
Abstract
Background
Participation by patients in their own health care improves quality and safety. Question prompt lists (QPLs) can improve participation, particularly with doctors’ endorsement. Few data have explored doctors’ attitudes on these tools. We sought the experiences and attitudes of general practitioners and other specialists toward patient question asking and QPLs in their practice.
Methods
In-depth, semistructured interviews and focus groups with purposively selected Australian doctors were conducted. Interview guides were used to explore doctors’ experiences of patient question asking, patients’ lists, and a sample QPL created using an Australian government-funded online tool, “Question Builder.” Recordings were transcribed verbatim and data analyzed thematically using the method by Braun and Clarke.
Results
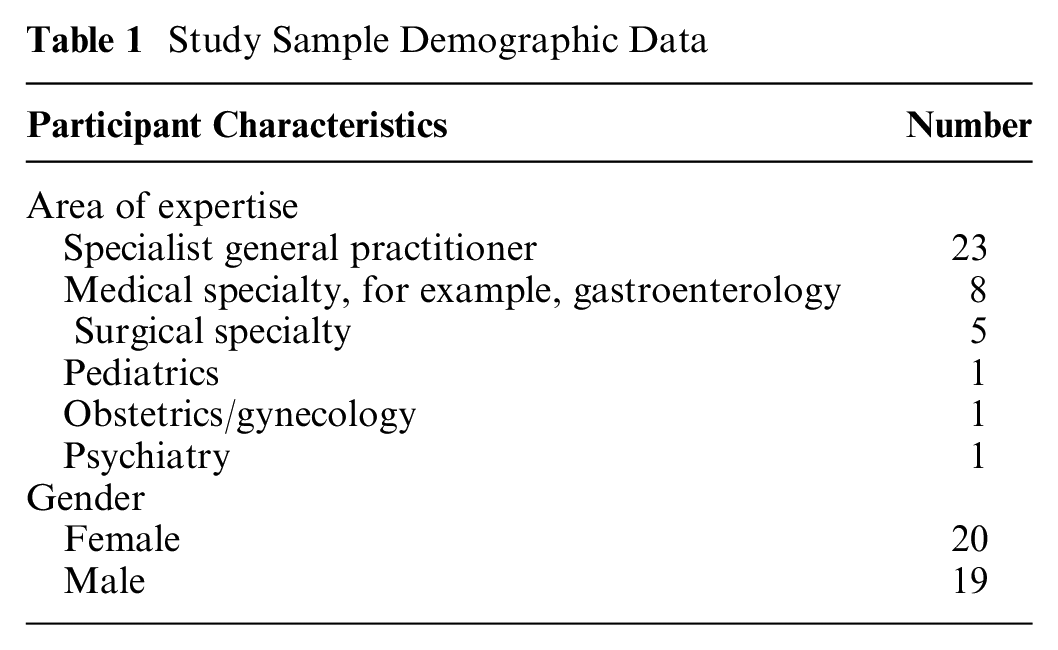
Focus groups with 3 to 9 participants and a further 17 individual interviews were conducted. There was a total of 40 participants, 23 general practitioners and 17 other specialists (e.g., physicians, surgeons, pediatricians). Our analysis was summarized into several themes. 1) The doctors expected, encouraged, and had significant experience of patient question asking and patients’ lists. They described many barriers for patients and their efforts to ensure patients had the information they needed. 2) The doctors felt responsible for creating an environment conducive to patient question asking, the delivery of answers, having strategies for unanswered questions, and balancing the agendas of both parties in the consultation. 3) Structured QPLs that prepared patients and facilitated the consultation agenda were viewed positively. The degree of time pressures participating doctors experienced in their context had a strong influence on how they responded to the sample QPL.
Conclusion
Doctors in this study expected patients to ask questions and endorsed the benefits of QPLs. However, there were more diverse views about the feasibility of implementing them in practice. Designing QPLs to fit within current workflows, via more succinct and tailored designs, may result in wider doctor acceptance and endorsement, hence maximizing the benefits of QPLs with improved patient participation and patient safety.
