
Abstract
Highlights
We explored expert knowledge and experience on how to successfully integrate shared decision making (SDM) and decision support tools into clinical practice guidelines (CPGs).
A combined development of CPGs and decision support tools was deemed essential; however, development processes often remain separate, with the CPG development group unaware of the decision support tool development group, and vice versa.
In addition to stating choice awareness in CPGs, participants highlighted the critical role of patient partners in considering SDM in CPG development, but resource issues and a culture that neglects patient involvement and SDM remain.
For CPG development groups to consider SDM and for health care professionals to practice it, things need to be as easy as possible.
This is a visual representation of the abstract.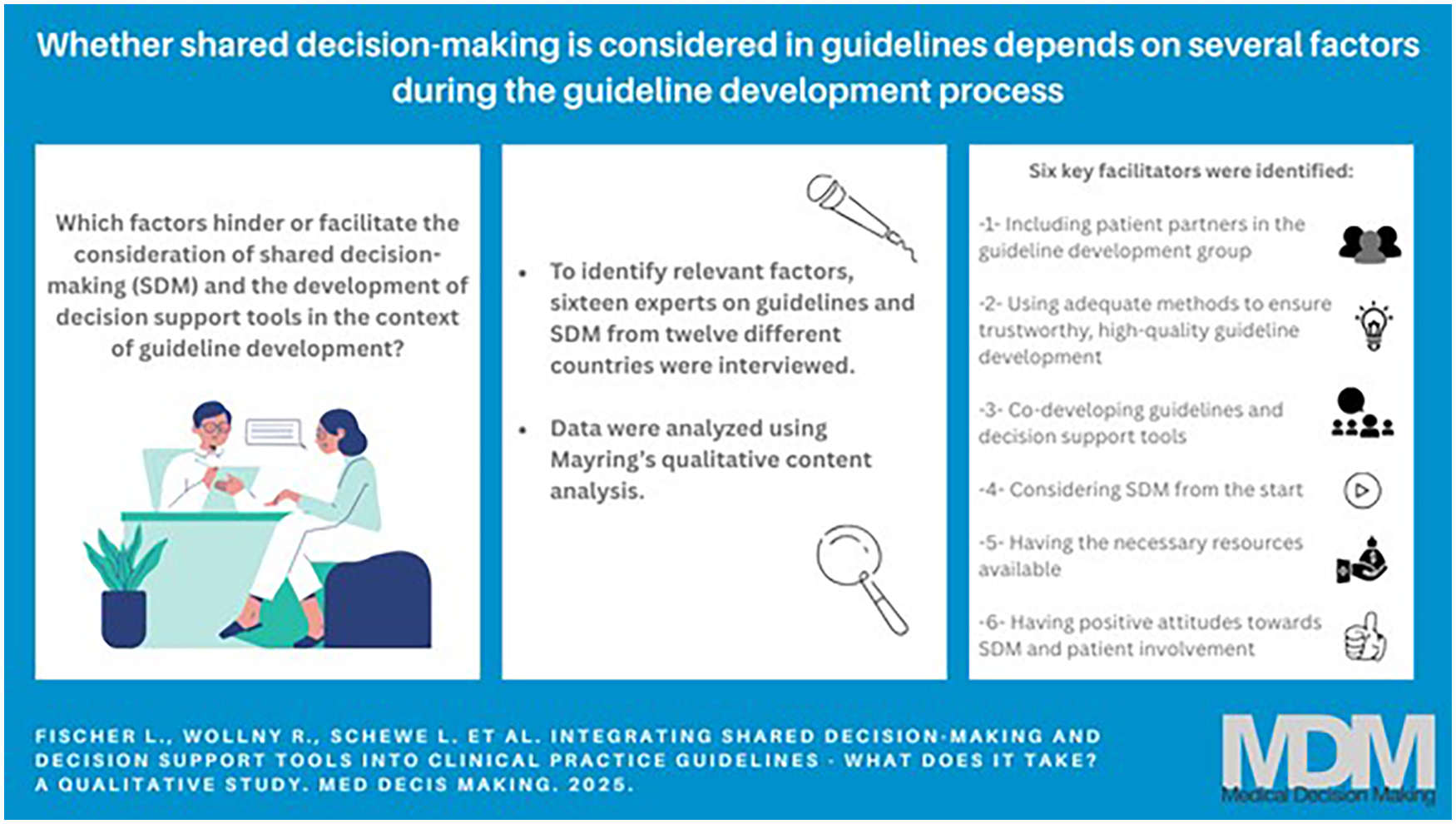
Keywords
Clinical practice guidelines (CPGs) are evidence-based statements intended to help health care professionals and patients make informed decisions about appropriate care.1,2 While CPGs provide general recommendations based on available evidence, they cannot account for individual patient preferences and circumstances (e.g., comorbidities, context), limiting their applicability in clinical decision making.3–5 To address this, shared decision making (SDM)—a collaborative approach in which health care professionals and patients make decisions together6,7—has been proposed as a strategy to enhance the recognition of person-centered care in CPGs.8–10
SDM helps to ensure that medical decisions align with the patient’s preferences and circumstances, but barriers to its application in clinical practice remain. For example, previous research has shown that health care professionals’ understanding of SDM varies,11,12 and their ability to understand and effectively communicate risks and benefits is often limited.13–15 Other studies have shown that patients benefit from SDM,16–18 but patients’ readiness to engage in SDM can vary, necessitating tailored support to enhance engagement. 19
Adapting CPGs to foster SDM and integrating decision support tools into CPGs may help increase health care professionals’ awareness of SDM, making patients more likely to receive SDM support. Nonetheless, the integration of SDM into CPGs remains inconsistent and insufficient.6,7 Evaluations have shown that CPGs addressed SDM only superficially or not at all.20–23 CPG recommendations have been found to often fail to reflect preference-sensitive decisions in how recommendations were framed, thus hindering SDM. 24
Little research has focused on how to adapt CPGs to foster SDM, and existing guidance is mainly based on practical experience during the CPG development process, 25 but some strategies have been proposed, targeting 1) the CPG development process, 2) CPG format and structure, 3) decision support tools, and 4) linking CPGs and decision support tools (see Table 1).25,26
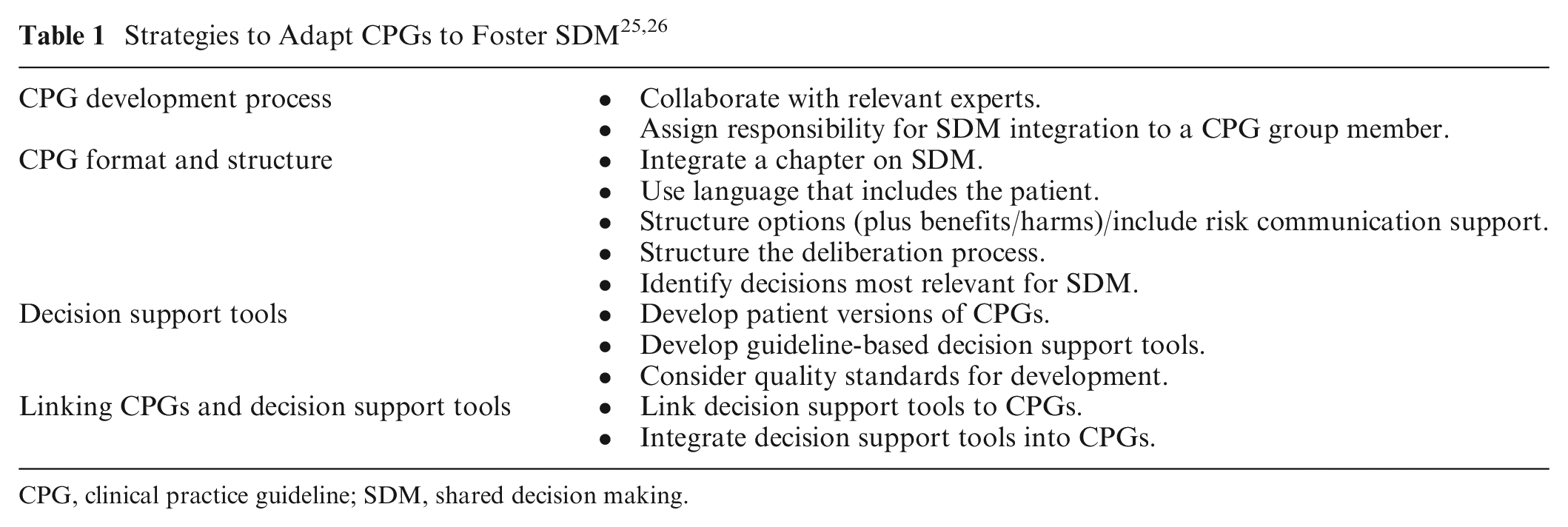
CPG, clinical practice guideline; SDM, shared decision making.
