
Abstract
Background
Conventional magnetic resonance imaging (MRI) can only show the degeneration-induced morphological changes but fail to quantitatively reveal the degree and extent of the axonal damage of nerve fibers. Diffusion tensor imaging (DTI) has the ability to detect the diffusion of water molecules and thus suitable to the study of axonal degeneration of central motor neurons.
Purpose
To illustrate and quantitatively evaluate the axonal degeneration of central motor neurons in patients with chronic cerebral stroke.
Material and Methods
DTI and conventional MRI were carried out with 10 normal control subjects and 25 patients who suffered from chronic cerebral stroke in the region supplied by middle cerebral artery and had varying degrees of limb movement disorders (the mean time of onset was 2.5 months), to measure the fractional anisotropy (FA), volume ratio (VR), apparent diffusion coefficient (ADC), tensor eigenvalues (λ1, λ2, and λ3), and signal intensity (SI) on T2-weighted images, of the central motor fibers (pyramidal tract) in the plane of cerebral peduncle. Results from the ipsilateral side were compared with those from the contralateral side in the same patient and with those from normal control.
Results
The axonal degeneration of central motor neurons manifests in DTI as the decline of FA of the pyramidal tract and the reduction and distortion of the high signal area. While all the FA, VR, ADC, and λ1 in the ipsilateral side reduce on DTI, λ3 increases; the T2-weighted signals exhibit no significant differences among groups.
Conclusion
The changes and diffusions of water molecule associated with the axonal degeneration of central motor neurons after chronic cerebral stroke can be detected by DTI, which can directly quantitatively reflect the degree and extent of axonal degeneration of central motor neurons and can compensate the shortcomings of conventional MRI and diffusion-weighted imaging (DWI).
Keywords
Introduction
Axon of nerve fiber or axon and myelin near the cell body of damaged neurons undergo anterograde degeneration that is also known as Wallerian degeneration. The occurrence of axonal degeneration in central motor neurons is closely related to the treatment and prognosis of patients with cerebral stroke, especially associated with the long-lasting damage to their motor functions (1). However, conventional magnetic resonance imaging (MRI) can only show the degeneration-induced morphological changes in some of the patients but fail to quantitatively reveal the degree and extent of the axonal damage of nerve fibers. To the contrast, diffusion tensor imaging (DTI) has the ability to detect the diffusion of water molecules and can provide information regarding the direction and intensity of water diffusion in the white matters to reveal the characteristics of tissue microstructure, which makes it suitable to the study of axonal degeneration of central motor neurons in patients with chronic cerebral stroke.
Material and Methods
Subjects
The study protocol was approved in accordance with the recommendations of the human research committee. All patients gave written informed consent.
Study group
This group included 25 patients, 14 men and 11 women, with a mean age of 65.6 ± 4.9 years, who visited our hospital for treatment of chronic cerebral strokes in the area supplied by the middle cerebral artery and suffered varying degrees of movement disorders. While the stroke lesions were mostly in the deep white matter in periventricular region, semioval center, or corona radiata, cortical areas were also implicated in some of the cases. The patients with old or asymptomatic lesions or with infarct lesions not in the path of central motor nerve fibers were excluded from this study.
Control group
This group contained four men and six women, with a mean age of 63.5 ± 7.1 years, who were healthy people with no special disease and performed MRI just because of general physical examination or body discomfort. There was no significant difference in age composition between both groups (P = 0.682). Each subject was informed with the purpose and methods of the study and signed informed consent.
MRI scanning method
All the patients in the study group underwent conventional MRI scans and serial DTI scans 2.5 months after the onset of cerebral stroke. All the subjects in the control group underwent conventional MRI scans and serial DTI scans, under the same scan protocol as the study group.
Conventional MRI scans
Transverse, sagittal, and coronal scans were carried out with a 1.5T whole-body scanner (Signa; GE Healthcare, Milwaukee, WI, USA), using phased-array head coil and fast spin echo sequence (FSE) and fast relaxation fast spin echo sequence (FRFSE). The scanning parameters were as follows: FSE T1-weighted image (TE, 12.2–12.5 ms; TR, 560–820 ms); FRFSE T2-weighted image (TE, 97–108 ms; TR, 3000–3500 ms); slice thickness, 5 mm; slice spacing, 2 mm; matrix, 256 × 256; and number of excitations (NEX), 2.
