
Abstract
Background
Triple-negative breast cancer (TNBC) is known to be associated with aggressive biologic features and a poor clinical outcome. Therefore, early detection of TNBC without missing cancer is mandatory to improve prognosis.
Purpose
To retrospectively evaluate the mammographic and sonographic features of TNBC compared to ER (+) cancers and HER2 (+) cancers.
Material and Methods
From June 2011 through June 2012, mammographic and sonographic features of 281 surgically confirmed ER (+) cancers (n = 153), HER2 (+) cancers (n = 83), and TNBC (n = 45) were retrospectively reviewed by two radiologists in consensus. The clinicopathological features were also compared between the three subtypes. Additionally the 45 TNBC cases were analyzed using morphologic criteria of ACR BI-RADS lexicon.
Results
Most TNBC (93.3%, 42 of 45) were mammographically seen and presented with mass or focal asymmetry without microcalcifications (P < 0.001). Ultrasonographically TNBC were presented as hypoechoic nodule without microcalcifications (P < 0.001). Palpable symptom (P < 0.001), a lower incidence of ductal carcinoma in situ (P < 0.001), invasive tumor size that is >2 cm (P = 0.028) and high histologic grade (P < 0.001) were significantly associated with TNBC. With regard to morphologic features of 45 TNBC cases, TNBC were most likely to be hyperdense mass (89.3%) with oval (68.9%) or lobular shape (28.6%) and indistinct (42.9%) or circumscribed margin (32.1%) on mammogram. Ultrasonographically TNBC were most likely to be a hypoechoic mass (82.2%) with irregular (68.9%) or oval (28.9%) shape and microlobulated (46.7%), circumscribed (17.8%) or indistinct margin (17.8%) and parallel orientation (68.9%).
Conclusion
Being familiar with combined mammographic and ultrasonographic features of TNBC may be useful to avoid false-negative cases of TNBC.
Breast cancer is a heterogeneous disease composed of different biological subgroups that have various morphologies, clinical outcomes, and responses to systemic therapy. Currently, gene expression analysis based on the extent of the expression of the estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2) has identified several subtypes with common molecular features: Luminal A and B (both ER-positive), normal breast-like, basal-like, and HER2-positive (all three ER-negative) (1, 2). Clinically, breast cancers are categorized into one of three major subtypes, using the three standard immunohistochemical markers, to facilitate targeted therapy; these subtypes are ER (+) cancer, HER2 (+) cancer, and triple-negative breast cancer (TNBC) (3, 4). Indeed, the basal-like subtype is composed almost entirely of triple-negative breast cancer, which is negative for ER, PR, and HER2 (5).
Triple-negative breast cancer (TNBC) is known to be associated with aggressive histologic features, a poor clinical outcome, and a shorter survival compared with other breast cancer subtypes (6–8). Contrary to its aggressive nature, TNBC has been described as having benign morphology by conventional imaging modalities (9–13). Therefore, being familiar with the mammographic and ultrasonographic imaging features of TNBC may help examiner to detect TNBC early without missing false-negative cases. However, to the best of our knowledge, there are a few studies reporting the imaging features of TNBC, especially compared to non-TNBC. In this study, we retrospectively evaluate the clinicopathological, mammographic and ultrasonographic features of triple-negative breast cancer in comparison with ER (+) cancer and HER2 (+) cancer.
Material and Methods
Study population
Our institutional review board approved this study, and the requirement for informed consent was waived. From June 2011 through June 2012, a total of 363 patients underwent surgery to treat breast cancer. Among these patients, 36 were excluded because three patients did not undergo immunohistochemical analysis and 34 patients did not undergo SISH (silver in situ hybridization) for determination of the HER2 status. In addition, 45 patients were excluded due to the non-availability or poor quality of their preoperative mammographic or ultrasonographic images. Finally, 278 patients (mean age, 49.8 years; range, 25–84 years) with 281 breast cancers were included in our study. The indications of initial mammography or ultrasound were as follows: 55.0% (153 of 278) were due to palpability, 39.9% (111 of 278) were for asymptomatic screening, 3.2% (9 of 278) were due to pain and 1.8% (5 of 278) were due to nipple discharge.
