
Abstract
Background
Micro-computed tomography (micro-CT) offers numerous advantages for small animal imaging, including the ability to monitor the same animals throughout a longitudinal study. However, concerns are often raised regarding the effects of X-ray dose accumulated over the course of the experiment.
Purpose
To scan C57BL/6 mice multiple times per week for 6 weeks, in order to determine the effect of the cumulative dose on pulmonary and cardiac tissue at the end of the study.
Material and Methods
C57BL/6 male mice were split into two groups (irradiated group = 10, control group = 10). The irradiated group was scanned (80 kVp/50mA) three times weekly for 6 weeks, resulting in a weekly dose of 0.84 Gy, and a total study dose of 5.04 Gy. The control group was scanned on the final week. Scans from week 6 were reconstructed and the lungs and heart were analyzed.
Results
Overall, there was no significant difference in lung volume or lung density or in left ventricular volume or ejection fraction between the control group and the irradiated group. Histological samples taken from excised lung and myocardial tissue also showed no evidence of inflammation or fibrosis in the irradiated group.
Conclusion
This study demonstrated that a 5 Gy X-ray dose accumulated over 6 weeks during a longitudinal micro-CT study had no significant effects on the pulmonary and myocardial tissue of C57BL/6 mice. As a result, the many advantages of micro-CT imaging, including rapid acquisition of high-resolution, isotropic images in free-breathing mice, can be taken advantage of in longitudinal studies without concern for negative dose-related effects.
Mouse models have become a critical element of preclinical research (1, 2); more specifically, mouse models have become popular for modeling cardiovascular disease. As a result, technological advances have led to the development of imaging techniques capable of visualizing small animal cardiovascular systems with sufficient detail. In particular, micro-computed tomography (micro-CT) offers numerous advantages for small animal imaging: rapid scan times ranging from seconds to minutes, and the acquisition of high-resolution images with isotropic voxels enables evaluation of the mouse with minimal impact on the animal's physiology (3). Additionally, dynamic acquisition of images using gating techniques enables functional measurements of the cardiovascular system in free-breathing mice, with scans that are both rapid and reproducible (4–7). As a result, micro-CT can be particularly useful for detecting the onset of, and monitoring the progression of, cardiac diseases (8).
The non-invasive quality of micro-CT enables its use in longitudinal studies (6), where the same animal can be scanned multiple times over the course of the study. Disease progression can therefore be tracked in an individual animal, allowing it to act as its own control, and potentially reducing the number of animals required to produce statistical significance in a study.
Commonly, concern over the X-ray dose delivered during a scan is identified as a drawback of micro-CT. The dose delivered has been studied both theoretically (9, 10), and experimentally (11–14). A typical full-body ungated micro-CT scan delivers an entrance dose of 10 cGy (12, 15), with the absorbed dose reported lower, in the range of 2–7 cGy, depending on the scan protocol used (11–13). These doses, although much smaller than the LD50 of the mouse (16), are larger than the dose delivered during a clinical cardiac CT (2–5 cGy) (17). This is particularly relevant in longitudinal studies, where more than one scan is performed per animal. When cardiac gating is required, larger doses typically in the range of 0.25–1.0 Gy (4, 7, 18) are delivered to provide images at multiple phases of the cardiac cycle.
Radiation damage has been shown to cause cardiac hypertrophy and decrease left ventricular systolic function in the form of a lowered ejection fraction (19), although a fairly high X-ray dose (16 Gy) is required to cause this damage. Pulmonary tissue is more sensitive to radiation-induced damage than myocardial tissue, and in a cardiovascular study the lungs will be exposed to the same amount of radiation as the heart. Decreases in lung function are linked to decreases in cardiac function (20), and as the lungs are more likely to display evidence of radiation exposure before the heart, it would be beneficial to evaluate the pulmonary tissue, in addition to the myocardial tissue, for adverse effects related to the delivered dose of a cardiac micro-CT study.
There have been a number of studies looking at the effect of dose on pulmonary tissue in mice (21–23) ; however, they have focused mainly on investigating radiotherapy doses of 10–20 Gy delivered in a single session at the beginning of the study. Additionally, evaluation of dose effects typically does not begin for 8–12 weeks following exposure. This creates some difficulties in trying to apply the results to a typical micro-CT study, where the doses are smaller, often by a factor of 100, delivered multiple times over a period of weeks, and often <8 weeks in length.
The objective of this study was to reproduce a longitudinal cardiac micro-CT study and evaluate the effects of dose on pulmonary and myocardial tissue. We scanned C57BL/6 mice multiple times per week for 6 weeks, and evaluated micro-CT images for any anatomic or functional changes to the lungs and heart, and performed histology to determine if any effects were seen at a cellular level.
Material and Methods
Animal groups and delivered dose
Twenty C57BL/6 male mice (24 ± 1 g) were split into two groups: the first was the Irradiated Group, which was scanned weekly for 6 weeks; each weekly session comprised three scans (thereby providing three times the dose of a typical micro-CT study). The second group was the Control Group, which was not scanned until week six. In an effort to assess both the pulmonary and cardiac systems, in the final week both groups were first scanned using respiratory gating to evaluate the lungs; a contrast agent (5 μL/g body weight eXIA 160XL; Binitio Biomedical Inc., Ottawa, Canada) was then administered via the tail vein and a cardiac-gated scan was acquired to evaluate the heart.
Each scan delivered an entrance dose of 0.28 Gy (7); as a result, the Irradiated Group received a weekly dose of 0.84 Gy, and a total entrance dose of 5.04 Gy by the end of the study. All studies performed were approved by the Animal Use Subcommittee of the University Council on Animal Care at our institution.
