
Abstract
Background
Thyroid cancer is one of the common head and neck malignancies and may be found incidentally with other head and neck cancers.
Purpose
To evaluate the prevalence and risk of malignancy in incidental thyroid lesions identified by ultrasound (US) in patients with head and neck cancer.
Material and Methods
We retrospectively reviewed medical records of all patients with head and neck cancer other than of thyroid origin between January 2004 and December 2011. A total of 690 patients (537 men and 153 women; mean age, 58.9 ± 12.9 years) underwent US of the neck for the evaluation of cervical lymph node status (including thyroid gland). We evaluated the prevalence of patients with incidental thyroid lesions identified by US and the risk of malignancy in these patients.
Results
Of the 690 patients with head and neck cancer, 234 (33.9%) had incidental thyroid lesions on US. Based on US findings, 61 patients underwent fine-needle aspiration, with 39 eventually undergoing thyroidectomy. Among these thyroid lesions, 24 incidental thyroid lesions of 22 patients were histologically proven to be malignant (23 papillary and 1 follicular carcinomas). The risk of malignancy was 9.4% on a patient-by-patient basis.
Conclusion
Screening of the thyroid gland should be included in the preoperative US examination for cervical lymph node metastases in patients with non-thyroidal head and neck cancer.
Introduction
Thyroid nodules are relatively common in the general population, with a reported prevalence of up to 50% at autopsy studies in adults with no thyroid-related disease (1). Incidental thyroid lesions (so-called thyroid incidentalomas) are defined as newly identified focal thyroid lesions encountered during imaging studies of the neck performed for reasons other than evaluation of the thyroid gland, such as ultrasound (US) (2–7), computed tomography (CT) (8,9), magnetic resonance imaging (MRI) (8,10), and 18 F-fluorodeoxyglucose (FDG) positron emission tomography (PET) or PET/CT (11–17). The further evaluation and management of these incidental thyroid lesions is an area of ongoing debate and present a challenge to both radiologists and clinicians (18).
Thyroid cancer is one of the common head and neck malignancies and may be found incidentally with other head and neck cancers. However, to our knowledge, there have been few studies to investigate incidentally detected lesions of the thyroid gland in patients with head and neck cancer (7,15).
The purpose of our study was to determine the prevalence and the risk of malignancy of incidental thyroid lesions identified by US in patients with non-thyroidal head and neck cancer.
Material and Methods
The protocol of this study was reviewed and approved by the institutional review board, and informed consent was waived as the patients' medical records and images were evaluated retrospectively and anonymously.
Patients
We retrospectively reviewed the medical records of all patients undergoing surgery for malignant tumors of the head and neck during the period from January 2004 to December 2011. A total of 709 patients underwent US of the neck (including thyroid gland) for the preoperative evaluation of cervical lymph node status during this period. It has been routine practice at our institution to screen the thyroid gland when surveying cervical lymph nodes in patients with known head and neck cancer. Among them, 19 studies were excluded because they: (i) revealed diffuse thyroid disease without a focal nodular appearance (n = 16); or (ii) were performed in patients with prior thyroidectomies (n = 3). This yielded a final study population of 690 patients (537 men and 153 women; mean age, 58.9 ± 12.9 years; range, 18–91 years). Sites of primary head and neck cancers were the larynx (n = 160), tongue (n = 111), hypopharynx (n = 83), tonsil (n = 78), oral cavity (n = 54), salivary gland (n = 51), paranasal sinus (n = 44), hard or soft palate (n = 35), nasopharynx (n = 26), and others (n = 48).
Thyroid US and US-guided FNA
Patients with focal thyroid lesions suspicious for malignancy subsequently underwent US-guided fine-needle aspiration (FNA). The FNA indications used in our institution were: (i) micro- or macrocalcifications; (ii) spiculated margins; (iii) markedly hypoechoic appearance; (iv) taller-than-wide shape; or (v) internal vascularity on color Doppler US.
All US and US-guided FNAs were performed by two radiologists (DYY and YLS), who had > 10 years of experience in thyroid and neck US, with an iU 22 ultrasound unit (Philips Medical Systems, Bothell, WA, USA) or Acuson Sequoia 512 (Siemens Medical Solutions, Mountain View, CA, USA) using a 5–15-MHz linear array transducer.
The FNA results were classified into the following four categories: malignant, suggestive (follicular neoplasm, Hürthle cell neoplasm, suspicious for papillary cancer), benign, and non-diagnostic (insufficient cells for diagnosis). Thyroidectomy was recommended for all patients with malignant or suggestive findings. Patients with benign or persistently non-diagnostic FNA results were routinely followed up by postoperative US.
