
Abstract
This cross-sectional study was conducted in 2019 on 204 postmenopausal women aged 45–55 years who referred to Yazd health centers to determine the predictors in initiating and sustaining nutritional behaviors to deal with menopausal symptoms based on the multi-theory model (MTM). The participants were required to complete the demographic information questionnaire and a researcher-made questionnaire over the effective nutritional behaviors in menopause based on the MTM. The data were summarized and analyzed using SPSS 18 and AMOS23 by running descriptive indicators and path analysis. Behavioral confidence (β = 0.61, P < 0.001) had a higher predictive power in initiating a nutritional behavior compared to the changes in the physical environment (β = 0.13, P < 0.05) and participatory dialogue (β = 0. 10, p < 0.05). Among the behavior-related constructs, only emotional transformation (β = 0.78, P < 0.001) could predict the behavioral sustaining. A positive and significant association was observed between nutritional behavior sustaining and quality of life (β = −0.41, P < 0.001). The MTM is an appropriate model for predicting the initiation and sustaining of the nutritional behaviors in dealing with menopause. The behavioral confidence, changes in physical environment, and participatory dialogue constructs played a significant role in predicting the initiation of behavior. The emotional transformation construct was also an important predictor in maintaining nutritional behaviors to deal with menopausal symptoms. So, future researchers are recommended to conduct MTM-based investigations according to the predictive constructs among menopausal women.
All women will experience menopause as a natural phenomenon and one of the evolutionary stages in their lives. The symptoms of this period can affect women's quality of life 1 and weaken their sense of well-being. 2 Natural menopause is defined as the permanent cessation of the menstrual cycle due to the loss of ovarian follicle activity diagnosed after 12 months of menstruation cessation. 3 Women spend one-third of their lives in menopause. The population of postmenopausal women in Iran is expected to reach 5 million by 2021. 4
The onset of menopause in women is accompanied by the following symptoms: hot flashes, sweating, palpitations, sleep disturbances, irritability, lethargy, depressed mood, forgetfulness, decreased libido, depression, vaginal dryness, painful intercourse, urinary symptoms, decreased memory, reduced concentration, restlessness, as well as joint and bone problems. During this period, gradual changes occur in bone metabolism, resulting in increased bone fractures. 5 Increased population of the elderly in Iran, the prevalence of various health problems, and menopausal symptoms can affect postmenopausal women's occupational status, social activity, enjoyment of life, leisure, sleep, quality of life, and health. All these problems are closely related to a person's nutritional behavior and lifestyle. Considering that special attention should be paid to women's health in this period of life, their appropriate nutritional behaviors should be maintained and promoted. 6 Women’s nutritional needs vary based on different factors such as age, socioeconomic status, culture, and developmental stages. 7
Hot flashes are the most common complication of menopause and women's most frequent reason to visit a doctor with a significant impact on the quality of life. 8 Hot flashes disrupt the sleep cycle and cause sleep deprivation, which may lead to mental illnesses, including depression. 9 In many studies, soy consumption decreased hot flashes during menopause.10–13 Reduced sugar intake and food consumption at specific times can also play an important role in reducing hot flashes during menopause. Evidence suggests that caffeinated substances (such as tea and coffee), spicy spices, and alcohol can exacerbate hot flashes.14,15 A high-fat diet is also associated with obesity and an increased risk of breast cancer during menopause. 16 However, regular consumption of fruits and vegetables during menopause is correlated with a reduction in symptoms of this period. 17
Menopausal problems cause significant stress not only on women, but also on the health care system. 18 One of the best ways to control menopause complications and improve quality of life in women is to design related interventions and educational programs. Application of behavioral models and theories in health education and health promotion predicts and changes personal, interpersonal, and evidence-based group behaviors. As a result, effective planning can be done by predicting factors related to the occurrence and change of behaviors in different cultures. 19
In this regard, the multi-theory model (MTM) of behavior change, designed by Sharma, is among the effective and efficient models. It is an effective model with flexible constructs applicable to a variety of behaviors (repetitive and long-term behaviors as well as behaviors that are performed once) and in different cultures. The MTM has two important parts: (1) Initiation of behavior change and (2) Sustaining of the behavior.