Scan protocol
Prior to scanning, mice were anesthetized with 1.5% isoflurane in O2, and placed prone on the micro-CT bed. When required for respiratory gating, a pneumatic pillow was placed beneath the diaphragm to measure breathing signals; likewise, when required for cardiac gating, neonatal electrodes (2269T, 3M Health Care, St. Paul, MN, USA) were affixed to the paws to measure ECG. These physiological signals were recorded using a monitoring and triggering system (BioVet; m2m Imaging Corp., Newark, NJ, USA). Temperature was maintained between 36°C and 37°C during the entire experiment.
Weekly scans were performed using a volumetric cone-beam micro-CT scanner (Locus Ultra, GE Healthcare, London, ON, Canada), equipped with a flat-panel detector mounted on a slip-ring gantry, enabling continuous acquisition of X-ray projections. Projection images were acquired at 80 kVp and 50 mA over 10 rotations (5 s per rotation, 416 projection images per rotation at a rate of 12 ms/projection) for a total acquisition time of 50 s per scan. Projections were acquired over a field of view of 14 cm (transaxial) × 5.4 cm (longitudinal), providing a nearly full-body scan of the mouse.
Entrance dose measurements were performed previously (15) using a small ‘pancake’ ion chamber (Model 35617, Keithley Instruments Inc., Cleveland, OH, USA) measuring exposure in air at the isocenter of the scanner.
Retrospectively-gated reconstruction
All gated reconstructions performed in this study were done using the technique described by Armitage et al. (24) and were reconstructed with 150 μm isotropic voxels (15).