Data analysis
The radiology reports, FNA biopsy results, the final pathology results, and medical records for these patients were reviewed by a radiologist (HCK). The main outcome measures were the prevalence and risk of malignancy of incidental thyroid lesions. The base rate and 95% confidence intervals (CIs) were computed using the Pearson’s confidence intervals. Comparisons between different groups were performed with the paired Student t-test for continuous variables and the chi-square test for categorical variables. A P value < 0.05 was considered to indicate a statistically significant difference. Statistical analysis was performed with commercially available software (SPSS 19.0 for Windows; SPSS, Chicago, IL, USA).
Results
Of 690 patients with head and neck cancer, 234 patients (33.9%; 95% CI, 30.4–37.4%) (152 men and 82 women; mean age, 62.5 ± 11.8 years) had one or more incidentally found focal thyroid lesions on US. Ninety-nine patients had a single thyroid nodule, 40 had two nodules, 12 had three nodules, and 83 had four or more nodules.
A significant age difference was found comparing patients with incidental thyroid lesions detected by US (mean age, 62.5 ± 11.8 years) and those without such findings (mean age, 57.1 ± 13.1 years) (P = 0.0000). In addition, the prevalence of incidental thyroid lesion was significantly higher in women (82/153; 53.6%) than in men (152/537; 28.3%) (P = 0.0000).
Based on US findings, 61 (26.1%) of 234 patients underwent US-guided FNA of the identified thyroid nodule on suspicion of malignancy. Among them, 10 patients had non-diagnostic FNA results and were followed-up with periodic US examinations after treatment of head and neck cancer. Thirty-nine patients underwent surgery for head and neck malignancies combined with thyroidectomy; 22 underwent total and 17 underwent partial thyroidectomy. In total, histopathological diagnosis was obtained in 56 patients (by FNA in 17, by FNA and surgery in 34, and by surgery in five).
Of these 56 patients, 24 focal thyroid lesions from the 22 patients were histologically proven to be malignant (23 papillary and one follicular carcinomas). Three patients had additional papillary microcarcinomas discovered by histologic examination of thyroidectomy specimen in locations away from the thyroid lesions found on US. Lymph node metastases from the thyroid cancer were proved in the central compartment (level VI) in two patients and in both central and lateral compartments in two patients. One patient had distant metastasis that was proven to be metastatic thyroid cancer by surgery. The TNM staging (19) was T1N0M0 in 18 patients, T1N1aM0 in two patients, T2N1bM0 in one patient, and T3N1bM1 in one patient. Twelve malignant nodules (50.0%) were in the right lobe, 10 (41.7%) in the left lobe, and two (8.3%) in isthmus of the thyroid. The size of the malignant thyroid nodules was in the range of 4–19 mm (mean, 9.8 ± 3.9 mm). The remaining 42 thyroid lesions from the 34 patients were histologically proven to be benign (nodular hyperplasia in 29, follicular adenoma in 10, and chronic thyroiditis in three).
Two hundred and twelve patients who did not undergo total thyroidectomy were subject to US follow-up investigations to decide the nature of incidentally detected lesions. Among them, US follow-up was not performed in 47 patients because they were followed up with other modalities (n = 30), lost to follow-up (n = 13), or died during the follow-up (n = 4). In the remaining 165 patients, US follow-up (for evaluation of both recurrent head and neck cancer and thyroid nodules) was performed (mean, 24.0 ± 18.5 months; range, 4–106 months) and demonstrated no radiologic evidence of thyroid malignancy in any of these patients.
Overall, of the 234 patients with incidental thyroid nodules discovered on US, 22 had a thyroid malignancy. If one assumes that all non-biopsied lesions were benign, the risk of malignancy for the entire population of patients with incidental thyroid lesions was 9.4% (22/234; 95% CI, 7.5–11.3%) on a patient-by-patient basis. No statistically significant difference was found between the malignant and benign groups with regard to age and sex (P = 0.1923 and 0.7638, respectively).
Discussion
Incidental thyroid lesions has been found with increasing frequency in the general population, as well as in cancer patients, likely a result of the widespread availability and advanced technology of imaging studies (20). Discovery of these lesions raises concern about malignancy and represents a significant dilemma, because there is no consensus regarding the most appropriate approach to management.
Reported prevalence of incidental thyroid lesions detected on US, CT, MR, PET, and PET/CT.