As recommended in guidance documents, considering SDM in CPGs should ideally start at the beginning and continue throughout the development process.25,26 However, to our knowledge, no studies have explored which factors in the CPG development process hinder or facilitate the integration of SDM into CPGs. In addition, although SDM relevance varies depending on the decision at hand,8,25 no common strategy exists to identify CPG recommendations for which SDM and the provision of decision support tools is most relevant.26,27
Of the various types of tools available to inform and educate patients and support them in decision making,28,29 patient decision aids (hereafter referred to as decision aids) are likely the most prominent. They provide evidence-based information about reasonable treatment or care options with associated benefits and harms and clarify personal values to support decision making.29–31 In this study, we use the terms “decision support tool” or “decision aid” (capturing pre/post and encounter decision aids) depending on whether we are referring more broadly to different types of decision support tools (which may still include decision aids) 29 or specifically to decision aids as defined above.
Despite high-quality research on the effectiveness of decision aids, 32 their development process is complex and resource intensive, and implementation barriers remain.33–35 Linking CPGs and decision aids—and their development process—might be a strategy to improve implementation, while ensuring that both are based on the same evidence. However, in a recent scoping review, we found that heterogeneous methods were used to develop and link decision aids in the context of CPGs, 27 raising questions on the most useful and practically feasible strategies for a linked development process.
To address the above-mentioned challenges associated with bringing CPGs, SDM, and decision support tools closer together, we conducted a qualitative study and interviewed experts in the fields of CPGs and SDM. We aimed to identify the following:
determinants of and strategies for selecting CPG recommendations where SDM and decision support tools are most relevant and
methods and strategies to connect CPGs and SDM, including factors that hinder or facilitate to consider SDM and to develop decision support tools in the context of CPG development.
Methods
This study is the second step in a multistage project aimed at developing a tool for CPG developers to systematically identify and prioritize CPG recommendations for which the integration of SDM and the provision of decision aids is most relevant. Our protocol with more details on the methodology is published elsewhere. 36 We followed the consolidated criteria for reporting qualitative research (COREQ) checklist to report our study. 37 The completed COREQ checklist is included in Supplementary Material 1.
Ethical Approval and Informed Consent Process
The study received an ethics waiver by Brandenburg Medical School, Germany (waiver No. 165122023-ANF). Participants were informed about the study’s objectives, its broader project context, the interviewer, the duration of the interview (approximately 45 min), and data protection measures. Participants who agreed to take part signed a consent form and sent it back to the interviewer. No incentives were provided for participation.
Participant Selection and Recruitment
We aimed to purposively 38 recruit experts on CPGs and SDM to ensure representation from a broad range of participants (i.e., different nationalities/health care systems; both CPG methodologists and developers, including health care professionals). To achieve this, we followed a 2-fold recruitment strategy until we reached data saturation. First, we contacted experts through the Guidelines International Network (GIN), as well as other CPG organizations that were not GIN members, via e-mail in January 2024. Second, we contacted the first authors of articles focusing on the link between CPGs and decision aids and their development process, as identified in a previous study. 27 Next to expertise in CPGs and SDM, interview participants needed to be ≥18 y old and fluent in English.
Interview Guide and Piloting
Based on the project’s objectives 36 and informed by previous research,3,25–27,39 a semi-structured interview guide (in English) was developed by 1 researcher (L.F.) and iteratively refined based on feedback from the project team (D.P., C.S., F.S., L.S., R.W.). The interview guide was available in 2 different versions: 1 more detailed interview guide for the interviewer (Supplementary Material 2) and 1 concise interview guide containing only the key questions for the participants (Table 2). All participants received the guide in advance.