There are three constructs for initiation: (1) participatory dialogue in which advantages of indulging in a changed behavior outweigh its disadvantages; (2) behavioral confidence, which is somewhat similar to self-efficacy because the ability to perform the behavior is partly internal but also can come from external sources and this construct is a projection of your sureness to perform a health behavior change in the future not in the present; (3) changes to the physical environment that its conceptualization pertains only to the “physical” and not the social environment and entails making changes to obtain ability, availability, accessibility, convenience, and readiness of resources.
There are three constructs for sustenance: (1) emotional transformation that relies on the individual’s ability to guide his feelings towards a goal and not succumbing to self-doubt; (2) practice for change entails constantly thinking about the health behavior change and making mid-term rectifications to one’s strategy, overcoming barriers, and remaining focused on health behavior change; (3) changes in social environment that entail establishing relationships to help goal attainment. This change in social environment can be natural or artificial. 20
In order to implement educational interventions aimed at improving the quality of life during menopause, factors associated with initiating and maintaining nutritional behaviors should be determined. These factors are important in controlling menopausal complications; so, the present study targeted at identifying the predictors in initiating and sustaining nutritional behaviors to deal with menopausal symptoms based on MTM.
Methods
Study Design and Participants
This cross-sectional study was conducted in Yazd, located in central Iran in 2019. To conduct this research, 204 postmenopausal women who referred to Yazd health centers and met the inclusion criteria were investigated. The eligible criteria to enter the study included: passing at least one year and a maximum of five years from the menopause, having natural menopause, having no physical illnesses or impaired consciousness, being within the age range of 45–55 years, having no addiction (according to the participants' self-report), having willingness to participate in the study, and signing the written form of conscious consent. In the path analysis studies, at least 10 participants are required for each parameter. 21 Considering loss of samples, 204 people were recruited using the stratified method. To this end, a list of health centers in Yazd City was prepared. The centers were divided into three categories of poor, moderate, and good based on the socio-economic status of the population covered by them. Later, two centers were randomly selected from each category. The list of 45–55 year-old women under the auspices of the mentioned centers was prepared. In the next stage, 34 people who met the inclusion criteria were selected from each center by simple random sampling.
Instrument
Data collection tool was a researcher-designed questionnaire with two sections. It takes 25–30 minutes for completing questionnaire by menopausal women. The first section was associated with assessment of demographic variables (included 26 items about the women's age, age at last menstrual period, age at first menstrual period, age at first pregnancy, age at last pregnancy, age of marriage, menopausal age of first-degree relatives, regularity or irregularity of the menstrual cycles, education, occupation, income, weight, and height).
The second section was associated with assessment of MTM constructs. The researcher-made nutritional behavior questionnaire was designed based on the MTM. This questionnaire included a total of 152 questions dealing with:1) initiation of behavioral change, containing three constructs of participatory dialogue, behavioral confidence, and changes in the physical environment; and 2) behavior sustaining , including three constructs of emotional transformation, practice for change, and changes in the social environment.
Advantages component of participatory dialogue were assessed with 37 questions, for example “If I reduce spicy food, I will have less hot flashes” The choices ranged from not at all (0), to some extent (1), very much (2). The scores for each question were summed to obtain a total possible score for advantages (ranging from 0 to 74 units). Disadvantages component of participatory dialogue were assessed with the 36 questions, for example “If I want to use soy in food, my family will not eat the food because of bad smelling. The choices ranged from not at all (0), to some extent (1), very much (2). The scores for each question were summed to obtain a total possible score for disadvantages (ranging from 0 to 72 units). We subtracted disadvantages score from advantages scores to calculate participatory dialogue construct score. The second construct, behavioral confidence was assessed with nine questions. For example, “I can reduce coffee and tea even if it is unpleasant for me”. The choices ranged from I am not sure at all (0), I am sure to some extent (1), I am completely sure (2). The scores for each question were summed to obtain a total possible score for behavioral confidence (ranging from 0 to 18 units). Third construct in initiation of behavior was change in physical environment which was assessed with four questions, For example, “I can set a plan for eating food”. The choices ranged from I am not sure at all (0), I am sure to some extent (1), I am completely sure (2). The scores for each question were summed to obtain a total possible score for behavioral confidence (ranging from 0 to 8 units).
