
Abstract
Trunk impairment from neurological conditions such as spinal cord injury, cerebral palsy, and stroke limits postural coordination and functional independence. Sense of agency (SoA), the perceived control over one’s movements, influences motor learning and rehabilitation engagement, yet has not been examined in seated postural training. This study investigates how robotic pelvic guidance and visual feedback (VF) designs influence motor coordination and SoA during a seated reaching task in virtual reality (VR), validated here with able-bodied subjects. Thirty-two healthy adults were randomly assigned to four groups (n = 8) in a 2 × 2 between-subjects design: pelvic guidance (guided vs unguided) and VF type (control VF, CVF: a pursuit-tracking moving target, vs error-based VF, EVF: displaying only the hand–target error). In the guided condition, the pelvic Wheelchair Robot for Active Postural Support (pWRAPS) actively guided pelvic orientation during a four-direction hand-tracking game. In the unguided condition, the robot operated in transparent mode. Participants receiving pelvic guidance showed significantly greater improvements in task performance and pelvis–trunk–hand coordination than unguided participants, regardless of VF type. EVF influenced trunk–pelvis coordination independently of guidance, with CVF yielding greater trunk–pelvis improvement. Trunk–pelvis coordination emerged as the strongest predictor of SoA, and SoA increased significantly at post-test, suggesting that perceived agency reflects coordination quality rather than the presence or absence of robotic assistance. Critically, guidance improved coordination without diminishing SoA, indicating compatible biomechanical and psychological rehabilitation goals. These findings support integrating robotic pelvic guidance with VR-based feedback for seated postural rehabilitation.
Keywords
1. Introduction
Trunk impairment is a common consequence of neurological conditions such as spinal cord injury (SCI) (Serra-Añó et al., 2013), cerebral palsy (CP) (Heyrman et al., 2013), and stroke (Genthon et al., 2007). This impairment leads to deficits in postural control, balance, and mobility that significantly impact functional independence and quality of life, particularly for wheelchair users.
In 2025, an estimated 308,620 people in the U.S. lived with traumatic SCI, with approximately 18,421 new cases each year. Since 2015, 67.4% of new injuries involved incomplete tetraplegia or complete paraplegia from cervical or high thoracic lesions, leading to wheelchair dependence and trunk deficits (National Spinal Cord Injury Statistical Center, 2025). Similarly, CP affects about 3.1 per 1,000 third-grade children, with 32% classified at Gross Motor Function Classification System (GMFCS) levels IV or V, often requiring posture and mobility assistance (Christensen et al., 2014). Stroke impacts roughly 795,000 Americans yearly, significantly impairing trunk function, balance, gait, and activities of daily living (ADLs) (Centers for Disease Control and Prevention (CDC), 2024; Collin and Wade, 1990; Verheyden et al., 2006). Despite retaining some upper limb function, individuals with impaired trunk control often struggle with essential ADLs such as eating, opening doors, and reaching for objects (Peeters et al., 2018a), highlighting the need to address trunk control deficits to improve functional independence and quality of life.
Trunk performance is not only functionally important but also a strong predictor of recovery: trunk control scores are among the earliest and most reliable indicators of mobility outcomes after stroke (Ishiwatari et al., 2021; Verheyden et al., 2007). The pelvis plays a crucial role in supporting functional seated movements and postural stability during daily activities (Kasahara et al., 2008; Peeters et al., 2018b). For individuals with impaired trunk control, stabilizing the pelvis and lower trunk segments may be key to regaining upper-body control and coordination (Haruyama et al., 2017; Miyake et al., 2013). These findings establish a clear clinical target: rehabilitation approaches that can improve pelvis–trunk–hand coordination have the potential to restore functional independence in seated tasks.
Conventional motor therapies for trunk impairment, however, often lack the mass practice, variability, and progressive postural challenge needed to drive lasting motor learning (Cirstea et al., 2003; Cirstea and Levin, 2000). Trunk-focused rehabilitation has shown promising benefits for functional activities in both stroke (Boswell-Ruys et al., 2010) and SCI patients (Kalaichandran, 2024), but these approaches are typically limited in their ability to deliver precise, repeatable, and individually scaled training stimuli. Furthermore, conventional therapy provides limited control over the specific body segments being trained: a therapist can cue trunk engagement verbally or manually, but such guidance is inherently variable across sessions and practitioners, difficult to quantify, and challenging to sustain at the precise timing and intensity required during dynamic reaching tasks.
A related challenge is that rehabilitation success depends not only on biomechanical improvement but also on the patient’s subjective engagement with the training process. Sense of agency (SoA), the experience of controlling one’s own movements, is a psychological construct with direct relevance to motor rehabilitation. SoA is strengthened when sensory feedback aligns with predicted motor outcomes (Haggard, 2017; Karsh and Eitam, 2015), and is diminished by the sensory and motor disruptions that accompany neurological injury (Burin et al., 2015). Reduced SoA can undermine movement intention and discourage active participation, creating a cycle in which disuse further weakens motor capacity. Conversely, interventions that preserve or enhance SoA may promote sustained engagement and facilitate motor learning through increased voluntary effort (Cesari et al., 2024).
Recent work on SoA in assisted and virtual tasks has shown that performance improvements induced by external assistance can be self-attributed by the user, even when they are aware of the assistance (Inoue et al., 2017; Wen et al., 2015), and that visual feedback modifications in VR can enhance perceived agency during continuous body movements (Aoyagi et al., 2021). In robotic and assistive device contexts specifically, temporal alignment between robotic assistance and user intent has been shown to be critical for preserving agency (Davis et al., 2025; Wen et al., 2021), and SoA has been examined alongside motor performance in upper-limb virtual reaching and rehabilitation tasks (Ly, 2025; Nataraj et al., 2020). However, these studies have focused primarily on distal upper-limb tasks. SoA has not been examined in the context of seated postural training, where robotic guidance acts on proximal body segments (pelvis and trunk) rather than the distal limbs, and visual feedback strategies may shape the learner’s perceived control in ways distinct from hand- or arm-focused interventions.
To support postural training, a cable-driven Trunk-Support-Trainer (TruST) was used to enhance sitting stability in children with CP and individuals with thoracic SCI. Assist-as-needed forces were applied when the trunk moved beyond its postural limits (Santamaria, Khan, et al., 2020; Santamaria, Luna, et al., 2020). However, while TruST is effective for those with partial pelvic control, individuals with more severe pelvic instability may require additional support to fully benefit from trunk rehabilitation.
To address this gap, we propose the use of a pelvic Wheelchair Robot for Active Postural Support (pWRAPS) (Ophaswongse and Agrawal, 2020; Ophaswongse et al., 2022). As pWRAPS is designed to support seated postural rehabilitation, it accommodates natural pelvic motion across all three rotational degrees-of-freedom and delivers safe, motor-controlled torques via a pelvic brace end-effector. pWRAPS enables active pelvic mobilization to support upper-body motor training. This function builds upon pelvic proprioceptive neuromuscular facilitation (PNF) principles, where guided resistance and movement patterns to the pelvis and lower trunk improve trunk control, balance, and functional outcomes in stroke patients (Sharma and Kaur, 2017). By synchronizing pelvic guidance with trunk and arm movements, pWRAPS may enhance upper-body coordination beyond training the upper limb in isolation (Ho et al., 2023), supporting more effective rehabilitation for ADLs (Guido and Stemm, 2007; Nguyen et al., 2022; Page, 2006).
While robotic guidance addresses the physical dimension of training, the visual feedback (VF) strategy used to convey task information to the learner is equally important. VF design determines what the learner attends to (the target, the error, or the movement itself) and thereby shapes the motor learning process. Virtual reality (VR) has been shown to offer a versatile platform for trunk rehabilitation in stroke and SCI populations (Alhwoaimel et al., 2024; Gao et al., 2021; Lee and Lee, 2021). It enables complex and adaptive training tasks through gamification and progressive difficulty adjustment, enhancing motivation and adherence (Ai et al., 2024). VR is particularly suitable for our seated reaching study. The 3D target-tracking task spans a wide spatial workspace where a monitor placed in front of the participant would introduce gaze-driven neck rotations and would confound the trunk–pelvis–hand coordination measures of interest. An immersive head-mounted display eliminates this confound by co-rotating the visual scene with the head. TruST has also been combined with a VR gaming environment for seated reaching tasks, where a single training session increased lower trunk range of motion comparably to physical-environment training (Khan et al., 2017), demonstrating the feasibility of integrating robotic trunk support with immersive VR. However, that study evaluated only kinematic outcomes; the effect of robotic trunk training in VR on the learner’s sense of agency was not explored. Our prior work demonstrated that integrating VR with pWRAPS enhanced upper-body coordination of a seated reaching task through real-time visual and somatosensory cues. The active pelvic guidance from pWRAPS facilitated pelvis–trunk–hand coordination to track hand paths at twice the subject’s self-paced speed (Ophaswongse et al., 2024).
Critically, VF design and robotic guidance may also interact to influence the learner’s sense of agency. Multisensory integration has been identified as the most relevant factor shaping both SoA and learning outcomes in virtual environments (Cesari et al., 2024), and VF strategies in VR can modulate both SoA and motor performance (Aoyagi et al., 2021; Sanford et al., 2022).
Our paradigm combines VF with haptic pelvic guidance and raises an important question that existing works have not addressed. A VF strategy that makes performance errors salient could enhance SoA, by providing clear evidence that one’s actions causally affect the display, or diminish it, if the error signal is perceived as evidence of poor control. When robotic guidance is layered on, the question sharpens further: does the learner perceive the robot-assisted improvement as self-generated (Inoue et al., 2017), or does external assistance reduce the sense of personal control? Resolving this interaction is essential for designing rehabilitation systems that are both biomechanically effective and psychologically engaging (Dutta, 2025).
Therefore, this study examines the combined effects of a novel VF strategy and active pelvic guidance from pWRAPS on both motor coordination and sense of agency. In the present study, we have a sample size of 32 able-bodied participants, assigned to four groups (n = 8 each) based on two factors: presence or absence of pelvic guidance and type of VF. Participants either received pWRAPS guidance or remained unguided, and trained with either a direct target display (control condition of VF) or a novel VF that highlights the hand–target trajectory mismatch.
To our knowledge, this is the first study to investigate the combined effects of robotic pelvic guidance and VR-based visual feedback on motor learning and sense of agency during seated reaching tasks that require multi-segmental postural coordination. Previous research has largely overlooked this intersection of robotic assistance and immersive feedback in the context of full-body seated movements, particularly in tasks involving multiple ways to execute the task by sharing the workload between the trunk and the upper arm (Levin and Demers, 2021).