Clinicopathologic data
The patients' medical records were reviewed to identify the clinical symptoms (e.g. the presence of a palpable mass). The pathological reports were also reviewed to determine the tumor size, histological grade, and presence of axillary lymph node metastasis. The patients' ER, PR, and HER2 statuses were determined by immunohistochemical analysis. For the immunohistochemical analysis, formalin-fixed, paraffin-embedded tissue sections were immunohistochemically stained. The Allred score was used to determine the ER and PR statuses. The results were classified as positive when the total score, expressed as the sum of the proportion and immunointensity scores, was 3 or more.
With regard to the HER2 evaluation, tumors with a 3+score were classified as HER2-positive and tumors with a 0 or 1+score were classified as negative. In tumors with a 2+score, gene amplification using SISH (silver in situ hybridization) was used to determine the HER2 status. The HER2 expression was considered positive if the ratio of the HER-2 gene copies to the chromosome 17 signal was>2.
Imaging analysis
Mammography was performed using a Selenia system (Lorad, Bedford, CT, USA). Standard two-view mammography (mediolateral oblique and craniocaudal) was performed, with additional views as deemed necessary. Breast ultrasound (US) was performed using 5–12-MHz transducers with an IU-22 (Philips Medical Systems, Best, The Netherlands) by two breast imaging radiologists.
Two breast radiologists with 4 and 8 years of clinical experience (MYK and NC) retrospectively reviewed the mammographic and ultrasonographic images in consensus without knowledge of the clinicopathological findings of the cases. On mammograms, lesions were described as mass or focal asymmetry with or without microcalcifications. If the lesion was associated with microcalcifications, the microcalcification was described as fine linear or pleomorphic, amorphous, or punctate. Breast density was also rated as fatty, scattered fibroglandular, heterogeneously dense, or dense. On ultrasonography, lesions were described as mass with or without microcalcifications. Also, both mammographic and ultrasonographic images of TNBC were reviewed by two radiologists in consensus. For image interpretation of TNBC, American College of Radiology Breast Imaging Reporting and Data System Lexicon was used for morphologic criteria (14).
