
Abstract
Background
Computed tomography (CT)-guided fine needle aspiration (FNA) and biopsies are well-established, minimally invasive diagnostic tools for pulmonary lesions.
Purpose
To analyze retrospectively the results of 1000 consecutive lung CT-guided FNA and/or core needle biopsies (CNB), the main outcome measures being diagnostic yield, and complication rates.
Material and Methods
Patients considered eligible were those referred to our department for lung lesions. The choice of FNA, CNB, or both was based upon the radiologist's judgment. Diagnostic yield was defined as the probability of having a definite result by cytology/histology.
Results
The study included 733 male patients and 267 female patients, with a mean (SD) age of 66.4 (11.4) years. The mean (SD) lesion size was 3.7 (2.4) cm in maximal diameter. Six hundred and forty-one (64%) patients underwent an FNA procedure, 245 (25%) a CNB, and 114 (11%) had been subjected to both. The diagnostic yield was 960/994 (96.6%); this decreased significantly with the use of CNB only (odds ratio [OR] 0.32; 95% CI 0.12–0.88; P = 0.03), while it increased with lesion size (OR 1.35; 95% CI 1.03–1.79; P = 0.03 per cm increase). In 506 patients (52.7%), a malignant process was diagnosed by cytopathology/histology. The complication rate reached 97/1000 (9.7%); complications included: hemorrhage, 62 (6.2%); pneumothorax, 28 (2.8%); hemorrhage and pneumothorax, 5 (0.5%); and hemoptysis, 2 (0.2%). It was not significantly affected by the type of procedure or localization of the lesion. The overall risk for complications was three times higher for lesions <4 cm (OR 3.26; 95% CI 1.96–5.42; P < 0.001).
Conclusion
CT-guided lung biopsy has a high diagnostic yield using FNA, CNB, or both. The CNB procedure alone will not suffice. Complication rates were acceptable and correlated inversely with lesion size, not localization or type of procedure.
Computed tomography (CT)-guided fine needle aspiration (FNA) biopsy is considered a safe procedure with high diagnostic accuracy (82–96%) in various clinical settings, including lung lesions undiagnosed at bronchoscopy (1). Results depend upon the location, histologic type, and type of needle used (2). Core needle biopsy (CNB) offers the physician the advantage of molecular analysis and the potential for a more targeted therapy (3). The most common complications include pneumothorax, parenchymal hemorrhage, and hemoptysis (4).
We retrospectively analyzed a large series of patients who underwent CT-guided FNA/CNB for pulmonary lesions. We present the diagnostic yield and complication rates, highlighting the techniques and related limits and pitfalls.
Material and Methods
The Department of Medical Imaging & Interventional Radiology is attached to a tertiary referral center for chest diseases, comprising 12 affiliated clinics. Patients considered eligible were those referred to our department for suspicious lung lesion(s) after a non-diagnostic bronchoscopy, transbronchial biopsy, and/or lavage, or for a lesion that was considered not feasible at bronchoscopic biopsy. Two types of needles were used, one for FNA and one for CNB, in line with the same protocol. A 22-gauge Chiba needle (Becton, Dickinson and Company, Franklin Lakes, NJ, USA) was used for FNA and cytologic analysis. The cutting needle biopsy and pathologic analysis involved an 18-gauge side cut needle with an automatic device to advance the cutting edge (Somatex, 18G, 100 mm length; Medical Technologies, GmbH, Teltow, Germany). In both types of biopsies, the single needle technique was used, rather than the co-axial technique. FNA, CNB or both were performed according to the radiologist's subjective judgment, based on size, localization, proximity to large vessels, or co-existent emphysema. FNA alone was preferentially performed in patients with smaller lesions, centrally localized, or lesions proximal to vessels, to reduce the risk of pneumothorax or hemorrhage. CNB was generally performed in cases of larger and more peripheral lesions. The final decision lay with the interventional radiologist. All biopsies were performed by the same interventional radiologist with 20 years of experience (LT). All patients gave informed consent before the procedure, in accordance with the Local Ethics Committee standards.
In the instance of both procedures being performed, FNA always preceded, since a hemorrhage due to CNB could alter cytologic results. Exclusion criteria included coagulopathy, INR >1.5 or a platelet count of <60,000/mm3.