DTI scans
The parameters for DTI scan were as follows: diffusion-sensitizing gradient orientations, 13; b value, 1000 s/mm2; TR/TE, 10,000/110 ms; FOV, 24 × 24 cm; matrix, 256 × 128; number of slices, 20; slice thickness, 5 mm; slice spacing, 0; and NEX, 2.
Postprocessing
The diagrams of FA, VR, and ADC were obtained after processing the data on workstation using Functool II software (Sun; GE Healthcare, Milwaukee, WI, USA). The respective values of FA (the higher the value, the higher the signal), VR, and ADC (the value positively correlates with the signal intensity) were measured individually. The diffusion tensor eigenvalues were measured using the latest version of Volume-one 1.64 and diffusion tensor visualizer 1.5 (DTV) software developed by the Laboratory of Imaging Calculation and Analysis, Department of Radiology, Tokyo University Hospital, Japan. The isotropic data were obtained by z-axis interpolation method (voxel size 0.9 × 0.9 × 0.9 mm), and the eigenvalues λ1, λ2, and λ3 corresponding to the three eigenvectors were obtained using the diagonal method and the method of least-squares based on the diffusion tensor components within each voxel.
Setting the region of interest (ROI)
According to the anatomical location of the pyramidal tract of central motor neurons (from the cerebral motor cortex via the internal capsule and cerebral peduncle to the pons), combined with information from T2-weighted image and FA diagram, the ROI was set at 3/4 outside the cerebral peduncle (Fig. 1) with a control size of approximately 16 pixels. The size of ROI was maintained as consistent as possible among individual subjects. The ratios between parameters of both ipsilateral and contralateral sides, such as rFA, rADC, et cetera (e.g. rFA = ipsilateral FA/contralateral FA), were calculated with each patient.
Localization of the ROI in the cross-sectional plane at the level of cerebral peduncle. (a) Cross-sectional FA image at the level of cerebral peduncle (FA values were measured in ROI selected at the outer 3/4 of cerebral peduncle); (b) cross-sectional T2-weighted image at the level of cerebral peduncle showing the anatomical location of ROI.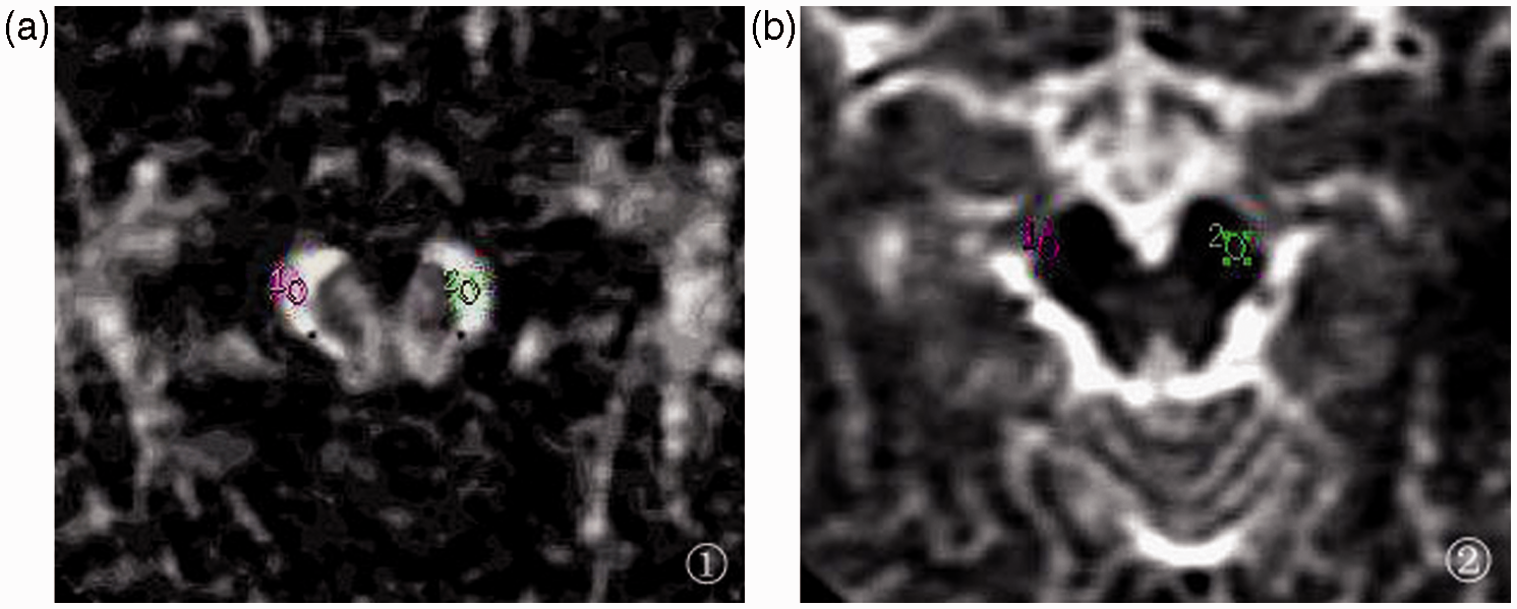