Health care provision, which reflects the personal preferences and values of the patient, is described as person-centered care. 1 Person-centered care is considered in international standards to be aligned with high-quality care and an essential part of improving patient safety.1–4 This can be facilitated through encouraging patient question asking to assist people in obtaining the information they need to participate in decisions about their health care. Shared decision making (SDM) facilitates patient-centered health care decisions and values-based care,2,5 with multiple campaigns now including strategies to encourage question asking as part of SDM and patient safety initiatives.6–8 For example, the Agency for Healthcare Research and Quality’s (AHRQ’s) “SHARE Approach” specifically trains health care professionals in how to engage patients in this process. 9
There are many reasons why patients ask, or want to ask, their doctor a question. Patient question asking in medical consultations serves a variety of purposes from personal social interaction to in-depth detail about the benefits and harms of possible treatments.2,10,11 To facilitate this, lists have been used in a variety of ways. In their most basic form, there are patients’ agenda lists, created by patients prior to a consultation. Patient agenda lists can include requests, such as for a prescription or a referral, and/or a list of problems and issues they want to raise in the consultation. 12 A second type, described in the literature as patient question prompt lists (PQPLs), involves question lists created by patients in response to a prompt before they go to the doctor with questions they have conceived (e.g., “When is my next appointment?”). 13 For clarity, in this article, we will refer to PQPLs as patient-generated question lists as there may not be a specific prompt. A third type is a question prompt list (QPL), which is a prepared list of questions developed by agencies or health care teams. Patients use a QPL by selecting from a predetermined list of questions those that they may want to ask in a consultation. 13 Examples of QPLs are the AHRQ “Question Builder” and the Australian adaptation of this tool.14,15
QPLs can also be described as an example of decision support tools for assisting patients when making decisions about their health care.13,16,17 Other decision support tools or interventions include decision aids and patient training. 18 Their purpose is to support patients and enhance SDM with their doctor. 13 QPLs have been shown to have benefits for both patients and doctors, to increase patient question asking and improving the quality of information that doctors provide.2,13 There is an abundance of QPLs available to patients, many of which are easily accessible online. However, the QPLs are of variable quality, and very few have been evaluated. 19 There is evidence that QPL tools are being used and that questions that facilitate SDM (e.g., “What are my options?” 2 ) are more likely to be prioritized by users. 20 Available QPLs contain a variety of types of questions reflecting the many reasons questions are asked in consultations.10,20
One important aspect in implementing QPLs into clinical practice is that they are most beneficial when endorsed by the doctor.6,13,21 In addition, stakeholder engagement and user-centered design are important in the development of such tools. 22 However, there are few data on the experiences and attitudes of doctors toward patients asking questions or their thoughts and experiences of different patient lists and QPLs in particular.12,23 This study sought to address this gap in understanding doctors’ experiences and attitudes toward patient question asking, agenda and patient-generated question lists, and QPLs in the context of their consultations. Data from this vital stakeholder group could be used to improve uptake and more successful implementation of QPLs.
Methods
Study Sample/and Recruitment
Ethics approval for the project was sought and granted by the University of Sydney Human Research Ethics Committee.
The study team purposively recruited a variety of specialist doctors, including general practitioners (GPs), which is a specialty in Australia. We will use the term GPs when referring to specialist and trainee GPs and other specialists for the remaining participants. We recruited GPs from established evidence-based practice meetings at 4 clinics in New South Wales, Australia. 24 One clinic was located at a regional center and 3 in metropolitan practices. Each of the focus groups consisted of doctors working in the same practice, and all groups included 1 to 3 doctors undergoing GP training. One GP, unable to attend their focus group, was interviewed individually.
The other participating specialists were purposively selected for the study from a variety of different specialty areas (e.g., surgeons, medical specialists, psychiatrists). They were identified by the research team as clinical leaders affiliated with the University of Sydney and were recruited via email to their university email address inviting them to participate in interviews. An interview methodology was prioritized for this group given that Australian specialists often work in solo practice and later on account of the coronavirus disease 2019 (COVID-19) pandemic. 25 Recruitment continued to achieve a range of other specialties and a balance of gender representation in both medical and surgical specialties as well as to achieve thematic saturation.