Statistical analysis
The clinicopathological, mammographic, and ultrasonographic features were compared between the three tumor subtypes using the chi-square or Fisher's exact tests for categorical variables and Student's t-test for continuous variables. All statistical analyses were carried out using SPSS version 17.0 for Windows (SPSS, Chicago, IL, USA), and P values<0.05 were considered significant.
Results
Clinicopathological and imaging features according to the tumor subtype
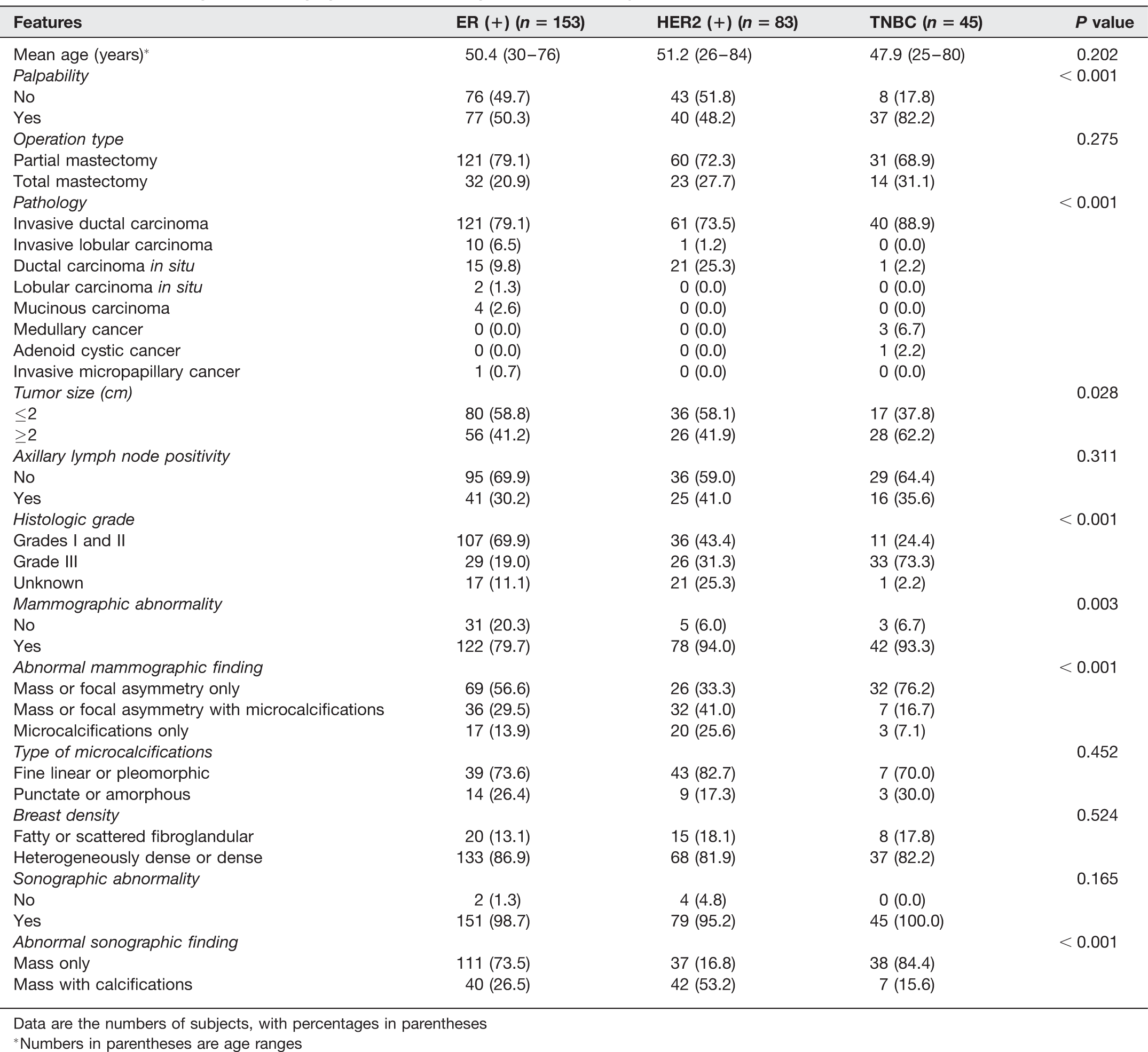
Data are the numbers of subjects, with percentages in parentheses
*Numbers in parentheses are age ranges
Pathologically invasive ductal carcinoma was the most common histologic type in ER (+) cancer (79.1%, 121 of 153), HER2 (+) cancer (73.5%, 61 of 83), and TNBC (88.9%, 40 of 45). Significantly lower incidence of ductal carcinoma in situ (DCIS) was observed in TNBC (2.2%, 1 of 45) compared to ER (+) cancer (9.8%, 15 of 153) and HER2 (+) cancer (25.3%, 21 of 83). All medullary (n = 3) and adenoid cystic (n = 1) carcinomas were TNBC.
By mammography, TNBC, ER (+) cancer, and HER2 (+) cancer were detected in 93.3% (42 of 45), 79.7% (122 of 153), and 94.0% (78 of 83) of the patients (P = 0.003), respectively. Masses or focal asymmetries without microcalcifications (76.2% in TNBC vs. 33.3% in HER2 (+) cancer vs. 56.6% in ER (+) cancer; P < 0.001) were significantly associated with TNBC, compared to ER (+) cancer and HER 2(+) cancer (Fig. 1). The types of microcalcifications and breast density were not different between the tumor subtypes (P = 0.452, P = 0.524). By ultrasonography, ER (+) cancer, HER2 (+) cancer, and TNBC were detected at levels of 98.7%, 95.2%, and 100% (P = 0.165), respectively. The presence of mass or focal asymmetry lacking microcalcifications (84.4% in TNBC vs. 16.8% in ER (+) cancer vs. 73.5% in HER2 (+) cancer; P < 0.001) was significantly associated with TNBC.