Computed tomography scans (Siemens, Somatom Emotion Duo, Erlangen, Germany) were used to localize the lesion and to guide the insertion of the needle. All procedures were performed under local anesthesia (20 cc 2% xylocaine). The patients were positioned in a prone, supine, or lateral decubitus position in order to allow optimal access to the lesion. Lesions were localized by means of contiguous scans of 5 mm in thickness. Passage through the aerated lung parenchyma was minimized in order to avoid pneumothorax. Whenever necessary, intravenous contrast injection was administered, or the position changed, so as to improve access. Patients were instructed to hold their breath during the insertion of the needle. To minimize the risk of specimen inadequacy, we aimed to obtain two specimens from each lesion. The exception was high-risk patients (e.g. emphysema, small lesions), where a second insertion was not performed. Following completion of the interventional procedure, all patients underwent CT scans to evaluate the presence of possible complications, including pneumothorax or parenchymal hemorrhage. Given that the Radiology Department does not have a 1-day clinic, patients were observed for 3 h. Patients without symptoms, such as thoracic pain or dyspnea, were discharged with instructions to come back for a chest radiograph the following morning, and to contact the referring physician should any symptoms emerge.
Statistical analysis
Statistical analysis was performed using the Stata v8 package. Count outcomes were compared using the chi-square test. Diagnostic yield was defined as the probability of having a definite result by cytology/histology (representing the number of cases with adequate sampling for a definitive diagnosis divided by the total number of cases). Univariable and multivariable logistic regression modeling was used for outcomes of interest (diagnostic yield, hemorrhage, pneumothorax), and odds ratios (OR) with 95% confidence intervals were reported. Histology (malignant vs. benign) was added post-hoc as a covariate to measure its effect on complications. A P value <0.05 was considered significant.
Results