This study is guided by three hypotheses. (H1): Improved task performance, as indicated by reduced hand trajectory error, is associated with smaller deviations between actual and target body segment coordination patterns. (H2): Active pelvic guidance from pWRAPS enhances task performance and coordination. Participants with active guidance will show greater reductions in movement error when compared to those without guidance, regardless of VF. (H3): Pelvic guidance and VF type interact to influence sense of agency. Specifically, the effect of robotic guidance on perceived control depends on the type of visual feedback: error-based VF may either amplify or attenuate the agency effects of guidance by altering how participants attribute coordination improvements to their own motor effort.
The remainder of this paper is organized as follows. Section 2 (Materials and Methods) describes the pWRAPS, experimental setup and protocol, VR environment, VF types, and analysis methods. Section 3 (Results) presents the baseline reaching range of motion (ROM). We test Hypothesis 1 (H1) by examining the correlation between task scores and body segmental coordination. We evaluate training effects on performance changes in H2. We analyze SoA in relation to motor outcomes and experimental conditions in H3. Section 4 (Discussions) interprets the findings in the context of seated trunk rehabilitation, followed by the Limitations and Future Work (Section 5) and Conclusions (Section 6).
2. Materials and methods
2.1. Robotic system
The 3-DOF kinematic architecture of pWRAPS is shown in Figure 1(a). The system consists of three actuated revolute joint axes (R) which are fixed in the bench frame {O
b
}, while the moving frame {O
p
} is attached to the pelvic brace. The universal joint center (U) in chain 1 and spherical joint centers (S) in chains 2 and 3 are fixed relative to {O
p
}. Each chain’s first joint is actuated by a Maxon EC60 brushless DC motor (Maxon Precision Motors, Inc., Taunton, MA, USA). Orthotic foam pads in the inner lining of the brace improve human comfort. The pWRAPS controller runs on a Control PC using ROS Noetic (Ubuntu 20.04), with motor/sensor communication via two Sensoray 826 PCIe I/O cards (Sensoray Co., Inc., Tigard, OR, USA). The physical prototype worn by a subject and the hardware setup are shown in Figure 1(b). Two feedback control modes were implemented for this study. (a) CAD Model of pWRAPS prototype with kinematic diagram and coordinate frames; R: revolute joint (R: actuated revolute joint); U: universal joint; S: spherical joint. (b) Experimental setup with an able-bodied subject wearing pWRAPS. (c) Control visual feedback (CVF) is represented by a red ball moving along a target hand trajectory. (d) Error-based visual feedback (EVF) is represented by a 3D line connecting the player’s hand and the current hand target position in the trajectory; the line color also changes based on the hand error distance.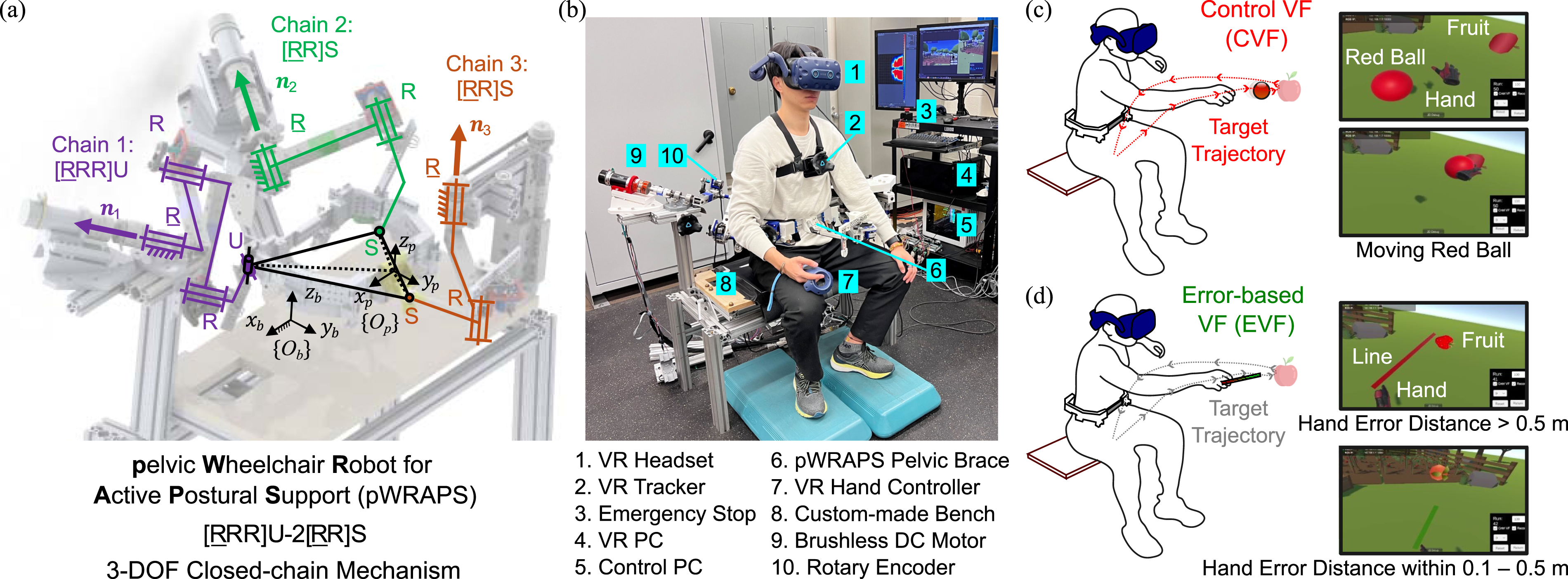
2.1.1. Transparent mode
Motors operate in zero-force control mode, where the controller outputs zero torques on the user, allowing unimpeded voluntary movement. The motors also actively compensate for the weight of the robot structure, so the user does not perceive the device’s weight. During user-initiated motion, the pelvic brace movement is recorded as a motion template or for assessment.
2.1.2. Trajectory mode
The pelvic brace trajectory recorded in the transparent mode is used to compute the desired motor shaft angles. A proportional-integral-derivative (PID) feedback position controller regulates the current in the motor to follow these varying target shaft angles. Additionally, the trajectory replay speed can be adjusted, for example, half (0.5×) or twice (2×) the original speed, within the training protocol.
2.2. Participants
Thirty-two able-bodied young adult subjects (10 females and 22 males) voluntarily participated in the study with an average age of 26.1 years (SD = 3.6 yr, range: 20–34 yr), 173.2 cm average height (SD = 11.5 cm, range: 150.0–198.0 cm), and 69.1 kg average weight (SD = 13.4 kg, range: 45.5–94.1 kg). Thirty-one subjects were right-hand dominant and one subject was ambidextrous. All could fit the pelvic brace within its adjustable range. The experiment protocol was approved by the Institutional Review Board (IRB) of Columbia University (Protocol No. AAAR7388). All participants provided written informed consent before the experiment. No subject had previous history of VR sickness, a neurological condition or musculoskeletal abnormalities (e.g., atypical spinal alignment, chronic musculoskeletal pain, or balance impairments). The entire experiment lasted about an hour, including setup, with each subject completing roughly 12 min of active VR trials.
2.3. Experimental setup and protocol
The experiment was conducted in a quiet room within a 2.5 m × 2.5 m area, with the pWRAPS bench positioned at the center of the work area. Four Vive Base Stations 2.0 (HTC, Taoyuan, Taiwan) were mounted on an overhead aluminum frame to track a Vive Pro headset, a Vive hand controller, and three Vive Trackers 2.0. The three trackers were placed on the stationary bench, the pelvic brace, and the subject’s chest. The VR application was developed in Unity (version 2022.3.13f1, Unity Technologies, San Francisco, CA) using Unity’s Robotics Hub and SteamVR, and streamed real-time pose data of the controller and the trackers to the Control PC via the ROS TCP Connector (Unity Technologies, 2021).
To begin setup, the pelvic brace was adjusted to fit the subject’s waist, with foam pads added to prevent slippage during movement. A footrest supported the feet to maintain an upright seated posture with 90° knee flexion. The pWRAPS kinematic model was updated to match the adjusted brace dimensions. The subject was then equipped with a chest-mounted tracker, a VR headset, and a right-hand controller (Figure 1(b)). The experimental protocol (Supplemental Video), shown in Figures 2(a)–(e), consisted of five sessions (1–2 min break in-between sessions): (a) Calibration: Subjects pushed balloons to determine maximum reach distances in four directions. (b) Baseline recording: Self-paced hand trajectories were recorded during maximum reaches. (c) Pre-test: Subjects tracked a red ball (Control VF) moving at twice the speed (2×) of their baseline hand path. (d) Reach game: Subjects experienced combinations of hand target visual feedback, Control VF (CVF) or Error-based VF (EVF), and robotic pelvic guidance, Unguided (U) or Guided (G), via pWRAPS; The Guided (G) group: pWRAPS moved at twice the speed (2×) of the baseline pelvic trajectory. (e) Post-test: Identical to the Pre-test; 1–2 min break in-between sessions. (f) Four reaching directions.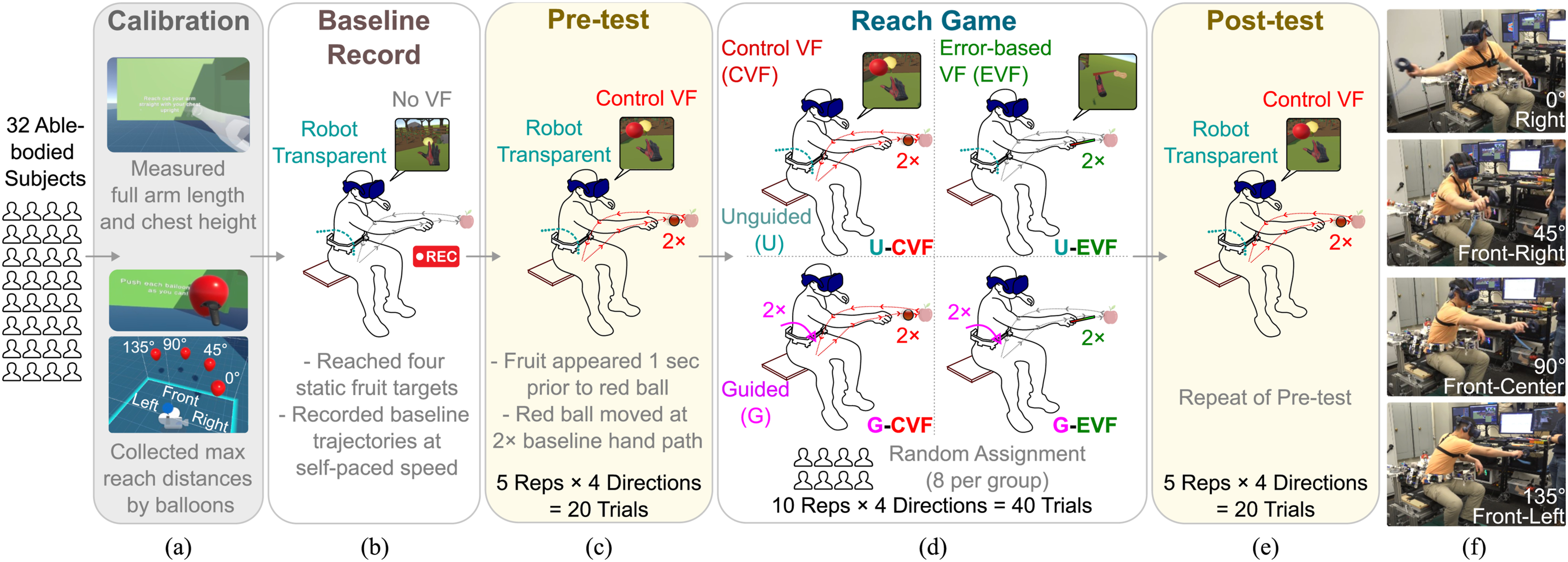
2.3.1. Calibration
The calibration scene featured a blue ground and green wall (Figure 2(a)), where subjects followed on-screen instructions and used a transparent mannequin for posture guidance to collect anthropometric data, including arm length and chest height. To determine maximum reach distances, subjects pushed virtual balloons constrained along four directions (0°: Right, 45°: Forward-Right, 90°: Forward-Center, and 135°: Forward-Left), as shown in Figure 2(f). These directions were chosen to elicit the variations in upper-body coordination, based on prior findings on direction-dependent motor control strategies (Dean and Shepherd, 1997). The pWRAPS controller remained in transparent mode (see Section 2.1.1) throughout the session.