A 26-year-old woman with palpable left breast mass. Left craniocaudal (a) and mediolateral oblique view (b) of mammograms showed an oval circumscribed hyperdense mass in the left upper outer quadrant and enlarged axillary lymph nodes with absence of fatty hilum, suggesting metastasis. Ultrasonographic images (c, d) showed a 3 cm oval microlobulated hypoechoic mass with posterior enhancement, which was classified as BI-RADS category 4. Two enlarged lymph nodes with cortical thickening were seen in left axilla. 14G gun biopsy was performed for the mass, which was confirmed to be invasive carcinoma. She underwent breast conserving surgery, which revealed a 2.8 cm medullary carcinoma with histologic grade III, and none of the six dissected axillary lymph nodes had metastasis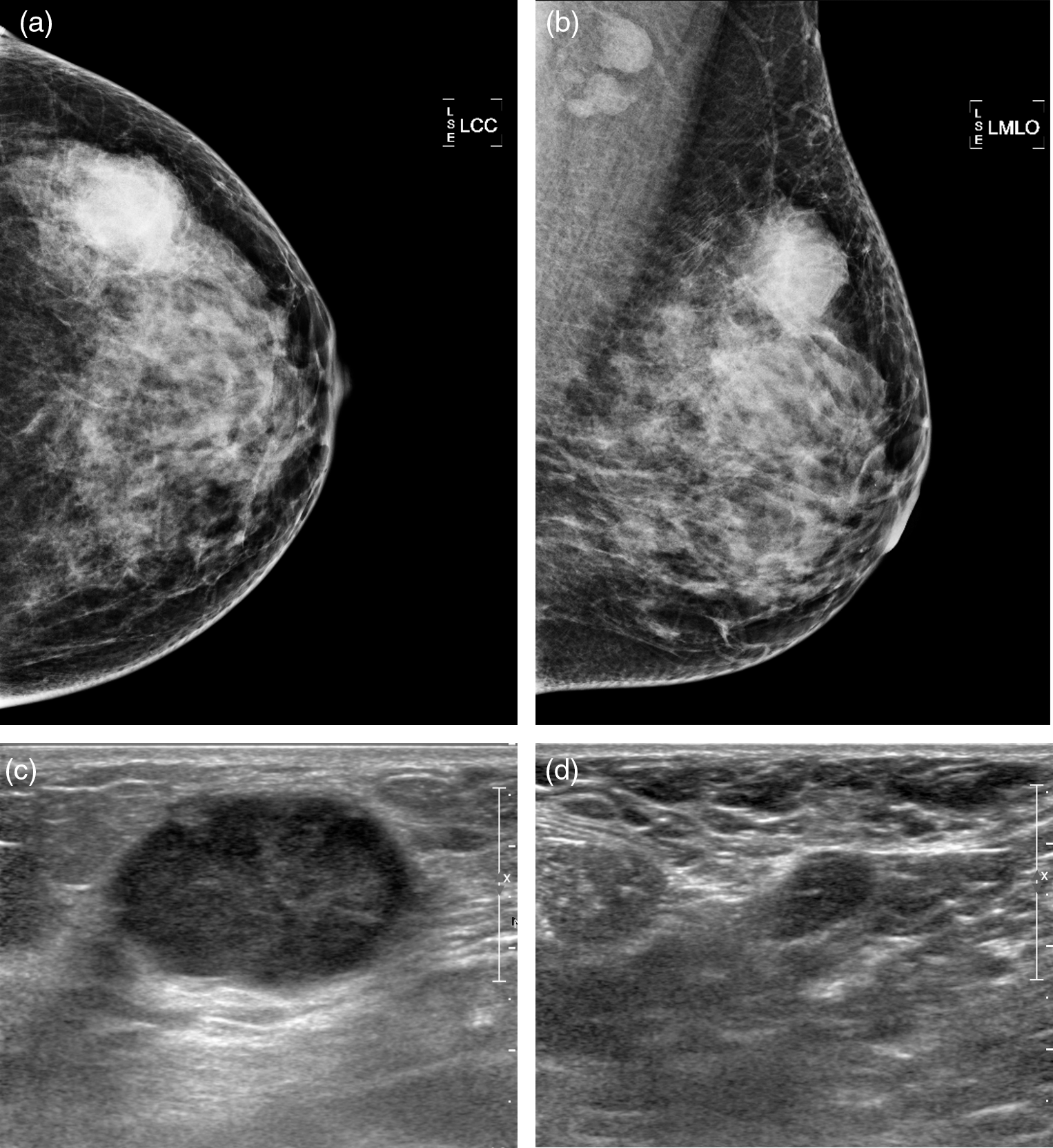
Mammographic findings of 28 triple-negative breast cancers presenting as masses
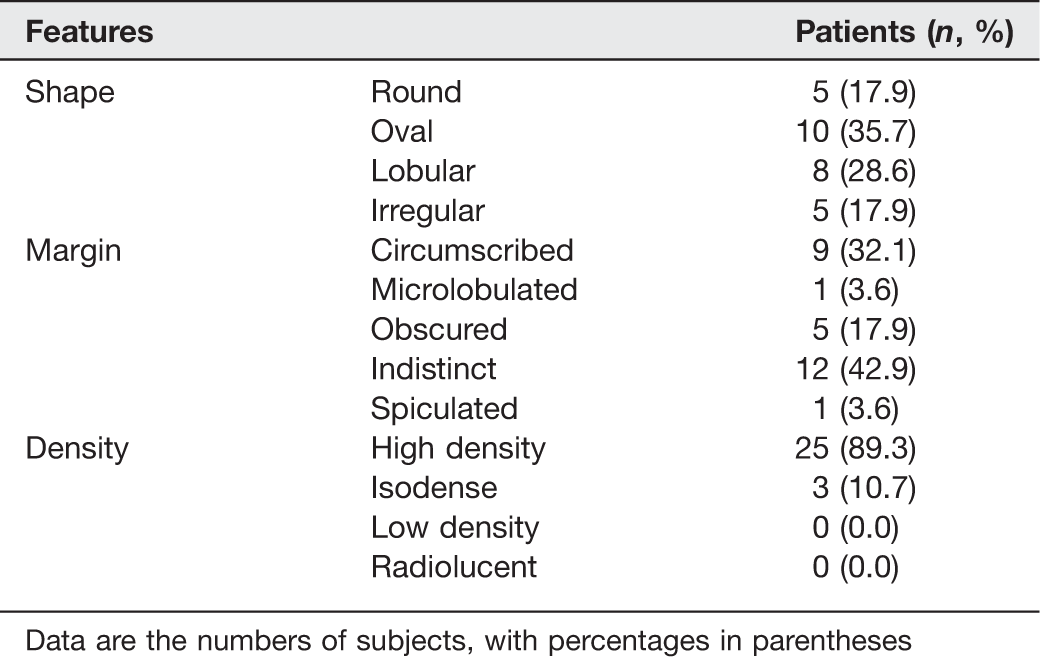
Data are the numbers of subjects, with percentages in parentheses
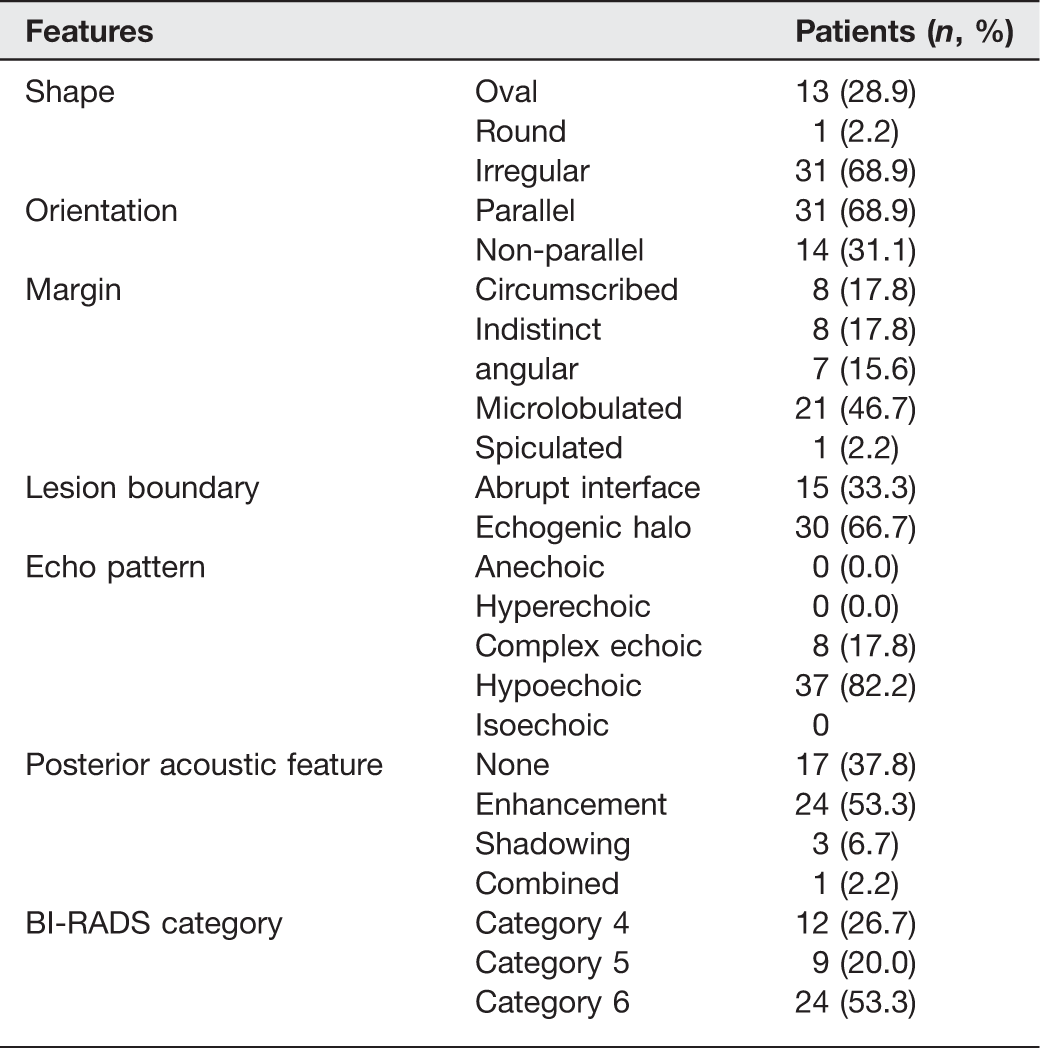
Ultrasonographic findings of 45 triple-negative breast cancers
Discussion
Triple receptor-negative cancer (TNBC) is a subtype of breast cancer characterized by a lack of expression of ER, PR, and HER2 (1). Many authors have reported that TNBC shows aggressive biologic features and is associated with high incidence of interval cancer due to rapid growth pattern (4–8). Compared with non-TNBC, TNBC cases are of high histologic grade, high nuclear grade, and unfavorable histology, such as anaplastic or metaplastic carcinoma (15, 16).