Statistical analysis
All the data were analyzed using statistical software package SPSS 11.5 (SPSS Inc., Chicago, IL, USA) and presented as mean ± standard deviation (SD). The indices from both ipsilateral and contralateral sides in the study group were compared and analyzed using paired samples t-test, while the parameters between both study and control groups were compared with independent sample t-test.
Results
Manifestation of axonal degeneration of the central motor neurons on MRI
The primary lesions in this series of cases were located in the deep white matters in periventricular region, semioval center, or corona radiata, and accompanied by implication of cortex in some of the cases. The images showed characteristics of typical chronic cerebral stroke, while T1-weighted image signals were low, the signals in T2-weighted image were high; the FA values of DTI were reduced, while the ADC values increase. In the conventional T1-weighted and T2-weighted images, the volume of cerebral peduncle in ipsilateral side was smaller than that in the contralateral side. Although slightly lower T1 and somewhat higher T2 signals of the pyramidal tract of central motor nerves could be vaguely detected, these images failed to clearly differentiate the pyramidal tract of central motor nerves that undergoes axonal degeneration. To the contrast, FA images of DTI clearly revealed the axonal degeneration of central motor neurons at the level of cerebral peduncle, which manifests as declined extent of high signal of central motor pyramidal tract, reduced signal intensity, and morphological changes. The anisotropy analysis of central motor pyramidal tract demonstrated that FA values in the ipsilateral side significantly decreased compared with those in the contralateral side. However, for the infarct lesions that were not in the path of central motor nerve fibers, axonal degenerations remained undetectable even with DTI. Although ADC image was able to reveal the morphological changes of cerebral peduncle, it could not directly show the signal abnormalities of central motor pyramidal tract (Figs. 2 and 3).