Respiratory gating: Respiratory-gated reconstructions were performed on week six scans for mice in both groups. Projection images were sorted based on the phase of the respiratory cycle during which they were acquired; images at both peak-inspiration and end-expiration phases were reconstructed. The average window sizes of the two phases were 63 ms and 140 ms, respectively.
Cardiac gating: Cardiac-gated reconstructions were performed on week six scans acquired following the injection of the contrast agent. Projection images were sorted based on the phase within the cardiac cycle during which they were acquired, enabling subsequent reconstruction of 3D images at 12-ms intervals. For this study, between nine and 12 3D images were reconstructed per cardiac cycle, depending on the heart rate.
Image analysis
Image analysis was performed using MicroView software (version ABA 2.2, GE Healthcare, London, ON, Canada). Images were initially converted to Hounsfield units (HU) using water and air samples in the reconstructed image as a reference.
Respiratory analysis: To calculate lung volume, an upper threshold was first identified for segmenting the lung from the surrounding thoracic tissue; this was performed by generating a region of interest (ROI) that contained 50% lung tissue and 50% surrounding tissue. The threshold was then automatically determined (25) as –220 HU. A lower threshold was chosen as –750 HU, which effectively segmented the lung parenchyma from the major airways (trachea, bronchi). An ROI was generated around both lungs, and a segmented region-growing algorithm segmented the lung tissue using the upper