Histopathologically, similar with prior reports, invasive tumor size that is > 2 cm (62.2%, 28 of 45) and high histologic grade (33 of 45, 75%) were more often in TNBC compared to non-TNBC in our study. As a result, TNBC was associated with palpable symptom (82.2%) and subsequently detected clinically rather than with imaging. And, there was no difference in the rate of axillary lymph node positivity between the tumor subtypes (30.2% in ER (+) cancer, 41.0% in HER2 (+) cancer, and 36.4% in TNBC; P = 0.311). Generally the larger the tumor, the rate of lymph node positivity increase, but this relationship was not observed in TNBC. Foulke et al. explained this phenomenon by mode of spread of TNBC and it is thought that TNBC spread hematogenously due to early vascular invasion (17).
Our results showed that most TNBC cases (93.3%, 42 of 45) were mammographically detected, and only 6.7% (3 of 45) were mammographically occult. As TNBC often presented clinically with a palpable mass (82.2%), mammographic examinations were frequently diagnostic rather than screening. By mammography, TNBC most commonly appeared as a mass or focal asymmetry lacking microcalcifications. The mass margin was more commonly indistinct (42.9%) and less commonly circumscribed (32.1%). These results are consistent with prior studies, which reported that TNBC was most likely a mass without calcifications by mammography (average 57.1%, 352 of 616) (9–12). Traditionally mammographic microcalcification is a hallmark feature of DCIS (18). In our results, a significantly lower incidence of DCIS was observed in TNBC compared with ER (+) cancer and HER2 (+) cancer (25.3%, 21 of 83), which may explain why TNBC is less likely to be associated with calcifications by mammography. Similarly, Yang et al. reported that TNBC is less likely to be associated with DCIS, which is concordant with a lack of mammographic calcifications (12).
With regard to ultrasonographic findings of TNBC, it was reported that TNBC shows circumscribed or lobulated margin more often rather than spiculated or angular margin (9, 13). Wojcinski et al. described this smooth appearance as a pushing border that is associated with non-infiltrative process by rapid tumor growth. In our study, TNBC was likely to be hypoechoic mass (82.2%) or complex mass (17.8%) with microlobulated (46.7%) or circumscribed (17.8%) or indistinct (17.8%) or angular (15.6%) margin (13). Mass lesion with circumscribed margin might be misinterpreted as benign. In such circumstances, we believe that microlobulated margin might be useful to avoiding false-negative cases of TNBC. Unlike prior studies, echogenic halo was observed more often in TNCB (66.7%) in our study. We suppose that the echogenic halo results from peritumoral edema caused by severe peritumoral inflammation which is representatively seen in high grade invasive carcinoma (19). TNBC were more likely to be associated with posterior acoustic enhancement (53.3%). It is well-known that high grade, highly cellular circumscribed carcinomas tends to have enhanced through-transmission (19). With regard to orientation of the tumor, TNBC were more likely to be horizontally orientated (68.9%), which is usually associated with benign nodule. This finding can be explained by a relatively large tumor size of TNBC at presentation. Traditionally a taller than wide shape is characteristic for small carcinoma (20). A growing tumor with pushing margins (expanding and not invading) would respect the limits of a breast segment or lobe, the functional unit of the breast. Indeed, in our study, invasive tumor size that is >2 cm was more often in TNBC (62.2%) compared to non-TNBC (41.2% for ER (+) cancer, 41.9% for HER2 (+) cancer) (P = 0.028).
Our study has several limitations. First, our study is retrospective, and its sample size was small. Second, we did not evaluate inter-observer variability regarding the classification of mammographic and ultrasonographic features which were carried out in consensus in our study. Third, we did not analyze the imaging features of TNBC according to the cancer stage, which might influence the imaging features at diagnosis. Fourth, we did not include the findings of other imaging modalities such as MRI, which may be more sensitive for the diagnosis of TNBC.
In conclusion, combined mammographic and ultrasonographic features of mass or focal asymmetry without microcalcifications that is hypoechoic mass with microlobulated or circumscribed margin can be suggestive of presence of TNBC. Ultrasonographically microlobulated margin can be helpful in avoiding false-negative cases of TNBC, especially when the nodule is horizontally-oriented. Being familiar with combined mammographic and ultrasonographic findings of TNBC would be useful for early detection of TNBC without missing cancer.