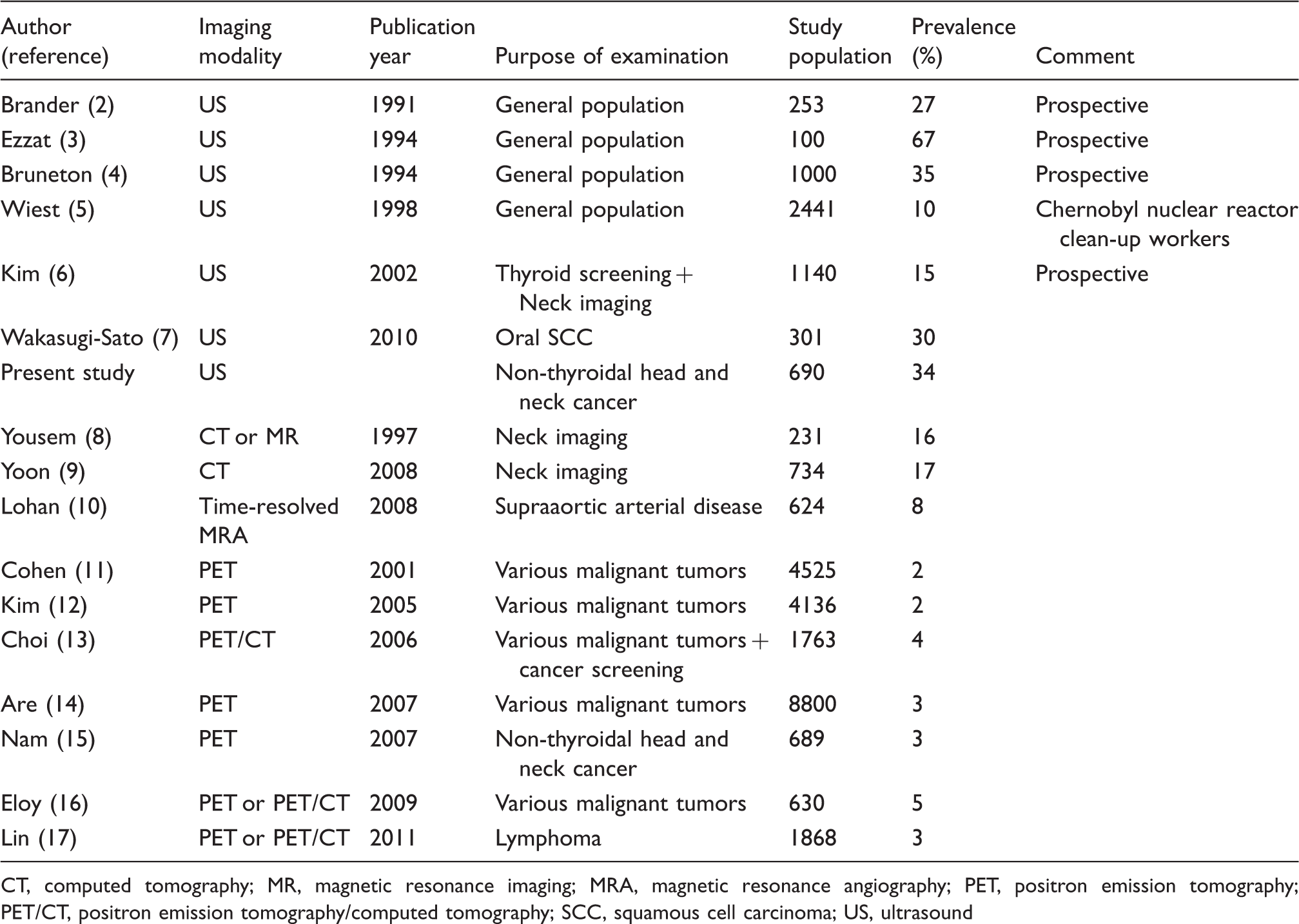
CT, computed tomography; MR, magnetic resonance imaging; MRA, magnetic resonance angiography; PET, positron emission tomography; PET/CT, positron emission tomography/computed tomography; SCC, squamous cell carcinoma; US, ultrasound
Several previous studies have documented various prevalence of incidental thyroid lesions as determined by other imaging techniques. Incidental thyroid lesions have been reported in 16–17% of cross-sectional scans (CT or MR) (8,9), 8% of time-resolved MR angiography (10), and 2–5% of PET or PET/CT scans (11–17) (Table 1).