2.3.2. Baseline record
This session recorded baseline reaching movements at the subject’s self-paced speed (Figure 2(b)). The VR environment was switched to a farm-themed scene, with pWRAPS in transparent mode. Four fruit targets (in 0°, 45°, 90°, and 135° directions) appeared one at a time in random order at the subject’s calibrated maximum reach positions, located midway between chest and pelvis heights. A preview of the four targets was shown before recording began.
Starting from a neutral seated position with the right hand on the lap, subjects reached for each target using the right-hand controller and returned to the initial posture after the target disappeared upon contact. Each reach was completed within 10 s, followed by a 3-s rest. A 3D hand model, measured by the VR controller, was the only visible body part. Instructions and a countdown timer were displayed throughout. Hand, chest, and pelvis trajectories were recorded as baseline templates for subsequent sessions, reflecting movement performed in a controlled, self-paced posture.
2.3.3. Pre-test
This session assessed the subject’s ability to track a fast-moving hand target in the VR environment (Figure 2(c)), where the robot remained transparent. In each trial, a fruit appeared to cue the target direction, and one second later, a red ball (0.16 m diameter) appeared and started to move, representing the Control Visual Feedback (CVF). Using the right-hand controller, the subject followed this red ball, which replayed their baseline hand path at twice the original speed (2×), as shown in Figure 1(c). Each movement included outbound and return paths completed within 5 s, followed by a 3-s rest. Participants were instructed to touch the fruit target while closely following the target hand path. Fruit directions were randomized and repeated five times, totaling 20 trials.
2.3.4. Reach game
This session evaluated subjects’ performance while tracking the same 2× hand-path targets. Participants were randomly assigned to one of four groups (n = 8 each) in a 2 × 2 factorial design based on pWRAPS guidance (Unguided, U; Guided, G) and VF type (Control VF, CVF; Error-based VF, EVF) (Figure 2(d)).
In the G condition, pWRAPS operated in trajectory mode (see Section 2.1.2), tracking each subject’s baseline pelvic trajectory at twice the original speed, synchronized with the hand target. Participants in the G condition were instructed to complete the same task while receiving pWRAPS actuation. In the U condition, pWRAPS remained in transparent mode.
In the EVF condition, the red ball of the CVF (described in Pre-test Section 2.3.3) was replaced by a 3D line linking the subject’s hand position to the current target point on the baseline path (Figure 1(d)). Line color indicated tracking error: red (
Each of the four reaching directions was repeated 10 times, totaling 40 trials—a dosage shown to support motor adaptation and performance assessment (Cirstea et al., 2003).
2.3.5. Post-test
This session evaluated subjects’ movements following exposure to the Reach Game (Figure 2(e)). All subjects repeated the Pre-test task, performing 20 trials with pWRAPS in transparent mode.
The 2× speed was based on pilot trials, where the fastest reaches by subjects took roughly half the time of self-paced movements. Because the template is derived from each participant’s own baseline, the 2× scaling is guaranteed to be feasible across subjects, standardizing the relative challenge level without imposing an arbitrary absolute speed. The speed scaling was chosen over alternative task manipulations (e.g., varied reaching distances or directions) because it preserves a consistent spatial reference template for RMSE-based pre-to-post comparison while increasing temporal challenge. Varying distance or direction would change spatial demands and require condition-specific templates, complicating interpretation of guidance effects.
This created a challenging condition requiring full ROM at a higher speed while maintaining the upper-body coordination toward a target at the boundary of one’s reach workspace, mirroring the difficulties faced by individuals with impaired trunk control (Peeters et al., 2018a). Critically, the 2× scaling applies to the full coordination template, not merely to the hand target speed: each participant’s baseline trial captures a naturally coordinated pelvis–trunk–hand movement with substantial trunk involvement, and the training target is this pattern reproduced at double speed. Although faster movements typically reduce trunk involvement when participants are free to choose their own strategy, our paradigm assigns a full-ROM coordination template as the tracking target; the 2× scaling therefore requires the participant to move all segments, including the trunk, at double speed, actively engaging rather than bypassing proximal coordination. This approach aligns with rehabilitation goals to retrain coordinated trunk–arm movements and reduce over-reliance on any single segment (Cirstea and Levin, 2000; Levin and Demers, 2021; Peeters et al., 2018a).
2.4. Sense of agency rating
At the end of each Pre-test, Reach Game, and Post-test session, participants responded to the same survey question: “How strongly did you feel you could control the error between your hand and the moving target?” Responses were recorded using a 7-point Likert scale, where 1 indicated no control and 7 indicated full control (Aoyagi et al., 2021; Likert, 1932).
Participants were not provided with additional feedback or numerical scores during any phase of the experiment. These choices were made so that the SoA ratings were not influenced by performance feedback (Hooyman et al., 2020; Kumar et al., 2014; Synofzik et al., 2008).
2.5. Data analysis
2.5.1. Reach phase segmentation
Data from the VR trackers and pWRAPS were synchronized and resampled at 50 Hz. Hand position data in the (x, y, z) directions were first filtered using a fourth-order Butterworth low-pass filter with a cutoff frequency of 2.5 Hz. Hand velocity was then computed from the filtered position signals using a first-order numerical derivative. The start of each reach interval was defined as the time point when the target hand speed exceeded 10% of the peak outbound speed, and the end was defined as the time point when the target hand speed dropped below 10% of the peak return speed (Marchesi et al., 2022). A representative trial is shown in Figure 3, where the shaded gray region denotes the segmented reaching interval used for computing performance scores. Representative trajectories during a front-center reach trial: (a) Hand position, (b) Pelvis–Seat, (c) Trunk–Pelvis, and (d) Hand–Trunk segment. Hand RMSE (Task Score) and Hand–Trunk weighted RMSE are expressed as a percentage of the baseline path length (PL), while Pelvis–Seat and Trunk–Pelvis RMSE are reported in degrees. Dotted lines represent target trajectories (2× baseline), solid lines indicate measured trajectories, and the shaded region denotes the reach interval derived from the target hand trajectory.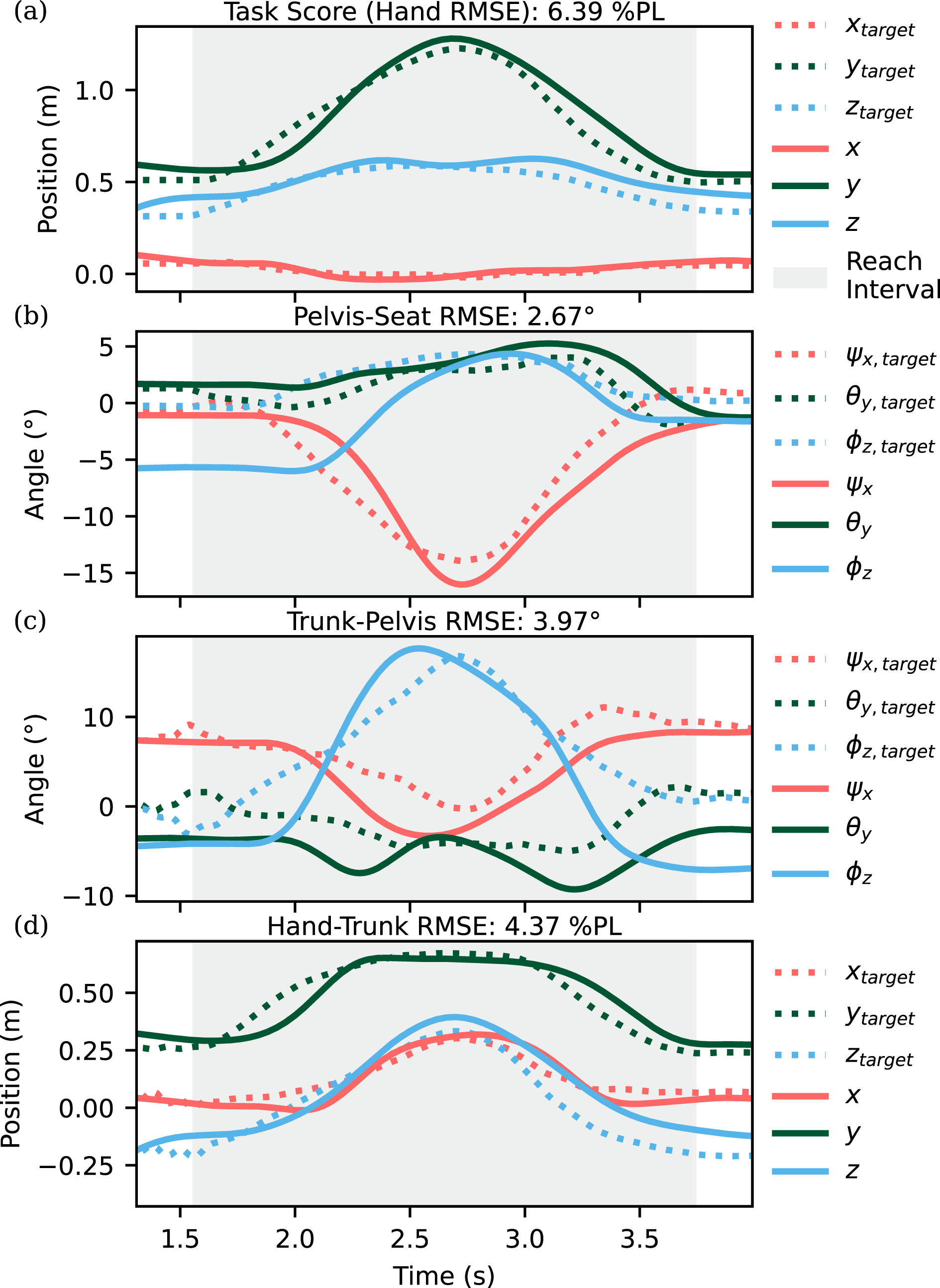
2.5.2. Reach task score
Hand-tracking performance in each trial was quantified using the root-mean-square error (RMSE) between the actual hand position and the hand target trajectory. The Task Score (Hand RMSE) was computed as:

2.5.3. Segmental coordination scores
Upper-body coordination was assessed using three relative motions between body segments: (1) pelvic rotation with respect to the seat frame {O b } (Pelvis–Seat), (2) thoracic rotation, measured by the chest tracker, relative to the pelvic frame {O p } (Trunk–Pelvis), and (3) hand position (x, y, z) relative to the thoracic frame (Hand–Trunk). Rotations were decomposed into pitch (ψ x ), roll (θ y ), and yaw (ϕ z ), corresponding to the sagittal, frontal, and transverse planes, respectively. Local coordinate axes at the neutral pose were defined as: x mediolateral, y anteroposterior, and z vertical.