and lower thresholds previously determined. Thresholds were the same for both inspiration and expiration. The volume was determined for both inspiration and expiration phases; the density for both phases was determined by finding the mean CT number of the segmented lung tissue.
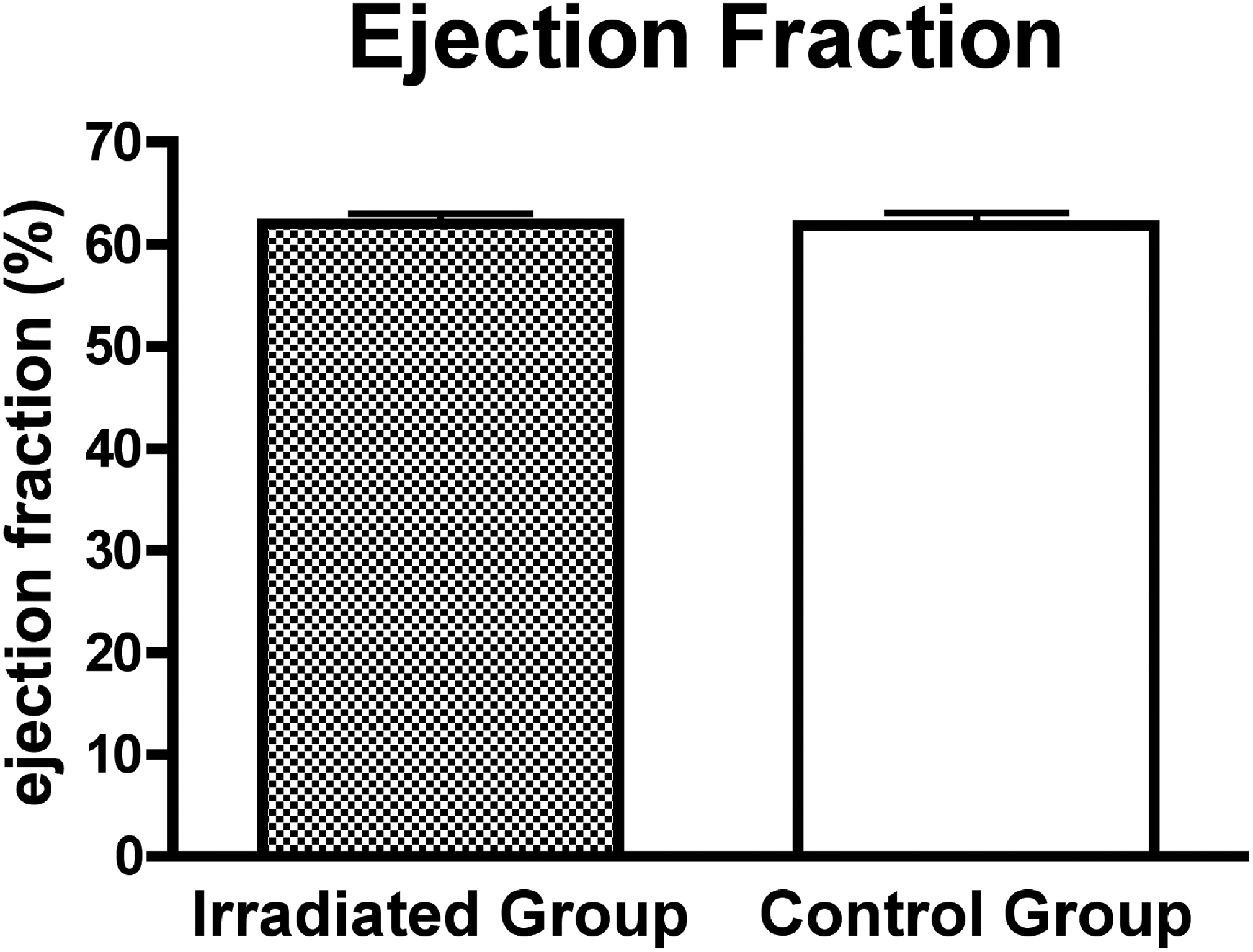
Cardiac analysis: To calculate LV volume, a threshold level that separated the myocardium from the blood pool was identified automatically (25); this was done separately for each scan, as contrast level in the blood changed over the course of the study. As described in prior studies (6, 7), automatic segmentation of the LV chamber from the myocardium was achieved using a region-growing approach. LV volume was calculated for all the images (reconstructed every 12 ms through the cardiac cycle), and the minimum and maximum were used as end-systolic volume (ESV) and end-diastolic volume (EDV), respectively. Knowledge of the ESV and EDV enabled ejection fraction (EF) to be calculated.
Histology
Following the final scan on week 6, the mice were euthanized and the lungs and heart were extracted. Lungs were inflated with 10% formalin, and both the lungs and heart were fixed in the formalin solution. The tissue was then embedded in paraffin and sliced 4 μm thick: the heart of each mouse was sliced in half along the short axis and three slices were taken and mounted on slides. Either the left or right lung of each mouse was also sliced in half along the short axis and three slices taken and mounted on slides. Slices were stained with hematoxylin and eosin and evaluated for evidence of dose-related damage (i.e. early inflammation in the form of inflammatory cells and edema).