First construct in sustaining behavior was emotional transformation which was assessed with 27 questions, For example, “I can overcome my doubts about not drinking hot drinks”. The choices ranged from I am not sure at all (0), I am sure to some extent (1), I am completely sure (2). The scores for each question were summed to obtain a total possible score for behavioral confidence (ranging from 0 to 54 units).
Second construct in sustaining behavior was practice for change which was assessed with 16 questions, For example, “I can write it down in my diary for comments on how much water I drink”. The choices ranged from I am not sure at all (0), I am sure to some extent (1), I am completely sure (2). The scores for each question were summed to obtain a total possible score for behavioral confidence (ranging from 0 to 32 units).
Third construct in sustaining behavior was changes in the social environment which was assessed with 5 questions, For example, “I can get help from my family members to buy fruits and vegetables.” The choices ranged from I am not sure at all (0), I am sure to some extent (1), I am completely sure (2). The scores for each question were summed to obtain a total possible score for behavioral confidence (ranging from 0 to 10 units).
The content and face validity of this questionnaire was approved by 14 experts in the field of reproductive health and health education and health promotion. The questionnaire's reliability was also confirmed with an alpha coefficient of 0.89 by 21 postmenopausal women using the test-retest method in an interval of two weeks. In this study, Cronbach's alpha reliability coefficients for various construct scales ranged from 0.82 to 0.98, indicates an acceptable internal consistency (the detailed results are not shown but are available from the main investigator).
Statistical Analysis
After entering the data into SPSS 22, the relationships between variables were examined by path analysis model using the AMOS software version 23. Path analysis, an extension of a multiple regression model that allows simultaneous examination of the multiple responses, was used to estimate and evaluate the causal relationships in terms of the MTM.
Results
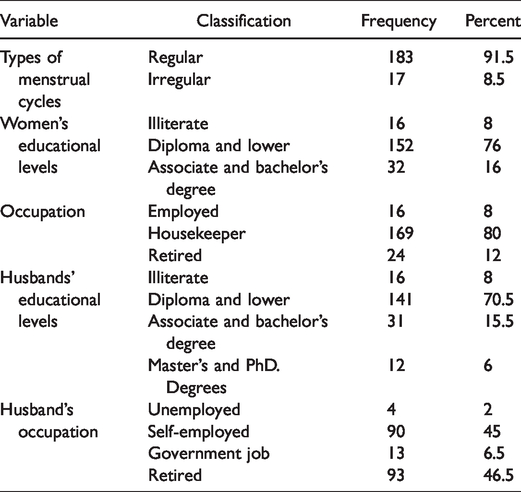
The individuals' mean (standard deviation) age, menopausal age, and menopausal age of first-degree relatives were 52.62 (2.03), 49.58 (2.04), and 49.44 (2.54), respectively. The mean (standard deviation) of the body mass index was 29.64 (4.29). The participants' other demographic information is reported in Table 1.
Frequency and Absolute Distribution of Research Units Based on Some Demographic Variables.
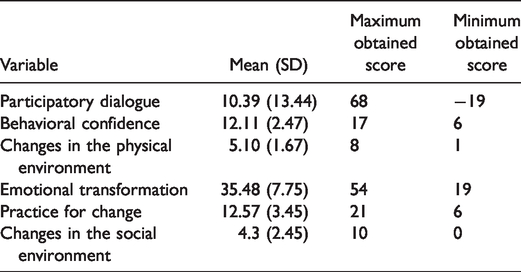
The mean, standard deviation, as well as minimum and maximum attainable scores from various constructs of the MTM are reported in Table 2.
Mean Score of MTM Constructs in Nutritional Behaviors.
Based on the path analysis, initiation of nutritional behaviors' constructs including participatory dialogue, behavioral confidence, and changes in the physical environment could predict initiation of the nutritional behaviors. The most predictive construct was behavioral confidence with a coefficient of 0.67. The emotional transformation was the most predictive construct of the behavioral maintenance with a coefficient of 0.78. Here, the overall model fit was used to assess the goodness-of-fit of the model to the observable data: goodness-of-fit index (GFI) was of 0.84, CFI was 0.79, and RMSEA was 0.281 (Table 3 and Figure 1).
