at a church in SC increased participants’ knowledge about colorectal cancer and examined their intentions to be screened. Results showed increased knowledge about colorectal cancer, increased awareness and understanding about the importance of colorectal cancer screening, and favorable intentions about colorectal cancer screening. 31
Both councils suggested that the neighborhood and built environment are directly intertwined with health care access and quality especially in rural areas where limited transportation acts as a physical barrier to access. Telehealth was mentioned as a potential strategy to increase access to care. Relating to the patient-centric dimension, ability to reach, and the system-centric dimension, availability and accommodation, telehealth has been shown to increase access to specialist care which is significant because rural areas have fewer available specialists.11,12,27,32 One RAC member discussed their affiliated organization’s efforts to implement telehealth initiatives but stated that they are observing a slower uptake of telehealth in rural areas. Limited access to broadband can serve as a barrier to the implementation of telehealth in rural areas and should be studied further in rural communities. 32
As suggested during interviews, individuals in rural areas may be reluctant to engage in preventive measures such as cancer screenings. Patients are still reluctant to seek health care unless they have chronic conditions. Individuals living in rural areas are nearly twice as likely to exhibit health care avoidance behaviors than those residing in metropolitan areas. 30 Each barrier discussed in this paper, including lack of transportation, education, providers, insurance, etc. contributes to the increased prevalence of health care avoidance in rural areas.30,33 Racial and ethnic minority groups continue to underutilize screening 29 despite screening serving as the most effective tool for reducing cancer-related health disparities in rural areas as long as communities are provided with resources for any needed follow-up care for diagnosis and treatment. 29
The suggestion that fear and lack of education contribute to a lack of ability to reach, as defined under the patient-centric dimensions that contribute to inadequate access to care, resonated with RAC members. Improvement of cancer-related health disparities requires an acknowledgement of the impact of stigma as it relates to health care avoidance in rural areas because it has the capacity to undermine cancer prevention and control efforts.30,34 Additional factors mentioned that could potentially relate to the health-avoidance behavior were related to lack of patient insurance and issues with provider reimbursement. 30 This also intersects with the system-centric dimensions of availability and affordability. 11
Availability and accommodation are directly related to the prevalent transportation barriers in rural areas. 11 In addition to cancer resources needs, CAC members identified the need for improved access to behavioral and mental health services, and substance abuse services. Rural areas are significantly less likely to have accessible substance abuse treatment facilities and behavioral and mental health services compared with urban areas.35,36 According to the 2020 snapshot of the state of oncology workforce in the U.S. by the American Society of Clinical Oncology, 66% of rural counties do not have a practicing oncologist; currently 1 in 6 Americans live in rural areas, and 32 million Americans live in counties without an oncologist. 37 A CAC member suggested that support groups are a useful strategy to provide treatment and health information to newly cancer-diagnosed individuals living in rural areas. This strategy is important to consider because of the transportation barriers.29,38,39
When asked what strategies were most effective in disseminating cancer information and resources to communities, both councils mentioned a variety of methods, and suggested that the strategies need to be tailored to the specific needs and dimensions of a community. Strategies included the benefits of using media such as email, mail, television, and social media outlets, as well as establishing sustainable partnerships. Strong relationships with trusted community organizations increase rural community members’ ability to seek, ability to reach, and ability to perceive, which are all essential in combating cancer-related health disparities in rural areas.11,38 Current literature suggests that using a variety of strategies is most effective in increasing breadth of reach. 40 Some council members discussed how they specifically adapt their efforts to the needs of the community. For example, some suggested that in-person trainings and educational programs were most effective for rural communities. Research Advisory Council members stated that they found trainings, webinars, and collaboration/partnerships with other organizations to be effective strategies in disseminating cancer information. However, due to the COVID pandemic, strategies had to be adapted to web-based formats as an alternative to in-person gatherings.
Mini grants can be used as a tool for improving cancer-related health disparities through the system-centric dimension of availability and accommodation by improving capacity building for implementation of EBIs in rural areas.11,16,39 Both CAC and RAC members provided their input on the effective recruitment of CHIP mini-grant applicants. The most commonly identified barrier to effective recruitment of applicants was a lack of awareness. Direct community engagement increases the reach of recruitment efforts because it allows for trust building and opens lines of communication with community leaders. Community Advisory Council members suggested that a clear and unambiguous process is essential for recruitment of applicants. 38 Research Advisory Council members stressed the importance of providing technical support throughout the application process and grant implementation period. This will help applicants who may feel overwhelmed by grant demands in addition to their current workload. 41
We believe that creating separate CAC and RAC was a sound decision as each council was new and working initially to establish their roles. It also is important to note that we also were encouraged by interactions between the two councils that occurred in the planning of the community mini-grants program and on webinars with grantees. Just as there are surmountable differences among different academic disciplines, differences in background, perspective, and worldview have the capacity to enrich the overall program by encouraging the RAC and CAC to interact. Indeed, we have written extensively on community-based participatory research (CBPR) as a model and paradigm for connecting interdisciplinary and translational research.42–44 We will need to do both in order to address large disparities that have been exacerbated by the Covid 19 pandemic.45–48
Limitations and Conclusions
This study has limitations. Interview data are from a small, highly selected sample of individuals advising on one cancer grant in one state. Generalizability to other populations or cancer network grants should be done with caution. However, the important input provided by council members is guiding the collaborative, community-engaged work of the grant network and strategies for reaching more rural and underserved populations across the state. Tailoring cancer prevention and control efforts to specific communities requires individualized assessments of the specific dimensions of access to care relating to that community. 31 While rural communities have many similarities, understanding each community is necessary for effectively addressing cancer-related health disparities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the University of South Carolina Magellan Scholar Award Program and the South Carolina Cancer Prevention and Control Research Network supported by Cooperative Agreement Number (U48 DP006401) from the Centers for Disease Control and Prevention. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Ethical Approval
In accordance with University of South Carolina IRB guidelines, CITI training modules were completed prior to the initiation of any research with human subjects.