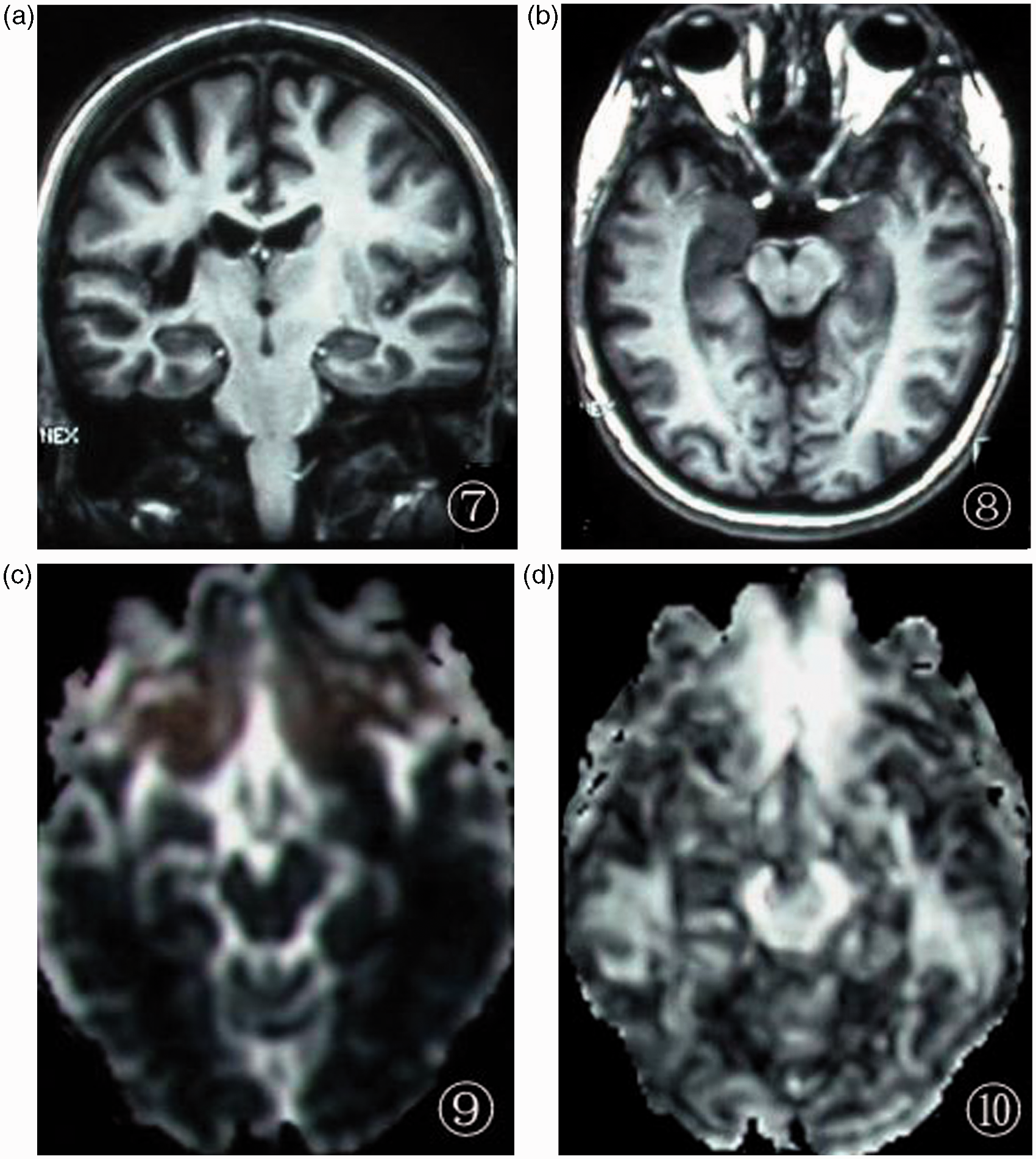
MRI manifestation of the brain of a 68-year-old male patient 2 months after the cerebral stroke. (a) Coronal T2-weighted image indicates that the primary lesion (wide arrow) is located in the right radiation crown, presenting as high signal, however, without the sign of central motor pyramidal tract; (b) coronal ADC image of the primary lesion manifests as slightly higher signal with no sign of central motor pyramidal tract; (c) coronal FA image shows that bilateral banded structures of central motor pyramidal tract are visible as high signal; the central motor pyramidal tract under the lesion in right side (narrow arrow) is narrower than that in the contralateral side, and the signal also becomes lower (FA value decreases); (d) transverse FA image shows the asymmetric bilateral cerebral peduncles and