Coefficients of the MTM Constructs in the Initiation and Maintenance of Nutritional Behaviors in Accordance With Menopause.
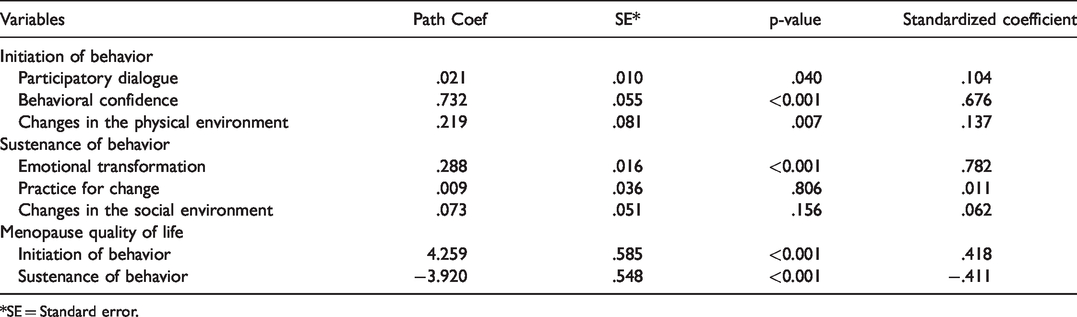
*SE = Standard error.
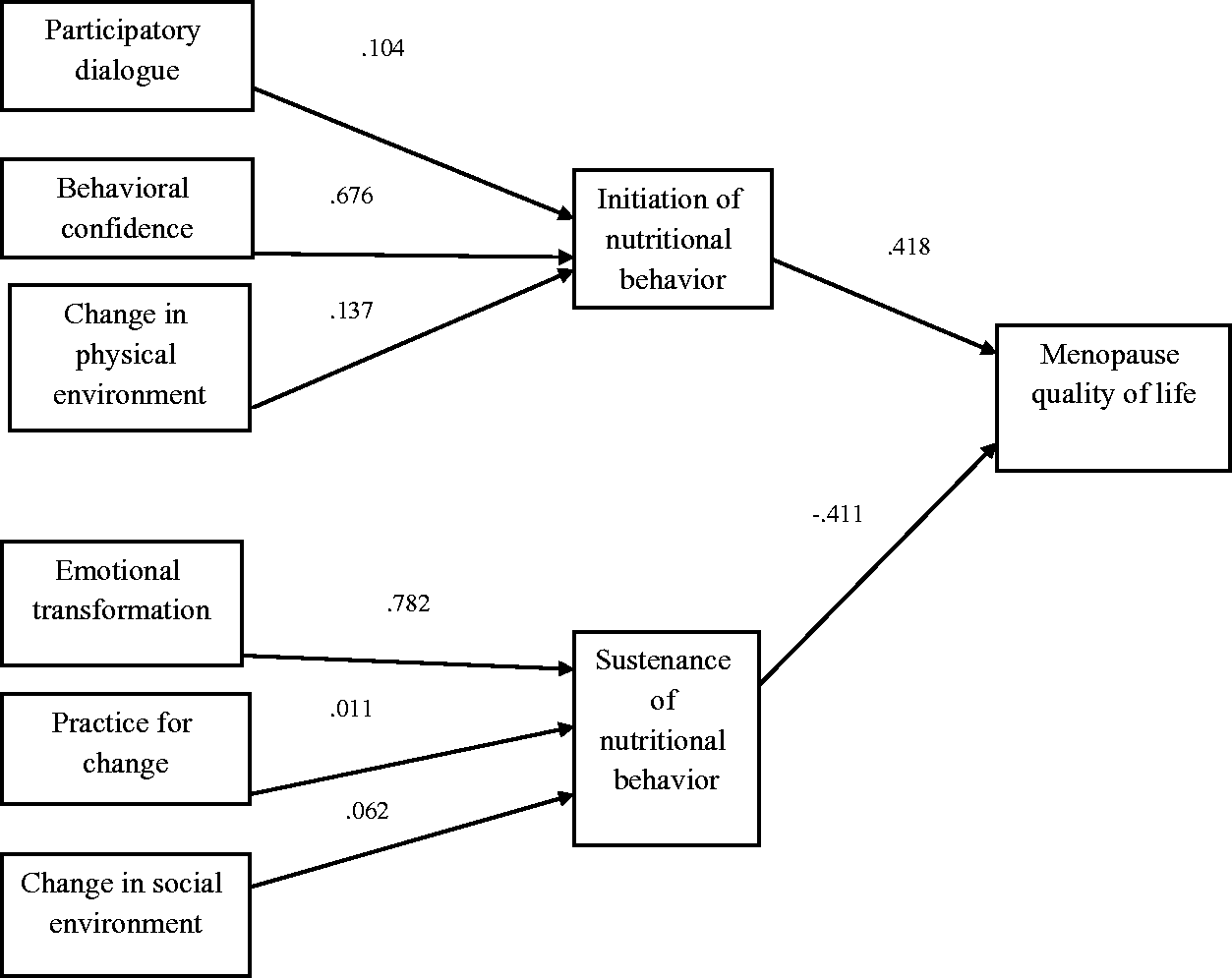
Path Analysis for the Effective Factors on Initiation and Sustenance of the Nutritional Behaviors and Quality of Life (Numbers Represent Standardized Coefficients of the Model).