The current widespread usage of whole-body FDG-PET and FDG-PET/CT in metastasis work-up of cancer patients has resulted in an increase in the detection of incidentally found thyroid lesions. Previous studies reported that the prevalence of PET or PET/CT identified thyroid incidentalomas ranged from 2% to 5% in a group of patients with various malignant tumors. These focal thyroid lesions identified by PET have been found to be associated with a high risk of malignancy, ranging from 30% to 50% (11–17).
This is the first large series which examines the prevalence as well as the significance of incidental thyroid lesions detected by US in patients with head and neck cancer. So far, there is only one study that has evaluated the US prevalence of incidental thyroid lesions in patients with non-thyroidal head and neck cancer. Wakasugi-Sato et al. (7) reported that incidental thyroid lesions were noted in 30% (90/301) of patients with oral squamous cell carcinoma who underwent US examinations for the detection of cervical lymph node metastases. In their study, however, no primary thyroid cancer was diagnosed in these 90 patients on further assessment (they did not mention how many patients underwent FNA or thyroidectomy).
Our prevalence of incidental thyroid lesion (33.9%) is similar to that of a previous report by Wakasugi-Sato et al. (7), who reported a prevalence of 30% in a group of patients evaluated for oral cavity cancer. However, different sex composition in our study group, as compared to the male-to-female ratio (1 : 1) of subjects in Wakasugi-Sato’s report, may underestimate the true prevalence of incidental thyroid lesion. Given the male predominance in head and neck cancer, our patient population consists of up to 80% of male patients; it is known that the prevalence of thyroid nodules is higher in women than in men (2–4).
In addition to detection and accurate localization of thyroid nodules, US also has the potential to characterize the lesions. Many studies have been published in which the ability to differentiate malignant from benign thyroid nodules on the basis of US findings was assessed. US features predictive of malignant nodules include taller-than-wide shape, spiculated margin, marked hypoechogenicity, absence of a halo, predominantly solid composition, the presence of micro- or macrocalcifications, and intranodular vascularity (21). In the present study, we followed the recommendations for FNA of thyroid nodules derived from a consensus statement by one of the large radiology groups (22).
Because incidental thyroid nodules are common, assessment of the risk of malignancy is important for appropriate management. In autopsy series, the reported risk of malignancy of asymptomatic thyroid nodules ranges from 2.9% to 12.5% on patient-by-patient basis (1,23,24). It is difficult to evaluate the real risk of malignancy in patients with incidental thyroid lesions on US because of different existing criteria in the selection of candidates for FNA or thyroidectomy. The risk of malignancy in incidental thyroid lesions in our study (9.4%) is in the low range of those of previous US studies, which has been reported as 7.7–21.6% (25–28).
The identification of incidental thyroid lesions may affect surgical planning in patients with head and neck cancer. These lesions deserve further diagnostic work-up prior to the treatment of head and neck malignancies to ensure adequate therapy and to avoid a second-stage operation. The easy availability and good cost-effectiveness of high-resolution US and US-guided FNA should encourage a more aggressive approach. Although some studies have shown substantial false-negative rates (29,30), US and US-guided FNA of thyroid nodules have been proven to be the methods of choice for diagnosing malignancy (31,32).
Most malignant lesions detected in our study were papillary carcinoma ranging from T1N0M0 to T1N1aM0, which generally has a high rate of long-term survival if treated appropriately with thyroidectomy. This suggests that early detection of the incidental thyroid cancer in patients with head and neck cancer may have a favorable influence on the survival of such patients.
A major limitation of our study is the fact that not all incidentally found thyroid lesions could be confirmed histologically in this retrospective study. We assumed that all non-histologically confirmed lesions were benign, and we used the total number of patients in the series as a denominator in the calculation of the prevalence of malignant lesions. Therefore, it is conceivable that this selection bias for histological diagnosis may result in underestimation of the true rate of malignancy among the incidental thyroid lesions detected on US. Furthermore, most benign conditions were diagnosed on the basis of FNA. Since US-guided FNA of thyroid nodules can be associated with substantial false-negative rates (29,30), some cancers may have been misclassified as benign lesions in our study.
In conclusion, the prevalence of incidental thyroid lesion identified by US was 33.9% (234/690) in this study, and the rate of malignancy was at least 9.4% (22/234) among these incidental thyroid lesions. We propose that screening of the thyroid gland should be included in the preoperative US examination for cervical lymph node metastases in patients with non-thyroidal head and neck cancer.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.