Statistical analysis
Data are presented as mean ± SD; all analysis was performed using Prism 4 (GraphPad Software, Inc., San Diego, CA, USA). Unpaired t-tests were used to evaluate changes in lung volume and lung density between the Irradiated Group and the Control Group, for both the inspiration and expiration phases. Unpaired t-tests were also used to assess differences in cardiac function between the two groups; systolic and diastolic volume, and EF were evaluated. Results were considered statistically significant at P < 0.05.
Results
Scans from all animals acquired in the final week were successfully reconstructed and analyzed. Overall, the X-ray dose delivered during the longitudinal study had no significant effect on mouse pulmonary and cardiac tissue.
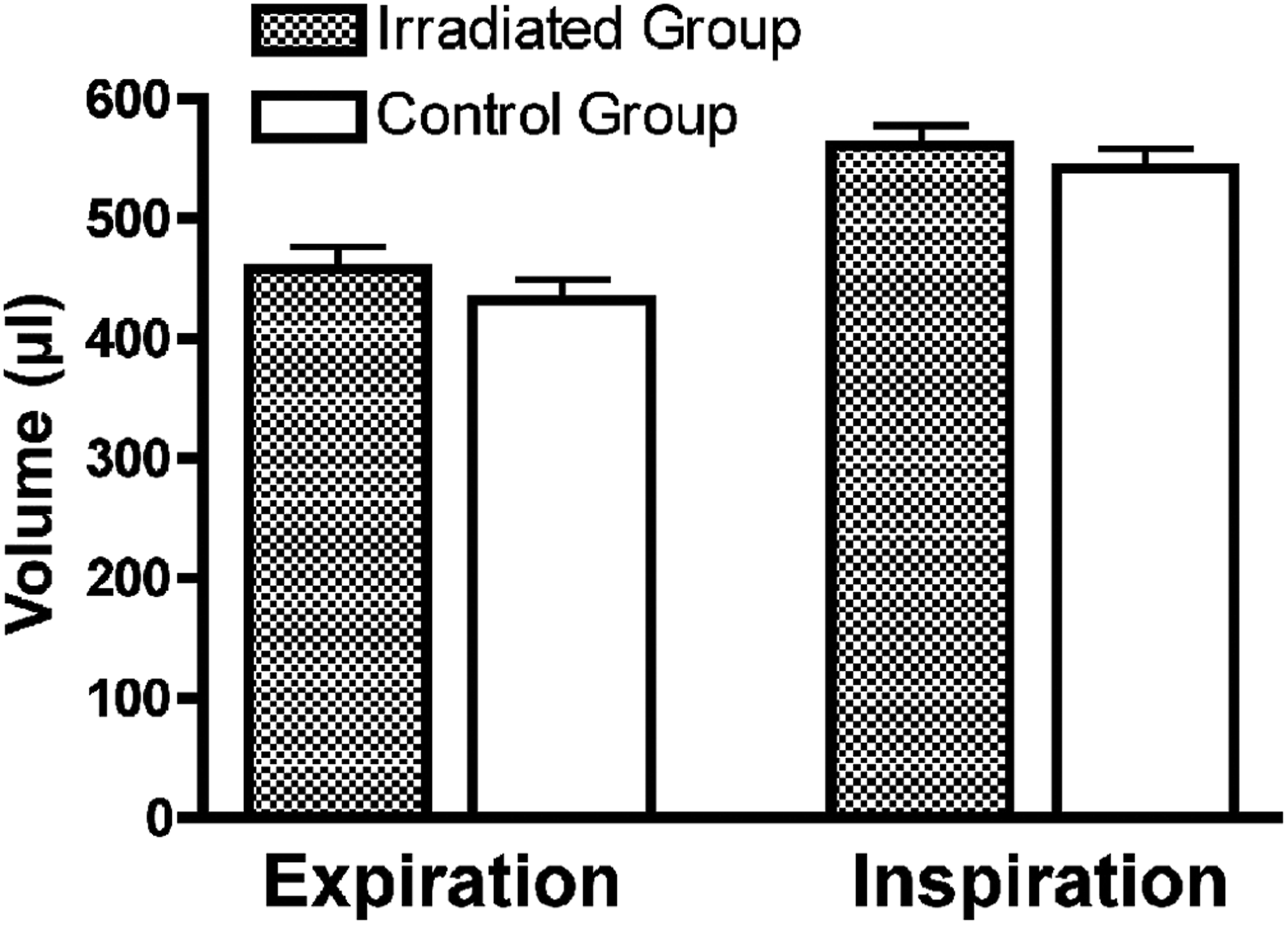
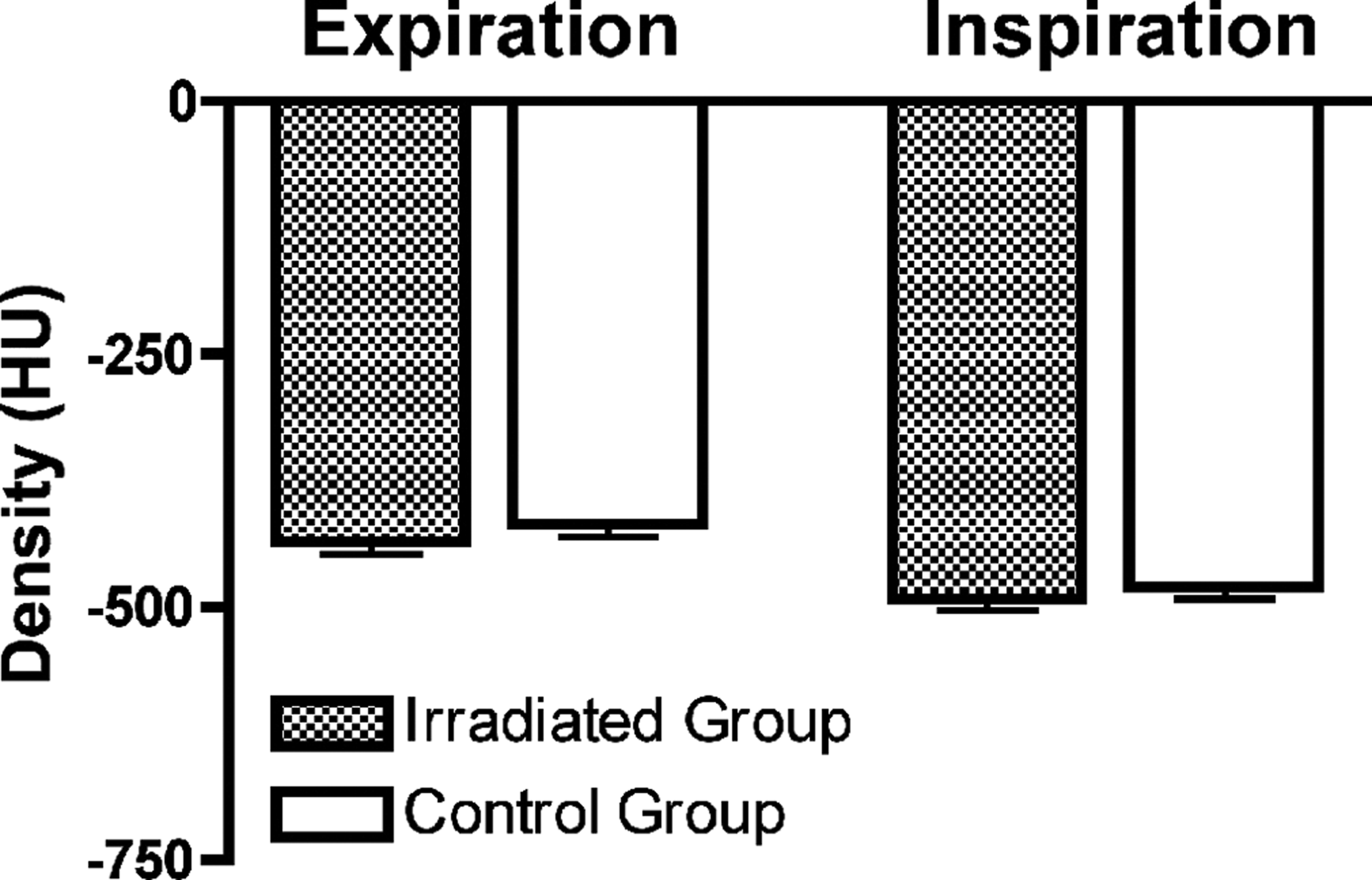
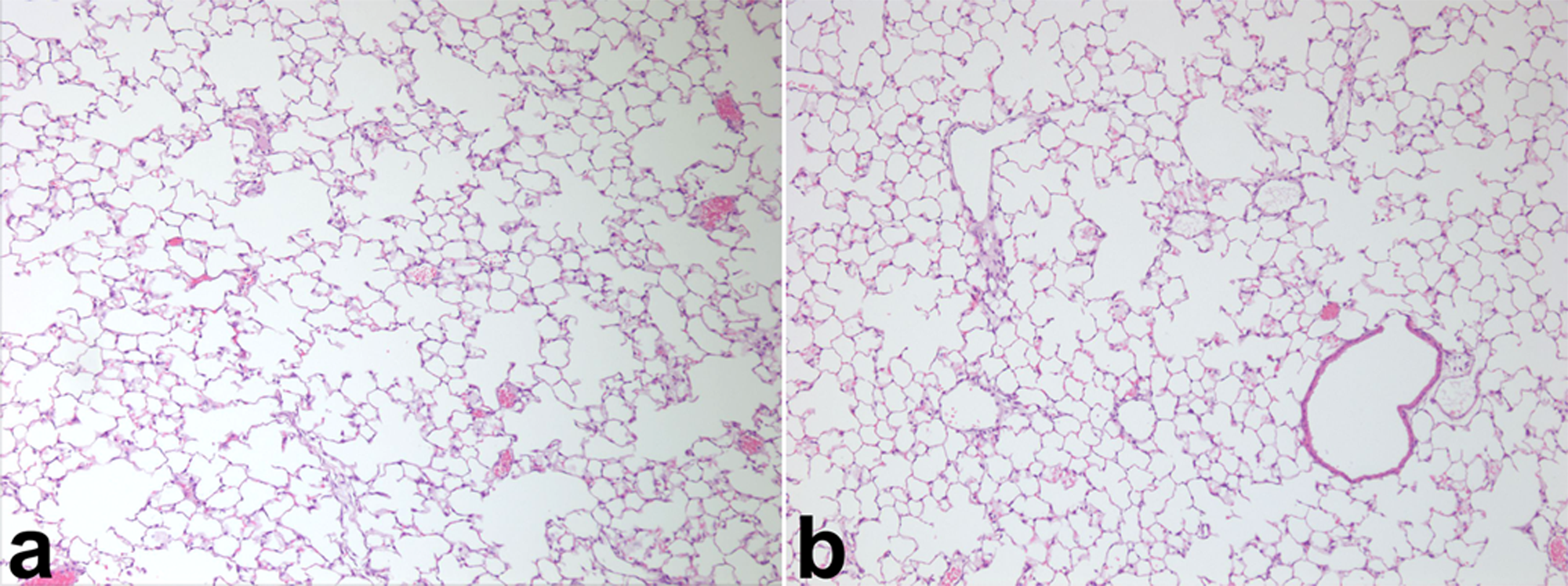
Qualitatively, the lungs displayed no visual differences between the two groups (Fig. 1). This was reflected quantitatively both in lung volume (Fig. 2) and lung density (Fig. 3). T-tests comparing lung volume between the Irradiated and Control groups indicated no significant differences in either expiration (P = 0.3492) or inspiration (P = 0.4841) phases. Similarly, t-tests comparing lung density showed no significant differences in either expiration (P = 0.3566) or inspiration (P = 0.4432). More importantly, histological samples of pulmonary tissue showed no early damage in the Irradiated Group as compared to the Control Group (Fig. 4). This early damage would show up in the form of inflammatory cells filling up the air spaces, but no evidence of this was present.