Discussion
Results of the path analysis test showed that participatory dialogue, behavioral confidence, and changes in the physical environment had a direct and significant association with initiation of the nutritional behaviors in menopause with coefficients of 0.10, 0.67, and 0.13, respectively. Participatory dialogue reflects an individual's attitude toward the benefits and barriers of engaging in a behavior; individuals can move toward a behavior by evaluating it. This finding confirms the results of research by Karimy and et al. over the health belief model (HBM) constructs regarding the nutritional behaviors of pregnant women. They found that perceived barriers and perceived benefits predicted nutritional behaviors in pregnant women. 22 The study by Morowati et al. on self-care predictors in diabetic patients based on the developed model of the health belief also indicated similar results. According to this research, the pure interests construct predicted self-care behaviors. 23 However, a US study of predictors of consuming water instead of sugar sweetened drinks in university students based on the MTM reported that participatory dialogue construct could not predict initiation of the behavior change. 24 This discrepancy in the findings can be due to cultural differences and the type of target population. In other words, since students are educated and self-aware of the advantages and disadvantages of specific behavior, this construct could not play a role in their decision making to start the behavior. However, since postmenopausal women in the present study had lower levels of education, this construct could play a predictive role in initiating the behavior.
Behavioral confidence indicates a person's self-confidence to start behavior in the future. It implies that a person with behavioral confidence is highly probable to initiate a behavior in the future. The predictive power of the behavioral confidence was also confirmed in the literature. Brown et al. investigated the application of MTM in explaining the women's fruit and vegetable consumption behavior. 25 Sharma et al. examined the application of MTM in predicting the initiating and sustaining food consumption behaviors in small meals among students. 26 Dokun-Moweteet al. studied predictors of reducing salt consumption in people with high blood pressure 27 and Sharma et al. explained predictors of water consumption instead of sugar sweetened beverages in students. 24 In other words, behavioral confidence is an important predictive factor in starting a behavior. This result contradicts the findings of Kouhi et al. regarding predictors of hand hygiene in dental centers' staff based on the HBM. 28 It is also inconsistent with the results of the study by Dehdari and Farshad regarding predictors of occupational behaviors that prevent infection in sweepers according to the HBM constructs. 29 Such differences in the findings can be attributed to differences in the target groups, topics under investigation, and studied model.
Changes in the physical environment indicate an alteration in accessibility and adaptability of the facilities and environmental resources that help individuals to initiate a behavior. In the present study, changes in the physical environment predicted initiation of the behavior, which is in line with findings reported by Dokun-Mowete, 27 Brown, 25 and Sharma et al., 24 but contradicts with the study by Sharma et al. 26 The variety in the results can be attributed to the type of behavior under study: In Sharma et al., 24 the students' environmental accessibility to sweet drinks should be limited in the university campus. However, in Sharma et al.'s study, 26 the participants required regular environmental access to fresh fruits and vegetables at reasonable prices and in different neighborhoods to facilitate their regular consumption of fruits and vegetables. In the case of the behavior such as reducing the volume of meals that has no significant association with environmental access, changes in the physical environment construct does not have a predictive role.