the defective, deformed high signal area of right central motor pyramidal tract (short arrow), suggesting decreased anisotropy and FA values. MRI manifestation of the brain of a 30-year-old female patient who has suffered from cerebral stroke for 3 months with residual limb dysfunction. (a) Coronal T1-weighted image shows low signal of the primary stroke lesion in the right side, with implication of the right insular cortex and the posterior portion of right caudate nucleus, however, without a clear sign of the central motor pyramidal tract; (b) transverse T1-weighted image shows the asymmetric bilateral cerebral peduncles and the significantly reduced size of right cerebral peduncle compared with that of the contralateral one; (c) transverse ADC image also indicates the asymmetric bilateral cerebral peduncles with atrophy in the right side, however, without an observable sign of the central motor pyramidal tract; (d) transverse FA image shows the atrophy of right central motor pyramidal tract at the level of cerebral peduncle, narrowing of the extent of high signal, and reduced FA values compared to those in the contralateral side.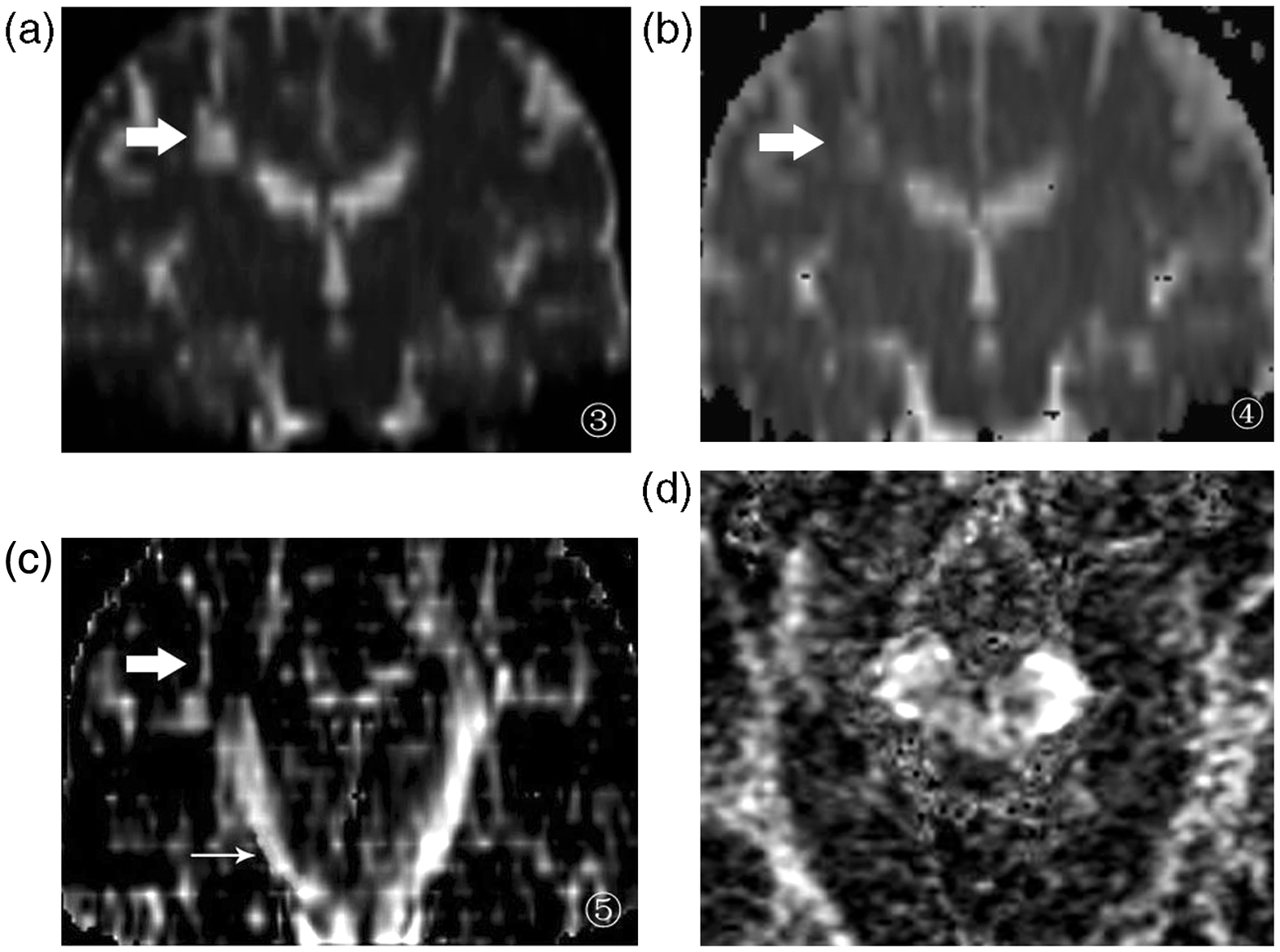
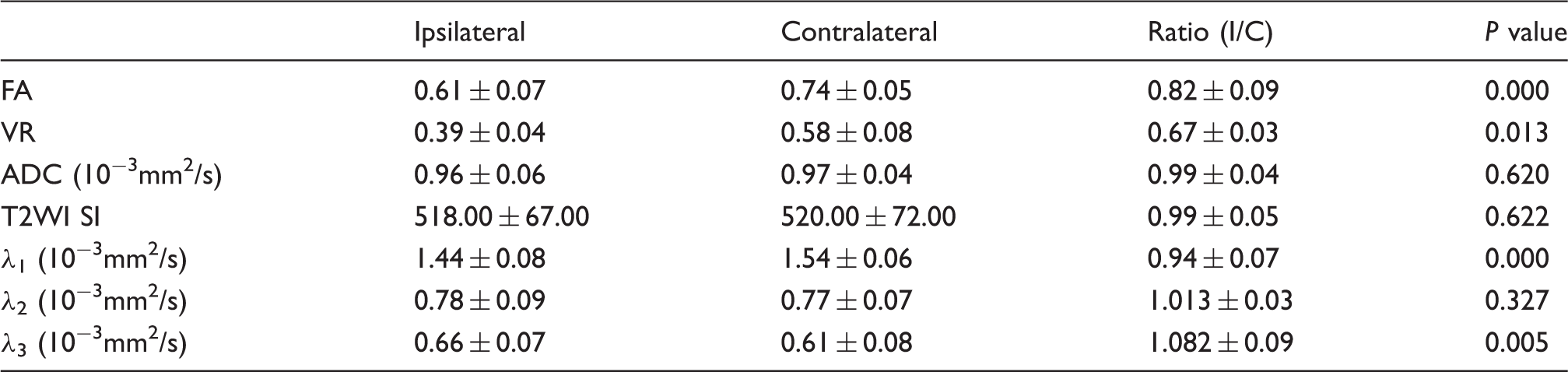
Comparison of the indices between ipsilateral and contralateral sides in study group
Comparison of the indices between ipsilateral (1) and contralateral (C) sides at the cerebral peduncle level in the brains of 25 chronic cerebral stroke patients.
Comparison of the indices between control and study groups
Comparison of the indices between subjects in the study and control groups.
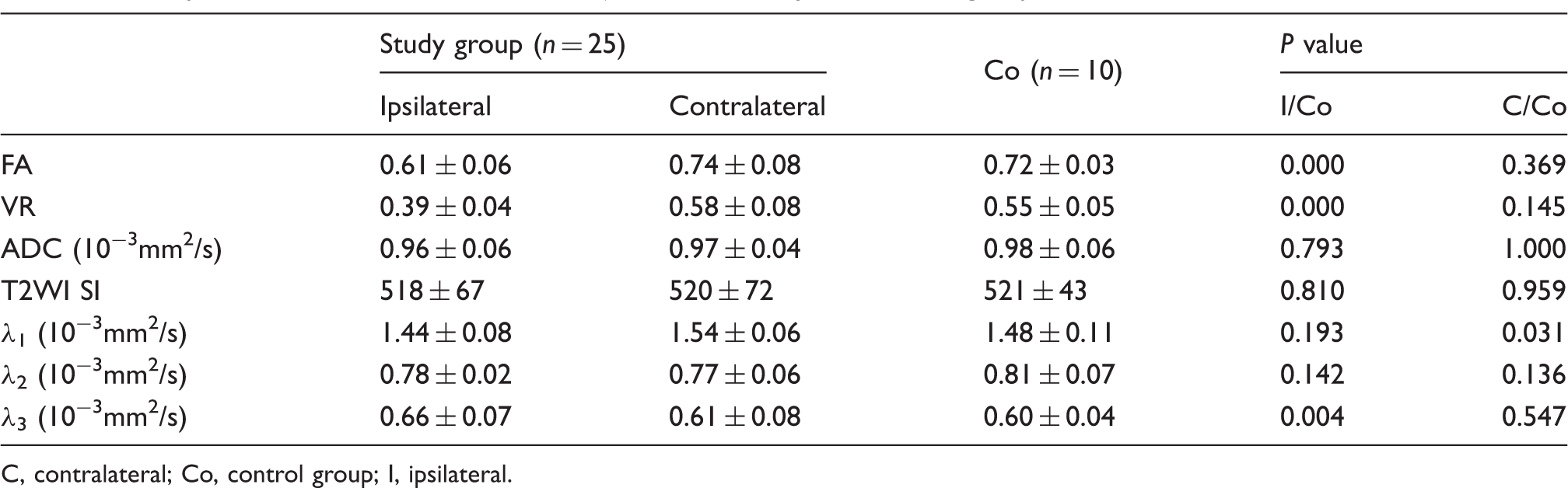
C, contralateral; Co, control group; I, ipsilateral.