Study Procedure
Semistructured interview and focus group questions were devised using concepts from existing literature about question asking. They sought participants’ experiences, combining concepts of phenomenology and the idea of user-centered design, to improve understanding and potential implementation. The focus groups and telephone interviews were recorded with the consent of all participants. MCT (moderator) and DMM (observer)—both of whom have conducted focus groups for previous research—conducted 3 focus groups together. Preliminary impressions were exchanged after each session. MCT conducted the regional focus group and all interviews independently. Participants were asked about their experiences, thoughts, and feelings when patients ask questions in consultations and how they felt when patients come with a list of questions. We opened discussion by asking, “Can you tell us a bit about your experiences of patients asking question when they come to see you?” See Appendix A—Focus group and interview guides.
We presented participants with sample question lists created using Question Builder, an online QPL tool hosted on the Healthdirect Australia consumer website (https://www.healthdirect.gov.au/question-builder) 15 (Appendix B). Healthdirect is a government funded, not-for-profit organization providing consumer health information through a variety of platforms and services. Question Builder comprises general questions about health care, such as “Do I need any tests?” rather than disease-specific questions. Users complete 4 steps to create a list: 1) choosing appointment type, GP, or specialist for new issue/first visit or follow-up appointment; 2) choosing questions from a list of possible questions; 3) choosing some questions most important to them in case there is limited time in the consultation (prioritization step); and 4) choosing from a list of questions that the doctor may ask them that they may wish to prepare for before the appointment.
Sample lists were created by MCT based on previous analysis of Question Builder’s use. 20 Each list represented the most frequently chosen questions, the average list length, and the average number of questions prioritized by users. Participants in the study were presented with 2 sample QPLs applicable to their area of practice, one for a new symptom/initial visit, the other with questions designed for follow-up consultations. The 2 lists for GPs had 22 “New symptoms” or 18 “Follow-up” questions, each with 4 and 2 prioritized questions, respectively. The other specialist lists had 38 “First visit” or 22 “Follow-up” questions with 8 and 4 prioritized questions, respectively. Prioritized questions were denoted with a star. Participants were initially given deidentified versions of the list for their response to the content prior to explaining Question Builder and continuing further discussion about the lists. Participants were asked about whether they would endorse the QPLs and/or recommend them to their patients.
All recordings of focus groups and interviews were transcribed verbatim using a secure external transcription service.
Analysis and Reflexivity
Initial coding of a sample of transcripts was undertaken by MCT and DMM. MCT is a GP and PhD candidate which was disclosed to all participants. MCT continuously reflected and discussed with the other authors on how these characteristics may have shaped the interviews and analysis. During focus groups and interviews, there was a concerted effort not to make assumptions, instead using probing questions to clarify participants’ statements. To avoid seeking to “confirm” conscious or unconscious preconceptions, we approached coding from an inductive orientation using thematic analysis. 26 In addition, we used double coding and discussion to refine and develop themes, and a third author, HLS, resolved disagreements. Initial thematic ideas were discussed by all authors prior to MCT coding the remaining transcripts. The funding sources that enabled the completion of this project played no role in the study.
Results
GP Focus Groups
Four focus groups took place over the course of a 6-week period mid-2019 involving 22 GPs. The focus groups ranged in size from 3 to 9 GPs, and each focus group ran from 45 to 60 minutes in length (average 56 minutes). As already noted, there was one 16-minute face-to-face interview with a GP participant.
Specialist Interviews
Email invitations were sent to 43 specialists between November 2019 and February 2020, 5 emails were undeliverable, and 16 specialists agreed to participate. All participants chose to be interviewed by telephone. The average length of interviews was 23 minutes and ranged from 16 to 36 minutes.
Pooled demographic data for participants are presented in Table 1.