We retrospectively analyzed 1000 consecutive patients who had undergone CT-guided lung biopsies, from January 2007 to October 2010, when the 1000th patient was recorded. Seven hundred and thirty-three procedures were performed on male patients and 267 on female patients. The mean (SD) age when the diagnostic procedure was performed was 66.4 years (11.4). Eighty percent of patients were found to have a solitary pulmonary lesion. The mean lesion size (SD) was 3.7 (2.4) cm in maximal diameter. The localization of the suspected lesion was right upper 29%, right-lower 24%, left upper 22%, left lower 15%, right middle 6%, and lingula 5% (Fig. 1).
Relative distributions of lesion localization, and ensuing complications. H, parenchymal hemorrhage; LL, left lower; LU, left upper; P, pneumothorax; RL, right lower; RM, right middle; RU, right upper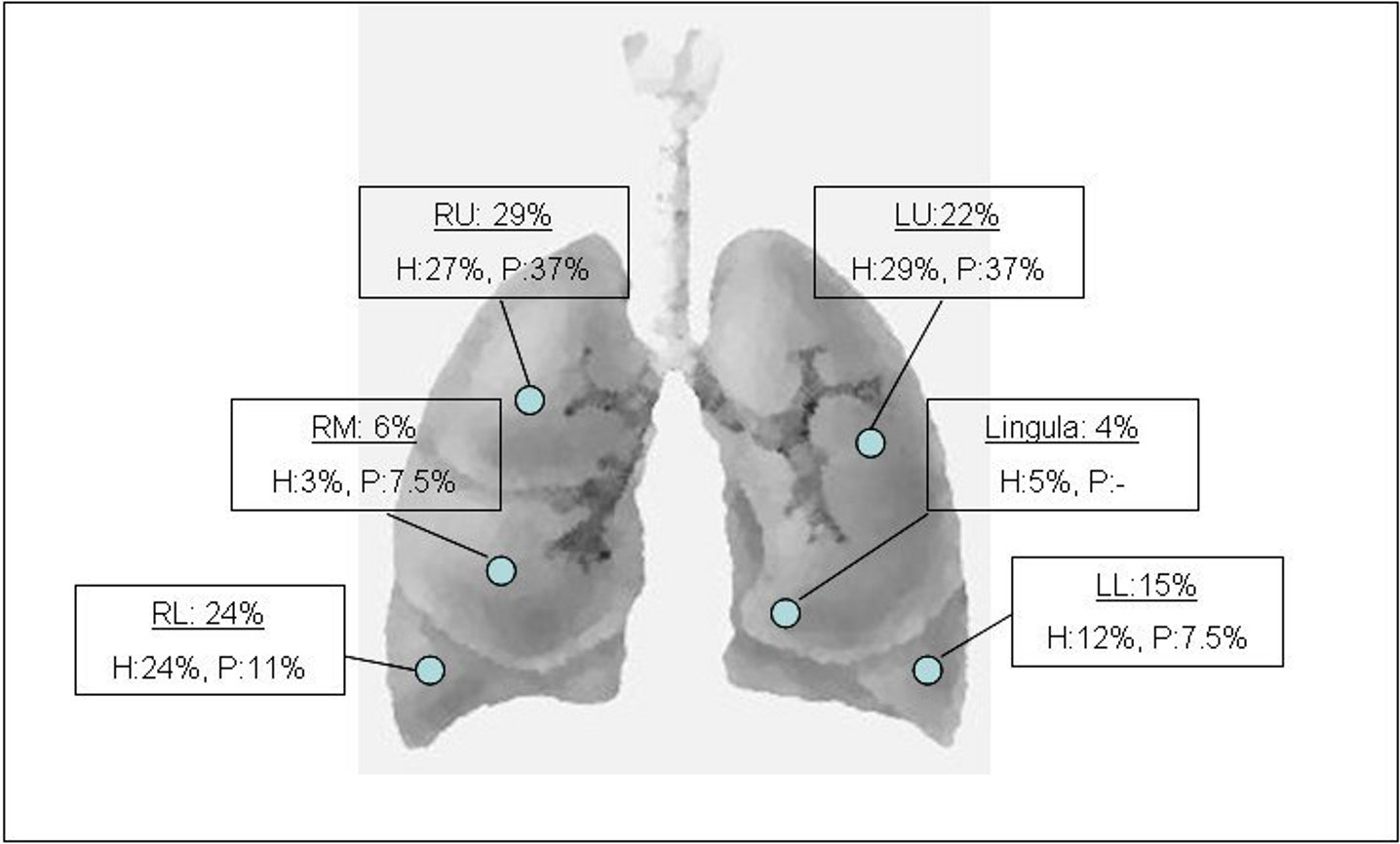
Of the total patient cohort, 641 (64%) had undergone an FNA procedure and 245 (25%) a CNB procedure; 114 (11%) had both procedures. The diagnostic yield, i.e. the proportion of successful tests with adequate sampling for a definitive diagnosis was 960/994 (96.6%) based on cytology/histology. Only 34 were non-diagnostic due to insufficient specimen collection/technical reasons, of which 19 were FNA biopsies and 15 were CNB. Six cases had missing data.
Results of 1000 CT-guided FNA/CNB samples (40 cases have no data, 34 due to insufficient sampling/technical errors and six due to missing records)
Univariable analysis (Table 2) showed that CNB alone had an adverse impact on diagnostic yield compared to FNA only. Localization of the lesion did not affect the success of the procedure, and lesion size had a marginal association. After adjusting for type of procedure (both, FNA only, CNB only) and maximal size of the lesion, CNB only and lesion size had a significant effect (Table 2). Fig. 2 depicts the predicted probabilities of a diagnostic procedure by lesion size, stratified by type procedure, based on the previous model. CNB alone is not preferable, especially for small lesions, as it is less successful than FNA and the combined procedure.
Predicted probabilities of a diagnostic procedure (diagnostic yield) by lesion size, stratified by type procedure, based on the previous model (Table 2). CNB only is not preferable, especially for small lesions, as success is less than FNA and combined procedure Diagnostic yield of CT-guided FNA/CNB. After adjusting for type of procedure (both, FNA only, CNB only) and maximal size of the lesion, CNB only and size had a significant effect on diagnostic yield (OR <1 denotes a decline, OR >1 denotes improvement)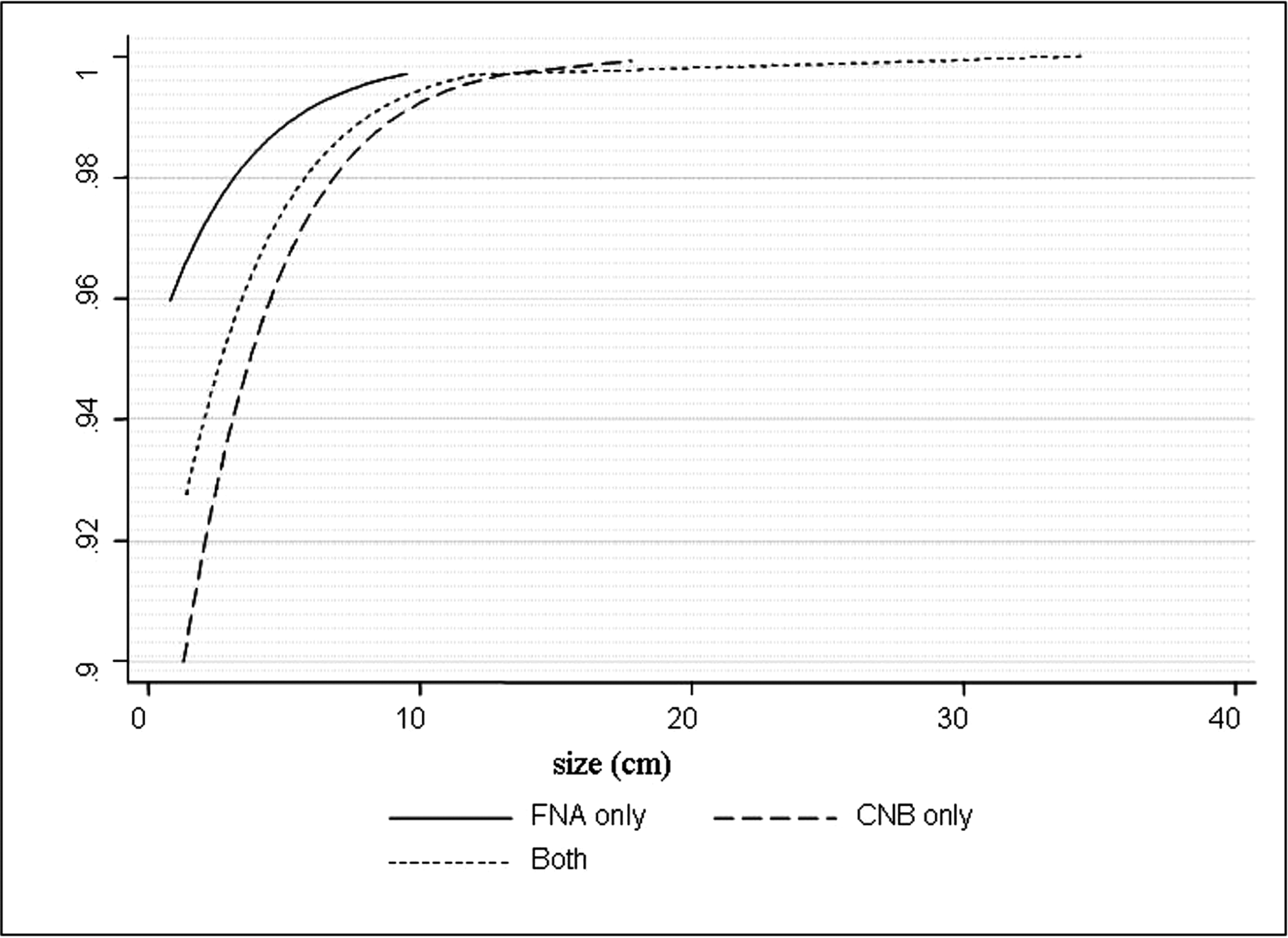