Interview Guide for Participants
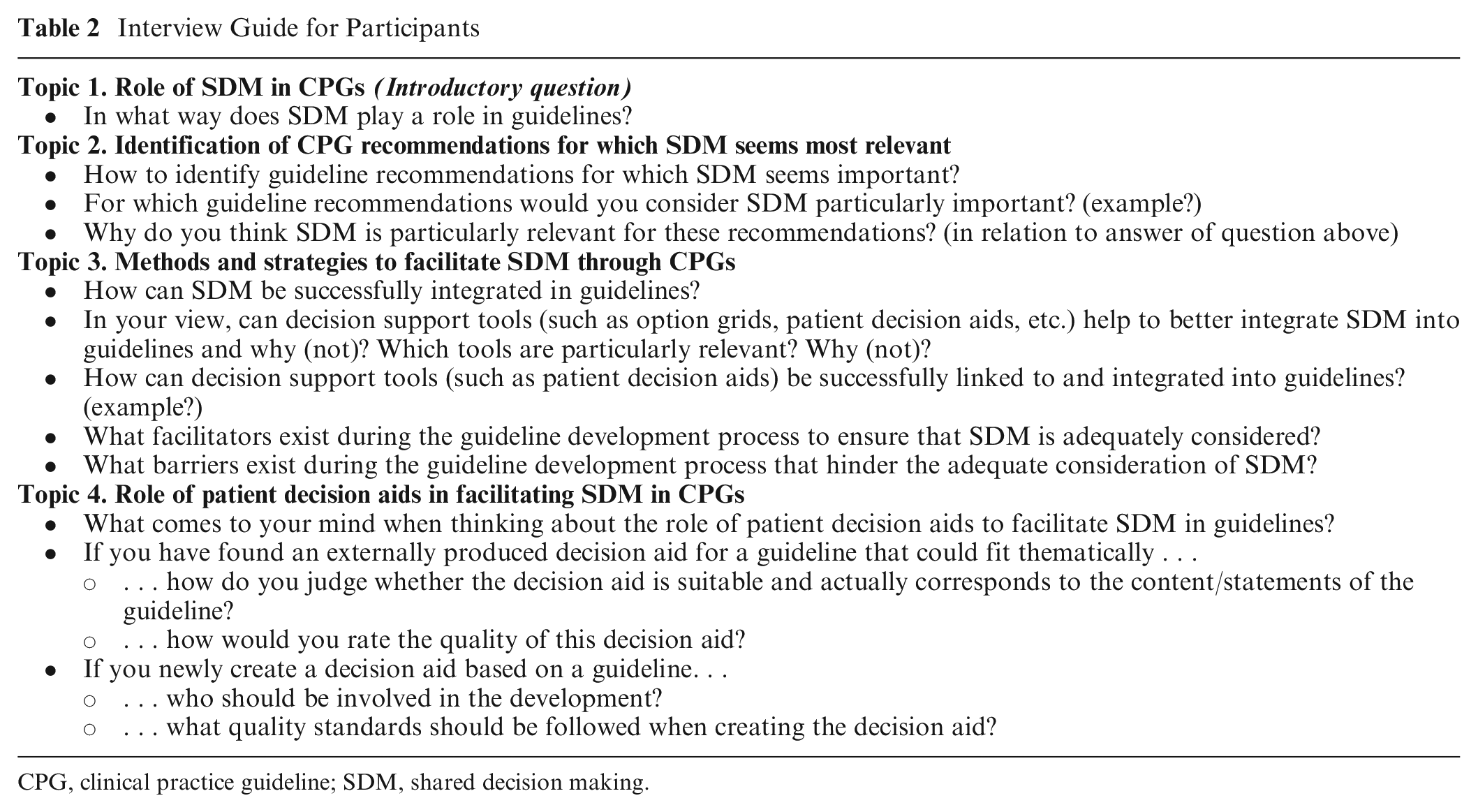
CPG, clinical practice guideline; SDM, shared decision making.
We piloted the interview guide with 3 members of the project’s international advisory board (anonymized for data protection purposes), consisting of experts in the fields of CPGs, SDM, and evidence-based health care. Before piloting started, all participants agreed to test the guide. Since no modifications to the interview guide were necessary after the pilot phase, the 3 pilot interviews were included in the data analysis after permission was obtained from the pilot participants.
Data Collection
One interviewer (L.F.) conducted all interviews in English using the semi-structured interview guide via an online meeting platform (Webex by Cisco). There was no connection between the interviewer and the participants except that the pilot participants had briefly met the interviewer at an unrelated meeting. Other than that, they did not know each other, and there were no further dependencies.
At the beginning of the interview, the interviewer and participant introduced themselves. The interviewer briefly explained what prior knowledge she had about the topic and that she was conducting the interviews for academic purposes. The interviews were digitally recorded, and the interviewer took notes during and/or immediately after the interviews to document any relevant information shared before the recording was started/after it was stopped. No repeat interviews were conducted. Before transcription, data were deidentified. A professional transcription service transcribed all interviews. One researcher (R.W.) conducted a quality check of the transcripts to ensure accuracy, particularly for topic-specific terminology. Following that, we sent out transcripts for comment and correction.
Data Analysis
Two researchers (L.F., R.W.) coded and analyzed data using qualitative content analysis as described by Mayring 40 with MAXQDA analysis software (standard version 18.2.4; Verbi GmbH). A category system was developed by using a deductive-inductive approach and then discussed within the research team. For each code and subcode, we created a memo that included the name of the code, a brief definition/description, and an example. The code book is included in Supplementary Material 3.
Finalizing the category system and the coding process was iterative and included 1) familiarization with the interview transcripts, 2) independent coding of a sample of the interviews by 2 researchers (L.F. and R.W.), followed by a discussion to refine and finalize the category system, and 3) finalization of the coding for all interviews by checking until consensus was reached. Interview participants did not provide any feedback on the final coding or findings.
Researcher Characteristics and Funding
As researchers’ characteristics and beliefs can influence the outcomes of qualitative research, 41 basic characteristics of the researchers that were primarily responsible for data collection and analysis were as follows: L.F., female, health scientist (MSc), little experience in conducting qualitative interviews (therefore trained by an experienced colleague), some experience in qualitative data analysis; R.W., female, medical student and student assistant of the project, little experience in qualitative data analysis (trained in advance). The funding sources of this project did not influence this study.
Results
After contacting 27 experts, we scheduled 17 interviews (of which 3 were pilot interviews), but 1 expert declined due to illness. In total, we conducted and analyzed 16 interviews in March and April 2024. Interview durations ranged from 27 min to 1 h, with a mean of 41 min. Participants came from 12 different countries, of whom 5 were from the Netherlands. All participants were engaged in research. The focus of their expertise varied depending on their background, although all had knowledge of CPGs and SDM (some also of decision support tools). Participant characteristics are shown in Table 3.
Participant Characteristics
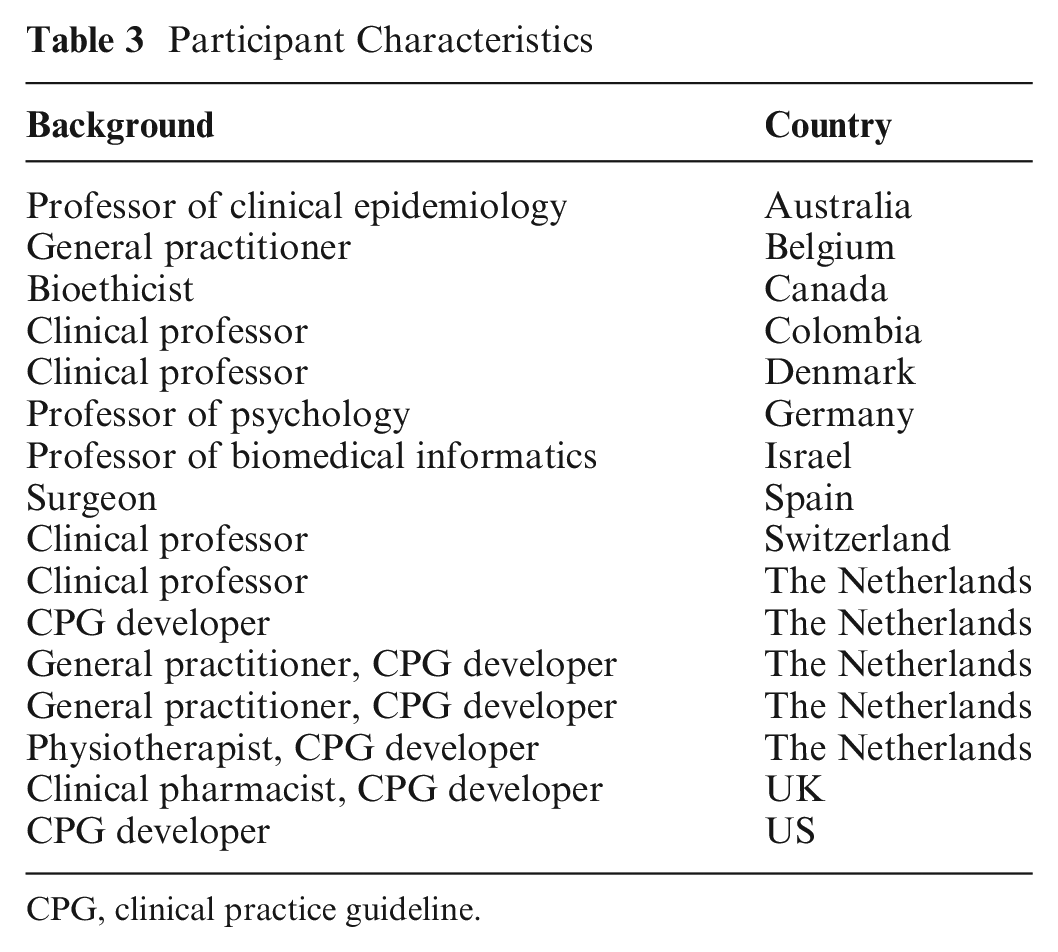
CPG, clinical practice guideline.