Study Sample Demographic Data
Theme Overview
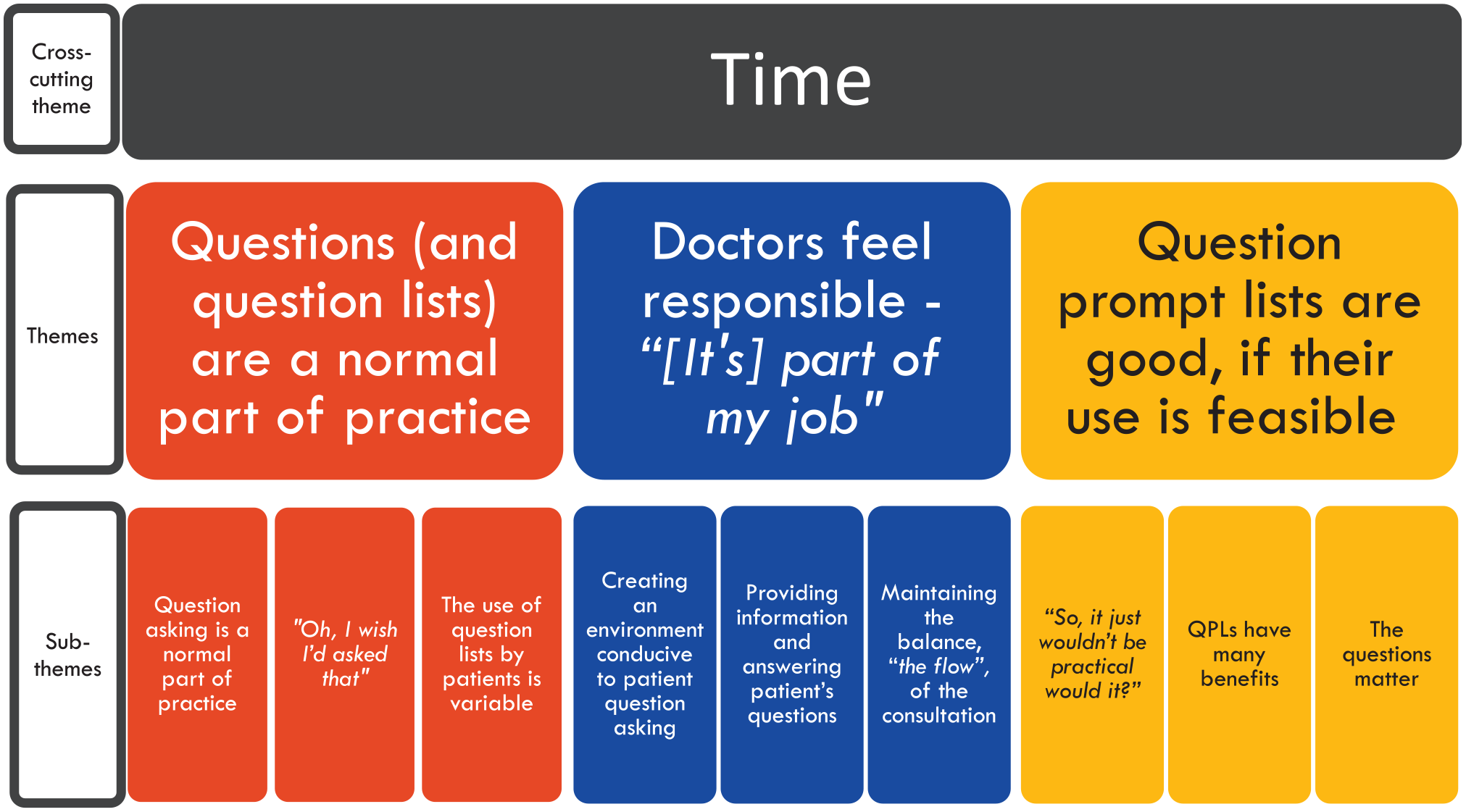
Participants’ narratives reflected that patients’ questions were a part of good-quality clinical care and that QPLs could facilitate patient question asking. The doctors in our study felt a responsibility to create and maintain an environment where patients’ questions could be asked and answered. They expressed the need to be able to fulfill their responsibilities to the patient in front of them and those in the waiting room. Their experiences and feelings about QPLs were heavily influenced by the amount of time and resources available to them. QPLs were acceptable to our participants, where they were feasible within the constraints of consultations. See Figure 1 for the thematic structure. Full quotes for each theme can be found in Appendix C.
Themes.
Time as a Cross-Cutting Theme
The importance of time was brought up frequently and in many contexts by all participants that it is described in this article as a cross-cutting theme. When discussing question asking by patients, both specialists and GPs reported the importance of time to “give space” to what they saw as a “normal part of practice.” The impact of time on how question asking is managed by participants is discussed further in theme 2, “Doctors feel responsible.” Reactions to QPLs were mostly aligned with the amount of time participants had in their practice to conduct their consultations. Those practicing in contexts that allowed for longer consultations, up to an hour, acknowledged that their context facilitated question asking and were less concerned about the impact of the sample QPLs.