Discussion
The occurrence of axonal degeneration in central motor neuron is closely related to the treatment and prognosis of patients with cerebral stroke. Conventional MRI can only show the degeneration-induced morphological changes in some of the patients but fail to quantitatively reveal the degree and extent of the axonal damage of nerve fibers. However, DTI can provide information of the microstructure of these tissues and has the ability to inspect and monitor the structural changes during axonal degeneration of the central motor neurons. Based on available experimental and histopathological data, some scholars have proposed that damages to the structural integrity of adjacent axons and the loss of myelin sheath may occur a few days after the cerebral stroke, while the astrocytic infiltration and chemical degeneration of myelin sheath appear 2 weeks after the brain injury. In a mouse model of cerebral ischemia, researchers have detected degeneration of the descending axons in brain stem by histological staining in the early phase of stroke (2–7), which also confirms the above hypothesis (2). Radlinska et al. have applied positron emission tomography (PET) in studying 21 cases of patients with cerebral stroke within 2 weeks from the onset and shown that there are increased numbers of active, pleomorphic microglia inside the central motor nerve tract adjacent to and underneath the infarct lesion; the authors believe that this is a form of neuronal inflammation (3). The present study has shown that the lower portion of most infarct lesions is located in the central motor nerves at the level of cerebral peduncle in the ipsilateral side. The conventional T1- and T2-weighted images can only reveal that the volume of cerebral peduncle in the ipsilateral side is smaller than that in the contralateral side, but are not able to exactly differentiate the signal abnormalities. To the contrast, FA images of DTI can clearly show the axonal degeneration of central motor neurons at the level of cerebral peduncle, which manifests as the reduction in extent of the high signal of pyramidal tract, the decrease of signal intensity, and morphological changes. Anisotropy analysis of the pyramidal tract indicates that FA values decrease in the stroke side and are significantly different from that in the contralateral side. Therefore, by monitoring the diffusion of water molecules in the pyramidal tract where axonal degeneration occurs, DTI can provide information of the microstructure of these tissues.
It is generally believed that axonal degeneration of the central motor neurons is closely related to the decrease of motor functions and the prognosis of cerebral stroke. Khong et al. have shown that after the occurrence of chronic stroke in middle cerebral artery, FA values of the corticospinal tract in the ipsilateral side, where axonal degeneration has occurred, decrease by 18% compared to that in the contralateral side, and the changes in neurological motor function are significantly related to the changes in FA ratios (r = −0.638, P = 0.035; (4). In addition, Watanabe et al. have studied a group of cerebral stroke patients 3 weeks after the onset and found that DTI with diffusion-sensitizing gradients in three directions can detect the early axonal degeneration in patients with poor prognosis but not in patients with good prognosis (5). Same results are observed in this study too; patients suffering axonal degeneration in the central motor nerves show varying degrees of limb motor dysfunctions in the affected side. In short, axonal degeneration in the descending central motor nerves after cerebral stroke is the important factor causing the decrease in motor function, and such decline in motor function is closely related to the severity of axonal degeneration. The degree and extent of axonal degeneration of the central motor neurons can be used to explain the symptoms of motor function and to evaluate the prognosis, as well as used as a new method to quantitatively evaluate the effectiveness of rehabilitation treatment.