Complications of CT-guided biopsies. Univariable and multivariable analysis. Effects are expressed as odds ratios (95% confidence intervals)
Discussion
In the present study, FNA, CNB or their combination gave a definitive diagnosis for underlying neoplasia in more than half the patients presenting with suspicious pulmonary lesions. A similar rate of malignancy was recently reported using CNB for pulmonary lesions (5). The benefit of obviating the need for a more invasive approach, i.e. open lung biopsy, is evident. For patients with high probability of cancer, open surgery remains the gold standard. However, the decision is influenced by the risks of general anesthesia and the surgery itself.
Sensitivity and specificity are high for malignancy (86% and 98.8%, respectively) (6) but drop for benign lesions (7, 8) and smaller nodules (5–7 mm) (9). FNA is optimally used in peripheral nodules, while CNB can be reserved for cases where FNA fails to provide a specific diagnosis, especially in cases of benign disease (10). In our series, a negative but specific result was obtained in 3%, including 12 cases of COP, suggesting that this approach is a viable alternative for confirming diagnosis, as previously described (11). CNB is more likely than FNA to provide a specific benign result. In a group of patients with benign nodules, a specific benign diagnosis was made in 69% of patients with CNB and in 31% of patients with FNA (12). Cutting needles are preferred because the tissue provided is superior, allowing diagnoses to be made and further pathological investigation to be performed, thereby achieving a higher success rate and diagnostic accuracy (88–95% for malignant lesions and 71–97% for benign) (13, 14). Diagnostic performance seems to have improved over the years (15). For NSCLC, FNA is considered an acceptable, minimally invasive procedure for diagnosis and treatment schedule, providing high positive predictive value and concordance between cytology and histologic typing (16). FNA also emerges as an accurate diagnostic tool in SCLC (17).