Theme 1: Questions (and Question Lists) Are a Normal Part of Practice
Subtheme 1.1: Question asking is a normal part of practice
Patient question asking was considered by participants to be part of routine clinical care, and they perceived that “everyone comes with a question” (GP4). There was “a huge spectrum” (GP18) to the amount of question asking by patients. Our participants expected patients to ask them questions and were unsurprised by a patient’s lists of issues and/or questions. Question asking was described as “a good thing” (GP2) by participants.
Patients’ questions appeared to have several roles according to participants: they were part of the social interaction, were a means of obtaining information, can assist in decision making, can help establish priorities, and can be used as a checklist. In general, our specialists thought patients “should be asking more questions” (S13) or “don’t ask as much as they should” (S5). GP participants also expressed that this was especially important when significant decisions were being made: “It’s part of the consultation process I guess to help them to understand what it is they come in with and how we understand that from a medical point of view. Questions are a good thing” (GP2). GP participants were acutely aware that “there’s a hidden question always” (GP1).
Subtheme 1.2: “Oh, I wish I’d asked that.”
“It depends on a lot of factors” (S7) as to whether all questions are asked during a consultation. The patient–doctor relationship, the patient’s familiarity with medical consultations, the acuity of the medical problem, individual patient and doctor factors, and time factors were all seen as potential barriers to patient question asking. “People often feel a sense that they’re being processed, and they’ve got to get in and out quickly, and that their questions might be unwelcome” (S1).
Patient factors participants described that influence question asking in consultations included the age of patients (“older people probably ask less questions” [S13]); language barriers (“I think people with non-English-speaking background perhaps probably ask less questions” [S13]); personality, such as “people who are too shy, or too scared to ask questions” (GP12); and even geography (“I used to work in Canberra. The Canberrans always asked questions” [S13]).
Doctor factors and the patient–doctor relationship were also cited as reasons for variation in question-asking behaviors: “Number one is probably the relationship they have with the individual clinician” (S14). Several acknowledged power imbalance: “The white coat is another barrier” (S3). Some reflected that their own acceptance of patient questions was a factor altering the likelihood of patients asking questions, such as “if someone’s burnt out they’re probably not keen on questions” (GP17). Although the concept of patient fear of asking the wrong question or losing face was noted, many participants expressed that “there’s really no such thing as a silly question” (S15).
People new to the role of being a patient were described as less likely to ask questions. Some of this was attributed to the fact they “wouldn’t have that much insight to how the consult was structured” (GP14), or “patients are just too overwhelmed to start with” (S2). The corollary of this was that more questions tended to be asked when “they’ve had a little bit of a chance to process things” (S6). Acute issues, serious diagnoses, and uncomfortable topics were cited as reasons why someone may not ask questions.
Time and the question’s relevance to participants were also a factor: “Sometimes they’re really operational questions. . . . They seem like really minor things, but that sort of stuff can take up a lot of time” (GP4).
Subtheme 1.3: Using question lists in consultations
Our participants had varied experiences of patients bringing different types of lists to consultations: “they bring in a question, . . . they bring in lists” (GP2). Agenda lists were viewed as one aid used by patients to give them “that sense of control” (GP6). GPs described that they saw fewer patient-generated question lists while specialists frequently had patients come with a list of questions rather than agenda lists: “It’s usually a lot of questions” (S13). Both GPs and specialists saw benefits for themselves and patients in the use of question lists: I quite like it when they come with a list of questions ‘cause I know that they’re going to walk out satisfied knowing that we’ve answered all their questions and they’re not going to walk out the door, “Oh, I should’ve asked that question.” (S6) It (a question list) actually makes it quite good because you know by the end, . . . that their priorities and our priorities are dealt with. (GP19)
Theme 2: Doctors Feel Responsible—“(It’s) Part of My Job”
In the time-pressured environment of medical consultations, participants described the many responsibilities they have to their patients to ensure that patients could ask questions and get the answers they needed while maintaining “that flow” (GP22) of the consultation (GP2, GP17, S1).