Coronal slice of micro-CT image from an irradiated mouse (a) and a control mouse (b) during inspiration. Note the apparent lack of density and volume changes in (a) compared to (b) A comparison of lung volume between the Irradiated and the Control Groups, for both expiration and inspiration phases. No significant differences were measured between groups for either phase A comparison of lung density between the Irradiated and the Control Groups, for both expiration and inspiration phases. Differences between groups were not significant for either phase Histological slides of pulmonary tissue taken from an irradiated mouse (a) and a control mouse (b). Magnification at x100. No evidence of early inflammation is present in the irradiated mouse, which would be identified by the occurrence of inflammatory cells and edema within the alveoli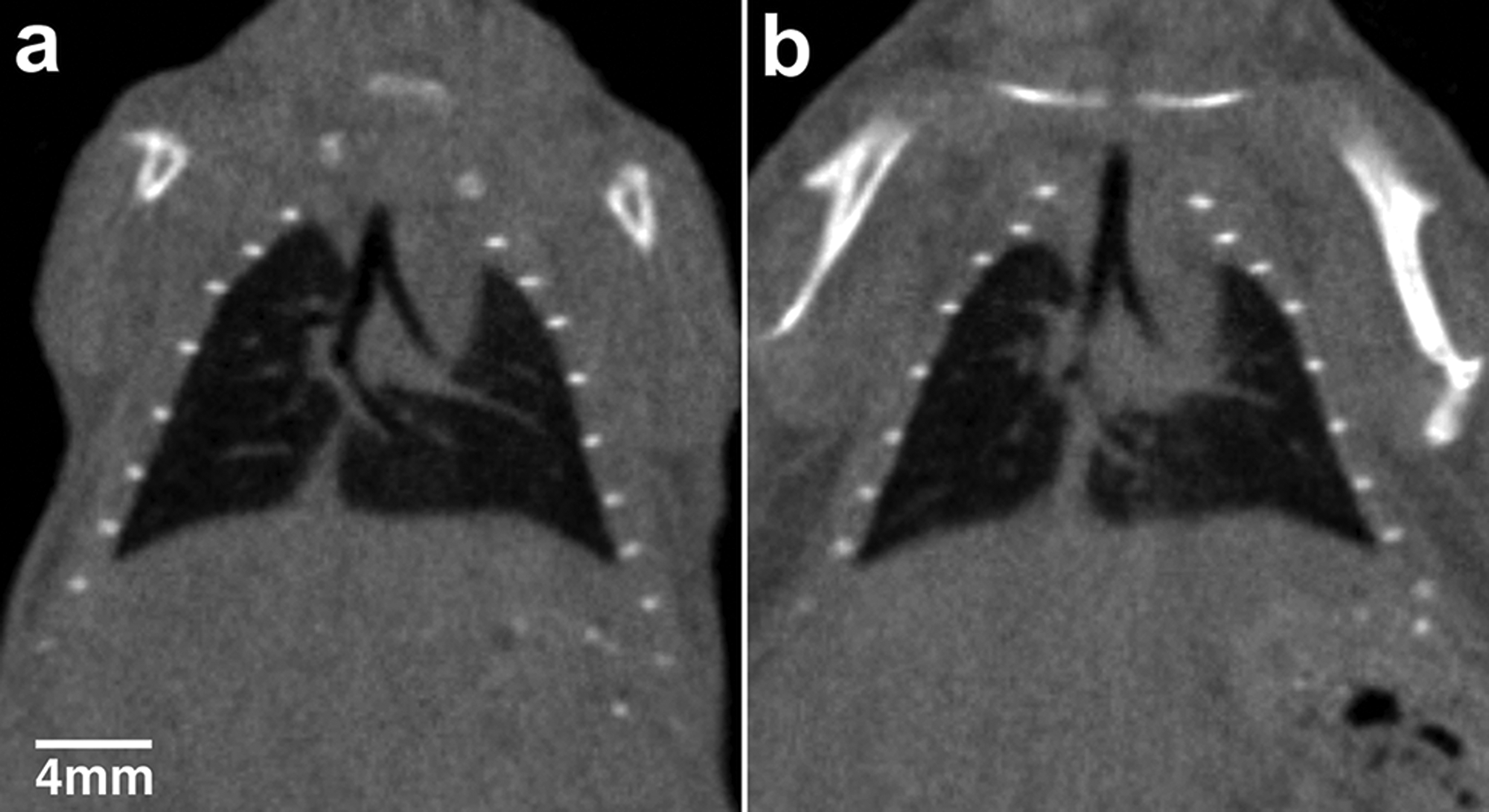
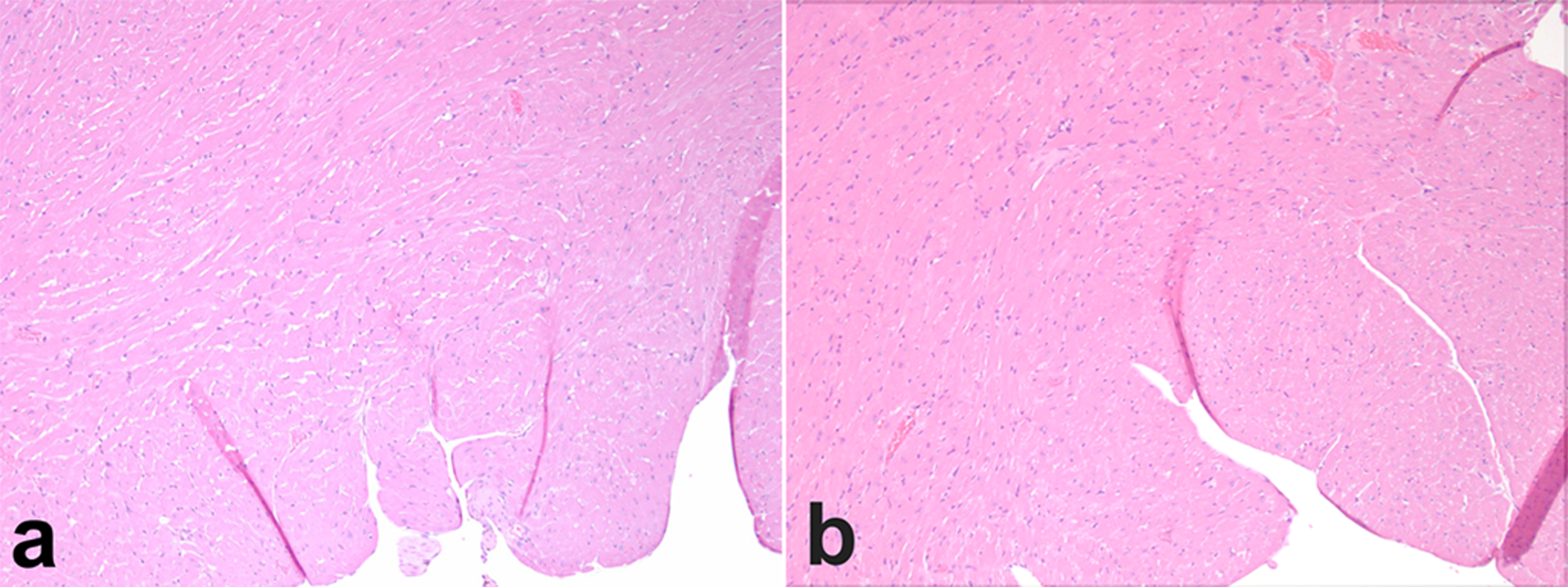
Cardiac function was also evaluated; qualitatively, no changes to the myocardium are evident, reflected quantitatively in the evaluation of LV volume and ejection fraction. No significant differences between the Irradiated and Control groups were witnessed in LV systolic (P = 0.1953) and diastolic (P = 0.0807) volumes (Fig. 5), nor were there any changes in ejection fraction (P = 0.9263) (Fig. 6). Similar to the evaluation of pulmonary tissue, histological samples of the myocardium were evaluated, and no signs of early dose-related damage were present (Fig. 7).