To quantify deviated coordination from the baseline, the Segment weighted RMSE (Segment RMSE) was computed for each relative movement as:

Target (2× baseline speed, described in Section 2.3.3) and actual segmental movements, captured via VR trackers, are shown in Figures 3(b)–(d). Trial-level RMSE values, indicating trajectory mismatches, are displayed in the title of each plot. This representative Forward-Center (90°) reach involved dominant sagittal-plane pitch (ψ x ) in the Pelvis–Seat segment. The Trunk–Pelvis segment exhibited combined pitch and yaw (ψ x , ϕ z ), reflecting trunk flexion and leftward rotation to advance the right shoulder. The Hand–Trunk trajectory showed prominent vertical (z) displacement with minor positive x and y motion, consistent with coordinated shoulder flexion and horizontal abduction.
2.6. Statistical analysis
Statistical analyses were performed using R (version 4.4.3) (R Core Team, 2025). A two-tailed alpha level of 0.05 was used to determine statistical significance.
2.6.1. Correlation between task and coordination scores (H1)
A linear mixed-effects model (LMM) was used to test how segmental coordination influences task performance (H1), focusing on the Post-test session, which reflects natural, unassisted behavior after training.
The model was fit to trial-level data (640 trials total; 20 trials per participant across five repetitions of four directions) using Restricted Maximum Likelihood (REML) estimation with Satterthwaite approximations for degrees-of-freedom. Task Score (Hand RMSE) was the dependent variable, with fixed effects for segmental coordination scores (Pelvis–Seat, Trunk–Pelvis, Hand–Trunk), Robot condition (U, G), VF type (CVF, EVF), and their interaction (Robot × VF). A random intercept for subject ID accounted for repeated measures.
Trials with standardized residuals beyond ±3 were considered extreme outliers and excluded. Additional diagnostics confirming model assumptions are (1) residual normality, (2) homoscedasticity (residuals vs fitted plots), (3) multicollinearity using variance inflation factors (VIF), and (4) influential observations (Cook’s distance).
2.6.2. ANOVA of reach score change (H2)
Mean ± SD of scores across four groups and sessions.
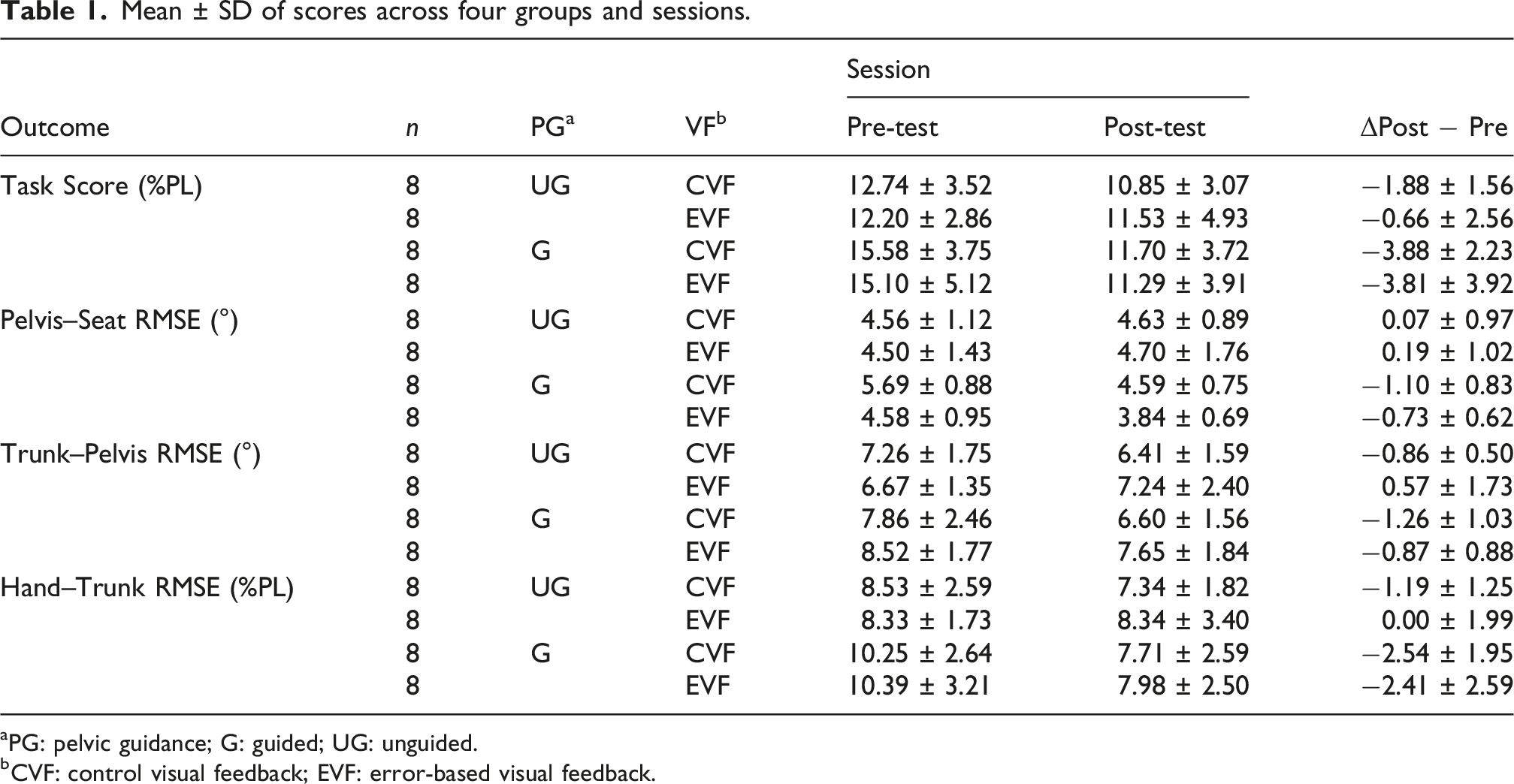
aPG: pelvic guidance; G: guided; UG: unguided.
bCVF: control visual feedback; EVF: error-based visual feedback.
One-way ANOVAs, or the Kruskal–Wallis test when parametric assumptions were violated, confirmed that there were no significant differences in pre-test scores across the four groups for any outcome measure (Table 6 in Supplemental material). Specifically, the Shapiro–Wilk test indicated non-normality for the Guided-EVF group on Pelvis–Seat pre-test scores (W = 0.815, p = .042); accordingly, the non-parametric Kruskal–Wallis test was used for the Pelvis–Seat baseline comparison. All other baseline measures satisfied the normality assumption (p > .05) and were analyzed with one-way ANOVA.
2.6.3. A Bayesian model of SoA rating (H3)
To model SoA ratings in relation to experimental conditions and performance metrics (H3), we employed a Bayesian cumulative ordinal logistic regression model (BCLM) (Bürkner, 2017). This approach is consistent with predictive coding theories, postulating that SoA emerges from the brain’s hierarchical inference about self-generated outcomes, integrating prior beliefs with sensory evidence. These inferences are shaped both by low-level sensorimotor signals and higher-level cognitive interpretations, such as intentions and beliefs about control (Friston, 2012; Synofzik et al., 2008).
The ordinal model treats Likert-scale responses as categorical outcomes originating from a continuous latent variable, θ, representing internal SoA (Haggard, 2017; Samejima, 1968). This latent variable is approximated by a linear predictor, η
i
, which captures the influence of observed predictors on each trial. The probability of selecting a specific SoA rating (1–7 scale) is modeled using a cumulative logit link function (see Supplemental material):
Using the BCLM, we estimate posterior distributions for the regression coefficients
3. Results
3.1. Reaching range of motion
Mean ± SD of baseline reach ROM (n = 32).
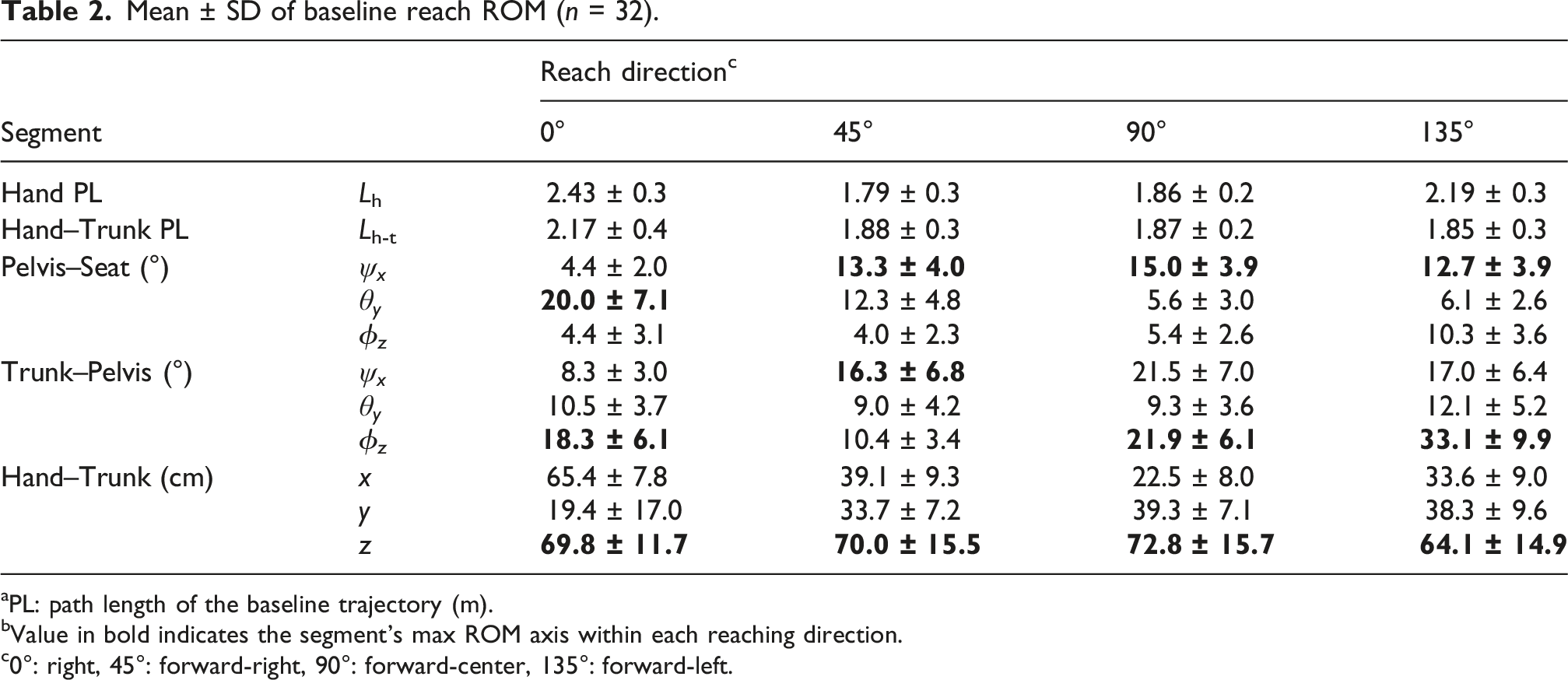
aPL: path length of the baseline trajectory (m).