Subtheme 2.1: Responsibility to create an environment conducive to patient question asking
The doctors in our study gave accounts of the substantial burden of ensuring patients can ask questions and have their questions answered where “consultations are time limited” (S1) and time was “a barrier” (S1). Some described trying to shield patients: “I mean part of my job I suppose is to try to minimise those barriers . . . give people the sense that I’m not pushing for time” (S1). “I think that it is respectful, to attempt to answer their question” (GP2).
Many participants had a myriad of approaches or “developed a drill” (S10) to encourage patients to ask questions and present their agenda for the consultation. “Before we start with the problem, let’s list them all” (GP19). “At the end of the conversation, ‘Do you have any questions?’” (GP13) was a common example from participants, which invites patient questions, but since it is frequently asked at the end of a consultation, it may also signal that the consultation is concluding.
Subtheme 2.2: Responsibility to provide information/answer patient questions
Our participants spoke of answering patients’ questions as a core function of their role: “It’s a question of my skill sets to be able to ensure that the patient will walk out feeling that they’ve got their questions answered” (S3). However, specialists described that patient questions were not always required: “Do they have lots of questions of those consultations? They usually don’t. I guess it’s that because I’m pre-empting them.” (S8)
They had various strategies they employed to help with information exchange both during and following consultations: “I do encourage people to use lists. I think they are good things” (S3).
Some doctors spoke of themselves as members of the clinical team and just one source of information patients could access if they had questions: “Our job is to help them get answers . . . so that’s part of the philosophy of the service that we provide” (S9). “Managing what you can and get them back for another time” (GP17) and the ability to call or “just email me questions” after a consultation were services offered by many.
Participants gave no examples of discomfort when dealing with patient questions even if “sometimes we don’t know, and it’s having some level of comfort of being able to say, ‘I’m not sure of the answer to that question’” (GP2).
Subtheme 2.3: Responsibility for maintaining the balance (or “that flow” of the consultation)
In this subtheme, focusing on responsibility for maintaining consultation “flow,” we describe how participants felt that they are best placed to make the necessary adjustments during consultations to facilitate patient question asking.
While most regarded patient agenda and patient-generated question lists as a normal part of practice, strategies regarding lists were learned: “I’ve definitely become ‘I get the list at the beginning person’” (GP5). They described that this helped establish the consultation agenda and achieve maximum benefit for both parties in the available time: “If I don’t say ‘Let’s get the list out’ at the beginning then it comes out 12 minutes in and then we’ve only covered half of it” (GP6). One of the crucial reasons given for this was to “avoid that ‘doorknob’ question” (GP11) that came up as an issue in 3 of the GP focus groups. Managing the consultation agenda was required to avoid the situation where “they always leave the really important questions ’till last” (GP13).
Theme 3: Question Prompt Lists Are Good, if Their Use Is Feasible
Again, time had a significant influence across these subthemes. Participants who expressed fewer concerns about the impact of the sample QPLs tended to be those who also described having longer consultations than peers.
Subtheme 3.1: “So, it just wouldn’t be practical, would it?”
The initial reactions to the sample QPLs were often expressed in quite strong terms such as “heartsink,”“overwhelmed,” and “horrific.” The main cause of these first reactions seemed to stem from their impressions that such lists would be unfeasible to manage: “I think on the whole they’re great questions. The issue is time” (GP17).
There was considerable concern voiced regarding implementation: I’m not sure about rapport, where that would go? . . . it just takes away that flow of the consultation. (GP22)
After initially “rolling my eyes” (S8), some would “say ‘Let’s put this aside and let’s address all your concerns today,’ and I’d do it like a consultation that I would normally do” (GP2), “and then after I’ve done that, go through and check it off and make sure we haven’t missed anything” (S8). Others felt, “Well, you just have to sit down and go through it, don’t have much choice. You can’t not do it, so—yeah, you just do it” (S5).
Subtheme 3.2: QPLs have many benefits
Participants expressed that QPLs could facilitate question asking and that patients “might feel a bit more empowered to ask those questions” (S6). There were concerns that “the people most likely to need this information are the least likely to be able to use it easily” (S9). Prompting for patients and doctors was expressed as a potential benefit of the QPLs raised by several participants: “I guess this could be used as a prompt for them to figure out what they want to ask” (GP13). It was also suggested that lists such as these might be useful for improving patient safety like “aviation checklist style things to make sure that all the essential information has been given and appropriately retained” (S8).