A comparison of systolic and diastolic LV volumes between the Irradiated Group and the Control Group. Differences between the groups were not significant for either phase A comparison of cardiac function between the Irradiated Group and the Control Group, measured using ejection fraction. No significant differences in function were measured between groups Histological slides of myocardial tissue taken from an irradiated mouse (a) and a control mouse (b). Magnification at x100. No evidence of fibrotic tissue is present in the irradiated mouse, indicating that X-ray dose had no adverse effects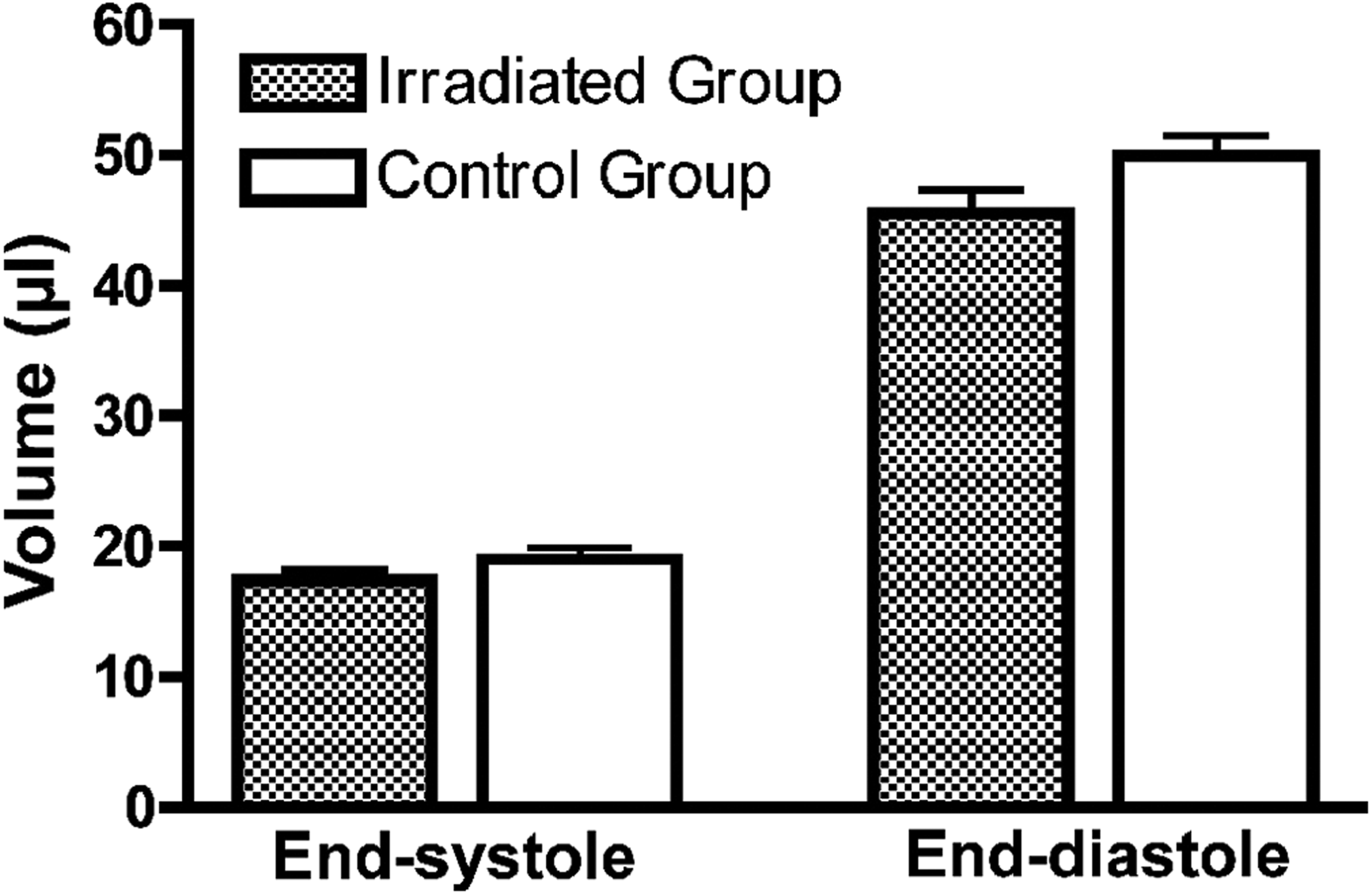
Discussion
The goal of this study was to determine the effects, if any, of X-ray dose delivered during a typical longitudinal cardiac micro-CT study on the myocardial and pulmonary tissue in C57BL/6 mice. Both pulmonary and cardiac tissue was evaluated because, during a cardiac scan, the field of view is centered on the heart and the lungs are inevitably irradiated, even with a narrow FOV. This is significant because pulmonary tissue has a higher radiosensitivity than myocardial tissue; any early indications of radiation-induced damage will present in the lungs.
Radiation-induced lung damage is generally split into two phases: an early acute inflammatory phase, often called radiation pneumonitis, and a later chronic fibrosis phase (26). As fibrosis typically develops 4–6 months following radiation exposure, an early inflammatory reaction would be the most likely to occur if a micro-CT study caused damage. Signs of an inflammatory reaction are marked by an increase in inflammatory cells and edema within the air spaces of pulmonary tissue, which can be seen histologically. On a micro-CT image, these changes would result in a decrease in lung volume, and an increase in lung density.
Referring to Figs. 2 and 3, there were no significant changes to either lung volume or lung density in the Irradiated Group compared to the Control Group, indicating that a cumulative entrance dose of 5.04 Gy caused no significant damage apparent at an anatomic level. More importantly, histology of the pulmonary tissue (Fig. 4) showed no early signs of inflammation at a cellular level – there were no inflammatory cells accumulating in the air spaces, no edema was present and no vascular dilation of the capillaries surrounding the alveoli. This is strong evidence that morphological changes due to the dose delivered during a longitudinal micro-CT study are highly unlikely.