bValue in bold indicates the segment’s max ROM axis within each reaching direction.
c0°: right, 45°: forward-right, 90°: forward-center, 135°: forward-left.
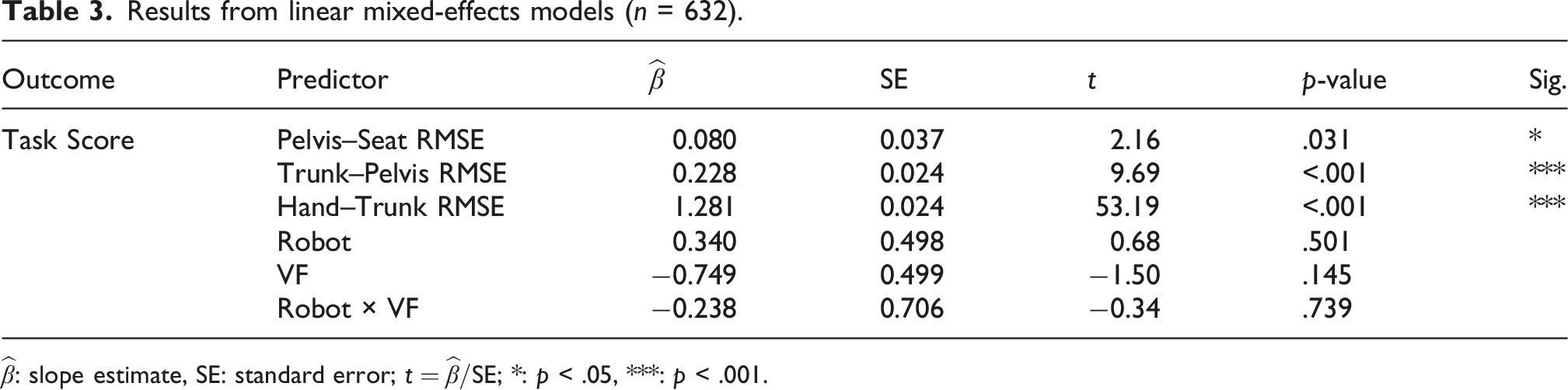
3.2. Linear mixed-effects model of task performance (H1)
Results from linear mixed-effects models (n = 632).
3.3. ANOVA of performance changes (H2)
Two-way ANOVA (type II) results of score changes (Δ).
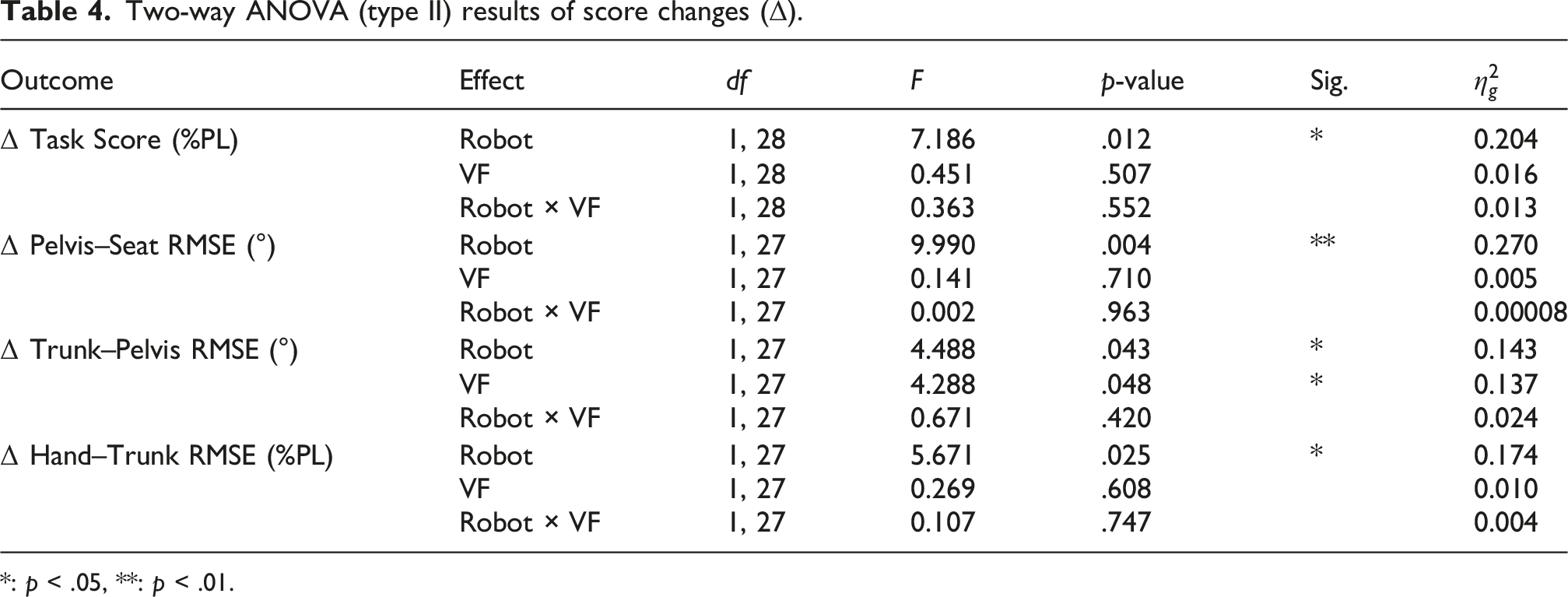
*: p < .05, **: p < .01.
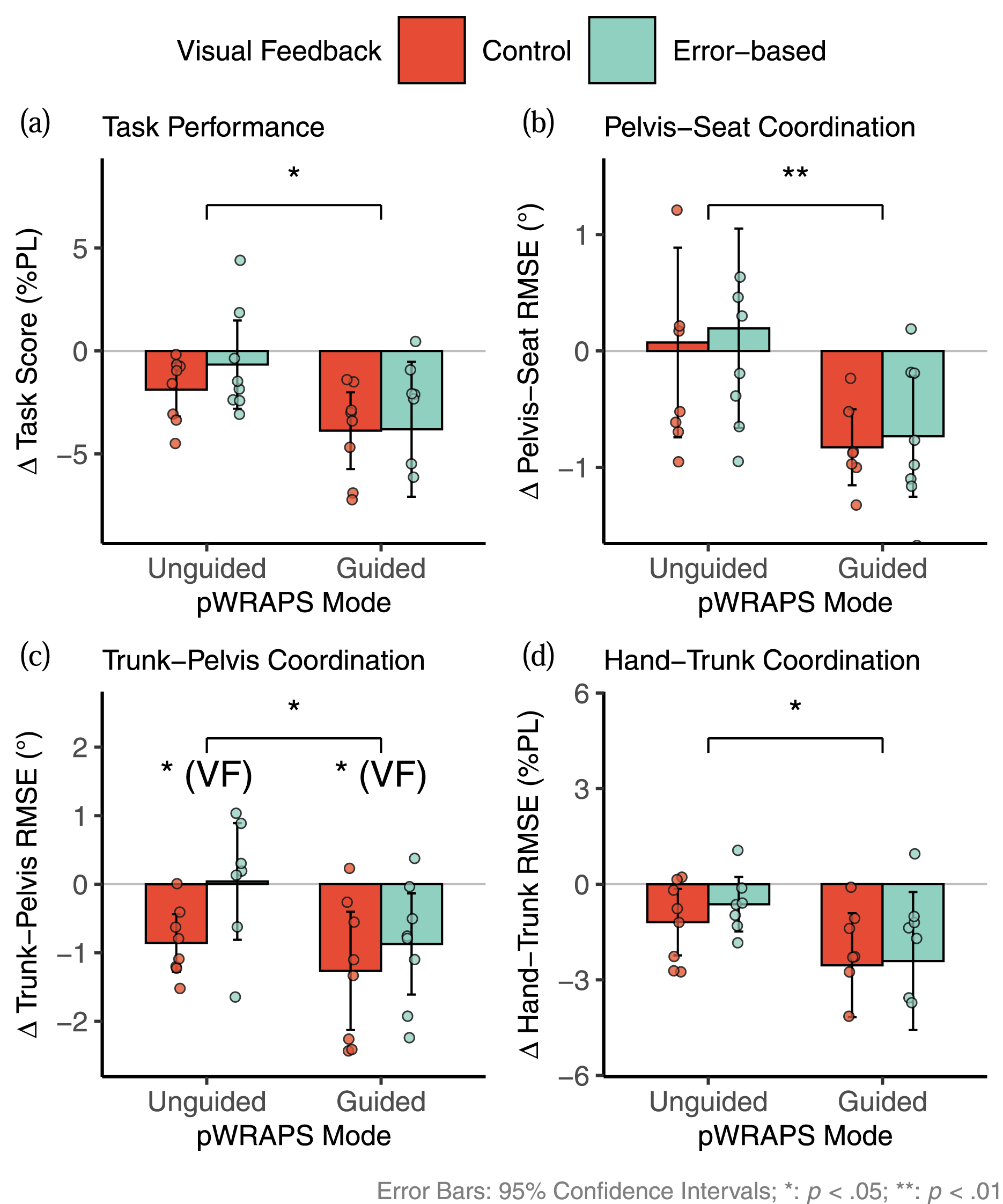
Individual changes (Δ) from pre-test to post-test across all directions for (a) task score, (b) pelvis–seat RMSE, (c) trunk–pelvis RMSE, and (d) hand–trunk RMSE. Negative values indicate improved performance, with zero indicating no change.