In terms of behavioral sustaining, only the emotional transformation construct (with a coefficient of 0.78) had a direct and significant effect on maintaining nutritional behaviors with regard to menopause. The two constructs of practice for change and changes in the social environment had no significant effect on sustenance of nutritional behaviors in menopause.
Emotional transformation expresses the direction of one's emotions and feelings towards the continuation of a given behavior so that the person can be interested in the behavior and be encouraged to continue it. This finding is consistent with the studies by Sharma et al., 24 Brown et al., 25 and Sadeghi et al. 30 It seems that individuals who are more confident about their strengths and weaknesses have the right self-evaluation and possess a strong sense of self-worth. As a result, they can better manage their emotions and have more confidence in making decisions. Practice for change reflects the constant thinking about changing behavior and creating solutions to overcome obstacles and to focus on a healthy behavior change. The practice for change construct could not predict sustenance of behavior, which is in the same line with some studies,26,31 but contradicts some others.24,25
On the one hand, in the case of institutionalized and habitual behaviors (such as smoking and certain eating habits), the individuals may not be able to encourage themselves to continue the behavior with interest. On the other hand, when a behavior is neither very unpleasant nor deeply rooted, the individuals can get interested in the new behavior and encourage themselves to continue the new behavior.
Changes in the social environment represent the creation of social support in the environment and indicate the effect of family members, friends, and health care team support on continuing a behavior. We found that changes in the social environment could not predict sustenance ofbehavior , which is supported by Sharma, 24 Nahar et al. 31 in application of MTM in quitting smoking, and Nahar et al. 32 in application of MTM in stress controlling behaviors among university students. This finding is rejected by Brown et al. 25 and Morovati et al. 33 The discrepancy in the findings can be caused by cultural differences, because in a society like Iran, the supportive role of family members is emphasized in quitting addiction. Regarding consumption of fruits and vegetables, family members, especially spouses, play a significant supportive role in preparing and buying fruits and vegetables. However, in the present study, we were dealing with a set of mainly personal nutritional behaviors, such as reducing consumption of spicy spices, reducing intake of caffeinated substances, refraining from eating hot food and drink, drinking 6–8 glasses of water, and chewing food well. These behaviors are completely personal and supportive role of the family members may not be effective.
Based on the findings, initiation of the nutritional behaviors could not predict the high quality of life, but the sustenance of the nutritional behaviors predicted a higher quality of life. This can be justified by the fact that nutritional behaviors cannot control complications and improve quality of life until they are institutionalized in the individual. This is in the same line with the findings reported by Yousefzadeh 34 and Alizadeh. 35 However, Ozcan 36 acknowledged that nutritional behavior had a positive and significant relationship only with the reduction of hot flashes, but did not have any significant association with the overall quality of life. This finding contradicted our results because other aspects of lifestyle, such as physical activity and stress management had a more prominent role in improving quality of life than nutrition.
One of the limitations of this study was the lack of using more objective methods for measuring nutritional behaviors. Future researchers are recommended to carry out similar studies in different cultures using more objective tools and on a larger scale. Also data gathering was via Self-report questionnaire and various factors are involved in predicting the nutritional behavior of postmenopausal women that due to the use of this model; it was not possible to study other factors.
According to the MTM, behavioral confidence, changes in the physical environment, and participatory dialogue constructs had a significant role in predicting the initiation of a behavior. The emotional transformation construct was an important predictor in sustenance of nutritional behaviors in accordance with menopausal symptoms. So, in order to improve the quality of life in menopausal women, related educational interventions should be designed by an emphasis on the effective constructs including participatory dialogue, behavioral confidence, changes in the physical environment, and emotional transformation.
Footnotes
Acknowledgements
This manuscript is part of a PhD dissertation in Health Education and Promotion. We would like to appreciate all officials of Yazd University of Medical Sciences, especially the School of Health, who helped us to conduct this research.
Authors’ Note
The study was conducted in accordance with the Helsinki Declaration and ethical approval was obtained from the Ethics Committee of Shahid Sadoughi University of Medical Sciences (IR.SSU.SPH.REC.1397.137). Written informed consent was obtained from all participants before administration of the questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.