An important potential benefit was expressed that QPLs might facilitate the consultation, “to make our time more efficient as well” (GP5). The section of the QPL with the list of “Questions that you might need to prepare for” 15 was well received with participants very positive about the concept of patients preparing for consultations, “anything that helps them to think about what they want to get out of limited consultation time is going to be beneficial” (S1).
Subtheme 3.3: The questions matter
The content of the QPLs was another consideration raised in participants’ assessment of the utility and relevance of the tool in practice: GP19: But, “Why am I feeling like this?” This isn’t going to save me time. GP18: It’s not specific enough.
Comparisons were made to whether these were the types of questions patients usually asked: “These are all reasonable questions, except the second one—‘Why do I feel like that?’ I’m not sure. I’ve never heard that one, I don’t think” (S5). Some mentioned that QPLs or specific questions had potential benefits for patient decision making and patient safety: “‘What are my treatment options?’ It absolutely is important for them to be asking what the alternatives are” (S2) and “Never assume that it’s all good ’cause no one called you. So, ‘How will I get my results?’ and, ‘What should I do if don’t get them?’ So that’s a good one” (S8).
Discussion
In this qualitative study with GPs and other specialist Australian doctors, we found that participants’ experiences and attitudes to patients asking questions, patients’ agenda lists, and patient-generated question lists are generally positive. GPs and other specialists welcomed and sought questions from their patients and considered that patient questions were a normal part of practice. They strived to create an atmosphere that was non-threatening and conducive to patient question asking with the provision of answers while balancing the agendas of both parties. We saw little evidence to support historic negative connotations toward question asking and patients’ lists.12,16 In fact, the doctors in this study expected and wanted patients to ask questions in consultations, and after an initial negative reaction to the length of the sample QPLs, they were generally viewed positively with benefits seen for patients and their own practice.
Participants scrutinized the questions provided by a QPL developed from Question Builder, an online tool hosted on the Healthdirect Australia consumer website, for feasibility, content, and the potential benefits of the QPLs. They described many questions as highly relevant, but not all saw the relevance of some questions to their practice. As well as the function of enabling patient question asking to get the information they need, QPLs were described as having additional potential benefits: helping patients prepare and therefore streamlining a consultation, as a tool for patient safety, and in assisting patients to prioritize issues. However, the time available in consultations and the perceived relevance of the questions in the QPL affected views on how they could be effectively implemented into clinical settings.
Overall, there was a strong sense that patients’ questions were a normal part of practice and there were many strategies in place for ensuring questions could be asked and patients could get the information they needed. Familiar patient agenda lists and patient-generated question lists had been incorporated into their “drill.” However, there was no strong sense of where QPLs would fit into practice. Participants expressed some concern about the feasibility of the Question Builder lists, particularly for those with shorter consultations, and the potential of QPLs to disrupt the “flow.”
Doctors use heuristics or “mental shortcuts” when making decisions in practice. 16 These are based on repeated encounters of discrete clinical scenarios/issues, in some cases through decades of practice in their specialty. The way that doctors conceptualize the place of question asking by patients in consultations is therefore likely to influence their endorsement of QPLs and incorporation into their usual practice. The QPLs did not fit participants’ current heuristics about how consultations are conducted. Prior to this study, there were no published data on provider attitudes to either version of the existing Question Builder tools, but previous research has found similar provider perceptions when implementing models and tools designed to increase SDM.18,27–29
International and national standards for safety and quality explicitly list patient involvement and SDM.1,3 Implementing strategies to improve SDM and patient safety in practice needs to involve both health care providers and those seeking health care. 18 QPLs are one tool shown to encourage participation through question asking, improve the information provided by doctors, and include patients in decisions about their health care.1,2,13,16 So while there are a vast number of available QPLs available directly to patients, 20 there needs to be consideration of how clinical practice and doctors’ heuristics might need to adjust to meet national standards. Furthermore, while some QPLs are focused on SDM,30,31 other QPLs that cover a broader range of purposes in consultations such as agenda setting or use as a checklist may need to align with different key points in existing heuristics to maximize endorsement and use.