The strongest effect was found in Δ Pelvis–Seat RMSE (F (1, 27) = 9.99, p = .004; MD = −0.91°, 19.64%Avg; Figure 4(b)). Significant effects of guidance were also seen in Δ Trunk–Pelvis RMSE (F (1, 27) = 4.49, p = .043; MD = −0.63°, 8.66%Avg) and Δ Hand–Trunk RMSE (F (1, 27) = 5.67, p = .025; MD = −1.55%PL, 18.00%Avg), shown in Figures 4(c) and (d), respectively. These findings confirm that active pelvic guidance led to significantly higher reduction in trajectory errors across all segments, especially at the pelvis, regardless of VF condition.
A main effect of VF was also found for Trunk–Pelvis coordination (F (1, 27) = 4.29, p = .048), with the EVF group showing smaller improvements than the CVF group (EVF-CVF: MD = +0.64°, 8.74%Avg), suggesting that EVF was less effective for reducing trunk coordination error (Figure 4(c)).
All significant results yielded moderate to large effect sizes (
3.4. Bayesian model of SoA ratings (H3)
Figure 5 shows mean and individual SoA ratings across sessions and conditions. Although SoA was rated on a 7-point Likert scale, no responses were recorded in categories 1 or 2, which is typical for able-bodied participants. The ordinal model, therefore, estimated four thresholds (τ1–τ4) separating the five observed categories (3–7). Mean sense of agency (SoA) ratings across sessions for each experimental condition. Dots represent individual subject ratings. Error bars indicate 95% confidence intervals of the group means.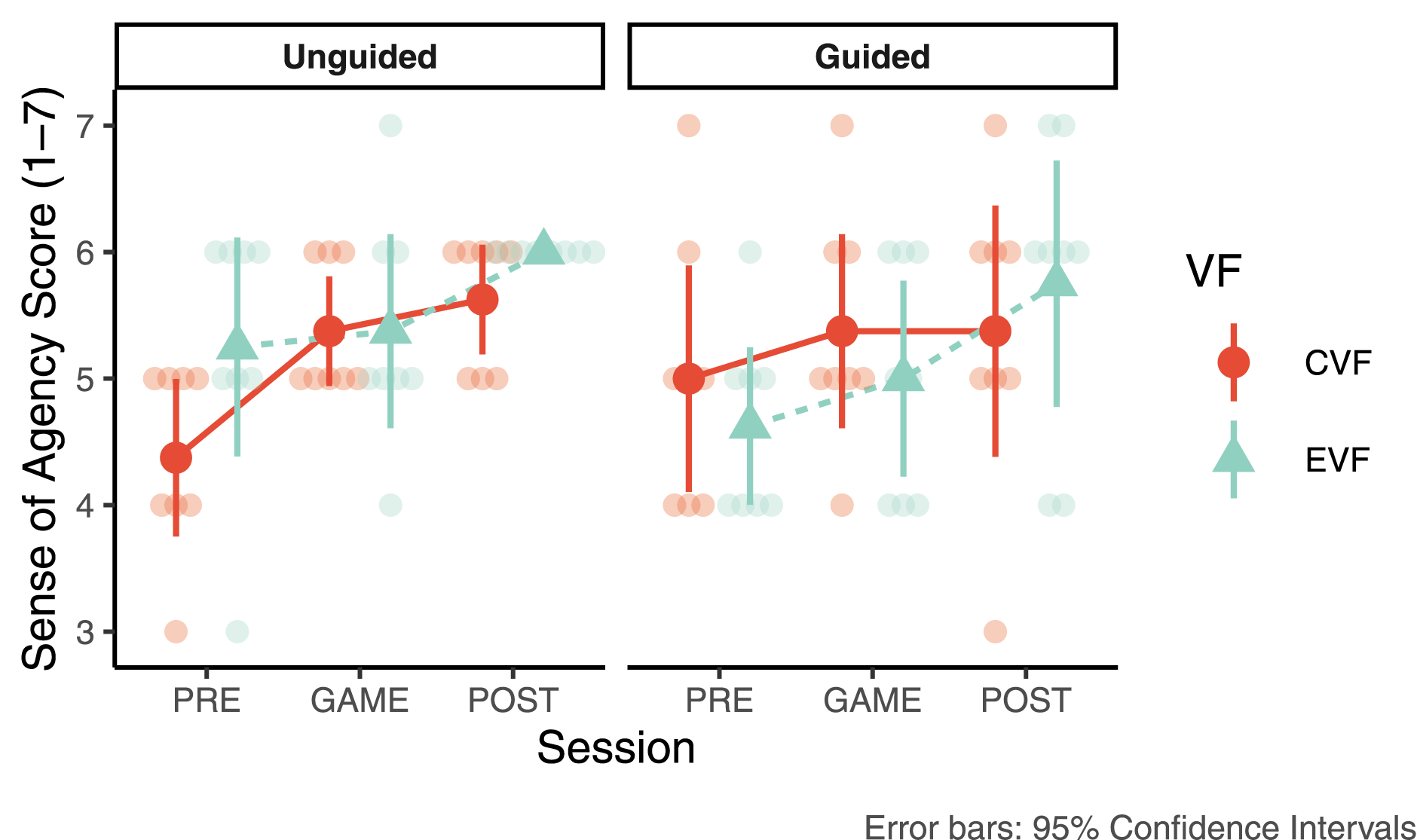
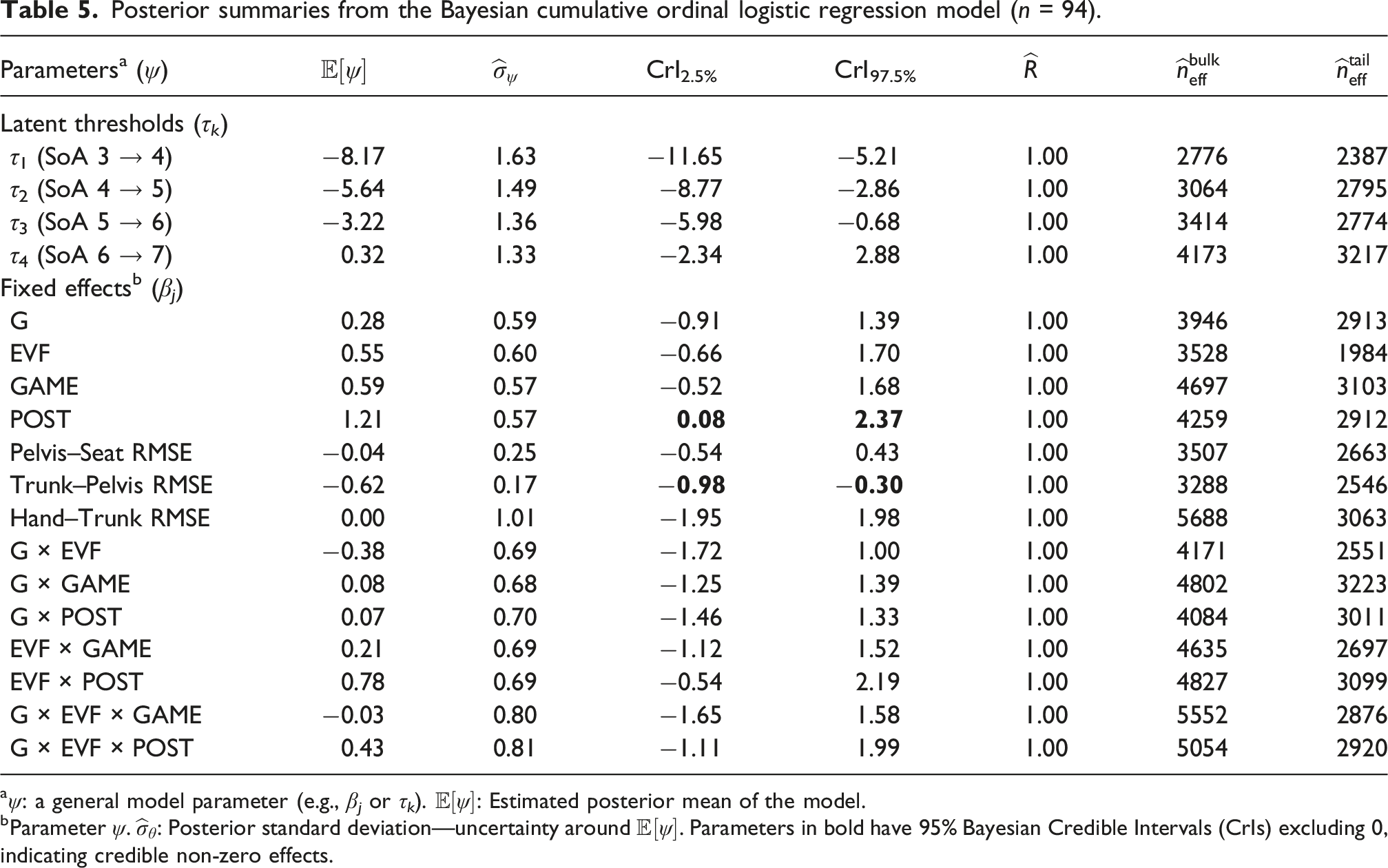
To examine predictors of SoA, we compared several BCLMs. The base model included only experimental conditions (Robot, VF, and Session), while extended models added coordination RMSEs (Pelvis–Seat, Trunk–Pelvis, and Hand–Trunk). Task Score was excluded due to high multicollinearity (VIF >17); all remaining RMSE predictors had VIF <2.0. Outlier filtering based on a 3× IQR criterion removed two extreme RMSE values, reducing the dataset from n = 96 to n = 94 while preserving the factorial structure.
All models used weakly informative priors:
Posterior summaries from the Bayesian cumulative ordinal logistic regression model (n = 94).
aψ: a general model parameter (e.g., β
j
or τ
k
).
bParameter ψ.