The results are organized according to the 2 main research questions. Supplementary Material 4 provides an overview relating the main coded categories to the research questions.
Identification of CPG Recommendations for Which SDM and Decision Support Tools Are Most Relevant
We distinguished between determinants of and strategies for identifying CPG recommendations for which SDM and decision support tools are relevant.
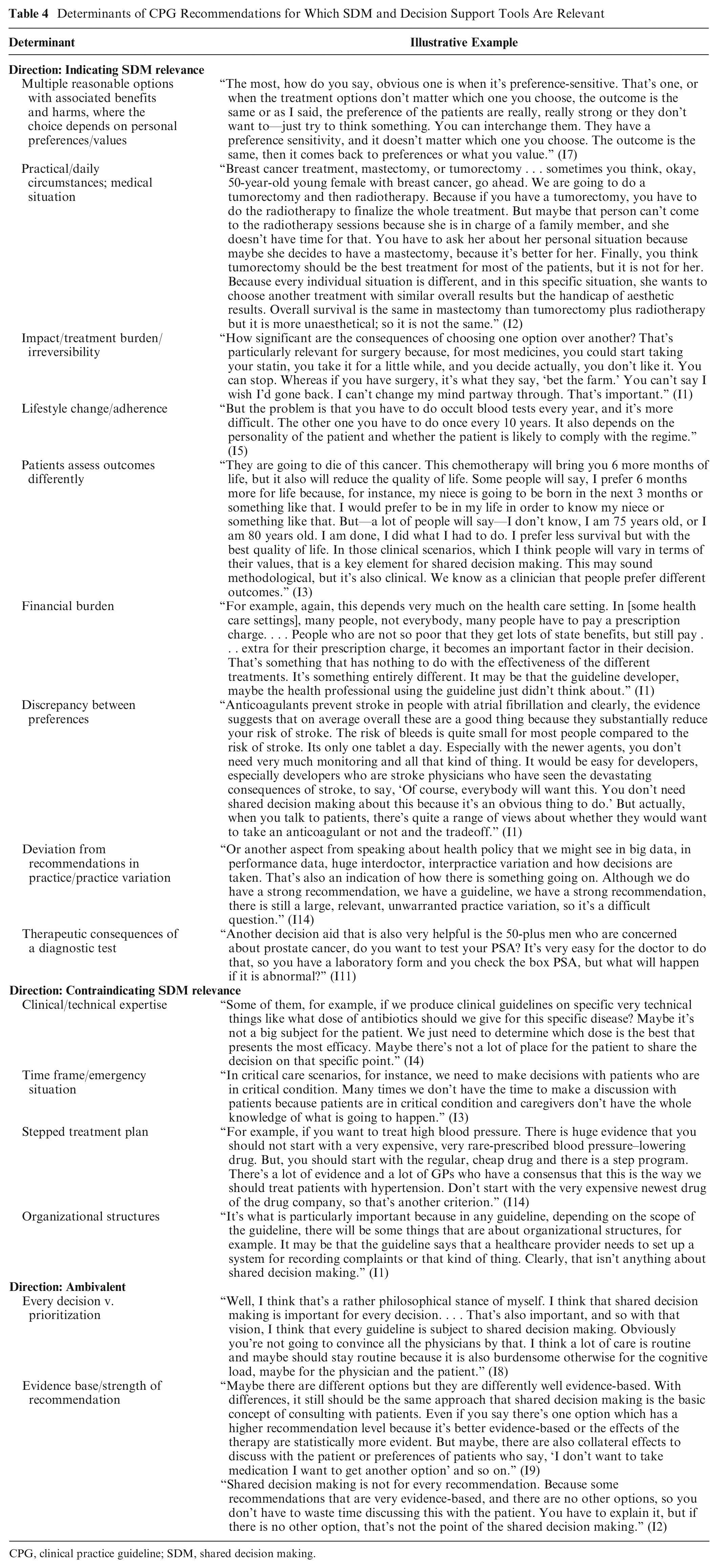
Table 4 provides an overview of determinants that indicated SDM relevance for a recommendation, contraindicated it, or were deemed ambivalent, plus example quotes. As determinants indicating SDM relevance, most participants mentioned multiple reasonable options with benefits and harms, where the choice depends on personal preferences as well as patients’ practical circumstances and medical situation. As determinants contraindicating SDM relevance, participants most often described technical expertise (e.g., determining the correct dosage of a drug). For a few determinants, there was ambivalence among participants. For example, some completely disagreed with the strength of a recommendation, while others argued that weak or conditional recommendations may be more important for SDM because they require more discussion about the balance of benefits and harms of interventions, depending on patient preferences (as opposed to strong recommendations, which most people would agree with). However, most participants argued that “there is more than just the type of recommendation” (I14).
Determinants of CPG Recommendations for Which SDM and Decision Support Tools Are Relevant
CPG, clinical practice guideline; SDM, shared decision making.