Translating research evidence into clinical practice has been characterized as “notoriously difficult.” 32 Johnson and May’s review 32 suggested that modification of practice norms through education and the use of opinion leaders might be more successful in achieving behavior change than focusing on individual action. In the case of the adoption and acceptance of QPL use in practice, the opinions of leaders such as many of our participants may be the future agents of change. Endorsement by peak bodies such as specialist colleges and normalizing the use of QPLs with active reflection as part of quality improvement and continuing professional development may also establish these norms.
Strengths and Limitations
The strengths of this study include that this is the first published data we are aware of seeking views of doctors’ attitudes to QPLs currently available online to health care consumers. We interviewed doctors across a broad range of clinical expertise and from both metropolitan and regional locations. Our cohort also included trainees, which broadened the scope of opinions we received. There was considerable concordance of views across the focus groups and interviews, and thematic saturation was reached quickly. We sought additional doctors to ensure a mix of genders and practice specialties to ensure broader consistency across the profession.
It should be noted that focus groups were composed coworkers of each practice site. There is potential for practice hierarchies of supervisors over trainees and owners v. employees to have influenced the views expressed. These groups have been working together for some time, and there are likely to be entrenched group dynamics. However, they have also been critically appraising evidence summaries and are attuned to rapidly assessing the likely benefits and disadvantages of support tools in practice. It should be noted that all focus group participants were encouraged by the facilitators to voice their views.
A limitation of this study could be our study sample of doctors engaged in teaching and/or research. Our participants were purposively selected as opinion leaders and early adopters of clinical advances and not considered as representative of the likely breadth of opinions. The use of local opinion leaders is a beneficial part of implementation strategy. 29 Ascertaining if our leaders would endorse a modified version of Question Builder lists would be a key step for future implementation of such tools.
We also acknowledge the issues inherent in combining data from focus groups and interviews. Focus groups are likely to provide more interactive data between participants and higher ecological validity by using regular practice meeting time to discuss the research questions. 26 The focus groups were conducted face-to-face, where rapport and communication were likely to be quite different to achieve in comparison to the telephone interviews.
Conclusion
Patients’ question asking and the types of lists that doctors currently encounter in practice were acceptable and manageable. However, QPL examples needed to be designed to minimize disruption of the workflow and to be most useful within the available consultation time.
Future QPL tool development needs to consider the time constraints of clinical practice while maintaining benefits to both parties in the consultation. Efforts should be made to rationalize list length, be clear about where they fit in consultation workflow, and ensure their relevance to clinical settings. Patients using QPLs need clear instructions regarding preparation and expectations for consultations and how to prioritize their questions. Such adjustments may enhance their usability, acceptance, and endorsement by doctors and ultimately increase benefits to patient safety and patient experience of SDM in practice.
Supplemental Material
sj-docx-1-mdm-10.1177_0272989X211029579 – Supplemental material for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study
Supplemental material, sj-docx-1-mdm-10.1177_0272989X211029579 for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study by Marguerite Clare Tracy, Danielle Maree Muscat, Heather L. Shepherd and Lyndal Jane Trevena in Medical Decision Making
Supplemental Material
sj-docx-2-mdm-10.1177_0272989X211029579 – Supplemental material for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study
Supplemental material, sj-docx-2-mdm-10.1177_0272989X211029579 for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study by Marguerite Clare Tracy, Danielle Maree Muscat, Heather L. Shepherd and Lyndal Jane Trevena in Medical Decision Making
Supplemental Material
sj-docx-3-mdm-10.1177_0272989X211029579 – Supplemental material for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study
Supplemental material, sj-docx-3-mdm-10.1177_0272989X211029579 for Doctors’ Attitudes to Patient Question Asking, Patient-Generated Question Lists, and Question Prompt Lists: A Qualitative Study by Marguerite Clare Tracy, Danielle Maree Muscat, Heather L. Shepherd and Lyndal Jane Trevena in Medical Decision Making
Footnotes
Acknowledgements
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by a grant from the University of Sydney PhD research scholarship (SC2396) funded by Healthdirect Australia Ltd. and by the National Health and Medical Research Council of Australia through the Ask, Share, Know: Rapid Evidence for General Practice Decisions Centre for Research Excellence (grant 1106542). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.