Figure 6(a) displays the posterior means (a) Posterior means and 95% Bayesian Credible Intervals (CrIs) of fixed effects from the Bayesian cumulative ordinal logistic regression model (BCLM); credible non-zero effects are shown in blue. (b–d) Predicted probabilities of sense of agency (SoA) categories (3–7) by Pelvis–Seat, Trunk–Pelvis, and Hand–Trunk RMSEs, conditional on reference levels and mean values of other RMSEs. (e) Predicted SoA probabilities by Trunk–Pelvis RMSE across sessions and VF conditions within the Unguided group. Shaded bands represent 95% CrIs.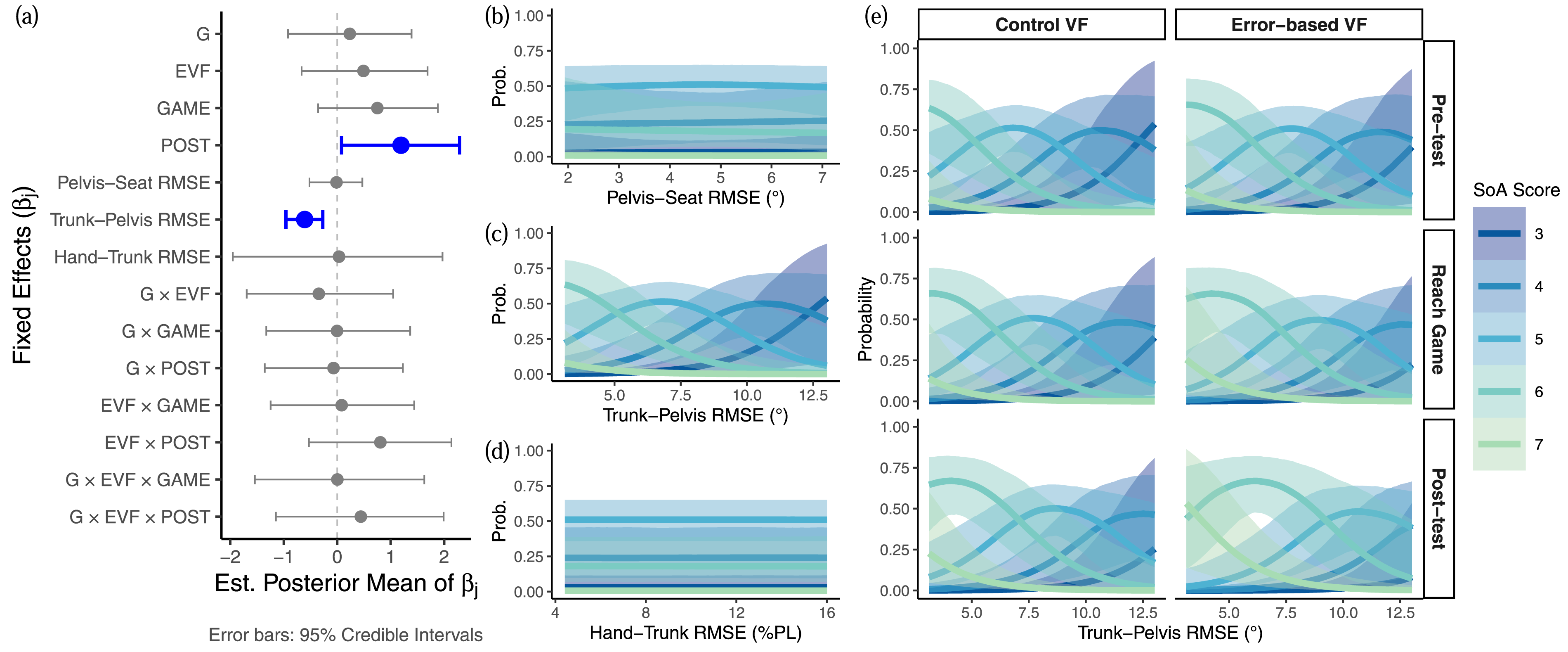
Figures 6(b)–(d) show predicted SoA probabilities (3–7) as functions of segment-level RMSEs, based on (3). Predictions are conditional on reference levels (Pre-test, Unguided, Control VF) and mean values of other RMSEs. Trunk–Pelvis RMSE (Figure 6(c)) showed the strongest gradient, with greater error linked to lower SoA probabilities, highlighting its effect on perceived agency.
Figure 6(e) shows predicted SoA probabilities by Trunk–Pelvis RMSE across sessions and VF conditions under the Unguided setting. Higher SoA ratings were more likely in the Post-test session at equivalent RMSE levels, consistent with the positive fixed effect of Post-test. A similar, though non-credible, trend appeared during the Reach Game (
Lastly, a spline-based model was tested to capture a potential nonlinear effect of Trunk–Pelvis RMSE. Although it slightly improved predictive accuracy (Δelpd = 3.2, SE = 2.2), the Bayes factor (BF = 0.57) provided only weak support. Given the marginal improvement and reduced interpretability, the linear model was retained. The proportional odds assumption was also upheld, as category-specific effects showed no credible deviation from proportionality.
4. Discussion
4.1. Task score and segmental coordination (H1)
Results from the linear mixed-effects model (Section 3.2) show that seated reaching performance is strongly linked to whole upper-body coordination, with Hand–Trunk RMSE emerging as the most reliable predictor of Task Score. The hierarchical β weights, Hand–Trunk (β = 1.281)
The absence of significant effects from training modalities (Robot and VF) supported our first hypothesis (H1), showing that the relationship between coordinated motion and task success remained stable across feedback conditions. These findings further validate self-paced coordination patterns as effective templates for task execution.
Segment-level coordination scores were designed to reveal deviations that might be masked by accurate global hand trajectories under kinematic redundancy. Each score is computed against a fixed reference template, which serves as a stable benchmark for meaningful pre-to-post comparison; an adaptive template that recalculates distal segment references to account for the actual proximal segment deviations would obscure the very coordination changes we aim to detect, complicate interpretation, and risk rewarding unnatural compensatory strategies. However, in a serial kinematic chain, errors in proximal segments (pelvis) alter the coordinate frame in which more distal segments operate, meaning that large pelvic errors can propagate upward and amplify trunk and hand penalties through compensatory adjustments. This propagation is not an artifact but a clinically relevant feature: it captures how poor pelvic control degrades downstream coordination. Despite these trade-offs, adherence to the fixed template consistently correlated with better task performance, and multicollinearity among scores remained acceptable.
4.2. Motor adaptation from pelvic guidance and visual feedback (H2)
The results in Section 3.3 support Hypothesis 2, indicating that active pelvic guidance provides postural control benefits as evident in its significant main effect on Pelvis–Seat RMSE regardless of VF. This highlights the influence of pelvic guidance in facilitating postural configuration and intersegmental coordination of the upper body during accurate hand movements. The added somatosensory cues likely enhanced sensorimotor integration, improving motor planning and online control (Manson et al., 2019). The lack of interaction between pelvic guidance and VF suggests that these two modalities operated on different segments: pelvic guidance improved proximal control, while VF primarily influenced distal hand control.
The type of VF, however, differentially affected the intermediate trunk–pelvis segment. EVF led to smaller Trunk–Pelvis improvements than CVF, likely reflecting an attentional capacity mechanism. Continuous error visualization in EVF, a real-time line connecting hand to target, increases cognitive demand relative to the simpler pursuit-tracking stimulus in CVF (Wulf, 2013), drawing attention to the hand–target mismatch and encouraging a distal correction strategy that prioritizes rapid hand adjustments at the cost of coordinated whole-body movement. This is consistent with visual dominance during fast reaches (Saunders and Knill, 2003), where high-demand VF promotes a more segmented coordination strategy that favors distal accuracy over proximal engagement (Engel et al., 2021). Notably, EVF did not hamper hand–trunk coordination; participants demonstrated effective error correction despite the increased visual demands, possibly due to the low inertia of their upper limbs and intact motor control. The trade-off was instead borne by the pelvis: participants receiving EVF without pelvic guidance showed a trend toward reduced pelvic control (positive Δ Pelvis–Seat RMSE). Critically, this negative effect was absent when pelvic guidance was provided, indicating that somatosensory input at the pelvis can counteract the attentional cost of complex VF.
These findings have practical implications for feedback design. Rather than assuming that more error information is always beneficial, clinicians should consider which body segments need engagement. A progressive strategy may be optimal: CVF early in training to establish whole-body coordination patterns, followed by EVF in later sessions to refine distal accuracy once the proximal postural foundation is stable.
With n = 8 per group, baseline randomization is inherently imperfect and numerical trends toward imbalance may exist despite non-significant one-way ANOVA and Kruskal–Wallis tests. Individual change scores (Δ = Post − Pre) partially mitigate this concern, though differential regression to the mean remains possible. Regarding functional interpretation, the 19.64%Avg reduction in Pelvis–Seat RMSE under guidance corresponds to approximately 0.91° improvement in pelvic tracking accuracy. Although no minimal clinically important difference (MCID) exists for this novel metric, this represents nearly one-fifth of the cohort-average error (%Avg) from a single 10-min exposure, and the significant effect (p = .004) was consistent across participants (Figure 4(b)). In comparison, TruST interventions in children with CP yielded a 233% increase in workspace area after 12 sessions (Santamaria, Khan, et al., 2020), suggesting that multi-session pWRAPS protocols could produce substantially larger effects.
4.3. Influence of trunk–pelvis coordination and VF on SoA (H3)
Across conditions, participants reported progressively higher SoA scores over time, suggesting improved perceptual-motor fluency (Section 3.4). However, neither pelvic guidance nor VF showed statistically credible effects on SoA. Instead, SoA was strongly associated with Trunk–Pelvis coordination, where improved trunk control was directly linked to higher SoA. The upper trunk’s high mobility without direct feedback supports the notion that agency emerges subconsciously from self-generated movements (Haggard, 2017), aligning with models integrating predictive and inferential processes (Friston, 2012; Synofzik et al., 2008). Thus, only part of Hypothesis 3 was supported: Trunk–Pelvis coordination was the strongest predictor of SoA, while guidance and VF showed no direct effects.
The absence of a significant guidance × VF interaction on SoA is informative when considered alongside this finding. Agency in our paradigm appears driven by the felt quality of coordination rather than by the presence or absence of robotic assistance. Guided participants were aware that external forces would be applied by the robot during reaching, but pelvic forces were temporally synchronized with the participant’s reaching movement, producing no mismatch between the felt assistance and the intended action. This temporal congruence likely preserved the sensorimotor prediction–outcome match that underpins SoA (Friston, 2012; Synofzik et al., 2008), making the guidance feel consistent with self-generated movement. This is consistent with prior work showing that assistance-induced performance improvements can be self-attributed by the user (Inoue et al., 2017); pelvic guidance further acts on a segment far from the primary locus of visual attention (the hand–target relationship), so Guided participants may have experienced smoother coordination without consciously attributing it to the robot.
From a rehabilitation design perspective, the null interaction is a positive finding: robotic pelvic guidance can improve coordination without diminishing perceived agency, indicating that the biomechanical and psychological goals of rehabilitation are compatible rather than in conflict (Davis et al., 2025). However, a stronger or more perceptible form of guidance, one that overrides rather than facilitates the participant’s intended pelvic motion, could reduce SoA. The temporally-synchronized, non-overriding character of pWRAPS guidance may be critical for preserving agency. Future studies should parametrically vary guidance intensity to identify the threshold at which external assistance begins to diminish perceived control.