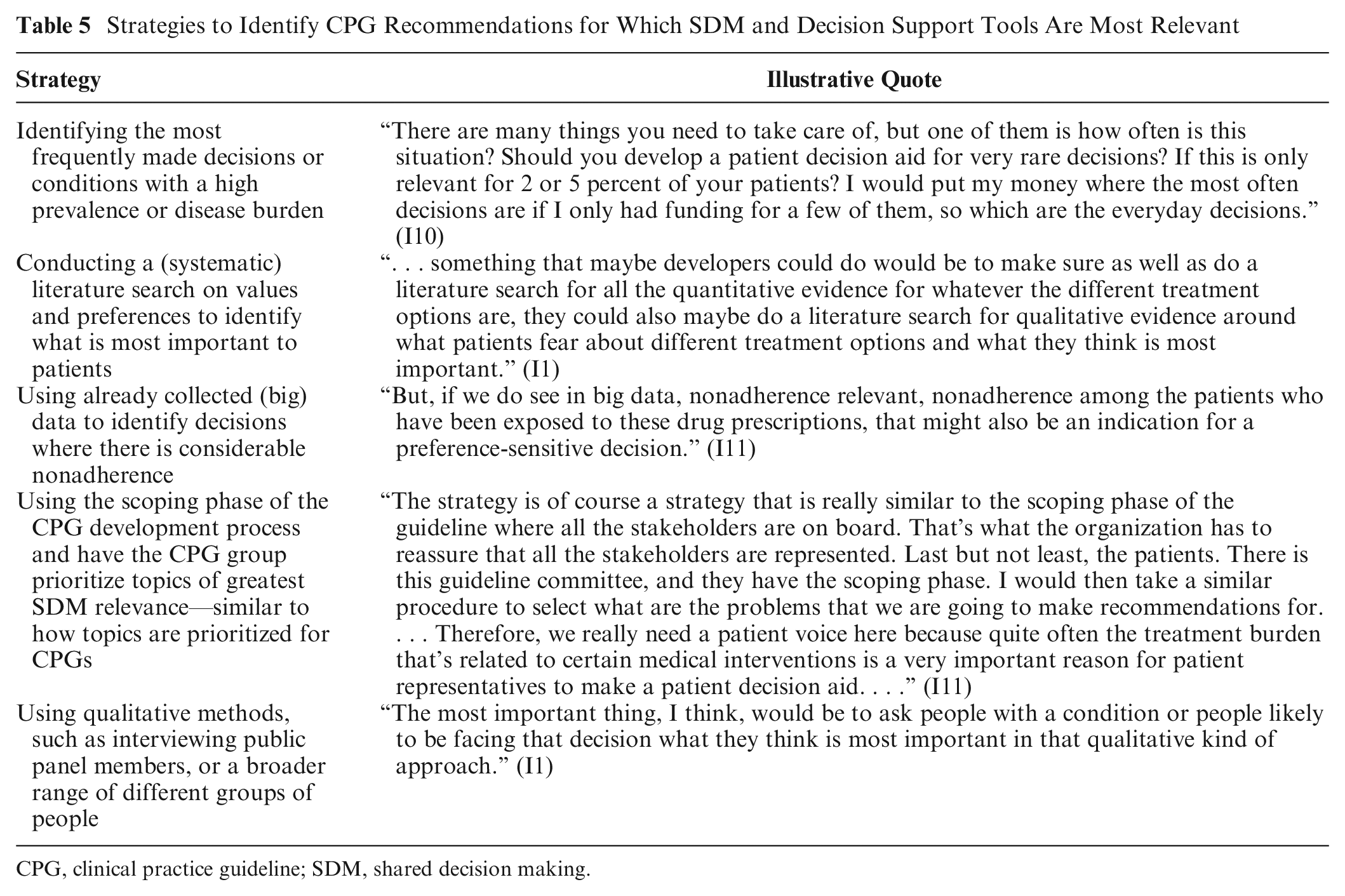
When asked how they would select the most relevant recommendations from a set of recommendations for which they consider SDM and the provision of decision support tools particularly important, participants suggested the strategies listed in Table 5. One participant argued that prioritizing CPG recommendations for the development of decision support tools might not be necessary, as the semiautomated production of these tools from structured evidence could mitigate current resource issues.
Strategies to Identify CPG Recommendations for Which SDM and Decision Support Tools Are Most Relevant
CPG, clinical practice guideline; SDM, shared decision making.
Methods and Strategies to Connect CPGs and SDM
The design and format of CPGs, the integration of CPGs and decision support tools, and factors in the CPG development process were discussed as ways to (more successfully) connect CPGs and SDM.
Design and format of CPGs
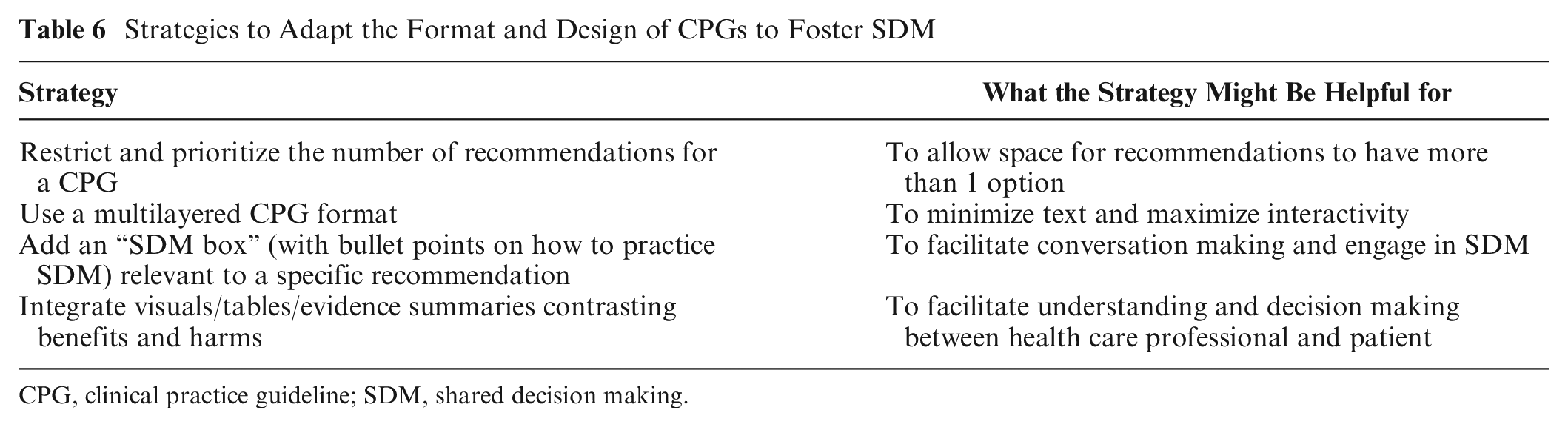
According to the participants, the design and format of CPGs were essential factors to better connect SDM and CPGs. On the one hand, participants deemed it important to make SDM an integral part of the CPG. This included adjusting the wording of the recommendations to emphasize that the patient should be involved in the decision making process and providing a balanced presentation of options with their pros and cons. On the other hand, participants argued that health care professionals are tired of reading “discuss with the patient” and do not have time to read the entire CPG, so if “. . . a recommendation to be put in place with clinicians, we may need to make things very easy for clinicians” (I3). They criticized the current format of CPGs as being cumbersome, complex, too lengthy, and therefore overwhelming. Suggestions to address this while better integrating SDM are shown in Table 6. While CPGs currently often include a chapter on SDM, some participants mentioned that they are just not read.
Strategies to Adapt the Format and Design of CPGs to Foster SDM
CPG, clinical practice guideline; SDM, shared decision making.
Decision support tools as a strategy to foster SDM in CPGs
Participants agreed that decision support tools serve as facilitators for closer linking CPGs and SDM, particularly when directly linked to the respective recommendation and vice versa or when CPGs and decision support tools are integrated and linked on a Web page or platform. The type of tool to use depends on the purpose, the decision to be made, and the characteristics and preferences of both patients and health care professionals.