The results presented are consistent with other studies that have evaluated radiation damage to the lungs in mice. In general, a dose threshold of 12 Gy needs to be exceeded in order for radiation pneumonitis to occur in mouse models (27–30). This is confirmed more recently by Jackson et al. (21), which showed that C57BL/6 mice irradiated with a single 15 Gy dose delivered to the thorax displayed no changes to lung volume or lung density at 16 weeks following exposure, and that changes at a cellular level were detectable histologically at 28–32 weeks. Interestingly, Johnston et al. has recently indicated that doses of 10 Gy delivered full-body may have an effect beyond 12 months (22); however, these effects, detectable histologically as the onset of fibrosis – with increased levels of collagen in areas of tissue remodeling and inflammation – did not result in changes to lung function, as measured by changes in breathing rate.
The myocardial tissue was also evaluated for evidence of dose effects. The most significant type of radiation-induced heart disease is myocardium damage (31, 32), which would result in evidence of degenerative morphological changes of cardiomyopathy such as myocyte degeneration/necrosis, increase in the amount of interstitial fibrous connective tissue, mineralization, and/or presence of mononuclear cells in histological analysis (33). On a micro-CT image, this would present as cardiac hypertrophy (a thickening of the LV wall and an enlargement of the heart), with a decrease in ejection fraction.
As Figs. 5 and 6 indicate, there were no significant changes to either the LV volume, or the ejection fraction in the Irradiated Group. It should be noted that the P value for the diastolic volume (0.0807) is close to a significant value, however, the lack of changes in wall thickness, along with no evidence of myocyte degeneration (Fig. 7), supports the conclusion that the differences witnessed between the two groups are due to biological variability rather than radiation damage. Additionally, radiation damage would manifest as an enlargement of the LV (19); the opposite is witnessed in this study (Fig. 5), further supporting an explanation of biological variability.
The lack of a dose effect in the cardiac tissue is not unexpected, given that no evidence of radiation damage was present in the pulmonary tissue; these results are also consistent with other studies evaluating radiation damage to the heart, which in general show that larger doses and a longer period of time are required to cause measurable damage. For example, Monceau et al. delivered a dose of 16 Gy to the thorax of C57BL/6 mice and witnessed radiation-induced cardiac hypertrophy 15 weeks following irradiation (19); however, a significant decrease in ejection fraction did not occur until 30 weeks. Qian et al. (34) evaluated short-term effects of 7 Gy delivered to the heart, and found that a mild myocyte degeneration was not witnessed until 100 days following treatment. A study which may have more relevance to micro-CT experiments was described by Baker et al. (35); performed in rats, they found that 10 Gy delivered full-body had the potential for indirectly contributing to heart disease development, compared to 10 Gy delivered to the thorax alone, which had no significant effect on the myocardium. It was proposed that full-body exposure had effects on non-thoracic organs that contributed to coronary sclerosis and ventricular dysfunction through changes in blood lipid profiles. However, it is important to note that these effects were not witnessed until 120 days following exposure, and that the animals were irradiated in a single dose much larger than would be delivered during a longitudinal micro-CT study.
The results presented in this study have relevance beyond the applicability to other cardiac micro-CT experiments. A scan protocol for retrospective gating was used, which means that these results can be applied to any micro-CT study that employs prospective gating, or ungated scans, which deliver a lower dose than presented here. Additionally, the dose was purposely tripled beyond a typical dose, widening the variety of studies to which these results can be applied. Finally, studies in which micro-CT is not used longitudinally can also benefit from the results presented, which indicate that the small dose delivered will have no adverse effects on the health of the animal.
The C57BL/6 mouse strain was used, as it is one of the most common strains used in biomedical applications (21). However, variation in radiation-induced damage between mouse strains (21, 29, 36) indicates that the damage has a genetic component. But from these studies we can also infer that, given the lower doses (below 12 Gy) of a longitudinal micro-CT study, and the short timeframe involved (<8 weeks), it is unlikely that strain-related differences in radiation effects would occur.
In retrospect, given that cardiovascular disease can exist in asymptomatic individuals that manifests under stress conditions, the addition of a stress agent during the final week of evaluation would have produced additional beneficial information regarding any latent dose effects on the heart. However, considering the length of time generally associated with the development of radiation-induced cardiac damage, combined with the lack of myocyte degeneration in this study, it is unlikely that a stress test would have produced results of significance.
Also not covered by this study is the effect of radiation dose on gene expression, which can occur at lower dose values than those reported here (37, 38). For example, Kerseman demonstrated increased DNA double-strand breaks 3 days following any scan delivering a dose higher than 1.5 cGy. However, these results did not translate to macroscopic changes. It may be important to keep this in mind, however, as it may have relevance depending on the focus of the study.
In conclusion, the X-ray dose delivered during a longitudinal cardiac micro-CT study had no significant effects on the pulmonary and myocardial tissue in mice. Due to the artificially high dose delivered during this study, the results presented can be applied to a wide variety of micro-CT experiments; therefore the benefits of using micro-CT, including rapid scan times that produce high-resolution isotropic images, can be safely taken advantage of without concern that the dose delivered will have an adverse effect on the animal or the study.
Footnotes
ACKNOWLEDGEMENTS
Partial funding for this study was provided by the Heart and Stroke Foundation of Canada (grant no. T6293). M Drangova is a Career Investigator of the Heart and Stroke Foundation of Ontario. The authors would like to thank Dr Christopher Howlett for evaluating the histological samples, Jennifer Hadway for performing the tail-vein injections, and Elsbeth Tate for performing a portion of the analysis.