Interestingly, participants exposed to EVF tended to report higher post-test SoA despite similar coordination levels, especially those transitioning from EVF to CVF. This rebound suggests that EVF may serve to recalibrate internal forward models that predict sensory outcomes of motor commands (Shadmehr et al., 2010; Taylor et al., 2014), updating and strengthening the sensorimotor prior. Returning to CVF likely reduced prediction errors and enhanced sensorimotor congruence, reinforcing agency attribution (Cressman and Henriques, 2009; Miall and Wolpert, 1996).
The observed SoA pattern, similar ratings at Pre-test and during the Reach Game with a significant increase at Post-test, admits three non-mutually-exclusive explanations. First, accumulated motor learning: the Post-test was the first opportunity to perform independently after training, and participants whose coordination had improved would naturally experience enhanced agency (Haggard, 2017; Synofzik et al., 2008), consistent with the strong Trunk–Pelvis RMSE–SoA association. Second, for Guided participants, removal of robotic assistance at Post-test provided clear evidence that their gains were self-generated, an “agency revelation” effect that could reinforce self-efficacy (Inoue et al., 2017). Third, a contrast effect: participants may have rated Post-test agency higher because they implicitly compared it against their earlier, less coordinated performance. Clinically, the finding that SoA increases primarily after training rather than during it suggests that real-time SoA feedback may not be necessary if agency consolidates post-training. Future robotic rehabilitation protocols might instead use indirect indicators such as Trunk–Pelvis coordination quality to modulate guidance intensity in real time, reserving explicit SoA assessment for post-session evaluation.
4.4. VR as a training context: Transfer considerations
An important question that has been raised when using VR as the training platform is whether coordination improvements acquired in VR transfer to real-world (non-VR) performance. Yarossi et al. (2021) proposed that VR constitutes a distinct sensorimotor context: when visual–vestibular conflicts are large, VR-learned motor representations may become “quarantined” and fail to generalize outside the headset. This context-dependency framework has significant implications for VR-based rehabilitation.
However, the degree of context-specificity depends on the magnitude of the sensory discrepancy between the VR and real-world environments (Yarossi et al., 2021). In our paradigm, participants were physically seated with the robot and performed real upper-body reaching movements. The somatosensory and vestibular inputs, including the interaction forces at the pelvis delivered by pWRAPS, the proprioceptive signals from the moving limbs and trunk, and the gravitational reference from the upright seated posture, were all consistent with the physical environment. Unlike locomotion-based VR paradigms, where visual optic flow implies self-motion while the vestibular system signals that the body is stationary, our setup does not introduce sensory conflict. The VR headset served solely as an alternative visual display; it did not alter the sensorimotor dynamics of the reaching task. This makes our paradigm at the low-conflict end of the Yarossi et al. (2021) spectrum, where transfer is least likely to be impeded. Moreover, the pelvic guidance provided by pWRAPS is a haptic–motor intervention that shapes coordination through physical interaction with the pelvis, not through visual mechanisms. The coordination patterns learned under robotic guidance, improved pelvis–seat coupling and more efficient trunk–pelvis sequencing, are biomechanical adaptations that are not inherently tied only to the visual display modality.
Nonetheless, we acknowledge that the present study did not include a post-training assessment without the VR headset, and therefore cannot empirically confirm transfer. We identify this as a limitation and a priority for future work (see Section 5).
4.5. Implications for trunk postural rehabilitation
Trunk–pelvis coordination emerged as a key target for adaptive guidance in seated postural rehabilitation using robotic exoskeletons and VR. This segment demonstrated the greatest mobility, showed the strongest association with SoA, and was influenced by somatosensory and visual cues from adjacent body segments, pelvic guidance from below and visual feedback at the hand from above. Progressive feedback strategies, switching between error-based cues (EVF) and a direct visual target (CVF), may facilitate postural recovery while promoting movement ownership, which is critical for long-term adherence. However, higher SoA does not always indicate better coordination, as complex visual cues can obscure postural sensorimotor adaptability, especially in patients with lower baseline control. Thus, perceived control should be interpreted with care, and complex VF should be properly selected and paired with proprioceptive inputs, such as active pelvic guidance, to enhance training effectiveness.
The primary target populations for pWRAPS-based training are individuals with residual trunk motor function who exhibit pelvic instability limiting seated upper-body coordination: (1) incomplete SCI classified as AIS C or D at thoracic or low cervical levels (Santamaria, Luna, et al., 2020); (2) chronic stroke with moderate trunk impairment (e.g., Trunk Impairment Scale) and sufficient motor capacity for active reaching; and (3) children with CP at GMFCS levels III–IV with low-thoracic trunk control deficits (Santamaria, Khan, et al., 2020). Motor-complete SCI (AIS A–B) would be excluded from this paradigm. Unlike trunk-level assist-as-needed systems such as TruST, pWRAPS actively mobilizes the pelvis across three rotational degrees-of-freedom, making it suited for individuals whose pelvic instability requires direct guidance rather than trunk support alone.
A clinical implementation could follow protocols validated in pediatric postural rehabilitation (Santamaria, Khan, et al., 2020), comprising multiple training sessions (e.g., 3 sessions per week over 2–4 weeks). pWRAPS would initially provide full pelvic guidance during goal-oriented VR reaching tasks, with the assistance intensity, that is, the controller gain that determines how strongly the robot drives the pelvis toward the reference trajectory, progressively reduced as coordination improves. Speed and task complexity would be scaled to individual capacity. Outcome measures should include biomechanical assessments (segmental coordination RMSE, sitting workspace area), functional clinical scales, and SoA ratings collected at baseline, post-training, and follow-up (Santamaria, Khan, et al., 2020; Santamaria, Luna, et al., 2020; Wen and Haggard, 2018).
Our results support integrating SoA as a longitudinal clinical outcome alongside motor measures. Session-by-session post-training SoA ratings, using the 7-point Likert scale from the present study supplemented by validated agency questionnaires that separately assess the feeling of agency (the in-the-moment experience of control) and the judgment of agency (the retrospective evaluation of whether one caused the observed outcome) (Haggard, 2017), would track whether perceived control increases in parallel with motor gains or declines as task difficulty progresses. A decline in SoA despite stable coordination could signal excessive assistance or motivational disengagement, prompting protocol adjustment. This dual-outcome approach, monitoring both what the patient can do and how they experience doing it, represents a step toward patient-centered rehabilitation design.
The choice of coordination template warrants careful consideration. Our training paradigm uses each participant’s individual baseline coordination pattern as the reference template. For able-bodied participants this pattern is presumably near-optimal, making the task one of maintaining coordination under increased speed demand rather than learning a novel strategy. This represents a necessary validation step before clinical application. For impaired populations, however, a patient’s spontaneous pattern may represent a compensatory adaptation that should be reshaped rather than reinforced, while a normative template derived from healthy individuals may set an unachievable target. A therapist-prescribed template, biomechanically informed but individualized to the patient’s capacity, is likely most appropriate for clinical translation. The present study demonstrates that pWRAPS can guide participants toward any predefined template; the choice of which template to target is a clinical decision for future studies with impaired populations.
5. Limitations and future work
This study involved only able-bodied participants and captured performance within a single 10–15-min session, limiting conclusions to short-term motor adaptation. Several specific limitations should be acknowledged.
First, the single-session design with immediate pre-to-post assessment provides no evidence of retention; multi-session protocols with delayed tests are needed to establish whether coordination gains persist and to evaluate longitudinal outcomes in clinical populations with trunk impairments.
Second, all assessments were conducted within VR; no out-of-headset evaluation was performed. It therefore remains unknown whether the observed coordination improvements transfer to non-VR contexts, a concern highlighted by the context-dependency framework of Yarossi et al. (2021). Although our seated, low-conflict paradigm minimizes the visual–vestibular discrepancies that drive context-specific learning, a direct comparison between VR and conventional monitor-based delivery would be needed to isolate display-specific effects from the robotic guidance effects that are the focus of this work.
Third, all participants were young, able-bodied adults; results may not generalize to clinical populations with different baseline coordination strategies, altered sensory processing, and distinct motor learning capacities.
Fourth, individual baseline coordination patterns served as training targets, an assumption reasonable for healthy participants but potentially problematic for impaired populations whose spontaneous patterns may reflect compensatory strategies that should be reshaped rather than reinforced; future studies should compare individual-baseline, therapist-prescribed, and normative reference templates.
Fifth, the sample size of n = 8 per group provides adequate power for main effects but limits detection of interaction effects and individual-difference patterns; the absence of a significant guidance × VF interaction may partly reflect insufficient power, and larger samples are recommended for future studies.
Additional measures such as pelvic interaction forces or surface electromyography (sEMG) could reveal underlying muscle activation patterns and compensatory strategies, particularly in the trunk. Expanding the system to include active trunk guidance may further enhance its capacity to support complex, full-body coordination tasks.
6. Conclusions
This study introduced a novel seated postural training that integrates robotic pelvic guidance with a virtual reality (VR) game to enhance multi-segment coordination during a reaching task. We examined the training effects on sense of agency (SoA), which reflects participants’ perceived movement control and engagement. Participants were assigned to one of four groups in a 2 × 2 factorial design based on the presence of pelvic guidance and the type of visual feedback (VF). One VF condition presented the target position directly, whereas the other emphasized the error between the hand and the target.
Pelvic guidance improved task performance and coordination learning across conditions, suggesting that somatosensory input at the pelvis facilitates whole upper-body control. In contrast, the complex error-based VF influenced Trunk–Pelvis coordination, likely due to increased visual attention directed toward the hand, particularly when pelvic support was absent.
SoA increased over the course of training and was strongly associated with Trunk–Pelvis coordination, a segment that received no direct feedback, highlighting the role of internal sensorimotor congruence from self-generated movement in perceived control. Notably, SoA tended to increase when participants transitioned from the error-based VF to the direct VF post-training, suggesting that brief exposure to more complex visual cues may enhance engagement, even if not significantly. However, postural training benefits were most pronounced when paired with active pelvic guidance.
Together, these insights support the design of rehabilitation strategies that prioritize volitional control of upper trunk mobility and varied visual cues in VR to sustain engagement, reinforce internal sensorimotor congruence, and enhance motor outcomes as a foundation for functional recovery.
Supplemental material
Supplemental Material - Effects of robotic pelvic guidance and visual feedback designs on upper body seated coordination and sense of agency in virtual reality
Supplemental Material for Effects of robotic pelvic guidance and visual feedback designs on upper body seated coordination and sense of agency in virtual reality by Chawin Ophaswongse, Victor Santamaria, Victoria Lent and Sunil K. Agrawal in The International Journal of Robotics Research.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New York State Innovative, Developmental or Exploratory Activities (IDEA) in Spinal Cord Injury (grant number C35595GG). Chawin Ophaswongse is supported by the New York State Individual Postdoctoral Fellowships in Spinal Cord Injury Research (grant number C39064GG, C37719GG).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.