When adapting decision aids from another country, participants outlined the need to ensure that the content is up to date, consistent with the recommendations of the CPG, and meets visual requirements. Some participants noted that their organizations do not adapt decision aids from other countries, even when they meet quality standards. One participant emphasized that the “not-invented-here syndrome” leads to duplication of efforts: “Everybody wants to build their own, and we don’t have time and resources for this. I think we should really put aside the ‘not-invented-here’ thing and be more open to adapting patient decision aids developed by your neighbor” (I13).
Participants considered the potential for decision support tools to go beyond their initial purpose of supporting patients, suggesting they could also help health care professionals better understand the benefits and harms of different options. Decision support tools were seen as promising tools for training health care professionals practicing SDM: “For me, it’s repurposing the shared decision making tools as a tool for teaching, a tool for didactic purpose and perhaps a top layer of your guideline rather than an adjunct tool” (I16).
Barriers and facilitators for considering SDM and developing decision support tools in CPG development
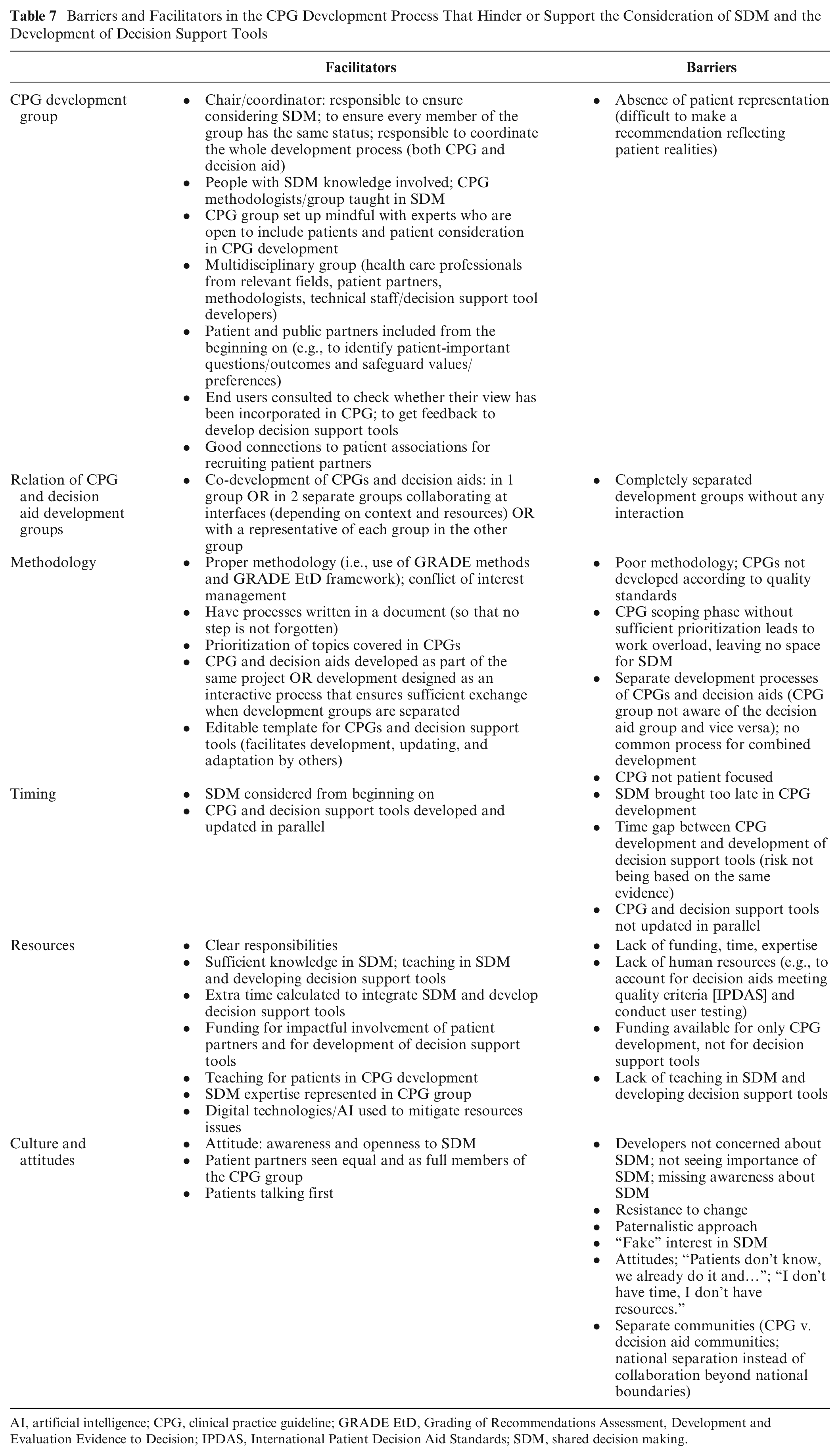
Whether SDM was considered in CPGs and decision support tools were developed depended on the underlying CPG development process. Table 7 gives an overview of the discussed barriers and facilitators that can either support or hinder the consideration of SDM and the development of decision support tools within the CPG development process.
Barriers and Facilitators in the CPG Development Process That Hinder or Support the Consideration of SDM and the Development of Decision Support Tools
AI, artificial intelligence; CPG, clinical practice guideline; GRADE EtD, Grading of Recommendations Assessment, Development and Evaluation Evidence to Decision; IPDAS, International Patient Decision Aid Standards; SDM, shared decision making.
CPG development group
Throughout all interviews, participants highlighted the particularly important role of patient partnership.
Have patients on your panel, so patient partnership. . . . Every time we had patients on the panel, it was better. But then it’s about facilitating their expression and understanding. . . . Because they give a flavor to any discussion afterwards. You might say the power of shame. You cannot say the same things equally strongly or with conflict or with tension if a patient just spoke. (I16)
It was deemed important that the CPG group received SDM teaching, and some group members took responsibility for ensuring that SDM was considered.
Relation of CPG and decision aid development groups
When asked whether the CPG group should play a role in decision aid development and vice versa and, if so, what that collaboration might look like, participants shared different options, depending on the context in which the CPG and decision aids were developed (i.e., whether it was a national/international CPG development; how the CPG/decision aid development process was organized, depending on the responsible organization). Generally, participants deemed the combined development of CPGs and decision aids important as “It doesn’t work very well if the guideline committee is producing their recommendations and then they go to another group and say, ‘Go on, then, you produce a patient decision aid or whatever support’” (I1). All emphasized the importance of at least maintaining communication with the other project group. However, according to the participants, this is currently not always the case: “. . . many patient decision aids are being developed and the guideline committee is not even aware of that. There is no connection whatsoever, which is, of course, not ideal, far from ideal” (I14).
Methodology
To have SDM adequately reflected in CPG development, participants highlighted the importance of 1) quality and trustworthy CPG development, 2) prioritization of topics that are covered in the CPG, and 3) clear processes for co-developing CPGs and decision support tools.