In our series, using the cut-off of ≤4 cm to define smaller lesions, FNA/CNB ratios were 1.1:1 for large lesions and 4.5:1 for small lesions. The trend leans towards using fine needles for smaller, deeper, and probably malignant lesions, reserving the use of cutting needles for larger, more outlying lesions (2). Previous studies have indicated that additional FNA to CNB does not increase the diagnostic yield in the absence of an on-site cytopathologist (18). However, we have shown that lesion size and procedure choice are the determinants of technical effectiveness; hence, small lesions may produce inadequate sampling, an outcome aggravated by the omission of FNA. FNA procedure may compensate for the potential technical inadequacy of CNB to obtain a diagnostic tissue specimen within the lesion margins, particularly in case of smaller lesions. Consequently, performing CNB alone is not warranted. The choice of needle would also depend upon the patient's coagulation status, the characteristics of each lesion, the access route, and the experience of both the radiologist and the pathologist. The combined use of both FNA and CNB, when feasible, can yield better results than the use of each one alone (19–20).
However, a negative result always poses a diagnostic challenge. A non-specific benign result does not exclude malignancy, and further evaluation is required. The lesion may be malignant, but the sample obtained may lie outside the nodule borders or come from a necrotic area, thus preventing pathologists from establishing a correct diagnosis. Clinical and radiographic follow-up are warranted. If further growth occurs after a non-specific benign diagnosis is obtained with FNA, repeat biopsy or resection is indicated (10).
Cytopathologists and pathologists also have key roles in the interpretation of biopsy specimens. FNA requires the presence of a cytopathologist on-site to assess the adequacy of samples. The diagnostic accuracy of CT-guided needle biopsy of lung lesions can be increased with immediate onsite cytological evaluation (21).
Complication rates are reported in the range of 15–33%; the most common complications are pneumothorax and hemorrhage (22, 23). Pneumothorax occurs in one-quarter of patients but is often not clinically significant. Only a minority of patients with a pneumothorax will eventually require a chest tube (6, 24). In our series, the overall complication rate was 9.7%, and it was associated with lesion size but not localization. Pneumothorax rates are underestimated in our series because small asymptomatic pneumothoraxes were not recorded; only those requiring on-site aspiration or chest tube placement were documented. However, these low rates were consistent with our previous studies (25, 26). The presence of emphysema, deep lesion location, a lengthy procedure, many pleural punctures, and traverse of the fissure, all increase the risk for pneumothorax (27, 28). Since urgent intervention may be required, radiologists who perform lung biopsy procedures must be competent at aspiration of pleural air and insertion of a chest tube (10).
Hemorrhage is almost always self-limiting, although it can occasionally be life-threatening (29). Bleeding complications occur more frequently in patients with bleeding diatheses or pulmonary artery hypertension. We have associated lesion size and malignant histological diagnosis with an increased risk of hemorrhage. Small lesion size and the extent of intrapulmonary needle trajectory are already considered risk factors for both pneumothorax and hemorrhage (30). Previous studies supported this association only as concerns pneumothorax, whereas bleeding risk was associated with CT signs of emphysema (31). No deaths were reported in our series, in consistency with the low rates reported (32).
We used a single needle technique in all our CNB procedures. Multiple-pass co-axial needle systems may reduce the number of pleural passes and rates of pneumothorax, but there is no solid evidence of better diagnostic performance. In addition, the single-pass needle has a lower cost, which was a significant consideration in our center (33, 34).
Our study is limited by its retrospective design. The final diagnosis for negative cases could not be established in the majority of patients unless they were referred for re-evaluation to our department by their attending physicians. Consequently, the final negative predictive values could not be estimated. Additionally, our policy to discharge clinically insignificant pneumothorax precludes an accurate calculation of its rate.
In conclusion, CT-guided FNA/CNB confers a diagnostic alternative with minimal risk and a high diagnostic yield for pulmonary lesions. A risk-adapted, individualized approach in experienced hands can achieve optimal results.