Le Bihan et al. have shown that the degree of anisotropy of the white matter nerve tract reflects the tissue's structural integrity and the restriction of water diffusion by the axonal membrane and myelin sheath; they believe that DTI is the suitable method to study the axonal degeneration of cerebral motor nerves underneath the stroke lesion (6). Our study has used DTI to analyze the axonal degeneration of central motor neurons after chronic cerebral stroke. In the 25 patients, the decrease of anisotropy of the ipsilateral pyramidal tract at the level of cerebral peduncle distal to the primary lesion, the reduction of signal intensity, and the decrease in high signal extent, can all be easily observed in the FA and VR diagrams, which also clearly show the changes of major eigenvectors, i.e. the decrease in largest eigenvalue λ1, and the increase in smallest eigenvalue λ3. Nonetheless, such abnormalities of the central motor neurons cannot be exactly revealed by T1- and T2-weighted images under conventional MRI. Guleria et al. have used DTI to study the corticospinal tract in 22 patients with chronic transection spinal cord injury and found accompanied retrograde axonal degeneration in the corticospinal tract in these patients (7). The study of Sawlani et al. suggests that in the chronic phase of axonal degeneration, the axonal atrophy and degeneration of central motor neurons can be observed under conventional MRI; however, the changes in signal intensity are difficult to differentiate, in particular the signal changes within 4 weeks after the stroke onset cannot be observed using conventional MRI (8,9). ADC imaging, similar to normal DWI, has a high sensitivity and specificity in detecting acute cerebral infarction, which has been consistently recognized by clinicians. However, in this group of cerebral stroke patients with an average follow-up time of 2.5 months, ADC imaging fails to reveal any abnormal signal changes that can reflect the axonal degeneration induced by the chronic cerebral stroke; meanwhile, ADC values in the ipsilateral side in study group show no significant difference from those in the contralateral side of the same group or from those in the control group, indicating that ADC is not as efficient as DTI in detecting the secondary axonal degeneration of central motor neurons in patients with chronic cerebral stroke. Moreover, the advantages of DTI detecting axonal degeneration of the central motor neurons also lie in that it can compose the eigenvector diagram, which provides a clear visual contrast between ipsilateral and contralateral central motor nerves, and that it has the ability to inspect and monitor the structural changes during axonal degeneration of the central motor neurons. In combination with longitudinal DTI imaging, DTI studies can better reveal the clinical evolution mode of cerebral strokes.
There are some uncertainties in this retrospective analysis. First, because the size and location of stroke lesions were not the same in our study, the retrograde axonal degeneration in the corticospinal tract and the related decline in motor function would differ; there was also some bias for DTI to inspect and monitor the structural changes during the axonal degeneration of central motor neurons. Second, this study could not include more clinical significance of DTI, or predict the patients’ final motor scores such as modified Rankin scale, which is due to the difference in stroke lesions. Such relationship between the decline in motor function and the severity of axonal degeneration is complex. DTI may be used to explain the symptoms of motor function and to evaluate the prognosis, but it is extremely difficult to quantitatively predict the scores of patient's final motor function. Third, although the size of the infarction might be a significant parameter, this study focused mainly on the location of infarction, i.e. we were only concerned whether the infarction lesions located in the path of central motor nerve fibers, though a number of unresolved issues needed further investigations.
In conclusion, the changes and diffusions of water molecules associated with the axonal degeneration of central motor neurons after chronic cerebral stroke can be detected by DTI, which can directly quantitatively reflect the degree and extent of axonal degeneration of central motor neurons and can compensate the shortcomings of conventional MRI and DWI, both of which cannot directly show the axonal degeneration of central motor neurons.
Footnotes
Funding
This study was supported by a research grant (N20110452) from the Department of Education of Zhejiang province, a research grant (N20070250) from Health Bureau of Zhejiang, the Fundamental Research Funds for the Central Universities, Ministry of Education, and the 985 Engineering Funds for Zhejiang University, Ministry of Education, China.