Timing
Not considering SDM from the beginning of the CPG development process was identified as a barrier, leading to an unfavorable format of CPGs and their recommendations: If you wait to the end, you’ve allocated hours and hours and perhaps months, different panel meetings and suddenly you say, okay, now, probably one of the implications of this is shared decision making. ‘Yes, we should say that in the guideline.’ Yes, you will say it in the guideline, but it’s not embodied in the thinking, in the writing and the framing of everything you say. (I16).
Resources
The availability of resources—in terms of time, funding, and expertise—can determine whether SDM would be considered in CPG development. Some participants observed in their environments that funding was available for CPGs but not for decision support tools, thus hindering the combined development. Developing decision support tools as part of the CPG without additional support for the CPG group was considered challenging as (human) resources were missing.
Culture and attitudes
Participants frequently identified the culture and attitudes of CPG development groups as barriers to SDM. The concept of SDM was sometimes misunderstood, overlooked, or considered unimportant. Some described feeling caught between separate communities: “Also, another barrier is the communities working in guidelines and evidence synthesis and the communities working in shared decision making. I feel I belong to both. I feel they’re not making sufficient effort to work together” (I16). Participants expressed a desire for closer interaction between these communities: “Then the ideal world is that we have one big community and one governance on developing guidelines and patient decision aids together, so we are far from that” (I14).
Throughout the interviews, participants frequently reflected on the implications for clinical practice if the CPG development process—and subsequently the design of CPGs and the development and integration of decision support tools—were adapted to better facilitate SDM. For example, many participants emphasized that while connecting CPGs and SDM more closely is an important strategy, it must be complemented by other strategies—above all, fostering a culture in which SDM becomes the standard approach to patient consultations. This also implied the need to provide training to health care professionals, equipping them with the necessary skills to share decisions and using decision support tools. Participants emphasized the importance of keeping things as simple as possible, both during the CPG development process (e.g., offering the CPG group a teaching on SDM and guideline-based decision aid development) and when linking CPGs and decision support tools (e.g., providing a central access point rather than multiple platforms, apps, and Web pages for decision support tools).
Discussion
Main Findings
In this qualitative study, experts in the field of CPGs and SDM from a variety of backgrounds and health care contexts provided insights into strategies for integrating SDM and decision support tools successfully into CPGs.
For research question 1, which aimed to identify determinants of and strategies for selecting CPG recommendations where SDM and decision support tools are most relevant, we categorized a total of 15 determinants that indicated SDM relevance for a recommendation (e.g., multiple reasonable options with their associated benefits and harms), contraindicated it (e.g., emergency situations), or were deemed ambivalent (e.g., the strength of a recommendation). In addition, participants also suggested some practical strategies (e.g., identifying what is most important to patients by conducting a systematic literature search).
Research question 2 aimed to identify methods and strategies for linking CPGs and SDM, including factors that hinder or facilitate the consideration of SDM and the development of decision support tools in the context of CPG development. Participants described the current complex format of CPGs as a barrier to integrating SDM into CPGs. The integration of decision support tools into CPGs was described as a facilitator, but these need to be easily accessible. In more depth and detail, they reflected on barriers and facilitators in the CPG development process. Whether or not to consider SDM may depend on the composition and attitudes of the CPG development group, its relationship with the decision aid development group, the underlying methodology and timing, and available resources. Participants emphasized the important role of patient partners in ensuring that SDM is considered. Inadequate resources in terms of time and funding and a culture in which patient involvement and SDM are not seen as essential were discussed as the key barriers. There was agreement on the need to link CPG and decision aid development processes and groups, but proposed approaches were heterogeneous depending on the context.
Discussion of Results and Comparison with Existing Literature
From the perspective of experts in CPG development, methodology, and SDM, this study provides insight into which CPG recommendations are particularly relevant for SDM and why. In addition to previous research,27,39 financial burden, which revolves around cost factors for patients, emerged as a new determinant to identify recommendations that may require SDM. Accounting for costs in SDM has recently been highlighted in research, calling for the routine inclusion of cost considerations in decision aids and SDM guidelines to address the potential financial burden on patients and their preference for cost to be discussed as part of treatment decisions. 42 However, it is necessary to consider that cost considerations may differ from country to country.
To better link CPGs and SDM, participants suggested adapting the design and format of CPGs and integrating decision support tools. Building on previous research, they addressed implementability features of applicability (i.e., providing information to help interpret and apply recommendations to individual patients) and communicability (i.e., including information that facilitates discussions with patients and supports their involvement in decision making). 43 Given that implementability features can improve the use of CPGs, 43 our findings suggest that considering SDM during CPG development—rather than after—may support implementability, which in turn may improve the subsequent implementation of CPGs.
To our knowledge, this is the first study to explore factors influencing the integration of SDM and decision support tools in CPG development. While previous studies have focused on barriers and facilitators to CPG implementation44,45 and adherence 46 or to the implementation of SDM,11,47,48 findings show overlapping challenges in both the development and implementation of CPGs. Similar to what we found for the development process, barriers to CPG implementation and adherence include CPG complexity44–46 and lack of resources and skills or training,44,46 while lack or inadequacy of resources (i.e., time and funding) and cultural or attitude-related factors were identified as barriers to implementing SDM.11,47 This overlap underscores the inherent connection between the development and implementation phases and suggests that the CPG development process influences the subsequent implementation of CPGs and SDM.
Uniquely, our findings highlight the important role attributed to patient partners in ensuring a person-centered CPG development process that enables SDM and facilitates the combined development of CPGs and decision support tools. In contrast, previous research found that no standard approach for involving patients and the public in CPG development is evident from research yet, 49 while patient involvement has been found to remain limited.50–52 In light of our findings, these shortcomings appear to jeopardize the adequate integration of SDM into CPGs. In addition, it must be clear that the CPG development group cannot ask patient partners to take responsibility for ensuring that SDM is integrated into CPGs. As previous research and the GIN Public Toolkit have shown, patient participation in CPG development can pose some challenges, such as the risk of missing the perspective of vulnerable groups who may not be part of the CPG group or, if they are, may feel intimidated to speak up.53,54 While it would be desirable that the CPG group as a whole works toward the integration of SDM into CPGs, other methods of patient involvement, such as consultation methods (e.g., surveys, focus groups, literatures searches on patient values and preferences)—combined with participation methods—could support fostering SDM in CPGs.
More than a decade ago, van der Weijden et al. (2012) discussed the inevitable relationship between CPGs and decision aids, 3 underscoring that linking CPGs and decision aids can foster SDM. However, participants in our study reported barriers to joint development, with CPG and decision aid development processes remaining separate and groups unaware of each other. In contrast, respondents did not question whether the two groups should collaborate. However, the how remained unclear and appeared to depend heavily on the context, available resources, and expertise in the CPG group. This reflects a recent finding that no standard methods have been established for joint development of CPGs and decision aids. 27 Our findings suggest that interview participants, many of whom are active members of both the CPG and SDM communities, still perceive these communities as separate. This may be a result of the different structures and responsibilities in which CPGs and decision aids are developed but underlines the need for establishing closer collaboration at an overarching level to better integrate SDM into CPGs.
Strengths and Limitations
A strength of our study is that we interviewed a wide range of experts with a different focus of expertise (i.e., CPG development/methodology, combined with SDM) and from different countries and health care contexts. The semi-structured format of the interviews ensured that key questions were addressed while allowing space for respondents to freely share their ideas and perspectives. We had the interview transcripts returned to participants for comment and correction to strengthen the validity of our study.
However, this work is not free of limitations. First, the researchers primarily responsible for data collection and analysis had limited experience conducting qualitative research before this study. However, they received training from an experienced researcher, including a simulated interview and interview analysis. In addition, they were supported by an experienced team that was consulted at key stages, such as the development of the interview guide or category system. Second, we did not interview patients and their partners themselves. We decided this because the interview topic is very specific and requires participants to have considerable knowledge of CPGs, their development process, and SDM. However, we discussed the results of the interviews with the patient partners in the project. They confirmed the findings from their point of view. Third, we purposively selected participants, most of whom were from Western countries (5 of the 16 were from the Netherlands), while we had only 1 expert from low- and middle-income countries interviewed. The strong representation of participants from the Netherlands was because this country may be considered a pioneer in the implementation of SDM and the linking of CPGs and SDM. It is plausible that a more culturally diverse interview sample would have offered additional ideas.
In reporting our findings, we used the broader term decision support tool and did not strictly differentiate between decision aid types (i.e., pre/post encounter or encounter decision aids). This may have led to the description of our findings becoming less precise. For example, shorter decision aids designed for the encounter will have a much smaller impact on the available resources than more complex decision aids will. We made this choice deliberately because it did not seem critical to our main research objective (to provide a more general overview of strategies for more successful integration of SDM and decision support tools into CPGs). We did not intend to assess the effects or outcomes of developing different types of decision aids as part of the CPG development process.
Future Research Directions and Practical Implications
Through the interviews, we did not identify a clear strategy for applying determinants to identify SDM-relevant recommendations. Further research is needed to refine these determinants and develop a systematic approach for their application. The proposed strategies that are not tied to specific determinants, such as using the CPG scoping phase or qualitative methods to identify SDM-relevant topics/recommendations, could serve as a starting point. These strategies are already used for other purposes in CPG development, such as prioritizing outcomes, making them readily adaptable for identifying CPGs topics and recommendations most relevant to SDM.
Our study highlighted the potentially critical role of patient partners in CPG development to enable the consideration of SDM. Thus, future studies should explore the perspectives of patients on these topics. CPG organizations should more rigorously translate their methods for engaging patients and the public in CPG development into practice. In addition, CPG groups need to be equipped with the necessary skills to consider SDM. Future studies could explore how culture and economic context (i.e., high- v. low- and middle-income countries) influence CPG groups’ attitudes toward SDM.
The findings indicate that decision support tools may be useful beyond their initial purpose, such as teaching health care professionals how to have SDM conversations. This field could be explored in more depth in future studies.
Further research is also needed on practically feasible strategies for the combined development of CPGs and decision aids, considering the context and available resources, and CPG organizations testing these. Given the remaining challenges to SDM-centered CPG development and the combined development of CPGs and decision support tools, new policies appear to be needed to address these challenges, also considering identified resource issues. We urge CPG and SDM communities to work toward closer collaboration.
Conclusion
Whether SDM is considered in CPG development depends on the development group, the underlying methodological approach, the culture, and the available resources and expertise. Involving patients and patient partners can support addressing SDM in CPGs, but this requires a supportive culture and appropriate facilitation (e.g., through teaching). Decision support tools can foster the link between CPGs and SDM, but it is critical that development groups merge or work in collaboration. The identified strategies can serve as a starting point for CPG organizations to explore ways for considering SDM and developing decision support tools in the CPG development process, taking into account facilitating and hindering circumstances in their specific context.
Supplemental Material
sj-docx-2-mdm-10.1177_0272989X251368866 – Supplemental material for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study
Supplemental material, sj-docx-2-mdm-10.1177_0272989X251368866 for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study by Lena Fischer, Rahel Wollny, Leon V. Schewe, Fülöp Scheibler, Torsten Karge, Thomas Langer, Corinna Schaefer, Ivan D. Florez, Andrew Hutchinson, Sheyu Li, Marta Maes-Carballo, Zachary Munn, Lilisbeth Perestelo-Perez, Livia Puljak, Anne Stiggelbout and Dawid Pieper in Medical Decision Making
Supplemental Material
sj-docx-3-mdm-10.1177_0272989X251368866 – Supplemental material for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study
Supplemental material, sj-docx-3-mdm-10.1177_0272989X251368866 for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study by Lena Fischer, Rahel Wollny, Leon V. Schewe, Fülöp Scheibler, Torsten Karge, Thomas Langer, Corinna Schaefer, Ivan D. Florez, Andrew Hutchinson, Sheyu Li, Marta Maes-Carballo, Zachary Munn, Lilisbeth Perestelo-Perez, Livia Puljak, Anne Stiggelbout and Dawid Pieper in Medical Decision Making
Supplemental Material
sj-docx-4-mdm-10.1177_0272989X251368866 – Supplemental material for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study
Supplemental material, sj-docx-4-mdm-10.1177_0272989X251368866 for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study by Lena Fischer, Rahel Wollny, Leon V. Schewe, Fülöp Scheibler, Torsten Karge, Thomas Langer, Corinna Schaefer, Ivan D. Florez, Andrew Hutchinson, Sheyu Li, Marta Maes-Carballo, Zachary Munn, Lilisbeth Perestelo-Perez, Livia Puljak, Anne Stiggelbout and Dawid Pieper in Medical Decision Making
Supplemental Material
sj-pdf-1-mdm-10.1177_0272989X251368866 – Supplemental material for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study
Supplemental material, sj-pdf-1-mdm-10.1177_0272989X251368866 for Integrating Shared Decision Making and Decision Support Tools into Clinical Practice Guidelines: What Does It Take? A Qualitative Study by Lena Fischer, Rahel Wollny, Leon V. Schewe, Fülöp Scheibler, Torsten Karge, Thomas Langer, Corinna Schaefer, Ivan D. Florez, Andrew Hutchinson, Sheyu Li, Marta Maes-Carballo, Zachary Munn, Lilisbeth Perestelo-Perez, Livia Puljak, Anne Stiggelbout and Dawid Pieper in Medical Decision Making
Footnotes
Acknowledgements
We would like to thank all interview participants for their time and valuable contribution to our study. ChatGPT has been used to check the grammar of some sentences.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by a grant from the Innovation Committee at the Federal Joint Committee (No. 01VSF23022).
Ethical Considerations
The study has received an ethics waiver by Brandenburg Medical School, Germany (waiver No. 165122023-ANF).
Consent to Participate
Participants who accepted to take part had to sign a consent form and send it back to the interviewer.
Consent for Publication
Not applicable.
ORCID iDs
Data Availability
The generated and analyzed datasets are not publicly available due to the need to protect participants’ privacy and confidentiality. These datasets are available from the corresponding author upon request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.